
Comparison of COVID-19 and Influenza-Related Outcomes in the United States during Fall–Winter 2022–2023: A Cross-Sectional Retrospective Study

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Data Sources
2.2. Cohort Construction
2.3. Patient Characteristics
2.4. Study Outcomes
2.5. Data Analysis
3. Results
3.1. Incidence Rate of COVID-19 or Influenza-Related Outcomes
3.2. COVID-19 and Influenza-Related Hospitalizations by Age
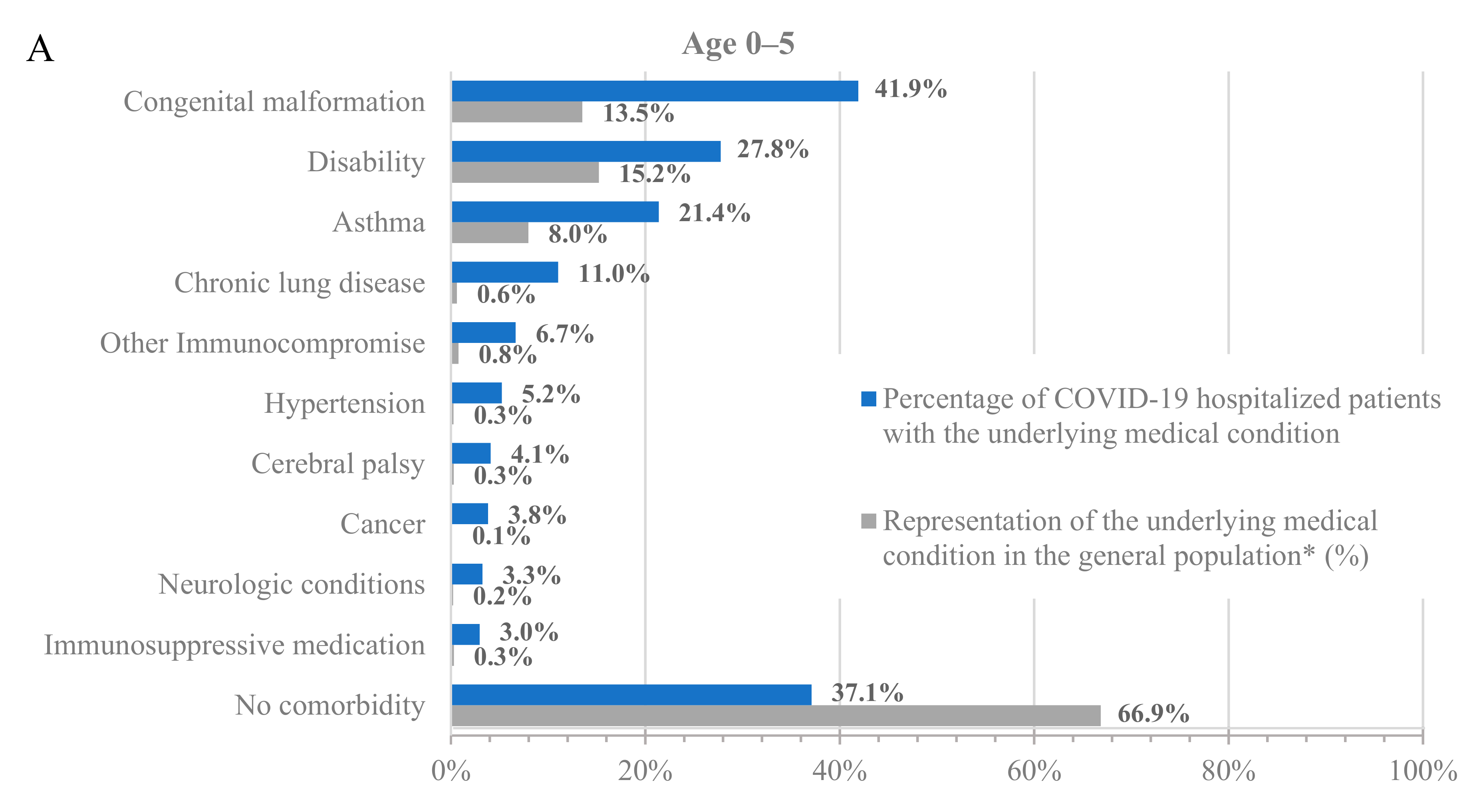
3.3. COVID-19 Hospitalizations by Underlying Medical Conditions
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y.; et al. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Lai, S.; Gao, G.F.; Shi, W. The emergence, genomic diversity and global spread of SARS-CoV-2. Nature 2021, 600, 408–418. [Google Scholar] [CrossRef] [PubMed]
- Markov, P.V.; Ghafari, M.; Beer, M.; Lythgoe, K.; Simmonds, P.; Stilianakis, N.I.; Katzourakis, A. The evolution of SARS-CoV-2. Nat. Rev. Microbiol. 2023, 21, 361–379. [Google Scholar] [CrossRef] [PubMed]
- Epic Research. Respiratory Illnesses. Epic Research. 31 August 2023. Available online: https://epicresearch.org/data-tracker/respiratory-illnesses (accessed on 2 September 2023).
- Seibold, M.A.; Moore, C.M.; Everman, J.L.; Williams, B.J.; Nolin, J.D.; Fairbanks-Mahnke, A.; Plender, E.G.; Patel, B.B.; Arbes, S.J.; Bacharier, L.B.; et al. Risk factors for SARS-CoV-2 infection and transmission in households with children with asthma and allergy: A prospective surveillance study. J. Allergy Clin. Immunol. 2022, 150, 302–311. [Google Scholar] [CrossRef] [PubMed]
- Silk, B.J.; Scobie, H.M.; Duck, W.M.; Palmer, T.; Ahmad, F.B.; Binder, A.M.; Cisewski, J.A.; Kroop, S.; Soetebier, K.; Park, M.; et al. COVID-19 Surveillance After Expiration of the Public Health Emergency Declaration―United States, May 11, 2023. MMWR Morb. Mortal. Wkly. Rep. 2023, 72, 523–528. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. COVID-NET: COVID-19-Associated Hospitalization Surveillance Network. Available online: https://gis.cdc.gov/grasp/covidnet/COVID19_3.html (accessed on 2 September 2023).
- Centers for Disease Control and Prevention. FluSurv-NET: Influenza Hospitalization Surveillance Network. Available online: https://gis.cdc.gov/GRASP/Fluview/FluHospRates.html (accessed on 2 September 2023).
- Fried, M.W.; Crawford, J.M.; Mospan, A.R.; Watkins, S.E.; Munoz, B.; Zink, R.C.; Elliott, S.; Burleson, K.; Landis, C.; Reddy, K.R.; et al. Patient Characteristics and Outcomes of 11721 Patients with Coronavirus Disease 2019 (COVID-19) Hospitalized Across the United States. Clin. Infect. Dis. 2021, 72, e558–e565. [Google Scholar] [CrossRef] [PubMed]
- Harrison, S.L.; Fazio-Eynullayeva, E.; Lane, D.A.; Underhill, P.; Lip, G.Y.H. Comorbidities associated with mortality in 31,461 adults with COVID-19 in the United States: A federated electronic medical record analysis. PLoS Med. 2020, 17, e1003321. [Google Scholar] [CrossRef]
- Marin, B.G.; Aghagoli, G.; Lavine, K.; Yang, L.; Siff, E.J.; Chiang, S.S.; Salazar-Mather, T.P.; Dumenco, L.; Savaria, M.C.; Aung, S.N.; et al. Predictors of COVID-19 severity: A literature review. Rev. Med. Virol. 2021, 31, 1–10. [Google Scholar] [CrossRef]
- Hernandez-Romieu, A.C.; Carton, T.W.; Saydah, S.; Azziz-Baumgartner, E.; Boehmer, T.K.; Garret, N.Y.; Bailey, L.C.; Cowell, L.G.; Draper, C.; Mayer, K.H.; et al. Prevalence of Select New Symptoms and Conditions Among Persons Aged Younger than 20 Years and 20 Years or Older at 31 to 150 Days after Testing Positive or Negative for SARS-CoV-2. JAMA Netw. Open 2022, 5, e2147053. [Google Scholar] [CrossRef]
- Bowe, B.; Xie, Y.; Al-Aly, Z. Postacute sequelae of COVID-19 at 2 years. Nat. Med. 2023, 29, 2347–2357. [Google Scholar] [CrossRef]
- Ballouz, T.; Menges, D.; Anagnostopoulos, A.; Domenghino, A.; Aschmann, H.E.; Frei, A.; Fehr, J.S.; Puhan, M.A. Recovery and symptom trajectories up to two years after SARS-CoV-2 infection: Population based, longitudinal cohort study. BMJ 2023, 381, e074425. [Google Scholar] [CrossRef] [PubMed]
- National Center for Health Statistics. U.S. Census Bureau, Household Pulse Survey, 2022–2023. Long COVID. 29 August 2023. Available online: https://www.cdc.gov/nchs/covid19/pulse/long-covid.htm (accessed on 8 September 2023).
- Zhang, V.; Fisher, M.; Hou, W.; Zhang, L.; Duong, T.Q. Incidence of New-Onset Hypertension Post–COVID-19: Comparison with Influenza. Hypertension 2023, 80, 2135–2148. [Google Scholar] [CrossRef] [PubMed]
- Scobie, H.M.; Johnson, A.G.; Suthar, A.B.; Severson, R.; Alden, N.B.; Balter, S.; Bertolino, D.; Blythe, D.; Brady, S.; Cadwell, B.; et al. Monitoring Incidence of COVID-19 Cases, Hospitalizations, and Deaths, by Vaccination Status—13 U.S. Jurisdictions, April 4–July 17, 2021. MMWR Morb. Mortal. Wkly. Rep. 2021, 70, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Tsampasian, V.; Elghazaly, H.; Chattopadhyay, R.; Debski, M.; Naing, T.K.P.; Garg, P.; Clark, A.; Ntatsaki, E.; Vassiliou, V.S. Risk Factors Associated With Post−COVID-19 Condition: A systematic review and meta-analysis. AMA Intern. Med. 2023, 183, 566–580. [Google Scholar] [CrossRef] [PubMed]
- Pegu, A.; Schmidt, S.D.; O’Dell, S.; Talana, C.A.; Lai, L.; Albert, J.; Bennett, H.; Corbett, K.S.; Flach, B.; Leav, B.; et al. Durability of mRNA-1273 vaccine–induced antibodies against SARS-CoV-2 variants. Science 2021, 373, 1372–1377. [Google Scholar] [CrossRef]
- Andrews, N.; Tessier, E.; Stowe, J.; Gower, C.; Kirsebom, F.; Simmons, R.; Gallagher, E.; Thelwall, S.; Groves, N.; Dabrera, G.; et al. Duration of Protection against Mild and Severe Disease by Covid-19 Vaccines. N. Engl. J. Med. 2022, 386, 340–350. [Google Scholar] [CrossRef] [PubMed]
- Chalkias, S.; McGhee, N.; Whatley, J.L.; Essink, B.; Brosz, A.; Tomassini, J.E.; Girard, B.; Wu, K.; Edwards, D.K.; Nasir, A.; et al. Safety and Immunogenicity of XBB.1.5-Containing mRNA Vaccines. medRxiv 2023, medRxiv:2023.08.22.23293434. [Google Scholar] [CrossRef]
- Johnson, A.G.; Amin, A.B.; Ali, A.R.; Hoots, B.; Cadwell, B.L.; Arora, S.; Avoundjian, T.; Awofeso, A.O.; Barnes, J.; Bayoumi, N.S.; et al. COVID-19 Incidence and Death Rates Among Unvaccinated and Fully Vaccinated Adults with and Without Booster Doses During Periods of Delta and Omicron Variant Emergence—25 U.S. Jurisdictions, April 4–December 25, 2021. MMWR. Morb. Mortal. Wkly. Rep. 2022, 71, 132–138. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. COVID Data Tracker. 2 September 2023. Available online: https://covid.cdc.gov/covid-data-tracker/ (accessed on 2 September 2023).
- Centers for Disease Control and Prevention. COVID Data Tracker—Vaccinations. Centers for Disease Control and Prevention. 13 October 2023. Available online: https://covid.cdc.gov/covid-data-tracker/#vaccination-states-jurisdictions (accessed on 8 November 2023).
- Centers for Disease Control and Prevention. Influenza Vaccination Coverage, Adults. 27 April 2023. Available online: https://www.cdc.gov/flu/fluvaxview/dashboard/vaccination-adult-coverage.html (accessed on 3 September 2023).
- Boikos, C.; Imran, M.; De Lusignan, S.; Ortiz, J.R.; Patriarca, P.A.; Mansi, J.A. Integrating Electronic Medical Records and Claims Data for Influenza Vaccine Research. Vaccines 2022, 10, 727. [Google Scholar] [CrossRef]
- McGovern, I.; Bogdanov, A.; Cappell, K.; Whipple, S.; Haag, M. Influenza Vaccine Uptake in the United States before and during the COVID-19 Pandemic. Vaccines 2022, 10, 1610. [Google Scholar] [CrossRef]
- Imran, M.; Ortiz, J.R.; McLean, H.Q.; Fisher, L.; O’Brien, D.; Bonafede, M.; Mansi, J.A.; Boikos, C. Relative Effectiveness of Cell-Based Versus Egg-Based Quadrivalent Influenza Vaccines in Adults During the 2019–2020 Influenza Season in the United States. Open Forum Infect. Dis. 2022, 9, ofac532. [Google Scholar] [CrossRef] [PubMed]
- Nguyen, V.H.; Boileau, C.; Bogdanov, A.; Sredl, M.; Bonafede, M.; Ducruet, T.; Chavers, S.; Rosen, A.; Martin, D.; Buck, P.; et al. Relative Effectiveness of BNT162b2, mRNA-1273, and Ad26.COV2.S Vaccines and Homologous Boosting in Preventing COVID-19 in Adults in the US. Open Forum Infect. Dis. 2023, 10, ofad288. [Google Scholar] [CrossRef] [PubMed]
- Santo, L.; Kang, K. National Hospital Ambulatory Medical Care Survey: 2019 National Summary Tables; National Center for Health Statistics (U.S.): Hyattsville, MD, USA, 2023; Volume 76. Available online: https://stacks.cdc.gov/view/cdc/123251 (accessed on 12 September 2023).
- Centers for Disease Control and Prevention. Underlying Medical Conditions Associated with Higher Risk for Severe COVID-19: Information for Healthcare Professionals. 9 February 2023. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/clinical-care/underlyingconditions.html (accessed on 5 September 2023).
- Ajufo, E.; Rao, S.; Navar, A.M.; Pandey, A.; Ayers, C.R.; Khera, A.U.S. population at increased risk of severe illness from COVID-19. Am. J. Prev. Cardiol. 2021, 6, 100156. [Google Scholar] [CrossRef] [PubMed]
- Delahoy, M.J.; Ujamaa, D.; Taylor, C.A.; Cummings, C.; Anglin, O.; Holstein, R.; Milucky, J.; O’Halloran, A.; Patel, K.; Pham, H.; et al. Comparison of Influenza and Coronavirus Disease 2019–Associated Hospitalizations Among Children Younger Than 18 Years Old in the United States: FluSurv-NET (October–April 2017–2021) and COVID-NET (October 2020–September 2021). Clin. Infect. Dis. 2023, 76, e450–e459. [Google Scholar] [CrossRef] [PubMed]
- Havers, F.P. COVID-19–Associated Hospitalizations among Infants, Children and Adults—COVID-NET, January–August 2023. In Proceedings of the ACIP COVID-19 Vaccines Work Group, Online, 12 September 2023; Available online: https://www.cdc.gov/vaccines/acip/meetings/downloads/slides-2023-09-12/03-COVID-Havers-508.pdf (accessed on 11 October 2023).
- Setayeshgar, S.; Wilton, J.; Sbihi, H.; Zandy, M.; Janjua, N.; Choi, A.; Smolina, K. Comparison of influenza and COVID-19 hospitalisations in British Columbia, Canada: A population-based study. BMJ Open Respir. Res. 2023, 10, e001567. [Google Scholar] [CrossRef] [PubMed]
- Donnino, M.W.; Moskowitz, A.; Thompson, G.S.; Heydrick, S.J.; Pawar, R.D.; Berg, K.M.; Mehta, S.; Patel, P.V.; Grossestreuer, A.V. Comparison between Patients Hospitalized with Influenza and COVID-19 at a Tertiary Care Center. J. Gen. Intern. Med. 2021, 36, 1689–1695. [Google Scholar] [CrossRef]
- Xie, Y.; Choi, T.; Al-Aly, Z. Risk of Death in Patients Hospitalized for COVID-19 vs Seasonal Influenza in Fall-Winter 2022–2023. JAMA 2023, 329, 1697–1699. [Google Scholar] [CrossRef] [PubMed]
- Lauring, A.S.; Tenforde, M.W.; Chappell, J.D.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D.; et al. Clinical severity of, and effectiveness of mRNA vaccines against, covid-19 from omicron, delta, and alpha SARS-CoV-2 variants in the United States: Prospective observational study. BMJ 2022, 376, e069761. [Google Scholar] [CrossRef]
- Lauring, A.S.; Hodcroft, E.B. Genetic Variants of SARS-CoV-2—What Do They Mean? JAMA 2021, 325, 529–531. [Google Scholar] [CrossRef]
- Bruxvoort, K.J.; Sy, L.S.; Qian, L.; Ackerson, B.K.; Luo, Y.; Lee, G.S.; Tian, Y.; Florea, A.; Takhar, H.S.; Tubert, J.E.; et al. Real-world effectiveness of the mRNA-1273 vaccine against COVID-19: Interim results from a prospective observational cohort study. Lancet Reg. Health Am. 2022, 6, 100134. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Weber, Z.A.; Natarajan, K.; Klein, N.P.; Kharbanda, A.B.; Stenehjem, E.; Embi, P.J.; Reese, S.E.; Naleway, A.L.; Grannis, S.J.; et al. Early Estimates of Bivalent mRNA Vaccine Effectiveness in Preventing COVID-19–Associated Emergency Department or Urgent Care Encounters and Hospitalizations Among Immunocompetent Adults—VISION Network, Nine States, September–November 2022. MMWR Morb. Mortal. Wkly. Rep. 2022, 71, 1616–1624. [Google Scholar] [CrossRef]
- Sedgley, R.; Winer-Jones, J.; Bonafede, M. Long COVID Incidence in a Large US Ambulatory Electronic Health Record System. Am. J. Epidemiol. 2023, 192, 1350–1357. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention. Influenza Activity in the United States during the 2022–23 Season and Composition of the 2023–24 Influenza Vaccine. 28 September 2023. Available online: https://www.cdc.gov/flu/spotlights/2023-2024/22-23-summary-technical-report.htm (accessed on 11 October 2023).




{kind=link}
{kind=link}
{kind=link}
| All Patients | ||
|---|---|---|
| N = 23,526,196 | ||
| Characteristics | N | % |
| Female sex | 13,634,220 | 58.0% |
| Age | ||
| 0–5 | 506,690 | 2.2% |
| 6–17 | 2,794,168 | 11.9% |
| 18–49 | 9,717,350 | 41.3% |
| 50–64 | 5,737,529 | 24.4% |
| 65+ | 4,770,459 | 20.3% |
| Underlying medical conditions a | ||
| Hypertension | 6,824,263 | 29.0% |
| Obesity (body mass index > 30) | 4,942,037 | 21.0% |
| Musculoskeletal conditions | 3,772,098 | 16.0% |
| Mental health disorders | 3,504,546 | 14.9% |
| Diabetes | 3,254,728 | 13.8% |
| Smoking (current and former) | 2,802,473 | 11.9% |
| Asthma | 1,998,127 | 8.5% |
| Heart disease | 1,918,234 | 8.2% |
| Chronic lung disease | 1,238,751 | 5.3% |
| ADHD | 1,139,822 | 4.8% |
| Chronic kidney disease | 1,112,167 | 4.7% |
| Cancer | 991,733 | 4.2% |
| Cerebrovascular disease | 807,423 | 3.4% |
| Congenital malformation | 736,570 | 3.1% |
| Immunosuppressive medications | 719,139 | 3.1% |
| Outcome | COVID-19 | Influenza | Incidence Ratio of COVID-19 to Influenza | ||||
|---|---|---|---|---|---|---|---|
| N = 1,179,960 | N = 698,002 | ||||||
| N | % a | Incidence b (95% CI) | N | % a | Incidence b (95% CI) | ||
| Outpatient visits (other) | 283,213 | 24.0% * | 1204 (1199–1208) | 50,835 | 7.3% | 216 (214–218) | 5.6 |
| Urgent care visit | 631,356 | 53.5% * | 2684 (2677–2690) | 486,406 | 69.7% | 2068 (2062–2073) | 1.3 |
| ED visit | 171,503 | 14.5% * | 729 (726–732) | 140,200 | 20.1% | 596 (593–599) | 1.2 |
| Hospitalization c | 82,234 | 7.0% * | 350 (347–352) | 18,032 | 2.6% | 77 (76–78) | 4.6 |
| ICU | 11,654 | 1.0% * | 50 (49–50) | 2529 | 0.4% | 11 (10–11) | 4.6 |
| Age Group | COVID-19 | Influenza | Count Ratio of COVID-19 vs. Influenza |
|---|---|---|---|
| N = 93,888 | N = 20,561 | ||
| N | N | ||
| Pediatrics | |||
| 0–5 | 706 * | 564 | 1.3 |
| 6–17 | 1529 * | 1260 | 1.2 |
| Adults | |||
| 18–49 | 26,242 * | 4693 | 5.6 |
| 50–64 | 22,947 * | 5529 | 4.2 |
| Older Adults | |||
| 65+ | 42,464 * | 8515 | 5 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kopel, H.; Bogdanov, A.; Winer-Jones, J.P.; Adams, C.; Winer, I.H.; Bonafede, M.; Nguyen, V.H.; Mansi, J.A. Comparison of COVID-19 and Influenza-Related Outcomes in the United States during Fall–Winter 2022–2023: A Cross-Sectional Retrospective Study. Diseases 2024, 12, 16. https://doi.org/10.3390/diseases12010016
Kopel H, Bogdanov A, Winer-Jones JP, Adams C, Winer IH, Bonafede M, Nguyen VH, Mansi JA. Comparison of COVID-19 and Influenza-Related Outcomes in the United States during Fall–Winter 2022–2023: A Cross-Sectional Retrospective Study. Diseases. 2024; 12(1):16. https://doi.org/10.3390/diseases12010016
Chicago/Turabian StyleKopel, Hagit, Alina Bogdanov, Jessamine P. Winer-Jones, Christopher Adams, Isabelle H. Winer, Machaon Bonafede, Van Hung Nguyen, and James A. Mansi. 2024. "Comparison of COVID-19 and Influenza-Related Outcomes in the United States during Fall–Winter 2022–2023: A Cross-Sectional Retrospective Study" Diseases 12, no. 1: 16. https://doi.org/10.3390/diseases12010016