
Factors Associated with Reclosure of Posterior Capsule Aperture by Flat Opacifications with Pearls after Nd:YAG Laser Posterior Capsulotomy

Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Participants
2.2. Ethical Considerations
2.3. Statistical Analyses
3. Results
3.1. Clinical Characteristics and Demographics of Participants
3.2. Characteristics of Intraocular Lens
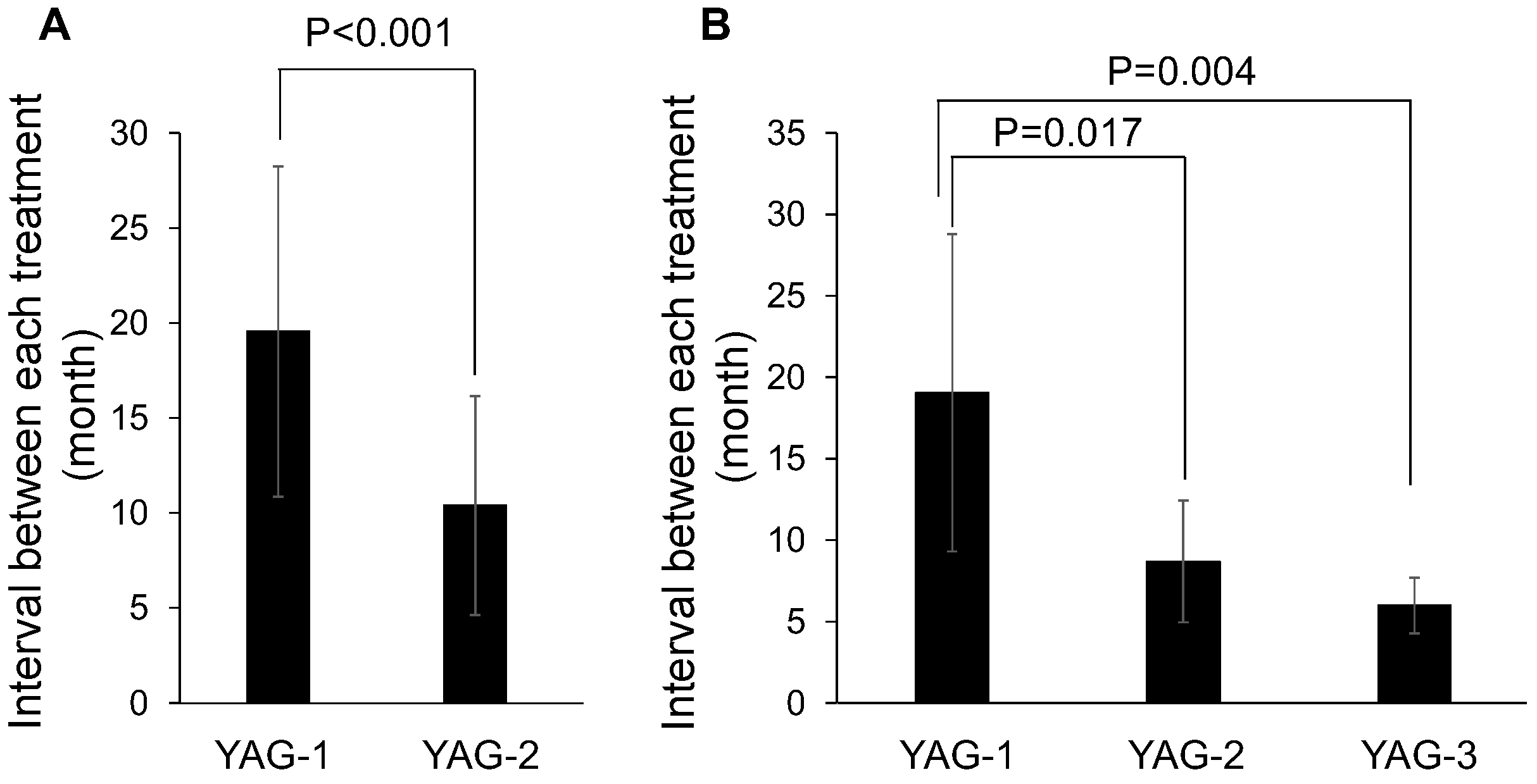
3.3. Interval between Laser Capsulotomies
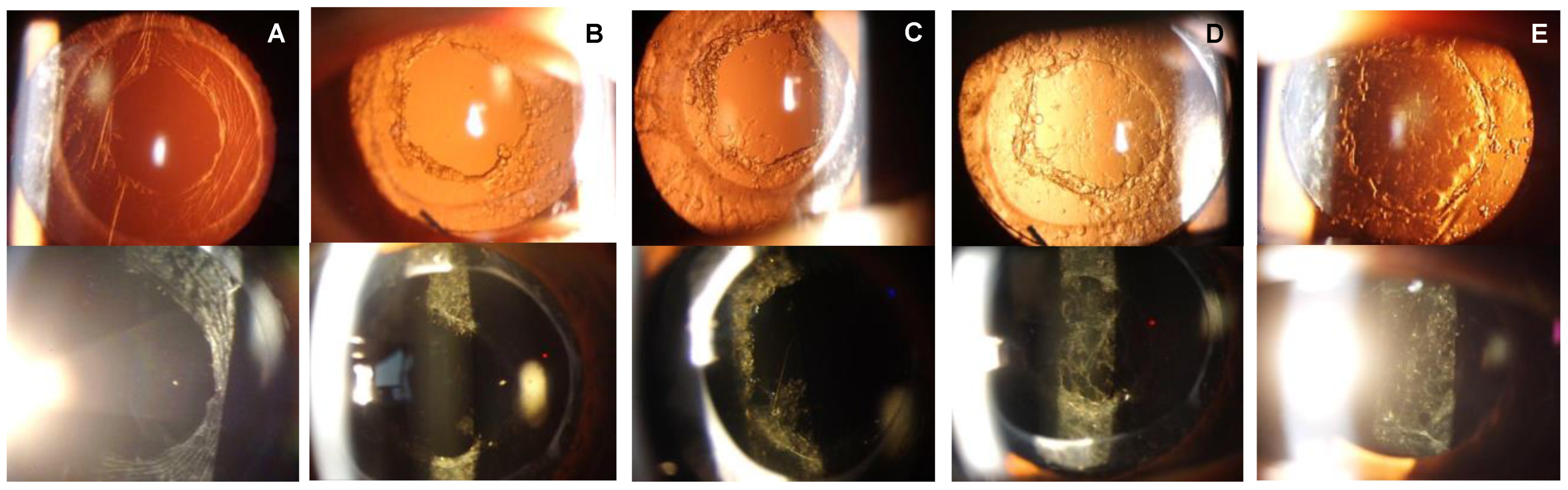
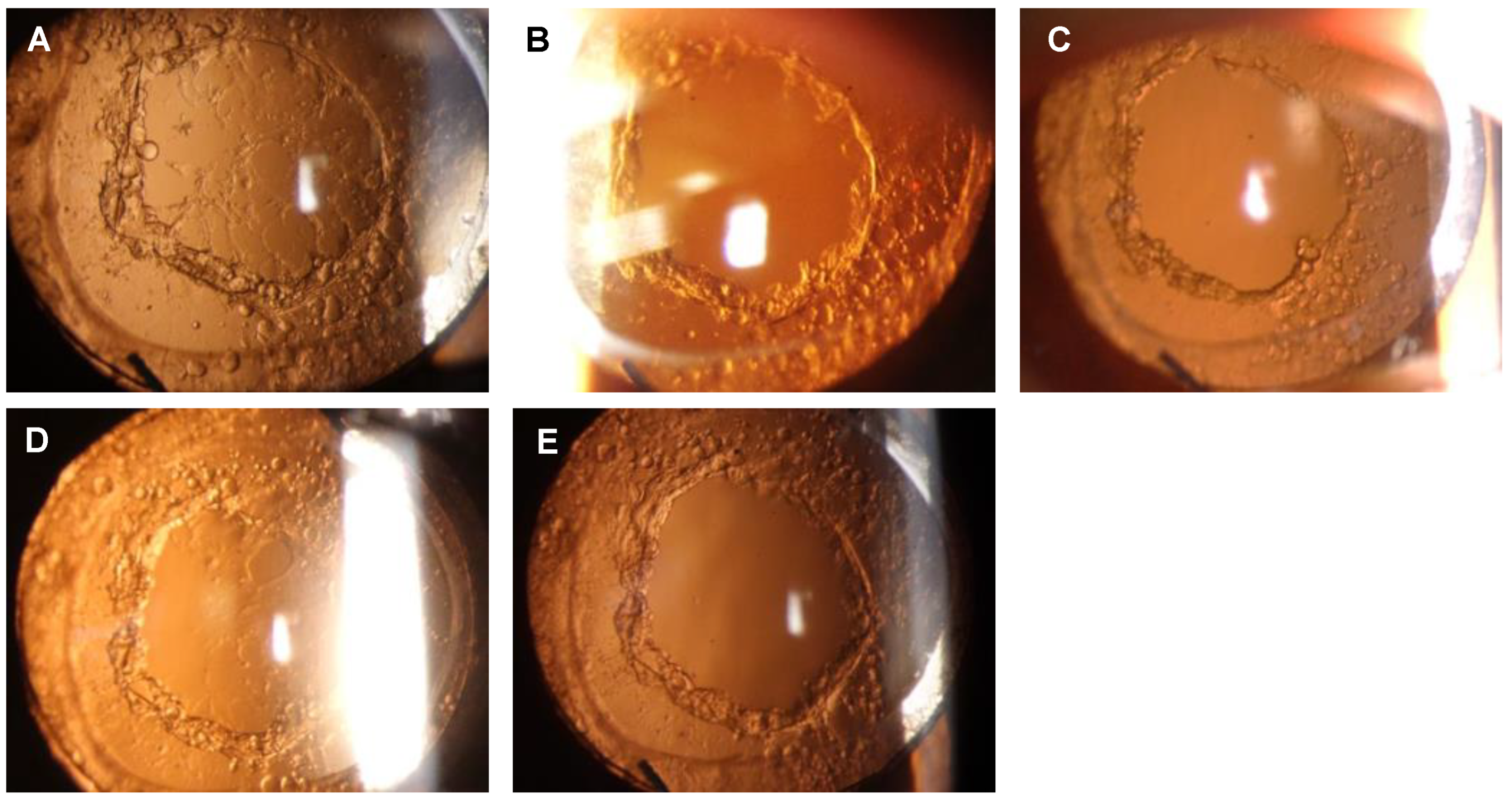
3.4. Staging of Posterior Capsule Reclosure
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Raj, S.M.; Vasavada, A.R.; Johar, S.R.; Vasavada, V.A.; Vasavada, V.A. Post-operative capsular opacification: A review. Int. J. Biomed. Sci. 2007, 3, 237–250. [Google Scholar] [PubMed]
- Donachie, P.H.J.; Barnes, B.L.; Olaitan, M.; Sparrow, J.M.; Buchan, J.C. The Royal College of Ophthalmologists’ National Ophthalmology Database study of cataract surgery: Report 9, Risk factors for posterior capsule opacification. Eye 2023, 37, 1633–1639. [Google Scholar] [CrossRef] [PubMed]
- Vasavada, A.R.; Raj, S.M.; Shah, A.; Shah, G.; Vasavada, V.; Vasavada, V. Comparison of posterior capsule opacification with hydrophobic acrylic and hydrophilic acrylic intraocular lenses. J. Cataract. Refract. Surg. 2011, 37, 1050–1059. [Google Scholar] [CrossRef] [PubMed]
- Caballero, A.; Garcia-Elskamp, C.; Losada, M.; Salinas, M.; Marin, J.-M. Natural evolution of Elschnig pearl posterior capsule opacification after posterior capsulotomy. J. Cataract. Refract. Surg. 2001, 27, 1979–1986. [Google Scholar] [CrossRef] [PubMed]
- Kurosaka, D.; Kato, K.; Kurosaka, H.; Yoshino, M.; Nakamura, K.; Negishi, K. Elschnig pearl formation along the neodymium:YAG laser posterior capsulotomy margin. Long-term follow-up. J. Cataract. Refract. Surg. 2002, 28, 1809–1813. [Google Scholar] [CrossRef] [PubMed]
- Kato, K.; Kurosaka, D.; Bissen-Miyajima, H.; Negishi, K.; Hara, E.; Nagamoto, T. Elschnig pearl formation along the posterior capsulotomy margin after neodymium:YAG capsulotomy. J. Cataract. Refract. Surg. 1997, 23, 1556–1560. [Google Scholar] [CrossRef] [PubMed]
- Jayaram, H.; Uppal, G.; Hugkulstone, C.E.; Gibbens, M.V.; Watt, L. YAG curios #1: Repeat Nd:YAG laser posterior capsulotomy. Acta Ophthalmol. Scand. 2005, 83, 242–244. [Google Scholar] [CrossRef] [PubMed]
- Jones, N.P.; McLeod, D.; Boulton, M.E. Massive proliferation of lens epithelial remnants after Nd-YAG laser capsulotomy. Br. J. Ophthalmol. 1995, 79, 261–263. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McPherson, R.J.; Govan, J.A. Posterior capsule reopacification after neodymium:YAG laser capsulotomy. J. Cataract. Refract. Surg. 1995, 21, 351–352. [Google Scholar] [CrossRef] [PubMed]
- Kalliath, J.; Prakash, G.; Avadhani, K.; Shakuntala, A. An after after-cataract: A curious case of visual axis re-opacification. Saudi J. Ophthalmol. 2016, 30, 264–267. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Georgopoulos, M.; Findl, O.; Menapace, R.; Buehl, W.; Wirtitsch, M.; Rainer, G. Influence of intraocular lens material on regeneratory posterior capsule opacification after neodymium:YAG laser capsulotomy. J. Cataract. Refract. Surg. 2003, 29, 1560–1565. [Google Scholar] [CrossRef] [PubMed]
- Congdon, N.; Fan, H.; Choi, K.; Huang, W.; Zhang, L.; Zhang, S.; Liu, K.; Hu, I.C.; Zheng, Z.; Lam, D.S.C. Impact of posterior subcapsular opacification on vision and visual function among subjects undergoing cataract surgery in rural China: Study of Cataract Outcomes and Up-Take of Services (SCOUTS) in the Caring is Hip Project, report 5. Br. J. Ophthalmol. 2008, 92, 598–603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ministry of Health, Labour and Welfare. National Health and Nutrition Survey 2017. Available online: http://www.mhlw.go.jp/toukei/itiran/gaiyo/k-eisei.html (accessed on 12 December 2022).
- Ollerton, A.; Werner, L.; Fuller, S.R.; Kavoussi, S.C.; McIntyre, J.S.; Mamalis, N. Evaluation of a new single-piece 4% water content hydrophobic acrylic intraocular lens in the rabbit model. J. Cataract. Refract. Surg. 2012, 38, 1827–1832. [Google Scholar] [CrossRef] [PubMed]
- Tetz, M.; Jorgensen, M.R. New Hydrophobic IOL Materials and Understanding the Science of Glistenings. Curr. Eye Res. 2015, 40, 969–981. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| Surgery | Eye | Age | Sex | Ophthalmic Disease | Systemic Disease | IOL Model | IOL Diameter (mm) | Water Content (%) | YAG1(M) | YAG2 (M) | YAG3 (M) |
|---|---|---|---|---|---|---|---|---|---|---|---|
| PI | R | 85 | M | None | HTN, CI, PCa | ZA9003 | 6 | <1.0 | 12.1 | 7.6 | 6.0 |
| L | None | ZA9003 | 6 | <1.0 | 12.4 | 15.1 | |||||
| R | 74 | F | uveitis | DM, HTN | X-60 | 6 | 4 | 14.0 | 12.1 | 7.0 | |
| R | 59 | F | None | None | NX-60 | 6 | 4 | 31.4 | 4.5 | 8.1 | |
| L | None | NX-60 | 6 | 4 | 17.7 | 14.5 | |||||
| R | 66 | F | None | Marfan, HTN | X-70 | 7 | 4 | 25.6 | 9.1 | ||
| L | None | X-70 | 7 | 4 | 25.5 | 4.4 | |||||
| R | 39 | F | None | None | SN60WF | 6 | 0.4 | 37.3 | 6.6 | ||
| L | 76 | M | None | HTN, BPH | NX-70S | 7 | 4 | 27.4 | 4.3 | ||
| L | 76 | F | None | Anemia | SY60WF | 6 | 1.5 | 10.3 | 26.6 | ||
| L | 57 | M | None | None | 255 | 6 | 0.24 | 24.1 | 5.9 | ||
| R | 36 | F | None | None | XY1 | 6 | 0.79 | 2.4 | 11.6 | ||
| PPV + PI | L | 74 | F | ERM | HTN, CI | NX-70 | 7 | 4 | 34.5 | 6.5 | 6.8 |
| R | 63 | F | ERM | None | NX-70 | 7 | 4 | 17.2 | 22.3 | ||
| R | 71 | F | ERM, DR | HTN, DM | NX-70 | 7 | 4 | 24.0 | 6.5 | ||
| L | ERM, DR | NX-70 | 7 | 4 | 23.8 | 6.5 | |||||
| L | 66 | M | ERM | None | NX-70 | 7 | 4 | 17.5 | 9.8 | ||
| L | 60 | F | ERM | None | NX-70S | 7 | 4 | 17.6 | 14.7 | 4.9 | |
| R | 76 | M | ERM | HTN, BPH | NX-70S | 7 | 4 | 20.0 | 11.4 | ||
| L | 61 | M | ERM, glaucoma | None | NX-70S | 7 | 4 | 11.5 | 13.3 | ||
| R | 80 | F | DME | DM, HTN | NX-70S | 7 | 4 | 12.3 | 10.0 | 6.3 | |
| R | 86 | F | ERM | HTN | NX-70S | 7 | 4 | 11.5 | 5.4 | 2.8 |
| Overall (17 Patients) | P + I (9 Patients) | P + I + PPV (9 Patients) | p-Value | |
|---|---|---|---|---|
| Age (years) | 66.4 ± 14.0 | 63.1 ± 17.0 | 70.8 ± 9.0 | 0.376 |
| Sex (Male/Female) | 5/12 | 3/6 | 3/6 | 1.000 |
| Diabetes mellitus | 3 | 1 | 2 | 0.585 |
| Hypertension | 9 | 4 | 5 | 0.684 |
| Overall (22 Eyes) | P + I (12 Eyes) | P + I + PPV (10 Eyes) | p-Value | |
|---|---|---|---|---|
| YAG-1 (months) | 19.6 ± 8.7 | 20.1 ± 10.1 | 19.0 ± 7.1 | 0.575 |
| YAG-2 (months) | 10.4 ± 5.8 | 10.2 ± 6.4 | 10.6 ± 5.2 | 0.717 |
| Overall (7 eyes) | P + I (3 eyes) | P + I + PPV (4 eyes) | p-value | |
| YAG-3 (months) | 6.0 ± 1.7 | 7.0 ± 1.1 | 5.2 ± 1.8 | 0.229 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ota, A.; Ota, I.; Kachi, S.; Miyake, G.; Haga, F.; Miyake, K.; Kondo, M.; Kato, K. Factors Associated with Reclosure of Posterior Capsule Aperture by Flat Opacifications with Pearls after Nd:YAG Laser Posterior Capsulotomy. Diseases 2023, 11, 82. https://doi.org/10.3390/diseases11020082
Ota A, Ota I, Kachi S, Miyake G, Haga F, Miyake K, Kondo M, Kato K. Factors Associated with Reclosure of Posterior Capsule Aperture by Flat Opacifications with Pearls after Nd:YAG Laser Posterior Capsulotomy. Diseases. 2023; 11(2):82. https://doi.org/10.3390/diseases11020082
Chicago/Turabian StyleOta, Akiko, Ichiro Ota, Shu Kachi, Goichiro Miyake, Fuminori Haga, Kensaku Miyake, Mineo Kondo, and Kumiko Kato. 2023. "Factors Associated with Reclosure of Posterior Capsule Aperture by Flat Opacifications with Pearls after Nd:YAG Laser Posterior Capsulotomy" Diseases 11, no. 2: 82. https://doi.org/10.3390/diseases11020082