
C-Reactive Protein: Pathophysiology, Diagnosis, False Test Results and a Novel Diagnostic Algorithm for Clinicians


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
2. Current Evidence on Potential Biochemical Properties and Genetics of C-Reactive Protein
2.1. Forms of C-Reactive Protein
2.2. Structure of C-Reactive Protein
2.2.1. The Monomeric or “Modified” CRP
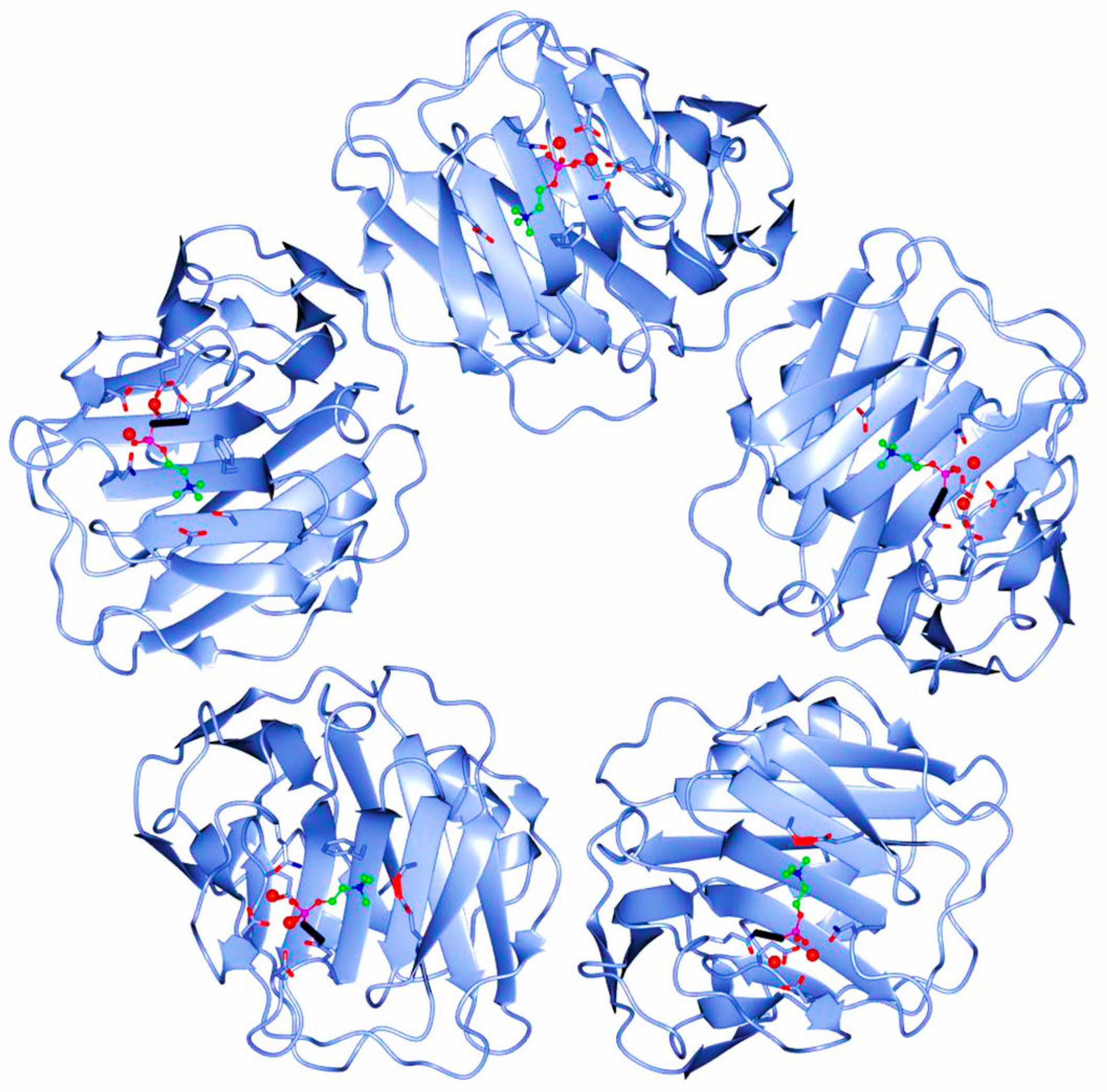
2.2.2. The Pentameric or “Native” CRP
2.3. Genetics of C-Reactive Protein
3. Current Evidence on Potential Pathobiology of C-Reactive Protein
3.1. Synthesis of C-Reactive Protein
3.2. Functions of C-Reactive Protein
3.2.1. The Monomeric or “Modified” CRP
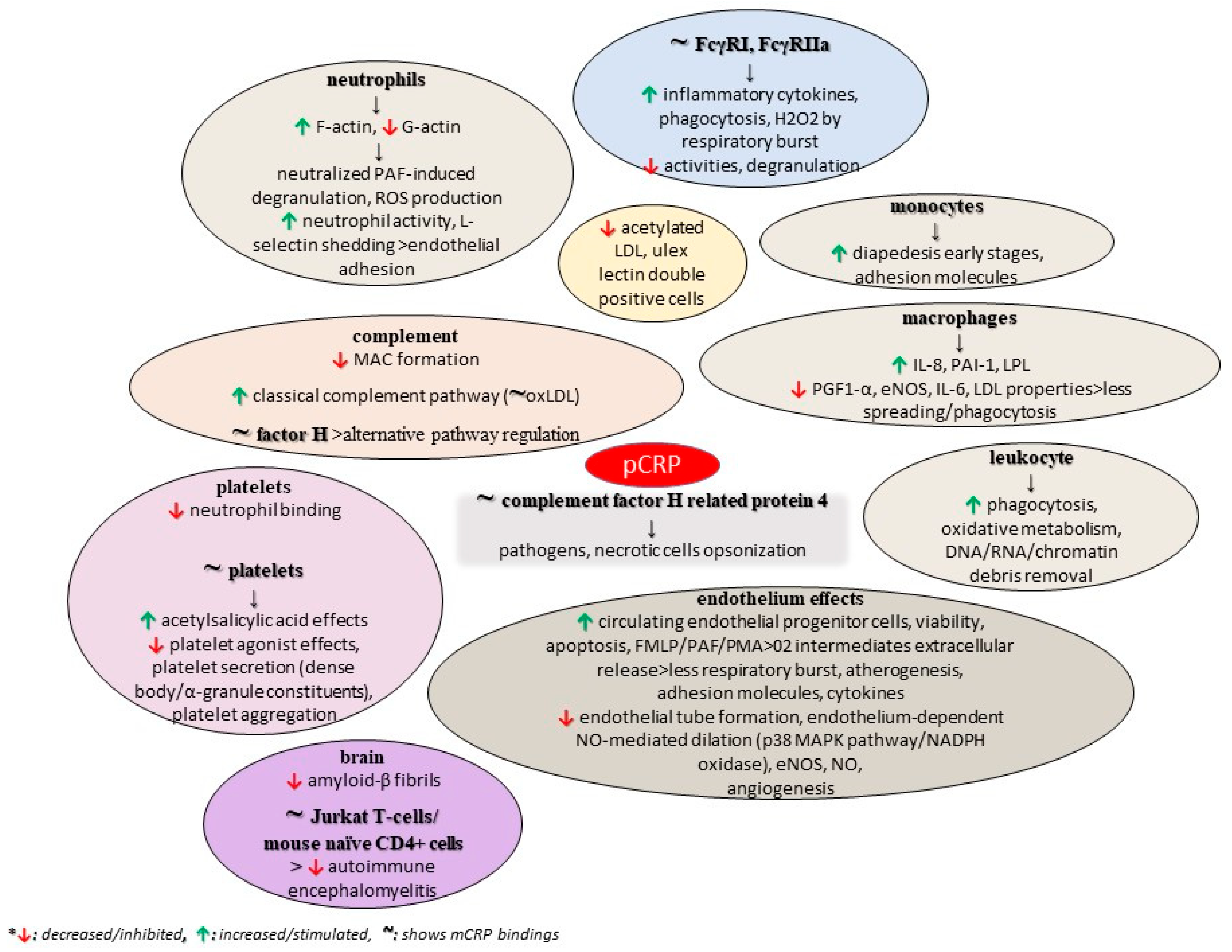
3.2.2. The Pentameric or “Native” CRP
3.2.3. No Precise Form of CRP
3.3. Function of Autoantibodies against C-Reactive Protein
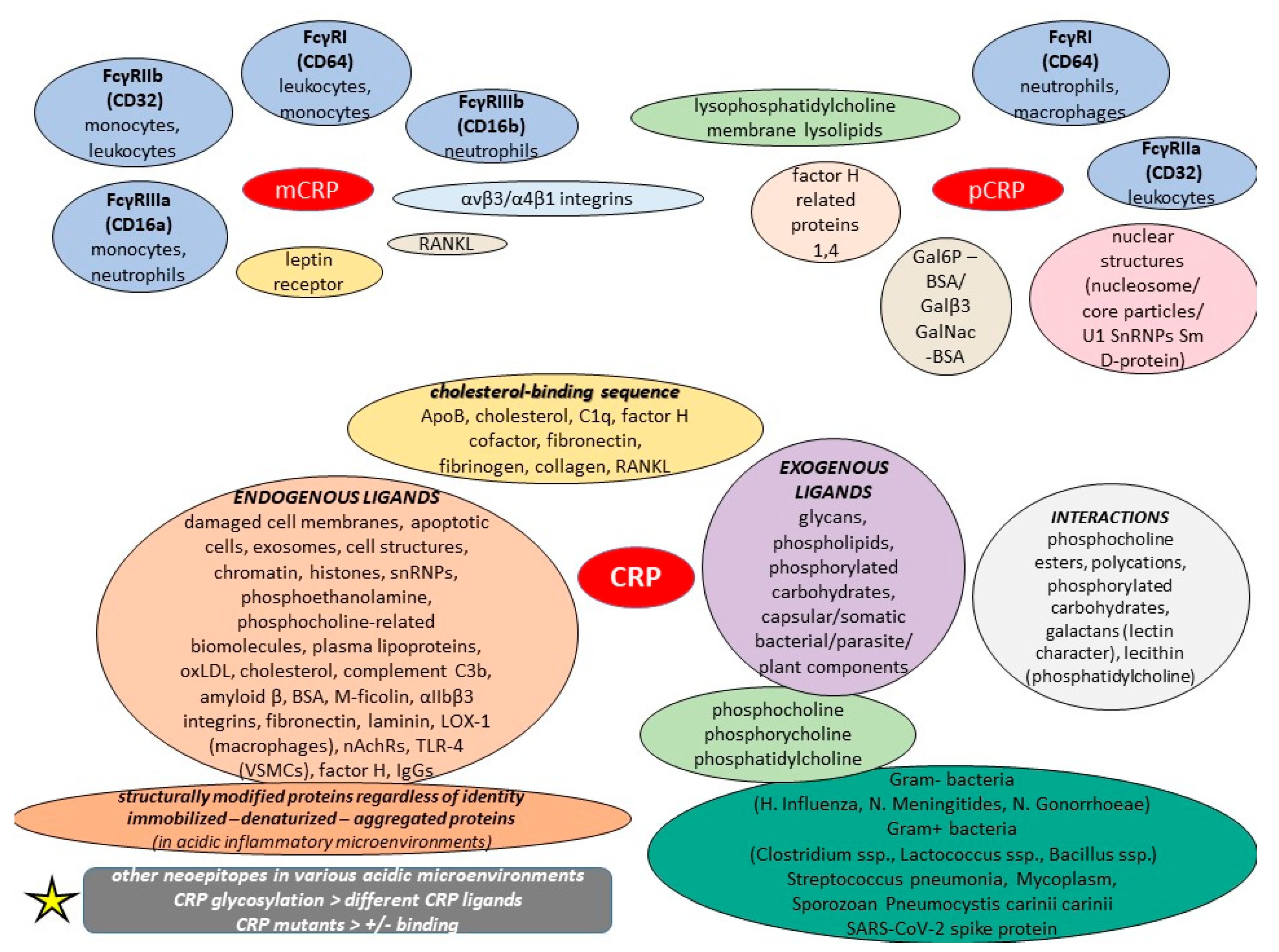
3.4. Receptors and Ligands of C-Reactive Protein
4. Current Evidence on C-Reactive Protein and Potential Conditions
4.1. C-Reactive Protein and Physiological Disorders
4.1.1. Cardiological Disorders
4.1.2. Vascular Disorders
4.1.3. Respiratory Disorders
4.1.4. Gastrointestinal Disorders
4.1.5. Hepatobiliary Disorders
4.1.6. Pancreatic Disorders
4.1.7. Renal Disorders
4.1.8. Gynecological and Andrological Disorders
4.1.9. Dermatological Disorders
4.1.10. Musculoskeletal Disorders
4.1.11. Oral, Otorhinolaryngological, and Ophthalmological Disorders
4.1.12. Neurological Disorders
4.1.13. Mental Disorders
4.1.14. Thyroid and Splenic Disorders
4.2. C-Reactive Protein and Autoimmune-Related Conditions
4.3. C-Reactive Protein and Neoplasms
4.4. C-Reactive Protein and Infections
4.5. C-Reactive Protein and Other Factors
5. Current Evidence on C-Reactive Protein and Potential Molecular Diagnostics
5.1. C-Reactive Protein and Principles of Common Diagnostic Assays
5.2. C-Reactive Protein and Possible False Test Results in Common Diagnostic Assays
6. The Expert’s Opinion: A Critical Appraisal of the Current Literature on C-Reactive Protein and the Mysterious Systemic Inflammation
7. C-Reactive Protein: A Novel Diagnostic Algorithm Every Physician Should Know
8. Conclusions
Funding
Acknowledgments
Conflicts of Interest
References
- Mouliou, D.S. Managing Viral Emerging Infectious Diseases via Current Molecular Diagnostics in the Emergency Department: The Tricky Cases. Expert Rev. Anti-Infect. Ther. 2022, 20, 1163–1169. [Google Scholar] [CrossRef] [PubMed]
- Mouliou, D.S.; Gourgoulianis, K.I. False-Positive and False-Negative COVID-19 Cases: Respiratory Prevention and Management Strategies, Vaccination, and Further Perspectives. Expert Rev. Respir. Med. 2021, 15, 993–1002. [Google Scholar] [CrossRef] [PubMed]
- Mouliou, D.S.; Pantazopoulos, I.; Gourgoulianis, K.I. COVID-19 Smart Diagnosis in the Emergency Department: All-in in Practice. Expert Rev. Respir. Med. 2022, 16, 263–272. [Google Scholar] [CrossRef]
- Mouliou, D.S.; Gourgoulianis, K.I. COVID-19 ‘Asymptomatic’ Patients: An Old Wives’ Tale. Expert Rev. Respir. Med. 2022, 16, 399–407. [Google Scholar] [CrossRef] [PubMed]
- Mouliou, D.S.; Pantazopoulos, I.; Gourgoulianis, K. COVID-19 Diagnosis in the Emergency Department: Seeing the Tree but Losing the Forest. Emerg. Med. J. 2022, 39, 563. [Google Scholar] [CrossRef]
- Abdelshaheed, N.N.; Goldberg, D.M. Biochemical Tests in Diseases of the Intestinal Tract: Their Contributions to Diagnosis, Management, and Understanding the Pathophysiology of Specific Disease States. Crit. Rev. Clin. Lab. Sci. 1997, 34, 141–223. [Google Scholar] [CrossRef]
- Jelski, W.; Mroczko, B. Biochemical Markers of Colorectal Cancer—Present and Future. Cancer Manag. Res. 2020, 12, 4789–4797. [Google Scholar] [CrossRef]
- Tumani, H.; Brettschneider, J. Biochemical Markers of Autoimmune Diseases of the Nervous System. Curr. Pharm. Des. 2012, 18, 4556–4563. [Google Scholar] [CrossRef]
- Castro, C.; Gourley, M. Diagnostic Testing and Interpretation of Tests for Autoimmunity. J. Allergy Clin. Immunol. 2010, 125, S238–S247. [Google Scholar] [CrossRef] [PubMed]
- Nikolaou, S.; Qiu, S.; Fiorentino, F.; Rasheed, S.; Tekkis, P.; Kontovounisios, C. Systematic Review of Blood Diagnostic Markers in Colorectal Cancer. Tech. Coloproctol. 2018, 22, 481–498. [Google Scholar] [CrossRef]
- Pierrakos, C.; Velissaris, D.; Bisdorff, M.; Marshall, J.C.; Vincent, J.-L. Biomarkers of Sepsis: Time for a Reappraisal. Crit. Care 2020, 24, 287. [Google Scholar] [CrossRef]
- Li, H.; Sun, K.; Zhao, R.; Hu, J.; Hao, Z.; Wang, F.; Lu, Y.; Liu, F.; Zhang, Y. Inflammatory Biomarkers of Coronary Heart Disease. Front. Biosci. (Schol. Ed.) 2018, 10, 185–196. [Google Scholar] [CrossRef]
- Jiang, Y.; Ni, K.; Fang, M.; Li, J. The Effects of Serum Hs-CRP on the Incidence of Lung Cancer in Male Patients with Pulmonary Tuberculosis. Iran. J. Public Health 2019, 48, 1265–1269. [Google Scholar] [CrossRef]
- Kadi, F.A.; Yuniati, T.; Sribudian, Y.; Rachmadi, D. C-Reactive Protein and Haemoglobin Level in Acute Kidney Injury among Preterm Newborns. Med. Glas. 2021, 18, 410–414. [Google Scholar] [CrossRef]
- Pitharouli, M.C.; Hagenaars, S.P.; Glanville, K.P.; Coleman, J.R.I.; Hotopf, M.; Lewis, C.M.; Pariante, C.M. Elevated C-Reactive Protein in Patients with Depression, Independent of Genetic, Health, and Psychosocial Factors: Results from the UK Biobank. Am. J. Psychiatry 2021, 178, 522–529. [Google Scholar] [CrossRef] [PubMed]
- Neumaier, M.; Braun, K.F.; Sandmann, G.; Siebenlist, S. C-Reactive Protein in Orthopaedic Surgery. Acta Chir. Orthop. Traumatol. Cech. 2015, 82, 327–331. [Google Scholar] [CrossRef] [PubMed]
- Figus, F.A.; Piga, M.; Azzolin, I.; McConnell, R.; Iagnocco, A. Rheumatoid Arthritis: Extra-Articular Manifestations and Comorbidities. Autoimmun. Rev. 2021, 20, 102776. [Google Scholar] [CrossRef] [PubMed]
- Erden, S.; Buyukozturk, S.; Vural, P.; Değirmencioğlu, S. Acute-Phase Reactans in Hashimoto Thyroiditis. Int. Immunopharmacol. 2008, 8, 1863–1865. [Google Scholar] [CrossRef] [PubMed]
- Kinoshita, A.; Onoda, H.; Imai, N.; Nishino, H.; Tajiri, H. C-Reactive Protein as a Prognostic Marker in Patients with Hepatocellular Carcinoma. Hepatogastroenterology 2015, 62, 966–970. [Google Scholar] [PubMed]
- Allin, K.H.; Nordestgaard, B.G. Elevated C-Reactive Protein in the Diagnosis, Prognosis, and Cause of Cancer. Crit. Rev. Clin. Lab. Sci. 2011, 48, 155–170. [Google Scholar] [CrossRef] [PubMed]
- Windgassen, E.B.; Funtowicz, L.; Lunsford, T.N.; Harris, L.A.; Mulvagh, S.L. C-Reactive Protein and High-Sensitivity C-Reactive Protein: An Update for Clinicians. Postgrad. Med. 2011, 123, 114–119. [Google Scholar] [CrossRef]
- Pohanka, M. Diagnoses Based on C-Reactive Protein Point-of-Care Tests. Biosensors 2022, 12, 344. [Google Scholar] [CrossRef] [PubMed]
- Tillett, W.S.; Francis, T. Serological reactions in pneumonia with a non-protein somatic fraction of pneumococcus. J. Exp. Med. 1930, 52, 561–571. [Google Scholar] [CrossRef]
- Macleod, C.; Avery, O. The occurrence during acute infections of a protein not normally present in the blood II. Isolation and properties of the reactive protein. J. Exp. Med. 1941, 73, 183–190. [Google Scholar]
- Volanakis, J.E.; Kaplan, M.H. Specifity of C-reactive protein for choline phosphate residues of pneumococcal C-polysaccharide. Proc. Soc. Exp. Biol. Med. 1971, 136, 612–614. [Google Scholar] [CrossRef]
- Boncler, M.; Wu, Y.; Watala, C. The Multiple Faces of C-Reactive Protein—Physiological and Pathophysiological Implications in Cardiovascular Disease. Molecules 2019, 24, 2062. [Google Scholar] [CrossRef]
- Wang, J.; Tang, B.; Liu, X.; Wu, X.; Wang, H.; Xu, D.; Guo, Y. Increased Monomeric CRP Levels in Acute Myocardial Infarction: A Possible New and Specific Biomarker for Diagnosis and Severity Assessment of Disease. Atherosclerosis 2015, 239, 343–349. [Google Scholar] [CrossRef] [PubMed]
- Pathak, A.; Agrawal, A. Evolution of C-Reactive Protein. Front. Immunol. 2019, 10, 943. [Google Scholar] [CrossRef]
- Wang, H.W.; Wu, Y.; Chen, Y.; Sui, S.F. Polymorphism of structural forms of C-reactive protein. Int. J. Mol. Med. 2002, 9, 665–667. [Google Scholar] [CrossRef] [PubMed]
- Taylor, K.E.; van den Berg, C.W. Structural and Functional Comparison of Native Pentameric, Denatured Monomeric and Biotinylated C-Reactive Protein. Immunology 2007, 120, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Potempa, L.A.; Siegel, J.N.; Fedel, B.A.; Potempa, R.T.; Gewurz, H. Expression, Detection and Assay of a Neoantigen (Neo-CRP) Associated with a Free, Human C-Reactive Protein Subunit. Mol. Immunol. 1987, 24, 531–541. [Google Scholar] [CrossRef]
- Blizniukov, O.P.; Kozmin, L.D.; Falikova, V.V.; Martynov, A.I.; Tischenko, V.M. Effect of Calcium Ions on Hydrodynamic Properties of Pentameric and Decameric C-Reactive Protein in Solution. Mol. Biol. 2003, 37, 912–919. [Google Scholar] [CrossRef]
- Kresl, J.J.; Potempa, L.A.; Anderson, B.E. Conversion of Native Oligomeric to a Modified Monomeric Form of Human C-Reactive Protein. Int. J. Biochem. Cell Biol. 1998, 30, 1415–1426. [Google Scholar] [CrossRef]
- Thompson, D.; Pepys, M.B.; Wood, S.P. The Physiological Structure of Human C-Reactive Protein and Its Complex with Phosphocholine. Structure 1999, 7, 169–177. [Google Scholar] [CrossRef] [PubMed]
- Salazar, J.; Martínez, M.S.; Chávez-Castillo, M.; Núñez, V.; Añez, R.; Torres, Y.; Toledo, A.; Chacín, M.; Silva, C.; Pacheco, E.; et al. C-Reactive Protein: An In-Depth Look into Structure, Function, and Regulation. Int. Sch. Res. Not. 2014, 2014, 653045. [Google Scholar] [CrossRef]
- Srinivasan, N.; White, H.E.; Emsley, J.; Wood, S.P.; Pepys, M.B.; Blundell, T.L. Comparative Analyses of Pentraxins: Implications for Protomer Assembly and Ligand Binding. Structure 1994, 2, 1017–1027. [Google Scholar] [CrossRef] [PubMed]
- Ashton, A.W.; Boehm, M.K.; Gallimore, J.R.; Pepys, M.B.; Perkins, S.J. Pentameric and Decameric Structures in Solution of Serum Amyloid P Component by X-ray and Neutron Scattering and Molecular Modelling analyses11Edited by R. Huber. J. Mol. Biol. 1997, 272, 408–422. [Google Scholar] [CrossRef] [PubMed]
- Black, S.; Kushner, I.; Samols, D. C-Reactive Protein. J. Biol. Chem. 2004, 279, 48487–48490. [Google Scholar] [CrossRef] [PubMed]
- Mullenix, M.C.; Mortensen, R.F. Calcium Ion Binding Regions in C-Reactive Protein: Location and Regulation of Conformational Changes. Mol. Immunol. 1994, 31, 615–622. [Google Scholar] [CrossRef]
- Agrawal, A.; Lee, S.; Carson, M.; Narayana, S.V.; Greenhough, T.J.; Volanakis, J.E. Site-Directed Mutagenesis of the Phosphocholine-Binding Site of Human C-Reactive Protein: Role of Thr76 and Trp67. J. Immunol. 1997, 158, 345–350. [Google Scholar] [CrossRef] [PubMed]
- Das, T.; Sen, A.; Kempf, T.; Pramanik, S.R.; Mandal, C.; Mandal, C. Induction of Glycosylation in Human C-Reactive Protein under Different Pathological Conditions. Biochem. J. 2003, 373, 345–355. [Google Scholar] [CrossRef]
- Singh, S.K.; Thirumalai, A.; Pathak, A.; Ngwa, D.N.; Agrawal, A. Functional Transformation of C-Reactive Protein by Hydrogen Peroxide. J. Biol. Chem. 2017, 292, 3129–3136. [Google Scholar] [CrossRef] [PubMed]
- Bang, R.; Marnell, L.; Mold, C.; Stein, M.-P.; Clos, K.T.D.; Chivington-Buck, C.; Clos, T.W.D. Analysis of Binding Sites in Human C-Reactive Protein for FcγRI, FcγRIIA, and C1q by Site-Directed Mutagenesis. J. Biol. Chem. 2005, 280, 25095–25102. [Google Scholar] [CrossRef]
- Gaboriaud, C.; Juanhuix, J.; Gruez, A.; Lacroix, M.; Darnault, C.; Pignol, D.; Verger, D.; Fontecilla-Camps, J.C.; Arlaud, G.J. The Crystal Structure of the Globular Head of Complement Protein C1q Provides a Basis for Its Versatile Recognition Properties. J. Biol. Chem. 2003, 278, 46974–46982. [Google Scholar] [CrossRef] [PubMed]
- Hage, F.G.; Szalai, A.J. C-Reactive Protein Gene Polymorphisms, C-Reactive Protein Blood Levels, and Cardiovascular Disease Risk. J. Am. Coll. Cardiol. 2007, 50, 1115–1122. [Google Scholar] [CrossRef] [PubMed]
- Woo, P.; Korenberg, J.R.; Whitehead, A.S. Characterization of genomic and complementary DNA sequence of human C-reactive protein, and comparison with the complementary DNA sequence of serum amyloid P component. J. Biol. Chem. 1985, 260, 13384–13388. [Google Scholar] [CrossRef] [PubMed]
- Lei, K.J.; Liu, T.; Zon, G.; Soravia, E.; Liu, T.Y.; Goldman, N.D. Genomic DNA Sequence for Human C-Reactive Protein. J. Biol. Chem. 1985, 260, 13377–13383. [Google Scholar] [CrossRef] [PubMed]
- Szalai, A.J.; Wu, J.; Lange, E.M.; McCrory, M.A.; Langefeld, C.D.; Williams, A.; Zakharkin, S.O.; George, V.; Allison, D.B.; Cooper, G.S.; et al. Single-nucleotide polymorphisms in the C-reactive protein (CRP) gene promoter that affect transcription factor binding, alter transcriptional activity, and associate with differences in baseline serum CRP level. J. Mol. Med. 2005, 83, 440–447. [Google Scholar] [CrossRef]
- Carlson, C.S.; Aldred, S.F.; Lee, P.K.; Tracy, R.P.; Schwartz, S.M.; Rieder, M.; Liu, K.; Williams, O.D.; Iribarren, C.; Lewis, E.C.; et al. Polymorphisms within the C-Reactive Protein (CRP) Promoter Region Are Associated with Plasma CRP Levels. Am. J. Hum. Genet. 2005, 77, 64–77. [Google Scholar] [CrossRef]
- Crawford, D.C.; Yi, Q.; Smith, J.D.; Shephard, C.; Wong, M.; Witrak, L.; Livingston, R.J.; Rieder, M.J.; Nickerson, D.A. Allelic Spectrum of the Natural Variation in CRP. Hum. Genet. 2006, 119, 496–504. [Google Scholar] [CrossRef] [PubMed]
- Dorajoo, R.; Li, R.; Ikram, M.K.; Liu, J.; Froguel, P.; Lee, J.; Sim, X.; Ong, R.T.-H.; Tay, W.T.; Peng, C.; et al. Are C-Reactive Protein Associated Genetic Variants Associated with Serum Levels and Retinal Markers of Microvascular Pathology in Asian Populations from Singapore? PLoS ONE 2013, 8, e67650. [Google Scholar] [CrossRef]
- Doumatey, A.P.; Chen, G.; Tekola Ayele, F.; Zhou, J.; Erdos, M.; Shriner, D.; Huang, H.; Adeleye, J.; Balogun, W.; Fasanmade, O.; et al. C-Reactive Protein (CRP) Promoter Polymorphisms Influence Circulating CRP Levels in a Genome-Wide Association Study of African Americans. Hum. Mol. Genet. 2012, 21, 3063–3072. [Google Scholar] [CrossRef] [PubMed]
- Elliott, P.; Chambers, J.C.; Zhang, W.; Clarke, R.; Hopewell, J.C.; Peden, J.F.; Erdmann, J.; Braund, P.; Engert, J.C.; Bennett, D.; et al. Genetic Loci Associated with C-Reactive Protein Levels and Risk of Coronary Heart Disease. JAMA 2009, 302, 37–48. [Google Scholar] [CrossRef]
- Stayoussef, M.; Zidi, S.; Kanabekova, P.; Mouellhi, L.; Almawi, W.Y.; Yaacoubi-Loueslati, B. Relation of CRP Gene Variants to Altered Risk of Helicobacter Pylori—Associated Chronic Gastritis: A Case-Control Study in Tunisia. Mol. Cell. Probes 2022, 66, 101864. [Google Scholar] [CrossRef] [PubMed]
- Amos, C.I.; Wu, X.; Broderick, P.; Gorlov, I.P.; Gu, J.; Eisen, T.; Dong, Q.; Zhang, Q.; Gu, X.; Vijayakrishnan, J.; et al. Genome-Wide Association Scan of Tag SNPs Identifies a Susceptibility Locus for Lung Cancer at 15q25.1. Nat. Genet. 2008, 40, 616–622. [Google Scholar] [CrossRef]
- Kim, J.-J.; Yun, S.W.; Yu, J.J.; Yoon, K.L.; Lee, K.-Y.; Kil, H.-R.; Kim, G.B.; Han, M.K.; Song, M.S.; Lee, H.D.; et al. Common Variants in the CRP Promoter Are Associated with a High C-Reactive Protein Level in Kawasaki Disease. Pediatr. Cardiol. 2015, 36, 438–444. [Google Scholar] [CrossRef]
- Russell, A.I. Polymorphism at the C-Reactive Protein Locus Influences Gene Expression and Predisposes to Systemic Lupus Erythematosus. Hum. Mol. Genet. 2003, 13, 137–147. [Google Scholar] [CrossRef]
- Papanicolaou, D.A. The Pathophysiologic Roles of Interleukin-6 in Human Disease. Ann. Intern. Med. 1998, 128, 127. [Google Scholar] [CrossRef]
- Gould, J.M.; Weiser, J.N. Expression of C-Reactive Protein in the Human Respiratory Tract. Infect. Immun. 2001, 69, 1747–1754. [Google Scholar] [CrossRef] [PubMed]
- CRP Gene—GeneCards|CRP Protein|CRP Antibody. Available online: https://www.genecards.org/cgi-bin/carddisp.pl?gene=CRP (accessed on 14 January 2023).
- Jabs, W.J.; Lögering, B.A.; Gerke, P.; Kreft, B.; Wolber, E.-M.; Klinger, M.H.F.; Fricke, L.; Steinhoff, J. The Kidney as a Second Site of Human C-Reactive Protein Formation in Vivo. Eur. J. Immunol. 2003, 33, 152–161. [Google Scholar] [CrossRef] [PubMed]
- Fehsel, K.; Plewe, D.; Kolb-Bachofen, V. Nitric Oxide-Induced Expression of C-Reactive Protein in Islet Cells as a Very Early Marker for Islet Stress in the Rat Pancreas. Nitric Oxide 1997, 1, 254–262. [Google Scholar] [CrossRef]
- Rajab, I.M.; Hart, P.C.; Potempa, L.A. How C-Reactive Protein Structural Isoforms with Distinctive Bioactivities Affect Disease Progression. Front. Immunol. 2020, 11, 2126. [Google Scholar] [CrossRef] [PubMed]
- Pepys, M.B.; Hirschfield, G.M. C-Reactive Protein: A Critical Update. J. Clin. Investig. 2003, 111, 1805–1812. [Google Scholar] [CrossRef] [PubMed]
- McFadyen, J.D.; Kiefer, J.; Braig, D.; Loseff-Silver, J.; Potempa, L.A.; Eisenhardt, S.U.; Peter, K. Dissociation of C-Reactive Protein Localizes and Amplifies Inflammation: Evidence for a Direct Biological Role of C-Reactive Protein and Its Conformational Changes. Front. Immunol. 2018, 9, 1351. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.-Y.; Ji, S.-R.; Bai, C.-J.; El Kebir, D.; Li, H.-Y.; Shi, J.-M.; Zhu, W.; Costantino, S.; Zhou, H.H.; Potempa, L.A.; et al. A redox switch in C-reactive protein modulates activation of endothelial cells. FASEB J. 2011, 25, 3186–3196. [Google Scholar] [CrossRef] [PubMed]
- Trial, J.; Potempa, L.A.; Entman, M. The role of C-reactive protein in innate and acquired inflammation: New perspectives. Inflam. Cell Signal. 2016, 3, e1409. [Google Scholar] [CrossRef]
- Thiele, J.R.; Habersberger, J.; Braig, D.; Schmidt, Y.; Goerendt, K.; Maurer, V.; Bannasch, H.; Scheichl, A.; Woollard, K.J.; Von Dobschütz, E.; et al. Dissociation of Pentameric to Monomeric C-Reactive Protein Localizes and Aggravates Inflammation: In Vivo Proof of a Powerful Proinflammatory Mechanism and a New Anti-Inflammatory Strategy. Circulation 2014, 130, 35–50. [Google Scholar] [CrossRef]
- Wang, H.W.; Sui, S.F. Dissociation and subunit rearrangement of membrane-bound human C-reactive proteins. Biochem. Biophys. Res. Commun. 2001, 288, 75–79. [Google Scholar] [CrossRef]
- Li, Q.; Li, H.; Fu, G.; Yu, F.; Wu, Y.; Zhao, M. Autoantibodies against C-Reactive Protein Influence Complement Activation and Clinical Course in Lupus Nephritis. J. Am. Soc. Nephrol. 2017, 28, 3044. [Google Scholar] [CrossRef]
- Radosevich, J.A.; Haines, G.K.; Motie, M.; Schaul, K.W.; Mehta, N.; Kolb, K.; Potempa, L.A. Immunohistochemical detection of epitopes expressed on CRP and modified CRP (i.e., neo-CRP) in human normal and diseased tissues. FASEB J. 1996, 10, 1466a. [Google Scholar]
- Diehl, E.E.; Haines, G.K.; Radosevich, J.A.; Potempa, L.A. Immunohistological localization of modified C-reactive protein antigen in normal human vascular tissue. Am. J. Med. Sci. 2000, 319, 79–83. [Google Scholar] [CrossRef]
- Zhang, C.-M.; Tan, Y.-B.; Zhou, H.-H.; Ge, Z.-B.; Feng, J.-R.; Lv, G.-B.; Sun, Z.-Y.; Fu, Y.; Wang, M.-Y. Intra-Subunit Disulfide Determines the Conversion and Structural Stability of CRP Isoforms. Inflammation 2020, 43, 466–477. [Google Scholar] [CrossRef] [PubMed]
- Fujita, M.; Takada, Y.K.; Izumiya, Y.; Takada, Y. The Binding of Monomeric C-Reactive Protein (MCRP) to Integrins Avβ3 and A4β1 Is Related to Its Pro-Inflammatory Action. PLoS ONE 2014, 9, e93738. [Google Scholar] [CrossRef] [PubMed]
- Ji, S.-R.; Ma, L.; Bai, C.-J.; Shi, J.-M.; Li, H.-Y.; Potempa, L.A.; Filep, J.G.; Zhao, J.; Wu, Y. Monomeric C-Reactive Protein Activates Endothelial Cells via Interaction with Lipid Raft Microdomains. FASEB J. 2009, 23, 1806–1816. [Google Scholar] [CrossRef] [PubMed]
- Potempa, L.A.; Rajab, I.M.; Olson, M.E.; Hart, P.C. C-Reactive Protein and Cancer: Interpreting the Differential Bioactivities of Its Pentameric and Monomeric, Modified Isoforms. Front. Immunol. 2021, 12, 744129. [Google Scholar] [CrossRef]
- Srikantiah, C. C-Reactive Protein: An Inflammatory Marker with Specific Role in Physiology, Pathology, and Diagnosis. IJRCI 2014, 2. [Google Scholar] [CrossRef]
- Mihlan, M.; Blom, A.M.; Kupreishvili, K.; Lauer, N.; Stelzner, K.; Bergström, F.; Niessen, H.W.; Zipfel, P.F. Monomeric C-reactive protein modulates classical complement activation on necrotic cells. FASEB J. 2011, 25, 4198–4210. [Google Scholar] [CrossRef] [PubMed]
- O’Flynn, J.; van der Pol, P.; Dixon, K.O.; Prohászka, Z.; Daha, M.R.; van Kooten, C. Monomeric C-Reactive Protein Inhibits Renal Cell-Directed Complement Activation Mediated by Properdin. Am. J. Physiol. Ren. Physiol. 2016, 310, F1308–F1316. [Google Scholar] [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front. Immunol. 2018, 9, 754. [Google Scholar] [CrossRef]
- Shephard, E.G.; Anderson, R.; Beer, S.M.; Van Rensburg, C.E.; de Beer, F.C. Neutrophil Lysosomal Degradation of Human CRP: CRP-Derived Peptides Modulate Neutrophil Function. Clin. Exp. Immunol. 1988, 73, 139–145. [Google Scholar]
- Khreiss, T.; József, L.; Potempa, L.A.; Filep, J.G. Loss of pentameric symmetry in C-reactive protein induces interleukin-8 secretion through peroxynitrite signaling in human neutrophils. Circ. Res. 2005, 97, 690–697. [Google Scholar] [CrossRef] [PubMed]
- Melnikov, I.; Kozlov, S.; Saburova, O.; Avtaeva, Y.; Guria, K.; Gabbasov, Z. Monomeric C-Reactive Protein in Atherosclerotic Cardiovascular Disease: Advances and Perspectives. Int. J. Mol. Sci. 2023, 24, 2079. [Google Scholar] [CrossRef] [PubMed]
- Li, R.; Ren, M.; Luo, M.; Chen, N.; Zhang, Z.; Luo, B.; Wu, J. Monomeric C-Reactive Protein Alters Fibrin Clot Properties on Endothelial Cells. Thromb. Res. 2012, 129, e251–e256. [Google Scholar] [CrossRef] [PubMed]
- Potempa, L.A.; Motie, M.; Wright, K.E.; Crump, B.L.; Radosevich, J.A.; Sakai, N.; Lai, G.; Tanaka, K.; Kojima, E.; Tsuboi, A. Stimulation of Megakaryocytopoiesis in Mice by Human Modified C-Reactive Protein (MCRP). Exp. Hematol. 1996, 24, 258–264. [Google Scholar]
- de la Torre, R.; Peña, E.; Vilahur, G.; Slevin, M.; Badimon, L. Monomerization of C-Reactive Protein Requires Glycoprotein IIb-IIIa Activation: Pentraxins and Platelet Deposition. J. Thromb. Haemost. 2013, 11, 2048–2058. [Google Scholar] [CrossRef]
- Molins, B.; Peña, E.; De La Torre, R.; Badimon, L. Monomeric C-Reactive Protein Is Prothrombotic and Dissociates from Circulating Pentameric C-Reactive Protein on Adhered Activated Platelets under Flow. Cardiovasc. Res. 2011, 92, 328–337. [Google Scholar] [CrossRef]
- Zha, Z.; Cheng, Y.; Cao, L.; Qian, Y.; Liu, X.; Guo, Y.; Wang, J. Monomeric CRP Aggravates Myocardial Injury after Myocardial Infarction by Polarizing the Macrophage to Pro-Inflammatory Phenotype through JNK Signaling Pathway. J. Inflamm. Res. 2021, 14, 7053–7064. [Google Scholar] [CrossRef]
- Chen, T.; Xu, P.-C.; Gao, S.; Hu, S.-Y.; Wei, L.; Yan, T.-K. Monomeric C-Reactive Protein Promotes Platelets to Release Mitochondrial DNA in Anti-Neutrophil Cytoplasmic Antibody-Associated Vasculitis. Mol. Immunol. 2021, 137, 228–237. [Google Scholar] [CrossRef]
- Ullah, N.; Ma, F.-R.; Han, J.; Liu, X.-L.; Fu, Y.; Liu, Y.-T.; Liang, Y.-L.; Ouyang, H.; Li, H.-Y. Monomeric C-Reactive Protein Regulates Fibronectin Mediated Monocyte Adhesion. Mol. Immunol. 2020, 117, 122–130. [Google Scholar] [CrossRef]
- Luan, Y.; Yao, Y. The Clinical Significance and Potential Role of C-Reactive Protein in Chronic Inflammatory and Neurodegenerative Diseases. Front. Immunol. 2018, 9, 1302. [Google Scholar] [CrossRef]
- Badimon, L.; Peña, E.; Arderiu, G.; Padró, T.; Slevin, M.; Vilahur, G.; Chiva-Blanch, G. C-Reactive Protein in Atherothrombosis and Angiogenesis. Front. Immunol. 2018, 9, 430. [Google Scholar] [CrossRef] [PubMed]
- Kang, D.-H.; Park, S.-K.; Lee, I.-K.; Johnson, R.J. Uric Acid–Induced C-Reactive Protein Expression: Implication on Cell Proliferation and Nitric Oxide Production of Human Vascular Cells. J. Am. Soc. Nephrol. 2005, 16, 3553. [Google Scholar] [CrossRef] [PubMed]
- Peña, E.; de la Torre, R.; Arderiu, G.; Slevin, M.; Badimon, L. MCRP Triggers Angiogenesis by Inducing F3 Transcription and TF Signalling in Microvascular Endothelial Cells. Thromb. Haemost. 2017, 117, 357–370. [Google Scholar] [CrossRef] [PubMed]
- Ahrens, I.; Domeij, H.; Eisenhardt, S.U.; Topcic, D.; Albrecht, M.; Leitner, E.; Viitaniemi, K.; Jowett, J.B.; Lappas, M.; Bode, C.; et al. Opposing Effects of Monomeric and Pentameric C-Reactive Protein on Endothelial Progenitor Cells. Basic Res. Cardiol. 2011, 106, 879–895. [Google Scholar] [CrossRef] [PubMed]
- Sudhakar, M.; Silambanan, S.; Chandran, A.S.; Prabhakaran, A.A.; Ramakrishnan, R. C-Reactive Protein (CRP) and Leptin Receptor in Obesity: Binding of Monomeric CRP to Leptin Receptor. Front. Immunol. 2018, 9, 1167. [Google Scholar] [CrossRef] [PubMed]
- Yuan, G.; Chen, X.; Ma, Q.; Qiao, J.; Li, R.; Li, X.; Li, S.; Tang, J.; Zhou, L.; Song, H.; et al. C-Reactive Protein Inhibits Adiponectin Gene Expression and Secretion in 3T3-L1 Adipocytes. J. Endocrinol. 2007, 194, 275–281. [Google Scholar] [CrossRef]
- Schwedler, S.B.; Hansen-Hagge, T.; Reichert, M.; Schmiedeke, D.; Schneider, R.; Galle, J.; Potempa, L.A.; Wanner, C.; Filep, J.G. Monomeric C-Reactive Protein Decreases Acetylated LDL Uptake in Human Endothelial Cells. Clin. Chem. 2009, 55, 1728–1731. [Google Scholar] [CrossRef] [PubMed]
- Zhao, X.Q.; Zhang, M.W.; Wang, F.; Zhao, Y.X.; Li, J.J.; Wang, X.P.; Bu, P.L.; Yang, J.M.; Liu, X.L.; Zhang, M.X.; et al. CRP Enhances Soluble LOX-1 Release from Macrophages by Activating TNF-α Converting Enzyme. J. Lipid Res. 2011, 52, 923–933. [Google Scholar] [CrossRef]
- Li, H.-Y.; Wang, J.; Meng, F.; Jia, Z.-K.; Su, Y.; Bai, Q.-F.; Lv, L.-L.; Ma, F.-R.; Potempa, L.A.; Yan, Y.-B.; et al. An Intrinsically Disordered Motif Mediates Diverse Actions of Monomeric C-Reactive Protein. J. Biol. Chem. 2016, 291, 8795–8804. [Google Scholar] [CrossRef]
- Li, H.-Y.; Gao, N.; Liu, C.-Y.; Liu, X.-L.; Wu, F.; Dai, N.; Han, J.; Li, Q.-Y. The Cholesterol-Binding Sequence in Monomeric C-Reactive Protein Binds to the SARS-CoV-2 Spike Receptor-Binding Domain and Blocks Interaction with Angiotensin-Converting Enzyme 2. Front. Immunol. 2022, 13, 918731. [Google Scholar] [CrossRef]
- Jia, Z.-K.; Li, H.-Y.; Liang, Y.-L.; Potempa, L.A.; Ji, S.-R.; Wu, Y. Corrigendum: Monomeric C-Reactive Protein Binds and Neutralizes Receptor Activator of NF-κB Ligand-Induced Osteoclast Differentiation. Front. Immunol. 2020, 11, 619847. [Google Scholar] [CrossRef]
- Mouliou, D.S.; Dardiotis, E. Current Evidence in SARS-CoV-2 mRNA Vaccines and Post-Vaccination Adverse Reports: Knowns and Unknowns. Diagnostics 2022, 12, 1555. [Google Scholar] [CrossRef]
- Ruiz-Fernández, C.; Gonzalez-Rodríguez, M.; Francisco, V.; Rajab, I.M.; Gómez, R.; Conde, J.; Lago, F.; Pino, J.; Mobasheri, A.; Gonzalez-Gay, M.A.; et al. Monomeric C-Reactive Protein (mCRP) Regulates Inflammatory Responses in Human and Mouse Chondrocytes. Lab. Investig. 2021, 101, 1550–1560. [Google Scholar] [CrossRef]
- Slevin, M.; Heidari, N.; Azamfirei, L. Monomeric C-Reactive Protein: Current Perspectives for Utilization and Inclusion as a Prognostic Indicator and Therapeutic Target. Front. Immunol. 2022, 13, 866379. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Na, H.; Gan, Q.; Tao, Q.; Alekseyev, Y.; Hu, J.; Yan, Z.; Yang, J.B.; Tian, H.; Zhu, S.; et al. Monomeric C-reactive Protein via Endothelial CD31 for Neurovascular Inflammation in an ApoE Genotype-dependent Pattern: A Risk Factor for Alzheimer’s Disease? Aging Cell 2021, 20, e13501. [Google Scholar] [CrossRef]
- Al-Baradie, R.S.; Abdel-Hadi, A.; Ahmad, F.; Alsagaby, S.A.; Slevin, M.; Alturaiki, W.; Madkhali, Y.; Aljarallah, B.M.; Alqahtani, M.; Miraj, M.; et al. Association of Monomeric C-Reactive Protein (m-CRP) with Hypothalamic Neurons after CRP Hippo-Campal Administration in a Model of Dementia. Eur. Rev. Med. Pharmacol. Sci. 2022, 26, 8713–8718. [Google Scholar] [CrossRef]
- Di Napoli, M.; Slevin, M.; Popa-Wagner, A.; Singh, P.; Lattanzi, S.; Divani, A.A. Monomeric C-Reactive Protein and Cerebral Hemorrhage: From Bench to Bedside. Front. Immunol. 2018, 9, 1921. [Google Scholar] [CrossRef] [PubMed]
- Slevin, M.; Matou-Nasri, S.; Turu, M.; Luque, A.; Rovira, N.; Badimon, L.; Boluda, S.; Potempa, L.; Sanfeliu, C.; De Vera, N.; et al. Modified C-Reactive Protein Is Expressed by Stroke Neovessels and Is a Potent Activator of Angiogenesis In Vitro: MCRP in Stroke Microvessels. Brain Pathol. 2010, 20, 151–165. [Google Scholar] [CrossRef] [PubMed]
- Molins, B.; Pascual, A.; Méndez; Llorenç, V.; Zarranz-Ventura, J.; Mesquida, M.; Adán, A.; Martorell, J. C-Reactive Protein Isoforms Differentially Affect Outer Blood-Retinal Barrier Integrity and Function. Am. J. Physiol. Cell Physiol. 2017, 312, C244–C253. [Google Scholar] [CrossRef]
- Molins, B.; Fuentes-Prior, P.; Adán, A.; Antón, R.; Arostegui, J.I.; Yagüe, J.; Dick, A.D. Complement Factor H Binding of Monomeric C-Reactive Protein Downregulates Proinflammatory Activity and Is Impaired with at Risk Polymorphic CFH Variants. Sci. Rep. 2016, 6, 22889. [Google Scholar] [CrossRef]
- Blizniukov, O.P.; Kozmin, L.D.; Falikova, V.V.; Titov, V.N.; Belen’kiĭ, A.G.; Tishchenko, V.M. Hydrodynamic parameters of native C-reactive protein molecule in a solution. Biofizika 2003, 48, 11–17. [Google Scholar]
- Kopp, A.; Hebecker, M.; Svobodová, E.; Józsi, M. Factor H: A Complement Regulator in Health and Disease, and a Mediator of Cellular Interactions. Biomolecules 2012, 2, 46–75. [Google Scholar] [CrossRef]
- Strang, F.; Schunkert, H. C-Reactive Protein and Coronary Heart Disease: All Said—Is Not It? Mediat. Inflamm. 2014, 2014, e757123. [Google Scholar] [CrossRef]
- Jones, S.A.; Novick, D.; Horiuchi, S.; Yamamoto, N.; Szalai, A.J.; Fuller, G.M. C-Reactive Protein: A Physiological Activator of Interleukin 6 Receptor Shedding. J. Exp. Med. 1999, 189, 599–604. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Liu, S.-H.; Wright, T.T.; Shen, Z.-Y.; Li, H.-Y.; Zhu, W.; Potempa, L.A.; Ji, S.-R.; Szalai, A.J.; Wu, Y. C-Reactive Protein Directly Suppresses Th1 Cell Differentiation and Alleviates Experimental Autoimmune Encephalomyelitis. J. Immunol. 2015, 194, 5243–5252. [Google Scholar] [CrossRef]
- Eisenhardt, S.U.; Thiele, J.R.; Bannasch, H.; Stark, G.B.; Peter, K. C-reactive protein: How conformational changes influence inflammatory properties. Cell Cycle 2009, 8, 3885–3892. [Google Scholar] [CrossRef] [PubMed]
- Polevshchikov, A.V.; Nazarov, P.G.; Berestovaia, L.K. C-reactive protein modulates neutrophil adhesiveness and biocidal activity. Zh. Mikrobiol. Epidemiol. Immunobiol. 1994, 69–72. [Google Scholar]
- Zouki, C.; Beauchamp, M.; Baron, C.; Filep, J.G. Prevention of In Vitro Neutrophil Adhesion to Endothelial Cells through Shedding of L-Selectin by C-Reactive Protein and Peptides Derived from C-Reactive Protein. J. Clin. Investig. 1997, 100, 522–529. [Google Scholar] [CrossRef]
- Agrawal, A.; Gang, T.B.; Rusiñol, A.E. Recognition Functions of Pentameric C-Reactive Protein in Cardiovascular Disease. Mediat. Inflamm. 2014, 2014, e319215. [Google Scholar] [CrossRef]
- Maingrette, F.; Li, L.; Renier, G. C-Reactive Protein Enhances Macrophage Lipoprotein Lipase Expression. J. Lipid Res. 2008, 49, 1926–1935. [Google Scholar] [CrossRef]
- Miller, Y.I.; Viriyakosol, S.; Binder, C.J.; Feramisco, J.R.; Kirkland, T.N.; Witztum, J.L. Minimally Modified LDL Binds to CD14, Induces Macrophage Spreading via TLR4/MD-2, and Inhibits Phagocytosis of Apoptotic Cells. J. Biol. Chem. 2003, 278, 1561–1568. [Google Scholar] [CrossRef]
- Eisenhardt, S.U.; Starke, J.; Thiele, J.R.; Murphy, A.; Björn Stark, G.; Bassler, N.; Sviridov, D.; Winkler, K.; Peter, K. Pentameric CRP Attenuates Inflammatory Effects of MmLDL by Inhibiting MmLDL-Monocyte Interactions. Atherosclerosis 2012, 224, 384–393. [Google Scholar] [CrossRef] [PubMed]
- Devaraj, S.; Venugopal, S.; Jialal, I. Native Pentameric C-Reactive Protein Displays More Potent pro-Atherogenic Activities in Human Aortic Endothelial Cells than Modified C-Reactive Protein. Atherosclerosis 2006, 184, 48–52. [Google Scholar] [CrossRef] [PubMed]
- Krayem, I.; Bazzi, S.; Karam, M. The combination of CRP isoforms with oxLDL decreases TNF-α and IL-6 release by U937-derived macrophages. Biomed. Rep. 2017, 7, 272–276. [Google Scholar] [CrossRef]
- Ngwa, D.N.; Agrawal, A. Structurally Altered, Not Wild-Type, Pentameric C-Reactive Protein Inhibits Formation of Amyloid-β Fibrils. J. Immunol. 2022, 209, 1180–1188. [Google Scholar] [CrossRef] [PubMed]
- Blaschke, F.; Bruemmer, D.; Yin, F.; Takata, Y.; Wang, W.; Fishbein, M.C.; Okura, T.; Higaki, J.; Graf, K.; Fleck, E.; et al. C-reactive protein induces apoptosis in human coronary vascular smooth muscle cells. Circulation 2004, 110, 579–587. [Google Scholar] [CrossRef] [PubMed]
- Du Clos, T.W. Function of C-Reactive Protein. Ann. Med. 2000, 32, 274–278. [Google Scholar] [CrossRef] [PubMed]
- Csincsi, Á.I.; Szabó, Z.; Bánlaki, Z.; Uzonyi, B.; Cserhalmi, M.; Kárpáti, É.; Tortajada, A.; Caesar, J.J.E.; Prohászka, Z.; Jokiranta, T.S.; et al. FHR-1 Binds to C-Reactive Protein and Enhances Rather than Inhibits Complement Activation. J. Immunol. 2017, 199, 292–303. [Google Scholar] [CrossRef]
- Weiner, S.M.; Prasauskas, V.; Lebrecht, D.; Weber, S.; Peter, H.H.; Vaith, P. Occurrence of C-Reactive Protein in Cryoglobulins. Clin. Exp. Immunol. 2001, 125, 316–322. [Google Scholar] [CrossRef]
- Devaraj, S.; Du Clos, T.W.; Jialal, I. Binding and Internalization of C-Reactive Protein by Fcgamma Receptors on Human Aortic Endothelial Cells Mediates Biological Effects. ATVB 2005, 25, 1359–1363. [Google Scholar] [CrossRef]
- Kibayashi, E.; Urakaze, M.; Kobashi, C.; Kishida, M.; Takata, M.; Akira, S.A.T.O.; Yamazaki, K.; Kobayashi, M. Inhibitory effect of pitavastatin (NK-104) on the C-reactive-protein-induced interleukin-8 production in human aortic endothelial cells. Clin. Sci. 2005, 108, 515–521. [Google Scholar] [CrossRef]
- Wigmore, S.J.; Fearon, K.C.; Maingay, J.P.; Lai, P.B.; Ross, J.A. Interleukin-8 can mediate acute-phase protein production by isolated human hepatocytes. Am. J. Physiol. 1997, 273, E720–E726. [Google Scholar] [CrossRef] [PubMed]
- Inatsu, A.; Kinoshita, M.; Nakashima, H.; Shimizu, J.; Saitoh, D.; Tamai, S.; Seki, S. Novel mechanism of C-reactive protein for enhancing mouse liver innate immunity. Hepatology 2009, 49, 2044–2054. [Google Scholar] [CrossRef]
- Richter, K.; Sagawe, S.; Hecker, A.; Küllmar, M.; Askevold, I.; Damm, J.; Heldmann, S.; Pöhlmann, M.; Ruhrmann, S.; Sander, M.; et al. C-Reactive Protein Stimulates Nicotinic Acetylcholine Receptors to Control ATP-Mediated Monocytic Inflammasome Activation. Front. Immunol. 2018, 9, 1604. [Google Scholar] [CrossRef]
- Bisoendial, R.J.; Kastelein, J.J.P.; Levels, J.H.M.; Zwaginga, J.J.; Van Den Bogaard, B.; Reitsma, P.H.; Meijers, J.C.M.; Hartman, D.; Levi, M.; Stroes, E.S.G. Activation of Inflammation and Coagulation After Infusion of C-Reactive Protein in Humans. Circ. Res. 2005, 96, 714–716. [Google Scholar] [CrossRef]
- Heuertz, R.M.; Schneider, G.P.; Potempa, L.A.; Webster, R.O. Native and Modified C-Reactive Protein Bind Different Receptors on Human Neutrophils. Int. J. Biochem. Cell Biol. 2005, 37, 320–335. [Google Scholar] [CrossRef]
- Lu, J.; Marjon, K.D.; Marnell, L.L.; Wang, R.; Mold, C.; Du Clos, T.W.; Sun, P. Recognition and Functional Activation of the Human IgA Receptor (FcαRI) by C-Reactive Protein. Proc. Natl. Acad. Sci. USA 2011, 108, 4974–4979. [Google Scholar] [CrossRef]
- Adukauskienė, D.; Čiginskienė, A.; Adukauskaitė, A.; Pentiokinienė, D.; Šlapikas, R.; Čeponienė, I. Clinical Relevance of High Sensitivity C-Reactive Protein in Cardiology. Medicina 2016, 52, 1–10. [Google Scholar] [CrossRef] [PubMed]
- Tanigaki, K.; Mineo, C.; Yuhanna, I.S.; Chambliss, K.L.; Quon, M.J.; Bonvini, E.; Shaul, P.W. C-Reactive Protein Inhibits Insulin Activation of Endothelial Nitric Oxide Synthase via the Immunoreceptor Tyrosine-Based Inhibition Motif of FcγRIIB and SHIP-1. Circ. Res. 2009, 104, 1275–1282. [Google Scholar] [CrossRef] [PubMed]
- Wallukat, G.; Mattecka, S.; Wenzel, K.; Schrödl, W.; Vogt, B.; Brunner, P.; Sheriff, A.; Kunze, R. C-Reactive Protein (CRP) Blocks the Desensitization of Agonistic Stimulated G Protein Coupled Receptors (GPCRs) in Neonatal Rat Cardiomyocytes. J. Clin. Med. 2022, 11, 1058. [Google Scholar] [CrossRef]
- Liu, N.; Liu, J.; Ji, Y.; Lu, P. Toll-Like Receptor 4 Signaling Mediates Inflammatory Activation Induced by C-Reactive Protein in Vascular Smooth Muscle Cells. CPB 2010, 25, 467–476. [Google Scholar] [CrossRef] [PubMed]
- Nabata, A.; Kuroki, M.; Ueba, H.; Hashimoto, S.; Umemoto, T.; Wada, H.; Yasu, T.; Saito, M.; Momomura, S.-I.; Kawakami, M. C-Reactive Protein Induces Endothelial Cell Apoptosis and Matrix Metalloproteinase-9 Production in Human Mononuclear Cells: Implications for the Destabilization of Atherosclerotic Plaque. Atherosclerosis 2008, 196, 129–135. [Google Scholar] [CrossRef] [PubMed]
- Hsuchou, H.; Kastin, A.J.; Mishra, P.K.; Pan, W. C-Reactive Protein Increases BBB Permeability: Implications for Obesity and Neuroinflammation. CPB 2012, 30, 1109–1119. [Google Scholar] [CrossRef] [PubMed]
- Zwaka, T.P.; Hombach, V.; Torzewski, J. C-Reactive Protein-Mediated Low Density Lipoprotein Uptake by Macrophages: Implications for Atherosclerosis. Circulation 2001, 103, 1194–1197. [Google Scholar] [CrossRef]
- Tugal, D.; Liao, X.; Jain, M.K. TIS21 (/BTG2/PC3) as a link between ageing and cancer: Cell cycle regulator and endogenous cell death molecule. Arterioscler. Thromb. Vasc. Biol. 2013, 33, 1135–1144. [Google Scholar] [CrossRef]
- Kim, Y.; Ryu, J.; Ryu, M.S.; Lim, S.; Han, K.O.; Lim, I.K.; Han, K.H. C-reactive protein induces G2/M phase cell cycle arrest and apoptosis in monocytes through the upregulation of B-cell translocation gene 2 expression. FEBS Lett. 2014, 588, 625–631. [Google Scholar] [CrossRef]
- Hart, S.P.; Alexander, K.M.; MacCall, S.M.; Dransfield, I. C-Reactive Protein Does Not Opsonize Early Apoptotic Human Neutrophils, but Binds Only Membrane-Permeable Late Apoptotic Cells and Has No Effect on Their Phagocytosis by Macrophages. J. Inflamm. 2005, 2, 5. [Google Scholar] [CrossRef]
- Devaraj, S.; Yun, J.-M.; Duncan-Staley, C.; Jialal, I. C-Reactive Protein Induces M-CSF Release and Macrophage Proliferation. J. Leukoc. Biol. 2009, 85, 262–267. [Google Scholar] [CrossRef]
- Mortensen, R.F.; Zhong, W. Regulation of Phagocytic Leukocyte Activities by C-Reactive Protein. J. Leukoc. Biol. 2000, 67, 495–500. [Google Scholar] [CrossRef]
- Secchiero, P.; Rimondi, E.; Di Iasio, M.G.; Agnoletto, C.; Melloni, E.; Volpi, I.; Zauli, G. C-Reactive Protein Downregulates TRAIL Expression in Human Peripheral Monocytes via an Egr-1–Dependent Pathway. Clin. Cancer Res. 2013, 19, 1949–1959. [Google Scholar] [CrossRef]
- Lepik, K.; Annilo, T.; Kukuškina, V.; eQTLGen Consortium; Kisand, K.; Kutalik, Z.; Peterson, P.; Peterson, H. C-Reactive Protein Upregulates the Whole Blood Expression of CD59—An Integrative Analysis. PLoS Comput. Biol. 2017, 13, e1005766. [Google Scholar] [CrossRef]
- Chen, J.; Huang, L.; Song, M.; Yu, S.; Gao, P.; Jing, J. C-Reactive Protein Upregulates Receptor for Advanced Glycation End Products Expression and Alters Antioxidant Defenses in Rat Endothelial Progenitor Cells. J. Cardiovasc. Pharmacol. 2009, 53, 359. [Google Scholar] [CrossRef]
- Jimenez, R.V.; Kuznetsova, V.; Connelly, A.N.; Hel, Z.; Szalai, A.J. C-Reactive Protein Promotes the Expansion of Myeloid Derived Cells with Suppressor Functions. Front. Immunol. 2019, 10, 2183. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, R.V.; Wright, T.T.; Jones, N.R.; Wu, J.; Gibson, A.W.; Szalai, A.J. C-Reactive Protein Impairs Dendritic Cell Development, Maturation, and Function: Implications for Peripheral Tolerance. Front. Immunol. 2018, 9, 372. [Google Scholar] [CrossRef] [PubMed]
- Kim, E.-S.; Kim, S.Y.; Koh, M.; Lee, H.-M.; Kim, K.; Jung, J.; Kim, H.S.; Moon, W.K.; Hwang, S.; Moon, A. C-Reactive Protein Binds to Integrin A2 and Fcγ Receptor I, Leading to Breast Cell Adhesion and Breast Cancer Progression. Oncogene 2018, 37, 28–38. [Google Scholar] [CrossRef] [PubMed]
- Das, T.; Mandal, C.; Mandal, C. Variations in Binding Characteristics of Glycosylated Human C-Reactive Proteins in Different Pathological Conditions. Glycoconj. J. 2003, 20, 537–543. [Google Scholar] [CrossRef]
- Okemefuna, A.I.; Stach, L.; Rana, S.; Buetas, A.J.; Gor, J.; Perkins, S.J. C-reactive protein exists in an NaCl concentration-dependent pentamer-decamer equilibrium in physiological buffer. J. Biol. Chem. 2010, 285, 1041–1052. [Google Scholar] [CrossRef]
- Sjöwall, C.; Wetterö, J. Pathogenic Implications for Autoantibodies against C-Reactive Protein and Other Acute Phase Proteins. Clin. Chim. Acta 2007, 378, 13–23. [Google Scholar] [CrossRef]
- Bell, S.A.; Faust, H.; Schmid, A.; Meurer, M. Autoantibodies to C-Reactive Protein (CRP) and Other Acute-Phase Proteins in Systemic Autoimmune Diseases. Clin. Exp. Immunol. 2001, 113, 327–332. [Google Scholar] [CrossRef]
- Fujita, C.; Sakurai, Y.; Yasuda, Y.; Takada, Y.; Huang, C.-L.; Fujita, M. Anti-Monomeric C-Reactive Protein Antibody Ameliorates Arthritis and Nephritis in Mice. J. Immunol. 2021, 207, 1755–1762. [Google Scholar] [CrossRef]
- Jakuszko, K.; Krajewska, M.; Hałoń, A.; Kościelska-Kasprzak, K.; Myszka, M.; Żabińska, M.; Augustyniak-Bartosik, H.; Rukasz, D.; Weyde, W.; Klinger, M. Pathogenic Role of Antibodies against Monomeric C-Reactive Protein in Tubulointerstitial Nephritis and Uveitis Syndrome. Intern. Med. J. 2014, 44, 809–812. [Google Scholar] [CrossRef]
- Tan, Y.; Yu, F.; Qu, Z.; Su, T.; Xing, G.-Q.; Wu, L.-H.; Wang, F.-M.; Liu, G.; Yang, L.; Zhao, M.-H. Modified C-Reactive Protein Might Be a Target Autoantigen of TINU Syndrome. Clin. J. Am. Soc. Nephrol. 2011, 6, 93. [Google Scholar] [CrossRef]
- Pu, L.; Zhang, P.; Li, G. IgG4-Related Acute Interstitial Nephritis and the Potential Role of mCRP Autoantibodies: A Case Report. Ren. Fail. 2019, 41, 657–661. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Tan, Y.; Yu, F.; Zhao, M. Interference of Antimodified C-Reactive Protein Autoantibodies from Lupus Nephritis in the Biofunctions of Modified C-Reactive Protein. Hum. Immunol. 2012, 73, 156–163. [Google Scholar] [CrossRef] [PubMed]
- Kraszewska-Głomba, B.; Myszka, M.; Krajewska, M.; Szenborn, L. High Prevalence of Autoantibodies Against Monomeric C Reactive Protein (CRP) in Children with PFAPA Syndrome. J. Med. Biochem. 2018, 37, 507–509. [Google Scholar] [CrossRef] [PubMed]
- Bondanza, A.; Zimmermann, V.S.; Dell’Antonio, G.; Cin, E.D.; Balestrieri, G.; Tincani, A.; Amoura, Z.; Piette, J.-C.; Sabbadini, M.G.; Rovere-Querini, P.; et al. Requirement of Dying Cells and Environmental Adjuvants for the Induction of Autoimmunity. Arthritis Rheum. 2004, 50, 1549–1560. [Google Scholar] [CrossRef] [PubMed]
- Tai, A.W.-H.; Newkirk, M.M. An Autoantibody Targeting Glycated IgG Is Associated with Elevated Serum Immune Complexes in Rheumatoid Arthritis (RA). Clin. Exp. Immunol. 2001, 120, 188–193. [Google Scholar] [CrossRef]
- Md Isa, S.H.; Najihah, I.; Nazaimoon, W.M.W.; Kamarudin, N.A.; Umar, N.A.; Mat, N.H.; Khalid, B.A.K. Improvement in C-Reactive Protein and Advanced Glycosylation End-Products in Poorly Controlled Diabetics Is Independent of Glucose Control. Diabetes Res. Clin. Pract. 2006, 72, 48–52. [Google Scholar] [CrossRef]
- Das, T.; Mandal, C.; Mandal, C. Protein A—A New Ligand for Human C-Reactive Protein. FEBS Letters 2004, 576, 107–113. [Google Scholar] [CrossRef]
- Janko, C.; Franz, S.; Munoz, L.E.; Siebig, S.; Winkler, S.; Schett, G.; Lauber, K.; Sheriff, A.; Van Der Vlag, J.; Herrmann, M. CRP/Anti-CRP Antibodies Assembly on the Surfaces of Cell Remnants Switches Their Phagocytic Clearance Toward Inflammation. Front. Immun. 2011, 2, 70. [Google Scholar] [CrossRef] [PubMed]
- Sjöwall, C.; Cardell, K.; Boström, E.A.; Bokarewa, M.I.; Enocsson, H.; Ekstedt, M.; Lindvall, L.; Frydén, A.; Almer, S. High Prevalence of Autoantibodies to C-Reactive Protein in Patients with Chronic Hepatitis C Infection: Association with Liver Fibrosis and Portal Inflammation. Hum. Immunol. 2012, 73, 382–388. [Google Scholar] [CrossRef]
- Wetterö, J.; Nilsson, L.; Jonasson, L.; Sjöwall, C. Reduced Serum Levels of Autoantibodies against Monomeric C-Reactive Protein (CRP) in Patients with Acute Coronary Syndrome. Clin. Chim. Acta 2009, 400, 128–131. [Google Scholar] [CrossRef]
- Onur, H.; Onur, A.R. Diagnostic Performance of Routine Blood Parameters in Periodic Fever, Aphthous Stomatitis, Pharyngitis, and Adenitis Syndrome. Clin. Lab. Anal. 2023, 37, e24934. [Google Scholar] [CrossRef]
- Bharadwaj, D.; Stein, M.-P.; Volzer, M.; Mold, C.; Clos, T.W.D. The Major Receptor for C-Reactive Protein on Leukocytes Is Fcγ Receptor II. J. Exp. Med. 1999, 190, 585–590. [Google Scholar] [CrossRef] [PubMed]
- Stein, M.-P.; Edberg, J.C.; Kimberly, R.P.; Mangan, E.K.; Bharadwaj, D.; Mold, C.; Clos, T.W.D. C-Reactive Protein Binding to FcγRIIa on Human Monocytes and Neutrophils Is Allele-Specific. J. Clin. Investig. 2000, 105, 369–376. [Google Scholar] [CrossRef]
- Ji, S.-R.; Wu, Y.; Potempa, L.A.; Liang, Y.-H.; Zhao, J. Effect of Modified C-Reactive Protein on Complement Activation: A Possible Complement Regulatory Role of Modified or Monomeric C-Reactive Protein in Atherosclerotic Lesions. ATVB 2006, 26, 935–941. [Google Scholar] [CrossRef] [PubMed]
- Hundt, M.; Zielinska-Skowronek, M.; Schmidt, R.E. Lack of Specific Receptors for C-Reactive Protein on White Blood Cells. Eur. J. Immunol. 2001, 31, 3475–3483. [Google Scholar] [CrossRef] [PubMed]
- Zeller, J.M.; Kubak, B.M.; Gewurz, H. Binding Sites for C-Reactive Protein on Human Monocytes Are Distinct from IgG Fc Receptors. Immunology 1989, 67, 51–55. [Google Scholar]
- Swanson, J.A.; Hoppe, A.D. The Coordination of Signaling during Fc Receptor-Mediated Phagocytosis. J. Leukoc. Biol. 2004, 76, 1093–1103. [Google Scholar] [CrossRef]
- Brennan, M.P.; Moriarty, R.D.; Grennan, S.; Chubb, A.J.; Cox, D. C-Reactive Protein Binds to AlphaIIbbeta3. J. Thromb. Haemost. 2008, 6, 1239–1241. [Google Scholar] [CrossRef]
- Marnell, L.; Mold, C.; Du Clos, T.W. C-Reactive Protein: Ligands, Receptors and Role in Inflammation. Clin. Immunol. 2005, 117, 104–111. [Google Scholar] [CrossRef]
- Szalai, A.J. The Antimicrobial Activity of C-Reactive Protein. Microbes Infect. 2002, 4, 201–205. [Google Scholar] [CrossRef]
- Tanio, M.; Wakamatsu, K.; Kohno, T. Binding Site of C-Reactive Protein on M-Ficolin. Mol. Immunol. 2009, 47, 215–221. [Google Scholar] [CrossRef] [PubMed]
- Lee, R.T.; Lee, Y.C. Carbohydrate Ligands of Human C-Reactive Protein: Binding of Neoglycoproteins Containing Galactose-6-Phosphate and Galactose-Terminated Disaccharide. Glycoconj. J. 2006, 23, 317–327. [Google Scholar] [CrossRef]
- Lee, R.T.; Lee, Y.C. Carbohydrate-Binding Properties of Human Neo-CRP and Its Relationship to Phosphorylcholine-Binding Site. Glycobiology 2003, 13, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Culley, F.J. C-Reactive Protein Binds to Phosphorylated Carbohydrates. Glycobiology 2000, 10, 59–65. [Google Scholar] [CrossRef]
- Mihlan, M.; Hebecker, M.; Dahse, H.M.; Hälbich, S.; Huber-Lang, M.; Dahse, R.; Zipfel, P.F.; Józsi, M. Human complement factor H-related protein 4 binds and recruits native pentameric C-reactive protein to necrotic cells. Mol. Immunol. 2009, 46, 335–344. [Google Scholar] [CrossRef] [PubMed]
- Frangogiannis, N.G. Monomeric C-reactive protein and inflammatory injury in myocardial infarction. Cardiovasc. Res. 2012, 96, 4–6. [Google Scholar] [CrossRef] [PubMed]
- Hammond, D.J.; Singh, S.K.; Thompson, J.A.; Beeler, B.W.; Rusiñol, A.E.; Pangburn, M.K.; Potempa, L.A.; Agrawal, A. Identification of Acidic PH-Dependent Ligands of Pentameric C-Reactive Protein. J. Biol. Chem. 2010, 285, 36235–36244. [Google Scholar] [CrossRef]
- Taskinen, S.; Kovanen, P.T.; Jarva, H.; Meri, S.; Pentikäinen, M.O. Binding of C-Reactive Protein to Modified Low-Density-Lipoprotein Particles: Identification of Cholesterol as a Novel Ligand for C-Reactive Protein. Biochem. J. 2002, 367, 403–412. [Google Scholar] [CrossRef]
- Taskinen, S.; Hyvönen, M.; Kovanen, P.T.; Meri, S.; Pentikäinen, M.O. C-Reactive Protein Binds to the 3beta-OH Group of Cholesterol in LDL Particles. Biochem. Biophys. Res. Commun. 2005, 329, 1208–1216. [Google Scholar] [CrossRef]
- Oka, Y.; Ushiba, S.; Miyakawa, N.; Nishio, M.; Ono, T.; Kanai, Y.; Watanabe, Y.; Tani, S.; Kimura, M.; Matsumoto, K. Ionic Strength-Sensitive and pH-Insensitive Interactions between C-Reactive Protein (CRP) and an Anti-CRP Antibody. Biophys. Physicobiol. 2022, 19, e190003. [Google Scholar] [CrossRef] [PubMed]
- Braig, D.; Nero, T.L.; Koch, H.-G.; Kaiser, B.; Wang, X.; Thiele, J.R.; Morton, C.J.; Zeller, J.; Kiefer, J.; Potempa, L.A.; et al. Transitional Changes in the CRP Structure Lead to the Exposure of Proinflammatory Binding Sites. Nat. Commun. 2017, 8, 14188. [Google Scholar] [CrossRef]
- Pathak, A.; Singh, S.K.; Thewke, D.P.; Agrawal, A. Conformationally Altered C-Reactive Protein Capable of Binding to Atherogenic Lipoproteins Reduces Atherosclerosis. Front. Immunol. 2020, 11, 1780. [Google Scholar] [CrossRef] [PubMed]
- Agrawal, A.; Simpson, M.J.; Black, S.; Carey, M.P.; Samols, D. A C-Reactive Protein Mutant That Does Not Bind to Phosphocholine and Pneumococcal C-Polysaccharide. J. Immunol. 2002, 169, 3217–3222. [Google Scholar] [CrossRef]
- Casas, J.P.; Shah, T.; Hingorani, A.D.; Danesh, J.; Pepys, M.B. C-Reactive Protein and Coronary Heart Disease: A Critical Review. J. Intern. Med. 2008, 264, 295–314. [Google Scholar] [CrossRef]
- Buckley, D.I.; Fu, R.; Freeman, M.; Rogers, K.; Helfand, M. C-Reactive Protein as a Risk Factor for Coronary Heart Disease: A Systematic Review and Meta-analyses for the U.S. Preventive Services Task Force. Ann. Intern. Med. 2009, 151, 483. [Google Scholar] [CrossRef] [PubMed]
- Ridker, P.M.; Cook, N. Clinical Usefulness of Very High and Very Low Levels of C-Reactive Protein across the Full Range of Framingham Risk Scores. Circulation 2004, 109, 1955–1959. [Google Scholar] [CrossRef]
- Bassuk, S.S.; Rifai, N.; Ridker, P.M. High-Sensitivity C-Reactive Protein: Clinical Importance. Curr. Probl. Cardiol. 2004, 29, 439–493. [Google Scholar] [CrossRef] [PubMed]
- Bera, D.; Shanthi Naidu, K.; Kaur Saggu, D.; Yalagudri, S.; Kishor Kadel, J.; Sarkar, R.; Narasimhan, C. Serum Angiotensin Converting Enzyme, Erythrocyte Sedimentation Rate and High Sensitive-C Reactive Protein Levels in Diagnosis of Cardiac Sarcoidosis—Where Do We Stand? Indian Pacing Electrophysiol. J. 2020, 20, 184–188. [Google Scholar] [CrossRef] [PubMed]
- Kang, S.; Fan, L.-Y.; Chen, M.; Li, J.; Liu, Z.-M. Relationship of High-Sensitivity C-Reactive Protein Concentrations and Systolic Heart Failure. Curr. Vasc. Pharmacol. 2017, 15, 390–396. [Google Scholar] [CrossRef] [PubMed]
- Michowitz, Y.; Arbel, Y.; Wexler, D.; Sheps, D.; Rogowski, O.; Shapira, I.; Berliner, S.; Keren, G.; George, J.; Roth, A. Predictive Value of High Sensitivity CRP in Patients with Diastolic Heart Failure. Int. J. Cardiol. 2008, 125, 347–351. [Google Scholar] [CrossRef] [PubMed]
- Celik, T.; Iyisoy, A.; Celik, M.; Yuksel, U.C.; Kardesoglu, E. C-Reactive Protein in Chronic Heart Failure: A New Predictor of Survival. Int. J. Cardiol. 2009, 135, 396–397. [Google Scholar] [CrossRef]
- Chivite, D.; Franco, J.; Formiga, F.; Salamanca-Bautista, P.; Manzano, L.; Conde-Martel, A.; Arévalo-Lorido, J.C.; Suárez-Pedreira, I.; Casado-Cerrada, J.; Montero-Pérez-Barquero, M. Valor pronóstico a corto plazo de la proteína C reactiva en ancianos con insuficiencia cardíaca aguda. Rev. Clín. Española 2019, 219, 10–17. [Google Scholar] [CrossRef] [PubMed]
- Świątkiewicz, I.; Magielski, P.; Kubica, J. C-Reactive Protein as a Risk Marker for Post-Infarct Heart Failure over a Multi-Year Period. Int. J. Mol. Sci. 2021, 22, 3169. [Google Scholar] [CrossRef]
- Lakhani, I.; Wong, M.V.; Hung, J.K.F.; Gong, M.; Waleed, K.B.; Xia, Y.; Lee, S.; Roever, L.; Liu, T.; Tse, G.; et al. Diagnostic and Prognostic Value of Serum C-Reactive Protein in Heart Failure with Preserved Ejection Fraction: A Systematic Review and Meta-Analysis. Heart Fail. Rev. 2021, 26, 1141–1150. [Google Scholar] [CrossRef]
- Ribeiro, É.C.T.; Sangali, T.D.; Clausell, N.O.; Perry, I.S.; Souza, G.C. C-Reactive Protein and Frailty in Heart Failure. Am. J. Cardiol. 2022, 166, 65–71. [Google Scholar] [CrossRef]
- Biasucci, L.; Liuzzo, G.; Colizzi, C.; Rizzello, V. Clinical Use of C-Reactive Protein for the Prognostic Stratification of Patients with Ischaemic Heart Disease. Ital. Heart J. 2001, 2, 164–171. [Google Scholar] [CrossRef]
- Al Aseri, Z.A.; Habib, S.S.; Marzouk, A. Predictive Value of High Sensitivity C-Reactive Protein on Progression to Heart Failure Occurring after the First Myocardial Infarction. Vasc. Health Risk Manag. 2019, 15, 221–227. [Google Scholar] [CrossRef] [PubMed]
- Ueda, S.; Ikeda, U.; Yamamoto, K.; Takahashi, M.; Nishinaga, M.; Nago, N.; Shimada, K. C-Reactive Protein as a Predictor of Cardiac Rupture after Acute Myocardial Infarction. Am. Heart J. 1996, 131, 857–860. [Google Scholar] [CrossRef]
- Pietilä, K.O.; Harmoinen, A.P.; Jokiniitty, J.; Pasternack, A.I. Serum C-Reactive Protein Concentration in Acute Myocardial Infarction and Its Relationship to Mortality during 24 Months of Follow-up in Patients under Thrombolytic Treatment. Eur. Heart J. 1996, 17, 1345–1349. [Google Scholar] [CrossRef] [PubMed]
- Hou, M.; Ren, Y.-P.; Wang, R.; Lu, L.-X. Early Cardiopulmonary Resuscitation on Serum Levels of Myeloperoxidase, Soluble ST2, and Hypersensitive C-Reactive Protein in Acute Myocardial Infarction Patients. World J. Clin. Cases 2021, 9, 10585–10594. [Google Scholar] [CrossRef] [PubMed]
- Wang, C.-G.; Qin, X.-C.; Nie, S.-P.; Wang, C.-M.; Ai, H.; Que, B. C-Reactive Protein as a Predictor of Malignant Ventricular Arrhythmias in Non-ST Elevation Myocardial Infarction. J. Geriatr. Cardiol. 2019, 16, 614–620. [Google Scholar] [CrossRef]
- Sheriff, A.; Kayser, S.; Brunner, P.; Vogt, B. C-Reactive Protein Triggers Cell Death in Ischemic Cells. Front. Immunol. 2021, 12, 630430. [Google Scholar] [CrossRef] [PubMed]
- Nijmeijer, R.; Lagrand, W.K.; Lubbers, Y.T.P.; Visser, C.A.; Meijer, C.J.L.M.; Niessen, H.W.M.; Hack, C.E. C-Reactive Protein Activates Complement in Infarcted Human Myocardium. Am. J. Pathol. 2003, 163, 269–275. [Google Scholar] [CrossRef] [PubMed]
- Barrett, T.D.; Hennan, J.K.; Marks, R.M.; Lucchesi, B.R. C-Reactive-Protein-Associated Increase in Myocardial Infarct Size after Ischemia/Reperfusion. J. Pharmacol. Exp. Ther. 2002, 303, 1007–1013. [Google Scholar] [CrossRef] [PubMed]
- Ries, W.; Torzewski, J.; Heigl, F.; Pfluecke, C.; Kelle, S.; Darius, H.; Ince, H.; Mitzner, S.; Nordbeck, P.; Butter, C.; et al. C-Reactive Protein Apheresis as Anti-Inflammatory Therapy in Acute Myocardial Infarction: Results of the CAMI-1 Study. Front. Cardiovasc. Med. 2021, 8, 591714. [Google Scholar] [CrossRef]
- Anzulović-Mirosević, D.; Razzolini, R.; Zaninotto, M.; Plebani, M.; Mion, M.M.; Rozga, A.; Dalla-Volta, S. The C-Reactive Protein Levels in Left Ventricular Dysfunction of Different Etiology. Inflamm. Allergy Drug Targets 2009, 8, 247–251. [Google Scholar] [CrossRef]
- Swiatkiewicz, I.; Taub, P.R. The Usefulness of C-Reactive Protein for the Prediction of Post-Infarct Left Ventricular Systolic Dysfunction and Heart Failure. Kardiol. Pol. 2018, 76, 821–829. [Google Scholar] [CrossRef]
- Li, X.; Peng, S.; Wu, X.; Guan, B.; Tse, G.; Chen, S.; Zhou, G.; Wei, Y.; Gong, C.; Lu, X.; et al. C-Reactive Protein and Atrial Fibrillation: Insights from Epidemiological and Mendelian Randomization Studies. Nutr. Metab. Cardiovasc. Dis. 2022, 32, 1519–1527. [Google Scholar] [CrossRef]
- Tanaka, M.; Imano, H.; Kubota, Y.; Yamagishi, K.; Umesawa, M.; Muraki, I.; Cui, R.; Hayama-Terada, M.; Shimizu, Y.; Okada, T.; et al. Serum High-Sensitivity C-Reactive Protein Levels and the Risk of Atrial Fibrillation in Japanese Population: The Circulatory Risk in Communities Study. J. Atheroscler. Thromb. 2021, 28, 194–202. [Google Scholar] [CrossRef] [PubMed]
- Xie, J.Y.-Y.; Noeman, M.; Pimenta, D.; Little, C. C-Reactive Protein as a Predictor for Developing Post-Operative Atrial Fibrillation. Europace 2021, 23, 159. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Z.; Dai, L.; Song, Z.; Li, H.; Shu, M. Association between C-Reactive Protein and Atrial Fibrillation Recurrence after Catheter Ablation: A Meta-Analysis. Clin. Cardiol. 2013, 36, 548–554. [Google Scholar] [CrossRef]
- Marott, S.C.W.; Nordestgaard, B.G.; Zacho, J.; Friberg, J.; Jensen, G.B.; Tybjaerg-Hansen, A.; Benn, M. Does Elevated C-Reactive Protein Increase Atrial Fibrillation Risk? A Mendelian Randomization of 47,000 Individuals from the General Population. J. Am. Coll. Cardiol. 2010, 56, 789–795. [Google Scholar] [CrossRef] [PubMed]
- Zhao, L.; Li, S.; Zhang, C.; Tian, J.; Lu, A.; Bai, R.; An, J.; Greiser, A.; Huang, J.; Ma, X. Cardiovascular Magnetic Resonance-Determined Left Ventricular Myocardium Impairment Is Associated with C-Reactive Protein and ST2 in Patients with Paroxysmal Atrial Fibrillation. J. Cardiovasc. Magn. Reson. 2021, 23, 30. [Google Scholar] [CrossRef]
- Zhou, R.; Xu, J.; Luan, J.; Wang, W.; Tang, X.; Huang, Y.; Su, Z.; Yang, L.; Gu, Z. Predictive Role of C-Reactive Protein in Sudden Death: A Meta-Analysis of Prospective Studies. J. Int. Med. Res. 2022, 50, 3000605221079547. [Google Scholar] [CrossRef]
- Faulkner, J.; Kalu, F.A. C-Reactive Protein: A Prognostic Indicator for Sudden Cardiac Death Post-Myocardial Infarction. Br. J. Cardiol. 2020, 27, 39. [Google Scholar] [CrossRef] [PubMed]
- Bravo-Tobar, I.D.; Nello-Pérez, C.; Fernández, A.; Mogollón, N.; Pérez, M.C.; Verde, J.; Concepción, J.L.; Rodriguez-Bonfante, C.; Bonfante-Cabarcas, R. Adenosine deaminase activity and serum c-reactive protein as prognostic markers of chagas disease severity. Rev. Inst. Med. Trop. Sao Paulo 2015, 57, 385–392. [Google Scholar] [CrossRef] [PubMed]
- Ronnow, B.S.; Reyna, S.P.; Muhlestein, J.B.; Horne, B.D.; Allen Maycock, C.A.; Bair, T.L.; Carlquist, J.F.; Kfoury, A.G.; Anderson, J.L.; Renlund, D.G.; et al. C-Reactive Protein Predicts Death in Patients with Non-Ischemic Cardiomyopathy. Cardiology 2005, 104, 196–201. [Google Scholar] [CrossRef]
- Chirinos, J.A.; Zambrano, J.P.; Chakko, S.; Schob, A.; Veerani, A.; Perez, G.O.; Mendez, A.J. Usefulness of C-Reactive Protein as an Independent Predictor of Death in Patients with Ischemic Cardiomyopathy. Am. J. Cardiol. 2005, 95, 88–90. [Google Scholar] [CrossRef]
- Zhu, L.; Zou, Y.; Wang, Y.; Luo, X.; Sun, K.; Wang, H.; Jia, L.; Liu, Y.; Zou, J.; Yuan, Z.; et al. Prognostic Significance of Plasma High-Sensitivity C-Reactive Protein in Patients with Hypertrophic Cardiomyopathy. J. Am. Heart Assoc. 2017, 6, e004529. [Google Scholar] [CrossRef] [PubMed]
- Karaahmet, T.; Yilmaz, F.; Tigen, K.; Mutlu, B.; Cevik, C.; Basaran, Y. Diagnostic Utility of Plasma N-Terminal pro-B-Type Natriuretic Peptide and C-Reactive Protein Levels in Differential Diagnosis of Pericardial Constriction and Restrictive Cardiomyopathy. Congest. Heart Fail. 2009, 15, 265–270. [Google Scholar] [CrossRef] [PubMed]
- Bonny, A.; Lellouche, N.; Ditah, I.; Hidden-Lucet, F.; Yitemben, M.T.; Granger, B.; Larrazet, F.; Frank, R.; Fontaine, G. C-Reactive Protein in Arrhythmogenic Right Ventricular Dysplasia/Cardiomyopathy and Relationship with Ventricular Tachycardia. Cardiol. Res. Pract. 2010, 2010, e919783. [Google Scholar] [CrossRef] [PubMed]
- Feng, J.; Tian, P.; Liang, L.; Chen, Y.; Wang, Y.; Zhai, M.; Huang, Y.; Zhou, Q.; Zhao, X.; Zhao, L.; et al. Outcome and Prognostic Value of N-Terminal pro-Brain Natriuretic Peptide and High-Sensitivity C-Reactive Protein in Mildly Dilated Cardiomyopathy vs. Dilated Cardiomyopathy. ESC Heart Fail. 2022, 9, 1625–1635. [Google Scholar] [CrossRef] [PubMed]
- Gili, S.; Cammann, V.L.; Schlossbauer, S.A.; Kato, K.; D’Ascenzo, F.; Di Vece, D.; Jurisic, S.; Micek, J.; Obeid, S.; Bacchi, B.; et al. Cardiac Arrest in Takotsubo Syndrome: Results from the InterTAK Registry. Eur. Heart J. 2019, 40, 2142–2151. [Google Scholar] [CrossRef] [PubMed]
- Dai, S.; Zhang, S.; Guo, Y.H.; Chu, J.; Hua, W.; Wang, F.Z. C-Reactive Protein and Atrial Fibrillation in Idiopathic Dilated Cardiomyopathy. Clin. Cardiol. 2009, 32, E45–E50. [Google Scholar] [CrossRef]
- Sarojini, A.; Sai Ravi Shanker, A.; Anitha, M. Inflammatory Markers-Serum Level of C-Reactive Protein, Tumor Necrotic Factor-α, and Interleukin-6 as Predictors of Outcome for Peripartum Cardiomyopathy. J. Obs. Gynaecol. India 2013, 63, 234–239. [Google Scholar] [CrossRef] [PubMed]
- Biteker, M.; Özlek, B.; Özlek, E.; Çil, C.; Çelik, O.; Doğan, V.; Başaran, Ö. Predictors of Early and Delayed Recovery in Peripartum Cardiomyopathy: A Prospective Study of 52 Patients. J. Matern. Fetal Neonatal Med. 2020, 33, 390–397. [Google Scholar] [CrossRef]
- Mohanan, S.; Nair, R.G.; Vellani, H.; Sajeev, C.G.; George, B.; Krishnan, M.N. Baseline C-Reactive Protein Levels and Prognosis in Patients with Infective Endocarditis: A Prospective Cohort Study. Indian Heart J. 2018, 70 (Suppl. S3), S43–S49. [Google Scholar] [CrossRef]
- Hellgren, U.; Julander, I. Are White Blood Cell Count, Platelet Count, Erythrocyte Sedimentation Rate and C-Reactive Protein Useful in the Diagnosis of Septicaemia and Endocarditis? Scand. J. Infect. Dis. 1986, 18, 487–488. [Google Scholar] [CrossRef] [PubMed]
- Kumar, A.K.; Yesilyaprak, A.; Furqan, M.M.; Jain, V.; Montane, B.; Imazio, M.; Wang, T.K.M.; Jellis, C.L.; Cremer, P.C.; Klein, A.L. Prognostic Value of Inflammatory Markers in Idiopathic Recurrent Pericarditis. J. Am. Coll. Cardiol. 2022, 79, 1644–1645. [Google Scholar] [CrossRef] [PubMed]
- Laurier, E.; Gosset, D.; Hennache, B.; Nuttens, M.C.; Debuire, B.; Lenoir, L.; Muller, P.H. Pericardial C-reactive protein. A marker of agonal cardiac disease? Presse Med. 1991, 20, 405–408. [Google Scholar] [PubMed]
- Mager, A.; Hammer, Y.; Ofek, H.; Kedmi, I.; Iakobishvili, Z.; Kornowski, R. Prognostic and Diagnostic Significance of Serum High-Sensitivity C-Reactive Protein Level in Patients with Acute Idiopathic Pericarditis. Isr. Med. Assoc. J. 2019, 21, 747–751. [Google Scholar] [PubMed]
- Caruso, S.; Marrone, G.; Gentile, G. Case 305: Loeffler Endocarditis. Radiology 2022, 304, 736–742. [Google Scholar] [CrossRef]
- Kanda, T. C-Reactive Protein (CRP) in the Cardiovascular System. Rinsho Byori 2001, 49, 395–401. [Google Scholar]
- Baritussio, A.; Cheng, C.-Y.; Lorenzoni, G.; Basso, C.; Rizzo, S.; De Gaspari, M.; Fachin, F.; Giordani, A.S.; Ocagli, H.; Pontara, E.; et al. A Machine-Learning Model for the Prognostic Role of C-Reactive Protein in Myocarditis. J. Clin. Med. 2022, 11, 7068. [Google Scholar] [CrossRef] [PubMed]
- Silva, D.; Pais de Lacerda, A. Proteína C reativa de alta sensibilidade como biomarcador de risco na doença coronária. Rev. Port. De Cardiol. 2012, 31, 733–745. [Google Scholar] [CrossRef]
- Jia, R.-F.; Li, L.; Li, H.; Cao, X.-J.; Ruan, Y.; Meng, S.; Wang, J.-Y.; Jin, Z.-N. Meta-Analysis of C-Reactive Protein and Risk of Angina Pectoris. Am. J. Cardiol. 2020, 125, 1039–1045. [Google Scholar] [CrossRef]
- Garcia-Moll, X.; Zouridakis, E.; Cole, D.; Kaski, J.C. C-Reactive Protein in Patients with Chronic Stable Angina: Differences in Baseline Serum Concentration between Women and Men. Eur. Heart J. 2000, 21, 1598–1606. [Google Scholar] [CrossRef]
- Camaj, A.; Giustino, G.; Kocovic, N.; Cao, D.; Claessen, B.E.; Sartori, S.; Zhang, Z.; Qiu, H.; Nicolas, J.; Hinohara, T.; et al. Effect of Elevated C-Reactive Protein on Outcomes After Complex Percutaneous Coronary Intervention for Angina Pectoris. Am. J. Cardiol. 2022, 168, 47–54. [Google Scholar] [CrossRef]
- de Winter, R.J.; Koch, K.T.; van Straalen, J.P.; Heyde, G.; Bax, M.; Schotborgh, C.E.; Mulder, K.J.; Sanders, G.T.; Fischer, J.; Tijssen, J.G.P.; et al. C-Reactive Protein and Coronary Events Following Percutaneous Coronary Angioplasty. Am. J. Med. 2003, 115, 85–90. [Google Scholar] [CrossRef]
- Yuan, D.; Wang, P.; Jia, S.; Zhang, C.; Zhu, P.; Jiang, L.; Liu, R.; Xu, J.; Tang, X.; Song, Y.; et al. Lipoprotein(a), High-Sensitivity C-Reactive Protein, and Cardiovascular Risk in Patients Undergoing Percutaneous Coronary Intervention. Atherosclerosis 2022, 363, 109–116. [Google Scholar] [CrossRef]
- Galante, A.; Pietroiusti, A.; Vellini, M.; Piccolo, P.; Possati, G.; De Bonis, M.; Grillo, R.L.; Fontana, C.; Favalli, C. C-Reactive Protein Is Increased in Patients with Degenerative Aortic Valvular Stenosis. J. Am. Coll. Cardiol. 2001, 38, 1078–1082. [Google Scholar] [CrossRef]
- Su, B.-J.; Dong, Y.; Tan, C.-C.; Hou, X.-H.; Xu, W.; Sun, F.-R.; Cui, M.; Dong, Q.; Tan, L.; Yu, J.-T. Elevated Hs-CRP Levels Are Associated with Higher Risk of Intracranial Arterial Stenosis. Neurotox. Res. 2020, 37, 425–432. [Google Scholar] [CrossRef]
- Aceña, Á.; Franco Peláez, J.A.; Pello Lázaro, A.M.; Gonzalez Parra, E.; Gonzalez Lorenzo, Ó.; Martínez-Milla, J.; Hernandez, I.; Martín-Mariscal, M.L.; Lopez Castillo, M.; Kallmeyer, A.; et al. PCSK9 and HS-CRP Predict Progression of Aortic Stenosis in Patients with Stable Coronary Artery Disease. J. Cardiovasc. Trans. Res. 2021, 14, 238–245. [Google Scholar] [CrossRef]
- Wang, Y.; Shen, G.; Wang, H.; Yao, Y.; Sun, Q.; Jing, B.; Liu, G.; Wu, J.; Yuan, C.; Liu, S.; et al. Association of High Sensitivity C-Reactive Protein and Abdominal Aortic Aneurysm: A Meta-Analysis and Systematic Review. Curr. Med. Res. Opin. 2017, 33, 2145–2152. [Google Scholar] [CrossRef]
- Qin, X.-Y.; Juan, J.; Xiang, X.; Wei, Y.-Q.; Zuo, S.-W.; Huang, T.; Chen, D.-F.; Marshall, R.; Xiong, J.; Guo, W.; et al. Plasma C-Reactive Protein and Abdominal Aortic Aneurysm: A Mendelian Randomization Analysis. Chin. Med. J. 2018, 131, 2630–2633. [Google Scholar] [CrossRef] [PubMed]
- Kano, M.; Nishibe, T.; Dardik, A.; Iwahashi, T.; Ogino, H. Association of High-Sensitivity C-Reactive Protein with Aneurysm Sac Shrinkage in Patients Undergoing Endovascular Abdominal Aneurysm Repair. J. Endovasc. Ther. 2022, 29, 866–873. [Google Scholar] [CrossRef] [PubMed]
- Mori, K.; Tamune, H.; Tanaka, H.; Nakamura, M. Admission Values of D-Dimer and C-Reactive Protein (CRP) Predict the Long-Term Outcomes in Acute Aortic Dissection. Intern. Med. 2016, 55, 1837–1843. [Google Scholar] [CrossRef] [PubMed]
- Kitai, T.; Kaji, S.; Kim, K.; Ehara, N.; Tani, T.; Kinoshita, M.; Furukawa, Y. Prognostic Value of Sustained Elevated C-Reactive Protein Levels in Patients with Acute Aortic Intramural Hematoma. J. Thorac. Cardiovasc. Surg. 2014, 147, 326–331. [Google Scholar] [CrossRef]
- Jan, M.I.; Khan, R.A.; Fozia; Ahmad, I.; Khan, N.; Urooj, K.; Shah, A.U.H.A.; Khan, A.U.; Ali, T.; Ishtiaq, A.; et al. C-Reactive Protein and High-Sensitive Cardiac Troponins Correlate with Oxidative Stress in Valvular Heart Disease Patients. Oxid. Med. Cell Longev. 2022, 2022, 5029853. [Google Scholar] [CrossRef] [PubMed]
- Sharma, G.; Shetkar, S.; Bhasin, A.; Ramakrishnan, L.; Juneja, R.; Naik, N.; Roy, A.; Ramakrishnan, S.; Bhargava, B.; Bahl, V.K. High Sensitive C-Reactive Protein and Interleukin 6 in Atrial Fibrillation with Rheumatic Mitral Stenosis from Indian Cohort. Indian Heart J. 2017, 69, 505–511. [Google Scholar] [CrossRef]
- Alyan, O.; Metin, F.; Kacmaz, F.; Ozdemir, O.; Maden, O.; Topaloglu, S.; Demir, A.D.; Karahan, Z.; Karadede, A.; Ilkay, E. High Levels of High Sensitivity C-Reactive Protein Predict the Progression of Chronic Rheumatic Mitral Stenosis. J. Thromb. Thrombolysis 2009, 28, 63–69. [Google Scholar] [CrossRef]
- Kurtoğlu, E.; Korkmaz, H.; Aktürk, E.; Yılmaz, M.; Altaş, Y.; Uçkan, A. Association of Mitral Annulus Calcification with High-Sensitivity C-Reactive Protein, Which Is a Marker of Inflammation. Mediat. Inflamm. 2012, 2012, 606207. [Google Scholar] [CrossRef] [PubMed]
- Turker, Y.; Ekinozu, I.; Turker, Y.; Akkaya, M. High Levels of High-Sensitivity C-Reactive Protein and Uric Acid Can Predict Disease Severity in Patients with Mitral Regurgitation. Rev. Port Cardiol. 2014, 33, 699–706. [Google Scholar] [CrossRef] [PubMed]
- Song, J.; Zheng, Q.; Ma, X.; Zhang, Q.; Xu, Z.; Zou, C.; Wang, Z. Predictive Roles of Neutrophil-to-Lymphocyte Ratio and C-Reactive Protein in Patients with Calcific Aortic Valve Disease. Int. Heart J. 2019, 60, 345–351. [Google Scholar] [CrossRef]
- Verberkmoes, N.J.; Akca, F.; Vandevenne, A.-S.; Jacobs, L.; Hamad, M.A.S.; Van Straten, A.H.M. Significantly Elevated C-Reactive Protein Levels after Epicardial Clipping of the Left Atrial Appendage. Innovations 2018, 13, 125–131. [Google Scholar] [CrossRef] [PubMed]
- Batra, J.; Truby, L.K.; Defilippis, E.M.; Takeda, K.; Takayama, H.; Naka, Y.; Yuzefpolskaya, M.; Colombo, P.C.; Sayer, G.; Farr, M.A.; et al. C-Reactive Protein Levels Predict Outcomes in Continuous-Flow Left Ventricular Assist Device Patients: An INTERMACS Analysis. ASAIO J. 2021, 67, 884–890. [Google Scholar] [CrossRef] [PubMed]
- Farias, J.S.; Villarreal, E.G.; Dhargalkar, J.; Kleinhans, A.; Flores, S.; Loomba, R.S. C-Reactive Protein and Procalcitonin after Congenital Heart Surgery Utilizing Cardiopulmonary Bypass: When Should We Be Worried? J. Card. Surg. 2021, 36, 4301–4307. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Yu, Y.; Wang, L.; Wang, S.; Gao, Y.; Ao, H. Can C-Reactive Protein Predict Coagulation in off Pump Coronary Artery Bypass Grafting? A Cohort Study. J. Cardiothorac. Surg. 2022, 17, 225. [Google Scholar] [CrossRef] [PubMed]
- Sousa, A.L.S.; Carvalho, L.A.F.; Salgado, C.G.; de Oliveira, R.L.; Lima, L.C.C.L.E.; de Mattos, N.D.F.G.; Fagundes, F.E.S.; Colafranceschi, A.S.; Mesquita, E.T. C-Reactive Protein as a Prognostic Marker of 1-Year Mortality after Transcatheter Aortic Valve Implantation in Aortic Stenosis. Arq. Bras. Cardiol. 2021, 117, 1018–1027. [Google Scholar] [CrossRef]
- Ruparelia, N.; Panoulas, V.F.; Frame, A.; Ariff, B.; Sutaria, N.; Fertleman, M.; Cousins, J.; Anderson, J.; Bicknell, C.; Chukwuemeka, A.; et al. Impact of Clinical and Procedural Factors upon C Reactive Protein Dynamics Following Transcatheter Aortic Valve Implantation. World J. Cardiol. 2016, 8, 425–431. [Google Scholar] [CrossRef] [PubMed]
- Crawford, J.R.; Trial, J.; Nambi, V.; Hoogeveen, R.C.; Taffet, G.E.; Entman, M.L. Plasma Levels of Endothelial Microparticles Bearing Monomeric C-Reactive Protein Are Increased in Peripheral Artery Disease. J. Cardiovasc. Transl. Res. 2016, 9, 184–193. [Google Scholar] [CrossRef] [PubMed]
- Fukase, T.; Dohi, T.; Kato, Y.; Chikata, Y.; Takahashi, N.; Endo, H.; Doi, S.; Nishiyama, H.; Okai, I.; Iwata, H.; et al. Long-Term Impact of High-Sensitivity C-Reactive Protein in Patients with Intermittent Claudication Due to Peripheral Artery Disease Following Endovascular Treatment. Heart Vessel. 2021, 36, 1670–1678. [Google Scholar] [CrossRef] [PubMed]
- Dix, C.; Zeller, J.; Stevens, H.; Eisenhardt, S.U.; Shing, K.S.C.T.; Nero, T.L.; Morton, C.J.; Parker, M.W.; Peter, K.; McFadyen, J.D. C-Reactive Protein, Immunothrombosis and Venous Thromboembolism. Front. Immunol. 2022, 13, 1002652. [Google Scholar] [CrossRef] [PubMed]
- Lippi, G.; Favaloro, E.J.; Montagnana, M.; Franchini, M. C-Reactive Protein and Venous Thromboembolism: Causal or Casual Association? Clin. Chem. Lab. Med. 2010, 48, 1693–1701. [Google Scholar] [CrossRef]
- Chou, C.-Y.; Kuo, H.-L.; Yung, Y.-F.; Liu, Y.-L.; Huang, C.-C. C-Reactive Protein Predicts Vascular Access Thrombosis in Hemodialysis Patients. BPU 2006, 24, 342–346. [Google Scholar] [CrossRef]
- Kapur, R.; Heitink-Pollé, K.M.J.; Porcelijn, L.; Bentlage, A.E.H.; Bruin, M.C.A.; Visser, R.; Roos, D.; Schasfoort, R.B.M.; de Haas, M.; van der Schoot, C.E.; et al. C-Reactive Protein Enhances IgG-Mediated Phagocyte Responses and Thrombocytopenia. Blood 2015, 125, 1793–1802. [Google Scholar] [CrossRef]
- Kabutomori, O.; Kanakura, Y.; Iwatani, Y. Characteristic Changes in Platelet-Large Cell Ratio, Lactate Dehydrogenase and C-Reactive Protein in Thrombocytosis-Related Diseases. Acta Haematol. 2007, 118, 84–87. [Google Scholar] [CrossRef]
- Barbui, T.; Carobbio, A.; Finazzi, G.; Vannucchi, A.M.; Barosi, G.; Antonioli, E.; Guglielmelli, P.; Pancrazzi, A.; Salmoiraghi, S.; Zilio, P.; et al. Inflammation and Thrombosis in Essential Thrombocythemia and Polycythemia Vera: Different Role of C-Reactive Protein and Pentraxin 3. Haematologica 2011, 96, 315–318. [Google Scholar] [CrossRef]
- Sugiura, S.; Ito, T.; Koyama, N.; Sasaki, N.; Ikai, H.; Imanaka, Y. Asymptomatic C-Reactive Protein Elevation in Neutropenic Children. Pediatr. Int. 2017, 59, 23–28. [Google Scholar] [CrossRef] [PubMed]
- Hofman, Z.L.M.; Relan, A.; Hack, C.E. C-Reactive Protein Levels in Hereditary Angioedema. Clin. Exp. Immunol. 2014, 177, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Garijo, N.; Sabaté-Brescó, M.; Azofra, J.; Baeza, M.L.; Donado, C.D.; Gaig, P.; Guilarte, M.; Herrera-Lasso, V.; Labrador-Horrillo, M.; Sala-Cunill, A.; et al. Angioedema Severity and Impact on Quality of Life: Chronic Histaminergic Angioedema versus Chronic Spontaneous Urticaria. J. Allergy Clin. Immunol. Pract. 2022, 10, 3039–3043.e3. [Google Scholar] [CrossRef] [PubMed]
- Leurs, A.; Chenivesse, C.; Lopez, B.; Gibier, J.-B.; Clément, G.; Groh, M.; Copin, M.-C.; Staumont-Sallé, D.; Mortuaire, G.; Balquet, M.-H.; et al. C-Reactive Protein as a Diagnostic Tool in Differential Diagnosis of Hypereosinophilic Syndrome and Antineutrophil Cytoplasmic Antibody-Negative Eosinophilic Granulomatosis with Polyangiitis. J. Allergy Clin. Immunol. Pract. 2019, 7, 1347–1351.e3. [Google Scholar] [CrossRef]
- Bisaria, S.; Terrigno, V.; Hunter, K.; Roy, S. Association of Elevated Levels of Inflammatory Marker High-Sensitivity C-Reactive Protein and Hypertension. J. Prim. Care Community Health 2020, 11, 2150132720984426. [Google Scholar] [CrossRef]
- Shafi Dar, M.; Pandith, A.A.; Sameer, A.S.; Sultan, M.; Yousuf, A.; Mudassar, S. Hs-CRP: A Potential Marker for Hypertension in Kashmiri Population. Indian J. Clin. Biochem. 2010, 25, 208–212. [Google Scholar] [CrossRef]
- Kong, H.; Qian, Y.-S.; Tang, X.-F.; Zhang, J.; Gao, P.-J.; Zhang, Y.; Zhu, D.-L. C-Reactive Protein (CRP) Gene Polymorphisms, CRP Levels and Risk of Incident Essential Hypertension: Findings from an Observational Cohort of Han Chinese. Hypertens. Res. 2012, 35, 1019–1023. [Google Scholar] [CrossRef]
- Su, S.; Lampert, R.; Zhao, J.; Bremner, J.D.; Miller, A.; Snieder, H.; Lee, F.; Khan, D.; Goldberg, J.; Vaccarino, V. Pleiotropy of C-Reactive Protein Gene Polymorphisms with C-Reactive Protein Levels and Heart Rate Variability in Healthy Male Twins. Am. J. Cardiol. 2009, 104, 1748–1754. [Google Scholar] [CrossRef]
- Makis, A.C.; Hatzimichael, E.C.; Stebbing, J.; Bourantas, K.L. C-Reactive Protein and Vascular Cell Adhesion Molecule-1 as Markers of Severity in Sickle Cell Disease. Arch. Intern. Med. 2006, 166, 366–368. [Google Scholar] [CrossRef]
- Okocha, C.; Manafa, P.; Ozomba, J.; Ulasi, T.; Chukwuma, G.; Aneke, J. C-Reactive Protein and Disease Outcome in Nigerian Sickle Cell Disease Patients. Ann. Med. Health Sci. Res. 2014, 4, 701–705. [Google Scholar] [CrossRef]
- Kathamuthu, G.R.; Moideen, K.; Kumar, N.P.; Sridhar, R.; Baskaran, D.; Babu, S. Altered Systemic Levels of Acute Phase Proteins in Tuberculous Lymphadenitis and Modulation after Treatment. PLoS ONE 2020, 15, e0233426. [Google Scholar] [CrossRef] [PubMed]
- Gupta, V.; Gor, S.; Cheema, A.S.; Bajwa, R.; Edelman, C.; Wasserman, E.J. Histiocytic Necrotizing Lymphadenitis, a Benign Mimic of Lymphoma Presenting with B Symptoms. Blood 2018, 132, 4949. [Google Scholar] [CrossRef]
- Ali, H.A.; Zeriouh, B.; Bouzayan, L.; Jabi, R.; Bouziane, M. Giant Cystic Lymphangioma of the Stomach: A Case Report. Ann. Med. Surg. 2021, 61, 8–12. [Google Scholar] [CrossRef] [PubMed]
- Mabrouk, A.; Ennaceur, F.; Karoui, Y.; Ben Nejma, E.; Jedidi, L.; Ben Moussa, M. Giant Retroperitoneal Lymphangioma in a 70-Year-Old Male: A Case Report. Pan Afr. Med. J. 2022, 42, 153. [Google Scholar] [CrossRef]
- Elbouti, A.; Massad, I.; Touab, R.; Andaloussi, M.R.; Chouikh, C.; Balkhi, H. Haemorrhagic Shock Following Spontaneous Rupture of a Cystic Lymphangioma of the Spleen—Case Report. Austin J. Anesth. Analg. 2020, 8, 1082. [Google Scholar]
- Agassandian, M.; Shurin, G.V.; Ma, Y.; Shurin, M.R. C-Reactive Protein and Lung Diseases. Int. J. Biochem. Cell Biol. 2014, 53, 77–88. [Google Scholar] [CrossRef] [PubMed]
- Takemura, M.; Matsumoto, H.; Niimi, A.; Ueda, T.; Matsuoka, H.; Yamaguchi, M.; Jinnai, M.; Muro, S.; Hirai, T.; Ito, Y.; et al. High Sensitivity C-Reactive Protein in Asthma. Eur. Respir. J. 2006, 27, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Monadi, M.; Firouzjahi, A.; Hosseini, A.; Javadian, Y.; Sharbatdaran, M.; Heidari, B. Serum C-Reactive Protein in Asthma and Its Ability in Predicting Asthma Control, a Case-Control Study. Casp. J. Intern. Med. 2016, 7, 37–42. [Google Scholar]
- Posadas, T.; Oscullo, G.; Zaldivar, E.; Villa, C.; Dobarganes, Y.; Girón, R.; Olveira, C.; Maíz, L.; García-Clemente, M.; Sibila, O.; et al. C-Reactive Protein Concentration in Steady-State Bronchiectasis: Prognostic Value of Future Severe Exacerbations. Data from the Spanish Registry of Bronchiectasis (RIBRON). Arch. Bronconeumol. 2021, 57, 21–27. [Google Scholar] [CrossRef]
- Hsieh, M.-H.; Fang, Y.-F.; Chen, G.-Y.; Chung, F.-T.; Liu, Y.-C.; Wu, C.-H.; Chang, Y.-C.; Lin, H.-C. The Role of the High-Sensitivity C-Reactive Protein in Patients with Stable Non-Cystic Fibrosis Bronchiectasis. Pulm. Med. 2013, 2013, e795140. [Google Scholar] [CrossRef]
- Girón-Moreno, R.M.; Justicia, J.L.; Yamamoto, S.; Valenzuela, C.; Cisneros, C.; Gómez-Punter, R.M.; Fernandes-Vasconcelos, G.; Ancochea, J. Role of C-Reactive Protein as a Biomarker for Prediction of the Severity of Pulmonary Exacerbations in Patients with Cystic Fibrosis. BMC Pulm. Med. 2014, 14, 150. [Google Scholar] [CrossRef] [PubMed]
- Matouk, E.; Nguyen, D.; Benedetti, A.; Bernier, J.; Gruber, J.; Landry, J.; Rousseau, S.; Ahlgren, H.G.; Lands, L.C.; Wojewodka, G.; et al. C-Reactive Protein in Stable Cystic Fibrosis: An Additional Indicator of Clinical Disease Activity and Risk of Future Pulmonary Exacerbations. J. Pulm. Respir. Med. 2016, 6, 1000375. [Google Scholar] [CrossRef]
- Cetinoglu, E.D.; Dilektasli, A.G.; Uzaslan, E.; Coskun, F.; Ediger, D.; Ozkaya, G. Does CRP Predicts Severity of Hospitalized Patients with Diffuse Interstitial Lung Disease? Eur. Respir. J. 2014, 44, 3766. [Google Scholar]
- Liu, X.; Mayes, M.D.; Pedroza, C.; Draeger, H.T.; Gonzalez, E.B.; Harper, B.E.; Reveille, J.D.; Assassi, S. Does C-Reactive Protein Predict the Long-Term Progression of Interstitial Lung Disease and Survival in Patients with Early Systemic Sclerosis?: Predictive Significance of CRP for ILD Progression in SSc. Arthritis Care Res. 2013, 65, 1375–1380. [Google Scholar] [CrossRef] [PubMed]
- Fiedorczuk, P.; Polecka, A.; Walasek, M.; Olszewska, E. Potential Diagnostic and Monitoring Biomarkers of Obstructive Sleep Apnea–Umbrella Review of Meta-Analyses. J. Clin. Med. 2023, 12, 60. [Google Scholar] [CrossRef]
- Heseltine-Carp, W.; Dale, V.; Van Eck Van Der Sluijs, J.; Van Der Feltz-Cornelis, C. Are Serum hsCRP and IL-6 Prognostic Markers in Somatic Symptom Disorder and Related Disorders? An Exploratory Analysis in a Prospective Cohort Study. J. Psychiatr. Res. 2023, 157, 88–95. [Google Scholar] [CrossRef]
- Omori, H.; Tsuji, M.; Sata, K.; Iyonaga, C.; Narimatsu, A.; Mihara, S.; Marubayashi, T.; Tomiguchi, S.; Nomori, H.; Kohrogi, H.; et al. Correlation of C-Reactive Protein with Disease Severity in CT Diagnosed Emphysema. Respirology 2009, 14, 551–558. [Google Scholar] [CrossRef]
- Kony, S.; Zureik, M.; Driss, F.; Neukirch, C.; Leynaert, B.; Neukirch, F. Association of Bronchial Hyperresponsiveness and Lung Function with C-Reactive Protein (CRP): A Population Based Study. Thorax 2004, 59, 892–896. [Google Scholar] [CrossRef] [PubMed]
- Chihara, J.; Urayama, O.; Yasuba, H.; Fukuda, K.; Yamamoto, T.; Kurachi, D.; Nakajima, S. Possible Low Response of C-Reactive Protein Production in Eosinophilic Pneumonia. J. Clin. Lab. Immunol. 1995, 47, 33–39. [Google Scholar] [PubMed]
- Linssen, C.F.M.; Bekers, O.; Drent, M.; Jacobs, J.A. C-Reactive Protein and Procalcitonin Concentrations in Bronchoalveolar Lavage Fluid as a Predictor of Ventilator-Associated Pneumonia. Ann. Clin. Biochem. 2008, 45, 293–298. [Google Scholar] [CrossRef]
- Mukamal, K.J.; Pai, J.K.; O’Meara, E.S.; Tracy, R.P.; Psaty, B.M.; Kuller, L.H.; Newman, A.B.; Yende, S.; Curhan, G.C.; Siscovick, D.S.; et al. CRP Gene Variation and Risk of Community-Acquired Pneumonia. Respirology 2010, 15, 160–164. [Google Scholar] [CrossRef]
- Quarck, R.; Nawrot, T.; Meyns, B.; Delcroix, M. C-Reactive Protein: A New Predictor of Adverse Outcome in Pulmonary Arterial Hypertension. J. Am. Coll. Cardiol. 2009, 53, 1211–1218. [Google Scholar] [CrossRef]
- Yang, P.; Li, H.; Zhang, J.; Xu, X. Research Progress on Biomarkers of Pulmonary Embolism. Clin. Respir. J. 2021, 15, 1046–1055. [Google Scholar] [CrossRef] [PubMed]
- Bell, D.Y.; Hook, G.E. Pulmonary Alveolar Proteinosis: Analysis of Airway and Alveolar Proteins. Am. Rev. Respir. Dis. 1979, 119, 979–990. [Google Scholar] [PubMed]
- Garcia-Pachon, E.; Llorca, I. Diagnostic Value of C-Reactive Protein in Exudative Pleural Effusions. Eur. J. Intern. Med. 2002, 13, 246–249. [Google Scholar] [CrossRef]
- Kogan, Y.; Sabo, E.; Odeh, M. Diagnostic Value of C-Reactive Protein in Discrimination between Uncomplicated and Complicated Parapneumonic Effusion. Diagnostics 2020, 10, 829. [Google Scholar] [CrossRef] [PubMed]
- Vos, R.; Vanaudenaerde, B.M.; De Vleeschauwer, S.I.; Willems-Widyastuti, A.; Scheers, H.; Van Raemdonck, D.E.; Dupont, L.J.; Verleden, G.M. Circulating and Intrapulmonary C-Reactive Protein: A Predictor of Bronchiolitis Obliterans Syndrome and Pulmonary Allograft Outcome. J. Heart Lung Transpl. 2009, 28, 799–807. [Google Scholar] [CrossRef]
- Vos, R.; Vanaudenaerde, B.M.; De Vleeschauwer, S.I.; Van Raemdonck, D.E.; Dupont, L.J.; Verleden, G.M. Plasma C-Reactive Protein Levels Correlate with Markers of Airway Inflammation after Lung Transplantation: A Role for Systemic Inflammation in Bronchiolitis Obliterans Syndrome? Transplant. Proc. 2009, 41, 595–598. [Google Scholar] [CrossRef]
- Kana, M.; Kalfert, D.; Lukes, P.; Zabrodsky, M.; Plzak, J. C-Reactive Protein as an Early Marker of Postoperative Leakage in Patients after Endoscopic Laser Assisted Zenker’s Diverticulotomy. Eur. Arch. Otorhinolaryngol. 2022, 280, 2007–2016. [Google Scholar] [CrossRef]
- Seabrook, N.; Kedar, A.; Bills, G.; Sarker, S.; Rock, W.A.; Pinkston, C.; Kedar, A.; Abell, T. Inflammatory Markers and Mortality in Diabetic Versus Idiopathic Gastroparesis. Am. J. Med. Sci. 2022, 363, 218–223. [Google Scholar] [CrossRef]
- Hod, K.; Ringel-Kulka, T.; Martin, C.F.; Maharshak, N.; Ringel, Y. High-Sensitive C-Reactive Protein as a Marker for Inflammation in Irritable Bowel Syndrome. J. Clin. Gastroenterol. 2016, 50, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Mosli, M.H.; Zou, G.; Garg, S.K.; Feagan, S.G.; MacDonald, J.K.; Chande, N.; Sandborn, W.J.; Feagan, B.G. C-Reactive Protein, Fecal Calprotectin, and Stool Lactoferrin for Detection of Endoscopic Activity in Symptomatic Inflammatory Bowel Disease Patients: A Systematic Review and Meta-Analysis. Am. J. Gastroenterol. 2015, 110, 802–819, quiz 820. [Google Scholar] [CrossRef] [PubMed]
- Menees, S.B.; Powell, C.; Kurlander, J.; Goel, A.; Chey, W.D. A Meta-Analysis of the Utility of C-Reactive Protein, Erythrocyte Sedimentation Rate, Fecal Calprotectin, and Fecal Lactoferrin to Exclude Inflammatory Bowel Disease in Adults with IBS. Am. J. Gastroenterol. 2015, 110, 444–454. [Google Scholar] [CrossRef]
- Kimura, M.; Shimomura, M.; Morishita, H.; Meguro, T.; Seto, S. Serum C-Reactive Protein in Food Protein-Induced Enterocolitis Syndrome versus Food Protein-Induced Proctocolitis in Japan. Pediatr. Int. 2016, 58, 836–841. [Google Scholar] [CrossRef] [PubMed]
- Pimenta, D.; Yilmaz, D.; Grossman, R.; Soin, B. An Unusual Cause of Constipation in a 72-Year-Old Man with a Rising Creatinine. Case Rep. 2013, 2013, bcr2013010219. [Google Scholar] [CrossRef]
- Gavela, T.; Cabeza, B.; Serrano, A.; Casado-Flores, J. C-Reactive Protein and Procalcitonin Are Predictors of the Severity of Acute Appendicitis in Children. Pediatr. Emerg. Care 2012, 28, 416–419. [Google Scholar] [CrossRef] [PubMed]
- Ricaño-Ponce, I.; Peeters, T.; Matzaraki, V.; Houben, B.; Achten, R.; Cools, P.; Netea, M.G.; Gyssens, I.C.; Kumar, V. Impact of Human Genetic Variation on C-Reactive Protein Concentrations and Acute Appendicitis. Front. Immunol. 2022, 13, 862742. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Rodríguez, R.; Montero-Pérez, F.J.; García-Olid, A.; Baena-Delgado, E.; Gallardo-Valverde, J.M.; Calderón de la Barca-Gázquez, J.M.; Jiménez-Murillo, L.M. Value of plasma C-reactive protein and lactate dehydrogenase levels in the diagnosis of intestinal obstruction in an emergency department. An. Sist. Sanit. Navar. 2016, 39, 115–122. [Google Scholar] [CrossRef] [PubMed]
- Salem, T.; Molloy, R.; O’Dwyer, P. Prospective Study on the Role of C-Reactive Protein (CRP) in Patients with an Acute Abdomen. Annals 2007, 89, 233–237. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.H.; Park, J.M.; Lee, S.-W.; Kang, S.H.; Lim, C.-H.; Cho, Y.K.; Lee, B.-I.; Lee, I.S.; Kim, S.W.; Choi, M.-G. C-Reactive Protein as a Prognostic Indicator for Rebleeding in Patients with Nonvariceal Upper Gastrointestinal Bleeding. Dig. Liver Dis. 2015, 47, 378–383. [Google Scholar] [CrossRef] [PubMed]
- Yeung, D.E.; Peterknecht, E.; Hajibandeh, S.; Hajibandeh, S.; Torrance, A.W. C-Reactive Protein Can Predict Anastomotic Leak in Colorectal Surgery: A Systematic Review and Meta-Analysis. Int. J. Colorectal. Dis. 2021, 36, 1147–1162. [Google Scholar] [CrossRef]
- Kerner, A.; Avizohar, O.; Sella, R.; Bartha, P.; Zinder, O.; Markiewicz, W.; Levy, Y.; Brook, G.J.; Aronson, D. Association between Elevated Liver Enzymes and C-Reactive Protein: Possible Hepatic Contribution to Systemic Inflammation in the Metabolic Syndrome. ATVB 2005, 25, 193–197. [Google Scholar] [CrossRef] [PubMed]
- López-Sánchez, G.N.; Dóminguez-Pérez, M.; Uribe, M.; Nuño-Lámbarri, N. The Fibrogenic Process and the Unleashing of Acute-on-Chronic Liver Failure. Clin. Mol. Hepatol. 2020, 26, 7–15. [Google Scholar] [CrossRef]
- Targher, G. Relationship between High-Sensitivity C-Reactive Protein Levels and Liver Histology in Subjects with Non-Alcoholic Fatty Liver Disease. J. Hepatol. 2006, 45, 879–881. [Google Scholar] [CrossRef] [PubMed]
- Park, S.H.; Kim, B.I.; Yun, J.W.; Kim, J.W.; Park, D.I.; Cho, Y.K.; Sung, I.K.; Park, C.Y.; Sohn, C.I.; Jeon, W.K.; et al. Insulin Resistance and C-Reactive Protein as Independent Risk Factors for Non-Alcoholic Fatty Liver Disease in Non-Obese Asian Men. J. Gastroenterol. Hepatol. 2004, 19, 694–698. [Google Scholar] [CrossRef]
- Cotto, W.; Hinkle, H.; Abadie, M.; Nair, S. Is C Reactive Protein (CRP) a Useful Test in Distinguishing. Steatosis from Steatohepatitis in Patients with Non Alcoholic. Fatty Liver. Disease (NAFLD)?: 283. Off. J. Am. Coll. Gastroenterol. ACG 2005, 100, S116. [Google Scholar] [CrossRef]
- Uchihara, M.; Izumi, N. High-sensitivity C-reactive protein (hs-CRP): A promising biomarker for the screening of non-alcoholic steatohepatitis (NASH). Nihon Rinsho 2006, 64, 1133–1138. [Google Scholar]
- Yoneda, M.; Mawatari, H.; Fujita, K.; Iida, H.; Yonemitsu, K.; Kato, S.; Takahashi, H.; Kirikoshi, H.; Inamori, M.; Nozaki, Y.; et al. High-Sensitivity C-Reactive Protein Is an Independent Clinical Feature of Nonalcoholic Steatohepatitis (NASH) and Also of the Severity of Fibrosis in NASH. J. Gastroenterol. 2007, 42, 573–582. [Google Scholar] [CrossRef] [PubMed]
- Rahman, S.H.; Evans, J.; Toogood, G.J.; Lodge, P.A.; Prasad, K.R. Prognostic Utility of Postoperative C-Reactive Protein for Posthepatectomy Liver Failure. Arch. Surg. 2008, 143, 247–253, discussion 253. [Google Scholar] [CrossRef] [PubMed]
- Zhu, C.; Huang, D.; Ma, H.; Qian, C.; You, H.; Bu, L.; Qu, S. High-Sensitive CRP Correlates with the Severity of Liver Steatosis and Fibrosis in Obese Patients with Metabolic Dysfunction Associated Fatty Liver Disease. Front. Endocrinol. 2022, 13, 848937. [Google Scholar] [CrossRef]
- Huang, J.; Wang, M.; Wu, Y.; Kumar, R.; Lin, S. Serum High-Sensitive C-Reactive Protein Is a Simple Indicator for All-Cause among Individuals with MAFLD. Front. Physiol. 2022, 13, 1012887. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.-L.; Cheng, C.-C.; Chang, C.-C.; Mai, F.-D.; Wang, C.-C.; Lee, S.-C.; Ho, A.-S.; Chen, L.-Y.; Chang, J. Discovery of Serum Biomarkers of Alcoholic Fatty Liver in a Rodent Model: C-Reactive Protein. J. Biomed. Sci. 2011, 18, 52. [Google Scholar] [CrossRef] [PubMed]
- Vanbiervliet, G.; Le Breton, F.; Rosenthal-Allieri, M.-A.; Gelsi, E.; Marine-Barjoan, E.; Anty, R.; Piche, T.; Benzaken, S.; Saint-Paul, M.-C.; Huet, P.-M.; et al. Serum C-Reactive Protein: A Non-Invasive Marker of Alcoholic Hepatitis. Scand. J. Gastroenterol. 2006, 41, 1473–1479. [Google Scholar] [CrossRef]
- Abbas, W.A.K. Alpha-Fetoprotein and High Sensitive C-Reactive Protein Levels in Iraqi Patients with Liver Cirrhosis. J. Popul. Ther. Clin. Pharmacol. 2022, 29, e11–e16. [Google Scholar] [CrossRef]
- Turco, L.; Garcia-Tsao, G.; Magnani, I.; Bianchini, M.; Costetti, M.; Caporali, C.; Colopi, S.; Simonini, E.; De Maria, N.; Banchelli, F.; et al. Cardiopulmonary Hemodynamics and C-Reactive Protein as Prognostic Indicators in Compensated and Decompensated Cirrhosis. J. Hepatol. 2018, 68, 949–958. [Google Scholar] [CrossRef] [PubMed]
- Di Martino, V.; Coutris, C.; Cervoni, J.-P.; Dritsas, S.; Weil, D.; Richou, C.; Vanlemmens, C.; Thevenot, T. Prognostic Value of C-Reactive Protein Levels in Patients with Cirrhosis. Liver Transpl. 2015, 21, 753–760. [Google Scholar] [CrossRef]
- Ichikawa, T.; Machida, N.; Kaneko, H.; Oi, I.; A Fujino, M. C-Reactive Protein Can Predict Patients with Cirrhosis at a High Risk of Early Mortality after Acute Esophageal Variceal Bleeding. Intern. Med. 2019, 58, 487–495. [Google Scholar] [CrossRef]
- Padillo, F.J.; Muntane, J.; Montero, J.L.; Briceño, J.; Miño, G.; Solorzano, G.; Sitges-Serra, A.; Pera-Madrazo, C. Effect of Internal Biliary Drainage on Plasma Levels of Endotoxin, Cytokines, and C-Reactive Protein in Patients with Obstructive Jaundice. World J. Surg. 2002, 26, 1328–1332. [Google Scholar] [CrossRef]
- Liu, Q.; Dai, X.; Lou, S.; Huang, T.; Chen, J.; Chen, Z.; Yu, H.; Lan, X.; Cao, Z.; Zhou, Y.; et al. Evaluation of Procalcitonin and C-Reactive Protein in Early Differential Diagnosis of Neonatal Jaundice. Clin. Lab. 2020, 66, 2503–2510. [Google Scholar] [CrossRef]
- Labrune, P.; Benattar, C.; Ammoury, N.; Chalas, J.; Lindenbaum, A.; Odièvre, M. Serum Concentrations of Albumin, C-Reactive Protein, Alpha 2-Macroglobulin, Prealbumin, Fibronectin, Fibrinogen, Transferrin, and Retinol Binding Protein in 55 Patients with Hepatic Glycogen Storage Diseases. J. Pediatr. Gastroenterol. Nutr. 1994, 18, 41–44. [Google Scholar] [CrossRef]
- Gertz, M.A.; Skinner, M.; Sipe, J.D.; Cohen, A.S.; Kyle, R.A. Serum Amyloid A Protein and C-Reactive Protein in Systemic Amyloidosis. Clin. Exp. Rheumatol. 1985, 3, 317–320. [Google Scholar] [PubMed]
- Liu, T.; Siyin, S.T.; Yao, N.; Duan, N.; Xu, G.; Li, W.; Qu, J.; Liu, S. Relationship between High-Sensitivity C Reactive Protein and the Risk of Gallstone Disease: Results from the Kailuan Cohort Study. BMJ Open 2020, 10, e035880. [Google Scholar] [CrossRef] [PubMed]
- Mok, K.W.J.; Reddy, R.; Wood, F.; Turner, P.; Ward, J.B.; Pursnani, K.G.; Date, R.S. Is C-Reactive Protein a Useful Adjunct in Selecting Patients for Emergency Cholecystectomy by Predicting Severe/Gangrenous Cholecystitis? Int. J. Surg. 2014, 12, 649–653. [Google Scholar] [CrossRef] [PubMed]
- Real-Noval, H.; Fernández-Fernández, J.; Soler-Dorda, G. Predicting Factors for the Diagnosis of Gangrene Acute Cholecystitis. Cir. Cir. 2019, 87, 443–449. [Google Scholar] [CrossRef]
- Gregory, G.C.; Kuzman, M.; Sivaraj, J.; Navarro, A.P.; Cameron, I.C.; Irving, G.; Gomez, D. C-Reactive Protein Is an Independent Predictor of Difficult Emergency Cholecystectomy. Cureus 2019, 11, e4573. [Google Scholar] [CrossRef]
- Rajab, I.M.; Majerczyk, D.; Olson, M.E.; Addams, J.M.B.; Choe, M.L.; Nelson, M.S.; Potempa, L.A. C-Reactive Protein in Gallbladder Diseases: Diagnostic and Therapeutic Insights. Biophys. Rep. 2020, 6, 49–67. [Google Scholar] [CrossRef]
- Jakubauskas, M.; Luksaite, R.; Sileikis, A.; Strupas, K.; Poskus, T. Gallstone Ileus: Management and Clinical Outcomes. Medicina 2019, 55, 598. [Google Scholar] [CrossRef]
- Wagner, K.-H.; Khoei, N.S.; Hana, C.A.; Doberer, D.; Marculescu, R.; Bulmer, A.C.; Hörmann-Wallner, M.; Mölzer, C. Oxidative Stress and Related Biomarkers in Gilbert’s Syndrome: A Secondary Analysis of Two Case-Control Studies. Antioxidants 2021, 10, 1474. [Google Scholar] [CrossRef]
- Cure, M.C.; Cure, E.; Kirbas, A.; Cicek, A.C.; Yuce, S. The Effects of Gilbert’s Syndrome on the Mean Platelet Volume and Other Hematological Parameters. Blood Coagul. Fibrinolysis 2013, 24, 484–488. [Google Scholar] [CrossRef]
- Wallner, M.; Bulmer, A.C.; Mölzer, C.; Müllner, E.; Marculescu, R.; Doberer, D.; Wolzt, M.; Wagner, O.F.; Wagner, K.-H. Haem Catabolism: A Novel Modulator of Inflammation in Gilbert’s Syndrome. Eur. J. Clin. Investig. 2013, 43, 912–919. [Google Scholar] [CrossRef]
- Mazidi, M.; Toth, P.P.; Banach, M. C-Reactive Protein Is Associated with Prevalence of the Metabolic Syndrome, Hypertension, and Diabetes Mellitus in US Adults. Angiology 2018, 69, 438–442. [Google Scholar] [CrossRef]
- Powe, C.E. Early Pregnancy Biochemical Predictors of Gestational Diabetes Mellitus. Curr. Diab. Rep. 2017, 17, 12. [Google Scholar] [CrossRef]
- Dorcely, B.; Katz, K.; Jagannathan, R.; Chiang, S.S.; Oluwadare, B.; Goldberg, I.J.; Bergman, M. Novel Biomarkers for Prediabetes, Diabetes, and Associated Complications. Diabetes Metabolic Syndr. Obes. 2017, 10, 345–361. [Google Scholar] [CrossRef]
- Li, J.; Chen, Z.; Li, L.; Lai, T.; Peng, H.; Gui, L.; He, W. Interleukin-6 Is Better than C-Reactive Protein for the Prediction of Infected Pancreatic Necrosis and Mortality in Patients with Acute Pancreatitis. Front. Cell. Infect. Microbiol. 2022, 12, 933221. [Google Scholar] [CrossRef] [PubMed]
- Dancu, G.M.; Popescu, A.; Sirli, R.; Danila, M.; Bende, F.; Tarta, C.; Sporea, I. The BISAP Score, NLR, CRP, or BUN: Which Marker Best Predicts the Outcome of Acute Pancreatitis? Medicine 2021, 100, e28121. [Google Scholar] [CrossRef]
- Hontsariuk, D.O.; Ferfetska, K.V.; Khrystych, T.M.; Fediv, O.I.; Temerivska, T.G.; Jiguleva, E.O.; Honcharuk, L.M.; Olinik, O.Y. Incides of C-Reactive Protein, Tumor Necrosis Factor-α, Adiponectin, Leptin and Resistin in the Blood of Patients Suffering from Chronic Pancreatitis and Type 2 Diabetes Mellitus. J. Med. Life 2020, 13, 568–571. [Google Scholar] [CrossRef] [PubMed]
- Hebanowska, A.; Mika, A.; Rojek, L.; Stojek, M.; Goyke, E.; Swierczynski, J.; Sledzinski, T.; Adrych, K. Serum N-3 Polyunsaturated Fatty Acids and C-Reactive Protein Concentrations Are Inversely Associated in Patients with Alcoholic Chronic Pancreatitis. Pancreas 2022, 51, e67–e69. [Google Scholar] [CrossRef]
- Guilbaud, T.; Birnbaum, D.J.; Lemoine, C.; Chirica, M.; Risse, O.; Berdah, S.; Girard, E.; Moutardier, V. C-Reactive Protein on Postoperative Day 1 Is a Reliable Predictor of Pancreas-Specific Complications After Pancreaticoduodenectomy. J. Gastrointest. Surg. 2018, 22, 818–830. [Google Scholar] [CrossRef] [PubMed]
- Tang, Y.; Mak, S.-K.; Xu, A.P.; Lan, H.-Y. Role of C-Reactive Protein in the Pathogenesis of Acute Kidney Injury: CRP in AKI. Nephrology 2018, 23, 50–52. [Google Scholar] [CrossRef]
- Yang, T.; Chou, Y.-C.; Chu, C.-H.; Lin, S.-H.; Hsieh, P.-C.; Hsu, C.-H.; Bai, C.-H.; You, S.-L.; Sun, C.-A. Metabolic Syndrome and C-Reactive Protein Concentration as Independent Correlates of Chronic Kidney Disease. Endocr. Res. 2014, 39, 94–98. [Google Scholar] [CrossRef] [PubMed]
- Panichi, V.; Migliori, M.; De Pietro, S.; Taccola, D.; Bianchi, A.M.; Giovannini, L.; Norpoth, M.; Metelli, M.R.; Cristofani, R.; Bertelli, A.A.E.; et al. C-Reactive Protein and Interleukin-6 Levels Are Related to Renal Function in Predialytic Chronic Renal Failure. Nephron 2002, 91, 594–600. [Google Scholar] [CrossRef] [PubMed]
- Uludag, K.; Boz, G.; Arikan, T.; Gunal, A.I. Temporal Evolution of C-Reactive Protein Levels and Its Association with the Incident Hospitalization Risk among Individuals with Stage 3–4 Chronic Kidney Disease. Int. Urol. Nephrol. 2022, 54, 609–617. [Google Scholar] [CrossRef] [PubMed]
- Lee, C.; Park, K.H.; Joo, Y.S.; Nam, K.H.; Chang, T.-I.; Kang, E.W.; Lee, J.; Oh, Y.K.; Jung, J.Y.; Ahn, C.; et al. Low High-Sensitivity C-Reactive Protein Level in Korean Patients with Chronic Kidney Disease and Its Predictive Significance for Cardiovascular Events, Mortality, and Adverse Kidney Outcomes: Results from KNOW-CKD. J. Am. Heart Assoc. 2020, 9, e017980. [Google Scholar] [CrossRef] [PubMed]
- Stuveling, E.M.; Hillege, H.L.; Bakker, S.J.L.; Gans, R.O.B.; De Jong, P.E.; De Zeeuw, D. C-Reactive Protein Is Associated with Renal Function Abnormalities in a Non-Diabetic Population. Kidney Int. 2003, 63, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Nakahara, C.; Kanemoto, K.; Saito, N.; Oyake, Y.; Kamoda, T.; Nagata, M.; Matsui, A. C-Reactive Protein Frequently Localizes in the Kidney in Glomerular Diseases. Clin. Nephrol. 2001, 55, 365–370. [Google Scholar]
- Shostak, E.; Krause, I.; Dagan, A.; Ben-Dor, A.; Keidar, M.; Davidovits, M. Is Serum CRP Level a Reliable Inflammatory Marker in Pediatric Nephrotic Syndrome? Pediatr. Nephrol. 2016, 31, 1287–1293. [Google Scholar] [CrossRef]
- Wasilewska, A.; Zoch-Zwierz, W.; Tobolczyk, J.; Tenderenda, E. High-Sensitivity C-Reactive Protein (Hs-CRP) Level in Children with Nephrotic Syndrome. Pediatr. Nephrol. 2007, 22, 403–408. [Google Scholar] [CrossRef]
- Ma, L.; Zhao, S. Risk Factors for Mortality in Patients Undergoing Hemodialysis: A Systematic Review and Meta-Analysis. Int. J. Cardiol. 2017, 238, 151–158. [Google Scholar] [CrossRef]
- Cobo, G.; Qureshi, A.R.; Lindholm, B.; Stenvinkel, P. C-Reactive Protein: Repeated Measurements Will Improve Dialysis Patient Care. Semin. Dial. 2016, 29, 7–14. [Google Scholar] [CrossRef]
- Oualha, M.; Pierrepont, S.; Krug, P.; Gitiaux, C.; Hubert, P.; Lesage, F.; Salomon, R. Postdiarrheal Hemolytic and Uremic Syndrome with Severe Multiorgan Involvement and Associated Early Risk Factors. Arch. Pediatr. 2018, 25, 118–125. [Google Scholar] [CrossRef] [PubMed]
- Stirbu, O.; Gadalean, F.; Pitea, I.V.; Ciobanu, G.; Schiller, A.; Grosu, I.; Nes, A.; Bratescu, R.; Olariu, N.; Timar, B.; et al. C-Reactive Protein as a Prognostic Risk Factor for Loss of Arteriovenous Fistula Patency in Hemodialyzed Patients. J. Vasc. Surg. 2019, 70, 208–215. [Google Scholar] [CrossRef]
- Fine, A. Relevance of C-Reactive Protein Levels in Peritoneal Dialysis Patients. Kidney Int. 2002, 61, 615–620. [Google Scholar] [CrossRef] [PubMed]
- Morath, C.; Sis, J.; Haensch, G.M.; Zeier, M.; Andrassy, K.; Schwenger, V. Procalcitonin as Marker of Infection in Patients with Goodpasture’s Syndrome Is Misleading. Nephrol. Dial. Transpl. 2007, 22, 2701–2704. [Google Scholar] [CrossRef] [PubMed]
- Bourgault, M.; Grimbert, P.; Verret, C.; Pourrat, J.; Herody, M.; Halimi, J.M.; Karras, A.; Amoura, Z.; Jourde-Chiche, N.; Izzedine, H.; et al. Acute Renal Infarction: A Case Series. Clin. J. Am. Soc. Nephrol. 2013, 8, 392. [Google Scholar] [CrossRef] [PubMed]
- Li, J.-J.; Fang, C.-H.; Jiang, H.; Hunag, C.-X.; Tang, Q.-Z.; Wang, X.-H.; Li, G.-S. Increased C-Reactive Protein Level after Renal Stent Implantation in Patients with Atherosclerotic Renal Stenosis. Angiology 2004, 55, 479–484. [Google Scholar] [CrossRef] [PubMed]
- Evévquoz, D.; Rosman, J.; Reichenstein, T.; Garzoni, D.; Rohrer, W.; Thiel, G. C-reactive protein and early diagnosis of kidney transplant rejection. Schweiz. Med. Wochenschr. 1993, 123, 1837–1842. [Google Scholar] [PubMed]
- Ruleva, N.Y.; Lyukova, T.K.; Tarabarko, N.V.; Komolov, I.S.; Domogatskii, S.P. Structure of C-Reactive Protein Excreted in Urine during Acute Rejection Episodes. Bull. Exp. Biol. Med. 2003, 135, 250–252. [Google Scholar] [CrossRef]
- Angulo, J.C.; Gaspar, M.J.; Rodríguez, N.; García-Tello, A.; Torres, G.; Núñez, C. The Value of C-Reactive Protein Determination in Patients with Renal Colic to Decide Urgent Urinary Diversion. Urology 2010, 76, 301–306. [Google Scholar] [CrossRef] [PubMed]
- Shoag, J.; Eisner, B.H. Relationship between C-Reactive Protein and Kidney Stone Prevalence. J. Urol. 2014, 191, 372–375. [Google Scholar] [CrossRef]
- Mohammad, E.J.; Abbas, K.M.; Hassan, A.F.; Abdulrazaq, A.A. Serum C-Reactive Protein as a Predictive Factor for Spontaneous Stone Passage in Patients with 4 to 8 Mm Distal Ureteral Stones. Int. Surg. J. 2018, 5, 1195–1200. [Google Scholar] [CrossRef]
- Guzel, O.; Aslan, Y.; Tuncel, A.; Senel, C.; Asfuroglu, A.; Oguz, E.F.; Yilmaz, F.M.; Balci, M. Diagnostic Role of Urine C-Reactive Protein Levels on Ureteral Stone Disease. Insight Urol. 2018, 39, 35–41. [Google Scholar]
- Chung, S.-D.; Liu, H.-T.; Lin, H.; Kuo, H.-C. Elevation of Serum C-Reactive Protein in Patients with OAB and IC/BPS Implies Chronic Inflammation in the Urinary Bladder. Neurourol. Urodyn. 2011, 30, 417–420. [Google Scholar] [CrossRef]
- Ganesan, V.; Brown, R.D.; Jiménez, J.A.; De, S.; Monga, M. C-Reactive Protein and Erythrocyte Sedimentation Rate Predict Systemic Inflammatory Response Syndrome After Percutaneous Nephrolithotomy. J. Endourol. 2017, 31, 638–644. [Google Scholar] [CrossRef]
- Gleason, J.L.; Thoma, M.E.; Zukerman Willinger, N.; Shenassa, E.D. Endometriosis and Uterine Fibroids and Their Associations with Elevated C-Reactive Protein and Leukocyte Telomere Length Among a Representative Sample of U.S. Women: Data from the National Health and Nutrition Examination Survey, 1999–2002. J. Womens Health 2022, 31, 1020–1028. [Google Scholar] [CrossRef]
- Sevostyanova, O.; Lisovskaya, T.; Chistyakova, G.; Kiseleva, M.; Sevostyanova, N.; Remizova, I.; Buev, Y. Proinflammatory Mediators and Reproductive Failure in Women with Uterine Fibroids. Gynecol. Endocrinol. 2020, 36, 33–35. [Google Scholar] [CrossRef]
- Souftas, V.; Deuteraiou, D.; Anthoulaki, X.; Chalkidou, A.; Bothou, A.; Gaidatzi, F.; Tsypsianis, G.; Iatrakis, G.; Zervoudis, S.; Souftas, D.; et al. Significance of Changes in Inflammatory Parameters Following Uterine Artery Embolization in Pre-menopausal Females. Exp. Ther. Med. 2020, 19, 3684–3690. [Google Scholar] [CrossRef] [PubMed]
- Genius, J.; Dong-Si, T.; Grau, A.P.; Lichy, C. Postacute C-Reactive Protein Levels Are Elevated in Cervical Artery Dissection. Stroke 2005, 36, e42–e44. [Google Scholar] [CrossRef]
- Taponen, S.; Martikainen, H.; Järvelin, M.-R.; Sovio, U.; Laitinen, J.; Pouta, A.; Hartikainen, A.-L.; McCarthy, M.I.; Franks, S.; Paldanius, M.; et al. Metabolic Cardiovascular Disease Risk Factors in Women with Self-Reported Symptoms of Oligomenorrhea and/or Hirsutism: Northern Finland Birth Cohort 1966 Study. J. Clin. Endocrinol. Metab. 2004, 89, 2114–2118. [Google Scholar] [CrossRef] [PubMed]
- Boulman, N.; Levy, Y.; Leiba, R.; Shachar, S.; Linn, R.; Zinder, O.; Blumenfeld, Z. Increased C-Reactive Protein Levels in the Polycystic Ovary Syndrome: A Marker of Cardiovascular Disease. J. Clin. Endocrinol. Metab. 2004, 89, 2160–2165. [Google Scholar] [CrossRef]
- Oh, J.Y.; Lee, J.-A.; Lee, H.; Oh, J.-Y.; Sung, Y.-A.; Chung, H. Serum C-Reactive Protein Levels in Normal-Weight Polycystic Ovary Syndrome. Korean J. Intern. Med. 2009, 24, 350–355. [Google Scholar] [CrossRef] [PubMed]
- Mucuk, S.; Yılmaz, M.; Onur, A. Relationship between Dysmenorrhea, Dietary Inflammatory Index, and C-Reactive Protein Level. Prog. Nutr. 2022, 23, e2021156. [Google Scholar] [CrossRef]
- Olasore, H.S.A.; Oyedeji, T.A.; Adebisi, A.A.; James, A.B.; Akinwunmi, D.; Ayoade, B.O.; Olayanju, S.A.; Uchefe, E.E.; Babalola, A.R. Plasma C-Reactive Protein, Prostaglandin-F2? Metabolite and 8-Isoprostane Were Elevated in Women with Dysmenorrhe. Med. Sci. 2022, 8. [Google Scholar]
- Merino, P.M.; Martínez, D.; Iñiguez, G.; Lopez, P.; Cassorla, F.; Perez-Bravo, F.; Codner, E. Elevation of C-Reactive Protein during the Luteal Phase in Healthy Adolescents. Gynecol. Endocrinol. 2015, 31, 260–263. [Google Scholar] [CrossRef] [PubMed]
- Gursoy, A.Y.; Caglar, G.S.; Kiseli, M.; Pabuccu, E.; Candar, T.; Demirtas, S. CRP at Early Follicular Phase of Menstrual Cycle Can Cause Misinterpretation for Cardiovascular Risk Assessment. Interv. Med. Appl. Sci. 2015, 7, 143–146. [Google Scholar] [CrossRef]
- Vashishta, S.; Gahlot, S.; Singh, A.; Goyal, R. Impact of Menstrual Cycle Phases on C-Reactive Protein Concentrations. Int. J. Res. Med. Sci. 2017, 5, 1090–1094. [Google Scholar] [CrossRef]
- Harris, B.S.; Steiner, A.Z.; Jukic, A.M.Z. Association between chronic inflammation and menstrual cycle length. Fertil. Steril. 2021, 116, e315–e316. [Google Scholar] [CrossRef]
- Wander, K.; Brindle, E.; O’Connor, K.A. C-Reactive Protein across the Menstrual Cycle. Am. J. Phys. Anthr. 2008, 136, 138–146. [Google Scholar] [CrossRef] [PubMed]
- Gold, E.B.; Wells, C.; Rasor, M.O. The Association of Inflammation with Premenstrual Symptoms. J. Womens Health 2016, 25, 865–874. [Google Scholar] [CrossRef] [PubMed]
- Nowicka, M.A.; Fritz-Rdzanek, A.; Grzybowski, W.; Walecka, I.; Niemiec, K.T.; Jakimiuk, A.J. C-Reactive Protein as the Indicator of Severity in Ovarian Hyperstimulation Syndrome. Gynecol. Endocrinol. 2010, 26, 399–403. [Google Scholar] [CrossRef]
- Sacks, G.P.; Seyani, L.; Lavery, S.; Trew, G. Maternal C-reactive protein levels are raised at 4 weeks gestation. Hum. Reprod. 2004, 19, 1025–1030. [Google Scholar] [CrossRef]
- Vecchié, A.; Bonaventura, A.; Carbone, F.; Maggi, D.; Ferraiolo, A.; Carloni, B.; Andraghetti, G.; Affinito Bonabello, L.; Liberale, L.; Dallegri, F.; et al. C-Reactive Protein Levels at the Midpregnancy Can Predict Gestational Complications. Biomed. Res. Int. 2018, 2018, 1070151. [Google Scholar] [CrossRef] [PubMed]
- Vanky, E.; Salvesen, K.A.; Asberg, A.; Carlsen, S.M. Haemoglobin, C-Reactive Protein and Androgen Levels in Uncomplicated and Complicated Pregnancies of Women with Polycystic Ovary Syndrome. Scand. J. Clin. Lab. Investig. 2008, 68, 421–426. [Google Scholar] [CrossRef] [PubMed]
- Boggess, K.A.; Lieff, S.; Murtha, A.P.; Moss, K.; Jared, H.; Beck, J.; Offenbacher, S. Maternal Serum C-Reactive Protein Concentration Early in Pregnancy and Subsequent Pregnancy Loss. Am. J. Perinatol. 2005, 22, 299–304. [Google Scholar] [CrossRef]
- Ahmed, S.K.; Mahmood, N.; Malalla, Z.H.; Alsobyani, F.M.; Al-Kiyumi, I.S.; Almawi, W.Y. C-Reactive Protein Gene Variants Associated with Recurrent Pregnancy Loss Independent of CRP Serum Levels: A Case-Control Study. Gene 2015, 569, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Pils, S.; Paternostro, C.; Bekos, C.; Hager, M.; Ristl, R.; Ott, J. Prognostic Laboratory Parameters in Placental Abruption: A Retrospective Case-Control Study. J. Clin. Med. 2019, 8, 482. [Google Scholar] [CrossRef] [PubMed]
- Institute for Mother and Child Care, Prague, Czech Republic; Straňák, Z.; Berka, I.; Širc, J.; Urbánek, J.; Feyereisl, J.; Korček, P. Role of Umbilical Interleukin-6, Procalcitonin and C-Reactive Protein Measurement in the Dia Gnosis of Fetal Inflammatory Response Syndrome. Ceska Gynekol. 2021, 86, 80–85. [Google Scholar] [CrossRef]
- Stepan, M.; Cobo, T.; Musilova, I.; Hornychova, H.; Jacobsson, B.; Kacerovsky, M. Maternal Serum C-Reactive Protein in Women with Preterm Prelabor Rupture of Membranes. PLoS ONE 2016, 11, e0150217. [Google Scholar] [CrossRef] [PubMed]
- Suryavanshi, A.; Kalra, R. Study of Association of C-Reactive Protein with Maternal Chorioamnionitis and Early-Onset Neonatal Sepsis in Premature Rupture of Membranes Deliveries: A Diagnostic Dilemma. Int. J. Appl. Basic Med. Res. 2019, 9, 236–240. [Google Scholar] [CrossRef] [PubMed]
- Asadi, N.; Faraji, A.; Keshavarzi, A.; Akbarzadeh-Jahromi, M.; Yoosefi, S. Predictive Value of Procalcitonin, C-Reactive Protein, and White Blood Cells for Chorioamnionitis among Women with Preterm Premature Rupture of Membranes. Int. J. Gynaecol. Obs. 2019, 147, 83–88. [Google Scholar] [CrossRef]
- Trochez-Martinez, R.D.; Smith, P.; Lamont, R.F. Use of C-Reactive Protein as a Predictor of Chorioamnionitis in Preterm Prelabour Rupture of Membranes: A Systematic Review. BJOG 2007, 114, 796–801. [Google Scholar] [CrossRef]
- Shim, S.-S.; Romero, R.; Jun, J.K.; Moon, K.C.; Kim, G.; Yoon, B.H. C-Reactive Protein Concentration in Vaginal Fluid as a Marker for Intra-Amniotic Inflammation/Infection in Preterm Premature Rupture of Membranes. J. Matern. Fetal Neonatal Med. 2005, 18, 417–422. [Google Scholar] [CrossRef]
- Huang, S.; Tian, J.; Liu, C.; Long, Y.; Cao, D.; Wei, L.; Zhu, X.; Tang, R.; Liu, W.; Zeng, D.; et al. Elevated C-Reactive Protein and Complement C3 Levels Are Associated with Preterm Birth: A Nested Case-Control Study in Chinese Women. BMC Pregnancy Childbirth 2020, 20, 131. [Google Scholar] [CrossRef] [PubMed]
- Ghezzi, F.; Franchi, M.; Raio, L.; Di Naro, E.; Bossi, G.; D’Eril, G.V.M.; Bolis, P. Elevated Amniotic Fluid C-Reactive Protein at the Time of Genetic Amniocentesis Is a Marker for Preterm Delivery. Am. J. Obstet. Gynecol. 2002, 186, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, M.; Ohkuchi, A.; Matsubara, S.; Izumi, A.; Hirashima, C.; Suzuki, M. C-Reactive Protein Levels at Pre-/Post-Indicated Cervical Cerclage Predict Very Preterm Birth. J. Perinat. Med. 2011, 39, 151–155. [Google Scholar] [CrossRef] [PubMed]
- Najat Nakishbandy, B.M.; Barawi, S.A.M. Level of C-Reactive Protein as an Indicator for Prognosis of Premature Uterine Contractions. J. Prenat. Med. 2014, 8, 25–30. [Google Scholar] [PubMed]
- Osoti, A.O.; Page, S.T.; Richardson, B.A.; Guthrie, B.L.; Kinuthia, J.; Polyak, S.J.; Farquhar, C. Postpartum Metabolic Syndrome and High-Sensitivity C-Reactive Protein after Gestational Hypertension and Pre-Eclampsia. Int. J. Gynaecol. Obstet. 2020, 151, 443–449. [Google Scholar] [CrossRef]
- Vallejo Vaz, A.J.; Guisado, M.L.M.; García-Junco, P.S.; Andreu, E.P.; Morillo, S.G.; Ortiz, J.V. Differences in the Prevalence of Metabolic Syndrome and Levels of C-Reactive Protein after Puerperium in Women with Hypertensive Disorders during Pregnancy. Hypertens. Res. 2010, 33, 1012–1017. [Google Scholar] [CrossRef]
- Johnstone, A.M.; Pudwell, J.; Ackerman-Banks, C.M.; Lundsberg, L.S.; Lipkind, H.S.; Smith, G.N. High-Sensitivity C-Reactive Protein Use in Cardiovascular Risk Screening at 6 to 12 Months Postpartum Following Hypertensive Disorders of Pregnancy. Am. J. Obstet. Gynecol. MFM 2023, 5, 100776. [Google Scholar] [CrossRef]
- Raio, L.; Bersinger, N.A.; Malek, A.; Schneider, H.; Messerli, F.H.; Hürter, H.; Rimoldi, S.F.; Baumann, M.U. Ultra-High Sensitive C-Reactive Protein during Normal Pregnancy and in Preeclampsia: A Pilot Study. J. Hypertens. 2019, 37, 1012–1017. [Google Scholar] [CrossRef] [PubMed]
- Serrano, N.C.; Guio, E.; Becerra-Bayona, S.M.; Quintero-Lesmes, D.C.; Bautista-Niño, P.K.; Colmenares-Mejía, C.; Páez, M.C.; Luna, M.L.; Díaz, L.A.; Ortiz, R.; et al. C-Reactive Protein, Interleukin-6 and Pre-Eclampsia: Large-Scale Evidence from the GenPE Case-Control Study. Scand. J. Clin. Lab. Investig. 2020, 80, 381–387. [Google Scholar] [CrossRef] [PubMed]
- Gammill, H.S.; Powers, R.W.; Clifton, R.G.; Van Dorsten, J.P.; Klebanoff, M.A.; Lindheimer, M.D.; Sibai, B.; Landon, M.B.; Miodovnik, M.; Dombrowski, M.; et al. Does C-Reactive Protein Predict Recurrent Preeclampsia? Hypertens. Pregnancy 2010, 29, 399–409. [Google Scholar] [CrossRef] [PubMed]
- Rebelo, F.; Schlüssel, M.M.; Vaz, J.S.; Franco-Sena, A.B.; Pinto, T.J.P.; Bastos, F.I.; Adegboye, A.R.A.; Kac, G. C-Reactive Protein and Later Preeclampsia: Systematic Review and Meta-Analysis Taking into Account the Weight Status. J. Hypertens. 2013, 31, 16–26. [Google Scholar] [CrossRef] [PubMed]
- Park, H. Association between Oral Contraceptive Use and the High-Sensitivity C-Reactive Protein Level in Premenopausal Korean Women. Healthcare 2022, 10, 361. [Google Scholar] [CrossRef] [PubMed]
- Cauci, S.; Francescato, M.P.; Curcio, F. Combined Oral Contraceptives Increase High-Sensitivity C-Reactive Protein but Not Haptoglobin in Female Athletes. Sports Med. 2017, 47, 175–185. [Google Scholar] [CrossRef]
- Nazmi, A.; Oliveira, I.O.; Victora, C.G. Correlates of C-Reactive Protein Levels in Young Adults: A Population-Based Cohort Study of 3827 Subjects in Brazil. Braz. J. Med. Biol. Res. 2008, 41, 357–367. [Google Scholar] [CrossRef] [PubMed]
- Connell, E.B.; Connell, J.T. C-Reactive Protein in Pregnancy and Contraception. Am. J. Obstet. Gynecol. 1971, 110, 633–639. [Google Scholar] [CrossRef]
- Ellström, M.; Bengtsson, A.; Tylman, M.; Haeger, M.; Olsson, J.H.; Hahlin, M. Evaluation of Tissue Trauma after Laparoscopic and Abdominal Hysterectomy: Measurements of Neutrophil Activation and Release of Interleukin-6, Cortisol, and C-Reactive Protein. J. Am. Coll. Surg. 1996, 182, 423–430. [Google Scholar]
- Labib, M.; Palfrey, S.; Paniagua, E.; Callender, R. The Postoperative Inflammatory Response to Injury Following Laparoscopic Assisted Vaginal Hysterectomy versus Abdominal Hysterectomy. Ann. Clin. Biochem. 1997, 34 Pt 5, 543–545. [Google Scholar] [CrossRef]
- Yuen, P.M.; Mak, T.W.; Yim, S.F.; Ngan Kee, W.D.; Lam, C.W.; Rogers, M.S.; Chang, A.M. Metabolic and Inflammatory Responses after Laparoscopic and Abdominal Hysterectomy. Am. J. Obstet. Gynecol. 1998, 179, 1–5. [Google Scholar] [CrossRef]
- Atabekoglu, C.; Sönmezer, M.; Güngör, M.; Aytaç, R.; Ortaç, F.; Ünlü, C. Tissue Trauma in Abdominal and Laparoscopic-Assisted Vaginal Hysterectomy. J. Am. Assoc. Gynecol. Laparosc. 2004, 11, 467–472. [Google Scholar] [CrossRef]
- Perrone, S.; Lotti, F.; Longini, M.; Rossetti, A.; Bindi, I.; Bazzini, F.; Belvisi, E.; Sarnacchiaro, P.; Scapellato, C.; Buonocore, G. C Reactive Protein in Healthy Term Newborns during the First 48 Hours of Life. Arch. Dis. Child. Fetal Neonatal Ed. 2018, 103, F163–F166. [Google Scholar] [CrossRef] [PubMed]
- Mjelle, A.B.; Guthe, H.J.T.; Reigstad, H.; Bjørke-Monsen, A.L.; Markestad, T. Serum Concentrations of C-Reactive Protein in Healthy Term-Born Norwegian Infants 48–72 Hours after Birth. Acta Paediatr. 2019, 108, 849–854. [Google Scholar] [CrossRef]
- Whitaker, K.M.; Marino, R.C.; Haapala, J.L.; Foster, L.; Smith, K.D.; Teague, A.M.; Jacobs, D.R.; Fontaine, P.L.; McGovern, P.M.; Schoenfuss, T.C.; et al. Associations of Maternal Weight Status before, during, and after Pregnancy with Inflammatory Markers in Breast Milk: Weight Status and Breast Milk Inflammatory Markers. Obesity 2017, 25, 2092–2099. [Google Scholar] [CrossRef]
- Sonnenschein-van Der Voort, A.M.M.; Jaddoe, V.W.V.; Moll, H.A.; Hofman, A.; Van Der Valk, R.J.P.; De Jongste, J.C.; Duijts, L. Influence of Maternal and Cord Blood C-Reactive Protein on Childhood Respiratory Symptoms and Eczema. Pediatr. Allergy Immunol. 2013, 24, 469–475. [Google Scholar] [CrossRef]
- Liu, G.; Zhang, Y.; Zhang, W.; Wu, X.; Jiang, H.; Huang, H.; Zhang, X. Novel Predictive Risk Factor for Erectile Dysfunction: Serum High-Sensitivity C-Reactive Protein. Andrology 2022, 10, 1096–1106. [Google Scholar] [CrossRef]
- Billups, K.L.; Kaiser, D.R.; Kelly, A.S.; Wetterling, R.A.; Tsai, M.Y.; Hanson, N.; Bank, A.J. Relation of C-Reactive Protein and Other Cardiovascular Risk Factors to Penile Vascular Disease in Men with Erectile Dysfunction. Int. J. Impot. Res. 2003, 15, 231–236. [Google Scholar] [CrossRef] [PubMed]
- Crawford, P.; Crop, J.A. Evaluation of Scrotal Masses. Am. Fam. Physician 2014, 89, 723–727. [Google Scholar]
- Asgari, S.A.; Mokhtari, G.; Falahatkar, S.; Mansour-Ghanaei, M.; Roshani, A.; Zare, A.; Zamani, M.; Khosropanah, I.; Salehi, M. Diagnostic Accuracy of C-Reactive Protein and Erythrocyte Sedimentation Rate in Patients with Acute Scrotum. Urol. J. 2006, 3, 104–108. [Google Scholar] [PubMed]
- Tanaka, K.; Ogasawara, Y.; Nikai, K.; Yamada, S.; Fujiwara, K.; Okazaki, T. Acute Scrotum and Testicular Torsion in Children: A Retrospective Study in a Single Institution. J. Pediatr. Urol. 2020, 16, 55–60. [Google Scholar] [CrossRef]
- Namazi, M.R.; Parhizkar, A.R.; Jowkar, F. serum levels of hypersensitive-C-reactive protein in moderate and severe acne. Indian Dermatol. Online J. 2015, 6, 253–257. [Google Scholar] [CrossRef] [PubMed]
- Monib, K.M.E.; El-fallah, A.A.; Salem, R.M. Inflammatory Markers in Acne Vulgaris: Saliva as a Novel Diagnostic Fluid. J. Cosmet. Dermatol. 2022, 21, 1280–1285. [Google Scholar] [CrossRef] [PubMed]
- El-Taweel, A.A.; Salem, R.M.; El-Shimi, O.S. Predictive Value of Serum Markers for Postacne Scarring. J. Cosmet. Dermatol. 2018, 17, 491–494. [Google Scholar] [CrossRef]
- Zinkevičienė, A.; Kainov, D.; Lastauskienė, E.; Kvedarienė, V.; Bychkov, D.; Byrne, M.; Girkontaitė, I. Serum Biomarkers of Allergic Contact Dermatitis: A Pilot Study. IAA 2015, 168, 161–164. [Google Scholar] [CrossRef] [PubMed]
- Vekaria, A.S.; Brunner, P.M.; Aleisa, A.I.; Bonomo, L.; Lebwohl, M.G.; Israel, A.; Guttman-Yassky, E. Moderate-to-Severe Atopic Dermatitis Patients Show Increases in Serum C-Reactive Protein Levels, Correlating with Skin Disease Activity. F1000Research 2017, 6, 1712. [Google Scholar] [CrossRef]
- Tosun, M.; Yasak Güner, R.; Akyol, M. Investigation of the Relationship between Inflammatory Blood Parameters and Seborrheic Dermatitis. J. Cosmet. Dermatol. 2022, 21, 5111–5115. [Google Scholar] [CrossRef]
- Duman, N.; Ersoy Evans, S.; Atakan, N. Rosacea and Cardiovascular Risk Factors: A Case Control Study. J. Eur. Acad. Dermatol. Venereol. 2014, 28, 1165–1169. [Google Scholar] [CrossRef]
- Li, Y.; Guo, L.; Hao, D.; Li, X.; Wang, Y.; Jiang, X. Association between Rosacea and Cardiovascular Diseases and Related Risk Factors: A Systematic Review and Meta-Analysis. Biomed. Res. Int. 2020, 2020, 7015249. [Google Scholar] [CrossRef] [PubMed]
- Sinikumpu, S.-P.; Huilaja, L.; Auvinen, J.; Jokelainen, J.; Puukka, K.; Ruokonen, A.; Timonen, M.; Tasanen, K. The Association Between Low Grade Systemic Inflammation and Skin Diseases: A Cross-Sectional Survey in the Northern Finland Birth Cohort 1966. Acta Derm. Venereol. 2018, 98, 65–69. [Google Scholar] [CrossRef]
- Sorensen, E.P.; Matiz, C.; Friedlander, S.F. An 8-Month-Old Boy with Purpuric Skin Lesions. Acute Hemorrhagic Edema of Infancy. Pediatr. Ann. 2014, 43, e4–e8. [Google Scholar] [CrossRef]
- Giraud-Kerleroux, L.; Bellon, N.; Welfringer-Morin, A.; Leclerc-Mercier, S.; Costedoat, I.; Coquin, J.; Brun, A.; Roguedas-Contios, A.-M.; Bernier, C.; Milpied, B.; et al. Childhood Epidermal Necrolysis and Erythema Multiforme Major: A Multicentre French Cohort Study of 62 Patients. J. Eur. Acad. Dermatol. Venereol. 2021, 35, 2051–2058. [Google Scholar] [CrossRef]
- Watanabe, R.; Watanabe, H.; Sotozono, C.; Kokaze, A.; Iijima, M. Critical Factors Differentiating Erythema Multiforme Majus from Stevens-Johnson Syndrome (SJS)/Toxic Epidermal Necrolysis (TEN). Eur. J. Dermatol. 2011, 21, 889–894. [Google Scholar] [CrossRef]
- Relvas, M.; Silva, J.; Matos, A.L.; Alves, F.; Gonçalo, M. Concomitant Evaluation of D-Dimer and C-Reactive Protein in Chronic Spontaneous Urticaria May Show Divergent Values. Eur. Ann. Allergy Clin. Immunol. 2022. [Google Scholar] [CrossRef]
- Yan, S.; Chen, W.; Su, J.; Chen, M.; Zhu, W.; Zhang, J.; Yi, M.; Chen, X.; Li, J. Association between C reactive protein and clinical characteristics in patients with chronic spontaneous urticaria. Zhong Nan Da Xue Xue Bao Yi Xue Ban 2017, 42, 168–172. [Google Scholar] [CrossRef]
- Kolkhir, P.; Altrichter, S.; Hawro, T.; Maurer, M. C-Reactive Protein Is Linked to Disease Activity, Impact, and Response to Treatment in Patients with Chronic Spontaneous Urticaria. Allergy 2018, 73, 940–948. [Google Scholar] [CrossRef]
- Aleem, S.; Masood, Q.; Hassan, I. Correlation of C-Reactive Protein Levels with Severity of Chronic Urticaria. Indian J. Dermatol. 2014, 59, 636. [Google Scholar] [CrossRef]
- Criado, R.F.; Bensi, C.G.; Criado, P.R.; Henriques, M.T.; de Espindola, B.A.R.; Machado Filho, C.D. Evaluation of Serum Levels of C-Reactive Protein, D-Dimer and Autologous Serum Skin Test in Patients with Chronic Spontaneous Urticaria in a Brazilian Tertiary Center: A Cross-Sectional Study. Bras. Dermatol. 2021, 96, 148–154. [Google Scholar] [CrossRef]
- Malekmakan, L.; Malekmakan, A.; Sayadi, M.; Pakfetrat, M.; Sepaskhah, M.; Roozbeh, J. Association of High-Sensitive C-Reactive Protein and Dialysis Adequacy with Uremic Pruritus. Saudi J. Kidney Dis. Transpl. 2015, 26, 890–895. [Google Scholar] [CrossRef]
- Bano, G.; Trevisan, C.; Carraro, S.; Solmi, M.; Luchini, C.; Stubbs, B.; Manzato, E.; Sergi, G.; Veronese, N. Inflammation and Sarcopenia: A Systematic Review and Meta-Analysis. Maturitas 2017, 96, 10–15. [Google Scholar] [CrossRef]
- Tuttle, C.S.L.; Thang, L.A.N.; Maier, A.B. Markers of Inflammation and Their Association with Muscle Strength and Mass: A Systematic Review and Meta-Analysis. Ageing Res. Rev. 2020, 64, 101185. [Google Scholar] [CrossRef] [PubMed]
- Shokri-Mashhadi, N.; Moradi, S.; Heidari, Z.; Saadat, S. Association of Circulating C-Reactive Protein and High-Sensitivity C-Reactive Protein with Components of Sarcopenia: A Systematic Review and Meta-Analysis of Observational Studies. Exp. Gerontol. 2021, 150, 111330. [Google Scholar] [CrossRef]
- Isaacs, A.W.; Macaluso, F.; Smith, C.; Myburgh, K.H. C-Reactive Protein Is Elevated Only in High Creatine Kinase Responders to Muscle Damaging Exercise. Front. Physiol. 2019, 10, 86. [Google Scholar] [CrossRef] [PubMed]
- Hanisch, F.; Zierz, S. C-Reactive Protein in Idiopathic Inflammatory Myopathies. MYOPAIN 2015, 23, 45–51. [Google Scholar] [CrossRef]
- Filková, M.; Hulejová, H.; Kuncová, K.; Pleštilová, L.; Cerezo, L.A.; Mann, H.; Klein, M.; Zámečník, J.; Gay, S.; Vencovský, J.; et al. Resistin in Idiopathic Inflammatory Myopathies. Arthritis Res. Ther. 2012, 14, R111. [Google Scholar] [CrossRef]
- Xiao, Y.; Haynes, W.L.; Michalek, J.E.; Russell, I.J. Elevated Serum High-Sensitivity C-Reactive Protein Levels in Fibromyalgia Syndrome Patients Correlate with Body Mass Index, Interleukin-6, Interleukin-8, Erythrocyte Sedimentation Rate. Rheumatol. Int. 2013, 33, 1259–1264. [Google Scholar] [CrossRef] [PubMed]
- Feinberg, T.; Sambamoorthi, U.; Lilly, C.; Innes, K.K. Potential Mediators between Fibromyalgia and C-Reactive Protein: Results from a Large U.S. Community Survey. BMC Musculoskelet. Disord. 2017, 18, 294. [Google Scholar] [CrossRef]
- Zetterman, T.; Markkula, R.; Kalso, E. Elevated highly sensitive C-reactive protein in fibromyalgia associates with symptom severity. Rheumatol. Adv. Pract. 2022, 6, rkac053. [Google Scholar] [CrossRef]
- Cruz-Guzmán, O.D.R.; Rodríguez-Cruz, M.; Escobar Cedillo, R.E. Systemic Inflammation in Duchenne Muscular Dystrophy: Association with Muscle Function and Nutritional Status. Biomed. Res. Int. 2015, 2015, 891972. [Google Scholar] [CrossRef] [PubMed]
- Hughes, A.; Kumari, M. Age Modification of the Relationship between C-Reactive Protein and Fatigue: Findings from Understanding Society (UKHLS). Psychol. Med. 2018, 48, 1341–1349. [Google Scholar] [CrossRef]
- Manzo, C.; Milchert, M. Polymyalgia rheumatica with normal values of both erythrocyte sedimentation rate and C-reactive protein concentration at the time of diagnosis: A four-point guidance. Rheumatology 2018, 56, 1–2. [Google Scholar] [CrossRef]
- Lund Håheim, L.; Nafstad, P.; Olsen, I.; Schwarze, P.; Rønningen, K.S. C-Reactive Protein Variations for Different Chronic Somatic Disorders. Scand. J. Public Health 2009, 37, 640–646. [Google Scholar] [CrossRef]
- Maugeri, D.; Russo, M.S.; Franzé, C.; Motta, V.; Motta, M.; Destro, G.; Speciale, S.; Santangelo, A.; Panebianco, P.; Malaguarnera, M. Correlations between C-Reactive Protein, Interleukin-6, Tumor Necrosis Factor-α and Body Mass Index during Senile Osteoporosis. Arch. Gerontol. Geriatr. 1998, 27, 159–163. [Google Scholar] [CrossRef] [PubMed]
- de Pablo, P.; Cooper, M.S.; Buckley, C.D. Association between Bone Mineral Density and C-Reactive Protein in a Large Population-Based Sample. Arthritis Rheum. 2012, 64, 2624–2631. [Google Scholar] [CrossRef]
- Ye, W.; Cheng, S.; Xiao, J.; Yu, H. High-Sensitivity C-Reactive Protein Could Be a Potential Indicator of Bone Mineral Density in Adolescents Aged 10-20 Years. Sci. Rep. 2022, 12, 7119. [Google Scholar] [CrossRef]
- Berglundh, S.; Malmgren, L.; Luthman, H.; McGuigan, F.; Åkesson, K. C-Reactive Protein, Bone Loss, Fracture, and Mortality in Elderly Women: A Longitudinal Study in the OPRA Cohort. Osteoporos. Int. 2015, 26, 727–735. [Google Scholar] [CrossRef]
- Sowers, M.; Jannausch, M.; Stein, E.; Jamadar, D.; Hochberg, M.; Lachance, L. C-Reactive Protein as a Biomarker of Emergent Osteoarthritis. Osteoarthr. Cartil. 2002, 10, 595–601. [Google Scholar] [CrossRef] [PubMed]
- Dainese, P.; Wyngaert, K.V.; De Mits, S.; Wittoek, R.; Van Ginckel, A.; Calders, P. Association between Knee Inflammation and Knee Pain in Patients with Knee Osteoarthritis: A Systematic Review. Osteoarthr. Cartil. 2022, 30, 516–534. [Google Scholar] [CrossRef] [PubMed]
- Liang, Y.; Xu, K.; Liu, W.; Liu, X.; Yuan, P.; Xu, P.; Li, H. Monomeric C-Reactive Protein Level Is Associated with Osteoarthritis. Exp. Ther. Med. 2022, 23, 277. [Google Scholar] [CrossRef]
- Wei, J.; Zhang, H.; Wang, Y.; Li, C.; Ma, A. Analysis of serum ferritin and high sensitive C reactive protein in patients with gout. Wei Sheng Yan Jiu 2017, 46, 232–236. [Google Scholar]
- Hanna, F.S.; Bell, R.J.; Cicuttini, F.M.; Davison, S.L.; Wluka, A.E.; Davis, S.R. High Sensitivity C-Reactive Protein Is Associated with Lower Tibial Cartilage Volume but Not Lower Patella Cartilage Volume in Healthy Women at Mid-Life. Arthritis Res. Ther. 2008, 10, R27. [Google Scholar] [CrossRef]
- Park, H.B.; Gwark, J.-Y.; Jung, J.; Jeong, S.-T. Association Between High-Sensitivity C-Reactive Protein and Idiopathic Adhesive Capsulitis. J. Bone Jt. Surg. Am. 2020, 102, 761–768. [Google Scholar] [CrossRef] [PubMed]
- Gwark, J.-Y.; Park, H.B. Association of High Sensitivity C-Reactive Protein with Tearing of the Long Head of the Biceps Tendon. BMC Musculoskelet. Disord. 2019, 20, 518. [Google Scholar] [CrossRef]
- Pritchett, J.W. C-Reactive Protein Levels Determine the Severity of Soft-Tissue Injuries. Am. J. Orthop. 1996, 25, 759–761. [Google Scholar] [PubMed]
- Windisch, C.; Brodt, S.; Roehner, E.; Matziolis, G. The C-Reactive Protein Level after Total Knee Arthroplasty Is Gender Specific. Knee Surg. Sports Traumatol. Arthrosc. 2016, 24, 3163–3167. [Google Scholar] [CrossRef] [PubMed]
- Shih, L.-Y.; Wu, J.-J.; Yang, D.-J. Erythrocyte Sedimentation Rate and C-Reactive Protein Values in Patients with Total Hip Arthroplasty. Clin. Orthop. Relat. Res. 1987, 225, 238. [Google Scholar] [CrossRef]
- Smith, J.W.; Martins, T.B.; Gopez, E.; Johnson, T.; Hill, H.R.; Rosenberg, T.D. Significance of C-Reactive Protein in Osteoarthritis and Total Knee Arthroplasty Outcomes. Ther. Adv. Musculoskelet. 2012, 4, 315–325. [Google Scholar] [CrossRef]
- Shen, H.; Zhang, N.; Zhang, X.; Ji, W. C-Reactive Protein Levels after 4 Types of Arthroplasty. Acta Orthop. 2009, 80, 330–333. [Google Scholar] [CrossRef]
- Foglar, C.; Lindsey, R.W. C-Reactive Protein in Orthopedics. Orthopedics 1998, 21, 687–691. [Google Scholar] [CrossRef]
- Førsvoll, J.A.; Oymar, K. C-Reactive Protein in the Periodic Fever, Aphthous Stomatitis, Pharyngitis and Cervical Adenitis (PFAPA) Syndrome. Acta Paediatr. 2007, 96, 1670–1673. [Google Scholar] [CrossRef]
- Lazea, C.; Damian, L.; Vulturar, R.; Lazar, C. PFAPA Syndrome: Clinical, Laboratory and Therapeutic Features in a Single-Centre Cohort. Int. J. Gen. Med. 2022, 15, 6871–6880. [Google Scholar] [CrossRef] [PubMed]
- Patil, V.A.; Desai, M.H. Effect of Periodontal Therapy on Serum C-Reactive Protein Levels in Patients with Gingivitis and Chronic Periodontitis: A Clinicobiochemical Study. J. Contemp. Dent. Pract. 2013, 14, 233–237. [Google Scholar] [CrossRef]
- Pitchika, V.; Thiering, E.; Metz, I.; Rothmaier, K.; Willenberg, A.; Hickel, R.; Standl, M.; Kocher, T.; Heinrich, J.; Kühnisch, J. Gingivitis and Lifestyle Influences on High-Sensitivity C-Reactive Protein and Interleukin 6 in Adolescents. J. Clin. Periodontol. 2017, 44, 372–381. [Google Scholar] [CrossRef] [PubMed]
- Bansal, T.; Dhruvakumar, D.; Pandey, A. Comparative Evaluation of C-Reactive Protein in Peripheral Blood of Patients with Healthy Gingiva, Gingivitis and Chronic Periodontitis: A Clinical and Particle-Enhanced Turbidimetric Immuno-Analysis. J. Indian Soc. Periodontol. 2014, 18, 739–743. [Google Scholar] [CrossRef] [PubMed]
- Machado, V.; Botelho, J.; Escalda, C.; Hussain, S.B.; Luthra, S.; Mascarenhas, P.; Orlandi, M.; Mendes, J.J.; D’Aiuto, F. Serum C-Reactive Protein and Periodontitis: A Systematic Review and Meta-Analysis. Front. Immunol. 2021, 12, 706432. [Google Scholar] [CrossRef] [PubMed]
- Paraskevas, S.; Huizinga, J.D.; Loos, B.G. A Systematic Review and Meta-Analyses on C-Reactive Protein in Relation to Periodontitis. J. Clin. Periodontol. 2008, 35, 277–290. [Google Scholar] [CrossRef]
- Liu, W.L.; Chen, C.F.; Lu, D.L.; Guo, L.F. Clinical evaluation value of visual analogue scale combined with C-reactive protein for the prognosis of peritonsillar abscess. Lin Chung Er Bi Yan Hou Tou Jing Wai Ke Za Zhi 2017, 31, 794–795. [Google Scholar] [CrossRef]
- Saadi, N.; Ghaib, N.H. Effect of Orthodontic Tooth Movement on Salivary Levels of Interleukin-1beta, Tumor Necrosis Factor-Alpha, and C- Reactive Protein. J. Baghdad Coll. Dent. 2013, 25, 120–125. [Google Scholar] [CrossRef]
- Graziani, F.; D’Aiuto, F.; Gennai, S.; Petrini, M.; Nisi, M.; Cirigliano, N.; Landini, L.; Bruno, R.M.; Taddei, S.; Ghiadoni, L. Systemic Inflammation after Third Molar Removal: A Case-Control Study. J. Dent. Res. 2017, 96, 1505–1512. [Google Scholar] [CrossRef]
- Kindler, S.; Mksoud, M.; Holtfreter, B.; Friedrich, N.; Bülow, R.; Ittermann, T. Do Third Molars Contribute to Systemic Inflammation? Results from a Population-Based Study from Northeast Germany. J. Oral Maxillofac. Surg. 2019, 77, 1541–1547. [Google Scholar] [CrossRef]
- Pay, J.B.; Shaw, A.M. Towards Salivary C-Reactive Protein as a Viable Biomarker of Systemic Inflammation. Clin. Biochem. 2019, 68, 1–8. [Google Scholar] [CrossRef]
- Shiva, A.; Arab, S.; Mousavi, S.J.; Zamanian, A.; Maboudi, A. Serum and Salivary Level of Nitric Oxide (NOx) and CRP in Oral Lichen Planus (OLP) Patients. J. Dent. (Shiraz.) 2020, 21, 6–11. [Google Scholar]
- Ersin Kalkan, R.; Öngöz Dede, F.; Gökmenoğlu, C.; Kara, C. Salivary Fetuin-A, S100A12, and High-Sensitivity C-Reactive Protein Levels in Periodontal Diseases. Oral Dis. 2018, 24, 1554–1561. [Google Scholar] [CrossRef] [PubMed]
- Bilgic, F.; Akinci Sozer, O.; Ozcan, O.; Gurpinar, A.B.; Yilmaz, H.; Ay, Y. Evaluation of Inflammation during Fixed Orthodontic Treatment. Arch. Oral Biol. 2016, 71, 54–58. [Google Scholar] [CrossRef]
- Ajwani, S.; Mattila, K.J.; Narhi, T.O.; Tilvis, R.S.; Ainamo, A. Oral Health Status, C-Reactive Protein and Mortality—A 10 Year Follow-up Study. Gerodontology 2003, 20, 32–40. [Google Scholar] [CrossRef]
- Babaei, M.; Rezaei, S.; Saghafi Khadem, S.; Shirinbak, I.; Basir Shabestari, S. The Role of Salivary C-Reactive Protein in Systemic and Oral Disorders: A Systematic Review. Med. J. Islam. Repub. Iran. 2022, 36, 138. [Google Scholar] [CrossRef]
- Marcano-Acuña, M.E.; Carrasco-Llatas, M.; Tortajada-Girbés, M.; Dalmau-Galofre, J.; Codoñer-Franch, P. Impact of Adenotonsillectomy on the Evolution of Inflammatory Markers. Clin. Otolaryngol. 2019, 44, 983–988. [Google Scholar] [CrossRef]
- Akinci, E.; Aygencel, G.; Keles, A.; Demircan, A.; Bildik, F. Role of C-Reactive Protein, D-Dimer, and Fibrinogen Levels in the Differential Diagnosis of Central and Peripheral Vertigo. Adv. Ther. 2007, 24, 1068–1077. [Google Scholar] [CrossRef]
- Koob, I.; Pickhard, A.; Buchberger, M.; Boxberg, M.; Reiter, R.; Piontek, G.; Straßen, U. Bradykinin Receptor B1 and C-Reactive Protein as Prognostic Factors for Pharyngocutaneous Fistula Development after Laryngectomy. Head Neck Pathol. 2020, 14, 341–352. [Google Scholar] [CrossRef] [PubMed]
- Wu, R.; Wang, J.J.; Tai, E.S.; Wong, T.Y. Cardiovascular Risk Factors, Inflammation, and Corneal Arcus: The Singapore Malay Eye Study. Am. J. Ophthalmol. 2010, 150, 581–587.e1. [Google Scholar] [CrossRef]
- Hong, I.H.; Ahn, J.K.; Chang, S.; Park, S.P. Diagnostic Efficacy of Total Homocysteine and C-Reactive Protein for Ocular Ischemic Syndrome. Eye 2011, 25, 1650–1654. [Google Scholar] [CrossRef]
- Duru, Z.; Altunel, O.; Alabay, B.; Sirakaya, E.; Sirakaya, E.; Kucuk, B.; Musaoglu, M. Elevated Monocyte-to-High-Density Lipoprotein Ratio as an Indicator of Systemic Inflammation in Patients with Branch Retinal Vein Occlusion. Beyoglu Eye J. 2021, 6, 212–216. [Google Scholar] [CrossRef]
- Lee, H.B.H.; Pulido, J.S.; McCannel, C.A.; Buettner, H. Role of Inflammation in Retinal Vein Occlusion. Can J. Ophthalmol. 2007, 42, 131–133. [Google Scholar] [CrossRef]
- Goldenberg-Cohen, N.; Cohen, Y.; Monselise, Y.; Eldar, I.; Axer-Siegel, R.; Weinberger, D.; Kramer, M. C-Reactive Protein Levels Do Not Correlate with Retinal Artery Occlusion but with Atherosclerosis. Eye 2009, 23, 785–790. [Google Scholar] [CrossRef]
- Yu, D.; Shi, L.; Zhang, X.; Yang, H.; Feng, J.; Wang, Y. Primary Empty Sella Syndrome-Caused Rhabdomyolysis Misdiagnosed as Recurrent Sepsis: A Case Report and Literature Review. Int. J. Infect. Dis. 2023, 130, 144–146. [Google Scholar] [CrossRef]
- Hong, T.; Tan, A.G.; Mitchell, P.; Wang, J.J. A Review and Meta-Analysis of the Association between C-Reactive Protein and Age-Related Macular Degeneration. Surv. Ophthalmol. 2011, 56, 184–194. [Google Scholar] [CrossRef]
- Feng, C.; Krogh Nielsen, M.; Sørensen, T.L.; Subhi, Y. Systemic Levels of C-Reactive Protein in Patients with Age-Related Macular Degeneration: A Systematic Review with Meta-Analyses. Mech. Ageing. Dev. 2020, 191, 111353. [Google Scholar] [CrossRef]
- Chen, R.C.; Palestine, A.G.; Lynch, A.M.; Patnaik, J.L.; Wagner, B.D.; Mathias, M.T.; Mandava, N. Increased Systemic C-Reactive Protein Is Associated with Choroidal Thinning in Intermediate Age-Related Macular Degeneration. Transl. Vis. Sci. Technol. 2021, 10, 7. [Google Scholar] [CrossRef]
- Lee, S.S.-Y.; Beales, D.J.; Chen, F.K.; Yazar, S.; Alonso-Caneiro, D.; Mackey, D.A. Associations between Seven-Year C-Reactive Protein Trajectory or Pack-Years Smoked with Choroidal or Retinal Thicknesses in Young Adults. Sci. Rep. 2021, 11, 6147. [Google Scholar] [CrossRef]
- Zaliuniene, D.; Paunksnis, A.; Gustiene, O.; Brazdzionyte, J.; Zaliunas, R. Pre- and Postoperative C-Reactive Protein Levels in Patients with Cataract and Age-Related Macular Degeneration. Eur. J. Ophthalmol. 2007, 17, 919–927. [Google Scholar] [CrossRef]
- Erol, M.K.; Balkarli, A.; Yucel, O.; Akar, Y.; Dogan, B.; Suren, E. Neutrophil/Lymphocyte Ratio and Mean Platelet Volume in Central Serous Chorioretinopathy. Ther. Clin. Risk Manag. 2017, 13, 945–950. [Google Scholar] [CrossRef]
- Choi, J.; Joe, S.G.; Seong, M.; Choi, J.Y.; Sung, K.R.; Kook, M.S. C-Reactive Protein and Lipid Profiles in Korean Patients with Normal Tension Glaucoma. Korean J. Ophthalmol. 2009, 23, 193–197. [Google Scholar] [CrossRef]
- Tervo, T.; van Setten, G.B.; Hovi, M.; Pakarinen, M.; Tarkkanen, A.; Valtonen, V. C-Reactive Protein Serum Levels in Patients with Ocular Disease. Acta Ophthalmol. 1994, 72, 110–113. [Google Scholar] [CrossRef] [PubMed]
- Mocan, M.C.; Dikmetas, O.; Irkec, M. Serum C-Reactive Protein Levels in Exfoliation Syndrome and Exfoliative Glaucoma. Eye 2011, 25, 1383–1384. [Google Scholar] [CrossRef] [PubMed]
- Lesiewska, H.; Malukiewicz, G.; Mańkowska-Cyl, A.; Odrowąż-Sypniewska, G. Lipids and C-Reactive Protein as Vascular Risk Markers in Pseudoexfoliation Syndrome. Acta Ophthalmol. 2016, 94, e380–e381. [Google Scholar] [CrossRef]
- Murakami, Y.; Ikeda, Y.; Nakatake, S.; Fujiwara, K.; Tachibana, T.; Yoshida, N.; Notomi, S.; Hisatomi, T.; Yoshida, S.; Ishibashi, T.; et al. C-Reactive Protein and Progression of Vision Loss in Retinitis Pigmentosa. Acta Ophthalmol. 2018, 96, e174–e179. [Google Scholar] [CrossRef] [PubMed]
- Barrett, A.; Gnehm, D.; Jones, J.; Trask, B.C. A1-Antitrypsin and C-Reactive Protein Levels in Tear Fluid after Continuous Contact Lens Wear. Clin. Exp. Optom. 2014, 97, 66–71. [Google Scholar] [CrossRef]
- Duan, J.; Leng, X.; Han, Z.; Cai, Y.; Wang, C.; Rajah, G.; Song, H.; Ding, Y.; Ji, X. Identifying Biomarkers Associated with Venous Infarction in Acute/Subacute Cerebral Venous Thrombosis. Aging Dis. 2021, 12, 93–101. [Google Scholar] [CrossRef]
- Hurth, H.; Birkenhauer, U.; Steiner, J.; Schlak, D.; Hennersdorf, F.; Ebner, F.H. Delayed Cerebral Ischemia in Patients with Aneurysmal Subarachnoid Hemorrhage—Serum D-Dimer and C-Reactive Protein as Early Markers. J. Stroke Cerebrovasc. Dis. 2020, 29, 104558. [Google Scholar] [CrossRef]
- Alessandro, O.; Rene, W.; Stefan, W.; Miodrag, F.; Martin, S.; Oliver, B.; Urs, P. C-Reactive Protein Elevation Predicts in-Hospital Deterioration after Aneurysmal Subarachnoid Hemorrhage: A Retrospective Observational Study. Acta Neurochir. 2022, 164, 1805–1814. [Google Scholar] [CrossRef]
- Lee, S.; Kim, Y.O.; Ryu, J.-A. Clinical Usefulness of Early Serial Measurements of C-Reactive Protein as Outcome Predictors in Patients with Subarachnoid Hemorrhage. BMC Neurol. 2020, 20, 112. [Google Scholar] [CrossRef]
- Wang, F.; Wang, L.; Jiang, T.; Xia, J.; Xu, F.; Shen, L.; Kang, W.; Ding, Y.; Mei, L.; Ju, X.; et al. Neutrophil-to-Lymphocyte Ratio Is an Independent Predictor of 30-Day Mortality of Intracerebral Hemorrhage Patients: A Validation Cohort Study. Neurotox. Res. 2018, 34, 347–352. [Google Scholar] [CrossRef]
- Wang, J.; Wang, W.; Liu, Y.; Zhao, X. Associations between Levels of High-Sensitivity C-Reactive Protein and Outcome after Intracerebral Hemorrhage. Front. Neurol. 2020, 11, 535068. [Google Scholar] [CrossRef] [PubMed]
- Gill, R.; Kemp, J.A.; Sabin, C.; Pepys, M.B. Human C-Reactive Protein Increases Cerebral Infarct Size after Middle Cerebral Artery Occlusion in Adult Rats. J. Cereb. Blood Flow Metab. 2004, 24, 1214–1218. [Google Scholar] [CrossRef]
- Inomata, K.; Mizobuchi, M.; Tanaka, S.; Iwatani, S.; Sakai, H.; Yoshimoto, S.; Nakao, H. Patterns of Increases in Interleukin-6 and C-Reactive Protein as Predictors for White Matter Injury in Preterm Infants. Pediatr. Int. 2014, 56, 851–855. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Wang, A.; Zhang, J.; Singh, M.; Liu, D.; Zuo, Y.; Wu, L.; Song, M.; Wang, W.; Feigin, V.; et al. Association of Plasma C-Reactive Protein with Ischaemic Stroke: A Mendelian Randomization Study. Eur. J. Neurol. 2020, 27, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Erdal, G.; Hursitoglu, M.; Erdogan, H.; Yildirim, G.; Yayla, V.; Issever, H.; Isiksacan, N.; Kural, A.; Cirak, M.; Kansu, A.; et al. Serum C-Reactive Protein and Sex Hormone Levels in the Early Hyperacute Phase of Stroke. Clin. Lab. 2021, 67. [Google Scholar] [CrossRef] [PubMed]
- Akhter, S.; Das, S.N.; Sutradhar, S.R.; Basher, M.S.; Khan, M.K. Level of Serum C-Reactive Protein among Patients with Stroke. Mymensingh Med. J. 2018, 27, 461–466. [Google Scholar] [PubMed]
- Mazaheri, S.; Reisi, E.; Poorolajal, J.; Ghiasian, M. C-Reactive Protein Levels and Clinical Outcomes in Stroke Patients: A Prospective Cohort Study. Arch. Iran. Med. 2018, 21, 8–12. [Google Scholar] [PubMed]
- Wang, Y.; Li, J.; Pan, Y.; Wang, M.; Meng, X.; Wang, Y. Association between High-Sensitivity C-Reactive Protein and Prognosis in Different Periods after Ischemic Stroke or Transient Ischemic Attack. J. Am. Heart Assoc. 2022, 11, e025464. [Google Scholar] [CrossRef]
- Yu, B.; Yang, P.; Xu, X.; Shao, L. C-Reactive Protein for Predicting All-Cause Mortality in Patients with Acute Ischemic Stroke: A Meta-Analysis. Biosci. Rep. 2019, 39, BSR20181135. [Google Scholar] [CrossRef]
- Yang, L.; Xu, B. Evaluation of Serum Levels of Homocysteine and C-Reactive Protein in Patients with Ischemic Stroke. Cell Mol. Biol. 2022, 68, 56–62. [Google Scholar] [CrossRef]
- Baba, S.S.; Yarube, I.U. Raised High-Sensitivity C-Reactive Protein and Cognitive Impairment among African Stroke Survivors within the First Three Months Following Stroke. J. Clin. Neurosci. 2021, 88, 191–196. [Google Scholar] [CrossRef]
- Gu, H.-Q.; Yang, K.-X.; Lin, J.-X.; Jing, J.; Zhao, X.-Q.; Wang, Y.-L.; Liu, L.-P.; Meng, X.; Jiang, Y.; Li, H.; et al. Association between High-Sensitivity C-Reactive Protein, Functional Disability, and Stroke Recurrence in Patients with Acute Ischaemic Stroke: A Mediation Analysis. EBioMedicine 2022, 80, 104054. [Google Scholar] [CrossRef]
- Chen, L.; Xiong, S.; Liu, Y.; Lin, M.; Wang, J.; Zhong, R.; Zhao, J.; Liu, W.; Zhu, L.; Shang, X. C-Reactive Protein Can Be an Early Predictor of Poststroke Apathy in Acute Ischemic Stroke Patients. J. Stroke Cerebrovasc. Dis. 2018, 27, 1861–1869. [Google Scholar] [CrossRef] [PubMed]
- Liu, X.; Wang, B.; Wang, X.; Tian, M.; Wang, X.; Zhang, Y. Elevated Plasma High-Sensitivity C-Reactive Protein at Admission Predicts the Occurrence of Post-Stroke Fatigue at 6 Months after Ischaemic Stroke. Eur. J. Neurol. 2020, 27, 2022–2030. [Google Scholar] [CrossRef] [PubMed]
- Klimiec-Moskal, E.; Slowik, A.; Dziedzic, T. Serum C-Reactive Protein Adds Predictive Information for Post-Stroke Delirium: The PROPOLIS Study. Acta Psychiatr. Scand. 2022, 147, 536–542. [Google Scholar] [CrossRef]
- Jiang, G.; Zhou, D.; Yan, X.; Zheng, Q.; Tang, Z. Association between C-Reactive Protein Levels and Development of Post-Stroke Depression: A Systematic Review and Meta-Analysis. Scott. Med. J. 2022, 67, 135–143. [Google Scholar] [CrossRef]
- Purroy, F.; Montaner, J.; Molina, C.A.; Delgado, P.; Arenillas, J.F.; Chacon, P.; Quintana, M.; Alvarez-Sabin, J. C-Reactive Protein Predicts Further Ischemic Events in Transient Ischemic Attack Patients. Acta Neurol. Scand. 2007, 115, 60–66. [Google Scholar] [CrossRef] [PubMed]
- Towfighi, A.; Cheng, E.M.; Ayala-Rivera, M.; Barry, F.; McCreath, H.; Ganz, D.A.; Lee, M.L.; Sanossian, N.; Mehta, B.; Dutta, T.; et al. Effect of a Coordinated Community and Chronic Care Model Team Intervention vs Usual Care on Systolic Blood Pressure in Patients with Stroke or Transient Ischemic Attack: The SUCCEED Randomized Clinical Trial. JAMA Netw. Open 2021, 4, e2036227. [Google Scholar] [CrossRef] [PubMed]
- Mengozzi, M.; Kirkham, F.A.; Girdwood, E.E.R.; Bunting, E.; Drazich, E.; Timeyin, J.; Ghezzi, P.; Rajkumar, C. C-Reactive Protein Predicts Further Ischemic Events in Patients with Transient Ischemic Attack or Lacunar Stroke. Front. Immunol. 2020, 11, 1403. [Google Scholar] [CrossRef] [PubMed]
- Tsushima, M.; Metoki, N.; Hagii, J.; Saito, S.; Shiroto, H.; Yasujima, M.; Kato, T.; Kudo, N.; Toyama, Y.; Yokono, Y.; et al. D-Dimer and C-Reactive Protein as Potential Biomarkers for Diagnosis of Trousseau’s Syndrome in Patients with Cerebral Embolism. J. Stroke Cerebrovasc. Dis. 2020, 29, 104534. [Google Scholar] [CrossRef]
- Mota Telles, J.P.; Rabelo, N.N.; Junior, J.R.; Teixeira, M.J.; Figueiredo, E.G. C-Reactive Protein Levels Are Higher in Patients with Fusiform Intracranial Aneurysms: A Case-Control Study. World Neurosurg. 2021, 146, e896–e901. [Google Scholar] [CrossRef] [PubMed]
- Mitaki, S.; Nagai, A.; Oguro, H.; Yamaguchi, S. C-Reactive Protein Levels Are Associated with Cerebral Small Vessel-Related Lesions. Acta Neurol. Scand. 2016, 133, 68–74. [Google Scholar] [CrossRef]
- Lippi, G.; Mattiuzzi, C.; Cervellin, G. C-Reactive Protein and Migraine. Facts or Speculations? Clin. Chem. Lab. Med. 2014, 52, 1265–1272. [Google Scholar] [CrossRef] [PubMed]
- Hagen, K.; Stovner, L.J.; Zwart, J.-A. High Sensitivity C-Reactive Protein and Risk of Migraine in a 11-Year Follow-up with Data from the Nord-Trøndelag Health Surveys 2006–2008 and 2017–2019. J. Headache Pain 2020, 21, 67. [Google Scholar] [CrossRef]
- Park, C.G.; Lee, S.H.; Chu, M.K. No Change in Interictal C-Reactive Protein Levels in Individuals with Episodic and Chronic Migraine: A Case-Control Study and Literature Review. Front. Neurol. 2022, 13, 1021065. [Google Scholar] [CrossRef]
- Hagen, K.; Stovner, L.J.; Nilsen, K.B.; Kristoffersen, E.S.; Winsvold, B.S. The Impact of C-Reactive Protein Levels on Headache Frequency in the HUNT Study 2006–2008. BMC Neurol. 2019, 19, 229. [Google Scholar] [CrossRef] [PubMed]
- Cyprien, F.; Courtet, P.; Maller, J.; Meslin, C.; Ritchie, K.; Ancelin, M.-L.; Artero, S. Increased Serum C-Reactive Protein and Corpus Callosum Alterations in Older Adults. Aging. Dis. 2019, 10, 463–469. [Google Scholar] [CrossRef] [PubMed]
- Arfanakis, K.; Fleischman, D.A.; Grisot, G.; Barth, C.M.; Varentsova, A.; Morris, M.C.; Barnes, L.L.; Bennett, D.A. Systemic Inflammation in Non-Demented Elderly Human Subjects: Brain Microstructure and Cognition. PLoS ONE 2013, 8, e73107. [Google Scholar] [CrossRef]
- Fan, Y.; McGowan, S.; Rubeiz, H.; Wollmann, R.; Javed, A.; Mastrianni, J. Acute Encephalopathy as the Initial Manifestation of CADASIL. Neurol. Clin. Pract. 2012, 2, 359–361. [Google Scholar] [CrossRef] [PubMed]
- Cilla, A.; Arnaez, J.; Benavente-Fernández, I.; Ochoa, C.; Vega, C.; Lubián-López, S.; Garcia-Alix, A. Effect of Hypothermia and Severity of Hypoxic-Ischemic Encephalopathy in the Levels of C-Reactive Protein during the First 120 Hours of Life. Am. J. Perinatol. 2020, 37, 722–730. [Google Scholar] [CrossRef]
- Sumlivaia, O.N.; Vorob’eva, N.N.; Karakulova, I.V. Diagnostic value of determination of the blood concentrations of serotonin and high-sensitivity C-reactive protein in patients with tick-borne encephalitis. Med. Parazitol. 2014, 25–29. [Google Scholar]
- Gibson, A.E.; Buchholz, A.C.; Martin Ginis, K.A. SHAPE-SCI Research Group C-Reactive Protein in Adults with Chronic Spinal Cord Injury: Increased Chronic Inflammation in Tetraplegia vs Paraplegia. Spinal Cord. 2008, 46, 616–621. [Google Scholar] [CrossRef] [PubMed]
- Estrores, I.M.; Harrington, A.; Banovac, K. C-Reactive Protein and Erythrocyte Sedimentation Rate in Patients with Heterotopic Ossification after Spinal Cord Injury. J. Spinal Cord Med. 2004, 27, 434–437. [Google Scholar] [CrossRef] [PubMed]
- Kharel, S.; Ojha, R.; Preethish-Kumar, V.; Bhagat, R. C-Reactive Protein Levels in Patients with Amyotrophic Lateral Sclerosis: A Systematic Review. Brain Behav. 2022, 12, e2532. [Google Scholar] [CrossRef]
- Lunetta, C.; Lizio, A.; Maestri, E.; Sansone, V.A.; Mora, G.; Miller, R.G.; Appel, S.H.; Chiò, A. Serum C-Reactive Protein as a Prognostic Biomarker in Amyotrophic Lateral Sclerosis. JAMA Neurol. 2017, 74, 660. [Google Scholar] [CrossRef]
- Zhu, Y.; Li, M.; Zhang, J.; Huang, X. Association Between C-Reactive Protein and Risk of Amyotrophic Lateral Sclerosis: A Mendelian Randomization Study. Front. Genet. 2022, 13, 919031. [Google Scholar] [CrossRef]
- Hu, Y.; Zhang, Y.; Zhang, H.; Gao, S.; Wang, L.; Wang, T.; Han, Z.; International Genomics of Alzheimer’s Project (IGAP); Liu, G. Mendelian Randomization Highlights Causal Association between Genetically Increased C-reactive Protein Levels and Reduced Alzheimer’s Disease Risk. Alzheimer’s Dement. 2022, 18, 2003–2006. [Google Scholar] [CrossRef]
- Hegazy, S.H.; Thomassen, J.Q.; Rasmussen, I.J.; Nordestgaard, B.G.; Tybjaerg-Hansen, A.; Frikke-Schmidt, R. C-Reactive Protein Levels and Risk of Dementia-Observational and Genetic Studies of 111,242 Individuals from the General Population. Alzheimer’s Dement. 2022, 18, 2262–2271. [Google Scholar] [CrossRef]
- Zhang, Z.; Wang, M.; Liu, X. C-Reactive Protein and Risk of Alzheimer’s Disease. Neurobiol. Aging. 2022, 109, 259–263. [Google Scholar] [CrossRef]
- Fernandes, A.; Tábuas-Pereira, M.; Duro, D.; Lima, M.; Gens, H.; Santiago, B.; Durães, J.; Almeida, M.R.; Leitão, M.J.; Baldeiras, I.; et al. C-Reactive Protein as a Predictor of Mild Cognitive Impairment Conversion into Alzheimer’s Disease Dementia. Exp. Gerontol. 2020, 138, 111004. [Google Scholar] [CrossRef]
- Hsu, P.-F.; Pan, W.-H.; Yip, B.-S.; Chen, R.C.-Y.; Cheng, H.-M.; Chuang, S.-Y. C-Reactive Protein Predicts Incidence of Dementia in an Elderly Asian Community Cohort. J. Am. Med. Dir. Assoc. 2017, 18, 277.e7–277.e11. [Google Scholar] [CrossRef] [PubMed]
- Kravitz, B.A.; Corrada, M.M.; Kawas, C.H. Elevated C-Reactive Protein Levels Are Associated with Prevalent Dementia in the Oldest-Old. Alzheimer’s Dement. 2009, 5, 318–323. [Google Scholar] [CrossRef] [PubMed]
- Qiu, X.; Xiao, Y.; Wu, J.; Gan, L.; Huang, Y.; Wang, J. C-Reactive Protein and Risk of Parkinson’s Disease: A Systematic Review and Meta-Analysis. Front. Neurol. 2019, 10, 384. [Google Scholar] [CrossRef] [PubMed]
- Umemura, A.; Oeda, T.; Yamamoto, K.; Tomita, S.; Kohsaka, M.; Park, K.; Sugiyama, H.; Sawada, H. Baseline Plasma C-Reactive Protein Concentrations and Motor Prognosis in Parkinson Disease. PLoS ONE 2015, 10, e0136722. [Google Scholar] [CrossRef]
- Sawada, H.; Oeda, T.; Umemura, A.; Tomita, S.; Kohsaka, M.; Park, K.; Yamamoto, K.; Sugiyama, H. Baseline C-Reactive Protein Levels and Life Prognosis in Parkinson Disease. PLoS ONE 2015, 10, e0134118. [Google Scholar] [CrossRef] [PubMed]
- Song, I.-U.; Chung, S.-W.; Kim, J.-S.; Lee, K.-S. Association between High-Sensitivity C-Reactive Protein and Risk of Early Idiopathic Parkinson’s Disease. Neurol. Sci. 2011, 32, 31–34. [Google Scholar] [CrossRef] [PubMed]
- King, E.; Thomas, A. Systemic Inflammation in Lewy Body Diseases: A Systematic Review. Alzheimer. Dis. Assoc. Disord. 2017, 31, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Hassin-Baer, S.; Cohen, O.S.; Vakil, E.; Molshazki, N.; Sela, B.-A.; Nitsan, Z.; Chapman, J.; Tanne, D. Is C-Reactive Protein Level a Marker of Advanced Motor and Neuropsychiatric Complications in Parkinson’s Disease? J. Neural Transm. 2011, 118, 539–543. [Google Scholar] [CrossRef]
- Song, I.-U.; Kim, J.-S.; Chung, S.-W.; Lee, K.-S. Is There an Association between the Level of High-Sensitivity C-Reactive Protein and Idiopathic Parkinson’s Disease? A Comparison of Parkinson’s Disease Patients, Disease Controls and Healthy Individuals. Eur. Neurol. 2009, 62, 99–104. [Google Scholar] [CrossRef]
- Liu, J.; Yin, W.; Zhou, C.; Zhu, Y.; Gu, M.; Liu, B.; Ren, H.; Yang, X. Association between Levels of High-Sensitivity C-Reactive Protein in Plasma and Freezing of Gait in Parkinson’s Disease. Aging Clin. Exp. Res. 2022, 34, 1865–1872. [Google Scholar] [CrossRef] [PubMed]
- Zhong, R.; Chen, Q.; Li, M.; Zhang, X.; Lin, W. Elevated Blood C-Reactive Protein Levels in Patients with Epilepsy: A Systematic Review and Meta-Analysis. Front. Neurol. 2019, 10, 974. [Google Scholar] [CrossRef] [PubMed]
- Tao, H.; Gong, Y.; Yu, Q.; Zhou, H.; Liu, Y. Elevated Serum Matrix Metalloproteinase-9, Interleukin-6, Hypersensitive C-Reactive Protein, and Homocysteine Levels in Patients with Epilepsy. J. Interferon Cytokine Res. 2020, 40, 152–158. [Google Scholar] [CrossRef]
- Ishikawa, N.; Kobayashi, Y.; Fujii, Y.; Kobayashi, M. Increased Interleukin-6 and High-Sensitivity C-Reactive Protein Levels in Pediatric Epilepsy Patients with Frequent, Refractory Generalized Motor Seizures. Seizure 2015, 25, 136–140. [Google Scholar] [CrossRef] [PubMed]
- Uher, T.; Bob, P. Neuropathic Pain, Depressive Symptoms, and C-Reactive Protein in Sciatica Patients. Int. J. Neurosci. 2013, 123, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Stürmer, T.; Raum, E.; Buchner, M.; Gebhardt, K.; Schiltenwolf, M.; Richter, W.; Brenner, H. Pain and High Sensitivity C Reactive Protein in Patients with Chronic Low Back Pain and Acute Sciatic Pain. Ann. Rheum. Dis. 2005, 64, 921–925. [Google Scholar] [CrossRef] [PubMed]
- Trotti, L.M.; Rye, D.B.; De Staercke, C.; Hooper, W.C.; Quyyumi, A.; Bliwise, D.L. Elevated C-Reactive Protein Is Associated with Severe Periodic Leg Movements of Sleep in Patients with Restless Legs Syndrome. Brain Behav. Immun. 2012, 26, 1239–1243. [Google Scholar] [CrossRef]
- Jiménez-Jiménez, F.J.; Alonso-Navarro, H.; García-Martín, E.; Agúndez, J.A.G. Inflammatory Factors and Restless Legs Syndrome: A Systematic Review and Meta-Analysis. Sleep Med. Rev. 2022, 68, 101744. [Google Scholar] [CrossRef] [PubMed]
- Dowsett, J.; Didriksen, M.; von Stemann, J.H.; Larsen, M.H.; Thørner, L.W.; Sørensen, E.; Erikstrup, C.; Pedersen, O.B.; Hansen, M.B.; Eugen-Olsen, J.; et al. Chronic Inflammation Markers and Cytokine-Specific Autoantibodies in Danish Blood Donors with Restless Legs Syndrome. Sci. Rep. 2022, 12, 1672. [Google Scholar] [CrossRef]
- Dos Santos, A.R.R.; De Albuquerque, R.R.; Doriqui, M.J.R.; Costa, G.C.; Dos Santos, A.P.S.A. Biochemical and Hematological Analysis in Acute Intermittent Porphyria (AIP): A Case Report. Acad. Bras. Cienc. 2013, 85, 1207–1214. [Google Scholar] [CrossRef]
- Yin, F.; Wang, H.; Liu, Z.; Gao, J. Association between Peripheral Blood Levels of C-Reactive Protein and Autism Spectrum Disorder in Children: A Systematic Review and Meta-Analysis. Brain Behav. Immun. 2020, 88, 432–441. [Google Scholar] [CrossRef]
- Shao, S.; Wang, J.; Huang, K.; Wang, S.; Liu, H.; Wan, S.; Yan, S.; Hao, J.; Zhu, P.; Tao, F. Prenatal Pregnancy-Related Anxiety Predicts Boys’ ADHD Symptoms via Placental C-Reactive Protein. Psychoneuroendocrinology 2020, 120, 104797. [Google Scholar] [CrossRef]
- Sanjari Moghaddam, H.; Valitabar, Z.; Ashraf-Ganjouei, A.; Mojtahed Zadeh, M.; Ghazi Sherbaf, F.; Aarabi, M.H. Cerebrospinal Fluid C-Reactive Protein in Parkinson’s Disease: Associations with Motor and Non-Motor Symptoms. Neuromolecular. Med. 2018, 20, 376–385. [Google Scholar] [CrossRef]
- Ahmed, M.A.; Askar, G.A.; Farghaly, H.S.; Ahmed, A.O.; Kamal, D.T.; Ahmed, S.S.; Mohamad, I.L. Accuracy of Cerebrospinal Fluid C-Reactive Protein and Multiplex Polymerase Chain Reaction and Serum Procalcitonin in Diagnosis of Bacterial and Viral Meningitis in Children. Acta Neurol. Taiwan 2022, 31, 61–71. [Google Scholar]
- Kalchev, Y.; Petkova, T.; Raycheva, R.; Argirova, P.; Stoycheva, M.; Murdjeva, M. Combined Testing of Cerebrospinal Fluid IL-12 (P40) and Serum C-Reactive Protein as a Possible Discriminator of Acute Bacterial Neuroinfections. Cytokine 2021, 140, 155423. [Google Scholar] [CrossRef] [PubMed]
- Coccaro, E.F.; Lee, R.; Coussons-Read, M. Cerebrospinal Fluid and Plasma C-Reactive Protein and Aggression in Personality-Disordered Subjects: A Pilot Study. J. Neural Transm. 2015, 122, 321–326. [Google Scholar] [CrossRef] [PubMed]
- Shen, X.-N.; Niu, L.-D.; Wang, Y.-J.; Cao, X.-P.; Liu, Q.; Tan, L.; Zhang, C.; Yu, J.-T. Inflammatory Markers in Alzheimer’s Disease and Mild Cognitive Impairment: A Meta-Analysis and Systematic Review of 170 Studies. J. Neurol. Neurosurg. Psychiatry 2019, 90, 590–598. [Google Scholar] [CrossRef]
- Milligan, C.; Atassi, N.; Babu, S.; Barohn, R.J.; Caress, J.B.; Cudkowicz, M.E.; Evora, A.; Hawkins, G.A.; Wosiski-Kuhn, M.; Macklin, E.A.; et al. Tocilizumab Is Safe and Tolerable and Reduces C-Reactive Protein Concentrations in the Plasma and Cerebrospinal Fluid of ALS Patients. Muscle Nerve 2021, 64, 309–320. [Google Scholar] [CrossRef] [PubMed]
- Neerland, B.E.; Hall, R.J.; Seljeflot, I.; Frihagen, F.; MacLullich, A.M.J.; Raeder, J.; Wyller, T.B.; Watne, L.O. Associations between Delirium and Preoperative Cerebrospinal Fluid C-Reactive Protein, Interleukin-6, and Interleukin-6 Receptor in Individuals with Acute Hip Fracture. J. Am. Geriatr. Soc. 2016, 64, 1456–1463. [Google Scholar] [CrossRef] [PubMed]
- Is, M.; Coskun, A.; Sanus, G.Z.; Tanriverdi, T.; Kafadar, A.M.; Hanimoglu, H.; Tanriover, N.; Gezen, F.; Uzan, M. High-Sensitivity C-Reactive Protein Levels in Cerebrospinal Fluid and Serum in Severe Head Injury: Relationship to Tumor Necrosis Factor-Alpha and Interleukin-6. J. Clin. Neurosci. 2007, 14, 1163–1171. [Google Scholar] [CrossRef] [PubMed]
- Fountas, K.N.; Tasiou, A.; Kapsalaki, E.Z.; Paterakis, K.N.; Grigorian, A.A.; Lee, G.P.; Robinson, J.S. Serum and Cerebrospinal Fluid C-Reactive Protein Levels as Predictors of Vasospasm in Aneurysmal Subarachnoid Hemorrhage. Clinical Article. Neurosurg. Focus 2009, 26, E22. [Google Scholar] [CrossRef]
- Abe, Y.; Harada, M.; Tada, K.; Yamaji, K.; Tamura, N. Elevated Cerebrospinal Fluid Levels of Total Protein in Patients with Secondary Central Nervous System Vasculitis and Giant Cell Arteritis. Mod. Rheumatol. 2020, 30, 1033–1038. [Google Scholar] [CrossRef] [PubMed]
- Noureldein, M.; Mardare, R.; Pickard, J.; Shing, H.L.; Eisenhut, M. Cerebrospinal Fluid Protein and Glucose Levels in Neonates with a Systemic Inflammatory Response without Meningitis. Fluids Barriers CNS 2018, 15, 8. [Google Scholar] [CrossRef]
- Chen, W.; Tan, Y.; Ge, Y.; Chen, Y.; Liu, X. The Effects of Levetiracetam on Cerebrospinal Fluid and Plasma NPY and GAL, and on the Components of Stress Response System, Hs-CRP, and S100B Protein in Serum of Patients with Refractory Epilepsy. Cell Biochem. Biophys. 2015, 73, 489–494. [Google Scholar] [CrossRef] [PubMed]
- Ligthart, S.; Vaez, A.; Võsa, U.; Stathopoulou, M.G.; de Vries, P.S.; Prins, B.P.; der Most, P.J.V.; Tanaka, T.; Naderi, E.; Rose, L.M.; et al. Genome Analyses of >200,000 Individuals Identify 58 Loci for Chronic Inflammation and Highlight Pathways That Link Inflammation and Complex Disorders. Am. J. Hum. Genet. 2018, 103, 691–706. [Google Scholar] [CrossRef]
- Orsolini, L.; Sarchione, F.; Vellante, F.; Fornaro, M.; Matarazzo, I.; Martinotti, G.; Valchera, A.; Di Nicola, M.; Carano, A.; Di Giannantonio, M.; et al. Protein-C Reactive as Biomarker Predictor of Schizophrenia Phases of Illness? A Systematic Review. Curr. Neuropharmacol. 2018, 16, 583–606. [Google Scholar] [CrossRef]
- Boozalis, T.; Teixeira, A.L.; Cho, R.Y.-J.; Okusaga, O. C-Reactive Protein Correlates with Negative Symptoms in Patients with Schizophrenia. Front. Public Health 2017, 5, 360. [Google Scholar] [CrossRef]
- Fond, G.; Lançon, C.; Auquier, P.; Boyer, L. C-Reactive Protein as a Peripheral Biomarker in Schizophrenia. An Updated Systematic Review. Front. Psychiatry 2018, 9, 392. [Google Scholar] [CrossRef] [PubMed]
- Canetta, S.; Sourander, A.; Surcel, H.-M.; Hinkka-Yli-Salomäki, S.; Leiviskä, J.; Kellendonk, C.; McKeague, I.W.; Brown, A.S. Elevated Maternal C-Reactive Protein and Increased Risk of Schizophrenia in a National Birth Cohort. Am. J. Psychiatry 2014, 171, 960–968. [Google Scholar] [CrossRef] [PubMed]
- Zou, Y.; Grigorian, A.; Karthikeyan, S.; Goldstein, B.I. Elevated C-Reactive Protein among Symptomatic Youth with Bipolar Disorder. J. Psychopharmacol. 2022, 36, 645–652. [Google Scholar] [CrossRef] [PubMed]
- Whitney, M.S.; Scott, S.L.; Perez, J.A.; Barnes, S.; McVoy, M.K. Elevation of C-Reactive Protein in Adolescent Bipolar Disorder vs. Anxiety Disorders. J. Psychiatr. Res. 2022, 156, 308–317. [Google Scholar] [CrossRef]
- Caldirola, D.; Daccò, S.; Cuniberti, F.; Grassi, M.; Lorusso, S.; Diaferia, G.; Perna, G. Elevated C-Reactive Protein Levels across Diagnoses: The First Comparison among Inpatients with Major Depressive Disorder, Bipolar Disorder, or Obsessive-Compulsive Disorder. J. Psychosom. Res. 2021, 150, 110604. [Google Scholar] [CrossRef]
- Chang, H.H.; Wang, T.-Y.; Lee, I.H.; Lee, S.-Y.; Chen, K.C.; Huang, S.-Y.; Yang, Y.K.; Lu, R.-B.; Chen, P.S. C-Reactive Protein: A Differential Biomarker for Major Depressive Disorder and Bipolar II Disorder. World J. Biol. Psychiatry 2017, 18, 63–70. [Google Scholar] [CrossRef]
- Abshad, M.; Das, B.; Kumar, M.; Dey, P.; Kshitiz, K.K. Role of High-Sensitivity C-Reactive Protein as a Biomarker and Endophenotype in Mania. Prim. Care Companion CNS Disord. 2022, 24, 21m03194. [Google Scholar] [CrossRef]
- Dickerson, F.; Stallings, C.; Origoni, A.; Boronow, J.; Yolken, R. Elevated Serum Levels of C-Reactive Protein Are Associated with Mania Symptoms in Outpatients with Bipolar Disorder. Prog. Neuropsychopharmacol. Biol. Psychiatry 2007, 31, 952–955. [Google Scholar] [CrossRef]
- Gorgulu, Y.; Uluturk, M.K.; Palabiyik, O. Comparison of Serum BDNF, IL-1β, IL-6, TNF-α, CRP and Leucocyte Levels in Unipolar Mania and Bipolar Disorder. Acta Neuropsychiatr. 2021, 33, 317–322. [Google Scholar] [CrossRef]
- Dimitrov, D.H.; Lee, S.; Yantis, J.; Honaker, C.; Braida, N.; Walss-Bass, C. Elevated Serum Levels of High-Sensitivity C-Reactive Proteins Are Associated with Severe Delusional Symptoms in a Subgroup of Patients with Schizophrenia. J. Clin. Psychiatry 2016, 77, 6373. [Google Scholar] [CrossRef]
- Sawada, H.; Oeda, T.; Umemura, A.; Tomita, S.; Hayashi, R.; Kohsaka, M.; Yamamoto, K.; Sudoh, S.; Sugiyama, H. Subclinical Elevation of Plasma C-Reactive Protein and Illusions/Hallucinations in Subjects with Parkinson’s Disease: Case-Control Study. PLoS ONE 2014, 9, e85886. [Google Scholar] [CrossRef]
- Park, S.; Miller, B.J. Meta-Analysis of Cytokine and C-Reactive Protein Levels in High-Risk Psychosis. Schizophr. Res. 2020, 226, 5–12. [Google Scholar] [CrossRef] [PubMed]
- Johnsen, E.; Fathian, F.; Kroken, R.A.; Steen, V.M.; Jørgensen, H.A.; Gjestad, R.; Løberg, E.-M. The Serum Level of C-Reactive Protein (CRP) Is Associated with Cognitive Performance in Acute Phase Psychosis. BMC Psychiatry 2016, 16, 60. [Google Scholar] [CrossRef] [PubMed]
- Courtet, P.; Jaussent, I.; Genty, C.; Dupuy, A.M.; Guillaume, S.; Ducasse, D.; Olié, E. Increased CRP Levels May Be a Trait Marker of Suicidal Attempt. Eur. Neuropsychopharmacol. 2015, 25, 1824–1831. [Google Scholar] [CrossRef] [PubMed]
- Miola, A.; Dal Porto, V.; Tadmor, T.; Croatto, G.; Scocco, P.; Manchia, M.; Carvalho, A.F.; Maes, M.; Vieta, E.; Sambataro, F.; et al. Increased C-Reactive Protein Concentration and Suicidal Behavior in People with Psychiatric Disorders: A Systematic Review and Meta-Analysis. Acta Psychiatr. Scand. 2021, 144, 537–552. [Google Scholar] [CrossRef] [PubMed]
- Kennedy, E.; Niedzwiedz, C.L. The Association of Anxiety and Stress-Related Disorders with C-Reactive Protein (CRP) within UK Biobank. Brain Behav. Immun. Health 2022, 19, 100410. [Google Scholar] [CrossRef]
- Chen, Y.; Meng, P.; Cheng, S.; Jia, Y.; Wen, Y.; Yang, X.; Yao, Y.; Pan, C.; Li, C.; Zhang, H.; et al. Assessing the Effect of Interaction between C-Reactive Protein and Gut Microbiome on the Risks of Anxiety and Depression. Mol. Brain 2021, 14, 133. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Ely, B.A.; Simkovic, S.; Alonso, C.M.; Gabbay, V. Lack of Associations Between C-Reactive Protein and Mood and Anxiety Symptoms in Adolescents. J. Child. Adolesc. Psychopharmacol. 2021, 31, 404–410. [Google Scholar] [CrossRef] [PubMed]
- Persons, J.E.; Pierce, G.L.; Fiedorowicz, J.G. Anxiety, C-Reactive Protein, and Obesity in NHANES 1999–2004. Heliyon 2019, 5, e02267. [Google Scholar] [CrossRef]
- Naudé, P.J.W.; Roest, A.M.; Stein, D.J.; de Jonge, P.; Doornbos, B. Anxiety Disorders and CRP in a Population Cohort Study with 54,326 Participants: The LifeLines Study. World J. Biol. Psychiatry 2018, 19, 461–470. [Google Scholar] [CrossRef]
- Turna, J.; Grosman Kaplan, K.; Anglin, R.; Patterson, B.; Soreni, N.; Bercik, P.; Surette, M.G.; Van Ameringen, M. The Gut Microbiome and Inflammation in Obsessive-Compulsive Disorder Patients Compared to Age- and Sex-Matched Controls: A Pilot Study. Acta Psychiatr. Scand. 2020, 142, 337–347. [Google Scholar] [CrossRef]
- Molnar, D.S.; Moore, J.; O’Leary, D.D.; MacNeil, A.J.; Wade, T.J. Perfectionistic Cognitions, Interleukin-6, and C-Reactive Protein: A Test of the Perfectionism Diathesis Stress Model. Brain Behav. Immun. Health 2021, 13, 100211. [Google Scholar] [CrossRef]
- Speer, K.; Upton, D.; Semple, S.; McKune, A. Systemic Low-Grade Inflammation in Post-Traumatic Stress Disorder: A Systematic Review. J. Inflamm. Res. 2018, 11, 111–121. [Google Scholar] [CrossRef]
- Friend, S.F.; Nachnani, R.; Powell, S.B.; Risbrough, V.B. C-Reactive Protein: Marker of Risk for Post-Traumatic Stress Disorder and Its Potential for a Mechanistic Role in Trauma Response and Recovery. Eur. J. Neurosci. 2022, 55, 2297–2310. [Google Scholar] [CrossRef]
- Laugsand, L.E.; Vatten, L.J.; Bjørngaard, J.H.; Hveem, K.; Janszky, I. Insomnia and High-Sensitivity C-Reactive Protein: The HUNT Study, Norway. Psychosom. Med. 2012, 74, 543–553. [Google Scholar] [CrossRef] [PubMed]
- Slavish, D.C.; Graham-Engeland, J.E.; Engeland, C.G.; Taylor, D.J.; Buxton, O.M. Insomnia Symptoms Are Associated with Elevated C-Reactive Protein in Young Adults. Psychol. Health 2018, 33, 1396–1415. [Google Scholar] [CrossRef]
- Li, T.; Geng, H.; Wang, Y.; Wu, Z.; Yang, S.; Hu, Y.-Q. Causal Association of Thyroid Signaling with C-Reactive Protein: A Bidirectional Mendelian Randomization. Comput. Math. Methods Med. 2022, 2022, 8954606. [Google Scholar] [CrossRef] [PubMed]
- Peixoto de Miranda, É.J.F.; Bittencourt, M.S.; Santos, I.S.; Lotufo, P.A.; Benseñor, I.M. Thyroid Function and High-Sensitivity C-Reactive Protein in Cross-Sectional Results from the Brazilian Longitudinal Study of Adult Health (ELSA-Brasil): Effect of Adiposity and Insulin Resistance. Eur. Thyroid. J. 2016, 5, 240–246. [Google Scholar] [CrossRef]
- Komiya, I.; Tomoyose, T.; Yagi, N.; Ouchi, G.; Wakugami, T. A Case of Thyrotoxicosis-Induced Anemia in a Patient with Painless Thyroiditis. Thyroid. Res. 2021, 14, 9. [Google Scholar] [CrossRef] [PubMed]
- Tang, C.; Dong, Y.; Lu, L.; Zhang, N. C-Reactive Protein and Thyroid-Stimulating Hormone Levels as Risk Factors for Hypothyroidism in Patients with Subacute Thyroiditis. Endocr. Connect 2021, 10, 965–972. [Google Scholar] [CrossRef]
- Czarnywojtek, A.; Owecki, M.; Zgorzalewicz-Stachowiak, M.; Woliński, K.; Szczepanek-Parulska, E.; Budny, B.; Florek, E.; Waligórska-Stachura, J.; Miechowicz, I.; Bączyk, M.; et al. The Role of Serum C-Reactive Protein Measured by High-Sensitive Method in Thyroid Disease. Arch. Immunol. Ther. Exp. 2014, 62, 501–509. [Google Scholar] [CrossRef]
- Yu, Y.-T.; Ho, C.-T.; Hsu, H.-S.; Li, C.-I.; Davidson, L.E.; Liu, C.-S.; Li, T.-C.; Shih, C.-M.; Lin, C.-C.; Lin, W.-Y. Subclinical Hypothyroidism Is Associated with Elevated High-Sensitive C-Reactive Protein among Adult Taiwanese. Endocrine 2013, 44, 716–722. [Google Scholar] [CrossRef]
- Christ-Crain, M.; Meier, C.; Guglielmetti, M.; Huber, P.R.; Riesen, W.; Staub, J.J.; Müller, B. Elevated C-Reactive Protein and Homocysteine Values: Cardiovascular Risk Factors in Hypothyroidism? A Cross-Sectional and a Double-Blind, Placebo-Controlled Trial. Atherosclerosis 2003, 166, 379–386. [Google Scholar] [CrossRef]
- Kar, F.; KïRaz, Z.K.; Kocatürk, E.; Uslu, S. The Level of Serum C-Reactive Protein and Neutrophil Lymphocyte Ratio According to Thyroid Function Status. Clin. Exp. Health Sci. 2020, 10, 142–147. [Google Scholar] [CrossRef]
- Destek, S.; Benturk, B.; Yapalak, Y.; Ozer, O.F. Clinical Significance of Erythrocyte Sedimentation Rate, Leukocyte, Fibrinogen, C-Reactive Protein, and Pentraxin 3 Values in Thyroid Nodules. Sisli Etfal. Hast. Tip. Bul. 2022, 56, 270–275. [Google Scholar] [CrossRef]
- Koliakos, E.; Papazarkadas, X.; Sleiman, M.-J.; Rotas, I.; Christodoulou, M. Wandering Spleen Volvulus: A Case Report and Literature Review of This Diagnostic Challenge. Am. J. Case Rep. 2020, 21, e925301-1–e925301-4. [Google Scholar] [CrossRef]
- Iñiguez, A.; Butte, J.M.; Zuñiga, J.M.; Torres, J.; Llanos, O. Splenic abscesses. Report of seven cases. Rev. Med. Chil. 2008, 136, 38–43. [Google Scholar]
- Martín-Jiménez, A.J.; Mera-Gallardo, O.; García-Gil, D. Splenic Vein Thrombosis: Rare Cause of Abdominal Pain. Emerg. Med. J. 2020, 37, 30–48. [Google Scholar] [CrossRef]
- Spaziani, E.; Di Filippo, A.; Picchio, M.; Pietricola, G.; Ceci, F.; Ottaviani, M.; Martellucci, A.; Pattaro, G.; De Angelis, F.; Parisella, F.; et al. A rare cause of acute abdomen: Splenic infarction. Case report and review of the literature. G. Chir. 2010, 31, 397–399. [Google Scholar]
- Hakoshima, M.; Kitakaze, K.; Adachi, H.; Katsuyama, H.; Yanai, H. Clinical, Hematological, Biochemical and Radiological Characteristics for Patients with Splenic Infarction: Case Series with Literature Review. J. Clin. Med. Res. 2023, 15, 38–50. [Google Scholar] [CrossRef] [PubMed]
- Schott, A.; Husak, R.; Kempf, M. Splenic cysts as an incidental finding—What’s next? Dtsch. Med. Wochenschr. 2014, 139, 2132–2135. [Google Scholar] [CrossRef] [PubMed]
- Szalai, A.J. C-Reactive Protein (CRP) and Autoimmune Disease: Facts and Conjectures. Clin. Dev. Immunol. 2004, 11, 221–226. [Google Scholar] [CrossRef]
- Clos, T.W.D. C-Reactive Protein as a Regulator of Autoimmunity and inflammation. Arthritis Rheum. 2003, 48, 1475–1477. [Google Scholar] [CrossRef] [PubMed]
- López, L.; Arai, K.; Giménez, E.; Jiménez, M.; Pascuzo, C.; Rodríguez-Bonfante, C.; Bonfante-Cabarcas, R. C-reactive protein and interleukin-6 serum levels increase as Chagas disease progresses towards cardiac failure. Rev. Esp. Cardiol. 2006, 59, 50–56. [Google Scholar] [CrossRef] [PubMed]
- Da Silva, C.A.; Fattori, A.; Sousa, A.L.; Mazon, S.B.; Alegre, S.M.; Almeida, E.A.; Guariento, M.E. Determining the C-Reactive Protein Level in Patients With Different Clinical Forms of Chagas Disease. Rev. Española Cardiol. (Engl. Ed.) 2010, 63, 1096–1099. [Google Scholar] [CrossRef]
- Chan, F.L.Y.; Lester, S.; Whittle, S.L.; Hill, C.L. The Utility of ESR, CRP and Platelets in the Diagnosis of GCA. BMC Rheumatol. 2019, 3, 14. [Google Scholar] [CrossRef] [PubMed]
- Laria, A.; Zoli, A.; Bocci, M.; Castri, F.; Federico, F.; Ferraccioli, G.F. Systematic Review of the Literature and a Case Report Informing Biopsy-Proven Giant Cell Arteritis (GCA) with Normal C-Reactive Protein. Clin. Rheumatol. 2012, 31, 1389–1393. [Google Scholar] [CrossRef] [PubMed]
- Kasashima, S.; Kawashima, A.; Kasashima, F.; Endo, M.; Matsumoto, Y.; Kawakami, K. Inflammatory Features, Including Symptoms, Increased Serum Interleukin-6, and C-Reactive Protein, in IgG4-Related Vascular Diseases. Heart Vessel. 2018, 33, 1471–1481. [Google Scholar] [CrossRef]
- Korsten, P.; Baier, E.; Hakroush, S.; Tampe, B. C-Reactive Protein Levels Are Associated with Complement C4 Deposits and Interstitial Arteritis in ANCA-Associated Renal Vasculitis. Int. J. Mol. Sci. 2023, 24, 3072. [Google Scholar] [CrossRef]
- Teng, X.; Wang, Y.; Lin, N.; Sun, M.; Wu, J. Evaluation of Serum Procalcitonin and C-Reactive Protein Levels as Biomarkers of Henoch-Schönlein Purpura in Pediatric Patients. Clin. Rheumatol. 2016, 35, 667–671. [Google Scholar] [CrossRef]
- Li, Y.; Chen, Z.; Zhu, S.; Bai, F.; Liu, Y.; Gao, L.; Li, X.; Geng, Y.; Zhang, G. Negative Anti-Neutrophil Cytoplasmic Antibodies and Eosinophilic Granulomatosis with Polyangiitis Accompanied by Cough Variant Asthma: A Case Report. Ann. Palliat. Med. 2021, 10, 112091215. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, H.; Komai, T.; Setoguchi, K.; Shoda, H.; Fujio, K. A Diagnostic Score for Eosinophilic Granulomatosis with Polyangiitis among Eosinophilic Disorders. Allergol. Int. 2023, 72, 316–323. [Google Scholar] [CrossRef]
- Hind, C.R.; Winearls, C.G.; Lockwood, C.M.; Rees, A.J.; Pepys, M.B. Objective Monitoring of Activity in Wegener’s Granulomatosis by Measurement of Serum C-Reactive Protein Concentration. Clin. Nephrol. 1984, 21, 341–345. [Google Scholar] [CrossRef]
- Kälsch, A.-I.; Csernok, E.; Münch, D.; Birck, R.; Yard, B.A.; Gross, W.; Kälsch, T.; Schmitt, W.H. Use of Highly Sensitive C-Reactive Protein for Followup of Wegener’s Granulomatosis. J. Rheumatol. 2010, 37, 2319–2325. [Google Scholar] [CrossRef]
- Huo, J.; Wu, Z.; Jiang, H.; Zhang, H. Multislice Computed Tomography Angiography Imaging Diagnosis of Lower Extremity Arteriosclerosis in Patients with Hypertension and Its Correlation with the Level of High-Sensitivity C-Reactive Protein. Comput. Math. Methods Med. 2022, 2022, 1768208. [Google Scholar] [CrossRef]
- Morita, A.; Nakayama, T.; Doba, N.; Hinohara, S.; Soma, M. Polymorphism of the C-Reactive Protein (CRP) Gene Is Related to Serum CRP Level and Arterial Pulse Wave Velocity in Healthy Elderly Japanese. Hypertens. Res. 2006, 29, 323–331. [Google Scholar] [CrossRef] [PubMed]
- Quinquenel, A.; Maestraggi, Q.; Lecoq-Lafon, C.; Régis, P.d.L.; Delmer, A.; Servettaz, A. Atypical Presentation of Paroxysmal Nocturnal Hemoglobinuria Treated by Eculizumab. Medicine 2017, 96, e6403. [Google Scholar] [CrossRef] [PubMed]
- Krishnaprasadh, D.; Kaminecki, I.; Sechser Perl, A.; Teitelbaum, J. Paroxysmal Nocturnal Hemoglobinuria: Diagnostic Challenges in Pediatric Patient. Case Rep. Pediatr. 2019, 2019, 4930494. [Google Scholar] [CrossRef]
- Freeman, A. Acquired Haemophilia A Presenting at a District General Hospital. BMJ. Case Rep. 2015, 2015, bcr2014208001. [Google Scholar] [CrossRef] [PubMed]
- Mo, L.; Bao, G.C. Acquired Factor VIII Deficiency: Two Case Reports and a Review of Literature. Exp. Hematol. Oncol. 2017, 6, 8. [Google Scholar] [CrossRef]
- Park, N.; Jang, J.S.; Cha, J.H. Acquired Hemophilia A with Gastrointestinal Bleeding. Clin. Endosc. 2019, 53, 90–93. [Google Scholar] [CrossRef]
- Azevedo, F.; Fernandes, H.; Silva, A.; Barbosa, A.; Correia, A.; Alves, R.P. IgA-Mediated Autoimmune Hemolytic Anemia. Eur. J. Intern. Med. 2013, 24, e164. [Google Scholar] [CrossRef]
- Vieira, D.G.; Costa-Carvalho, B.T.; Hix, S.; da Silva, R.; Correia, M.S.G.; Sarni, R.O.S. Higher Cardiovascular Risk in Common Variable Immunodeficiency and X-Linked Agammaglobulinaemia Patients. ANM 2015, 66, 237–241. [Google Scholar] [CrossRef] [PubMed]
- Cummer, E.; Donaldson, B.; Marlowe, E.; Rosenthal, N.S.; Dixon, N.; Harry, O. Autoimmune Myelofibrosis as a Presenting Feature of Childhood-Onset Systemic Lupus Erythematosus: A Case Report with Review of Pediatric Literature. JCR J. Clin. Rheumatol. 2021, 27, S378–S381. [Google Scholar] [CrossRef]
- Pérez-Segura, P.; de Dios, O.; Herrero, L.; Vales-Villamarín, C.; Aragón-Gómez, I.; Gavela-Pérez, T.; Garcés, C.; Soriano-Guillén, L. Children with Type 1 Diabetes Have Elevated High-Sensitivity C-Reactive Protein Compared with a Control Group. BMJ Open Diabetes Res. Care 2020, 8, e001424. [Google Scholar] [CrossRef] [PubMed]
- Chase, H.P.; Cooper, S.; Osberg, I.; Stene, L.C.; Barriga, K.; Norris, J.; Eisenbarth, G.S.; Rewers, M. Elevated C-Reactive Protein Levels in the Development of Type 1 Diabetes. Diabetes 2004, 53, 2569–2573. [Google Scholar] [CrossRef] [PubMed]
- Prado, M.M.; Carrizo, T.; Abregú, A.V.; Meroño, T. Non-HDL-Cholesterol and C-Reactive Protein in Children and Adolescents with Type 1 Diabetes. J. Pediatr. Endocrinol. Metab. 2017, 30, 285–288. [Google Scholar] [CrossRef]
- Ito, A.; Ishida, T.; Tachibana, H.; Arita, M.; Yamazaki, A.; Washio, Y. Utility of Procalcitonin for Differentiating Cryptogenic Organising Pneumonia from Community-Acquired Pneumonia. Clin. Chem. Lab. Med. 2019, 57, 1632–1637. [Google Scholar] [CrossRef] [PubMed]
- Zhang, K.; Li, A.; Zhou, J.; Zhang, C.; Chen, M. Genetic association of circulating C-reactive protein levels with idiopathic pulmonary fibrosis: A two-sample Mendelian randomization study. Respir. Res. 2023, 24, 7. [Google Scholar] [CrossRef]
- Lee, S.H.; Shim, H.S.; Cho, S.H.; Kim, S.Y.; Lee, S.K.; Son, J.Y.; Jung, J.Y.; Kim, E.Y.; Lim, J.E.; Lee, K.J.; et al. Prognostic Factors for Idiopathic Pulmonary Fibrosis: Clinical, Physiologic, Pathologic, and Molecular Aspects. Sarcoidosis Vasc. Diffus. Lung. Dis. 2011, 28, 102–112. [Google Scholar]
- Dellon, E.S.; Gibbs, W.B.; Fritchie, K.J.; Rubinas, T.C.; Wilson, L.A.; Woosley, J.T.; Shaheen, N.J. Clinical, Endoscopic, and Histologic Findings Distinguish Eosinophilic Esophagitis from Gastroesophageal Reflux Disease. Clin. Gastroenterol. Hepatol. 2009, 7, 1305–1313. [Google Scholar] [CrossRef]
- Altun, E.; Yildiz, A.; Cevik, C.; Turan, G. The Role of High Sensitive C-Reactive Protein and Histopathological Evaluation in Chronic Gastritis Patients with or without Helicobacter Pylori Infection. Acta Cir. Bras. 2019, 34, e201900310. [Google Scholar] [CrossRef]
- Morii, K.; Nagano, Y.; Yamamoto, T.; Nakamura, S.; Okushin, H. Increasing Incidence of Elderly-Onset Autoimmune Hepatitis: Influence of Immunosenescence. Geriatr. Gerontol. Int. 2017, 17, 1722–1728. [Google Scholar] [CrossRef]
- Ertem, E.; Ertem, İ.S.; Binicier, Ö.B. A Rare Case of Autoimmune Hepatitis Presented with Acute Onset of High Fever. Int. J. Infect. Dis. 2014, 21, 152. [Google Scholar] [CrossRef]
- Ito, T.; Ikeura, T.; Notohara, K.; Masuda, M.; Nakamaru, K.; Nakayama, S.; Shimatani, M.; Takaoka, M.; Okazaki, K.; Naganuma, M. A Case of Type 2 Autoimmune Pancreatitis with Spontaneous Remission. Clin. J. Gastroenterol. 2023, 16, 297–302. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.; Lee, H.J.; Seo, A.N.; Bae, H.I.; Kwon, H.J.; Cho, C.M.; Lee, S.M.; Choe, B.-H.; Kang, B. Case Report: Development of Type 1 Autoimmune Pancreatitis in an Adolescent with Ulcerative Colitis Mimicking Pancreatic Cancer. Front. Pediatr. 2021, 9, 791840. [Google Scholar] [CrossRef]
- Parsaei, A.; Moradi, S.; Masoumi, M.; Davatchi, F.; Najafi, A.; Kooshki, A.M.; Hajighadery, A.; Akhlaghi, M.; Faezi, T.; Kavosi, H. Predictive Value of Erythrocyte Sedimentation Rate and C-Reactive Protein in Behcet’s Disease Activity and Manifestations: A Cross-Sectional Study. BMC Rheumatol. 2022, 6, 9. [Google Scholar] [CrossRef] [PubMed]
- Kang, E.A.; Park, J.W.; Park, Y.; Park, S.J.; Kim, T.I.; Kim, W.H.; Cho, M.S.; Cheon, J.H. C-Reactive Protein Is Associated with Postoperative Outcomes in Patients with Intestinal Behçet’s Disease. BMC Gastroenterol. 2021, 21, 362. [Google Scholar] [CrossRef] [PubMed]
- Tack, G.J.; van Wanrooij, R.L.J.; Von Blomberg, B.M.E.; Amini, H.; Coupe, V.M.H.; Bonnet, P.; Mulder, C.J.J.; Schreurs, M.W.J. Serum Parameters in the Spectrum of Coeliac Disease: Beyond Standard Antibody Testing—A Cohort Study. BMC Gastroenterol. 2012, 12, 159. [Google Scholar] [CrossRef] [PubMed]
- Moran, C.J.; Kaplan, J.L.; Winter, H.S. Genetic Variation Affects C-Reactive Protein Elevations in Crohn’s Disease. Inflamm. Bowel Dis. 2018, 24, 2048–2052. [Google Scholar] [CrossRef]
- Yang, D.-H.; Yang, S.-K.; Park, S.H.; Lee, H.-S.; Boo, S.-J.; Park, J.-H.; Na, S.Y.; Jung, K.W.; Kim, K.-J.; Ye, B.D.; et al. Usefulness of C-Reactive Protein as a Disease Activity Marker in Crohn’s Disease According to the Location of Disease. Gut Liver 2015, 9, 80–86. [Google Scholar] [CrossRef] [PubMed]
- Sjöwall, C.; Olin, A.I.; Skogh, T.; Wetterö, J.; Mörgelin, M.; Nived, O.; Sturfelt, G.; Bengtsson, A.A. C-Reactive Protein, Immunoglobulin G and Complement Co-Localize in Renal Immune Deposits of Proliferative Lupus Nephritis. Autoimmunity 2013, 46, 205–214. [Google Scholar] [CrossRef]
- Ishida, N.; Higuchi, T.; Miyazu, T.; Tamura, S.; Tani, S.; Yamade, M.; Iwaizumi, M.; Hamaya, Y.; Osawa, S.; Furuta, T.; et al. C-Reactive Protein Is Superior to Fecal Biomarkers for Evaluating Colon-Wide Active Inflammation in Ulcerative Colitis. Sci. Rep. 2021, 11, 12431. [Google Scholar] [CrossRef]
- Gao, Y.; Huo, S.; Sun, M.; Zhang, C.; Wang, J.; Gao, J.; Wang, N.; Lv, Y. Evaluation of Several Immune and Inflammatory Indicators and Their Association with Alopecia Areata. J. Cosmet. Dermatol. 2022, 21, 2995–3001. [Google Scholar] [CrossRef]
- Kalaycı, B.N.; Balta, İ. Evaluation of the Serum C-Reactive Protein-Albumin Ratio and Its Relationship with Disease Severity IN Alopecia Areata: A Prospective Case-Control Study. J. Cosmet. Dermatol. 2022, 21, 7194–7199. [Google Scholar] [CrossRef] [PubMed]
- Georgin-Lavialle, S.; Terrier, B.; Guedon, A.F.; Heiblig, M.; Comont, T.; Lazaro, E.; Lacombe, V.; Terriou, L.; Ardois, S.; Bouaziz, J.-D.; et al. Further Characterization of Clinical and Laboratory Features in VEXAS Syndrome: Large-Scale Analysis of a Multicentre Case Series of 116 French Patients. Br. J. Dermatol. 2022, 186, 564–574. [Google Scholar] [CrossRef] [PubMed]
- Miesbach, W.; Gökpinar, B.; Gilzinger, A.; Claus, D.; Scharrer, I. Predictive Role of Hs-C-Reactive Protein in Patients with Antiphospholipid Syndrome. Immunobiology 2005, 210, 755–760. [Google Scholar] [CrossRef]
- Bećarević, M.; Majkić-Singh, N. High-Sensitivity C-Reactive Protein: Discriminator between Patients with Primary and Secondary Antiphospholipid Syndrome. Clin. Biochem. 2008, 41, 1449–1453. [Google Scholar] [CrossRef] [PubMed]
- Dima, A.; Opris, D.; Jurcut, C.; Baicus, C. Is There Still a Place for Erythrocyte Sedimentation Rate and C-Reactive Protein in Systemic Lupus Erythematosus? Lupus 2016, 25, 1173–1179. [Google Scholar] [CrossRef]
- Biondo, M.I.; Fiorentino, C.; Persechino, S.; Tammaro, A.; Koverech, A.; Bartolazzi, A.; Raffa, S.; Canzoni, M.; Picchianti-Diamanti, A.; Di Rosa, R.; et al. May Bacterial Infections Trigger Bullous Pemphigoid? Case Report and Review of Literature. Microorganisms 2021, 9, 1235. [Google Scholar] [CrossRef]
- Kumar, A.; Sharma, A.; Agarwal, A. CREST Syndrome. Postgrad. Med. J. 2021, 97, 746. [Google Scholar] [CrossRef]
- Wang, H.; Tang, J.; Chen, X.; Li, F.; Luo, J. Lipid Profiles in Untreated Patients with Dermatomyositis. J. Eur. Acad. Dermatol. Venereol. 2013, 27, 175–179. [Google Scholar] [CrossRef]
- Haas, R.H.; Dyck, R.F.; Dubowitz, V.; Pepys, M.B. C-Reactive Protein in Childhood Dermatomyositis. Ann. Rheum. Dis. 1982, 41, 483–485. [Google Scholar] [CrossRef]
- Foss, N.T.; de Oliveira, E.B.; Silva, C.L. Correlation between TNF Production, Increase of Plasma C-Reactive Protein Level and Suppression of T Lymphocyte Response to Concanavalin A during Erythema Nodosum Leprosum. Int. J. Lepr. Other Mycobact. Dis. 1993, 61, 218–226. [Google Scholar]
- Starba, A.; Chowaniec, M.; Wiland, P. Erythema Nodosum—Presentation of Three Cases. Reumatologia 2016, 54, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.M.; Lowes, M.A.; Cserti, C.; Alavi, A. Hemoglobin Levels and Serum C-Reactive Protein in Patients with Moderate to Severe Hidradenitis Suppurativa. J. Cutan. Med. Surg. 2019, 23, 501–506. [Google Scholar] [CrossRef] [PubMed]
- Gibson, R.S.; Porter, M.L.; Kimball, A.B. Erythrocyte Sedimentation Rate, Rather than C-Reactive Protein, May Be the Preferred Biomarker for Hidradenitis Suppurativa. JAAD. Int. 2022, 8, 47–48. [Google Scholar] [CrossRef] [PubMed]
- Sahin, M.; Bilgili, S.G.; Simsek, H.; Akdag, S.; Akyol, A.; Gumrukcuoglu, H.A.; Yaman, M.; Bayram, Y.; Karadag, A.S. Increased P-Wave Dispersion in Patients with Newly Diagnosed Lichen Planus. Clinics 2013, 68, 846–850. [Google Scholar] [CrossRef]
- Li, X.; Wang, Z. Mechanisms of Reactive Oxygen Species in Oral Lichen Planus: A Literature Review. Eur. J. Inflamm. 2022, 20, 1721727X2211043. [Google Scholar] [CrossRef]
- Farshchian, M.; Ansar, A.; Sobhan, M.; Hoseinpoor, V. C-Reactive Protein Serum Level in Patients with Psoriasis before and after Treatment with Narrow-Band Ultraviolet B. Bras. Dermatol. 2016, 91, 580–583. [Google Scholar] [CrossRef] [PubMed]
- Vadakayil, A.R.; Dandekeri, S.; Kambil, S.M.; Ali, N.M. Role of C-Reactive Protein as a Marker of Disease Severity and Cardiovascular Risk in Patients with Psoriasis. Indian Dermatol. Online J. 2015, 6, 322. [Google Scholar] [CrossRef]
- Ogdie, A.; Tillett, W.; Booth, N.; Howell, O.; Schubert, A.; Peterson, S.; Chakravarty, S.D.; Coates, L.C. Usage of C-Reactive Protein Testing in the Diagnosis and Monitoring of Psoriatic Arthritis (PsA): Results from a Real-World Survey in the USA and Europe. Rheumatol. Ther. 2022, 9, 285–293. [Google Scholar] [CrossRef]
- Namazi, M.R.; Nozari, F.; Ghoreyshi, H. Serum Levels of Hypersensitive-C-Reactive Protein in Vitiligo. Indian Dermatol. Online J. 2018, 9, 53–54. [Google Scholar] [CrossRef]
- Ruof, J.; Stucki, G. Validity Aspects of Erythrocyte Sedimentation Rate and C-Reactive Protein in Ankylosing Spondylitis: A Literature Review. J. Rheumatol. 1999, 26, 966–970. [Google Scholar]
- Su, J.; Cui, L.; Yang, W.; Shi, H.; Jin, C.; Shu, R.; Li, H.; Zeng, X.; Wu, S.; Gao, X. Baseline High-Sensitivity C-Reactive Protein Predicts the Risk of Incident Ankylosing Spondylitis: Results of a Community-Based Prospective Study. PLoS ONE 2019, 14, e0211946. [Google Scholar] [CrossRef]
- Sundström, B.; Ljung, L.; Wållberg-Jonsson, S. Exercise Habits and C-Reactive Protein May Predict Development of Spinal Immobility in Patients with Ankylosing Spondylitis. Clin. Rheumatol. 2018, 37, 2881–2885. [Google Scholar] [CrossRef] [PubMed]
- Baraliakos, X.; Szumski, A.; Koenig, A.S.; Jones, H. The Role of C-Reactive Protein as a Predictor of Treatment Response in Patients with Ankylosing Spondylitis. Semin. Arthritis Rheum. 2019, 48, 997–1004. [Google Scholar] [CrossRef]
- Claushuis, T.A.M.; de Vries, M.K.; van der Weijden, M.A.C.; Visman, I.M.; Nurmohamed, M.T.; Twisk, J.W.R.; Van der Horst-Bruinsma, I.E.; Crusius, J.B.A. C-Reactive Protein Polymorphisms Influence Serum CRP-Levels Independent of Disease Activity in Ankylosing Spondylitis. Clin. Exp. Rheumatol. 2015, 33, 159–165. [Google Scholar] [PubMed]
- Blackmond, N.; Kanke, J.; Brown, K.; Weitzman, R. Eosinophilic Fasciitis: A Rare and Challenging Diagnosis in a Free Clinic Setting. Cureus 2022, 14, e25668. [Google Scholar] [CrossRef] [PubMed]
- Coimbra, T.M.; dos Santos, J.B.; Shinkado, Y.R.; Delicato, G.; Arimura, A.M.; de Paiva, E.F.; Lichtenstein, A. Eosinophilic fasciitis: Clinical signs leading to diagnosis. AIM Clin. Cases 2022, 1, e220237. [Google Scholar] [CrossRef]
- Miossi, R.; de Souza, F.H.C.; Shinjo, S.K. Could C-Reactive Protein and Erythrocyte Sedimentation Rate Support Monitoring of Dermatomyositis and Polymyositis Activity? Med. Express 2017, 4, M170205. [Google Scholar] [CrossRef]
- Gwyther, M.; Schwarz, H.; Howard, A.; Ansell, B.M. C-Reactive Protein in Juvenile Chronic Arthritis: An Indicator of Disease Activity and Possibly Amyloidosis. Ann. Rheum. Dis. 1982, 41, 259–262. [Google Scholar] [CrossRef]
- Di Benedetto, P.; Cipriani, P.; Iacono, D.; Pantano, I.; Caso, F.; Emmi, G.; Grembiale, R.D.; Cantatore, F.P.; Atzeni, F.; Perosa, F.; et al. Ferritin and C-Reactive Protein Are Predictive Biomarkers of Mortality and Macrophage Activation Syndrome in Adult Onset Still’s Disease. Analysis of the Multicentre Gruppo Italiano Di Ricerca in Reumatologia Clinica e Sperimentale (GIRRCS) Cohort. PLoS ONE 2020, 15, e0235326. [Google Scholar] [CrossRef]
- Fujita, C.; Sakurai, Y.; Yasuda, Y.; Homma, R.; Huang, C.-L.; Fujita, M. MCRP as a Biomarker of Adult-Onset Still’s Disease: Quantification of MCRP by ELISA. Front. Immunol. 2022, 13, 938173. [Google Scholar] [CrossRef]
- Erre, G.L.; Cacciapaglia, F.; Sakellariou, G.; Manfredi, A.; Bartoloni, E.; Viapiana, O.; Fornaro, M.; Cauli, A.; Mangoni, A.A.; Woodman, R.J.; et al. C-Reactive Protein and 10-Year Cardiovascular Risk in Rheumatoid Arthritis. Eur. J. Intern. Med. 2022, 104, 49–54. [Google Scholar] [CrossRef] [PubMed]
- Shadick, N.A.; Cook, N.R.; Karlson, E.W.; Ridker, P.M.; Maher, N.E.; Manson, J.E.; Buring, J.E.; Lee, I.-M. C-Reactive Protein in the Prediction of Rheumatoid Arthritis in Women. Arch. Intern. Med. 2006, 166, 2490–2494. [Google Scholar] [CrossRef] [PubMed]
- Gitlin, J.D.; Gitlin, J.I.; Gitlin, D. Localizing of C-Reactive Protein in Synovium of Patients with Rheumatoid Arthritis. Arthritis Rheum. 1977, 20, 1491–1499. [Google Scholar] [CrossRef] [PubMed]
- Amos, R.S.; Constable, T.J.; Crockson, R.A.; Crockson, A.P.; McConkey, B. Rheumatoid Arthritis: Relation of Serum C-Reactive Protein and Erythrocyte Sedimentation Rates to Radiographic Changes. Br. Med. J. 1977, 1, 195–197. [Google Scholar] [CrossRef]
- Wang, J.; Xi, H.; Zhang, K.; Li, Z.; Li, L.; Chen, J.; Lou, Z. Circulating C-Reactive Protein to Prealbumin Ratio and Prealbumin to Fibrinogen Ratio Are Two Promising Inflammatory Markers Associated with Disease Activity in Rheumatoid Arthritis. Clin. Lab. 2020, 66, 757–762. [Google Scholar] [CrossRef]
- Mallya, R.K.; Hind, C.R.; Berry, H.; Pepys, M.B. Serum C-Reactive Protein in Polymyalgia Rheumatica. A Prospective Serial Study. Arthritis Rheum. 1985, 28, 383–387. [Google Scholar] [CrossRef]
- Bolhuis, T.E.; Marsman, D.; Van Den Hoogen, F.H.J.; Broeder, A.A.D.; Broeder, N.D.; Van Der Maas, A. (Dis)Agreement of Polymyalgia Rheumatica Relapse Criteria, and Prediction of Relapse in a Retrospective Cohort. BMC Rheumatol. 2022, 6, 45. [Google Scholar] [CrossRef] [PubMed]
- Gorthey, S.W.; Pathak, S.; Vambutas, A. The Correlation of Clinical Corticosteroid Responsiveness with Expression of IL-6 in Peripheral Blood Immune Cells (PBMC) in Patients with Autoimmune Inner Ear Disease (AIED). Otol. Neurotol. 2021, 42, 1422–1428. [Google Scholar] [CrossRef]
- Lasisi, A.O.; Arinola, O.G. Acute Phase Reactants in Immune-Related Inner Ear Disease. Afr. J. Biomed. Res. 2010, 13, 113–117. [Google Scholar]
- Chuah, T.; Lui, N. Relapsing Polychondritis in Singapore: A Case Series and Review of Literature. SMEDJ 2017, 58, 201–205. [Google Scholar] [CrossRef]
- Muangchan, C.; Harding, S.; Khimdas, S.; Bonner, A.; Canadian Scleroderma Research group; Baron, M.; Pope, J. Association of C-Reactive Protein with High Disease Activity in Systemic Sclerosis: Results from the Canadian Scleroderma Research Group. Arthritis Care Res. 2012, 64, 1405–1414. [Google Scholar] [CrossRef]
- Muangchan, C.; Pope, J.E. The significance of interleukin-6 and C-reactive protein in systemic sclerosis: A systematic literature review. Clin. Exp. Rheumatol. 2013, 31 (Suppl. S76), S122–S134. [Google Scholar]
- Ikeda, M.; Okazaki, H.; Minota, S. Cogan’s Syndrome with Antineutrophil Cytoplasmic Autoantibody. Ann. Rheum. Dis. 2002, 61, 761–762. [Google Scholar] [CrossRef]
- Jenifer, L.; Rodrigo Binkowski De, A. Primary Sjögren’s Syndrome and the Therapeutic Response to Rituximab: Case Report. Ann. Public Health Rep. 2019, 3. [Google Scholar] [CrossRef]
- Moutsopoulos, H.M.; Elkon, K.B.; Mavridis, A.K.; Acritidis, N.C.; Hughes, G.R.; Pepys, M.B. Serum C-Reactive Protein in Primary Sjögren’s Syndrome. Clin. Exp. Rheumatol. 1983, 1, 57–58. [Google Scholar]
- Kirzhner, M.; Jakobiec, F.A. Ocular Cicatricial Pemphigoid: A Review of Clinical Features, Immunopathology, Differential Diagnosis, and Current Management. Semin. Ophthalmol. 2011, 26, 270–277. [Google Scholar] [CrossRef]
- Huhtinen, M.; Repo, H.; Laasila, K.; Jansson, S.-E.; Kautiainen, H.; Karma, A.; Leirisalo-Repo, M. Systemic Inflammation and Innate Immune Response in Patients with Previous Anterior Uveitis. Br. J. Ophthalmol. 2002, 86, 412–417. [Google Scholar] [CrossRef] [PubMed]
- Heng, K.Y.C.; Lee, J.H.; Thomas, T. Anti-N-Methyl-D-aspartate Receptor Encephalitis Masquerading as Fever of Unknown Origin. Clin. Case Rep. 2021, 9, 2323–2327. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Liang, J.; Liu, Q.; Luo, C.; Liu, J.; Fan, R.; Chen, Z.; Chen, Y.; Peng, F.; Jiang, Y. Elevated Plasma Homocysteine Levels in Anti-N-Methyl-D-Aspartate Receptor Encephalitis. Front. Neurol. 2019, 10, 464. [Google Scholar] [CrossRef]
- Hara, M.; Yamada, S.; Nakamura, Y.; Oka, H.; Kamimura, T.; Nakane, S.; Tsuruya, K.; Harada, A. Autoimmune Autonomic Ganglionopathy Manifesting as Acute-Onset Orthostatic Hypotension in a Patient Undergoing Peritoneal Dialysis. CEN Case Rep. 2015, 5, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Nagata, R.; Matsuura, E.; Nozuma, S.; Dozono, M.; Noguchi, Y.; Ando, M.; Hiramatsu, Y.; Kodama, D.; Tanaka, M.; Kubota, R.; et al. Anti-Ganglionic Acetylcholine Receptor Antibodies in Functional Neurological Symptom Disorder/Conversion Disorder. Front. Neurol. 2023, 14, 1137958. [Google Scholar] [CrossRef]
- Gu, W.-J.; Zhang, Q.; Zhu, J.; Li, J.; Wei, S.-H.; Mu, Y.-M. Rituximab Was Used to Treat Recurrent IgG4-Related Hypophysitis with Ophthalmopathy as the Initial Presentation. Medicine 2017, 96, e6934. [Google Scholar] [CrossRef]
- Ethemoglu, O.; Calik, M. Effect of Serum Inflammatory Markers on the Prognosis of Adult and Pediatric Patients with Guillain-Barré Syndrome. Neuropsychiatr. Dis. Treat. 2018, 14, 1255–1260. [Google Scholar] [CrossRef]
- Štětkářová, I.; Ehler, E.; Židó, M.; Lauer, D.; Polák, J.; Keller, J.; Peisker, T. Influence of Hyperglycaemia and CRP on the Need for Mechanical Ventilation in Guillain-Barré Syndrome. Front. Neurol. 2022, 13, 875714. [Google Scholar] [CrossRef] [PubMed]
- Soilu-Hänninen, M.; Koskinen, J.O.; Laaksonen, M.; Hänninen, A.; Lilius, E.-M.; Waris, M. High Sensitivity Measurement of CRP and Disease Progression in Multiple Sclerosis. Neurology 2005, 65, 153–155. [Google Scholar] [CrossRef] [PubMed]
- Grut, V.; Biström, M.; Salzer, J.; Stridh, P.; Lindam, A.; Alonso-Magdalena, L.; Andersen, O.; Jons, D.; Gunnarsson, M.; Vrethem, M.; et al. Systemic Inflammation and Risk of Multiple Sclerosis—A Presymptomatic Case-Control Study. Mult. Scler. J. Exp. Transl. Clin. 2022, 8, 20552173221139770. [Google Scholar] [CrossRef] [PubMed]
- Olsson, A.; Gustavsen, S.; Gisselø Lauridsen, K.; Chenoufi Hasselbalch, I.; Sellebjerg, F.; Bach Søndergaard, H.; Bang Oturai, A. Neutrophil-to-Lymphocyte Ratio and CRP as Biomarkers in Multiple Sclerosis: A Systematic Review. Acta Neurol. Scand. 2021, 143, 577–586. [Google Scholar] [CrossRef]
- Furuya, K.; Itoh, N.; Furuya, K.; Itoh, N. A Rare Case of Neuromyelitis Optica Spectrum Disorders with Unknown Fever and Subacute Cognitive Decline with Normal Images. Cureus 2022, 14, e24950. [Google Scholar] [CrossRef] [PubMed]
- Shu, Y.; Li, R.; Qiu, W.; Chang, Y.; Sun, X.; Fang, L.; Chen, C.; Yang, Y.; Lu, Z.; Hu, X.; et al. Association of Serum Gamma-Glutamyltransferase and C-Reactive Proteins with Neuromyelitis Optica and Multiple Sclerosis. Mult. Scler. Relat. Disord. 2017, 18, 65–70. [Google Scholar] [CrossRef]
- Watanabe, S.; Takeda, M.; Saito, T.; Kimura, A.; Yoshikawa, H. “Chronic” Optic Neuropathy in Chronic Inflammatory Demyelinating Polyneuropathy: A Case Report. Neurol. Clin. Neurosci. 2013, 1, 78–81. [Google Scholar] [CrossRef]
- Larson, J.; Twohig, P.; Hutchins, K. Chronic Inflammatory Demyelinating Polyneuropathy after Therapy with Infliximab Biosimilar. ACG Case Rep. J. 2023, 10, e00993. [Google Scholar] [CrossRef]
- Cardinaels, N.; De Ruysscher, D.; Poesen, K.; Gheysens, O.; Doyen, C.; Delforge, M. A case report of an atypical POEMS syndrome. Belg. J. Hematol. 2015, 6, 156–161. [Google Scholar]
- Apolinario, M.; Brussels, A.; Cook, C.B.; Yang, S. Autoimmune Polyglandular Syndrome Type 3: A Case Report of an Unusual Presentation and Literature Review. Clin. Case Rep. 2022, 10, e05391. [Google Scholar] [CrossRef]
- Ramos-Casals, M.; Retamozo, S.; Sisó-Almirall, A.; Pérez-Alvarez, R.; Pallarés, L.; Brito-Zerón, P. Clinically-Useful Serum Biomarkers for Diagnosis and Prognosis of Sarcoidosis. Expert Rev. Clin. Immunol. 2019, 15, 391–405. [Google Scholar] [CrossRef] [PubMed]
- Sweiss, N.J.; Barnathan, E.S.; Lo, K.; Judson, M.A.; Baughman, R. T48 Investigators C-Reactive Protein Predicts Response to Infliximab in Patients with Chronic Sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2010, 27, 49–56. [Google Scholar]
- Nott, K.; Nott, V.; Lever, E.; Deakin, C.; Galloway, J.; Fisher, C.; Compeyrot-Lacassagne, S. Pediatric Sarcoidosis: Retrospective Analysis of Biopsy-Proven Patients. J. Rheumatol. 2022, 50, 924–933. [Google Scholar] [CrossRef]
- McDonnell, M.J.; Saleem, M.I.; Wall, D.; Gilmartin, J.J.; Rutherford, R.M.; O’Regan, A. Predictive Value of C-Reactive Protein and Clinically Relevant Baseline Variables in Sarcoidosis. Sarcoidosis Vasc. Diffus. Lung Dis. 2016, 33, 331–340. [Google Scholar]
- Hind, C.R.; Flint, K.C.; Hudspith, B.N.; Felmingham, D.; Brostoff, J.; Johnson, N.M. Serum C-Reactive Protein Concentrations in Patients with Pulmonary Sarcoidosis. Thorax 1987, 42, 332–335. [Google Scholar] [CrossRef]
- Hu, C.; Zou, Y.; Pan, J.; Yang, J.; Yang, T.; Tan, T.; Li, J. Analysis of Clinical Characteristics, Pathological Changes and Changes of Interleukin-6 (IL-6) and C-Reactive Protein (CRP) in Children with Castleman’s Disease. Med. Sci. Monit. 2020, 26, e924783-1–e924783-6. [Google Scholar] [CrossRef] [PubMed]
- Jiang, J.-P.; Shen, X.-F.; Du, J.-F.; Guan, W.-X. A Retrospective Study of 34 Patients with Unicentric and Multicentric Castleman’s Disease: Experience from a Single Institution. Oncol. Lett. 2018, 15, 2407–2412. [Google Scholar] [CrossRef] [PubMed]
- Pamukcu, M.; Badem, A.; Parlak, O. Autoimmune Thyroiditis CRP Association. Int. J. Res. Med. Sci. 2018, 6, 3270–3275. [Google Scholar] [CrossRef]
- Ranganadane, R.; Sumathi, S.S.; Raghavan, S.A.; Shafiulla, A.; Subramanian, G.; Nachimuthu, M.K.S. Cardiovascular Risk in Hashimoto\’s Thyroiditis: Role of Thyroid Autoimmunity. SBV J. Basic Clin. Appl. Health Sci. 2021, 4, 20–22. [Google Scholar] [CrossRef]
- Wallace, Z.S.; Deshpande, V.; Mattoo, H.; Mahajan, V.S.; Kulikova, M.; Pillai, S.; Stone, J.H. IgG4-Related Disease: Clinical and Laboratory Features in One Hundred Twenty-Five Patients. Arthritis Rheumatol. 2015, 67, 2466–2475. [Google Scholar] [CrossRef] [PubMed]
- Shrotriya, S.; Walsh, D.; Nowacki, A.S.; Lorton, C.; Aktas, A.; Hullihen, B.; Benanni-Baiti, N.; Hauser, K.; Ayvaz, S.; Estfan, B. Serum C-Reactive Protein Is an Important and Powerful Prognostic Biomarker in Most Adult Solid Tumors. PLoS ONE 2018, 13, e0202555. [Google Scholar] [CrossRef]
- Zhu, M.; Ma, Z.; Zhang, X.; Hang, D.; Yin, R.; Feng, J.; Xu, L.; Shen, H. C-Reactive Protein and Cancer Risk: A Pan-Cancer Study of Prospective Cohort and Mendelian Randomization Analysis. BMC Med. 2022, 20, 301. [Google Scholar] [CrossRef] [PubMed]
- Liu, T.; Zhang, Q.; Song, C.; Siyin, S.T.; Chen, S.; Zhang, Q.; Song, M.; Cao, L.; Shi, H. C-Reactive Protein Trajectories and the Risk of All Cancer Types: A Prospective Cohort Study. Int. J. Cancer 2022, 151, 297–307. [Google Scholar] [CrossRef]
- Hart, P.C.; Rajab, I.M.; Alebraheem, M.; Potempa, L.A. C-Reactive Protein and Cancer—Diagnostic and Therapeutic Insights. Front. Immunol. 2020, 11, 595835. [Google Scholar] [CrossRef]
- Herishanu, Y.; Polliack, A.; Shenhar-Tsarfaty, S.; Weinberger, R.; Gelman, R.; Ziv-Baran, T.; Zeltser, D.; Shapira, I.; Berliner, S.; Rogowski, O. Increased Serum C-Reactive Protein Levels Are Associated with Shorter Survival and Development of Second Cancers in Chronic Lymphocytic Leukemia. Ann. Med. 2017, 49, 75–82. [Google Scholar] [CrossRef]
- Jiang, L.; Zhang, X.; Chen, Y.; Huo, X.; Deng, S.; Yang, X.; Luo, Y.; Luo, Y.; Lu, X.; Zhang, M.; et al. Alteration of Serum 25(OH) Vitamin D, Vitamin D Binding Protein, and C-Reactive Protein Levels in Acute Leukemia Patients. Clin. Lab. 2018, 64, 1553–1559. [Google Scholar] [CrossRef]
- Artz, A.S.; Logan, B.; Zhu, X.; Akpek, G.; Bufarull, R.M.; Gupta, V.; Lazarus, H.M.; Litzow, M.; Loren, A.; Majhail, N.S.; et al. The Prognostic Value of Serum C-Reactive Protein, Ferritin, and Albumin Prior to Allogeneic Transplantation for Acute Myeloid Leukemia and Myelodysplastic Syndromes. Haematologica 2016, 101, 1426–1433. [Google Scholar] [CrossRef]
- Yanagisawa, H.; Kawabata, H.; Ueda, Y.; Arita, K.; Iwao-Kawanami, H.; Sakai, T.; Kawanami, T.; Yamada, K.; Mizuta, S.; Fukushima, T.; et al. Prognostic Impacts of Serum Levels of C-Reactive Protein, Albumin, and Total Cholesterol in Patients with Myelodysplastic Syndromes. Int. J. Hematol. 2022, 116, 81–88. [Google Scholar] [CrossRef] [PubMed]
- Baba, Y.; Saito, B.; Shimada, S.; Sasaki, Y.; Fujiwara, S.; Arai, N.; Kawaguchi, Y.; Kabasawa, N.; Tsukamoto, H.; Uto, Y.; et al. Increased Serum C-Reactive Protein Is an Adverse Prognostic Factor in Low-Risk Myelodysplastic Syndromes. Int. J. Hematol. 2021, 114, 441–448. [Google Scholar] [CrossRef] [PubMed]
- Lussana, F.; Rambaldi, A. Inflammation and Myeloproliferative Neoplasms. J. Autoimmun. 2017, 85, 58–63. [Google Scholar] [CrossRef] [PubMed]
- Brown, R.D.; Snowdon, L.; Uhr, E.; Gibson, J.; Joshua, D. C-Reactive Protein (CRP) Levels Do Not Reflect Disease Status in Patients with Multiple Myeloma. Leuk. Lymphoma 1993, 9, 509–512. [Google Scholar] [CrossRef]
- Tienhaara, A.; Pulkki, K.; Mattila, K.; Irjala, K.; Pelliniemi, T.T. Serum Immunoreactive Interleukin-6 and C-Reactive Protein Levels in Patients with Multiple Myeloma at Diagnosis. Br. J. Haematol. 1994, 86, 391–393. [Google Scholar] [CrossRef] [PubMed]
- Zahlten-Hinguranage, A.; Goldschmidt, H.; Cremer, F.W.; Egerer, G.; Moehler, T.; Witte, D.; Bernd, L.; Sabo, D.; Zeifang, F. Preoperative Elevation of Serum C-Reactive Protein Is Predictive for Prognosis in Myeloma Bone Disease after Surgery. Br. J. Cancer 2006, 95, 782–787. [Google Scholar] [CrossRef]
- Chakraborty, R.; Muchtar, E.; Kumar, S.K.; Buadi, F.K.; Dingli, D.; Dispenzieri, A.; Hayman, S.R.; Hogan, W.J.; Kapoor, P.; Lacy, M.Q.; et al. Elevated Pre-Transplant C-Reactive Protein Identifies a High-Risk Subgroup in Multiple Myeloma Patients Undergoing Delayed Autologous Stem Cell Transplantation. Bone Marrow Transpl. 2018, 53, 155–161. [Google Scholar] [CrossRef]
- Mallard, J.; Gagez, A.-L.; Baudinet, C.; Herbinet, A.; Maury, J.; Bernard, P.L.; Cartron, G. C-Reactive Protein Level: A Key Predictive Marker of Cachexia in Lymphoma and Myeloma Patients. J. Hematol. 2019, 8, 55–59. [Google Scholar] [CrossRef]
- Qin, W.; Yuan, Q.; Wu, J.; Yu, H.; Wang, Y.; Chen, Q. Prognostic Value of Pre-Therapy C-Reactive Protein Level in Diffuse Large B-Cell Lymphoma: A Meta-Analysis. Leuk. Lymphoma 2019, 60, 358–366. [Google Scholar] [CrossRef]
- Advani, R.H.; Skrypets, T.; Civallero, M.; Spinner, M.A.; Manni, M.; Kim, W.S.; Shustov, A.R.; Horwitz, S.M.; Hitz, F.; Cabrera, M.E.; et al. Outcomes and Prognostic Factors in Angioimmunoblastic T-Cell Lymphoma: Final Report from the International T-Cell Project. Blood 2021, 138, 213–220. [Google Scholar] [CrossRef]
- Mărginean, C.O.; Meliţ, L.E.; Horvath, E.; Gozar, H.; Chinceşan, M.I. Non-Hodgkin Lymphoma, Diagnostic, and Prognostic Particularities in Children—A Series of Case Reports and a Review of the Literature (CARE Compliant). Medicina 2018, 97, e9802. [Google Scholar] [CrossRef]
- Zahzeh, M.R.; Zahzeh, T. Evaluation of Protein, Lipid and Inflammatory Profiles in Patients with Non-Hodgkin Lymphoma in the Western Region of Algeria. J. Drug Deliv. Ther. 2020, 10, 1–5. [Google Scholar] [CrossRef]
- Kawaguchi, Y.; Saito, B.; Nakata, A.; Matsui, T.; Sasaki, Y.; Shimada, S.; Abe, M.; Watanuki, M.; Baba, Y.; Murai, S.; et al. Elevated C-Reactive Protein Level Is Associated with Poor Prognosis in Follicular Lymphoma Patients Undergoing Rituximab-Containing Chemotherapy. Int. J. Hematol. 2020, 112, 341–348. [Google Scholar] [CrossRef]
- Rafiq, M.; Abel, G.; Renzi, C.; Lyratzopoulos, G. Inflammatory Marker Testing in Primary Care in the Year before Hodgkin Lymphoma Diagnosis: A UK Population-Based Case–Control Study in Patients Aged ≤50 Years. Br. J. Gen. Pract. 2022, 72, e546–e555. [Google Scholar] [CrossRef] [PubMed]
- Legouffe, E.; Rodriguez, C.; Picot, M.C.; Richard, B.; Klein, B.; Rossi, J.F.; Commes, T. C-reactive protein serum level is a valuable and simple prognostic marker in non Hodgkin’s lymphoma. Leuk. Lymphoma 1998, 31, 351–357. [Google Scholar] [CrossRef]
- Li, Y.; Yang, C.; Mao, L.; Wang, J.; Li, C.; Qian, W. Clinical Characteristics of Angioimmunoblastic T-Cell Lymphoma in China and C-Reactive Protein as an Independent Prognostic Factor. Medicine 2017, 96, e8091. [Google Scholar] [CrossRef] [PubMed]
- Li, Y.J.; Li, Z.M.; Xia, Y.; Huang, J.J.; Huang, H.Q.; Xia, Z.J.; Lin, T.Y.; Li, S.; Cai, X.Y.; Wu-Xiao, Z.J.; et al. Serum C-reactive protein (CRP) as a simple and independent prognostic factor in extranodal natural killer/T-cell lymphoma, nasal type. PLoS ONE 2013, 8, e64158. [Google Scholar] [CrossRef] [PubMed]
- Lim, Y.; Park, J.-H.; Lee, D.-Y. Prognostic Value of Leukocytosis in Systemic Anaplastic Large-Cell Lymphoma with Cutaneous Involvement. Ann. Dermatol. 2018, 30, 721–724. [Google Scholar] [CrossRef]
- Kostiala, A.A.; Kostiala, I.; Valtonen, V.V.; Teerenhovi, L. Levels of C-Reactive Protein in Patients with Hematologic Malignancies. Scand. J. Infect. Dis. 1985, 17, 407–410. [Google Scholar] [CrossRef]
- Chaturvedi, A.K.; Caporaso, N.E.; Katki, H.A.; Wong, H.-L.; Chatterjee, N.; Pine, S.R.; Chanock, S.J.; Goedert, J.J.; Engels, E.A. C-Reactive Protein and Risk of Lung Cancer. J. Clin. Oncol. 2010, 28, 2719–2726. [Google Scholar] [CrossRef]
- Wu, X.-R.; Peng, H.-X.; Xiong, S.; Wen, Y.-K.; Chen, J.-N.; Li, C.-C.; Jiang, Y.; Su, Z.-X.; Liu, J.; He, J.-X.; et al. A Multiethnic Bidirectional Mendelian Randomization Study Negates Causal Effects of C-Reactive Protein Concentrations on Lung Cancer. Transl. Lung Cancer Res. 2021, 10, 4380–4389. [Google Scholar] [CrossRef] [PubMed]
- Ji, M.; Du, L.; Ma, Z.; Xie, J.; Huang, Y.; Wei, X.; Jiang, X.; Xu, J.; Yin, R.; Wang, Y.; et al. Circulating C-reactive Protein Increases Lung Cancer Risk: Results from a Prospective Cohort of UK Biobank. Int. J. Cancer 2022, 150, 47–55. [Google Scholar] [CrossRef]
- McDonald, L.; Carroll, R.; Harish, A.; Tanna, N.; Mehmud, F.; Alikhan, R.; Ramagopalan, S.V. Suspected Cancer Symptoms and Blood Test Results in Primary Care before a Diagnosis of Lung Cancer: A Case–Control Study. Future Oncol. 2019, 15, 3755–3762. [Google Scholar] [CrossRef] [PubMed]
- Hong, S.; Kang, Y.A.; Cho, B.C.; Kim, D.J. Elevated Serum C-Reactive Protein as a Prognostic Marker in Small Cell Lung Cancer. Yonsei Med. J. 2012, 53, 111–117. [Google Scholar] [CrossRef] [PubMed]
- Ni, X.-F.; Wu, P.; Wu, C.-P.; Ji, M.; Wu, J.; Gu, X.-F.; Jiang, Z.-X. Elevated Serum C-Reactive Protein, Carcinoembryonic Antigen and N2 Disease Are Poor Prognostic Indicators in Non-Small Cell Lung Cancer. Asia Pac. J. Clin. Oncol. 2015, 11, e22–e30. [Google Scholar] [CrossRef]
- Hotta, T.; Nakashima, K.; Hata, K.; Tsubata, Y.; Isobe, T. High Serum C-Reactive Protein Levels Predict Survival in Patients with Treated Advanced Lung Adenocarcinoma. J. Thorac. Dis. 2021, 13, 1476–1484. [Google Scholar] [CrossRef] [PubMed]
- Okita, R.; Okada, M.; Inokawa, H.; Murakami, T.; Ikeda, E. Prognostic Values of Preoperative C-Reactive Protein, Albumin, and Neutrophil Ratios in Patients with Malignant Pleural Mesothelioma Who Underwent Extrapleural Pneumonectomy. Surg. Oncol. 2022, 43, 101813. [Google Scholar] [CrossRef]
- Huang, Y.; Feng, J.-F.; Liu, J.-S.; Chen, Q.-X. Prognostic Role of Serum C-Reactive Protein in Esophageal Cancer: A Systematic Review and Meta-Analysis. Ther. Clin. Risk Manag. 2015, 11, 89–94. [Google Scholar] [CrossRef]
- Huang, W.; Wu, L.; Liu, X.; Long, H.; Rong, T.; Ma, G. Preoperative Serum C-Reactive Protein Levels and Postoperative Survival in Patients with Esophageal Squamous Cell Carcinoma: A Propensity Score Matching Analysis. J. Cardiothorac. Surg. 2019, 14, 167. [Google Scholar] [CrossRef]
- Lorton, C.M.; Higgins, L.; O’Donoghue, N.; Donohoe, C.; O’Connell, J.; Mockler, D.; Reynolds, J.V.; Walsh, D.; Lysaght, J. C-Reactive Protein and C-Reactive Protein-Based Scores to Predict Survival in Esophageal and Junctional Adenocarcinoma: Systematic Review and Meta-Analysis. Ann. Surg. Oncol. 2022, 29, 1853–1865. [Google Scholar] [CrossRef]
- Motoyama, S.; Miura, M.; Hinai, Y.; Maruyama, K.; Usami, S.; Nakatsu, T.; Saito, H.; Minamiya, Y.; Suzuki, T.; Ogawa, J. C-Reactive Protein 1059G>CGenetic Polymorphism Influences Serum C-Reactive Protein Levels after Esophagectomy in Patients with Thoracic Esophageal Cancer. J. Am. Coll. Surg. 2009, 209, 477–483. [Google Scholar] [CrossRef] [PubMed]
- Lukaszewicz-Zając, M.; Mroczko, B.; Kozłowski, M.; Nikliński, J.; Laudański, J.; Siewko, M.; Szmitkowski, M. Comparative Evaluation of Serum C-Reactive Protein (CRP) Levels in the Different Histological Subtypes of Esophageal Cancer (Squamous Cell Carcinoma and Adenocarcinoma of Esophagus). J. Clin. Lab. Anal 2012, 26, 73–81. [Google Scholar] [CrossRef] [PubMed]
- Cebi, A.; Mert, H.; Mert, N. Evaluation of Some Tumor Markers, Acute Phase Proteins, Sialic Acid and Lipid Bound Sialic Acid before and after Chemotherapy in Stomach Cancer. Med. Sci. Discov. 2016, 3, 22–27. [Google Scholar] [CrossRef]
- Baba, H.; Kuwabara, K.; Ishiguro, T.; Hatano, S.; Matsuzawa, T.; Fukuchi, M.; Kumagai, Y.; Ishibashi, K.; Mochiki, E.; Ishida, H. C-Reactive Protein as a Significant Prognostic Factor for Stage IV Gastric Cancer Patients. Anticancer Res. 2013, 33, 5591–5595. [Google Scholar]
- Yu, Q.; Yu, X.-F.; Zhang, S.-D.; Wang, H.-H.; Wang, H.-Y.; Teng, L.-S. Prognostic Role of C-Reactive Protein in Gastric Cancer: A Meta-Analysis. Asian Pac. J. Cancer Prev. 2013, 14, 5735–5740. [Google Scholar] [CrossRef]
- Shimura, T.; Kitagawa, M.; Yamada, T.; Ebi, M.; Mizoshita, T.; Tanida, S.; Kataoka, H.; Kamiya, T.; Joh, T. C-Reactive Protein Is a Potential Prognostic Factor for Metastatic Gastric Cancer. Anticancer Res. 2012, 32, 491–496. [Google Scholar]
- Nozoe, T.; Iguchi, T.; Adachi, E.; Matsukuma, A.; Ezaki, T. Preoperative Elevation of Serum C-Reactive Protein as an Independent Prognostic Indicator for Gastric Cancer. Surg. Today 2011, 41, 510–513. [Google Scholar] [CrossRef]
- Cardoso, M.F.; Lourenço, L.C.; Oliveira, A.M.; Boléo-Tomé, J.P.; Reis, J. Gastric Gastrointestinal Stromal Tumor Presenting with an Intraluminal Draining Abscess and Left Pleural Effusion. Endoscopy 2016, 48, E399–E400. [Google Scholar] [CrossRef]
- Cao, X.; Cui, J.; Li, Z.; Zhao, G. Preoperative C-Reactive Protein/Albumin Ratio Is a Prognostic Indicator for Survival in Surgically Treated Gastrointestinal Stromal Tumors: A Retrospective Cohort Study. Cancer Manag. Res. 2021, 13, 4155–4167. [Google Scholar] [CrossRef]
- Muñoz-Cedeño, R.G.; Santillán-López, W.; Paullán-Sani, V.; Rodríguez-Chica, G. Giant Extraintestinal Gastrointestinal Stromal Tumor: Case Report and Bibliography Review. Rev. Colomb. Gastroenterol. 2021, 36, 532–537. [Google Scholar] [CrossRef]
- van de Poll, M.C.G.; Klaver, Y.L.B.; Lemmens, V.E.P.P.; Leenders, B.J.M.; Nienhuijs, S.W.; de Hingh, I.H.J.T. C-Reactive Protein Concentration Is Associated with Prognosis in Patients Suffering from Peritoneal Carcinomatosis of Colorectal Origin. Int. J. Color. Dis. 2011, 26, 1067–1073. [Google Scholar] [CrossRef]
- Asmar, A.E.; Bendavides, M.; Moreau, M.; Hendlisz, A.; Deleporte, A.; Khalife, M.; Donckier, V.; Liberale, G. Postoperative C-Reactive Protein Kinetics Predict Postoperative Complications in Patients Treated with Cytoreductive Surgery and Hyperthermic Intraperitoneal Chemotherapy for Peritoneal Carcinomatosis. World J. Surg. Oncol. 2020, 18, 311. [Google Scholar] [CrossRef]
- Zhou, B.; Shu, B.; Yang, J.; Liu, J.; Xi, T.; Xing, Y. C-Reactive Protein, Interleukin-6 and the Risk of Colorectal Cancer: A Meta-Analysis. Cancer Causes Control 2014, 25, 1397–1405. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Dai, J.Y.; Albanes, D.; Arndt, V.; Berndt, S.I.; Bézieau, S.; Brenner, H.; Buchanan, D.D.; Butterbach, K.; Caan, B.; et al. Mendelian Randomization Analysis of C-Reactive Protein on Colorectal Cancer Risk. Int. J. Epidemiol. 2019, 48, 767–780. [Google Scholar] [CrossRef]
- Crockett, S.D.; Mott, L.A.; Barry, E.L.; Figueiredo, J.C.; Burke, C.A.; Baxter, G.J.; Sandler, R.S.; Baron, J.A. C-Reactive Protein and Risk of Colorectal Adenomas or Serrated Polyps: A Prospective Study. Cancer Prev. Res. 2014, 7, 1122–1127. [Google Scholar] [CrossRef]
- Chen, R.; Wang, L.; Zhao, Q.; Li, Z.; Chen, M.; Lian, G.; Zhang, J. Platelet-to-Lymphocyte Ratio and C-Reactive Protein as Markers for Colorectal Polyp Histological Type. BMC Cancer 2021, 21, 556. [Google Scholar] [CrossRef] [PubMed]
- Sieghart, W.; Pinter, M.; Hucke, F.; Graziadei, I.; Schöniger-Hekele, M.; Müller, C.; Vogel, W.; Trauner, M.; Peck-Radosavljevic, M. Single Determination of C-Reactive Protein at the Time of Diagnosis Predicts Long-Term Outcome of Patients with Hepatocellular Carcinoma. Hepatology 2013, 57, 2224–2234. [Google Scholar] [CrossRef]
- Gerhardt, T.; Milz, S.; Schepke, M.; Feldmann, G.; Wolff, M.; Sauerbruch, T.; Dumoulin, F.L. C-Reactive Protein Is a Prognostic Indicator in Patients with Perihilar Cholangiocarcinoma. World J. Gastroenterol. 2006, 12, 5495–5500. [Google Scholar] [CrossRef]
- Yeh, Y.-C.; Lei, H.-J.; Chen, M.-H.; Ho, H.-L.; Chiu, L.-Y.; Li, C.-P.; Wang, Y.-C. C-Reactive Protein (CRP) Is a Promising Diagnostic Immunohistochemical Marker for Intrahepatic Cholangiocarcinoma and Is Associated with Better Prognosis. Am. J. Surg. Pathol. 2017, 41, 1630–1641. [Google Scholar] [CrossRef] [PubMed]
- Lin, Z.-Y.; Liang, Z.-X.; Zhuang, P.-L.; Chen, J.-W.; Cao, Y.; Yan, L.-X.; Yun, J.-P.; Xie, D.; Cai, M.-Y. Intrahepatic Cholangiocarcinoma Prognostic Determination Using Pre-Operative Serum C-Reactive Protein Levels. BMC Cancer 2016, 16, 792. [Google Scholar] [CrossRef] [PubMed]
- Pine, J.K.; Fusai, K.G.; Young, R.; Sharma, D.; Davidson, B.R.; Menon, K.V.; Rahman, S.H. Serum C-Reactive Protein Concentration and the Prognosis of Ductal Adenocarcinoma of the Head of Pancreas. Eur. J. Surg. Oncol. 2009, 35, 605–610. [Google Scholar] [CrossRef]
- Sanjay, P.; de Figueiredo, R.S.; Leaver, H.; Ogston, S.; Kulli, C.; Polignano, F.M.; Tait, I.S. Preoperative Serum C-Reactive Protein Levels and Post-Operative Lymph Node Ratio Are Important Predictors of Survival after Pancreaticoduodenectomy for Pancreatic Ductal Adenocarcinoma. JOP 2012, 13, 199–204. [Google Scholar]
- Tani, M.; Iida, H.; Maehira, H.; Mori, H.; Miyake, T.; Kaida, S. A High C-Reactive Protein Level on Postoperative Day 7 Is Associated with Poor Survival of Patients with Pancreatic Ductal Adenocarcinoma After Resection. Am. Surg. 2022, 88, 2024–2029. [Google Scholar] [CrossRef]
- O’Brian, D.; Prunty, M.; Hill, A.; Shoag, J. The Role of C-Reactive Protein in Kidney, Bladder, and Prostate Cancers. Front. Immunol. 2021, 12, 721989. [Google Scholar] [CrossRef] [PubMed]
- Grimm, T.; Buchner, A.; Schneevoigt, B.; Kretschmer, A.; Apfelbeck, M.; Grabbert, M.; Jokisch, J.F.; Stief, C.G.; Karl, A. Impact of Preoperative Hemoglobin and CRP Levels on Cancer-Specific Survival in Patients Undergoing Radical Cystectomy for Transitional Cell Carcinoma of the Bladder: Results of a Single-Center Study. World J. Urol. 2016, 34, 703–708. [Google Scholar] [CrossRef]
- Barahona Ponce, C.; Scherer, D.; Brinster, R.; Boekstegers, F.; Marcelain, K.; Gárate-Calderón, V.; Müller, B.; de Toro, G.; Retamales, J.; Barajas, O.; et al. Gallstones, Body Mass Index, C-Reactive Protein, and Gallbladder Cancer: Mendelian Randomization Analysis of Chilean and European Genotype Data. Hepatology 2021, 73, 1783–1796. [Google Scholar] [CrossRef] [PubMed]
- Eggers, H.; Seidel, C.; Schrader, A.J.; Lehmann, R.; Wegener, G.; Kuczyk, M.A.; Steffens, S. Serum C-Reactive Protein: A Prognostic Factor in Metastatic Urothelial Cancer of the Bladder. Med. Oncol. 2013, 30, 705. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Li, X.; Qian, H.; Di, G.; Zhou, R.; Dong, Y.; Chen, W.; Ren, Q. C-Reactive Protein as a Prognostic Biomarker for Gynecologic Cancers: A Meta-Analysis. Comput. Intell. Neurosci. 2022, 2022, 6833078. [Google Scholar] [CrossRef]
- Nishigaya, Y.; Kobayashi, Y.; Matsuzawa, Y.; Hasegawa, K.; Fukasawa, I.; Watanabe, Y.; Tokunaga, H.; Yaegashi, N.; Iwashita, M. Diagnostic Value of Combination Serum Assay of Lactate Dehydrogenase, D-Dimer, and C-Reactive Protein for Uterine Leiomyosarcoma. J. Obstet. Gynaecol. Res. 2019, 45, 189–194. [Google Scholar] [CrossRef]
- Peres, L.C.; Mallen, A.R.; Townsend, M.K.; Poole, E.M.; Trabert, B.; Allen, N.E.; Arslan, A.A.; Dossus, L.; Fortner, R.T.; Gram, I.T.; et al. High Levels of C-Reactive Protein Are Associated with an Increased Risk of Ovarian Cancer: Results from the Ovarian Cancer Cohort Consortium. Cancer Res. 2019, 79, 5442–5451. [Google Scholar] [CrossRef]
- Said, S.; Pazoki, R.; Karhunen, V.; Võsa, U.; Ligthart, S.; Bodinier, B.; Koskeridis, F.; Welsh, P.; Alizadeh, B.Z.; Chasman, D.I.; et al. Genetic Analysis of over Half a Million People Characterises C-Reactive Protein Loci. Nat. Commun. 2022, 13, 2198. [Google Scholar] [CrossRef] [PubMed]
- Al Ghazal, A.; Steffens, S.; Steinestel, J.; Lehmann, R.; Schnoeller, T.J.; Schulte-Hostede, A.; Wegener, G.; Jentzmik, F.; Schrader, M.; Kuczyk, M.A.; et al. Elevated C-Reactive Protein Values Predict Nodal Metastasis in Patients with Penile Cancer. BMC Urol. 2013, 13, 53. [Google Scholar] [CrossRef]
- Steffens, S.; Al Ghazal, A.; Steinestel, J.; Lehmann, R.; Wegener, G.; Schnoeller, T.J.; Cronauer, M.V.; Jentzmik, F.; Schrader, M.; Kuczyk, M.A.; et al. High CRP Values Predict Poor Survival in Patients with Penile Cancer. BMC Cancer 2013, 13, 223. [Google Scholar] [CrossRef] [PubMed]
- Ghoshal, A.; Garmo, H.; Arthur, R.; Hammar, N.; Jungner, I.; Malmström, H.; Lambe, M.; Walldius, G.; Van Hemelrijck, M. Serum Biomarkers to Predict Risk of Testicular and Penile Cancer in AMORIS. Ecancermedicalscience 2017, 11, 762. [Google Scholar] [CrossRef]
- Spassova, I.; Ugurel, S.; Kubat, L.; Zimmer, L.; Terheyden, P.; Mohr, A.; Andtback, H.B.; Villabona, L.; Leiter, U.; Eigentler, T.; et al. Clinical and Molecular Characteristics Associated with Response to Therapeutic PD-1/PD-L1 Inhibition in Advanced Merkel Cell Carcinoma. J. Immunother. Cancer 2022, 10, e003198. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, T.; Ichikawa, J.; Giuroiu, I.; Laino, A.S.; Hao, Y.; Krogsgaard, M.; Vassallo, M.; Woods, D.M.; Stephen Hodi, F.; Weber, J. C Reactive Protein Impairs Adaptive Immunity in Immune Cells of Patients with Melanoma. J. Immunother. Cancer 2020, 8, e000234. [Google Scholar] [CrossRef] [PubMed]
- Schildbach, V.A.S.; Horn, S.; Hidalgo-Gadea, G.; Johannis, W.; Mauch, C.; Franklin, C. C-Reactive Protein and Lymphocyte-to-Monocyte Ratio Predict Recurrence in Stage III Melanoma Patients with Microscopic Sentinel Lymph Node Metastasis. Cancers 2023, 15, 702. [Google Scholar] [CrossRef]
- Fang, S.; Wang, Y.; Sui, D.; Liu, H.; Ross, M.I.; Gershenwald, J.E.; Cormier, J.N.; Royal, R.E.; Lucci, A.; Schacherer, C.W.; et al. C-Reactive Protein As a Marker of Melanoma Progression. J. Clin. Oncol. 2015, 33, 1389–1396. [Google Scholar] [CrossRef]
- Tartour, E.; Dorval, T.; Mosseri, V.; Deneux, L.; Mathiot, C.; Brailly, H.; Montero, F.; Joyeux, I.; Pouillart, P.; Fridman, W.H. Serum Interleukin 6 and C-Reactive Protein Levels Correlate with Resistance to IL-2 Therapy and Poor Survival in Melanoma Patients. Br. J. Cancer 1994, 69, 911–913. [Google Scholar] [CrossRef]
- Fang, S.; Wang, Y.; Dang, Y.; Gagel, A.; Ross, M.I.; Gershenwald, J.E.; Cormier, J.N.; Wargo, J.; Haydu, L.E.; Davies, M.A.; et al. Association between Body Mass Index, C-Reactive Protein Levels, and Melanoma Patient Outcomes. J. Investig. Dermatol. 2017, 137, 1792–1795. [Google Scholar] [CrossRef]
- Meijer, N.; de Bruyn, D.P.; de Klein, A.; Paridaens, D.; Verdijk, R.M.; Berendschot, T.T.J.M.; Brosens, E.; Jager, M.J.; Kiliç, E. High C-Reactive Protein Levels Are Related to Better Survival in Patients with Uveal Melanoma. Ophthalmol. Sci. 2022, 2, 100117. [Google Scholar] [CrossRef]
- Nemecek, E.; Funovics, P.T.; Hobusch, G.M.; Lang, S.; Willegger, M.; Sevelda, F.; Brodowicz, T.; Stihsen, C.; Windhager, R.; Panotopoulos, J. C-Reactive Protein: An Independent Predictor for Dedifferentiated Chondrosarcoma. J. Orthop. Res. 2018, 36, 2797–2801. [Google Scholar] [CrossRef] [PubMed]
- Errani, C.; Traversari, M.; Cosentino, M.; Manfrini, M.; Basoli, S.; Tsukamoto, S.; Mavrogenis, A.F.; Bordini, B.; Donati, D.M. The Prognostic Value of the Serum Level of C-Reactive Protein for Survival of Children with Ewing’s Sarcoma. Cancers 2023, 15, 1573. [Google Scholar] [CrossRef] [PubMed]
- Yi, J.-H.; Wang, D.; Li, Z.-Y.; Hu, J.; Niu, X.-F.; Liu, X.-L. C-Reactive Protein as a Prognostic Factor for Human Osteosarcoma: A Meta-Analysis and Literature Review. PLoS ONE 2014, 9, e94632. [Google Scholar] [CrossRef]
- Hobusch, G.M.; Bodner, F.; Walzer, S.; Marculescu, R.; Funovics, P.T.; Sulzbacher, I.; Windhager, R.; Panotopoulos, J. C-Reactive Protein as a Prognostic Factor in Patients with Chordoma of Lumbar Spine and Sacrum—A Single Center Pilot Study. World J. Surg. Oncol. 2016, 14, 111. [Google Scholar] [CrossRef] [PubMed]
- Li, W.; Luo, X.; Liu, Z.; Chen, Y.; Li, Z. Prognostic Value of C-Reactive Protein Levels in Patients with Bone Neoplasms: A Meta-Analysis. PLoS ONE 2018, 13, e0195769. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Liu, S.; Zhao, X.; Fang, E.; Zhao, X. The Value of C-Reactive Protein as an Independent Prognostic Indicator for Disease-Specific Survival in Patients with Soft Tissue Sarcoma: A Meta-Analysis. PLoS ONE 2019, 14, e0219215. [Google Scholar] [CrossRef]
- Chen, Y.; Cong, R.; Ji, C.; Ruan, W. The Prognostic Role of C-Reactive Protein in Patients with Head and Neck Squamous Cell Carcinoma: A Meta-Analysis. Cancer Med. 2020, 9, 9541–9553. [Google Scholar] [CrossRef]
- Kruse, A.L.; Luebbers, H.T.; Grätz, K.W. C-Reactive Protein Levels: A Prognostic Marker for Patients with Head and Neck Cancer? Head Neck Oncol. 2010, 2, 21. [Google Scholar] [CrossRef]
- Adachi, M.; Nakayama, M.; Matsumoto, S.; Shima, Y.; Uemaetomari, I.; Yoshimura, T.; Onishi, K.; Senarita, M.; Tabuchi, K. Elevation of C-Reactive Protein during Concurrent Chemoradiotherapy Is a Poor Predictive Factor for Head and Neck Cancer. Auris Nasus Larynx 2023, 50, 601–606. [Google Scholar] [CrossRef]
- Graupp, M.; Schaffer, K.; Wolf, A.; Vasicek, S.; Weiland, T.; Pondorfer, P.; Holzmeister, C.; Moser, U.; Thurnher, D. C-reactive Protein Is an Independent Prognostic Marker in Patients with Tongue Carcinoma—A Retrospective Study. Clin. Otolaryngol. 2018, 43, 1050–1056. [Google Scholar] [CrossRef] [PubMed]
- Vankadara, S.; Padmaja, K.; Balmuri, P.K.; Naresh, G.; Reddy, V. Evaluation of Serum C-Reactive Protein Levels in Oral Premalignancies and Malignancies: A Comparative Study. J. Dent. 2018, 15, 358–364. [Google Scholar] [CrossRef]
- Gosavi, S.R.; Torkadi, A.A. Serum C-Reactive Protein in Oral Submucous Fibrosis and Oral Squamous Cell Carcinoma: A Cross-Sectional Study. J. Oral Maxillofac. Pathol. 2020, 24, 46–51. [Google Scholar] [CrossRef] [PubMed]
- Metgud, R.; Bajaj, S. Altered Serum and Salivary C-Reactive Protein Levels in Patients with Oral Premalignant Lesions and Oral Squamous Cell Carcinoma. Biotech. Histochem. 2016, 91, 96–101. [Google Scholar] [CrossRef]
- Zeng, Y.-C.; Xue, M.; Chi, F.; Xu, Z.-G.; Fan, G.-L.; Wu, R.; Fan, Y.-C.; Zhong, W.-Z.; Wang, S.-L.; Zhang, X.-Y.; et al. C-Reactive Protein Level Predicts Prognosis in Patients with Locoregionally Advanced Laryngeal Carcinoma Treated with Chemoradiotherapy. Tumour Biol. 2012, 33, 891–895. [Google Scholar] [CrossRef] [PubMed]
- Woodley, N.; Rogers, A.D.G.; Turnbull, K.; Slim, M.A.M.; Ton, T.; Montgomery, J.; Douglas, C. Prognostic Scores in Laryngeal Cancer. Eur. Arch. Otorhinolaryngol. 2022, 279, 3705–3715. [Google Scholar] [CrossRef]
- Fang, Y.; Xu, C.; Wu, P.; Zhang, L.-H.; Li, D.-W.; Sun, J.-H.; Li, W.-F.; Liao, Z.-S. Prognostic Role of C-Reactive Protein in Patients with Nasopharyngeal Carcinoma. Medicine 2017, 96, e8463. [Google Scholar] [CrossRef]
- Chen, R.; Zhou, Y.; Yuan, Y.; Zhang, Q.; He, S.; Chen, Y.; Ren, Y. Effect of CRP and Kinetics of CRP in Prognosis of Nasopharyngeal Carcinoma. Front. Oncol. 2019, 9, 89. [Google Scholar] [CrossRef]
- Xia, W.-X.; Ye, Y.-F.; Lu, X.; Wang, L.; Ke, L.-R.; Zhang, H.-B.; Roycik, M.D.; Yang, J.; Shi, J.-L.; Cao, K.-J.; et al. The Impact of Baseline Serum C-Reactive Protein and C-Reactive Protein Kinetics on the Prognosis of Metastatic Nasopharyngeal Carcinoma Patients Treated with Palliative Chemotherapy. PLoS ONE 2013, 8, e76958. [Google Scholar] [CrossRef]
- Wach, J.; Güresir, Á.; Borger, V.; Schuss, P.; Becker, A.; Coch, C.; Schmitz, M.-T.; Hölzel, M.; Toma, M.; Herrlinger, U.; et al. Elevated Baseline C-Reactive Protein Levels Predict Poor Progression-Free Survival in Sporadic Vestibular Schwannoma. J. Neurooncol. 2022, 156, 365–375. [Google Scholar] [CrossRef]
- Radziunas, A.; Tamasauskas, S.; Deltuva, V.P.; Tamasauskas, A.; Bunevicius, A. Greater High-Sensitivity C-Reactive Protein and Interleukin-6 Concentrations Are Associated with Greater Mood and Anxiety Symptoms and Worse Cognitive Functioning of Acoustic Neuroma Patients. J. Neurol. Surg. B Skull Base 2016, 77, FP-18. [Google Scholar] [CrossRef]
- Marques, P.; De, V.F.; Van, F.W.; Korbonits, M.; Biermasz, N.; Pereira, A.M. Pre-Operative Full Blood Count, C-Reactive Protein and Serum Inflammation-Based Scores May Predict Aggressive or Refractory Disease in Patients with Pituitary Adenomas. Endocr. Abstr. 2020, 70, EP295. [Google Scholar]
- Feng, Y.; Wang, J.; Tan, D.; Cheng, P.; Wu, A. Relationship between Circulating Inflammatory Factors and Glioma Risk and Prognosis: A Meta-analysis. Cancer Med. 2019, 8, 7454–7468. [Google Scholar] [CrossRef] [PubMed]
- Wach, J.; Apallas, S.; Schneider, M.; Güresir, A.; Schuss, P.; Herrlinger, U.; Vatter, H.; Güresir, E. Baseline Serum C-Reactive Protein and Plasma Fibrinogen-Based Score in the Prediction of Survival in Glioblastoma. Front. Oncol. 2021, 11, 653614. [Google Scholar] [CrossRef] [PubMed]
- Dharmajaya, R.; Sari, D.K. Role and Value of Inflammatory Markers in Brain Tumors: A Case Controlled Study. Ann. Med. Surg. 2021, 63, 102107. [Google Scholar] [CrossRef]
- Prost, S.; Bouthors, C.; Fuentes, S.; Charles, Y.-P.; Court, C.; Mazel, C.; Blondel, B.; Bonnevialle, P.; Sailhan, F. Influence of Preoperative Biological Parameters on Postoperative Complications and Survival in Spinal Bone Metastasis. Multicent. Prospect. Study Orthop. Traumatol. Surg. Res. 2020, 106, 1033–1038. [Google Scholar] [CrossRef]
- Ozisik, H.; Yurekli, B.S.; Suner, A.; Copur, O.; Sozmen, E.Y.; Ozbek, S.S.; Karabulut, A.K.; Simsir, I.Y.; Erdogan, M.; Cetinkalp, S.; et al. High Chitotriosidase and AGE Levels in Acromegaly: A Case-Control Study. Hormones 2023, 22, 61–69. [Google Scholar] [CrossRef]
- Ozkan, C.; Altinova, A.E.; Cerit, E.T.; Yayla, C.; Sahinarslan, A.; Sahin, D.; Dincel, A.S.; Toruner, F.B.; Akturk, M.; Arslan, M. Markers of Early Atherosclerosis, Oxidative Stress and Inflammation in Patients with Acromegaly. Pituitary 2015, 18, 621–629. [Google Scholar] [CrossRef]
- Kałuzny, M.; Bolanowski, M.; Daroszewski, J.; Szuba, A. The Role of Fibrinogen and CRP in Cardiovascular Risk in Patients with Acromegaly. Endokrynol. Pol. 2010, 61, 83–88. [Google Scholar]
- Seki, Y.; Ichihara, A. Increased Serum High-Sensitivity C-Reactive Protein in Growth Hormone-Deficient Patients with Non-Functioning Pituitary Tumors. J. Endocr. Soc. 2021, 5, A645–A646. [Google Scholar] [CrossRef]
- Sesmilo, G.; Miller, K.K.; Hayden, D.; Klibanski, A. Inflammatory Cardiovascular Risk Markers in Women with Hypopituitarism. J. Clin. Endocrinol. Metab. 2001, 86, 5774–5781. [Google Scholar] [CrossRef]
- Valdivia, D.; Cheufou, D.; Fels, B.; Puhlvers, S.; Mardanzai, K.; Zaatar, M.; Weinreich, G.; Taube, C.; Theegarten, D.; Stuschke, M.; et al. Potential Prognostic Value of Preoperative Leukocyte Count, Lactate Dehydrogenase and C-Reactive Protein in Thymic Epithelial Tumors. Pathol. Oncol. Res. 2021, 27, 629993. [Google Scholar] [CrossRef] [PubMed]
- Bangaraiahgari, R.; Panchangam, R.B.; Bangaraiahgari, R.; U, U.K.; Mayilvaganan, S. Pro-Inflammatory Biomarkers in Papillary Thyroid Cancer. Endocr. Abstr. 2022, 81, EP618. [Google Scholar]
- Shimura, T.; Shibata, M.; Gonda, K.; Matsumoto, Y.; Nakano, K.; Iwadate, M.; Suzuki, S.; Suzuki, S. Prognostic Impact of Elevated Preoperative C-Reactive Protein on Patients with Differentiated Thyroid Carcinoma. J. Surg. Res. 2018, 231, 338–345. [Google Scholar] [CrossRef] [PubMed]
- Eshraghi, M.; Hosseini, S.J.E.; Razavinia, F.S.; Noori, E. Comparative Study of the Level of Inflammatory Factors of Erythrocyte Sedimentation Rate and Reactive Protein C in Benign and Malignant Thyroid Nodules. Pesqui. Bras. Odontopediatria Clín. Integr. 2021, 21, e0052. [Google Scholar] [CrossRef]
- Emam, A.A.; Mousa, S.G.; Ahmed, K.Y.; Al-Azab, A.A. Inflammatory Biomarkers in Patients with Asymptomatic Primary Hyperparathyroidism. Med. Princ. Pract. 2012, 21, 249–253. [Google Scholar] [CrossRef]
- Farahnak, P.; Lärfars, G.; Sten-Linder, M.; Nilsson, I.-L. Mild Primary Hyperparathyroidism: Vitamin D Deficiency and Cardiovascular Risk Markers. J. Clin. Endocrinol. Metab. 2011, 96, 2112–2118. [Google Scholar] [CrossRef]
- Almqvist, E.G.; Bondeson, A.-G.; Bondeson, L.; Svensson, J. Increased Markers of Inflammation and Endothelial Dysfunction in Patients with Mild Primary Hyperparathyroidism. Scand. J. Clin. Lab. Investig. 2011, 71, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Ahlers, A.A.; Schønheyder, H.C. C-reactive protein in patients with infection. Ugeskr Laeger 1990, 153, 13–16. [Google Scholar]
- Korppi, M.; Kröger, L. C-Reactive Protein in Viral and Bacterial Respiratory Infection in Children. Scand. J. Infect. Dis. 1993, 25, 207–213. [Google Scholar] [CrossRef] [PubMed]
- Vanderschueren, S.; Deeren, D.; Knockaert, D.C.; Bobbaers, H.; Bossuyt, X.; Peetermans, W. Extremely Elevated C-Reactive Protein. Eur. J. Intern. Med. 2006, 17, 430–433. [Google Scholar] [CrossRef] [PubMed]
- Ris, T.; Teixeira-Carvalho, A.; Coelho, R.M.P.; Brandao-de-Resende, C.; Gomes, M.S.; Amaral, L.R.; Pinto, P.H.O.M.; Santos, L.J.S.; Salles, J.T.; Roos-Hesselink, J.; et al. Inflammatory Biomarkers in Infective Endocarditis: Machine Learning to Predict Mortality. Clin. Exp. Immunol. 2019, 196, 374–382. [Google Scholar] [CrossRef] [PubMed]
- Urban, S.; Fułek, M.; Błaziak, M.; Iwanek, G.; Jura, M.; Fułek, K.; Guzik, M.; Garus, M.; Gajewski, P.; Lewandowski, Ł.; et al. COVID-19 Related Myocarditis in Adults: A Systematic Review of Case Reports. J. Clin. Med. 2022, 11, 5519. [Google Scholar] [CrossRef] [PubMed]
- Usui, E.; Nagaoka, E.; Ikeda, H.; Ohmori, M.; Tao, S.; Yonetsu, T.; Maejima, Y.; Arai, H.; Amemiya, K.; Ikeda, Y.; et al. Fulminant Myocarditis with COVID-19 Infection Having Normal C-reactive Protein and Serial Magnetic Resonance Follow-up. ESC Heart Fail. 2022, 10, 1426–1430. [Google Scholar] [CrossRef]
- Imazio, M.; Brucato, A.; Maestroni, S.; Cumetti, D.; Dominelli, A.; Natale, G.; Trinchero, R. Prevalence of C-Reactive Protein Elevation and Time Course of Normalization in Acute Pericarditis: Implications for the Diagnosis, Therapy, and Prognosis of Pericarditis. Circulation 2011, 123, 1092–1097. [Google Scholar] [CrossRef]
- Koos, R.; Schröder, J.; Kühl, H.P. Acute viral pericarditis without typical electrocardiographic changes assessed by cardiac magnetic resonance imaging. Eur. Heart J. 2009, 30, 2844. [Google Scholar] [CrossRef] [PubMed]
- McCabe, R.E.; Remington, J.S. C-Reactive Protein in Patients with Bacteremia. J. Clin. Microbiol. 1984, 20, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Crouzet, J.; Faucher, J.-F.; Toubin, M.; Hoen, B.; Estavoyer, J.-M. Serum C-Reactive Protein (CRP) and Procalcitonin (PCT) Levels and Kinetics in Patients with Leptospirosis. Eur. J. Clin. Microbiol. Infect. Dis. 2011, 30, 299–302. [Google Scholar] [CrossRef] [PubMed]
- Le Turnier, P.; Bonifay, T.; Mosnier, E.; Schaub, R.; Jolivet, A.; Demar, M.; Bourhy, P.; Nacher, M.; Djossou, F.; Epelboin, L. Usefulness of C-Reactive Protein in Differentiating Acute Leptospirosis and Dengue Fever in French Guiana. Open Forum Infect. Dis. 2019, 6, ofz323. [Google Scholar] [CrossRef] [PubMed]
- Noursadeghi, M.; Miller, R.F. Clinical Value of C-Reactive Protein Measurements in HIV-Positive Patients. Int. J. STD AIDS 2005, 16, 438–441. [Google Scholar] [CrossRef]
- Sereti, I.; Rodger, A.J.; French, M.A. Biomarkers in Immune Reconstitution Inflammatory Syndrome: Signals from Pathogenesis. Curr. Opin. HIV AIDS 2010, 5, 504–510. [Google Scholar] [CrossRef]
- Bannaga, A.S.; Tabuso, M.; Farrugia, A.; Chandrapalan, S.; Somal, K.; Lim, V.K.; Mohamed, S.; Nia, G.J.; Mannath, J.; Wong, J.L.; et al. C-Reactive Protein and Albumin Association with Mortality of Hospitalised SARS-CoV-2 Patients: A Tertiary Hospital Experience. Clin. Med. 2020, 20, 463–467. [Google Scholar] [CrossRef]
- Ganguly, M.; Nandi, A.; Banerjee, P.; Gupta, P.; Sarkar, S.D.; Basu, S.; Pal, P. A Comparative Study of IL-6, CRP and NT-proBNP Levels in Post-COVID Multisystem Inflammatory Syndrome in Children (MISC) and Kawasaki Disease Patients. Int. J. Rheum. Dis. 2022, 25, 27–31. [Google Scholar] [CrossRef]
- Babu, G.; Ganguly, N.K.; Singhi, S.; Walia, B.N. Value of C-Reactive Protein Concentration in Diagnosis and Management of Acute Lower Respiratory Infections. Trop. Geogr. Med. 1989, 41, 309–315. [Google Scholar]
- Holm, A.; Pedersen, S.S.; Nexoe, J.; Obel, N.; Nielsen, L.P.; Koldkjaer, O.; Pedersen, C. Procalcitonin versus C-Reactive Protein for Predicting Pneumonia in Adults with Lower Respiratory Tract Infection in Primary Care. Br. J. Gen. Pract. 2007, 57, 555–560. [Google Scholar]
- Koster, M.J.; Broekhuizen, B.D.L.; Minnaard, M.C.; Balemans, W.A.F.; Hopstaken, R.M.; de Jong, P.A.; Verheij, T.J.M. Diagnostic Properties of C-Reactive Protein for Detecting Pneumonia in Children. Respir. Med. 2013, 107, 1087–1093. [Google Scholar] [CrossRef]
- van der Meer, V.; Neven, A.K.; van den Broek, P.J.; Assendelft, W.J.J. Diagnostic Value of C Reactive Protein in Infections of the Lower Respiratory Tract: Systematic Review. BMJ 2005, 331, 26. [Google Scholar] [CrossRef]
- Higdon, M.M.; Le, T.; O’Brien, K.L.; Murdoch, D.R.; Prosperi, C.; Baggett, H.C.; Brooks, W.A.; Feikin, D.R.; Hammitt, L.L.; Howie, S.R.C.; et al. Association of C-Reactive Protein with Bacterial and Respiratory Syncytial Virus–Associated Pneumonia Among Children Aged <5 Years in the PERCH Study. Clin. Infect. Dis. 2017, 64, S378–S386. [Google Scholar] [CrossRef] [PubMed]
- Waydande, S.; Deshpande, V.; Reddy, N.; Kumar, S.; Mhaske, S.N.; Shinde, A. The Use of C-Reactive Protein in Predicting Bacterial Co-Infection in Children with Bronchiolitis. Spec. Ugdym. 2022, 2, 570–576. [Google Scholar]
- Isa, H.M.; Mohroofi, A.D.; Alkhan, F.N.; Hasan, A.Z.; Alkubisi, M.M.; Alhewaizem, S.S.; Khalifa, S.I.; Alromaihi, N.G. C-Reactive Protein Levels in Children with Acute Bronchiolitis. Int. J. Pediatr. 2022, 2022, 1311936. [Google Scholar] [CrossRef] [PubMed]
- Costa, S.; Rocha, R.; Tavares, M.; Bonito-Vítor, A.; Guedes-Vaz, L.; João, H.S. C Reactive Protein and Disease Severity in Bronchiolitis. Rev. Port. Pneumol. 2009, 15, 55–65. [Google Scholar] [CrossRef] [PubMed]
- Yoon, C.; Chaisson, L.H.; Patel, S.M.; Drain, P.K.; Wilson, D.; Cattamanchi, A. Diagnostic Accuracy of C-Reactive Protein for Active Pulmonary Tuberculosis: A Systematic Review and Meta-Analysis. Int. J. Tuberc. Lung Dis. 2017, 21, 1013–1019. [Google Scholar] [CrossRef] [PubMed]
- Brown, J.; Clark, K.; Smith, C.; Hopwood, J.; Lynard, O.; Toolan, M.; Creer, D.; Barker, J.; Breen, R.; Brown, T.; et al. Variation in C-Reactive Protein Response According to Host and Mycobacterial Characteristics in Active Tuberculosis. BMC Infect. Dis. 2016, 16, 265. [Google Scholar] [CrossRef] [PubMed]
- Vasileva, D.; Badawi, A. C-Reactive Protein as a Biomarker of Severe H1N1 Influenza. Inflamm. Res. 2019, 68, 39–46. [Google Scholar] [CrossRef]
- Wu, W.; Shi, D.; Fang, D.; Guo, F.; Guo, J.; Huang, F.; Chen, Y.; Lv, L.; Li, L. A New Perspective on C-Reactive Protein in H7N9 Infections. Int. J. Infect. Dis. 2016, 44, 31–36. [Google Scholar] [CrossRef] [PubMed]
- Lindbäck, S.; Hellgren, U.; Julander, I.; Hansson, L.-O. The Value of C-Reactive Protein as a Marker of Bacterial Infection in Patients with Septicaemia/Endocarditis and Influenza. Scand. J. Infect. Dis. 1989, 21, 543–549. [Google Scholar] [CrossRef] [PubMed]
- Haran, J.P.; Beaudoin, F.L.; Suner, S.; Lu, S. C-Reactive Protein as Predictor of Bacterial Infection among Patients with an Influenza-like Illness. Am. J. Emerg. Med. 2013, 31, 137–144. [Google Scholar] [CrossRef]
- Wang, C.; Zhang, H.; Zhang, Y.; Xu, L.; Miao, M.; Yang, H.; Liu, Y.; He, S.; Pang, L. Analysis of Clinical Characteristics of Severe Pertussis in Infants and Children: A Retrospective Study. BMC Pediatr. 2021, 21, 65. [Google Scholar] [CrossRef] [PubMed]
- Kuwabara, M.; Tanemori, N.; Kawaguti, Y.; Nakamura, K.; Nomiyama, S.; Terada, M.; Mitsutou, Y.; Imura, K.; Yamakido, M. Clinical features of 36 cases of psittacosis. Kansenshogaku Zasshi 1990, 64, 498–503. [Google Scholar] [CrossRef]
- Paul, R.; Bhattacharya, R.; Raychaudhuri, P.; Sinha, P.; Banerjee, A.; Mondal, J. Study of C Reactive Protein as a Prognostic Marker in Malaria from Eastern India. Adv. Biomed. Res. 2012, 1, 41. [Google Scholar] [CrossRef]
- Wilairatana, P.; Mahannop, P.; Tussato, T.; Hayeedoloh, I.; Boonhok, R.; Klangbud, W.K.; Mala, W.; Kotepui, K.U.; Kotepui, M. C-Reactive Protein as an Early Biomarker for Malaria Infection and Monitoring of Malaria Severity: A Meta-Analysis. Sci. Rep. 2021, 11, 22033. [Google Scholar] [CrossRef]
- Krel, M.; Petraitis, V.; Petraitiene, R.; Jain, M.R.; Zhao, Y.; Li, H.; Walsh, T.J.; Perlin, D.S. Host Biomarkers of Invasive Pulmonary Aspergillosis To Monitor Therapeutic Response. Antimicrob. Agents Chemother. 2014, 58, 3373–3378. [Google Scholar] [CrossRef]
- Chai, L.A.; Netea, M.G.; Teerenstra, S.; Earnest, A.; Vonk, A.G.; Schlamm, H.T.; Herbrecht, R.; Troke, P.F.; Kullberg, B.J. Early Proinflammatory Cytokines and C-reactive Protein Trends as Predictors of Outcome in Invasive Aspergillosis. J. Infect. Dis. 2010, 202, 1454–1462. [Google Scholar] [CrossRef] [PubMed]
- Ishida, Y.; Suzuki, K.; Taki, K.; Niwa, T.; Kurotsuchi, S.; Ando, H.; Iwase, A.; Nishio, K.; Wakai, K.; Ito, Y.; et al. Significant Association between Helicobacter Pylori Infection and Serum C-Reactive Protein. Int. J. Med. Sci. 2008, 5, 224–229. [Google Scholar] [CrossRef] [PubMed]
- Pourcyrous, M.; Korones, S.B.; Yang, W.; Boulden, T.F.; Bada, H.S. C-Reactive Protein in the Diagnosis, Management, and Prognosis of Neonatal Necrotizing Enterocolitis. Pediatrics 2005, 116, 1064–1069. [Google Scholar] [CrossRef] [PubMed]
- Ibrohim, I.S.; Pratama, H.A.; Fauzi, A.R.; Iskandar, K.; Agustriani, N. Gunadi Association between Prognostic Factors and the Clinical Deterioration of Preterm Neonates with Necrotizing Enterocolitis. Sci. Rep. 2022, 12, 13911. [Google Scholar] [CrossRef] [PubMed]
- Borgnolo, G.; Barbone, F.; Guidobaldi, G.; Olivo, G. C-Reactive Protein in Viral and Bacterial Gastroenteritis in Childhood. Acta Paediatr. 1996, 85, 670–674. [Google Scholar] [CrossRef]
- Marcus, N.; Mor, M.; Amir, L.; Mimouni, M.; Waisman, Y. The Quick-Read C-Reactive Protein Test for the Prediction of Bacterial Gastroenteritis in the Pediatric Emergency Department. Pediatr. Emerg. Care 2007, 23, 634–637. [Google Scholar] [CrossRef]
- Szalai, A.J.; VanCott, J.L.; McGhee, J.R.; Volanakis, J.E.; Benjamin, W.H. Human C-Reactive Protein Is Protective against Fatal Salmonella Enterica Serovar Typhimurium Infection in Transgenic Mice. Infect. Immun. 2000, 68, 5652–5656. [Google Scholar] [CrossRef]
- Meloni, G.F.; Tomasi, P.A.; Spanu, P.; Piga, S.; Porcu, A. C-reactive protein levels for diagnosis of salmonella gastroenteritis. Pediatr. Infect. Dis. J. 1999, 18, 471. [Google Scholar] [CrossRef] [PubMed]
- Al-Haboobi, Z.A.; Jasim, A.K.A.; Al-Quraishi, M.A. The Pattern of Leucocytes Parameters and C-reactive Protein Findings of G. lamblia and E. histolytica Intestinal Infections in Children. Int. J. Rec. Biotech. 2013, 1, 5–14. [Google Scholar]
- Choo, K.E.; Davis, T.M.E.; Henry, R.L.; Chan, L.P. Serum C-Reactive Protein Concentrations in Malaysian Children with Enteric Fever. J. Trop. Pediatr. 2001, 47, 211–214. [Google Scholar] [CrossRef] [PubMed]
- Tan, J.P.L.; Barazanchi, A.W.H.; Singh, P.P.; Hill, A.G.; Maccormick, A.D. Predictors of Acute Diverticulitis Severity: A Systematic Review. Int. J. Surg. 2016, 26, 43–52. [Google Scholar] [CrossRef] [PubMed]
- Kechagias, A.; Sofianidis, A.; Zografos, G.; Leandros, E.; Alexakis, N.; Dervenis, C. Index C-Reactive Protein Predicts Increased Severity in Acute Sigmoid Diverticulitis. Ther. Clin. Risk Manag. 2018, 14, 1847–1853. [Google Scholar] [CrossRef]
- Mousa, N.; Besheer, T.; Abdel-Razik, A.; Hamed, M.; Deiab, A.; Sheta, T.; Eldars, W. Can Combined Blood Neutrophil to Lymphocyte Ratio and C-Reactive Protein Be Used for Diagnosis of Spontaneous Bacterial Peritonitis? Br. J. Biomed. Sci. 2018, 75, 71–75. [Google Scholar] [CrossRef]
- Yuan, L.-Y.; Ke, Z.-Q.; Wang, M.; Li, Y. Procalcitonin and C-Reactive Protein in the Diagnosis and Prediction of Spontaneous Bacterial Peritonitis Associated with Chronic Severe Hepatitis B. Ann. Lab. Med. 2013, 33, 449–454. [Google Scholar] [CrossRef]
- Havens, W.P.; Eichman, H.L.; Knowlton, M. Failure to Find C-Reactive Protein in Viral Hepatitis. Exp. Biol. Med. 1950, 75, 108–110. [Google Scholar] [CrossRef]
- Singh, S.; Bansal, A.; Kumar, P. CRP Levels in Viral Hepatitis: A Meta-Analysis Study. Int. J. Infect. 2021, 8. [Google Scholar] [CrossRef]
- Shima, M.; Nakao, K.; Kato, Y.; Nakata, K.; Ishii, N.; Nagataki, S. Comparative Study of C-Reactive Protein in Chronic Hepatitis B and Chronic Hepatitis C. Tohoku J. Exp. Med. 1996, 178, 287–297. [Google Scholar] [CrossRef]
- Ozaras, R.; Mert, A.; Yilmaz, M.H.; Celik, A.D.; Tabak, F.; Bilir, M.; Ozturk, R. Acute Viral Cholecystitis Due to Hepatitis A Virus Infection. J. Clin. Gastroenterol. 2003, 37, 79. [Google Scholar] [CrossRef] [PubMed]
- Fajardo, J.; Núñez, E.; Szafranska, J.; Poca, M.; Lobo, D.; Martín, B.; Hernández, D.; Roig, C.; Huerta, A.; Corominas, H.; et al. We Report a Patient Who Presented Intrahepatic Cholangitis and Cholecystitis after SARS-CoV-2 Infection. J. Gastroenterol. Hepatol. 2021, 36, 2037. [Google Scholar] [CrossRef]
- Lagona, E.; Sharifi, F.; Voutsioti, A.; Mavri, A.; Markouri, M.; Attilakos, A. Epstein-Barr Virus Infectious Mononucleosis Associated with Acute Acalculous Cholecystitis. Infection 2007, 35, 118–119. [Google Scholar] [CrossRef] [PubMed]
- Gomes, M.M.; Antunes, H.; Lobo, A.L.; Branca, F.; Correia-Pinto, J.; Moreira-Pinto, J. Acute Alithiasic Cholecystitis and Human Herpes Virus Type-6 Infection: First Case. Case Rep. Pediatr. 2016, 2016, e9130673. [Google Scholar] [CrossRef] [PubMed]
- Ono, S.K.; Bassit, L.; Van Vaisberg, V.; Alves, V.A.F.; Caldini, E.G.; Herman, B.D.; Shabman, R.; Fedorova, N.B.; Paranaguá-Vezozzo, D.; Sampaio, C.T.; et al. Acute Acalculous Cholecystitis during Zika Virus Infection in an Immunocompromised Patient. Hepatology 2018, 67, 2051–2054. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H.; Park, S.; Choi, J. Acalculous Cholecystitis Associated with Hantaan Virus: A Case Report. Ann. Hepatobiliary Pancreat. Surg. 2019, 23, 278–281. [Google Scholar] [CrossRef] [PubMed]
- Setyawati, A.N.; Tjahjono Dk, K.; Chionardes, M.A.; Arkhaesi, N. Acute Acalculous Cholecystitis in a Pediatric Dengue Hemorrhagic Fever Patient: A Case Report, Lesson Learned from Limited Resource Setting. Ann. Med. Surg. 2022, 81, 104437. [Google Scholar] [CrossRef] [PubMed]
- Gunal, E.K.; Topkaya, A.E.; Arisoy, A.; Aydiner, O.; Gökçen, G.; Aksungar, F.B.; Karabulut, M.; Tulbek, M.Y.; Aytug, O.N. Cholecystitis Related to Brucella Melitensis: A Rare Presentation. Infect. Dis. Clin. Pract. 2008, 16, 134. [Google Scholar] [CrossRef]
- Clerckx, C.; Yombi, J.-C.; Belkhir, L.; Vandercam, B. O Measles-Associated Acute Acalculous Cholecystitis. Adv. Infect. Dis. 2012, 2, 25304. [Google Scholar] [CrossRef]
- Azizia, M.M.; Irvine, L.M.; Coker, M.; Sanusi, F.A. The Role of C-Reactive Protein in Modern Obstetric and Gynecological Practice. Acta Obstet. Gynecol. Scand. 2006, 85, 394–401. [Google Scholar] [CrossRef] [PubMed]
- Chuang, Y.-C.; Tyagi, V.; Liu, R.-T.; Chancellor, M.B.; Tyagi, P. Urine and Serum C-Reactive Protein Levels as Potential Biomarkers of Lower Urinary Tract Symptoms. Urol. Sci. 2010, 21, 132–136. [Google Scholar] [CrossRef]
- Xu, R.-Y.; Liu, H.-W.; Liu, J.-L.; Dong, J.-H. Procalcitonin and C-Reactive Protein in Urinary Tract Infection Diagnosis. BMC Urol. 2014, 14, 45. [Google Scholar] [CrossRef] [PubMed]
- Gervaix, A.; Galetto-Lacour, A.; Gueron, T.; Vadas, L.; Zamora, S.; Suter, S.; Girardin, E. Usefulness of Procalcitonin and C-Reactive Protein Rapid Tests for the Management of Children with Urinary Tract Infection. Pediatr. Infect. Dis. J. 2001, 20, 507. [Google Scholar] [CrossRef] [PubMed]
- Hellerstein, S.; Duggan, E.; Welchert, E.; Mansour, F. Serum C-Reactive Protein and the Site of Urinary Tract Infections. J. Pediatr. 1982, 100, 21–25. [Google Scholar] [CrossRef]
- Terao, M.; Koga, K.; Fujimoto, A.; Wada-Hiraike, O.; Osuga, Y.; Yano, T.; Kozuma, S. Factors That Predict Poor Clinical Course among Patients Hospitalized with Pelvic Inflammatory Disease: Factors Related to Poor Course of PID. J. Obstet. Gynaecol. Res. 2014, 40, 495–500. [Google Scholar] [CrossRef]
- Miettinen, A.K.; Heinonen, P.K.; Laippala, P.; Paavonen, J. Test Performance of Erythrocyte Sedimentation Rate and C-Reactive Protein in Assessing the Severity of Acute Pelvic Inflammatory Disease. Am. J. Obstet. Gynecol. 1993, 169, 1143–1149. [Google Scholar] [CrossRef]
- Demirtas, O.; Akman, L.; Demirtas, G.S.; Hursitoglu, B.S.; Yilmaz, H. The Role of the Serum Inflammatory Markers for Predicting the Tubo-Ovarian Abscess in Acute Pelvic Inflammatory Disease: A Single-Center 5-Year Experience. Arch. Gynecol. Obstet. 2013, 287, 519–523. [Google Scholar] [CrossRef] [PubMed]
- Tokmak, A.; Özer, İ.; Erkilinç, S.; Güzel, A.; Kokanali, M.; Uğur, M. Vaginal Washing Fluid C-Reactive Protein Levels in Women with Recurrent or Treatment Resistant Vaginitis. J. Clin. Exp. Invest. 2015, 6, 5–9. [Google Scholar] [CrossRef]
- Batrakova, T.V.; Zazerskaya, I.E.; Vavilova, T.V.; Kustarov, V.N. Clinical value of c-reactive protein level in predicting the development of postpartum endometritis. J. Obstet. Women’s Dis. 2020, 69, 5–14. [Google Scholar] [CrossRef]
- Zhao, C.; Chen, X.; Qu, F.; Xie, H.; Cui, H. Study on the correlation analysis and the mechanism of PCT, CRP level and the puerperal infection after cesarean section. J. Chin. Phys. 2018, 554–557. [Google Scholar]
- Aggarwal, A.; Pahwa, S. Evaluation of the Role of CRP as an Early Predictor of Chorioamnionitis in PPROM. International. J. Reprod. Contracept. Obstet. Gynecol. 2018, 7, 1351–1357. [Google Scholar] [CrossRef]
- Wiwanitkit, V. Maternal C-Reactive Protein for Detection of Chorioamnionitis: An Appraisal. Infect. Dis. Obstet. Gynecol. 2005, 13, 179–181. [Google Scholar] [CrossRef]
- Smith, E.J.; Muller, C.L.; Sartorius, J.A.; White, D.R.; Maslow, A.S. C-Reactive Protein as a Predictor of Chorioamnionitis. J. Osteopat. Med. 2012, 112, 660–664. [Google Scholar]
- Schrödl, W.; Krüger, M.; Hien, T.T.; Füldner, M.; Kunze, R. C-reactive protein as a new parameter of mastitis. Tierarztl. Prax. 1995, 23, 337–341. [Google Scholar] [PubMed]
- Mansour, T.; Yehudai, N.; Tobia, A.; Shihada, R.; Brodsky, A.; Khnifies, R.; Barzilai, R.; Srugo, I.; Luntz, M. Acute Mastoiditis: 20 Years of Experience with a Uniform Management Protocol. Int. J. Pediatr. Otorhinolaryngol. 2019, 125, 187–191. [Google Scholar] [CrossRef] [PubMed]
- Trojian, T.H.; Lishnak, T.S.; Heiman, D. Epididymitis and Orchitis: An Overview. AFP 2009, 79, 583–587. [Google Scholar]
- Ahn, H.K.; Koo, K.C.; Chung, B.H.; Lee, K.S. Comparison of the Delta Neutrophil Index with Procalcitonin, Erythrocyte Sedimentation Rate, and C-Reactive Protein as Predictors of Sepsis in Patients with Acute Prostatitis. Prostate Int. 2018, 6, 157–161. [Google Scholar] [CrossRef]
- Girgis, S.M.; Ekladios, E.; Iskandar, R.M.; El-Haggar, S.; Moemen, N.; El-Kassem, S.M.A. C-Reactive Protein in Semen and Serum of Men with Chronic Prostatitis. Andrologia 2009, 15, 151–154. [Google Scholar] [CrossRef] [PubMed]
- Jansen, M.; van Ess, E.; Ouburg, S.; Gerds, M.; Morré, S.; Land, J. C-reactive protein as a marker of persistent Chlamydia trachomatis infection is not associated with tubal factor infertility—An independent clinical validation study. Human Reprod. Open 2019, 2019, hoz029. [Google Scholar] [CrossRef]
- Tseng, Y.-T.; Chou, P.-Y.; Tai, M.-H.; Dai, C.-Y.; Lee, S.S.-J.; Chen, Y.-S.; Tsai, H.-C.; Chen, Y.-H. High Baseline C-Reactive Protein Level Can Predict the Occurrence of the Jarisch–Herxheimer Reaction in Patients with Active Syphilis. Infect. Drug Resist. 2021, 14, 5121–5129. [Google Scholar] [CrossRef]
- Joo, E.-J.; Chang, Y.; Kwon, M.-J.; Cho, A.; Cheong, H.S.; Ryu, S. High-Risk Human Papillomavirus Infection and the Risk of Cardiovascular Disease in Korean Women: A Cohort Study. Circ. Res. 2019, 124, 747–756. [Google Scholar] [CrossRef] [PubMed]
- Johnson-Obaseki, S.; Caulley, L.; Corsten, M.; Liu, G.; Dimitroulakos, J.; Goldstein, D.; Irish, J.; Rider, J. C-reactive Protein in HPV-Positive and HPV-Negative Oropharyngeal Cancer. Otolaryngol. Head Neck Surg. 2019, 160, 494–501. [Google Scholar] [CrossRef] [PubMed]
- Ryan, E.C.; Ahn, J.; Wukich, D.K.; Kim, P.J.; La Fontaine, J.; Lavery, L.A. Diagnostic Utility of Erythrocyte Sedimentation Rate and C-Reactive Protein in Osteomyelitis of the Foot in Persons without Diabetes. J. Foot Ankle Surg. 2019, 58, 484–488. [Google Scholar] [CrossRef]
- van Asten, S.A.; Jupiter, D.C.; Mithani, M.; La Fontaine, J.; Davis, K.E.; Lavery, L.A. Erythrocyte Sedimentation Rate and C-reactive Protein to Monitor Treatment Outcomes in Diabetic Foot Osteomyelitis. Int. Wound J. 2016, 14, 142–148. [Google Scholar] [CrossRef] [PubMed]
- Soleimani, Z.; Amighi, F.; Vakili, Z.; Momen-Heravi, M.; Moravveji, S.A. Diagnostic Value of Procalcitonin, Erythrocyte Sedimentation Rate (ESR), Quantitative C-Reactive Protein (CRP) and Clinical Findings Associated with Osteomyelitis in Patients with Diabetic Foot. Hum. Antibodies 2021, 29, 115–121. [Google Scholar] [CrossRef] [PubMed]
- Lavery, L.A.; Ahn, J.; Ryan, E.C.; Bhavan, K.; Oz, O.K.; La Fontaine, J.; Wukich, D.K. What Are the Optimal Cutoff Values for ESR and CRP to Diagnose Osteomyelitis in Patients with Diabetes-Related Foot Infections? Clin. Orthop. Relat. Res. 2019, 477, 1594–1602. [Google Scholar] [CrossRef] [PubMed]
- Lee, H.T.; Pukenas, B.A.; Sebro, R. Change in Bone CT Attenuation and C-Reactive Protein Are Predictors of Bone Biopsy Culture Positivity in Patients with Vertebral Discitis/Osteomyelitis. Spine 2020, 45, 1208. [Google Scholar] [CrossRef] [PubMed]
- Yan, D.; Song, Y. Diagnostic Value of Erythrocyte Sedimentation Rate Combined with C-Reactive Protein in Postprocedure Discitis. Curr. Orthop. Pract. 2012, 23, 567–571. [Google Scholar] [CrossRef]
- Levine, M.J.; McGuire, K.J.; McGowan, K.L.; Flynn, J.M. Assessment of the Test Characteristics of C-Reactive Protein for Septic Arthritis in Children. J. Pediatr. Orthop. 2003, 23, 373. [Google Scholar] [CrossRef]
- Basmaci, R.; Ilharreborde, B.; Bonacorsi, S.; Kahil, M.; Mallet, C.; Aupiais, C.; Doit, C.; Dugué, S.; Lorrot, M. Septic arthritis in children with normal initial C-reactive protein: Clinical and biological features. Arch. Pediatr. 2014, 21, 1195–1199. [Google Scholar] [CrossRef] [PubMed]
- Peltola, H.; Vahvanen, V.; Aalto, K. Fever, C-Reactive Protein, and Erythrocyte Sedimentation Rate in Monitoring Recovery from Septic Arthritis: A Preliminary Study. J. Pediatr. Orthop. 1984, 4, 170–174. [Google Scholar] [CrossRef]
- Karppelin, M.; Siljander, T.; Aittoniemi, J.; Hurme, M.; Huttunen, R.; Huhtala, H.; Kere, J.; Vuopio, J.; Syrjänen, J. Predictors of Recurrent Cellulitis in Five Years. Clinical Risk Factors and the Role of PTX3 and CRP. J. Infect. 2015, 70, 467–473. [Google Scholar] [CrossRef]
- Eriksson, B.; Jorup-Rönström, C.; Karkkonen, K.; Sjöblom, A.C.; Holm, S.E. Erysipelas: Clinical and Bacteriologic Spectrum and Serological Aspects. Clin. Infect. Dis. 1996, 23, 1091–1098. [Google Scholar] [CrossRef] [PubMed]
- Nevet, A.; Yarden-Bilavsky, H.; Ashkenazi, S.; Livni, G. C-Reactive Protein Levels in Children with Primary Herpetic Gingivostomatitis. Isr. Med. Assoc. J. 2014, 16, 700–702. [Google Scholar]
- Oskay, T.; Keskin, C.; Özen, M. Antioxidant and Inflammatory Biomarkers in Herpes Zoster. J. Med. Virol. 2022, 94, 3924–3929. [Google Scholar] [CrossRef] [PubMed]
- Silva, E.A.; Iyer, A.; Ura, S.; Lauris, J.R.; Naafs, B.; Das, P.K.; Vilani-Moreno, F. Utility of Measuring Serum Levels of Anti-PGL-I Antibody, Neopterin and C-Reactive Protein in Monitoring Leprosy Patients during Multi-Drug Treatment and Reactions: Monitoring Leprosy Patients. Trop. Med. Int. Health 2007, 12, 1450–1458. [Google Scholar] [CrossRef] [PubMed]
- Ridley, M.J.; Ridley, D.S.; De Beer, F.C.; Pepys, M.B. C-Reactive Protein and ApoB Containing Lipoproteins Are Associated with Mycobacterium Leprae in Lesions of Human Leprosy. Clin. Exp. Immunol. 1984, 56, 545–552. [Google Scholar] [PubMed]
- Uhde, M.; Ajamian, M.; Li, X.; Wormser, G.P.; Marques, A.; Alaedini, A. Expression of C-Reactive Protein and Serum Amyloid A in Early to Late Manifestations of Lyme Disease. Clin. Infect. Dis. 2016, 63, 1399–1404. [Google Scholar] [CrossRef]
- Ashdown, L.R. Serial Serum C-Reactive Protein Levels as an Aid to the Management of Melioidosis. Am. J. Trop. Med. Hyg. 1992, 46, 151–157. [Google Scholar] [CrossRef]
- Cheng, A.C.; O’brien, M.; Jacups, S.P.; Anstey, N.M.; Currie, A.B.J. C-reactive protein in the diagnosis of melioidosis. Am. J. Trop. Med. Hyg. 2004, 70, 580–582. [Google Scholar] [CrossRef]
- Syrjälä, H. Peripheral Blood Leukocyte Counts, Erythrocyte Sedimentation Rate and C-Reactive Protein in Tularemia Caused by the Type B Strain of Francisella Tularensis. Infection 1986, 14, 51–54. [Google Scholar] [CrossRef]
- Komaroff, A.L.; Pass, T.M.; Aronson, M.D.; Ervin, C.T.; Cretin, S.; Winickoff, R.N.; Branch, W.T. The Prediction of Streptococcal Pharyngitis in Adults. J. Gen. Intern. Med. 1986, 1, 1–7. [Google Scholar] [CrossRef]
- Calviño, O.; Llor, C.; Gómez, F.; González, E.; Sarvisé, C.; Hernández, S. Association between C-Reactive Protein Rapid Test and Group A Streptococcus Infection in Acute Pharyngitis. J. Am. Board. Fam. Med. 2014, 27, 424–426. [Google Scholar] [CrossRef] [PubMed]
- Spiekermann, C.; Russo, A.; Stenner, M.; Rudack, C.; Roth, J.; Vogl, T. Increased Levels of S100A8/A9 in Patients with Peritonsillar Abscess: A New Promising Diagnostic Marker to Differentiate between Peritonsillar Abscess and Peritonsillitis. Dis. Markers 2017, 2017, e9126560. [Google Scholar] [CrossRef]
- Strati, I.; Copelovici, Y.; Cajal, N.; Marinescu, G.; Vulcan, V. Presence of C-reactive protein in the development of acute mumps infection. Preliminary report. Virologie 1987, 38, 121–125. [Google Scholar]
- Lindbaek, M.; Hjortdahl, P. The Clinical Diagnosis of Acute Purulent Sinusitis in General Practice—A Review. Br. J. Gen. Pract. 2002, 52, 491–495. [Google Scholar] [PubMed]
- Bjerrum, L.; Gahrn-Hansen, B.; Munck, A.P. C-Reactive Protein Measurement in General Practice May Lead to Lower Antibiotic Prescribing for Sinusitis. Br. J. Gen. Pract. 2004, 54, 659–662. [Google Scholar] [PubMed]
- Groen-Hakan, F.; Eurelings, L.; van Laar, J.; Rothova, A. Relevance of Erythrocyte Sedimentation Rate and C-Reactive Protein in Patients with Active Uveitis. Graefes Arch. Clin. Exp. Ophthalmol. 2019, 257, 175–180. [Google Scholar] [CrossRef]
- Tejani, N.R.; Chonmaitree, T.; Rassin, D.K.; Howie, V.M.; Owen, M.J.; Goldman, A.S. Use of C-Reactive Protein in Differentiation between Acute Bacterial and Viral Otitis Media. Pediatrics 1995, 95, 664–669. [Google Scholar] [PubMed]
- Peltola, H. C-reactive protein for rapid monitoring of infections of the central nervous system. Lancet 1982, 319, 980–983. [Google Scholar] [CrossRef]
- Sormunen, P.; Kallio, M.J.T.; Kilpi, T.; Peltola, H. C-Reactive Protein Is Useful in Distinguishing Gram Stain–Negative Bacterial Meningitis from Viral Meningitis in Children. J. Pediatr. 1999, 134, 725–729. [Google Scholar] [CrossRef] [PubMed]
- Sanaei Dashti, A.; Alizadeh, S.; Karimi, A.; Khalifeh, M.; Shoja, S.A. Diagnostic Value of Lactate, Procalcitonin, Ferritin, Serum-C-Reactive Protein, and Other Biomarkers in Bacterial and Viral Meningitis. Medicine 2017, 96, e7637. [Google Scholar] [CrossRef]
- Hansson, L.-O.; Axelsson, G.; Linne, T.; Aurelius, E.; Lindquist, L. Serum C-Reactive Protein in the Differential Diagnosis of Acute Meningitis. Scand. J. Infect. Dis. 1993, 25, 625–630. [Google Scholar] [CrossRef] [PubMed]
- Mouliou, D.S.; Dardiotis, E. Temelimab for MS and SARS-CoV-2: Could It Be a Double-Edged Blessing? Mult. Scler. Relat. Disord. 2022, 64, 103938. [Google Scholar] [CrossRef]
- Lanzillo, R.; Liuzzi, R.; Vallefuoco, L.; Moccia, M.; Amato, L.; Vacca, G.; Vacchiano, V.; Portella, G.; Brescia Morra, V. JC Virus Antibody Index in Natalizumab-Treated Patients: Correlations with John Cunningham Virus DNA and C-Reactive Protein Level. Ther. Clin. Risk Manag. 2014, 10, 807–814. [Google Scholar] [CrossRef] [PubMed]
- Tosun, S.; Batirel, A.; Oluk, A.I.; Aksoy, F.; Puca, E.; Bénézit, F.; Ural, S.; Nayman-Alpat, S.; Yamazhan, T.; Koksaldi-Motor, V.; et al. Tetanus in Adults: Results of the Multicenter ID-IRI Study. Eur. J. Clin. Microbiol. Infect. Dis. 2017, 36, 1455–1462. [Google Scholar] [CrossRef] [PubMed]
- Moynan, D.; O’Riordan, R.; O’Connor, R.; Merry, C. Tetanus—A Rare But Real Threat. IDCases 2018, 12, 16–17. [Google Scholar] [CrossRef]
- Yamashita, P.; Kelsey, J.; Henderson, S.O. Subcutaneous Cysticercosis. J. Emerg. Med. 1998, 16, 583–586. [Google Scholar] [CrossRef]
- Matesanz, J.L.; Fernández, E.; Fernández, J.M.; Viejo, G. Plasma Procalcitonin and C-Reactive Protein Concentrations in Pediatric Patients with Epstein–Barr Virus Infection. Clin. Chem. 2003, 49, 2103–2104. [Google Scholar] [CrossRef] [PubMed]
- Zhu, J.; Quyyumi, A.A.; Norman, J.E.; Csako, G.; Epstein, S.E. Cytomegalovirus in the Pathogenesis of Atherosclerosis. J. Am. Coll. Cardiol. 1999, 34, 1738–1743. [Google Scholar] [CrossRef]
- Tappe, D.; Nachtigall, S.; Kapaun, A.; Schnitzler, P.; Günther, S.; Schmidt-Chanasit, J. Acute Zika Virus Infection after Travel to Malaysian Borneo, September 2014. Emerg. Infect. Dis. 2015, 21, 911–913. [Google Scholar] [CrossRef]
- Hunt, L.; Gupta-Wright, A.; Simms, V.; Tamba, F.; Knott, V.; Tamba, K.; Heisenberg-Mansaray, S.; Tamba, E.; Sheriff, A.; Conteh, S.; et al. Clinical Presentation, Biochemical, and Haematological Parameters and Their Association with Outcome in Patients with Ebola Virus Disease: An Observational Cohort Study. Lancet Infect. Dis. 2015, 15, 1292–1299. [Google Scholar] [CrossRef]
- Navarro, J.M.; Mendoza, J.; Leiva, J.; Rodríguez-Contreras, R.; de la Rosa, M. C-Reactive Protein as a Prognostic Indicator in Acute Brucellosis. Diagn. Microbiol. Infect. Dis. 1990, 13, 269–270. [Google Scholar] [CrossRef] [PubMed]
- Kosmidou, M.; Papamichail, G.; Klouras, E.; Tsamis, K.; Sarmas, I.; Rapti, I.; Milionis, H. Trichinosis Imitating an Inflammatory Systematic Disease. Korean J. Parasitol. 2021, 59, 497–499. [Google Scholar] [CrossRef]
- Strle, F. Human Granulocytic Ehrlichiosis in Europe. Int. J. Med. Microbiol. Suppl. 2004, 293, 27–35. [Google Scholar] [CrossRef]
- Sasaki, T.; Matsumoto, N.; Nakao, H.; Katoh, T.; Fukuda, Y.; Nakazato, M.; Okayama, A. An Outbreak of Legionnaires’ Disease Associated with a Circulating Bathwater System at a Public Bathhouse. I: A Clinical Analysis. J. Infect. Chemother. 2008, 14, 117–122. [Google Scholar] [CrossRef]
- Caicedo, Y.; Paez, A.; Kuzmin, I.; Niezgoda, M.; Orciari, L.A.; Yager, P.A.; Recuenco, S.; Franka, R.; Velasco-Villa, A.; Willoughby, R.E. Virology, Immunology and Pathology of Human Rabies During Treatment. Pediatr. Infect. Dis. J. 2015, 34, 520–528. [Google Scholar] [CrossRef] [PubMed]
- Reach, P.; Paugam, A.; Kahan, A.; Allanore, Y.; Wipff, J. Coccidioidomycosis of the Spine in an Immunocompetent Patient. Jt. Bone Spine 2010, 77, 611–613. [Google Scholar] [CrossRef]
- Reed, W.B.; Heiskell, C.L.; Holeman, C.W.; Carpenter, C. Serum protein profiles in coccidioidomycosis. Calif. Med. 1962, 97, 333–337. [Google Scholar] [PubMed]
- Bories, P.; Zink, E.; Mattern, J.F.; Villard, O.; Berceanu, A.; Bilger, K.; Candolfi, E.; Herbrecht, R.; Abou-Bacar, A.; Lioure, B. Febrile Pancytopenia as Uncommon Presentation of Disseminated Toxoplasmosis after BMT. Bone Marrow Transpl. 2012, 47, 301–303. [Google Scholar] [CrossRef] [PubMed]
- Sandri, V.; Gonçalves, I.L.; Machado das Neves, G.; Romani Paraboni, M.L. Diagnostic Significance of C-Reactive Protein and Hematological Parameters in Acute Toxoplasmosis. J. Parasit. Dis. 2020, 44, 785–793. [Google Scholar] [CrossRef]
- Qadri, F.; Raqib, R.; Ahmed, F.; Rahman, T.; Wenneras, C.; Das, S.K.; Alam, N.H.; Mathan, M.M.; Svennerholm, A.-M. Increased Levels of Inflammatory Mediators in Children and Adults Infected with Vibrio Cholerae O1 and O139. Clin. Diagn. Lab. Immunol. 2002, 9, 221–229. [Google Scholar] [CrossRef]
- Ozturk, B.; Tutuncu, E.; Kuscu, F.; Gurbuz, Y.; Sencan, I.; Tuzun, H. Evaluation of Factors Predictive of the Prognosis in Crimean-Congo Hemorrhagic Fever: New Suggestions. Int. J. Infect. Dis. 2012, 16, e89–e93. [Google Scholar] [CrossRef] [PubMed]
- Lin, I.-F.; Lin, J.-N.; Tsai, C.-T.; Wu, Y.-Y.; Chen, Y.-H.; Lai, C.-H. Serum C-Reactive Protein and Procalcitonin Values in Acute Q Fever, Scrub Typhus, and Murine Typhus. BMC Infect. Dis. 2020, 20, 334. [Google Scholar] [CrossRef] [PubMed]
- Grahn, A.; Bråve, A.; Lagging, M.; Dotevall, L.; Ekqvist, D.; Hammarström, H.; Karlberg, H.; Lagerqvist, N.; Sansone, M.; Tegnell, A.; et al. Imported Case of Lassa Fever in Sweden with Encephalopathy and Sensorineural Hearing Deficit. Open Forum Infect. Dis. 2016, 3, ofw198. [Google Scholar] [CrossRef] [PubMed]
- Argüello, A.P.; Hun, L.; Rivera, P.; Taylor, L. A Fatal Urban Case of Rocky Mountain Spotted Fever Presenting an Eschar in San José, Costa Rica. Am. J. Trop. Med. Hyg. 2012, 87, 345–348. [Google Scholar] [CrossRef]
- Liu, Y.; Zhao, L.; Wu, Z. Accuracy of C-Reactive Protein Test for Neonatal Septicemia: A Diagnostic Meta-Analysis. Med. Sci. Monit. 2019, 25, 4076–4081. [Google Scholar] [CrossRef]
- Pradhan, S.; Ghimire, A.; Bhattarai, B.; Khanal, B.; Pokharel, K.; Lamsal, M.; Koirala, S. The Role of C-Reactive Protein as a Diagnostic Predictor of Sepsis in a Multidisciplinary Intensive Care Unit of a Tertiary Care Center in Nepal. Indian J. Crit. Care Med. 2016, 20, 417–420. [Google Scholar] [CrossRef] [PubMed]
- Fendl, B.; Weiss, R.; Eichhorn, T.; Linsberger, I.; Afonyushkin, T.; Puhm, F.; Binder, C.J.; Fischer, M.B.; Weber, V. Extracellular Vesicles Are Associated with C-Reactive Protein in Sepsis. Sci. Rep. 2021, 11, 6996. [Google Scholar] [CrossRef] [PubMed]
- Tominaga, H.; Setoguchi, T.; Ishidou, Y.; Nagano, S.; Yamamoto, T.; Komiya, S. Risk Factors for Surgical Site Infection and Urinary Tract Infection after Spine Surgery. Eur. Spine J. 2016, 25, 3908–3915. [Google Scholar] [CrossRef]
- Wang, T.; Wang, H.; Yang, D.-L.; Jiang, L.-Q.; Zhang, L.-J.; Ding, W.-Y. Factors Predicting Surgical Site Infection after Posterior Lumbar Surgery: A Multicenter Retrospective Study. Medicine 2017, 96, e6042. [Google Scholar] [CrossRef] [PubMed]
- Visser, M.; Bouter, L.M.; McQuillan, G.M.; Wener, M.H.; Harris, T.B. Elevated C-Reactive Protein Levels in Overweight and Obese Adults. JAMA 1999, 282, 2131–2135. [Google Scholar] [CrossRef]
- Li, Q.; Wang, Q.; Xu, W.; Ma, Y.; Wang, Q.; Eatman, D.; You, S.; Zou, J.; Champion, J.; Zhao, L.; et al. C-Reactive Protein Causes Adult-Onset Obesity through Chronic Inflammatory Mechanism. Front. Cell Dev. Biol. 2020, 8, 18. [Google Scholar] [CrossRef]
- Kaplan, M.; Tendler, Y.; Mahamid, R.; Shiner, M.; Aviram, M.; Hayek, T. High Glucose Upregulates C-Reactive Protein Synthesis in Macrophages. Clin. Chem. 2010, 56, 1036–1038. [Google Scholar] [CrossRef]
- Mazidi, M.; Gao, H.-K.; Vatanparast, H.; Kengne, A.P. Impact of the Dietary Fatty Acid Intake on C-Reactive Protein Levels in US Adults. Medicine 2017, 96, e5736. [Google Scholar] [CrossRef] [PubMed]
- Desroches, S.; Roodly Archer, W.; Paradis, M.-E.; Dériaz, O.; Couture, P.; Bergeron, J.; Bergeron, N.; Lamarche, B. Baseline Plasma C-Reactive Protein Concentrations Influence Lipid and Lipoprotein Responses to Low-Fat and High Monounsaturated Fatty Acid Diets in Healthy Men1. J. Nutr. 2006, 136, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Ley, S.H.; Sun, Q.; Willett, W.C.; Eliassen, A.H.; Wu, K.; Pan, A.; Hu, F.B. Associations between red meat intake and biomarkers of inflammation and glucose metabolism in women. Am. J. Clin. Nutr. 2014, 99, 352–360. [Google Scholar] [CrossRef] [PubMed]
- Rankin, J.W.; Turpyn, A.D. Low Carbohydrate, High Fat Diet Increases C-Reactive Protein during Weight Loss. J. Am. Coll. Nutr. 2007, 26, 163–169. [Google Scholar] [CrossRef] [PubMed]
- Papier, K.; Hartman, L.; Tong, T.Y.N.; Key, T.J.; Knuppel, A. Higher Meat Intake Is Associated with Higher Inflammatory Markers, Mostly Due to Adiposity: Results from UK Biobank. J. Nutr. 2022, 152, 183–189. [Google Scholar] [CrossRef] [PubMed]
- Lopes, A.E.D.S.C.; Araújo, L.F.; Levy, R.B.; Barreto, S.M.; Giatti, L. Association between Consumption of Ultra-Processed Foods and Serum C-Reactive Protein Levels: Cross-Sectional Results from the ELSA-Brasil Study. Sao Paulo Med. J. 2019, 137, 169–176. [Google Scholar] [CrossRef]
- Kuczmarski, M.F.; Mason, M.A.; Allegro, D.; Zonderman, A.B.; Evans, M.K. Diet Quality Inversely Associated with C-Reactive Protein Levels in Urban, Low-Income African American and White Adults. J. Acad. Nutr. Diet. 2013, 113, 1620–1631. [Google Scholar] [CrossRef]
- Mouliou, D.S. The Deceptive COVID-19: Lessons from Common Molecular Diagnostics and a Novel Plan for the Prevention of the Next Pandemic. Diseases 2023, 11, 20. [Google Scholar] [CrossRef]
- Lopez-Garcia, E.; Schulze, M.B.; Meigs, J.B.; Manson, J.E.; Rifai, N.; Stampfer, M.J.; Willett, W.C.; Hu, F.B. Consumption of Trans Fatty Acids Is Related to Plasma Biomarkers of Inflammation and Endothelial Dysfunction. J. Nutr. 2005, 135, 562–566. [Google Scholar] [CrossRef]
- Voutilainen, E.K.; Hantunen, S.; Ruusunen, A.; Tuomainen, T.-P.; Virtanen, J.K. Associations of Fermented and Non-Fermented Dairy Consumption with Serum C-Reactive Protein Concentrations—A Cross-Sectional Analysis. Clin. Nutr. ESPEN 2022, 48, 401–407. [Google Scholar] [CrossRef]
- Tognon, G.; Rothenberg, E.; Petrolo, M.; Sundh, V.; Lissner, L. Dairy Product Intake and Mortality in a Cohort of 70-Year-Old Swedes: A Contribution to the Nordic Diet Discussion. Eur. J. Nutr. 2018, 57, 2869–2876. [Google Scholar] [CrossRef] [PubMed]
- Dennis, M.; Lee, A.R.; McCarthy, T. Nutritional Considerations of the Gluten-Free Diet. Gastroenterol. Clin. N. Am. 2019, 48, 53–72. [Google Scholar] [CrossRef] [PubMed]
- Calder, P.C. Dietary Arachidonic Acid: Harmful, Harmless or Helpful? Br. J. Nutr. 2007, 98, 451–453. [Google Scholar] [CrossRef] [PubMed]
- Pollard, K.M.; Cauvi, D.M.; Toomey, C.B.; Hultman, P.; Kono, D.H. Mercury-Induced Inflammation and Autoimmunity. Biochim. Biophys. Acta (BBA) Gen. Subj. 2019, 1863, 129299. [Google Scholar] [CrossRef]
- Lee, H.; Kim, K.-N.; Lim, Y.-H.; Hong, Y.-C. Interaction of Vitamin D and Smoking on Inflammatory Markers in the Urban Elderly. J. Prev. Med. Public Health 2015, 48, 249–256. [Google Scholar] [CrossRef]
- Gebreselassie, S.G.; Gase, F.E.; Deressa, M.U. Prevalence and Correlates of Prenatal Vitamin A Deficiency in Rural Sidama, Southern Ethiopia. J. Health Popul. Nutr. 2013, 31, 185–194. [Google Scholar] [CrossRef]
- Shea, M.K.; Dallal, G.E.; Dawson-Hughes, B.; Ordovas, J.M.; O’Donnell, C.J.; Gundberg, C.M.; Peterson, J.W.; Booth, S.L. Vitamin K, circulating cytokines, and bone mineral density in older men and women. Am. J. Clin. Nutr. 2008, 88, 356–363. [Google Scholar] [CrossRef] [PubMed]
- Reece, A.S. High-Sensitivity CRP in Opiate Addiction: Relative and Age-Dependent Elevations. Cardiovasc. Toxicol. 2012, 12, 149–157. [Google Scholar] [CrossRef]
- Costello, E.J.; Copeland, W.E.; Shanahan, L.; Worthman, C.M.; Angold, A. C-Reactive Protein and Substance Use Disorders in Adolescence and Early Adulthood: A Prospective Analysis. Drug Alcohol. Depend. 2013, 133, 712–717. [Google Scholar] [CrossRef]
- Morcuende, A.; Navarrete, F.; Nieto, E.; Manzanares, J.; Femenía, T. Inflammatory Biomarkers in Addictive Disorders. Biomolecules 2021, 11, 1824. [Google Scholar] [CrossRef] [PubMed]
- Tsai, M.Y.; Hanson, N.Q.; Straka, R.J.; Hoke, T.R.; Ordovas, J.M.; Peacock, J.M.; Arends, V.L.; Arnett, D.K. Effect of Influenza Vaccine on Markers of Inflammation and Lipid Profile. J. Lab. Clin. Med. 2005, 145, 323–327. [Google Scholar] [CrossRef] [PubMed]
- Broad, J.; Church, J.; Mutasa, K.; Majo, F.D.; Tavengwa, N.V.; Chasekwa, B.; Humphrey, J.H.; Ntozini, R.; Prendergast, A.J. C Reactive Protein Response after Routine Vaccination among Rural Zimbabwean Infants. Arch. Dis. Child. 2023, 108, 146–147. [Google Scholar] [CrossRef] [PubMed]
- Blumenfeld, Z.; Boulman, N.; Leiba, R.; Siegler, E.; Shachar, S.; Linn, R.; Levy, Y. High C-Reactive Protein Levels Are Associated with Oral Hormonal Menopausal Therapy but Not with Intrauterine Levonorgestrel and Transdermal Estradiol. Scand. J. Clin. Lab. Investig. 2007, 67, 257–263. [Google Scholar] [CrossRef] [PubMed]
- Hefner, G.; Shams, M.E.E.; Unterecker, S.; Falter, T.; Hiemke, C. Inflammation and Psychotropic Drugs: The Relationship between C-Reactive Protein and Antipsychotic Drug Levels. Psychopharmacology 2016, 233, 1695–1705. [Google Scholar] [CrossRef]
- Mintzer, S. Metabolic Consequences of Antiepileptic Drugs. Curr. Opin. Neurol. 2010, 23, 164. [Google Scholar] [CrossRef]
- Tarp, S.; Bartels, E.M.; Bliddal, H.; Furst, D.E.; Boers, M.; Danneskiold-Samsøe, B.; Rasmussen, M.; Christensen, R. Effect of Nonsteroidal Antiinflammatory Drugs on the C-Reactive Protein Level in Rheumatoid Arthritis: A Meta-Analysis of Randomized Controlled Trials. Arthritis Rheum. 2012, 64, 3511–3521. [Google Scholar] [CrossRef]
- Vyas, D.; Laput, G.; Vyas, A.K. Chemotherapy-Enhanced Inflammation May Lead to the Failure of Therapy and Metastasis. Onco Targets Ther. 2014, 7, 1015–1023. [Google Scholar] [CrossRef] [PubMed]
- Brown, T.; Sykes, D.; Allen, A.R. Implications of Breast Cancer Chemotherapy-Induced Inflammation on the Gut, Liver, and Central Nervous System. Biomedicines 2021, 9, 189. [Google Scholar] [CrossRef]
- Demaria, M.; O’Leary, M.N.; Chang, J.; Shao, L.; Liu, S.; Alimirah, F.; Koenig, K.; Le, C.; Mitin, N.; Deal, A.M.; et al. Cellular Senescence Promotes Adverse Effects of Chemotherapy and Cancer Relapse. Cancer Discov. 2017, 7, 165–176. [Google Scholar] [CrossRef] [PubMed]
- Ghahramani, M.; Karbalaeifar, S.; Zokaei, A. The Effect of Physical Activity on Cardiovascular Markers. J. Clin. Res. Paramed. Sci. 2019, 8. [Google Scholar] [CrossRef]
- Kohut, M.L.; McCann, D.A.; Russell, D.W.; Konopka, D.N.; Cunnick, J.E.; Franke, W.D.; Castillo, M.C.; Reighard, A.E.; Vanderah, E. Aerobic Exercise, but Not Flexibility/Resistance Exercise, Reduces Serum IL-18, CRP, and IL-6 Independent of β-Blockers, BMI, and Psychosocial Factors in Older Adults. Brain Behav. Immun. 2006, 20, 201–209. [Google Scholar] [CrossRef]
- Bourassa, K.J.; Cornelius, T.; Birk, J.L. Bereavement Is Associated with Reduced Systemic Inflammation: C-Reactive Protein Before and After Widowhood. Brain Behav. Immun. 2020, 88, 925–929. [Google Scholar] [CrossRef]
- Meier-Ewert, H.K.; Ridker, P.M.; Rifai, N.; Regan, M.M.; Price, N.J.; Dinges, D.F.; Mullington, J.M. Effect of Sleep Loss on C-Reactive Protein, an Inflammatory Marker of Cardiovascular Risk. J. Am. Coll. Cardiol. 2004, 43, 678–683. [Google Scholar] [CrossRef]
- Chiang, J.-K. Short Duration of Sleep Is Associated with Elevated High-Sensitivity C-Reactive Protein Level in Taiwanese Adults: A Cross-Sectional Study. J. Clin. Sleep Med. 2014, 10, 743–749. [Google Scholar] [CrossRef] [PubMed]
- Hughes, S.M.; Levy, C.N.; Calienes, F.L.; Martinez, K.A.; Selke, S.; Tapia, K.; Chohan, B.H.; Oluoch, L.; Kiptinness, C.; Wald, A.; et al. Starting to Have Sexual Intercourse Is Associated with Increases in Cervicovaginal Immune Mediators in Young Women: A Prospective Study and Meta-Analysis. eLife 2022, 11, e78565. [Google Scholar] [CrossRef] [PubMed]
- Kappelmann, N.; Khandaker, G.M.; Dal, H.; Stochl, J.; Kosidou, K.; Jones, P.B.; Dalman, C.; Karlsson, H. Systemic Inflammation and Intelligence in Early Adulthood and Subsequent Risk of Schizophrenia and Other Non-Affective Psychoses: A Longitudinal Cohort and Co-Relative Study. Psychol. Med. 2019, 49, 295–302. [Google Scholar] [CrossRef] [PubMed]
- Cook, S.H.; Slopen, N.; Scarimbolo, L.; Mirin, N.; Wood, E.P.; Rosendale, N.; Chunara, R.; Burke, C.W.; Halkitis, P.N. Discrimination Is Associated with C-Reactive Protein among Young Sexual Minority Men. J. Behav. Med. 2022, 45, 649–657. [Google Scholar] [CrossRef]
- Stöwhas, A.-C.; Latshang, T.D.; Lo Cascio, C.M.; Lautwein, S.; Stadelmann, K.; Tesler, N.; Ayers, L.; Berneis, K.; Gerber, P.A.; Huber, R.; et al. Effects of Acute Exposure to Moderate Altitude on Vascular Function, Metabolism and Systemic Inflammation. PLoS ONE 2013, 8, e70081. [Google Scholar] [CrossRef]
- Hartmann, G.; Tschöp, M.; Fischer, R.; Bidlingmaier, C.; Riepl, R.; Tschöp, K.; Hautmann, H.; Endres, S.; Toepfer, M. High Altitude Increases Circulating Interleukin-6, Interleukin-1 Receptor Antagonist and C-Reactive Protein. Cytokine 2000, 12, 246–252. [Google Scholar] [CrossRef] [PubMed]
- Miele, C.H.; Schwartz, A.R.; Gilman, R.H.; Pham, L.; Wise, R.A.; Davila-Roman, V.G.; Jun, J.C.; Polotsky, V.Y.; Miranda, J.J.; Leon-Velarde, F.; et al. Increased Cardiometabolic Risk and Worsening Hypoxemia at High Altitude. High Alt. Med. Biol. 2016, 17, 93–100. [Google Scholar] [CrossRef]
- Hong, Y.-C.; Kim, H.; Oh, S.-Y.; Lim, Y.-H.; Kim, S.-Y.; Yoon, H.-J.; Park, M. Association of Cold Ambient Temperature and Cardiovascular Markers. Sci. Total Environ. 2012, 435–436, 74–79. [Google Scholar] [CrossRef] [PubMed]
- Kang, Y.; Tang, H.; Jiang, L.; Wang, S.; Wang, X.; Chen, Z.; Zhang, L.; Zheng, C.; Wang, Z.; Huang, G.; et al. Air Temperature Variability and High-Sensitivity C Reactive Protein in a General Population of China. Sci. Total Environ. 2020, 749, 141588. [Google Scholar] [CrossRef]
- Owczarczyk-Saczonek, A.; Zdanowska, N.; Wygonowska, E.; Placek, W. The Immunogenicity of Hyaluronic Fillers and Its Consequences. CCID 2021, 14, 921–934. [Google Scholar] [CrossRef]
- Kassir, M.; Gupta, M.; Galadari, H.; Kroumpouzos, G.; Katsambas, A.; Lotti, T.; Vojvodic, A.; Grabbe, S.; Juchems, E.; Goldust, M. Complications of Botulinum Toxin and Fillers: A Narrative Review. J. Cosmet. Dermatol. 2020, 19, 570–573. [Google Scholar] [CrossRef]
- Witmanowski, H.; Błochowiak, K. The Whole Truth about Botulinum Toxin—A Review. Postep. Dermatol. Alergol. 2020, 37, 853–861. [Google Scholar] [CrossRef] [PubMed]
- Wollina, U. Severe Adverse Events Related to Tattooing: An Retrospective Analysis of 11 Years. Indian J. Dermatol. 2012, 57, 439–443. [Google Scholar] [CrossRef] [PubMed]
- Rubin, C.B.; Brod, B. Natural Does Not Mean Safe—The Dirt on Clean Beauty Products. JAMA Dermatol. 2019, 155, 1344–1345. [Google Scholar] [CrossRef]
- Hartman, R.; Tang, H.; Hang, D.; Song, M.; Nan, H.; Li, X. Red Hair Color Is Associated with Elevated C-Reactive Protein Levels among U.S. Women. J. Investig. Dermatol. 2021, 141, 1342–1344. [Google Scholar] [CrossRef] [PubMed]
- Rubin, I.M.C.; Dabelsteen, S.; Nielsen, M.M.; White, I.R.; Johansen, J.D.; Geisler, C.; Bonefeld, C.M. Repeated Exposure to Hair Dye Induces Regulatory T Cells in Mice. Br. J. Dermatol. 2010, 163, 992–998. [Google Scholar] [CrossRef]
- Klann, A.M.; Rosenberg, J.; Wang, T.; Parker, S.E.; Harlow, B.L. Exploring Hygienic Behaviors and Vulvodynia. J. Low Genit. Tract Dis. 2019, 23, 220–225. [Google Scholar] [CrossRef]
- Chang, P.-Y.; Wu, T.-L.; Tsao, K.-C.; Sun, C.-F.; Wu, L.L.; Wu, J.T. Cosmetic Liposuction Causes Only Transient Elevation of Acute Inflammatory Response and Does Not Advance to Oxidative and Nitrosative Stress. J. Clin. Lab. Anal. 2007, 21, 418–425. [Google Scholar] [CrossRef]
- Mouliou, D.S.; Pantazopoulos, I.; Gourgoulianis, K.I. Medical/Surgical, Cloth and FFP/(K)N95 Masks: Unmasking Preference, SARS-CoV-2 Transmissibility and Respiratory Side Effects. JPM 2022, 12, 325. [Google Scholar] [CrossRef] [PubMed]
- Kanzow, P.; Dylla, V.; Mahler, A.M.; Hrasky, V.; Rödig, T.; Barre, F.; Scheithauer, S.; Wiegand, A. COVID-19 Pandemic: Effect of Different Face Masks on Self-Perceived Dry Mouth and Halitosis. Int. J. Environ. Res. Public Health 2021, 18, 9180. [Google Scholar] [CrossRef] [PubMed]
- Wilcha, R.-J. Does Wearing a Face Mask During the COVID-19 Pandemic Increase the Incidence of Dermatological Conditions in Health Care Workers? Narrative Literature Review. JMIR Dermatol. 2021, 4, e22789. [Google Scholar] [CrossRef] [PubMed]
- Wai, K.; Thompson, P.D.; Kimber, T.E. Fashion Victim: Rhabdomyolysis and Bilateral Peroneal and Tibial Neuropathies as a Result of Squatting in ‘Skinny Jeans’. J. Neurol. Neurosurg. Psychiatry 2016, 87, 782. [Google Scholar] [CrossRef]
- Pimentel, J.C.; Avila, R.; Lourenço, A.G. Respiratory disease caused by synthetic fibres: A new occupational disease. Thorax 1975, 30, 204. [Google Scholar] [CrossRef]
- van Dijk, F.; Song, S.; van Eck, G.; Wu, X.; Bos, I.; Boom, D.; Kooter, I.; Spierings, D.; Wardenaar, R.; Cole, M.; et al. Inhalable textile microplastic fibers impair lung repair. bioRxiv 2021. preprint. [Google Scholar] [CrossRef]
- Hirt, N.; Body-Malapel, M. Immunotoxicity and Intestinal Effects of Nano- and Microplastics: A Review of the Literature. Part. Fibre Toxicol. 2020, 17, 57. [Google Scholar] [CrossRef] [PubMed]
- Donkers, J.M.; Höppener, E.M.; Grigoriev, I.; Will, L.; Melgert, B.N.; van der Zaan, B.; van de Steeg, E.; Kooter, I.M. Advanced epithelial lung and gut barrier models demonstrate passage of microplastic particles. Microplast. Nanoplast. 2022, 2, 6. [Google Scholar] [CrossRef]
- Warheit, D.B.; Hart, G.A.; Hesterberg, T.W.; Collins, J.J.; Dyer, W.M.; Swaen, G.M.H.; Castranova, V.; Soiefer, A.I.; Kennedy, G.L. Potential pulmonary effects of manmade organic fiber (MMOF) dusts. Crit. Rev. Toxicol. 2001, 31, 697. [Google Scholar] [CrossRef] [PubMed]
- Pilz, V.; Wolf, K.; Breitner, S.; Rückerl, R.; Koenig, W.; Rathmann, W.; Cyrys, J.; Peters, A.; Schneider, A.; KORA-Study group. C-Reactive Protein (CRP) and Long-Term Air Pollution with a Focus on Ultrafine Particles. Int. J. Hyg. Environ. Health 2018, 221, 510–518. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; Shi, S.; Wang, B.; Liu, L.; Yang, Y.; Sun, X.; Ni, Z.; Wang, X. Effect of Urban Air Pollution on CRP and Coagulation: A Study on Inpatients with Acute Exacerbation of Chronic Obstructive Pulmonary Disease. BMC Pulm. Med. 2021, 21, 296. [Google Scholar] [CrossRef]
- Ostro, B.; Malig, B.; Broadwin, R.; Basu, R.; Gold, E.B.; Bromberger, J.T.; Derby, C.; Feinstein, S.; Greendale, G.A.; Jackson, E.A.; et al. Chronic PM2.5 Exposure and Inflammation: Determining Sensitive Subgroups in Mid-Life Women. Environ. Res. 2014, 132, 168–175. [Google Scholar] [CrossRef]
- Swiston, J.R.; Davidson, W.; Attridge, S.; Li, G.T.; Brauer, M.; Eeden, S.F. van Wood Smoke Exposure Induces a Pulmonary and Systemic Inflammatory Response in Firefighters. Eur. Respir. J. 2008, 32, 129–138. [Google Scholar] [CrossRef]
- Kim, G.; Baek, S.; Park, H.W.; Ryu, Y.J.; Kang, E.K. Association with Elevated Level of Inflammatory Biomarkers and Attention Deficit in Korean Farmers. J. Neurol. Sci. 2019, 405, 174. [Google Scholar] [CrossRef]
- Isara, A.R.; Adam, V.Y.; Aigbokhaode, A.Q.; Alenoghena, I.O. Respiratory Symptoms and Ventilatory Functions among Quarry Workers in Edo State, Nigeria. Pan Afr. Med. J. 2016, 23, 212. [Google Scholar] [CrossRef]
- Baumann, R.; Brand, P.; Chaker, A.; Markert, A.; Rack, I.; Davatgarbenam, S.; Joraslafsky, S.; Gerhards, B.; Kraus, T.; Gube, M. Human Nasal Mucosal C-Reactive Protein Responses after Inhalation of Ultrafine Welding Fume Particles: Positive Correlation to Systemic C-Reactive Protein Responses. Nanotoxicology 2018, 12, 1130–1147. [Google Scholar] [CrossRef]
- Mogal, M.R.; Islam, M.D.; Hasan, M.I.; Junayed, A.; Sompa, S.A.; Mahmod, M.R.; Akter, A.; Abedin, M.Z.; Sikder, M.A. The Impact of Wood Dust on Pulmonary Function and Blood Immunoglobulin E, Erythrocyte Sedimentation Rate, and C- Reactive Protein: A Cross-sectional Study among Sawmill Workers in Tangail, Bangladesh. Health Sci. Rep. 2022, 5, e646. [Google Scholar] [CrossRef]
- Kobayashi, H.; Kanoh, S.; Motoyoshi, K.; Aida, S. Diffuse Lung Disease Caused by Cotton Fibre Inhalation but Distinct from Byssinosis. Thorax 2004, 59, 1095–1097. [Google Scholar] [CrossRef] [PubMed]
- Blanco-Pérez, J.J.; Blanco-Dorado, S.; Rodríguez-García, J.; Gonzalez-Bello, M.E.; Salgado-Barreira, Á.; Caldera-Díaz, A.C.; Pallarés-Sanmartín, A.; Fernandez-Villar, A.; González-Barcala, F.J. Serum Levels of Inflammatory Mediators as Prognostic Biomarker in Silica Exposed Workers. Sci. Rep. 2021, 11, 13348. [Google Scholar] [CrossRef] [PubMed]
- Bhandari, J.; Thada, P.K.; Sedhai, Y.R. Asbestosis; StatPearls Publishing: Treasure Island, FL, USA, 2023. [Google Scholar]
- François, A.; Milliat, F.; Guipaud, O.; Benderitter, M. Inflammation and Immunity in Radiation Damage to the Gut Mucosa. BioMed Res. Int. 2013, 2013, e123241. [Google Scholar] [CrossRef] [PubMed]
- Schaue, D.; Micewicz, E.D.; Ratikan, J.A.; Xie, M.W.; Cheng, G.; McBride, W.H. Radiation & Inflammation. Semin. Radiat. Oncol. 2015, 25, 4–10. [Google Scholar] [CrossRef]
- Kiprian, D.; Czarkowska-Paczek, B.; Wyczalkowska-Tomasik, A.; Fuksiewicz, M.; Kotowicz, B.; Paczek, L. Radiotherapy and Radiochemotherapy Increase Serum Levels of Pro-Inflammatory Interleukin-6 and C-Reactive Protein in Patients with Head and Neck Cancers. Transl. Cancer Res. 2018, 7, 41–47. [Google Scholar] [CrossRef]
- Yahyapour, R.; Amini, P.; Rezapour, S.; Cheki, M.; Rezaeyan, A.; Farhood, B.; Shabeeb, D.; Musa, A.E.; Fallah, H.; Najafi, M. Radiation-Induced Inflammation and Autoimmune Diseases. Mil. Med. Res. 2018, 5, 9. [Google Scholar] [CrossRef] [PubMed]
- Cengiz, M.; Akbulut, S.; Atahan, I.L.; Grigsby, P.W. Acute Phase Response during Radiotherapy. Int. J. Radiat Oncol. Biol. Phys. 2001, 49, 1093–1096. [Google Scholar] [CrossRef]
- Simkó, M.; Mattsson, M.-O. 5G Wireless Communication and Health Effects—A Pragmatic Review Based on Available Studies Regarding 6 to 100 GHz. Int. J. Environ. Res. Public Health 2019, 16, 3406. [Google Scholar] [CrossRef] [PubMed]
- Pall, M.L. Wi-Fi Is an Important Threat to Human Health. Environ. Res. 2018, 164, 405–416. [Google Scholar] [CrossRef] [PubMed]
- Ciążyńska, M.; Olejniczak-Staruch, I.; Sobolewska-Sztychny, D.; Narbutt, J.; Skibińska, M.; Lesiak, A. Ultraviolet Radiation and Chronic Inflammation—Molecules and Mechanisms Involved in Skin Carcinogenesis: A Narrative Review. Life 2021, 11, 326. [Google Scholar] [CrossRef]
- Hruza, L.L.; Pentland, A.P. Mechanisms of UV-Induced Inflammation. J. Investig. Dermatol. 1993, 100, S35–S41. [Google Scholar] [CrossRef]
- Esmaillzadeh, A.; Kimiagar, M.; Mehrabi, Y.; Azadbakht, L.; Hu, F.B.; Willett, W.C. Fruit and Vegetable Intakes, C-Reactive Protein, and the Metabolic Syndrome. Am. J. Clin. Nutr. 2006, 84, 1489–1497. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, A.; Rodríguez-Artalejo, F.; Lopes, C. The Association of Fruits, Vegetables, Antioxidant Vitamins and Fibre Intake with High-Sensitivity C-Reactive Protein: Sex and Body Mass Index Interactions. Eur. J. Clin. Nutr. 2009, 63, 1345–1352. [Google Scholar] [CrossRef]
- Qureshi, M.M.; Singer, M.R.; Moore, L.L. A Cross-Sectional Study of Food Group Intake and C-Reactive Protein among Children. Nutr. Metab. 2009, 6, 40. [Google Scholar] [CrossRef] [PubMed]
- Sahebkar, A.; Gurban, C.; Serban, A.; Andrica, F.; Serban, M.-C. Effects of Supplementation with Pomegranate Juice on Plasma C-Reactive Protein Concentrations: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. Phytomedicine 2016, 23, 1095–1102. [Google Scholar] [CrossRef] [PubMed]
- Na, W.; Yu, T.Y.; Sohn, C. Development of a Food-Based Index of Dietary Inflammatory Potential for Koreans and Its Relationship with Metabolic Syndrome. Nutr. Res. Pract. 2019, 13, 150–158. [Google Scholar] [CrossRef] [PubMed]
- Sarkhosh-Khorasani, S.; Hosseinzadeh, M. The Effect of Grape Products Containing Polyphenols on C-Reactive Protein Levels: A Systematic Review and Meta-Analysis of Randomised Controlled Trials. Br. J. Nutr. 2021, 125, 1230–1245. [Google Scholar] [CrossRef]
- Kim, M.J.; Hwang, J.H.; Ko, H.J.; Na, H.B.; Kim, J.H. Lemon Detox Diet Reduced Body Fat, Insulin Resistance, and Serum Hs-CRP Level without Hematological Changes in Overweight Korean Women. Nutr. Res. 2015, 35, 409–420. [Google Scholar] [CrossRef] [PubMed]
- Carvajal-Zarrabal, O.; Nolasco-Hipolito, C.; Aguilar-Uscanga, M.G.; Melo-Santiesteban, G.; Hayward-Jones, P.M.; Barradas-Dermitz, D.M. Avocado Oil Supplementation Modifies Cardiovascular Risk Profile Markers in a Rat Model of Sucrose-Induced Metabolic Changes. Dis. Markers 2014, 2014, 386425. [Google Scholar] [CrossRef]
- Varshney, R.; Budoff, M.J. Garlic and Heart Disease1, 2, 3. J. Nutr. 2016, 146, 416S–421S. [Google Scholar] [CrossRef]
- Hsieh, C.-T.; Wang, J.; Chien, K.-L. Association between Dietary Flavonoid Intakes and C-Reactive Protein Levels: A Cross-Sectional Study in Taiwan. J. Nutr. Sci. 2021, 10, e15. [Google Scholar] [CrossRef]
- Mazidi, M.; Rezaie, P.; Banach, M. Effect of Magnesium Supplements on Serum C-Reactive Protein: A Systematic Review and Meta-Analysis. Arch. Med. Sci. 2018, 14, 707–716. [Google Scholar] [CrossRef]
- Kaddam, L.A.; Kaddam, A.S. Effect of Gum Arabic (Acacia Senegal) on C-Reactive Protein Level among Sickle Cell Anemia Patients. BMC Res. Notes 2020, 13, 162. [Google Scholar] [CrossRef] [PubMed]
- Gorabi, A.M.; Abbasifard, M.; Imani, D.; Aslani, S.; Razi, B.; Alizadeh, S.; Bagheri-Hosseinabadi, Z.; Sathyapalan, T.; Sahebkar, A. Effect of Curcumin on C-Reactive Protein as a Biomarker of Systemic Inflammation: An Updated Meta-Analysis of Randomized Controlled Trials. Phytother. Res. 2022, 36, 85–97. [Google Scholar] [CrossRef] [PubMed]
- Mazidi, M.; Gao, H.-K.; Rezaie, P.; Ferns, G.A. The Effect of Ginger Supplementation on Serum C-Reactive Protein, Lipid Profile and Glycaemia: A Systematic Review and Meta-Analysis. Food Nutr. Res. 2016, 60, 32613. [Google Scholar] [CrossRef]
- Vallianou, N.; Tsang, C.; Taghizadeh, M.; Davoodvandi, A.; Jafarnejad, S. Effect of Cinnamon (Cinnamomum zeylanicum) Supplementation on Serum C-Reactive Protein Concentrations: A Meta-Analysis and Systematic Review. Complement. Ther. Med. 2019, 42, 271–278. [Google Scholar] [CrossRef] [PubMed]
- Mirahmad, M.; Mohseni, S.; Tabatabaei-Malazy, O.; Esmaeili, F.; Alatab, S.; Bahramsoltani, R.; Ejtahed, H.-S.; Qulami, H.; Bitarafan, Z.; Arjmand, B.; et al. Antioxidative Hypoglycemic Herbal Medicines with in Vivo and in Vitro Activity against C-Reactive Protein: A Systematic Review. Phytomedicine 2023, 109, 154615. [Google Scholar] [CrossRef]
- Mazidi, M.; Rezaie, P.; Ferns, G.A.; Gao, H. Impact of Different Types of Tree Nut, Peanut, and Soy Nut Consumption on Serum C-Reactive Protein (CRP). Medicine 2016, 95, e5165. [Google Scholar] [CrossRef] [PubMed]
- Hariri, M.; Amirkalali, B.; Baradaran, H.R.; Gholami, A. A Systematic Review and Meta-Analysis of Almond Effect on C-Reactive Protein and Interleukin-6 in Adults. Complement. Ther. Med. 2023, 72, 102911. [Google Scholar] [CrossRef]
- Sutliffe, J.T.; Wilson, L.D.; de Heer, H.D.; Foster, R.L.; Carnot, M.J. C-Reactive Protein Response to a Vegan Lifestyle Intervention. Complement. Ther. Med. 2015, 23, 32–37. [Google Scholar] [CrossRef]
- Shah, B.; Newman, J.D.; Woolf, K.; Ganguzza, L.; Guo, Y.; Allen, N.; Zhong, J.; Fisher, E.A.; Slater, J. Anti-Inflammatory Effects of a Vegan Diet Versus the American Heart Association–Recommended Diet in Coronary Artery Disease Trial. JAHA 2018, 7, e011367. [Google Scholar] [CrossRef]
- Aly, S.M. Role of Intermittent Fasting on Improving Health and Reducing Diseases. Int. J. Health Sci. 2014, 8, V–VI. [Google Scholar] [CrossRef]
- Kulkarni, A.P. Immunocompromised Hosts: Infections and Biomarkers. South Asian J. Cancer 2013, 2, 209–210. [Google Scholar] [CrossRef]
- Franeková, J.; Protuš, M.; Kieslichová, E.; Březina, A.; Komrsková, J.; Vymětalík, J.; Jabor, A. Changes in Sepsis Biomarkers after Immunosuppressant Administration in Transplant Patients. Mediat. Inflamm. 2021, 2021, e8831659. [Google Scholar] [CrossRef] [PubMed]
- Dufaux, B.; Order, U.; Geyer, H.; Hollmann, W. C-Reactive Protein Serum Concentrations in Well-Trained Athletes. Int. J. Sports Med. 1984, 05, 102–106. [Google Scholar] [CrossRef] [PubMed]
- Fancourt, D.; Ockelford, A.; Belai, A. The Psychoneuroimmunological Effects of Music: A Systematic Review and a New Model. Brain Behav. Immun. 2014, 36, 15–26. [Google Scholar] [CrossRef]
- Borges, L.; Passos, M.E.P.; Silva, M.B.B.; Santos, V.C.; Momesso, C.M.; Pithon-Curi, T.C.; Gorjão, R.; Gray, S.R.; Lima, K.C.A.; de Freitas, P.B.; et al. Dance Training Improves Cytokine Secretion and Viability of Neutrophils in Diabetic Patients. Mediat. Inflamm. 2019, 2019, 2924818. [Google Scholar] [CrossRef]
- Roy, B.; Diez-Roux, A.V.; Seeman, T.; Ranjit, N.; Shea, S.; Cushman, M. The Association of Optimism and Pessimism with Inflammation and Hemostasis in the Multi-Ethnic Study of Atherosclerosis (MESA). Psychosom. Med. 2010, 72, 134–140. [Google Scholar] [CrossRef] [PubMed]
- Handbook of Art Therapy; Malchiodi, C.A. (Ed.) Guilford Press: New York, NY, USA, 2003; ISBN 9781572308091. [Google Scholar]
- Pullen, P.R.; Nagamia, S.H.; Mehta, P.K.; Thompson, W.R.; Benardot, D.; Hammoud, R.; Parrott, J.M.; Sola, S.; Khan, B.V. Effects of Yoga on Inflammation and Exercise Capacity in Patients with Chronic Heart Failure. J. Card. Fail. 2008, 14, 407–413. [Google Scholar] [CrossRef] [PubMed]
- Koenig, H.G. Maintaining Health and Well-Being by Putting Faith into Action During the COVID-19 Pandemic. J. Relig. Health 2020, 59, 2205–2214. [Google Scholar] [CrossRef]
- Bornstein, D.L.; Schiffman, G.; Bernheimer, H.P.; Austrian, R. Capsulation of pneumococcus with soluble c-like (Cs) polysaccharide. J. Exp. Med. 1968, 128, 1385–1400. [Google Scholar] [CrossRef]
- Jia, J.; Shi, W.; Dong, F.; Meng, Q.; Yuan, L.; Chen, C.; Yao, K. Identification and Molecular Epidemiology of Routinely Determined Streptococcus Pneumoniae with Negative Quellung Reaction Results. Clin. Lab. Anal. 2022, 36, e24293. [Google Scholar] [CrossRef]
- Vashist, S.K.; Venkatesh, A.G.; Marion Schneider, E.; Beaudoin, C.; Luppa, P.B.; Luong, J.H.T. Bioanalytical Advances in Assays for C-Reactive Protein. Biotechnol. Adv. 2016, 34, 272–290. [Google Scholar] [CrossRef]
- Otsuji, S.; Shibata, H.; Umeda, M. Turbidimetric immunoassay of serum C-reactive protein. Clin. Chem. 1982, 28, 2121–2124. [Google Scholar] [CrossRef]
- Johnson, A.M. Nephelometric Immunoassay. J. Pharm. Biomed. Anal. 1987, 5, 803–809. [Google Scholar] [CrossRef]
- Montagne, P.; Laroche, P.; Cuillière, M.L.; Varcin, P.; Pau, B.; Duheille, J. Microparticle-Enhanced Nephelometric Immunoassay for Human C-Reactive Protein. J. Clin. Lab. Anal. 1992, 6, 24–29. [Google Scholar] [CrossRef]
- Aydin, S. A Short History, Principles, and Types of ELISA, and Our Laboratory Experience with Peptide/Protein Analyses Using ELISA. Peptides 2015, 72, 4–15. [Google Scholar] [CrossRef]
- Cinquanta, L.; Fontana, D.E.; Bizzaro, N. Chemiluminescent Immunoassay Technology: What Does It Change in Autoantibody Detection? Auto Immun. Highlights 2017, 8, 9. [Google Scholar] [CrossRef] [PubMed]
- Hicks, J.M. Fluorescence Immunoassay. Hum. Pathol. 1984, 15, 112–116. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.S.; Black, J.C.; Knowles, M.K.; Reed, S.M. C-reactive protein (CRP) aptamer binds to monomeric but not pentameric form of CRP. Anal. Bioanal. Chem. 2011, 401, 1309–1318. [Google Scholar] [CrossRef] [PubMed]
- Mouliou, D.S.; Pantazopoulos, I.; Gourgoulianis, K.I. Societal Criticism towards COVID-19: Assessing the Theory of Self-Diagnosis Contrasted to Medical Diagnosis. Diagnostics 2021, 11, 1777. [Google Scholar] [CrossRef] [PubMed]
- Wauthier, L.; Plebani, M.; Favresse, J. Interferences in Immunoassays: Review and Practical Algorithm. Clin. Chem. Lab. Med. (CCLM) 2022, 60, 808–820. [Google Scholar] [CrossRef] [PubMed]
- Nikolac, N. Lipemia: Causes, Interference Mechanisms, Detection and Management. Biochem. Med. 2014, 24, 57–67. [Google Scholar] [CrossRef] [PubMed]
- Elliott, G.B.; Horner, G. False-positive C-Reactive Protein Reactions Due to Serum Lipoproteins. Am. Rev. Respir. Dis. 2001, 90, 453–454. [Google Scholar]
- Verougstraete, N.; Verbeke, F.; Delanghe, J.R. Exogenous Triglycerides Interfere with a Point of Care CRP Assay: A Pre-Analytical Caveat. Clin. Chem. Lab. Med. (CCLM) 2021, 59, e141–e143. [Google Scholar] [CrossRef] [PubMed]
- Sato, M.; Sugimoto, M.; Nanba, S.; Kasatori, N.; Urayama, T. Hepatic Cirrhosis Showing False-Positive Serum C-Reactive Protein Reaction. Intern. Med. 1993, 32, 498–501. [Google Scholar] [CrossRef]
- Emerson, J.F.; Lai, K.K.Y. Endogenous Antibody Interferences in Immunoassays. Lab. Med. 2013, 44, 69–73. [Google Scholar] [CrossRef]
- Gaće, M.; Prskalo, Z.Š.; Dobrijević, S.; Mayer, L. Most common interferences in immunoassays. Libri Oncol. 2015, 43, 23–27. [Google Scholar]
- Kaplan, I.V.; Levinson, S.S. When Is a Heterophile Antibody Not a Heterophile Antibody? When It Is an Antibody against a Specific Immunogen. Clin. Chem. 1999, 45, 616–618. [Google Scholar] [CrossRef]
- Bowen, R.A.R.; Bertholf, R.L.; Holmquist, B. Chapter 1—Maximizing the Value of Laboratory Tests. In Handbook of Diagnostic Endocrinology, 3rd ed.; Winter, W.E., Holmquist, B., Sokoll, L.J., Bertholf, R.L., Eds.; Academic Press: Cambridge, MA, USA, 2021; pp. 1–45. ISBN 9780128182772. [Google Scholar]
- Benoist, J.F.; Orbach, D.; Biou, D. False Increase in C-Reactive Protein Attributable to Heterophilic Antibodies in Two Renal Transplant Patients Treated with Rabbit Antilymphocyte Globulin. Clin. Chem. 1998, 44, 1980–1985. [Google Scholar] [CrossRef] [PubMed]
- Dasgupta, A.; Wahed, A. Chapter 2—Immunoassay Platform and Designs. In Clinical Chemistry, Immunology and Laboratory Quality Control; Dasgupta, A., Wahed, A., Eds.; Elsevier: San Diego, CA, USA, 2014; pp. 19–34. ISBN 9780124078215. [Google Scholar]
- Dasgupta, A. Chapter 5—Issues of Interferences in Clinical Chemistry Tests Including Heterophilic Antibody Interferences. In Biotin and Other Interferences in Immunoassays; Dasgupta, A., Ed.; Elsevier: Amsterdam, The Netherlands, 2019; pp. 75–98. ISBN 9780128164297. [Google Scholar]
- High Sensitivity C-Reactive Protein (hs-CRP) ELISA. Available online: https://dbc-labs.com/wp-content/uploads/pdfs/hsCRP-ELISA.pdf (accessed on 9 April 2023).
- Hawkins, B.R.; Saueracker, G.C.; Dawkins, R.L.; Davey, M.G.; O’Connor, K.J. Population Study of Heterophile Antibodies. Vox Sang. 1980, 39, 339–342. [Google Scholar] [CrossRef]
- Chaulin, A.M. On the Effect of Heterophilic Antibodies on Serum Levels of Cardiac Troponins: A Brief Descriptive Review. Life 2022, 12, 1114. [Google Scholar] [CrossRef] [PubMed]
- Svehag, S.E.; Olander, R.; Sundqvist, K.G. Occurrence and Cross-Reactivity of Heterophile Antibodies and Anti-Kidney Antibodies in Kidney Transplanted Patients and Patients with Renal Disease. Clin. Exp. Immunol. 1973, 13, 191–202. [Google Scholar] [PubMed]
- Hamwi, A.; Födinger, M.; Sunder-Plassmann, G.; Hörl, W.H.; Vukovich, T.C. Disturbed Latex Immunoassays for C-Reactive Protein and Ferritin in a Renal Transplant Patient Due to Polyclonal IgM Hypergammaglobulinaemia. Nephrol. Dial. Transpl. 1997, 12, 1229–1233. [Google Scholar] [CrossRef] [PubMed]
- Johnson, A.J.; Zywiel, M.G.; Stroh, A.; Marker, D.R.; Mont, M.A. Serological Markers Can Lead to False Negative Diagnoses of Periprosthetic Infections Following Total Knee Arthroplasty. Int. Orthop. 2011, 35, 1621–1626. [Google Scholar] [CrossRef] [PubMed]
- Beer, P. The heterophile antibodies in infectious mononucleosis and after the injection of serum. J. Clin. Investig. 1936, 15, 591–599. [Google Scholar] [CrossRef] [PubMed]
- Orban, T.; Kent, S.C.; Malik, P.; Milner, J.D.; Schuster, K.; Jackson, R.A.; Hafler, D.A. Heterophile Antibodies Indicate Progression of Autoimmunity in Human Type 1 Diabetes Mellitus before Clinical Onset. Autoimmunity 2001, 34, 247–264. [Google Scholar] [CrossRef] [PubMed]
- Ohtake, T.; Kano, S.; Watanabe, K. Interference in turbidimetric immunoassay for serum C-reactive protein due to serum protein abnormalities an immune complex and rheumatoid factor. Rinsho Byori 2000, 48, 752–759. [Google Scholar]
- Müller, W.; Mierau, R.; Wohltmann, D. Interference of IgM Rheumatoid Factor with Nephelometric C-Reactive Protein Determinations. J. Immunol. Methods 1985, 80, 77–90. [Google Scholar] [CrossRef]
- Motyckova, G.; Murali, M. Laboratory Testing for Cryoglobulins. Am. J. Hematol. 2011, 86, 500–502. [Google Scholar] [CrossRef]
- Morishita, Y.; Iinuma, Y.; Nakashima, N. A consideration on discrepancy of results obtained between commercial CRP measurement kits. Rinsho Byori 2000, 48, 746–751. [Google Scholar] [PubMed]
- Lammers, M. Interference with Nephelometric Assay of C-Reactive Protein by Monoclonal Immunoglobulin. Clin. Chem. 1998, 44, 1584–1585. [Google Scholar] [CrossRef]
- Yamada, K.; Yagihashi, A.; Ishii, S.; Tanemura, K.; Kida, T.; Watanabe, N.; Niitsu, Y. Interference with Nephelometric Assay of C-Reactive Protein and Antistreptolysin-O by Monoclonal IgM-Kappa from a Myeloma Patient. Clin. Chem. 1997, 43, 2435–2437. [Google Scholar] [CrossRef]
- Daly, M.-L.; Cartwright, D.J.; Lehner, P.J.; Javid, B. A 58-Year-Old Woman with Abdominal Symptoms and Elevated C-Reactive Protein. PLoS Med. 2008, 5, e149. [Google Scholar] [CrossRef]
- Yu, A.; Pira, U. False Increase in Serum C-Reactive Protein Caused by Monoclonal IgM-λ: A Case Report. Clin. Chem. Lab. Med. 2001, 39, 983–987. [Google Scholar] [CrossRef] [PubMed]
- Young, D.S. Effects of Drugs on Clinical Laboratory Test, 4th ed.; AACC Press: Washington, DC, USA, 1995. [Google Scholar]
- Laboratory Procedure Manual High Sensitivity C-Reactive Protein (hs-CRP). Available online: https://wwwn.cdc.gov/nchs/data/nhanes/2017-2018/labmethods/HSCRP-J-MET-508.pdf (accessed on 10 April 2023).
- DIALAB. CRP (C-Reactive Protein) Diagnostic Reagent for the Quantitative In Vitro Determination of CRP (C-Reactive Protein) in Human Serum by Turbidimetric Assay. Available online: https://diameb.ua/manuals/eng/A00519.pdf (accessed on 10 April 2023).
- Design Verification. CRP (C-Reactive Protein) Multipurpose Reagent. Available online: http://www.human-de.com/data/gb/vr/tu-crp.pdf (accessed on 10 April 2023).
- Stein, C.D.S.; Cassol, J.P.E.; Moresco, R.N. Potential Interference of in Vitro Carbamylation on C-Reactive Protein Laboratory Measurement. Scand. J. Clin. Lab. Investig. 2023, 83, 183–186. [Google Scholar] [CrossRef] [PubMed]
- Oh, J.; Joung, H.-A.; Han, H.S.; Kim, J.K.; Kim, M.-G. A Hook Effect-Free Immunochromatographic Assay (HEF-ICA) for Measuring the C-Reactive Protein Concentration in One Drop of Human Serum. Theranostics 2018, 8, 3189–3197. [Google Scholar] [CrossRef]
- He, G.; Dong, T.; Yang, Z.; Jiang, Z. Mitigating Hook Effect in One-Step Quantitative Sandwich Lateral Flow Assay by Timed Conjugate Release. Talanta 2022, 240, 123157. [Google Scholar] [CrossRef]
- Namburi, R.P.; Kancherla, V.; Ponnala, A.R. High-Dose Hook Effect. J. Dr. NTR Univ. Health Sci. 2014, 3, 5. [Google Scholar] [CrossRef]
- Schouwers, S.M.E.; Delanghe, J.R.; Devreese, K.M.J. Lupus Anticoagulant (LAC) Testing in Patients with Inflammatory Status: Does C-Reactive Protein Interfere with LAC Test Results? Thromb. Res. 2010, 125, 102–104. [Google Scholar] [CrossRef] [PubMed]
- LineaR. CRP—Turbidimetric. Available online: https://www.linear.es/wp-content/uploads/2018/03/3120025-CRP-ing-Rev.-05.pdf (accessed on 10 April 2023).
- Wide Range C-Reactive Protein (Wr-CRP) Turbidimetric Immunoassay Kit. Available online: https://www.immunodiagnostics.com.hk/product-page/wide-range-c-reactive-protein-turbidimetric-immunoassay-reagent-kit (accessed on 10 April 2023).
- High Sensitivity C-Reactive Protein (Hs-CRP) Turbidimetric Immunoassay Kit. Available online: https://www.immunodiagnostics.com.hk/product-page/hs-crp-ita-reagent-kit (accessed on 10 April 2023).
- C-Reactive Protein. Available online: https://www.certest.es/products/c-reactive-protein/ (accessed on 10 April 2023).
- MonlabTest. Available online: https://monlab.com/document/Bioquimica/Turbidimetria/Turbidimetria/IFU%20PCR%20monlabtest%20EN.pdf (accessed on 10 April 2023).
- Laboratory Procedure Manual. C-Reactive Protein in Serum. NHANES 2005–2006. Available online: https://www.cdc.gov/nchs/data/nhanes/nhanes_05_06/crp_d_met_protein.pdf (accessed on 4 January 2023).
- C-Reactive Protein (CRP) Test Kit (Homogeneous Chemiluminescence Immunoassay). Available online: https://www.linkedin.com/pulse/c-reactive-protein-crp-test-kit-homogeneous-immunoassay-%E8%BF%9B-%E9%AB%98 (accessed on 10 April 2023).
- Abnova. CRP (Human) CLIA Kit. Available online: http://www.abnova.com/protocol_pdf/KA3640.pdf (accessed on 10 April 2023).
- NEPHSTAR® C-Reactive Protein (CRP) Kit. Available online: http://weldonbiotech.com/wp-content/uploads/2018/06/NEPHSTAR-CRP-EN-V0707.pdf (accessed on 4 January 2023).
- Griswold, W.R. A Quantitative Relationship Between Antibody Affinity and Antibody Avidity. Immunol. Investig. 1987, 16, 97–106. [Google Scholar] [CrossRef]
- Chang, X.; Zha, L.; Wallimann, A.; Mohsen, M.O.; Krenger, P.; Liu, X.; Vogel, M.; Bachmann, M.F. Low-affinity but High-avidity Interactions May Offer an Explanation for IgE-mediated Allergen Cross-reactivity. Allergy 2021, 76, 2565–2574. [Google Scholar] [CrossRef]
- Reverberi, R.; Reverberi, L. Factors Affecting the Antigen-Antibody Reaction. Blood Transfus. 2007, 5, 227–240. [Google Scholar] [CrossRef] [PubMed]
- Laurent, P.; Potempa, L.A.; Gewurz, H.; Fiedel, B.A.; Allen, R.C. The Titration Curve of Native C Reactive Protein. Electrophoresis 1983, 4, 316–317. [Google Scholar] [CrossRef]
- Shields, M.J. A Hypothesis Resolving the Apparently Disparate Activities of Native and Altered Forms of Human C-Reactive Protein. Immunol. Res. 1993, 12, 37–47. [Google Scholar] [CrossRef] [PubMed]
- Ying, S.C.; Gewurz, H.; Kinoshita, C.M.; Potempa, L.A.; Siegel, J.N. Identification and Partial Characterization of Multiple Native and Neoantigenic Epitopes of Human C-Reactive Protein by Using Monoclonal Antibodies. J. Immunol. 1989, 143, 221–228. [Google Scholar] [CrossRef]
- Crawford, J.P.; Movat, H.Z.; Minta, J.O.; Opas, M. Acute Inflammation Induced by Immune Complexes in the Microcirculation. Exp. Mol. Pathol. 1985, 42, 175–193. [Google Scholar] [CrossRef]
- Kushner, I. C-Reactive Protein—My Perspective on Its First Half Century, 1930–1982. Front. Immunol. 2023, 14, 1150103. [Google Scholar] [CrossRef]
- Oliveira, E.B.; Gotschlich, C.; Liu, T.Y. Primary Structure of Human C-Reactive Protein. J. Biol. Chem. 1979, 254, 489–502. [Google Scholar] [CrossRef]
- Plumptre, C.D.; Ogunniyi, A.D.; Paton, J.C. Surface Association of Pht Proteins of Streptococcus Pneumoniae. Infect. Immun. 2013, 81, 3644–3651. [Google Scholar] [CrossRef] [PubMed]
- Mitchell, T.J.; Andrew, P.W.; Saunders, F.K.; Smith, A.N.; Boulnois, G.J. Complement Activation and Antibody Binding by Pneumolysin via a Region of the Toxin Homologous to a Human Acute-Phase Protein. Mol. Microbiol. 1991, 5, 1883–1888. [Google Scholar] [CrossRef] [PubMed]
- Salzberg, S.L.; White, O.; Peterson, J.; Eisen, J.A. Microbial Genes in the Human Genome: Lateral Transfer or Gene Loss? Science 2001, 292, 1903–1906. [Google Scholar] [CrossRef] [PubMed]
- Griffith, F. The Significance of Pneumococcal Types. J. Hyg. 1928, 27, 113–159. [Google Scholar] [CrossRef]
- van der Meer, A.J.; Kroeze, A.; Hoogendijk, A.J.; Soussan, A.A.; Ellen van der Schoot, C.; Wuillemin, W.A.; Voermans, C.; van der Poll, T.; Zeerleder, S. Systemic Inflammation Induces Release of Cell-Free DNA from Hematopoietic and Parenchymal Cells in Mice and Humans. Blood Adv. 2019, 3, 724–728. [Google Scholar] [CrossRef]
- Moore, M.E.; Lam, A.; Bhatnagar, S.; Solnick, J.V. Environmental Determinants of Transformation Efficiency in Helicobacter Pylori. J. Bacteriol. 2014, 196, 337–344. [Google Scholar] [CrossRef]
- Coykendall, A.L. Classification and Identification of the Viridans Streptococci. Clin. Microbiol. Rev. 1989, 2, 315–328. [Google Scholar] [CrossRef] [PubMed]
- Kellogg, J.A.; Bankert, D.A.; Elder, C.J.; Gibbs, J.L.; Smith, M.C. Identification of Streptococcus Pneumoniae Revisited. J. Clin. Microbiol. 2001, 39, 3373–3375. [Google Scholar] [CrossRef] [PubMed]
- Richter, S.S.; Heilmann, K.P.; Dohrn, C.L.; Riahi, F.; Beekmann, S.E.; Doern, G.V. Accuracy of Phenotypic Methods for Identification of Streptococcus Pneumoniae Isolates Included in Surveillance Programs. J. Clin. Microbiol. 2008, 46, 2184–2188. [Google Scholar] [CrossRef]
- Kadioglu, A.; Weiser, J.N.; Paton, J.C.; Andrew, P.W. The Role of Streptococcus Pneumoniae Virulence Factors in Host Respiratory Colonization and Disease. Nat. Rev. Microbiol. 2008, 6, 288–301. [Google Scholar] [CrossRef]
- Chao, Y.; Marks, L.R.; Pettigrew, M.M.; Hakansson, A.P. Streptococcus Pneumoniae Biofilm Formation and Dispersion during Colonization and Disease. Front. Cell. Infect. Microbiol. 2015, 4, 194. [Google Scholar] [CrossRef]
- Kuscuoglu, D.; Janciauskiene, S.; Hamesch, K.; Haybaeck, J.; Trautwein, C.; Strnad, P. Liver—Master and Servant of Serum Proteome. J. Hepatol. 2018, 69, 512–524. [Google Scholar] [CrossRef]
- Hurme, M.; Kivimäki, M.; Pertovaara, M.; Lehtimäki, T.; Karhunen, P.J.; Jylhä, M.; Hervonen, A.; Eklund, C. CRP Gene Is Involved in the Regulation of Human Longevity: A Follow-up Study in Finnish Nonagenarians. Mech. Ageing Dev. 2007, 128, 574–576. [Google Scholar] [CrossRef] [PubMed]
- Siggins, M.K.; Sriskandan, S. Bacterial Lymphatic Metastasis in Infection and Immunity. Cells 2021, 11, 33. [Google Scholar] [CrossRef] [PubMed]
- Lal, R.B.; Dhawan, R.R.; Ramzy, R.M.; Farris, R.M.; Gad, A.A. C-Reactive Protein in Patients with Lymphatic Filariasis: Increased Expression on Lymphocytes in Chronic Lymphatic Obstruction. J. Clin. Immunol. 1991, 11, 46–53. [Google Scholar] [CrossRef]
- Dwyer, J.; Foulkes, E.; Evans, M.; Ausman, L. Acid/Alkaline Ash Diets: Time for Assessment and Change. J. Am. Diet. Assoc. 1985, 85, 841–845. [Google Scholar] [CrossRef] [PubMed]
- Luo, X.; Huang, X.; Luo, Z.; Wang, Z.; He, G.; Tan, Y.; Zhang, B.; Zhou, H.; Li, P.; Shen, T.; et al. Electromagnetic Field Exposure-Induced Depression Features Could Be Alleviated by Heat Acclimation Based on Remodeling the Gut Microbiota. Ecotoxicol. Environ. Saf. 2021, 228, 112980. [Google Scholar] [CrossRef]
- Ulker, İ.; Yildiran, H. The Effects of Bariatric Surgery on Gut Microbiota in Patients with Obesity: A Review of the Literature. Biosci. Microbiota Food Health 2019, 38, 3–9. [Google Scholar] [CrossRef]
- Tun, H.M.; Konya, T.; Takaro, T.K.; Brook, J.R.; Chari, R.; Field, C.J.; Guttman, D.S.; Becker, A.B.; Mandhane, P.J.; Turvey, S.E.; et al. Exposure to Household Furry Pets Influences the Gut Microbiota of Infants at 3–4 Months Following Various Birth Scenarios. Microbiome 2017, 5, 40. [Google Scholar] [CrossRef] [PubMed]
- Noguera-Julian, M.; Rocafort, M.; Guillén, Y.; Rivera, J.; Casadellà, M.; Nowak, P.; Hildebrand, F.; Zeller, G.; Parera, M.; Bellido, R.; et al. Gut Microbiota Linked to Sexual Preference and HIV Infection. eBioMedicine 2016, 5, 135–146. [Google Scholar] [CrossRef]
- Salim, S.Y.; Kaplan, G.G.; Madsen, K.L. Air Pollution Effects on the Gut Microbiota. Gut Microbes 2014, 5, 215–219. [Google Scholar] [CrossRef]
- Wei, L.; Wen, X.-S.; Xian, C.J. Chemotherapy-Induced Intestinal Microbiota Dysbiosis Impairs Mucosal Homeostasis by Modulating Toll-like Receptor Signaling Pathways. Int. J. Mol. Sci. 2021, 22, 9474. [Google Scholar] [CrossRef] [PubMed]
- Hua, X.; Cao, Y.; Morgan, D.M.; Miller, K.; Chin, S.M.; Bellavance, D.; Khalili, H. Longitudinal Analysis of the Impact of Oral Contraceptive Use on the Gut Microbiome. J. Med. Microbiol. 2022, 71, 001512. [Google Scholar] [CrossRef] [PubMed]
- Russell, J.T.; Zhou, Y.; Weinstock, G.M.; Bubier, J.A. The Gut Microbiome and Substance Use Disorder. Front. Neurosci. 2021, 15, 725500. [Google Scholar] [CrossRef] [PubMed]
- Syromyatnikov, M.; Nesterova, E.; Gladkikh, M.; Smirnova, Y.; Gryaznova, M.; Popov, V. Characteristics of the Gut Bacterial Composition in People of Different Nationalities and Religions. Microorganisms 2022, 10, 1866. [Google Scholar] [CrossRef] [PubMed]
- Bossa, L.; Kline, K.; McDougald, D.; Lee, B.B.; Rice, S.A. Urinary Catheter-Associated Microbiota Change in Accordance with Treatment and Infection Status. PLoS ONE 2017, 12, e0177633. [Google Scholar] [CrossRef] [PubMed]
- Wu, Z.; Zhang, Q.; Yang, J.; Zhang, J.; Fu, J.; Dang, C.; Liu, M.; Wang, S.; Lin, Y.; Hao, J.; et al. Significant Alterations of Intestinal Symbiotic Microbiota Induced by Intraperitoneal Vaccination Mediate Changes in Intestinal Metabolism of NEW Genetically Improved Farmed Tilapia (NEW GIFT, Oreochromis Niloticus). Microbiome 2022, 10, 221. [Google Scholar] [CrossRef]
- Razdolsky Michalczyk, E.; Senderak, A.R.; Melfyn Jones, R.; Coulter, W.H.; Goudy, S.L. Changes in the Microbiome during Oral Wound Healing. Dent. Rev. 2022, 2, 100040. [Google Scholar] [CrossRef]
- Conteville, L.C.; Vicente, A.C.P. Skin Exposure to Sunlight: A Factor Modulating the Human Gut Microbiome Composition. Gut Microbes 2020, 11, 1135–1138. [Google Scholar] [CrossRef]
- Smith, R.P.; Easson, C.; Lyle, S.M.; Kapoor, R.; Donnelly, C.P.; Davidson, E.J.; Parikh, E.; Lopez, J.V.; Tartar, J.L. Gut Microbiome Diversity Is Associated with Sleep Physiology in Humans. PLoS ONE 2019, 14, e0222394. [Google Scholar] [CrossRef]
- Hylander, B.L.; Repasky, E.A. Temperature as a Modulator of the Gut Microbiome: What Are the Implications and Opportunities for Thermal Medicine? Int. J. Hyperth. 2019, 36, 83–89. [Google Scholar] [CrossRef]
- Monda, V.; Villano, I.; Messina, A.; Valenzano, A.; Esposito, T.; Moscatelli, F.; Viggiano, A.; Cibelli, G.; Chieffi, S.; Monda, M.; et al. Exercise Modifies the Gut Microbiota with Positive Health Effects. Oxid. Med. Cell Longev. 2017, 2017, 3831972. [Google Scholar] [CrossRef]
- Tugal, D.; Liao, X.; Jain, M.K. Transcriptional Control of Macrophage Polarization. ATVB 2013, 33, 1135–1144. [Google Scholar] [CrossRef] [PubMed]
- Jimenez, R.V.; Szalai, A.J. Therapeutic Lowering of C-Reactive Protein. Front. Immunol. 2021, 11, 619564. [Google Scholar] [CrossRef] [PubMed]
- Ito, H. The Difficulty in Interpreting the Value of C-Reactive Protein in the Context of Acute Medicine. Am. J. Med. 2021, 134, e402. [Google Scholar] [CrossRef]
- Goldberg, I.; Shalmon, D.; Shteinvil, R.; Berliner, S.; Paran, Y.; Zeltser, D.; Shapira, I.; Shenhar-Tsarfaty, S.; Meilik, A.; Wasserman, A.; et al. A Second C-Reactive Protein (CRP) Test to Detect Inflammatory Burst in Patients with Acute Bacterial Infections Presenting with a First Relatively Low CRP. Medicine 2020, 99, e22551. [Google Scholar] [CrossRef] [PubMed]






Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mouliou, D.S. C-Reactive Protein: Pathophysiology, Diagnosis, False Test Results and a Novel Diagnostic Algorithm for Clinicians. Diseases 2023, 11, 132. https://doi.org/10.3390/diseases11040132
Mouliou DS. C-Reactive Protein: Pathophysiology, Diagnosis, False Test Results and a Novel Diagnostic Algorithm for Clinicians. Diseases. 2023; 11(4):132. https://doi.org/10.3390/diseases11040132
Chicago/Turabian StyleMouliou, Dimitra S. 2023. "C-Reactive Protein: Pathophysiology, Diagnosis, False Test Results and a Novel Diagnostic Algorithm for Clinicians" Diseases 11, no. 4: 132. https://doi.org/10.3390/diseases11040132