

Istaroxime for Patients with Acute Heart Failure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials

 , , , ,
, , , ,  and
and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Protocol Registration
2.2. Data Sources and Search Strategy
2.3. Eligibility Criteria and Study Selection
2.4. Study Selection
2.5. Data Extraction
2.6. Risk of Bias and Certainty of Evidence
2.7. Statistical Analysis
3. Results
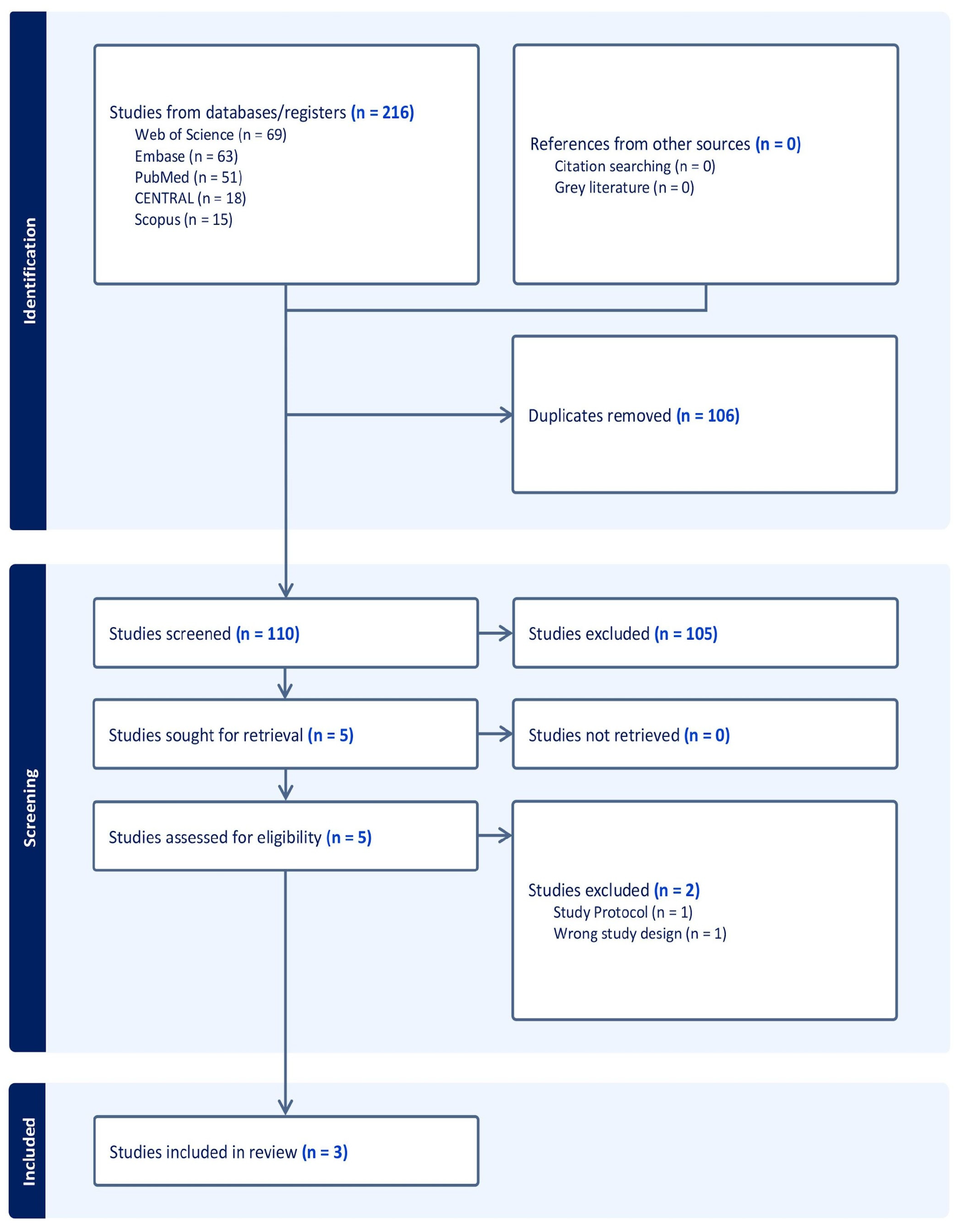
3.1. Search Results and Study Selection
3.2. Characteristics of the Included Studies
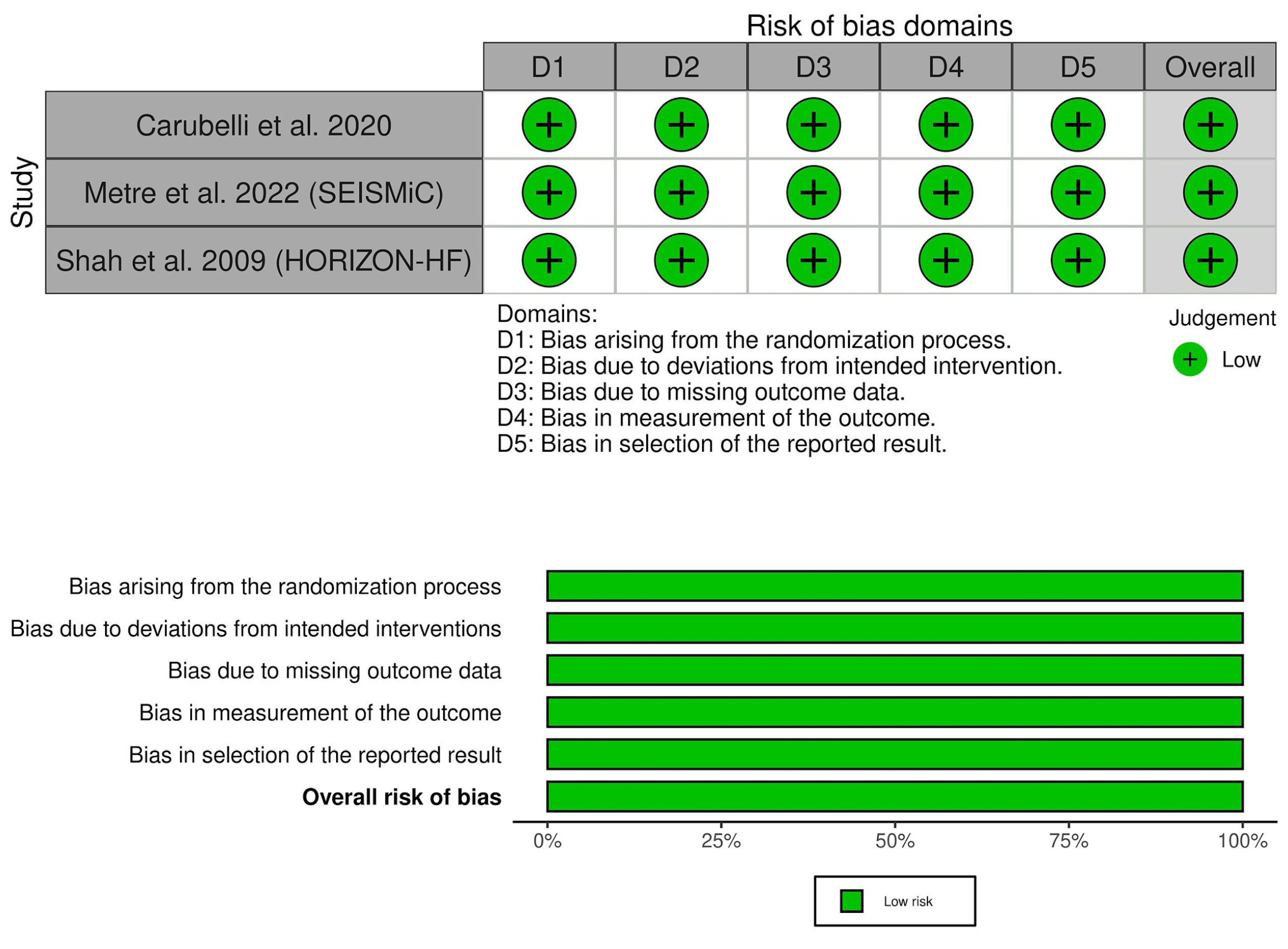
3.3. Risk of Bias and Certainty of Evidence
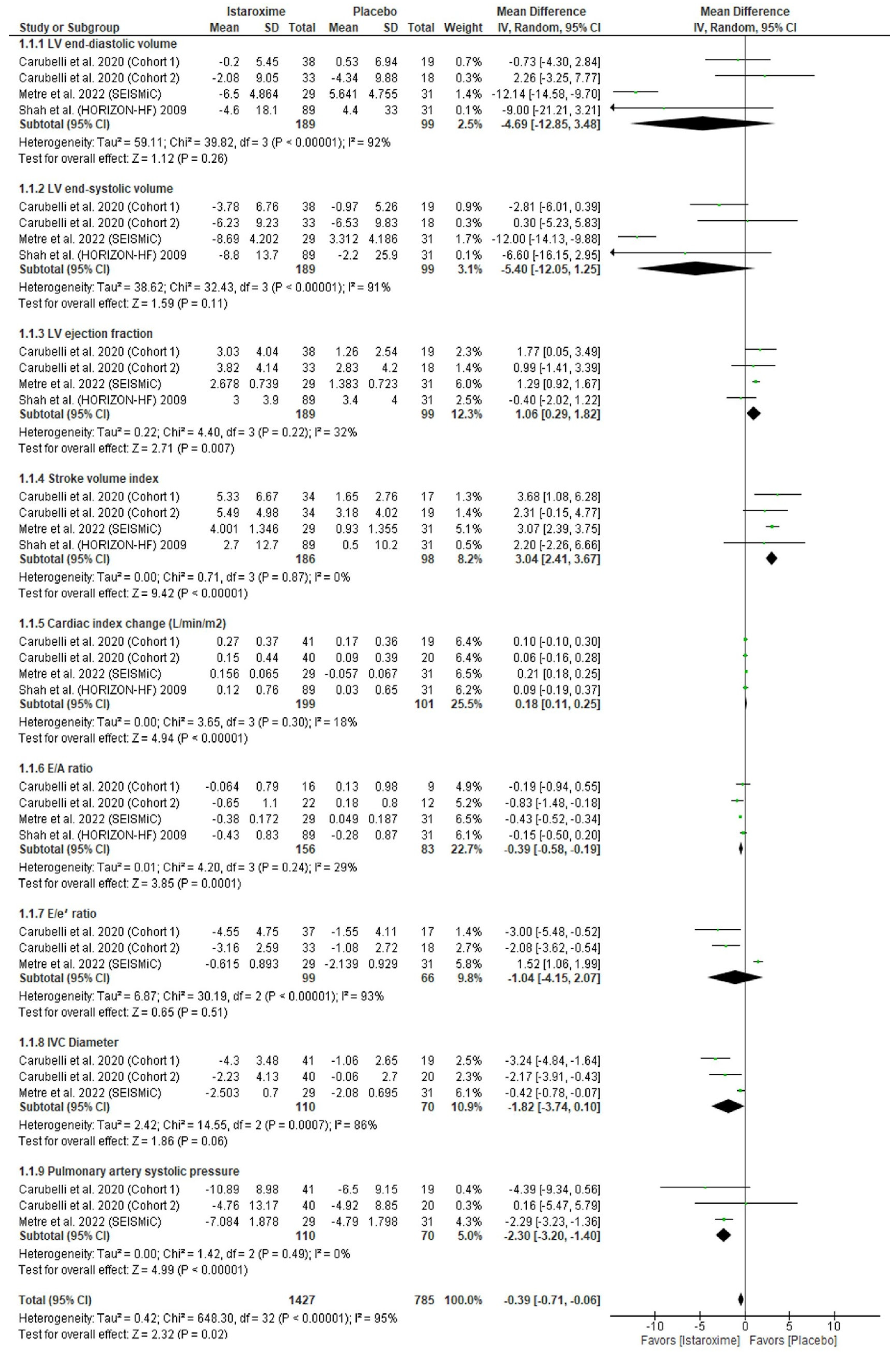
3.4. Echocardiographic Parameters
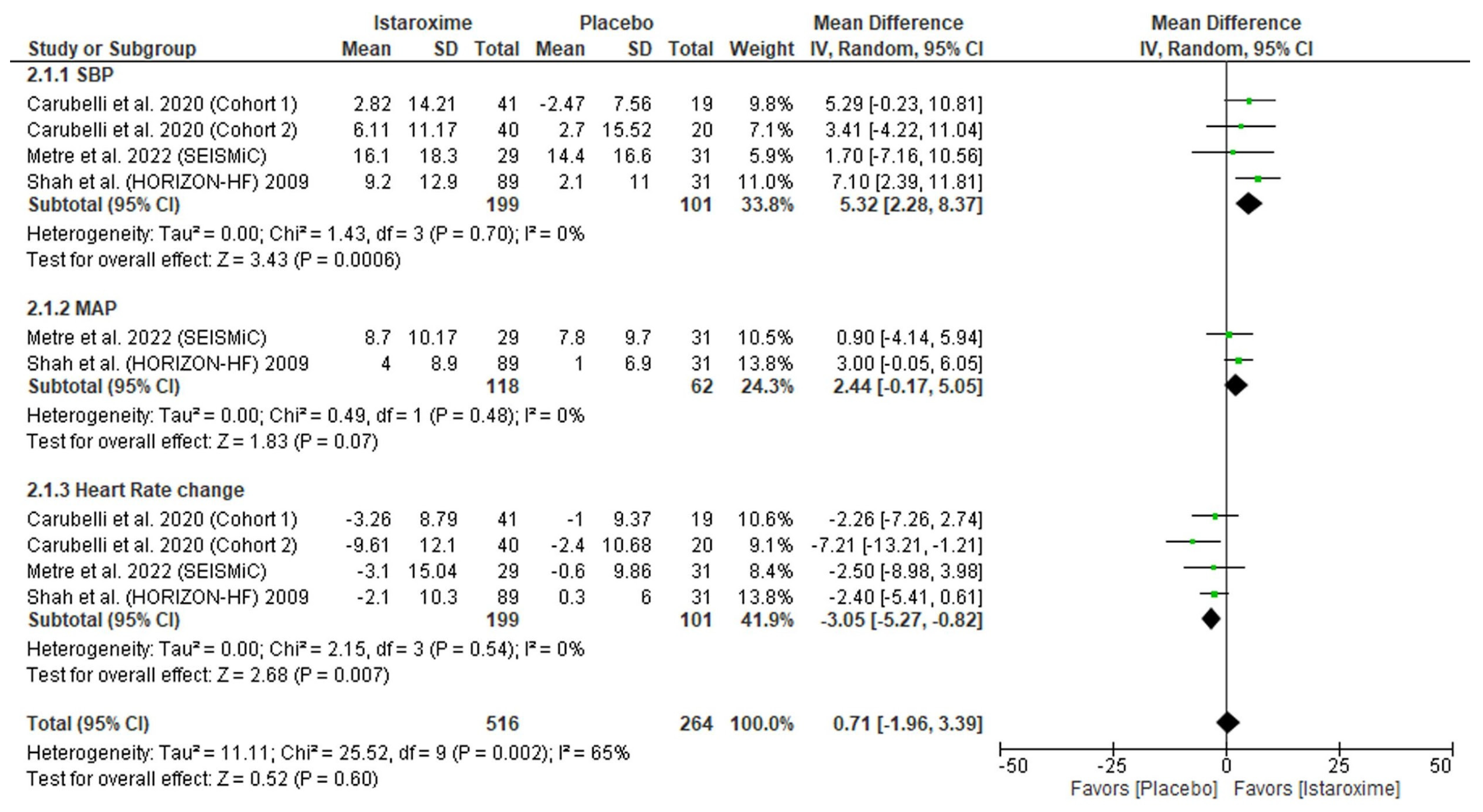
3.5. Hemodynamic Parameters
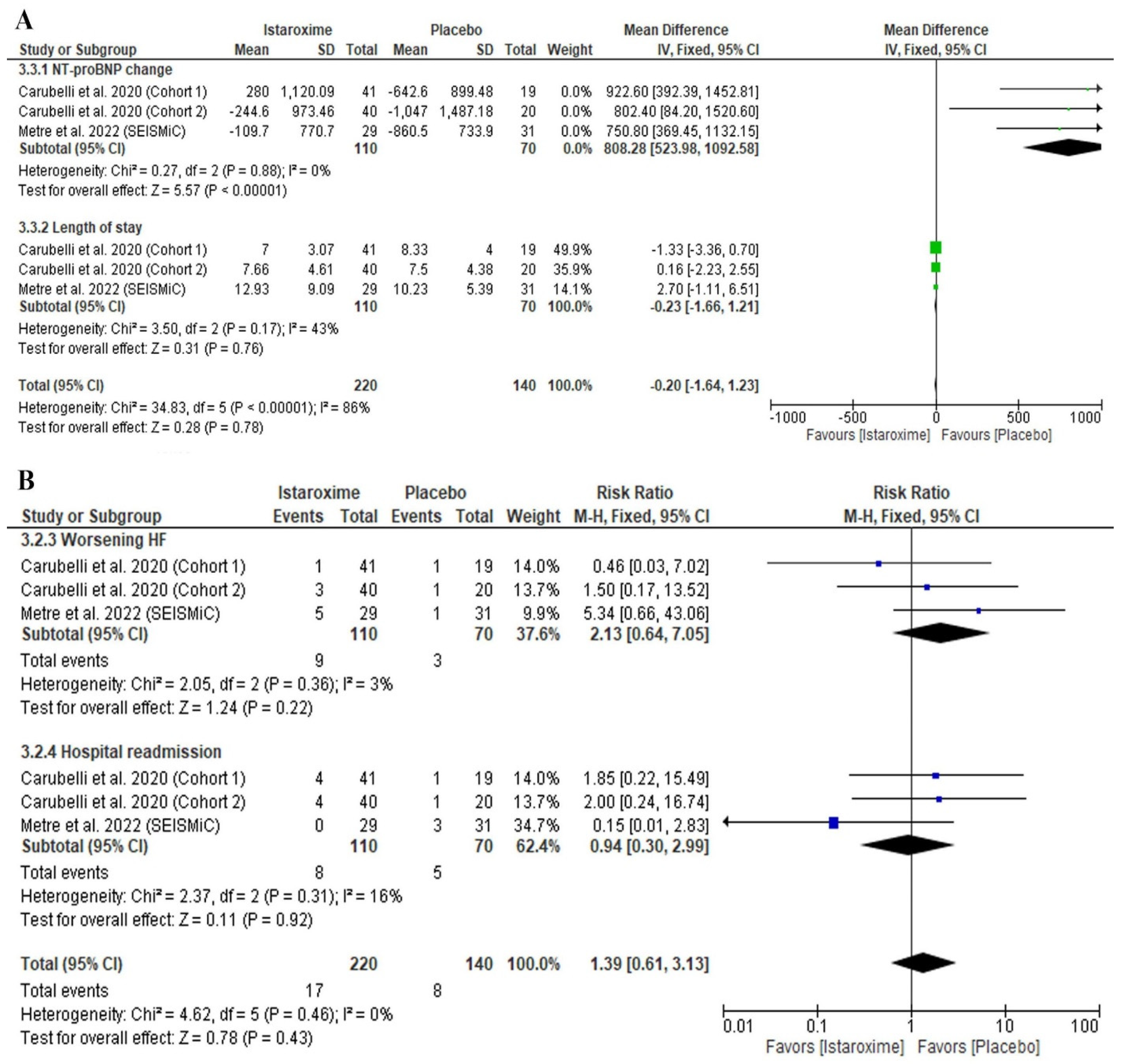
3.6. Clinical Parameters
3.7. Safety Outcomes
4. Discussion
Strengths and Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
| ACA/AHA | American College of Cardiology/American Heart Association |
| AF | Atrial fibrillation |
| AHF | Acute heart failure |
| BMI | Body mass index |
| bpm | Beats per minute |
| CABG | Coronary artery bypass graft |
| CI | Confidence interval |
| CKD | Chronic kidney disease |
| CS | Cardiogenic shock |
| DIG | Digitalis Investigation Group |
| DBP | Diastolic blood pressure |
| df | Degrees of freedom |
| DM | Diabetes mellitus |
| EC | Excitation–contraction |
| ESC | European Society of Cardiology |
| HFrEF | Heart failure with reduced ejection fraction |
| HR | Heart rate |
| HTN | Hypertension |
| I | Istaroxime |
| IVC | Inferior vena cava |
| ID | Identification |
| L | Liter |
| LV | Left ventricle |
| LVEDV | Left ventricular end-diastolic volume |
| LVEF | Left ventricular ejection fraction |
| LVESV | Left ventricular end-systolic volume |
| M | Mean |
| MAP | Mean arterial pressure |
| MD | Mean difference |
| N | Number |
| NCX | Na+/Ca+2 exchange |
| p | Probability |
| PICO | Population Intervention Comparison Outcomes |
| Pl | Placebo |
| PCI | Percutaneous coronary intervention |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RCT | Randomized controlled trial |
| SBP | Systolic blood pressure |
| SCAI | Society of Cardiovascular Angiography and Interventions |
| SD | Standard deviation |
| SERCA2a | Sarcoplasmic reticulum Ca+2 adenosine triphosphatase isoform 2a |
| US | United States |
| . (period) | Missing data. |
References
- Tsao, C.W.; Aday, A.W.; Almarzooq, Z.I.; Alonso, A.; Beaton, A.Z.; Bittencourt, M.S.; Boehme, A.K.; Buxton, A.E.; Carson, A.P.; Commodore-Mensah, Y.; et al. Heart Disease and Stroke Statistics--2022 Update: A report from the American Heart Association. Circulation 2022, 145, E153–E639. [Google Scholar] [CrossRef] [PubMed]
- GBD 2019 Diseases and Injuries Collaborators. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: A systematic analysis for the Global Burden of Disease Study 2019. Lancet 2020, 396, 1204–1222. [Google Scholar] [CrossRef]
- Yusuf, S.; Reddy, S.; Ôunpuu, S.; Anand, S. Global burden of cardiovascular diseases: Part I: General considerations, the epidemiologic transition, risk factors, and impact of urbanization. Circulation 2001, 104, 2746–2753. [Google Scholar] [CrossRef] [PubMed]
- McDonagh, T.A.; Metra, M.; Adamo, M.; Gardner, R.S.; Baumbach, A.; Böhm, M.; Burri, H.; Butler, J.; Čelutkienė, J.; Chioncel, O.; et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure. Eur. Heart J. 2021, 42, 3599–3726. [Google Scholar] [CrossRef]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: Executive Summary: A report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. J. Am. Coll. Cardiol. 2022, 79, 1757–1780. [Google Scholar] [CrossRef] [PubMed]
- Gheorghiade, M.; Abraham, W.T.; Albert, N.M.; Greenberg, B.H.; O’Connor, C.M.; She, L.; Stough, W.G.; Yancy, C.W.; Young, J.B.; Fonarow, G.C. Systolic blood pressure at admission, clinical characteristics, and outcomes in patients hospitalized with acute heart failure. JAMA 2006, 296, 2217–2226. [Google Scholar] [CrossRef] [PubMed]
- van Diepan, S.; Katz, J.N.; Albert, N.M.; Henry, T.D.; Jacobs, A.K.; Kapur, N.K.; Kilic, A.; Menon, V.; Ohman, E.M.; Sweitzer, N.K.; et al. Contemporary management of cardiogenic shock: A scientific statement from the American Heart Association. Circulation 2017, 136, e232–e268. [Google Scholar] [CrossRef] [PubMed]
- Chioncel, O.; Parissis, J.; Mebazaa, A.; Thiele, H.; Desch, S.; Bauersachs, J.; Harjola, V.P.; Antohi, E.L.; Arrigo, M.; Ben Gal, T.; et al. Epidemiology, pathophysiology and contemporary management of cardiogenic shock—A position statement from the Heart Failure Association of the European Society of Cardiology. Eur. J. Heart Fail. 2020, 22, 1315–1341. [Google Scholar] [CrossRef]
- Baran, D.A.; Grines, C.L.; Bailey, S.; Burkhoff, D.; Hall, S.A.; Henry, T.D.; Hollenberg, S.M.; Kapur, N.K.; O’Neill, W.; Ornato, J.P.; et al. SCAI clinical expert consensus statement on the classification of cardiogenic shock: This document was endorsed by the American College of Cardiology (ACC), the American Heart Association (AHA), the Society of Critical Care Medicine (SCCM), and the Society of Thoracic Surgeons (STS) in April 2019. Catheter. Cardiovasc. Interv. 2019, 94, 29–37. [Google Scholar] [CrossRef]
- Singh, T.; Samson, R.; Ayinapudi, K.; Motwani, A.; Le Jemtel, T.H. Precardiogenic shock: A new clinical entity. Cardiol. Rev. 2019, 27, 198–201. [Google Scholar] [CrossRef]
- Mebazaa, A.; Nieminen, M.S.; Packer, M.; Cohen-Solal, A.; Kleber, F.X.; Pocock, S.J.; Thakkar, R.; Padley, R.J.; Põder, P.; Kivikko, M.; et al. Levosimendan vs dobutamine for patients with acute decompensated heart failure: The SURVIVE Randomized Trial. JAMA 2007, 297, 1883–1891. [Google Scholar] [CrossRef] [PubMed]
- Maack, C.; Eschenhagen, T.; Hamdani, N.; Heinze, F.R.; Lyon, A.R.; Manstein, D.J.; Metzger, J.; Papp, Z.; Tocchetti, C.G.; Yilmaz, M.B.; et al. Treatments targeting inotropy. Eur. Heart J. 2019, 40, 3626–3644. [Google Scholar] [CrossRef] [PubMed]
- Micheletti, R.; Palazzo, F.; Barassi, P.; Giacalone, G.; Ferrandi, M.; Schiavone, A.; Moro, B.; Parodi, O.; Ferrari, P.; Bianchi, G. Istaroxime, a stimulator of sarcoplasmic reticulum calcium adenosine triphosphatase isoform 2a activity, as a novel yherapeutic approach to heart failure. Am. J. Cardiol. 2007, 99, S24–S32. [Google Scholar] [CrossRef] [PubMed]
- Mattera, G.G.; Lo Giudice, P.; Loi, F.M.P.; Vanoli, E.; Gagnol, J.P.; Borsini, F.; Carminati, P. Istaroxime: A new luso-inotropic agent for heart failure. Am. J. Cardiol. 2007, 99, S33–S40. [Google Scholar] [CrossRef] [PubMed]
- Gheorghiade, M.; Sabbah, H.N. Istaroxime: An investigational luso-inotropic agent for acute heart failure syndromes. Am. J. Cardiol. 2007, 99, 1A–3A. [Google Scholar] [CrossRef] [PubMed]
- Teerlink, J.R.; Metra, M.; Zacà, V.; Sabbath, H.N.; Cotter, G.; Gheorghiade, M.; Cas, L.D. Agents with inotropic properties for the management of acute heart failure syndromes. Traditional agents and beyond. Heart Fail. Rev. 2009, 14, 243–253. [Google Scholar] [CrossRef]
- Chioncel, O.; Collins, S.P.; Butler, J. Istaroxime in acute heart failure: The holy grail is at HORIZON? Eur. J. Heart Fail. 2020, 22, 1694–1697. [Google Scholar] [CrossRef]
- Forzano, I.; Mone, P.; Mottola, G.; Kansakar, U.; Salemme, L.; De Luca, A.; Tesorio, T.; Varzideh, F.; Santulli, G. Efficacy of the new inotropic agent istaroxime in acute heart failure. J. Clin. Med. 2022, 11, 7503. [Google Scholar] [CrossRef]
- Metra, M.; Chioncel, O.; Cotter, G.; Davison, B.; Filippatos, G.; Mebazaa, A.; Novosadova, M.; Ponikowski, P.; Simmons, P.; Soffer, J.; et al. Safety and efficacy of istaroxime in patients with acute heart failure-related pre-cardiogenic shock—A multicentre, randomized, double-blind, placebo-controlled, parallel group study (SEISMiC). Eur. J. Heart Fail. 2022, 24, 1967–1977. [Google Scholar] [CrossRef]
- Carubelli, V.; Zhang, Y.; Metra, M.; Lombardi, C.; Felker, G.M.; Filippatos, G.; O’Connor, C.M.; Teerlink, J.R.; Simmons, P.; Segal, R.; et al. Treatment with 24 hour istaroxime infusion in patients hospitalised for acute heart failure: A randomised, placebo-controlled trial. Eur. J. Heart Fail. 2020, 22, 1684–1693. [Google Scholar] [CrossRef]
- Shah, S.J.; Blair, J.E.A.; Filippatos, G.S.; MacArie, C.; Ruzyllo, W.; Korewicki, J.; Bubenek-Turconi, S.I.; Ceracchi, M.; Bianchetti, M.; Carminati, P.; et al. Effects of istaroxime on diastolic stiffness in acute heart failure syndromes: Results from the Hemodynamic, Echocardiographic, and Neurohormonal Effects of Istaroxime, a Novel Intravenous Inotropic and Lusitropic Agent: A Randomized Controlled Trial in Patients with Heart Failure (HORIZON-HF) trial. Am. Heart J. 2009, 157, 1035–1041. [Google Scholar] [CrossRef] [PubMed]
- Gheorghiade, M.; Blair, J.E.A.; Filippatos, G.S.; Macarie, C.; Ruzyllo, W.; Korewicki, J.; Bubenek-Turconi, S.I.; Ceracchi, M.; Bianchetti, M.; Carminati, P.; et al. Hemodynamic, echocardiographic, and neurohormonal effects of istaroxime, a novel intravenous inotropic and lusitropic agent: A randomized controlled trial in patients hospitalized with heart failure. J. Am. Coll. Cardiol. 2008, 51, 2276–2285. [Google Scholar] [CrossRef] [PubMed]
- Dec, G.W. Istaroxime in heart failure new hope or more hype. J. Am. Coll. Cardiol. 2008, 51, 2286–2288. [Google Scholar] [CrossRef] [PubMed]
- Khalid Khan, S.; Rawat, A.; Khan, Z.; Reyaz, I.; Kumar, V.; Batool, S.; Yadav, R.; Hirani, S. Safety and efficacy of istaroxime in patients with acute heart failure: A meta-analysis of randomized controlled trials. Cureus 2023, 15, e41084. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Kunz, R.; Vist, G.E.; Falck-Ytter, Y.; Schünemann, H.J. What is “quality of evidence” and why is it important to clinicians? BMJ 2008, 336, 995. [Google Scholar] [CrossRef] [PubMed]
- Guyatt, G.H.; Oxman, A.D.; Vist, G.E.; Kunz, R.; Falck-Ytter, Y.; Alonso-Coello, P.; Schünemann, H.J. GRADE: An emerging consensus on rating quality of evidence and strength of recommendations. BMJ 2008, 336, 924. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372. [Google Scholar] [CrossRef]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. Cochrane Handbook for Systematic Reviews of Interventions, 2nd ed.; Wiley: Chichester, UK, 2019; pp. 1–694. [Google Scholar] [CrossRef]
- Covidence. Available online: http://www.covidence.org/ (accessed on 11 November 2023).
- Sterne, J.A.C.; Savović, J.; Page, M.J.; Elbers, R.G.; Blencowe, N.S.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Cochrane Training. RevMan. Available online: https://training.cochrane.org/online-learning/core-software-cochrane-reviews/revman (accessed on 11 November 2023).
- Bers, D.M. Altered cardiac myocyte Ca regulation in heart failure. Physiology 2006, 21, 380–387. [Google Scholar] [CrossRef]
- Boroń, L.; Szczyglowski, K.; Konieczny, A.; Legocki, A.B. Glutamine synthetase in Lupinus luteus. Identification and preliminary characterization of nodule-specific CDNA clone. Acta Biochim. Pol. 1989, 36, 295–301. [Google Scholar]
- Grandi, E.; Pasqualini, F.S.; Bers, D.M. A novel computational model of the human ventricular action potential and Ca transient. J. Mol. Cell. Cardiol. 2010, 48, 112–121. [Google Scholar] [CrossRef] [PubMed]
- The Digitalis Investigation Group. The effect of digoxin on mortality and morbidity in patients with heart failure. N. Engl. J. Med. 1997, 336, 525–533. [Google Scholar] [CrossRef] [PubMed]
- Heidenreich, P.A.; Bozkurt, B.; Aguilar, D.; Allen, L.A.; Byun, J.J.; Colvin, M.M.; Deswal, A.; Drazner, M.H.; Dunlay, S.M.; Evers, L.R.; et al. 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. J. Am. Coll. Cardiol. 2022, 79, e263–e421. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.P.; Jankowska, E.J.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef] [PubMed]
- Tacon, C.L.; McCaffrey, J.; Delaney, A. Dobutamine for patients with severe heart failure: A systematic review and meta-analysis of randomised controlled trials. Intensive Care Med. 2012, 38, 359–367. [Google Scholar] [CrossRef] [PubMed]
- Packer, M.; Carver, J.R.; Rodeheffer, R.J.; Ivanhoe, R.J.; DiBianco, R.; Zeldis, S.M.; Hendrix, G.H.; Bommer, W.J.; Elkayam, U.; Kukin, M.L.; et al. Effect of oral milrinone on mortality in severe chronic heart failure. N. Engl. J. Med. 1991, 325, 1468–1475. [Google Scholar] [CrossRef] [PubMed]
- Mebazaa, A.; Parissis, J.; Porcher, R.; Gayat, E.; Nikolaou, M.; Boas, F.V.; Delgado, J.F.; Follath, F. Short-term survival by treatment among patients hospitalized with acute heart failure: The global ALARM-HF registry using propensity scoring methods. Intensive Care Med. 2011, 37, 290–301. [Google Scholar] [CrossRef] [PubMed]
- Radke, M.B.; Taft, M.H.; Stapel, B.; Hilfiker-Kleiner, D.; Preller, M.; Manstein, D.J. Small molecule-mediated refolding and activation of myosin motor function. eLife 2014, 3, e01603. [Google Scholar] [CrossRef]
- Schlecht, W.; Li, K.L.; Hu, D.; Dong, W. Fluorescence based characterization of calcium sensitizer action on the troponin complex. Chem. Biol. Drug Des. 2016, 87, 171–181. [Google Scholar] [CrossRef]
- Schober, T.; Huke, S.; Venkataraman, R.; Gryshchenko, O.; Kryshtal, D.; Hwang, H.S.; Baudenbacher, F.J.; Knollmann, B.C. Myofilament Ca sensitization increases cytosolic Ca binding affinity, alters intracellular Ca homeostasis, and causes pause-dependent Ca-triggered arrhythmia. Circ. Res. 2012, 111, 170–179. [Google Scholar] [CrossRef]
- Mebazaa, A.; Nieminen, M.S.; Filappatos, G.S.; Cleland, J.G.; Salon, J.E.; Thakkar, R.; Padley, R.J.; Huang, B.; Cohen-Solal, A. Levosimendan vs. dobutamine: Outcomes for acute heart failure patients on beta-blockers in SURVIVE. Eur. J. Heart Fail. 2009, 11, 304–311. [Google Scholar] [CrossRef] [PubMed]
- Tumminello, G.; Cereda, A.; Barbieri, L.; Biondi-Zoccai, G.; Lucreziotti, S.; Mafrici, A.; Carugo, S. Meta-analysis of placebo-controlled trials of levosimendan in acute myocardial infarction. J. Cardiovasc. Dev. Dis. 2021, 8, 129. [Google Scholar] [CrossRef] [PubMed]
- Gordon, A.C.; Perkins, G.D.; Singer, M.; McAuley, D.F.; Orme, R.M.L.; Santhakumaran, S.; Mason, A.J.; Cross, M.; Al-Beidh, F.; Best-Lane, J.; et al. Levosimendan for the prevention of acute organ dysfunction in sepsis. N. Engl. J. Med. 2016, 375, 1638–1648. [Google Scholar] [CrossRef] [PubMed]
- Syed, Y.Y. Landiolol: A review in tachyarrhythmias. Drugs 2018, 78, 377–388. [Google Scholar] [CrossRef] [PubMed]
- Cereda, A.; Laricchia, A.; Marini, C.; Franchina, G.; Conconi, B.; Lucreziotti, S. Literature case series review on landiolol in acute decompensated heart failure secondary to tachyarrhythmias. Eur. Heart J. Suppl. 2022, 24 (Suppl. K), suac121.143. [Google Scholar] [CrossRef]
- Cereda, A.; Laricchia, A.; Franchina, G.A.; Tumminello, G.; Sangiorgi, G.M.; Lucreziotti, S. Case series review on landiolol in acute decompensated heart failure secondary to tachyarrhythmias: New drug applications for an unmet medical need in critically ill patients. Medp. Cardiol. Vasc. Med. 2022, 2, mpcvm-202205002. [Google Scholar]
- Rao, S.J.; Kanwal, A.; Kanwal, A.; Danilov, A.; Frishman, W.H. Landiolol: An Ultra-Short-Acting β-Blocker. Cardiol. Rev. 2023; online ahead of print. [Google Scholar] [CrossRef]
- Liang, L.; Huang, L.; Zhao, X.; Zhao, L.; Tian, P.; Huang, B.; Feng, J.; Zhang, J.; Zhang, Y. Prognostic value of RDW alone and in combination with NT-ProBNP in patients with heart failure. Clin. Cardiol. 2022, 45, 802–813. [Google Scholar] [CrossRef]
- Ibrahim, N.E.; Januzzi, J.L., Jr. Established and emerging roles of biomarkers in heart failure. Circ. Res. 2018, 123, 614–629. [Google Scholar] [CrossRef]
- Bertero, E.; Maack, C. Calcium signaling and reactive oxygen species in mitochondria. Circ. Res. 2018, 122, 1460–1478. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study ID | Study Design | Country | Total Participants | Istaroxime | Primary Outcome | |
|---|---|---|---|---|---|---|
| Dosage | Treatment Duration | |||||
| Carubelli et al., 2020 [20] | Double-blinded multicenter phase II RCT | Italy and China | 120 | 0.5 μg/kg/min (cohort 1), 1.0 μg/kg/min in (cohort 2) | 24 h | E/e′ ratio change |
| Metra et al., 2022 [19] (SEISMiC) | Double-blinded multicenter phase II RCT | US, Italy, Russia, Romania, and Poland | 60 | 1.0–1.5 μg/kg/min | 24 h | SBP change |
| Shah et al., 2009 [21] (HORIZON-HF) | Double-blinded multicenter RCT | US, Italy, Greece, Romania, and Poland | 120 | 0.5, 1.0, or 1.5 μg/kg/min | 6 h | Pulmonary capillary wedge pressure change |
| Study ID | Number of Patients in Each Group | Age (Years) Mean (SD) | Gender (Male) N (%) | BMI Mean (SD) | SBP Mean (SD) | DBP Mean (SD) | HR Mean (SD) | Comorbidities N (%) | ||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| I | Pl | I | Pl | I | Pl | I | Pl | I | Pl | I | Pl | I | Pl | AF | HTN | PCI | CABG | DM | CKD | |||||||
| I | Pl | I | Pl | I | Pl | I | Pl | I | Pl | I | Pl | |||||||||||||||
| Carubelli et al., 2020 Cohort 1) [20] | 41 | 19 | 60 (16) | 58 (17) | 34 (83) | 16 (84) | 25 (4) | 25 (3) | 105 (12) | 105 (8) | . | . | 72 (13) | 77 (17) | 8 (20) | 5 (26) | 17 (42) | 11 (58) | . | . | . | . | 14 (34) | 5 (26) | 12 (29) | 5 (26) |
| Carubelli et al., 2020 Cohort 2) [20] | 40 | 20 | 52 (13) | 56 (16) | 34 (85) | 18 (90) | 23 (4) | 24 (4) | 106 (10) | 108 (10) | . | . | 78 (11) | 79 (13) | 11 (28) | 6 (30) | 14 (35) | 7 (35) | . | . | . | . | 6 (15) | 4 (20) | 10 (24) | 6 (30) |
| Metra et al., 2022 [19] (SEISMiC) | 29 | 31 | 65 (10) | 63 (13) | 22 (76) | 27 (87) | 28 (6) | 27 (6) | 88 (3) | 87 (3) | . | . | 84 (16) | 84 (19) | 16 (55) | 18 (58) | 25 (86) | 23 (74) | 9 (31) | 17 (55) | 4 (14) | 3 (10) | 9 (31) | 14 (45) | 2 (7) | 2 (6) |
| Shah et al., 2009 [21] (HORIZON-HF) | 89 | 31 | 55 (11) | 57 (10) | 80 (90) | 25 (81) | . | . | 117 (12) | 114 (15) | 70 (7) | 70 (8) | 74 (9) | 72 (11) | . | . | . | . | 20 (22) | 10 (32) | 4 (4) | 4 (13) | 16 (18) | 5 (16) | . | . |
| Certainty Assessment | Summary of Findings | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|
| Participants (Studies) Follow-up | Risk of Bias | Inconsistency | Indirectness | Imprecision | Publication Bias | Overall Certainty of Evidence | Study Event Rates (%) | Relative Effect (95% CI) | Anticipated Absolute Effects | ||
| With [Placebo] | With [Istaroxime] | Risk with [Placebo] | Risk Difference with [Istaroxime] | ||||||||
| Echo-LV end-diastolic volume | |||||||||||
| 288 (4 RCTs) | not serious | very serious a | not serious | very serious b | none | ⨁◯◯◯ Very low | 99 | 189 | - | The mean echo-LV end-diastolic volume was 0 | MD 4.69 lower (12.85 lower to 3.48 higher) |
| Echo-LV end-systolic volume | |||||||||||
| 288 (4 RCTs) | not serious | very serious a | not serious | very serious b | none | ⨁◯◯◯ Very low | 99 | 189 | - | The mean echo-LV end-systolic volume was 0 | MD 5.4 lower (12.05 lower to 1.25 higher) |
| Echo-LV ejection fraction | |||||||||||
| 288 (4 RCTs) | not serious | not serious | not serious | Serious b | none | ⨁⨁⨁◯ Moderate | 99 | 189 | - | The mean echo-LV ejection fraction was 0 | MD 1.06 higher (0.29 higher to 1.82 higher) |
| Echo-stroke volume index | |||||||||||
| 284 (4 RCTs) | not serious | not serious | not serious | not serious | none | ⨁⨁⨁⨁ High | 98 | 186 | - | The mean echo-stroke volume index was 0 | MD 3.04 higher (2.41 higher to 3.67 higher) |
| Echo-cardiac index change (L/min/m2) | |||||||||||
| 300 (4 RCTs) | not serious | not serious | not serious | not serious | none | ⨁⨁⨁⨁ High | 101 | 199 | - | The mean echo- cardiac index change (L/min/m2) was 0 | MD 0.18 higher (0.11 higher to 0.25 higher) |
| Echo-E/A ratio | |||||||||||
| 239 (4 RCTs) | not serious | not serious | not serious | not serious | none | ⨁⨁⨁⨁ High | 83 | 156 | - | The mean echo-E/A ratio was 0 | MD 0.39 lower (0.58 lower to 0.19 lower) |
| Echo-E/e′ ratio | |||||||||||
| 165 (3 RCTs) | not serious | very serious a | not serious | very serious b | none | ⨁◯◯◯ Very low | 66 | 99 | - | The mean echo-E/e′ ratio was 0 | MD 1.04 lower (4.15 lower to 2.07 higher) |
| Echo-IVC diameter | |||||||||||
| 180 (3 RCTs) | not serious | very serious a | not serious | very serious b | none | ⨁◯◯◯ Very low | 70 | 110 | - | The mean echo-IVC diameter was 0 | MD 1.82 lower (3.74 lower to 0.1 higher) |
| Echo-pulmonary artery systolic pressure | |||||||||||
| 180 (3 RCTs) | not serious | not serious | not serious | Serious b | none | ⨁⨁⨁◯ Moderate | 70 | 110 | - | The mean echo- pulmonary artery systolic pressure was 0 | MD 2.3 lower (3.2 lower to 1.4 lower) |
| Hemodynamic-SBP | |||||||||||
| 300 (4 RCTs) | not serious | not serious | not serious | Serious b | none | ⨁⨁⨁◯ Moderate | 101 | 199 | - | The mean hemodynamic outcomes-SBP was 0 | MD 5.32 higher (2.28 higher to 8.37 higher) |
| Hemodynamic-MAP | |||||||||||
| 180 (2 RCTs) | not serious | not serious | not serious | Serious b | none | ⨁⨁⨁◯ Moderate | 62 | 118 | - | The mean hemodynamic outcomes-MAP was 0 | MD 2.44 higher (0.17 lower to 5.05 higher) |
| Hemodynamic-HR | |||||||||||
| 300 (4 RCTs) | not serious | not serious | not serious | Serious b | none | ⨁⨁⨁◯ Moderate | 101 | 199 | - | The mean hemodynamic outcomes-HR change was 0 | MD 3.05 lower (5.27 lower to 0.82 lower) |
| Clinical-NT-proBNP change | |||||||||||
| 180 (3 RCTs) | not serious | not serious | not serious | very serious b | strong association | ⨁⨁⨁◯ Moderate | 70 | 110 | - | The mean clinical outcomes-NT-proBNP change was 0 | MD 808.28 higher (523.98 higher to 1092.58 higher) |
| Clinical-length of hospital stay | |||||||||||
| 180 (3 RCTs) | not serious | not serious | not serious | not serious | none | ⨁⨁⨁⨁ High | 70 | 110 | - | The mean clinical outcomes-length of stay was 0 | MD 0.23 lower (1.66 lower to 1.21 higher) |
| Clinical-worsening HF | |||||||||||
| 180 (3 RCTs) | not serious | not serious | not serious | very serious b | none | ⨁⨁◯◯ Low | 3/70 (4.3%) | 9/110 (8.2%) | RR 2.13 (0.64 to 7.05) | 43 per 1000 | 48 more per 1000 (from 15 fewer to 259 more) |
| Clinical-hospital readmission | |||||||||||
| 180 (3 RCTs) | not serious | not serious | not serious | very serious b | none | ⨁⨁◯◯ Low | 5/70 (7.1%) | 8/110 (7.3%) | RR 0.94 (0.30 to 2.99) | 71 per 1000 | 4 fewer per 1000 (from 50 fewer to 142 more) |
| Safety-any adverse event | |||||||||||
| 180 (2 RCTs) | not serious | not serious | not serious | very serious b | none | ⨁⨁◯◯ Low | 48/70 (68.6%) | 91/110 (82.7%) | RR 1.26 (1.05 to 1.51) | 686 per 1000 | 178 more per 1000 (from 34 more to 350 more) |
| Safety-any serious adverse event | |||||||||||
| 180 (2 RCTs) | not serious | not serious | not serious | very serious b | none | ⨁⨁◯◯ Low | 8/70 (11.4%) | 14/110 (12.7%) | RR 1.34 (0.58 to 3.11) | 114 per 1000 | 39 more per 1000 (from 48 fewer to 241 more) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Abuelazm, M.; Ali, S.; AlBarakat, M.M.; Mahmoud, A.; Tanashat, M.; Suilik, H.A.; Abdelazeem, B.; Brašić, J.R. Istaroxime for Patients with Acute Heart Failure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Diseases 2023, 11, 183. https://doi.org/10.3390/diseases11040183
Abuelazm M, Ali S, AlBarakat MM, Mahmoud A, Tanashat M, Suilik HA, Abdelazeem B, Brašić JR. Istaroxime for Patients with Acute Heart Failure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Diseases. 2023; 11(4):183. https://doi.org/10.3390/diseases11040183
Chicago/Turabian StyleAbuelazm, Mohamed, Shafaqat Ali, Majd M. AlBarakat, Abdelrahman Mahmoud, Mohammad Tanashat, Husam Abu Suilik, Basel Abdelazeem, and James Robert Brašić. 2023. "Istaroxime for Patients with Acute Heart Failure: A Systematic Review and Meta-Analysis of Randomized Controlled Trials" Diseases 11, no. 4: 183. https://doi.org/10.3390/diseases11040183