
Impact of the COVID-19 Pandemic Period on Patients with Head and Neck Carcinoma: A Systematic Review

 , , and
, , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design and Eligibility Criteria
2.2. Search Strategy
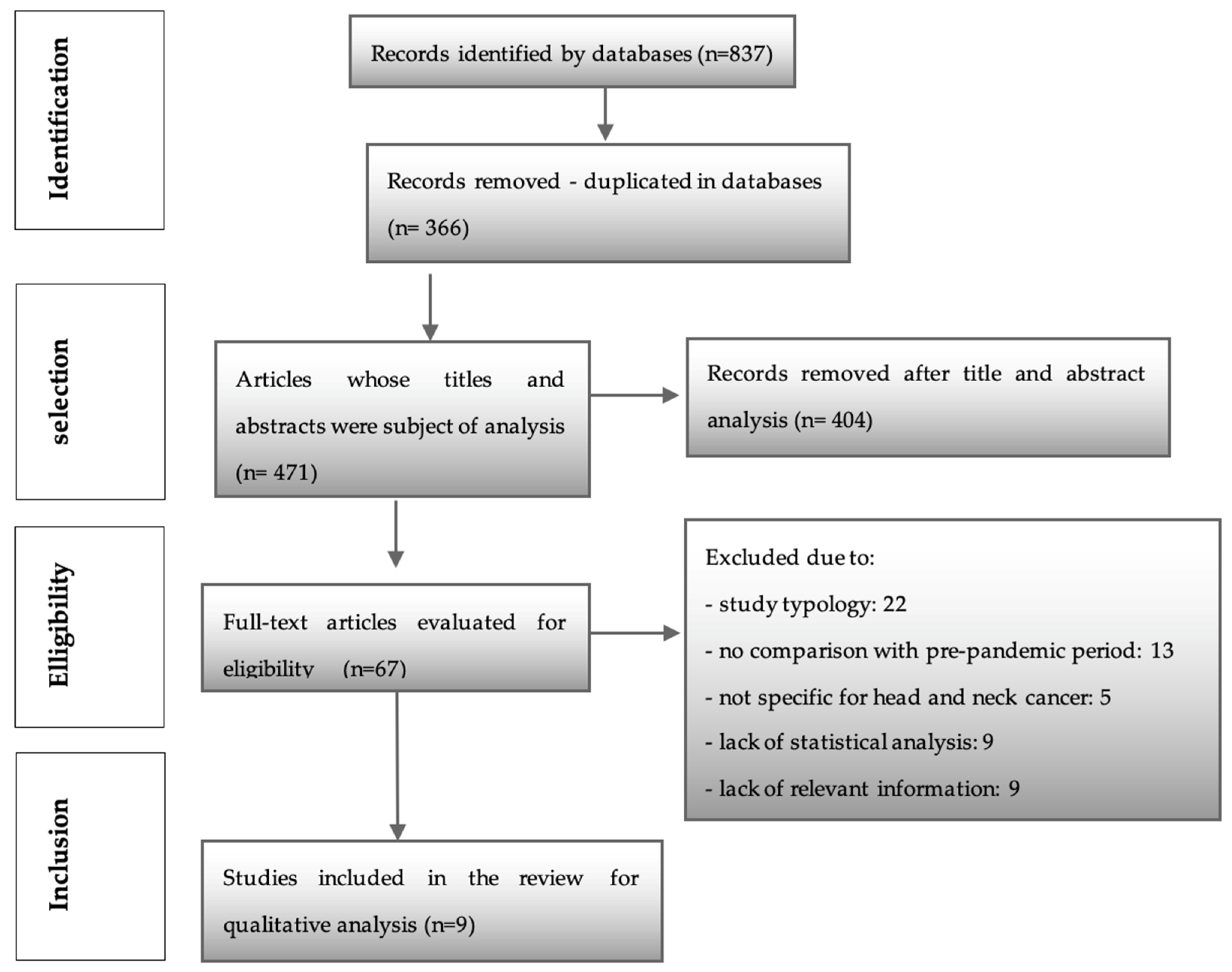
2.3. Study Selection
3. Results
4. Discussion
4.1. Impact of the Pandemic on Patients and Healthcare
4.2. Limitations of the Study
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Harapan, H.; Itoh, N.; Yufika, A.; Winardi, W.; Keam, S.; Te, H.; Megawati, D.; Hayati, Z.; Wagner, A.L.; Mudatsir, M. Coronavirus disease 2019 (COVID-19): A literature review. J. Infect. Public Health 2020, 13, 667–673. [Google Scholar] [CrossRef] [PubMed]
- Esakandari, H.; Nabi-Afjadi, M.; Fakkari-Afjadi, J.; Farahmandian, N.; Miresmaeili, S.M.; Bahreini, E. A comprehensive review of COVID-19 characteristics. Biol. Proced. Online 2020, 22, 19. [Google Scholar] [CrossRef] [PubMed]
- Halboub, E.; AL-Maweri, S.A.; Al-Soneidar, W.A. Utilization of COVID-19 testing for opportunistic screening of oral cancer. Oral. Oncol. 2020, 106, 104775. [Google Scholar] [CrossRef] [PubMed]
- dos Santos Gonçalves, R.M.; Fernandes, G.V.O.; Fernandes, J.C.H.; Seabra, M.; Figueiredo, A. Impact of COVID-19 on Portuguese Dental Students: A Cohort Study. Healthcare 2023, 11, 818. [Google Scholar] [CrossRef] [PubMed]
- Han, A.Y.; Miller, J.E.; Long, J.L.; St John, M.A. Time for a Paradigm Shift in Head and Neck Cancer Management During the COVID-19 Pandemic. Otolaryngology–Head Neck Surg. 2020, 163, 447–454. [Google Scholar] [CrossRef]
- Kowalski, L.P.; Sanabria, A.; Ridge, J.A.; Ng, W.T.; de Bree, R.; Rinaldo, A.; Takes, R.P.; Mäkitie, A.A.; Carvalho, A.L.; Bradford, C.R.; et al. COVID-19 pandemic: Effects and evidence-based recommendations for otolaryngology and head and neck surgery practice. Head Neck 2020, 42, 1259–1267. [Google Scholar] [CrossRef] [Green Version]
- Rod, J.E.; Oviedo-Trespalacios, O.; Cortes-Ramirez, J. A brief-review of the risk factors for covid-19 severity. Rev. Saude Publica 2020, 54, 1–11. [Google Scholar] [CrossRef]
- Prasad, A.; Carey, R.M.; Rajasekaran, K. Head and neck virtual medicine in a pandemic era: Lessons from COVID-19. Head Neck 2020, 42, 1308–1309. [Google Scholar] [CrossRef]
- Araujo, S.E.A.; Leal, A.; Centrone, A.F.Y.; Teich, V.D.; Malheir1, D.T.; Cypriano, A.S.; Neto, M.S.; Klajner, S. Impacto da COVID-19 sobre o atendimento de pacientes oncológicos: Experiência de um centro oncológico localizado em um epicentro Latino-Americano da pandemia. Einstein 2021, 19, 1–8. [Google Scholar]
- Tevetoğlu, F.; Kara, S.; Aliyeva, C.; Yıldırım, R.; Yener, H.M. Delayed presentation of head and neck cancer patients during COVID-19 pandemic. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 5081–5085. [Google Scholar] [CrossRef]
- Wai, K.C.; Xu, M.J.; Lee, R.H.; El-Sayed, I.H.; George, J.R.; Heaton, C.M.; Knott, P.D.; Park, A.M.; Ryan, W.R.; Seth, R.; et al. Head and neck surgery during the coronavirus-19 pandemic: The University of California San Francisco experience. Head Neck 2021, 43, 622–629. [Google Scholar] [CrossRef]
- Kiong, K.L.; Diaz, E.M.; Gross, N.D.; Diaz, E.M.; Hanna, E.Y. The impact of COVID-19 on head and neck cancer diagnosis and disease extent. Head Neck 2021, 43, 1890–1897. [Google Scholar] [CrossRef]
- Laccourreye, O.; Mirghani, H.; Evrard, D.; Bonnefont, P.; Brugel, L.; Tankere, F. Impact of the first month of Covid-19 lockdown on oncologic surgical activity in the Ile de France region university hospital otorhinolaryngology departments. Eur. Ann. Otorhinolaryngol. Head Neck Dis. 2020, 137, 273–276. [Google Scholar] [CrossRef]
- He, J.; Yang, L.; Tao, Z.; Yang, J.; Zhou, Y.; Wang, R.; Zhang, Y.; Huang, Y.; Zhou, L.; Sun, B.; et al. Impact of the 2019 novel coronavirus disease (COVID-19) epidemic on radiotherapy-treated patients with cancer: A single-center descriptive study. Cancer Manag. Res. 2021, 13, 37–43. [Google Scholar] [CrossRef]
- Akhtar, N.; Rajan, S.; Chakrabarti, D.; Kumar, V.; Gupta, S.; Misra, S.; Chaturvedi, A.; Azhar, T.; Parveen, S.; Qayoomet, S.; et al. Continuing cancer surgery through the first six months of the COVID-19 pandemic at an academic university hospital in India: A lower-middle-income country experience. J. Surg. Oncol. 2021, 123, 1177–1187. [Google Scholar] [CrossRef]
- Salzano, G.; Maglitto, F.; Guida, A.; Perri, F.; Maglione, M.G.; Buonopane, S.; Muto, P.; Ionna, F. Surgical oncology of the head and neck district during COVID-19 pandemic. Eur. Arch. Oto-Rhino-Laryngol. 2021, 278, 3107–3111. [Google Scholar] [CrossRef]
- Batra, T.K.; Tilak, M.R.; Pai, E.; Verma, N.; Gupta, B.K.; Yadav, G.; Dubey, R.K.; Francis, N.J.; Pandey, M. Increased tracheostomy rates in head and neck cancer surgery during the COVID-19 pandemic. Int. J. Oral. Maxillofac. Surg. 2021, 50, 989–993. [Google Scholar] [CrossRef]
- Riemann, S.; Speck, I.; Gerstacker, K.; Becker, C.; Knopf, A. Collateral damage of the COVID-19 pandemic: An alarming decline in critical procedures in otorhinolaryngology in a German university hospital. Eur. Arch. Oto-Rhino-Laryngol. 2020, 15, 3417–3423. [Google Scholar] [CrossRef]
- National Comprehensive Cancer Network. Head and Neck Cancers; National Comprehensive Cancer Network: Plymouth Meeting, PA, USA, 2020. [Google Scholar]
- US Government Accountability Office. Status of the Healthcare System in New Orleans; US Government Accountability Office: Washington, DC, USA, 2006; Volume 717, pp. 1–15.
- Yan, F.; Knochelmann, H.M.; Morgan, P.F.; Kaczmar, J.M.; Neskey, D.M.; Graboyes, E.M.; Nguyen, S.A.; Ogretmen, B.; Sharma, A.K.; Day, T.A. The evolution of care of cancers of the head and neck region: State of the science in 2020. Cancers 2020, 12, 1543. [Google Scholar] [CrossRef]
- Barbosa, T.P.; da Costa, F.B.P.; Ramos, A.C.V.; Berra, T.Z.; Arroyo, L.H.; Alves, Y.M.; Santos, F.L.D.; Arcêncio, F.L.A. COVID-19 morbidity and mortality associated with chronic disorders, healthcare services, and inequity: Evidence for a syndemic. Rev. Panam. Salud Publica 2022, 46, e6. [Google Scholar]
- Jensen, A.R.; Nellemann, H.M.; Overgaard, J. Tumor progression in waiting time for radiotherapy in head and neck cancer. Radiother. Oncol. 2007, 84, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Kiong, K.L.; Guo, T.; Yao, C.M.K.L.; Gross, N.D.; Hanasono, M.M.; Ferrarotto, R.; Rosenthal, D.I.; Myers, J.N.; Hanna, E.Y.; Lai, S.Y. Changing practice patterns in head and neck oncologic surgery in the early COVID-19 era. Head Neck 2020, 42, 1179–1186. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Selection Criteria | Inclusion Criteria | Exclusion Criteria |
|---|---|---|
| Participants | Patients with head and neck carcinoma | Patients with other carcinomas |
| Interventions | Studies that analyze the impact of the pandemic on the treatment and management of these patients | Studies that analyze other variables |
| Comparisons | Comparison with the same period of previous years with p-values | Studies that do not compare with the pre-pandemic period |
| Outcomes | Influence of the pandemic on the way in which this pathology is treated and managed, presenting statistical analysis of the data | Studies that only assess the impact of the pandemic on the diagnosis of these patients; without statistical analysis |
| Study types | Controlled clinical trials, case-controls, experimental, quasi-experimental, analytical cross-studies, observational studies | Reviews, systematic reviews and meta-analysis, comments, expert opinion |
| Publication date | 2020–2021 | Before 2020 |
| Languages | Portuguese, Spanish, English | Other languages |
| Authors | Year | Country | Study Type | Sample | Objective | Statistical Tests |
|---|---|---|---|---|---|---|
| Tevetoglu et al. [10] | 2021 | Turkey | Retrospective observational study | 56 patients were diagnosed and scheduled for head and neck surgery at the Tertiary Care Center from 15 March to 15 September 2020, compared to 60 patients scheduled in the same period of 2019. | Assess how COVID-19 affected patients with head and neck cancer. | Mann-Whitney U test Chi-square test |
| Wai et al. [11] | 2020 | USA | Retrospective observational study | 83 patients were scheduled for cancer or reconstructive surgery at the Oncology Center of the University of California San Francisco from 16 March to 16 April 2020, compared to 56 patients scheduled in the same period in 2019. | Assess how the COVID-19 pandemic has affected health care for patients with head and neck cancer. | Chi-square test t-test |
| Kiong et al. [12] | 2021 | USA | Retrospective observational study | 183 patients evaluated in MTM at the University of Texas from 14 March to 18 June 2020, compared to 252 patients evaluated in the homonymous period of 2019. | Assess the impact of the COVID-19 pandemic on healthcare and head and neck cancer patients. | Chi-square test Fisher’s exact test Mann-Whitney U test |
| Laccourreye et al. [13] | 2020 | France | Prospective observational study | 118 patients were admitted to six ENT departments of university hospitals in the Ile de France region from 17 February to 17 March 2020, compared to 106 patients admitted from 18 March to 18 April. | Impact of the pandemic on the otolaryngology department of the university hospital in the Ile-de-France region, where the epidemic was most felt. | Chi-square test Fisher’s exact test Mann–Whitney U test |
| He et al. [14] | 2021 | China | Retrospective observational study | 36 patients with head and neck cancer were treated at a radiotherapy center from 29 January to 11 April 2020, compared to 32 patients admitted to a radiotherapy center in the same period of 2019. | Compare information regarding patients admitted for radiotherapy before and after the pandemic. | Mann–Whitney U test Chi-square test Fisher’s exact test |
| Akhtar et al. [15] | 2021 | India | Retrospective observational study | 248 patients were admitted for head and neck surgery in the oncology surgery department of an academic and university hospital in North India from April to September 2020, comparing 310 patients admitted in the same period in 2019. | Evaluate the performance of this cancer care center during the first six months of the pandemic. | Chi-square test |
| Salzano et al. [16] | 2020 | Italy | Retrospective observational study | 113 patients were admitted for surgery at the ENT and maxillofacial cancer surgery department of the National Cancer Institute of Naples from 21 February to 25 May 2020, comparing 101 patients admitted in the same period in 2019. | Understanding the possible influence of the pandemic on the results of cancer surgery in patients with head and neck cancer. | t-test |
| Batra et al. [17] | 2021 | India | Prospective cohort study | 21 patients underwent head and neck surgery at a tertiary care center in India between 19 May 2020, and 30 June 2020, compared to 193 patients who underwent surgery in the same period in 2019. | Identify trends and changes experienced in surgical practice compared to the pre-COVID period. | Pearson’s correlation coefficient |
| Riemann et al. [18] | 2020 | Germany | Observational study | Patients admitted for surgical procedures in the department of otolaryngology and head and neck surgery at Freiburg Hospital 8 weeks before and 8 weeks after 16 March 2020. | Estimating the collateral damage caused by the COVID-19 pandemic in ENT patients. | Mann–Whitney U test |
| Article | Average Age | Gender (M/F) | N of Patients with COVID-19 | ||||
|---|---|---|---|---|---|---|---|
| Pre-Pandemic | Pandemic | p | Pre-Pandemic | Pandemic | p | n | |
| Tevetoglu et al. [10] | 61.2 ± 8.3 years | 59.6 ± 7.7 years | 0.47 | nr | nr | nr | 3 |
| Wai et al. [11] | 58 ± 15 years | 63 ± 15 years | 0.03 | 51/32 | 34/22 | 0.93 | 0 |
| Kiong et al. [12] | 64 years | 65 years | 0.747 | 121/35 | 87/30 | 0.538 | nr |
| Laccourreye et al. [13] | 64 years | 63 years | 0.92 | 80/38 | 79/27 | 0.3 | 3 |
| Batra et al. [17] | 47 years | 49 years | 0.58 | 165/28 | 14/7 | 0.06 | 1 |
| Riemann et al. [18] | 45.17 years | 49.02 years | 0.015 | nr | nr | nr | nr |
| Article | Time until First Hospital Admission | Time from First Admission to Surgery | ||||
|---|---|---|---|---|---|---|
| 2019 | 2020 | p | 2019 | 2020 | p | |
| Tevetoglu et al. [10] | 16.6 ± 5.9 weeks | 19.01 ± 4.6 weeks | 0.02 | 2.9 ± 1.2 weeks | 3.4 ± 2.5 weeks | 0.06 |
| Wai et al. [11] | 22 ± 50 days | 9.7 ± 8.7 days | 0.12 | In cases of microvascular reconstruction ± ablation: 35 ± 23 days | 14 ± 12 days | 0.0002 |
| Kiong et al. [12] | 12 weeks | 12 weeks | 0.391 | nr | nr | nr |
| Article | Length of Stay (Days) | Number of ICU Days | ||||
|---|---|---|---|---|---|---|
| Pre-Pandemic | Pandemic | p | Pre-Pandemic | Pandemic | p | |
| Wai et al. [11] | In cases of microvascular reconstruction ± ablation: 7.3 ± 2.5 | In cases of microvascular reconstruction ± ablation: 7.1 ± 2.5 | 0.87 | 0.63 | 0.86 | 0.33 |
| For ablation only: 2.2 ± 1.8 | For ablation only: 2.9 ± 1.6 | 0.93 | ||||
| Laccourreye et al. [13] | 3 | 3 | 0.46 | 0 | 2 | 0.86 |
| He et al. [14] | 47.5 | 47 | 0.839 | nr | nr | nr |
| Batra et al. [17] | 7 | 10 | 0.001 | nr | nr | nr |
| Article | TNM | Overall Stage | |||||||
|---|---|---|---|---|---|---|---|---|---|
| Pre-Pandemic | Pandemic | Pre-Pandemic | Pandemic | p | |||||
| T | N | T | p | N | p | ||||
| Tevetoglu et al. [10] | 43 T1–T2 | 16N+ | 26 T1–T2 | 0.049 | 20 N+ | 0.29 | n/a | n/a | n/a |
| 17 T3–T4 | 30 T3–T4 | ||||||||
| Wai et al. [11] | 19 T1–T2 (76%) | 12 N+ (40%) | 14 T1–T2 (55%) | 0.14 | 12 N+ (44%) | 0.91 | I or II: 24 (80%) | I or II: 18 (53%) | (p = 0.02) |
| 2 T3–T4 (8%) | 8 T3–T4 (30%) | III or IV: 6 (20%) | III or IV: 16 (47%) | ||||||
| Kiong et al. [12] | Of 128 patients: | 50N+ (46.7%) | Of 103 patients: | 0.111 | 36N+ (46.2%) | 0.656 | I or II: 64 (60.9%) III or IV: 41 (39.0%) | I or II: 45 (60.8%) III or IV: 29 (39.2%) | 0.782 |
| 71 T1–T2 (66.6%) | 42 T1–T2 (53.8%) | ||||||||
| 35 T3–T4 (32.7%) | 31 T3–T4 (39.8%) | ||||||||
| Laccourreye et al. [13] | 48 T1–T2 | 63 N0–N1 6N2–N3 | 28 T1–T2 | 0.002 | 40 N0–N1 21 N2–N3 | 0.0004 | nr | nr | nr |
| 12 T3–T4 | 26 T3–T4 | ||||||||
| Batra et al. [17] | 8 T0 (4.1%) | 95 N0 (49.2%) 98 N+ (50.8%) | 12 T1–T2 (57.2%) 9 T3–T4 (42.8%) | 0.09 | 9 N0 (42.9%) 12 N+ (57.1%) | 0.28 | nr | nr | nr |
| 57 T1–T2 (29.5%) | |||||||||
| 128 T3–T4 (66.4%) | |||||||||
| Article | Number of Patients with a History of Pre-Surgical Treatment | Number of Patients with a History of Recurrence | ||||
|---|---|---|---|---|---|---|
| Pre-Pandemic | Pandemic | p | Pre-Pandemic | Pandemic | p | |
| Wai et al. [11] | 9 (11%) | 3 (5%) | 0.18 | 16 (34%) | 12 (27%) | 0.39 |
| Kiong et al. [12] | 28 (17.9%) | 14 (12%) | 0.175 | 31 (19.9%) | 30 (25.6%) | 0.257 |
| Batra et al. [17] | 71 (36.8%) | 10 (47.6%) | 0.35 | nr | nr | nr |
| Article | Diagnostic Procedures | Total surgical procedures | ||||
|---|---|---|---|---|---|---|
| Pre-Pandemic | Pandemic | p | Pre-Pandemic | Pandemic | p | |
| Wai et al. [11] | 6 (7%) | 7 (11%) | 0.4 | Transoral Robotic Surgery: 6 (7%) | Transoral Robotic Surgery: 11 (17%) | 0.05 |
| Thyroid: 19 (23%) | Thyroid: 1 (2%) | <0.0001 | ||||
| Other Surgeries: 59 | Other Surgeries: 51 | >0.05 | ||||
| Laccourreye et al. [13] | 47 | 44 | 0.81 | 71 | 62 | 0.54 |
| Akhtar et al. [15] | nr | nr | nr | 310 (52%) | 248 (60%) | 0.012 |
| Salzano et al. [16] | nr | nr | nr | 101 | 113 | 0.0011 |
| Riemann et al. [18] | 22/week | 12/week | <0.005 | nr | nr | nr |
| Article | Reconstructive Surgeries | Postoperative Complications | ||||
|---|---|---|---|---|---|---|
| Pre-Pandemic | Pandemic | p | Pre-Pandemic | Pandemic | p | |
| Tevetoglu et al. [10] | Total: 6 | 9 | 0.19 | nr | nr | nr |
| Only oral cavity: 5 | 8 | 0.024 | ||||
| Wai et al. [11] | Microvascular Reconstruction ± ablation: 10 (12%) | Microvascular Reconstruction ± ablation: 15 (24%) | 0.06 | 16 (19%) | 14 (22%) | >0.05 |
| Local Reconstruction: 4 (5%) | Local Reconstruction: 9 (14%) | 0.04 | ||||
| Laccourreye et al. [13] | 16 | 19 | 0.32 | 17 | 16 | 0.99 |
| Akhtar et al. [15] | nr | nr | nr | 27 (8%) | 30 (12%) | 0.114 |
| Batra et al. [17] | 115 (59.6%) | 7 (33.3%) | 0.03 | nr | nr | nr |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pereira, M.C.P.; Fernandes, J.C.H.; Fernandes, G.V.O.; Nor, F.; Marques, T.; Couto, P. Impact of the COVID-19 Pandemic Period on Patients with Head and Neck Carcinoma: A Systematic Review. Diseases 2023, 11, 61. https://doi.org/10.3390/diseases11020061
Pereira MCP, Fernandes JCH, Fernandes GVO, Nor F, Marques T, Couto P. Impact of the COVID-19 Pandemic Period on Patients with Head and Neck Carcinoma: A Systematic Review. Diseases. 2023; 11(2):61. https://doi.org/10.3390/diseases11020061
Chicago/Turabian StylePereira, Maria Carolina Pinto, Juliana Campos Hasse Fernandes, Gustavo Vicentis Oliveira Fernandes, Felipe Nor, Tiago Marques, and Patrícia Couto. 2023. "Impact of the COVID-19 Pandemic Period on Patients with Head and Neck Carcinoma: A Systematic Review" Diseases 11, no. 2: 61. https://doi.org/10.3390/diseases11020061