
Similarities in Bacterial Uropathogens and Their Antimicrobial Susceptibility Profile in Diabetics and Their Non-Diabetic Caregivers at a National Diabetes Management and Research Centre, Accra-Ghana
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design, Site and Sampling
2.2. Sample Sizes Determination
2.3. Identification and Antimicrobial Susceptibility Testing of Bacteria Isolates
2.4. Statistical Analysis
2.5. Ethical Clearance
3. Results
3.1. Sociodemographic Data of Study Participants
3.2. Prevalence of Urinary Tract Bacterial Pathogens in the Diabetic and Non-Diabetic Individuals
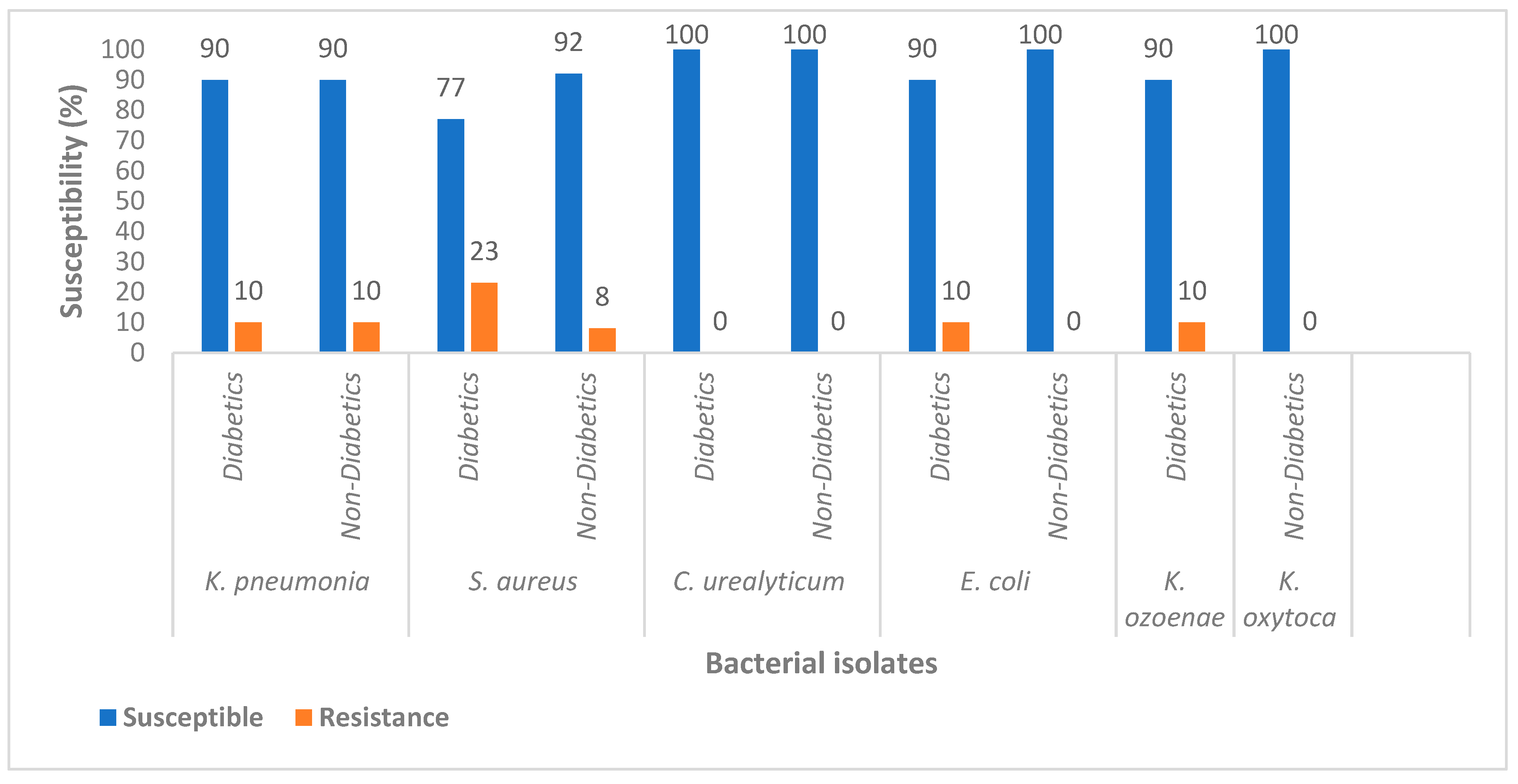
3.3. Susceptibility Profile of Bacteria Pathogens Isolated from Diabetic and Non-Diabetics
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- American Diabetes Association (ADA). 2. Classification and diagnosis of diabetes. Diabetes Care. 2015, 38 (Suppl. 1), S8–S16. [Google Scholar] [CrossRef] [Green Version]
- Schneeberger, C.; Kazemier, B.M.; Geerlings, S.E. Asymptomatic bacteriuria and urinary tract infections in special patient groups: Women with diabetes mellitus and pregnant women. Curr. Opin. Infect. Dis. 2014, 27, 108–114. [Google Scholar] [CrossRef] [Green Version]
- Abdul-Sahib, K.Y. Study of ciprofloxacin resistant Escherichia coli (CREC) in type 2 diabetic patients with symptomatic urinary tract infections. Iraqi J. Commun. Med. 2008, 21, 58–63. [Google Scholar]
- Wautier, J.L.; Guillausseau, P.J. Advanced glycation end products, their receptors and diabetic angiopathy. Diabetes Metab. 2001, 27, 535–542. [Google Scholar] [CrossRef]
- Beckman, J.A.; Creager, M.A.; Libby, P. Diabetes and atherosclerosis: Epidemiology, pathophysiology, and management. JAMA 2002, 287, 2570–2581. [Google Scholar] [CrossRef]
- Fu, A.Z.; Qiu, Y.; Radican, L.; Wells, B.J. Health care and productivity costs associated with diabetic patients with macrovascular comorbid conditions. Diabetes Care 2009, 32, 2187–2192. [Google Scholar] [CrossRef] [Green Version]
- Aikins, A.D.-G.; Agyei-Mensah, S.; Agyemang, C. Chronic Non-Communicable Diseases in Ghana: Multidisciplinary Perspectives, 1st ed.; Sub Sahara Publishers: Accra, Ghana, 2013; Chapter 3; pp. 41–55. [Google Scholar]
- Asamoah-Boaheng, M.; Sarfo-Kantanka, O.; Tuffour, A.B.; Eghan, B.; Mbanya, J.C. Prevalence and risk factors for diabetes mellitus among adults in Ghana: A systematic review and meta-analysis. Int. Health 2019, 11, 83–92. [Google Scholar] [CrossRef]
- Ribera, M.C.; Pascual, R.; Orozco, D.; Barba, C.P.; Pedrera, V.; Gil, V. Incidence and risk factors associated with urinary tract infection in diabetic patients with and without asymptomatic bacteriuria. Eur. J. Clin. Microbiol. Infect. Dis. 2006, 25, 389–393. [Google Scholar] [CrossRef]
- Julka, S. Genitourinary infection in diabetes. Indian J. Endocrinol. Metab. 2013, 17 (Suppl. 1), S83–S87. [Google Scholar] [CrossRef]
- Sussman, M.; Gally, D.L. The biology of cystitis: Host and bacterial factors. Annu. Rev. Med. 1999, 50, 149–158. [Google Scholar] [CrossRef]
- Donkor, E.S.; Horlortu, P.Z.; Dayie, N.T.; Obeng-Nkrumah, N.; Labi, A.K. Community acquired urinary tract infections among adults in Accra, Ghana. Infect. Drug Resist. 2019, 12, 2059–2067. [Google Scholar] [CrossRef] [PubMed]
- Worku, G.Y.; Alamneh, Y.B.; Abegaz, W.E. Prevalence of Bacterial Urinary Tract Infection and Antimicrobial Susceptibility Patterns Among Diabetes Mellitus Patients Attending Zewditu Memorial Hospital, Addis Ababa, Ethiopia. Infect. Drug Resist. 2021, 14, 1441–1454. [Google Scholar] [CrossRef] [PubMed]
- Akbar, D.H. Urinary tract infection. Diabet. Non-Diabet. Patients. Saudi Med. J. 2001, 22, 326–329. [Google Scholar]
- Ramrakhia, S.; Raja, K.; Dev, K.; Kumar, A.; Kumar, V.; Kumar, B. Comparison of Incidence of Urinary Tract Infection in Diabetic vs Non-Diabetic and Associated Pathogens. Cureus 2020, 12, e10500. [Google Scholar] [CrossRef]
- Geerlings, S.E.; Stolk, R.P.; Camps, M.J.; Netten, P.M.; Hoekstra, J.B.; Bouter, K.P.; Bravenboer, B.; Collet, J.T.; Jansz, A.R.; Hoepelman, A.I. Asymptomatic bacteriuria may be considered a complication in women with diabetes. Diabetes Care 2000, 23, 744–749. [Google Scholar] [CrossRef] [Green Version]
- Johnsson, K.M.; Ptaszynska, A.; Schmitz, B.; Sugg, J.; Parikh, S.J.; List, J.F. Urinary tract infections in patients with diabetes treated with dapagliflozin. J. Diabetes Its Complicat. 2013, 27, 473–478. [Google Scholar] [CrossRef] [PubMed]
- Nitzan, O.; Elias, M.; Chazan, B.; Saliba, W. Urinary tract infections in patients with type 2 diabetes mellitus: Review of prevalence, diagnosis, and management. Diabetes Metab. Syndr. Obes 2015, 8, 129–136. [Google Scholar]
- Abebe, M.; Adane, T.; Kefyalew, K.; Munduno, T.; Fasil, A.; Biadgo, B.; Ambachew, S.; Shahnawaz, S. Variation of Urine Parameters among Diabetic Patients: A Cross-Sectional Study. Ethiop. J. Health Sci. 2019, 29, 877–886. [Google Scholar] [CrossRef]
- Walsh, C.; Collyns, T. Pathophysiology of urinary tract infections. Surgery 2017, 35, 293–298. [Google Scholar]
- Monteiro, A.; Cardoso, J.; Guerra, N.; Ribeiro, E.; Viegas, C.; Cabo Verde, S.; Sousa-Uva, A. Exposure and Health Effects of Bacteria in Healthcare Units: An Overview. Appl. Sci. 2022, 12, 1958. [Google Scholar] [CrossRef]
- Khan, M.I.; Xu, S.; Ali, M.M.; Ali, R.; Kazmi, A.; Akhtar, N.; Bilal, M.; Hu, Y.; Li, F. Assessment of multidrug resistance in bacterial isolates from urinary tract-infected patients. J. Radiat. Res. Appl. Sci. 2020, 13, 267–275. [Google Scholar] [CrossRef] [Green Version]
- Madrazo, M.; Esparcia, A.; López-Cruz, I.; Alberola, J.; Piles, L.; Viana, A.; Eiros, J.M.; Artero, A. Clinical impact of multidrug-resistant bacteria in older hospitalized patients with community-acquired urinary tract infection. BMC Infect. Dis. 2021, 21, 1232. [Google Scholar] [CrossRef]
- Patterson, J.E.; Andriole, V.T. Bacterial urinary tract infections in diabetes. Infect. Dis. Clin. N. Am. 1997, 11, 735–750. [Google Scholar] [CrossRef]
- Gorter, K.J.; Hak, E.; Zuithoff, N.P.; Hoepelman, A.I.; Rutten, G.E. Risk of recurrent acute lower urinary tract infections and prescription pattern of antibiotics in women with and without diabetes in primary care. Fam. Pract. 2010, 27, 379–385. [Google Scholar] [CrossRef]
- Salari, N.; Karami, M.M.; Bokaee, S.; Chaleshgar, M.; Shohaimi, S.; Akbari, H.; Mohammadi, M. The prevalence of urinary tract infections in type 2 diabetic patients: A systematic review and meta-analysis. Eur. J. Med. Res. 2022, 27, 20. [Google Scholar] [CrossRef]
- Hamdan, H.Z.; Kubbara, E.; Adam, A.M.; Hassan, O.S.; Suliman, S.O.; Adam, I. Urinary tract infections and antimicrobial sensitivity among diabetic patients at Khartoum, Sudan. Ann. Clin. Microbiol. Antimicrob. 2015, 14, 26. [Google Scholar] [CrossRef] [Green Version]
- Jagadeesan, S.; Tripathi, B.K.; Patel, P.; Muthathal, S. Urinary tract infection and Diabetes Mellitus-Etio-clinical profile and antibiogram: A North Indian perspective. J. Fam. Med. Prim. Care 2022, 11, 1902–1906. [Google Scholar] [CrossRef]
- Yeshitela, B.; Gebre-Selassie, S.; Feleke, Y. Asymptomatic bacteriuria and symptomatic urinary tract infections (UTI) in patients with diabetes mellitus in Tikur Anbessa Specialized University Hospital. Addis Ababa, Ethiopia. Ethiop. Med. J. 2012, 50, 239–249. [Google Scholar]
- Mgbakogu, R.A.; Eledo, B.O. Studies on urinary tract infection among diabetic patients in some eastern state of Nigeria. Adv. Life Sci. Technol. 2015, 34, 42–46. [Google Scholar]
- Bissong, M.E.A.; Fon, P.; Tabe-Besong, F.; Akenji, T.N. Asymptomatic bacteriuria in diabetic mellitus patients in southwest Cameroun. Afr. Health Sci. 2013, 13, 661–666. [Google Scholar]
- Sakyi, S.A.; Ephraim, R.K.D.; Adebisi, B.O.; Yeboah, J.O.; Osei-Berchie, G. Asymptomatic bacteri- uria among type 2 diabetics in the Sekondi-Takoradi Metropolis, Ghana. J. Med. Sci. 2013, 13, 290–295. [Google Scholar] [CrossRef] [Green Version]
- Bonadio, M.; Meini, M.; Gigli, C.; Longo, B.; Vigna, A. Urinary Tract Infection in Diabetic Patients. Urol. Int. 1999, 63, 215–219. [Google Scholar] [CrossRef] [PubMed]
- Mohammadshahi, J.; Iranparvar, M.; Habibzadeh, S.; Teimourpour, R. Microbiological Profile and Antibiotic Resistance Pattern of Uropathogens in Diabetic and Non-Diabetic Patients. J. Res. Appl. Basic Med. Sci. 2020, 6, 216–232. [Google Scholar]
- Gupta, S.; Jain, U.; Chauhan, N. Laboratory diagnosis of HbA1c: A review. J. Nanomed. Res. 2017, 5, 00120. [Google Scholar]
- Inzucchi, S.E.; Bergenstal, R.M.; Buse, J.B.; Diamant, M.; Ferrannini, E.; Nauck, M.; Peters, A.; Tsapas, A.; Wender, R.; Matthews, D.R. Management of hyperglycaemia in type 2 diabetes, 2015: A patient-centred approach. Update to a position statement of the American Diabetes Association and the European Association for the Study of Diabetes. Diabetologia 2015, 58, 429–442. [Google Scholar] [CrossRef]
- Djonor, S.K.; Ako-Nnubeng, I.T.; Owusu, E.A.; Akuffo, K.O.; Nortey, P.; Agyei-Manu, E.; Danso-Appiah, A. Determinants of blood glucose control among people with Type 2 diabetes in a regional hospital in Ghana. PLoS ONE 2021, 16, e0261455. [Google Scholar] [CrossRef]
- Owusu, E.; Ahorlu, M.M.; Afutu, E.; Akumwena, A.; Asare, G.A. Antimicrobial Activity of Selected Medicinal Plants from a Sub-Saharan African Country against Bacterial Pathogens from Post-Operative Wound Infections. Med. Sci. 2021, 9, 23. [Google Scholar] [CrossRef]
- Flournoy, D.J.; Wongpradit, S.; Silberg, S.L. Facilitating Identification of Lactose-Fermenting Enterobacteriaceae on MacConkey Agar. Proc. Okla. Acad. Sci. 1990, 70, 5–8. [Google Scholar]
- Bauer, A.W.; Kirby, W.M.; Sherris, J.C.; Turck, M. Antibiotic susceptibility testing by a standardized single disk method. Am. J. Clin. Pathol. 1966, 45, 493–496. [Google Scholar] [CrossRef]
- National Committee for Clinical Laboratory Standards. Performance Standards for Antimicrobial Susceptibility Testing. Fifteenth Informational Supplement. NCCLS Document M100-S15. 2005. Available online: http://www.clsi.org/ (accessed on 6 November 2021).
- Todar, K. Todar’s Online Textbook of Bacteriology: Streptococcus Pneumonia. 2004. Available online: http://www.textbookofbacteriology.net/S.pneumoniae.html (accessed on 8 September 2013).
- Ryan, K.J.; Ray, C.G. (Eds.) Sherris Medical Microbiology, 4th ed.; McGraw Hill: New York, NY, USA, 2004. [Google Scholar]
- Jimah, T.; Fenny, A.P.; Ogunseitan, O.A. Antibiotics stewardship in Ghana: A cross-sectional study of public knowledge, attitudes, and practices among communities. One Health Outlook 2020, 2, 12. [Google Scholar] [CrossRef]
- Diao, X.; Magalhaes, E.; Silver, J. Cities and Rural Transformation: A Spatial Analysis of Rural Youth Livelihoods in Ghana. IFPRI Discussion Paper 1599. 2017. Available online: https://papers.ssrn.com/sol3/papers.cfm?abstract_id=2908519// (accessed on 24 August 2022).
- Ekwealor, C.C.; Alaribe, O.J.; Ogbukagu, C.M.; Alaribe, J.R.; Kyrian-Ogbonna, E.A. Urinary Tract Infections and Antimicrobial Sensitivity Patterns of Uropathogens Isolated from Diabetic and Non-diabetic Patients Attending Some Hospitals in Awka. Am. J. Microbiol. Res. 2021, 9, 83–91. [Google Scholar]
- Nigussie, D.; Amsalu, A. Prevalence of uropathogen and their antibiotic resistance pattern among diabetic patients. Turk. J. Urol. 2017, 43, 85–92. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Akinnibosun, F.I.; Iriakpe, H.J. Prevalence of Uropathogens in Diabetic Patients and their Antimicrobial Susceptibility Pattern. Niger. J. Microbiol. 2016, 30, 3235–3240. [Google Scholar]
- Anejo-Okopi, J.A.; Okojokwu, O.J.; Ramyil, S.M.; Bakwet, P.B.; Okechalu, J.; Agada, G.; Bassi, P.A.; Adeniyi, S.D. Bacterial and antibiotic susceptibility pattern of urinary tract infection isolated from asymptomatic and symptomatic diabetic patients attending tertiary hospital in Jos. Nigeria. Trends Med. 2017, 17, 1–5. [Google Scholar] [CrossRef] [Green Version]
- Adeyeba, O.A.; Adesiji, Y.O.; Omosigho, P.O. Bacterial urinary tract infections in patients with diabetes mellitus. Int. Trop. J. Med. 2007, 2, 89–92. [Google Scholar]
- Shah, M.A.; Kassab, Y.W.; Anwar, M.F.; Al-dahoul, H.K.; Menon, S. Prevalence and associated factors of urinary tract infections among diabetic patients. Health Sci. J. 2019, 13, 646. [Google Scholar]
- Nabaigwa, B.I.; Mwambi, B.; Okiria, J.; Oyet, C. Common uropathogens among diabetic patients with urinary tract infection at Jinja Regional Referral Hospital, Uganda. Afr. J. Lab. Med. 2018, 7, a621. [Google Scholar] [CrossRef] [Green Version]
- Goswami, R.; Bal, C.S.; Tejaswi, S.; Punjabi, G.V.; Kapil, A.; Kochupillai, N. Prevalence of urinary tract infection and renal scars in patients with diabetes mellitus. Diabetes Res. Clin. Pract. 2001, 53, 181–186. [Google Scholar] [CrossRef]
- Bashir, M.F.; Qazi, J.I.; Ahmad, N.; Riaz, S. Diversity of urinary tract pathogens and drug resistant isolates of Escherichia coli in different age and gender groups of Pakistanis. Trop. J. Pharm. Res. 2008, 7, 1025–1031. [Google Scholar] [CrossRef]
- Andriole, V.T. Asymptomatic bacteriuria in patients with diabetes—enemy or innocent visitor? N. Engl. J. Med. 2002, 347, 1617–1618. [Google Scholar] [CrossRef]
- Dudley, J.P. Atrophic rhinitis: Antibiotic treatment. Am. J. Otolaryngol. 1987, 8, 387–390. [Google Scholar] [CrossRef] [PubMed]
- Nielsen, B.C.; Olinder-Nielsen, A.M.; Malmborg, A.S. Successful treatment of ozena with ciprofloxacin. Rhinology 1995, 33, 57–60. [Google Scholar] [PubMed]
- Podschun, R.; Ullmann, U. Klebsiella spp. as nosocomial pathogens: Epidemiology, taxonomy, typing methods, and pathogenicity factors. Clin. Microbiol. Rev. 1998, 11, 589–603. [Google Scholar] [CrossRef] [Green Version]
- Mete, B.; Aybar Bilir, Y.; Aygun, G.; Yilmaz, M.; Urkmez, S.; Dilmen, Y.; Ozturk, R. Klebsiella oxytoca outbreak in an intensive care unit: A probable link to common insulin vial use. Anaesth Intensive Care 2013, 41, 266–268. [Google Scholar]
- Korvick, J.A.; Bryan, C.S.; Farber, B.; Beam, T.R.; Schenfeld, L.; Muder, R.R.; Weinbaum, D.; Lumish, R.; Gerding, D.N.; Wagener, M.M. Prospective observational study of Klebsiella bacteremia in 230 patients: Outcome for antibiotic combinations versus monotherapy. Antimicrob. Agents Chemother. 1992, 36, 2639–2644. [Google Scholar] [CrossRef] [PubMed]
- Woldemariam, H.K.; Geleta, D.A.; Tulu, K.D.; Aber, N.A.; Legese, M.H.; Fenta, G.M.; Ali, I. Common uropathogens and their antibiotic susceptibility pattern among diabetic patients. BMC Infect. Dis. 2019, 19, 43. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Squadrito, F.J.; del Portal, D. Nitrofurantoin. In StatPearls [Internet]; StatPearls Publishing: Treasure Island, FL, USA, 2022. Available online: https://www.ncbi.nlm.nih.gov/books/NBK470526/ (accessed on 8 June 2022).
- Porreca, A.; D’Agostino, D.; Romagnoli, D.; Del Giudice, F.; Maggi, M.; Palmer, K.; Falabella, R.; De Berardinis, E.; Sciarra, A.; Ferro, M.; et al. The Clinical Efficacy of Nitrofurantoin for Treating Uncomplicated Urinary Tract Infection in Adults: A Systematic Review of Randomized Control Trials. Urol. Int. 2021, 105, 531–540. [Google Scholar] [CrossRef]
- Bischoff, S.; Walter, T.; Gerigk, M.; Ebert, M.; Vogelmann, R. Empiric antibiotic therapy in urinary tract infection in patients with risk factors for antibiotic resistance in a German emergency department. BMC Infect. Dis. 2018, 18, 56. [Google Scholar] [CrossRef]
- D’Arcy, N.; Ashiru-Oredope, D.; Olaoye, O.; Afriyie, D.; Akello, Z.; Ankrah, D.; Asima, D.M.; Banda, D.C.; Barrett, S.; Brandish, C.; et al. Antibiotic Prescribing Patterns in Ghana, Uganda, Zambia and Tanzania Hospitals: Results from the Global Point Prevalence Survey (G-PPS) on Antimicrobial Use and Stewardship Interventions Implemented. Antibiotics 2021, 10, 1122. [Google Scholar] [CrossRef]
- Onanuga, A.; Awhowho, G.O. Antimicrobial resistance of Staphylococcus aureus strains from patients with urinary tract infections in Yenagoa, Nigeria. J. Pharm. Bioallied Sci. 2012, 4, 226–230. [Google Scholar] [CrossRef]
- Balamurugan, P.; Hema, M.; Gurmeet, K.; Sridharan, V.; Prabu, P.C.; Sumana, M.N.; Adline, P.S. Development of a biofilm inhibitor molecule against multidrug resistant Staphylococcus aureus associated with gestational urinary tract infections. Front. Microbiol. 2015, 6, 832. [Google Scholar] [CrossRef] [PubMed]
- Ramírez-Castillo, F.Y.; Moreno-Flores, A.C.; Avelar-González, F.J.; Márquez-Díaz, F.; Harel, J.; Guerrero-Barrera, A.L. An evaluation of multidrug-resistant Escherichia coli isolates in urinary tract infections from Aguascalientes, Mexico: Cross-sectional study. Ann. Clin. Microbiol. Antimicrob. 2018, 17, 34. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Diabetics | Non-Diabetics | |||
|---|---|---|---|---|
| Age Range | Sex | Sex | ||
| Female | Male | Female | Male | |
| 18–30 | 10 | 2 | 4 | 4 |
| 31–40 | 20 | 6 | 18 | 12 |
| 41–60 | 52 | 10 | 44 | 18 |
| Bacteria | Diabetic Group | Non-Diabetic Group | p-Value | ||
|---|---|---|---|---|---|
| n | % | n | % | ||
| E. coli | 14 | 50 | 8 | 30.77 | 0.894 |
| S. aureus | 2 | 7.14 | 4 | 15.38 | |
| K. pneumoniae | 4 | 14.29 | 8 | 30.77 | |
| K. ozoenae | 2 | 7.14 | 0 | 0 | |
| K. oxytoca | 0 | 0 | 4 | 15.38 | |
| C. urealyticum | 6 | 21.43 | 2 | 7.69 | |
| Total | 28 | 100 | 26 | 100 | |
| Antibiotics | Pattern (S or R) | K. pneumonia (n = 4) | K. ozoenae (n = 2) | S. aureus (n = 2) | C. urealyticum (n = 6) | E. coli (n = 14) |
|---|---|---|---|---|---|---|
| NIT | S R | 4 (100) 0 (0) | 2 (100) 0 (0) | 2 (100) 0 (0) | 6 (100) 0 (0) | 14 (100) 0 (0) |
| AMP | S R | 2 (50) 2 (50) | 2 (100) 0 (0) | 2 (100) 0 (0) | 6 (100) 0 (0) | 8 (57.1) 6 (42.9) |
| TS | S R | 4 (100) 0 (0) | 2 (100) 0 (0) | 0 (0) 2 (100) | 4 (66.7) 2 (33.3) | 6 (42.9) 8 (57.1) |
| GM | S R | 4 (100) 0 (0) | 2 (100) 0 (0) | 2 (100) 0 (0) | 6 (100) 0 (0) | 12 (85.7) 2 (14.3) |
| CXM | S R | 4 (100) 0 (0) | 2 (100) 0 (0) | 2 (100) 0 (0) | 6 (100) 0 (0) | 14 (100) 0 (0) |
| CRO | S R | 4 (100) 0 (0) | 2 (100) 0 (0) | 2 (100) 0 (0) | 6 (100) 0 (0) | 14 (100) 0 (0) |
| CTX | S R | 4 (100) 0 (0) | 2 (100) 0 (0) | 2 (100) 0 (0) | 6 (100) 0 (0) | 14 (100) 0 (0) |
| CIP | S R | 4 (100) 0 (0) | 2 (100) 0 (0) | 2 (100) 0 (0) | 6 (100) 0 (0) | 10 (71.4) 4 (28.6) |
| LEV | S R | 4 (100) 0 (0) | 2 (100) 0 (0) | 0 (0) 2 (100) | 4 (66.7) 2 (33.3) | 8 (57.1) 6 (42.9) |
| CEZ | S R | 4 (100) 0 (0) | 0 (0) 2 (100) | 2 (100) 0 (0) | 4 (66.7) 2 (33.3) | 12 (85.7) 2 (14.3) |
| PG | S R | NT | NT | 2 (100) 0 (0) | 6 (100) 0 (0) | NT |
| AMK | S R | 4 (100) 0 (0) | 2 (100) 0 (0) | 0 (0) 2 (100) | 6 (100) 0 (0) | 14 (100) 0 (0) |
| OX | S R | NT | NT | 2 (100) 0 (0) | 6 (100) 0 (0) | NT |
| Antibiotics | Pattern (S or R) | K. Pneumonia (n = 8) | K. Oxytoca (n = 4) | S. aureus (n = 4) | C. urealyticum (n = 2) | E. coli (n = 8) |
|---|---|---|---|---|---|---|
| NIT | S R | 8 (100) 0 (0) | 4 (100) 0 (0) | 4 (100) 0 (0) | 2 (100) 0 (0) | 8 (100) 0 (0) |
| AMP | S R | 0 (0) 8 (100) | 4 (100) 0 (0) | 4 (100) 0 (0) | 2 (100) 0 (0) | 8 (100) 0 (0) |
| TS | S R | 8 (100) 0 (0) | 4 (100) 0 (0) | 0 (0) 4 (100) | 2 (100) 0 (0) | 8 (100) 0 (0) |
| GM | S R | 8 (100) 0 (0) | 4 (100) 0 (0) | 4 (100) 0 (0) | 2 (100) 0 (0) | 8 (100) 0 (0) |
| CXM | S R | 8 (100) 0 (0) | 4 (100) 0 (0) | 4 (100) 0 (0) | 2 (100) 0 (0) | 8 (100) 0 (0) |
| CRO | S R | 8 (100) 0 (0) | 4 (100) 0 (0) | 4 (100) 0 (0) | 2 (100) 0 (0) | 8 (100) 0 (0) |
| CTX | S R | 8 (100) 0 (0) | 4 (100) 0 (0) | 4 (100) 0 (0) | 2 (100) 0 (0) | 8 (100) 0 (0) |
| CIP | S R | 8 (100) 0 (0) | 4 (100) 0 (0) | 4 (100) 0 (0) | 2 (100) 0 (0) | 8 (100) 0 (0) |
| LEV | S R | 8 (100) 0 (0) | 4 (100) 0 (0) | 4 (100) 0 (0) | 2 (100) 0 (0) | 8 (100) 0 (0) |
| CEZ | S R | 8 (100) 0 (0) | 4 (100) 0 (0) | 4 (100) 0 (0) | 2 (100) 0 (0) | 6 (75) 2 (25) |
| PG | S R | NT | NT | 4 (100) 0 (0) | 2 (100) 0 (0) | NT |
| AMK | S R | 8 (100) 0 (0) | 4 (100) 0 (0) | 4 (100) 0 (0) | 2 (100) 0 (0) | 8 (100) 0 (0) |
| OX | S R | NT | NT | 4 (100) 0 (0) | 2 (100) 0 (0) | NT |
| Antibiotics | S/R | Diabetics, n (%) n = 14 | Non-Diabetics, n (%) n = 8 | p-Value | Total, n (%) |
|---|---|---|---|---|---|
| NIT | S R | 14 (100) 0 (0) | 8 (100) 0 (0) | 0.702 | 22 (100) 0 (0) |
| AMP | S R | 8 (57.1) 6 (42.9) | 8 (100) 0 (0) | 0.106 | 16 (100) 6 (0) |
| TS | S R | 6 (42.9) 8 (57.1) | 8 (100) 0 (0) | 0.076 | 14 (100) 8 (0) |
| GM | S R | 12 (85.7) 2 (14.3) | 8 (100) 0 (0) | 0.825 | 20 (100) 2 (0) |
| CXM | S R | 14 (100) 0 (0) | 8 (100) 0 (0) | 0.702 | 22 (100) 0 (0) |
| CRO | S R | 14 (100) 0 (0) | 8 (100) 0 (0) | 0.702 | 22 (100) 0 (0) |
| CTX | S R | 14 (100) 0 (0) | 8 (100) 0 (0) | 0.702 | 22 (100) 0 (0) |
| CIP | S R | 10 (71.4) 4 (28.6) | 8 (100) 0 (0) | 0.321 | 18 (100) 4 (0) |
| LEV | S R | 8 (57.1) 6 (42.9) | 8 (100) 0 (0) | 0.106 | 16 (100) 6 (0) |
| CEZ | S R | 12 (85.7) 2 (14.3) | 6 (75) 2 (25) | 0.530 | 18 (75) 4 (25) |
| PG | S R | NT | NT | NT | |
| AMK | S R | 14 (100) 0 (0) | 8 (100) 0 (0) | 0.702 | 22 (100) 0 (0) |
| OX | S R | NT | NT | NT |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Owusu, E.; Adjei, H.; Afutu, E. Similarities in Bacterial Uropathogens and Their Antimicrobial Susceptibility Profile in Diabetics and Their Non-Diabetic Caregivers at a National Diabetes Management and Research Centre, Accra-Ghana. Diseases 2022, 10, 124. https://doi.org/10.3390/diseases10040124
Owusu E, Adjei H, Afutu E. Similarities in Bacterial Uropathogens and Their Antimicrobial Susceptibility Profile in Diabetics and Their Non-Diabetic Caregivers at a National Diabetes Management and Research Centre, Accra-Ghana. Diseases. 2022; 10(4):124. https://doi.org/10.3390/diseases10040124
Chicago/Turabian StyleOwusu, Enid, Henrietta Adjei, and Emmanuel Afutu. 2022. "Similarities in Bacterial Uropathogens and Their Antimicrobial Susceptibility Profile in Diabetics and Their Non-Diabetic Caregivers at a National Diabetes Management and Research Centre, Accra-Ghana" Diseases 10, no. 4: 124. https://doi.org/10.3390/diseases10040124