
Functional Gastrointestinal Diseases and Dietary Practices among Pakistani Children—A Schools Based Cross-Sectional Study

 , , and
, , and
Abstract
:1. Introduction
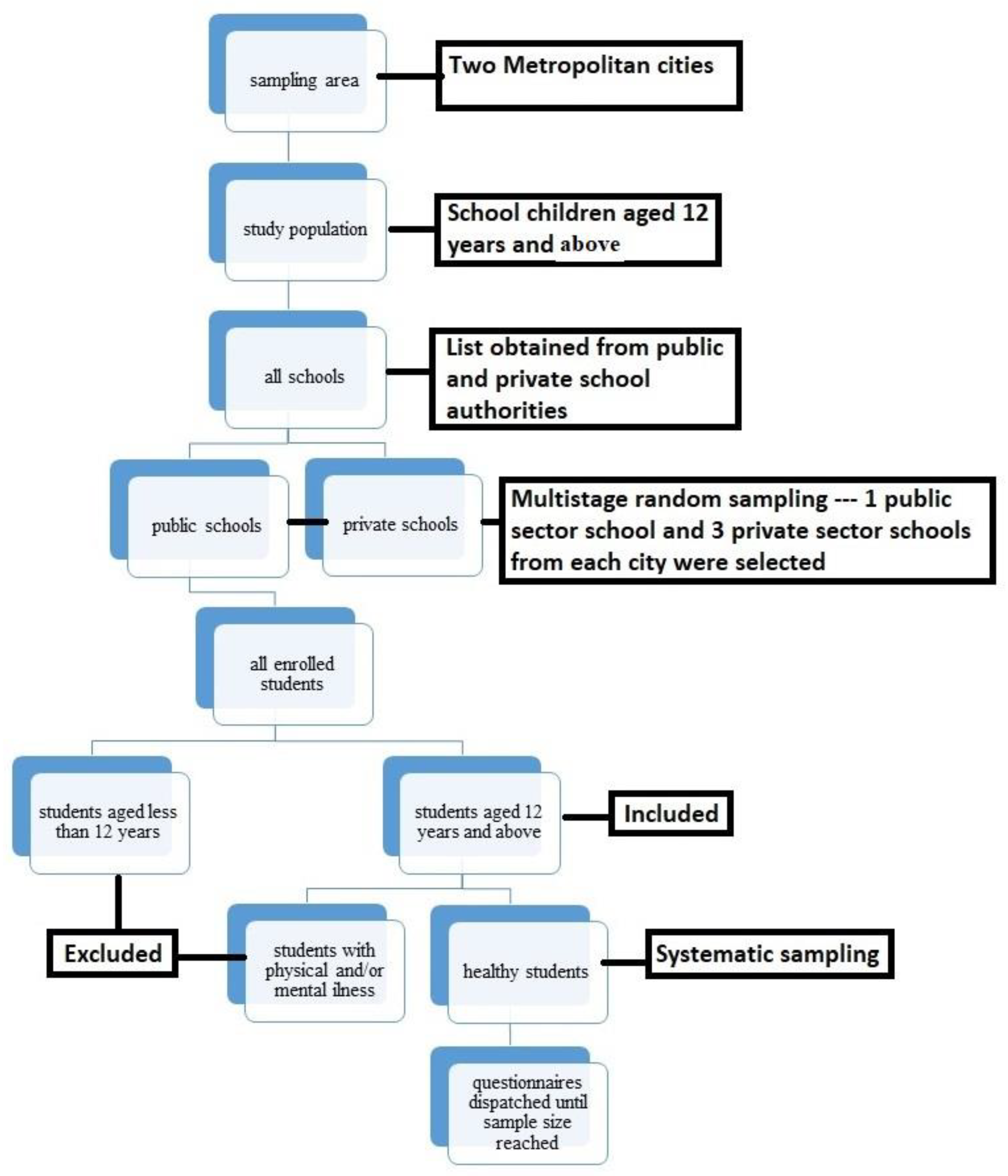
2. Methodology
- (a)
- Socio-Demographics
- (b)
- Dietary Information
- (c)
- Rome IV Criteria
Statistical Analysis
3. Results
- (a)
- Descriptive Results
Associative Relationship between Functional Gastrointestinal Disease Prevalence and Various Socio-Demographics and Dietary Factors
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Avramidou, M.; Angst, F.; Angst, J.; Aeschlimann, A.; Rössler, W.; Schnyder, U. Epidemiology of gastrointestinal symptoms in young and middle-aged Swiss adults: Prevalences and comorbidities in a longitudinal population cohort over 28 years. BMC Gastroenterol. 2018, 18, 21. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Robin, S.; Keller, C.; Zwiener, R.; Hyman, P.; Nurko, S.; Saps, M.; Di Lorenzo, C.; Shulman, R.; Hyams, J.; Palsson, O.; et al. Prevalence of pediatric functional gastrointestinal disorders utilizing the Rome IV criteria. J. Pediatr. 2018, 195, 134–139. [Google Scholar] [CrossRef] [PubMed]
- Lewis, M.L.; Palsson, O.S.; Whitehead, W.E.; van Tilburg, M.A. Prevalence of functional gastrointestinal disorders in children and adolescents. J. Pediatr. 2016, 177, 39–43. [Google Scholar] [CrossRef] [PubMed]
- Thomson, C.; Edwards, C.; Garcia, A. Digestive symptoms in UK adults and the perceived effect of foods. Curr. Dev. Nutr. 2021, 5, 458. [Google Scholar] [CrossRef]
- Thapar, N.; Benninga, M.A.; Crowell, M.D.; Di Lorenzo, C.; Mack, I.; Nurko, S.; Saps, M.; Shulman, R.J.; Szajewska, H.; van Tilburg, M.A.; et al. Paediatric functional abdominal pain disorders. Nat. Rev. Dis. Prim. 2020, 6, 89. [Google Scholar] [CrossRef]
- Ibrahim, A.T.; Hamdy, A.M.; Elhodhod, M.A. Prevalence of functional gastrointestinal disorders among school-aged children and adolescents, a multicenter study. QJM Int. J. Med. 2020, 113, hcaa063.029. [Google Scholar] [CrossRef]
- Altamimi, E.; Scarpato, E.; Saleh, I.; Tantawi, K.; Alassaf, M.; Ijam, M.; Khdour, M.; Batieneh, M.; Alsarayrah, Y.; Alaqtam, B. National prevalence of functional gastrointestinal disorders in Jordanian children. Clin. Exp. Gastroenterol. 2020, 13, 267. [Google Scholar] [CrossRef]
- Bhatia, V.; Deswal, S.; Seth, S.; Kapoor, A.; Sibal, A.; Gopalan, S. Prevalence of functional gastrointestinal disorders among adolescents in Delhi based on Rome III criteria: A school-based survey. Indian J. Gastroenterol. 2016, 35, 294–298. [Google Scholar] [CrossRef]
- Bachani, P.; Kumar, L.; Kumar, N.; Fatima, M.; Naz, S.; Memon, M.K.; Memon, S.; Rizwan, A. Prevalence of irritable bowel syndrome and frequency of symptoms in the general population of Pakistan. Cureus 2021, 13, e12541. [Google Scholar] [CrossRef]
- Tauseef, H.; Siddque, H.; Akhtar, M.; Hurera, A. Frequency of irritable bowel syndrome (IBS) and its risk factors among MBBS students of Allama Iqbal Medical College, Lahore. Pak. J. Med. Health Sci. 2021, 15, 2062–2067. [Google Scholar] [CrossRef]
- Mawani, M.; Azeem, A.; Gheewala, S.; Butt, N.; Abid, S. Understanding constipation: A cross-sectional study from a developing country setting. J. Coll. Physicians Surg. Pak. 2019, 29, 284–286. [Google Scholar] [CrossRef] [PubMed]
- Muhammad, S.; Nawaz, G.; Jamil, I.; Rehman, A.U.; Hussain, I.; Akhter, S. Constipation in pediatric patients with lower urinary tract symptoms. J. Coll. Physicians Surg. Pak. 2015, 25, 815–818. [Google Scholar] [PubMed]
- Fikree, A.; Byrne, P. Management of functional gastrointestinal disorders. Clin. Med. 2021, 21, 44. [Google Scholar] [CrossRef] [PubMed]
- Corsello, A.; Pugliese, D.; Gasbarrini, A.; Armuzzi, A. Diet and nutrients in gastrointestinal chronic diseases. Nutrients 2020, 12, 2693. [Google Scholar] [CrossRef] [PubMed]
- Fifi, A.C.; Saps, M. Diet and functional gastrointestinal disorders in children. Is the focus on food exaggerated? Nutrients 2019, 11, 250. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kosola, S.; Mundy, L.K.; Sawyer, S.M.; Canterford, L.; van der Windt, D.A.; Dunn, K.M.; Patton, G.C. Pain and learning in primary school: A population-based study. Pain 2017, 158, 1825–1830. [Google Scholar] [CrossRef]
- Malki, A. Effects of Student Nutrition on Academic Performance. Master’s Thesis, California State University, San Diego, CA, USA, 2018. [Google Scholar]
- Rome Foundation Rome IV Criteria. Available online: https://theromefoundation.org/rome-iv/rome-iv-criteria/ (accessed on 24 May 2022).
- Edwards, T.; Friesen, C.; Schurman, J.V. Classification of pediatric functional gastrointestinal disorders related to abdominal pain using Rome III vs. Rome IV criterions. BMC Gastroenterol. 2018, 18, 41. [Google Scholar] [CrossRef] [Green Version]
- Schmulson, M.J.; Drossman, D.A. What is new in Rome IV. J. Neurogastroenterol. Motil. 2017, 23, 151. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Tan, S.Y.; Parikh, P.; Buthmanaban, V.; Rajindrajith, S.; Benninga, M.A. Prevalence of functional gastrointestinal disorders in infants and young children in China. BMC Pediatr. 2021, 21, 131. [Google Scholar] [CrossRef]
- Khayat, A.; Algethami, G.; Baik, S.; Alhajori, M.; Banjar, D. The effect of using Rome IV criteria on the prevalence of functional abdominal pain disorders and functional constipation among children of the Western Region of Saudi Arabia. Glob. Pediatr. Health 2021, 8, 2333794X211022265. [Google Scholar] [CrossRef]
- Kim, Y.S.; Kim, N. Sex-gender differences in irritable bowel syndrome. J. Neurogastroenterol. Motil. 2018, 24, 544. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Johannesson, E.; Ringström, G.; Abrahamsson, H.; Sadik, R. Intervention to increase physical activity in irritable bowel syndrome shows long-term positive effects. World J. Gastroenterol. 2015, 21, 600. [Google Scholar] [CrossRef] [PubMed]
- Ghosh, D.K.; Nath, M.; Biswas, A.; Khondakar, M.F.; Ghosh, C.K. Prevalence of irritable bowel syndrome: A comparison between rural and urban settings in Bangladesh: IBS among rural and urban population. Bangladesh Med. Res. Counc. Bull. 2021, 47, 70–77. [Google Scholar] [CrossRef]
- Ng, S.C.; Kaplan, G.G.; Tang, W.; Banerjee, R.; Adigopula, B.; Underwood, F.E.; Tanyingoh, D.; Wei, S.C.; Lin, W.C.; Lin, H.H.; et al. Population density and risk of inflammatory bowel disease: A prospective population-based study in 13 countries or regions in Asia-Pacific. ACG 2019, 114, 107–115. [Google Scholar] [CrossRef] [PubMed]
- Brusaferro, A.; Farinelli, E.; Zenzeri, L.; Cozzali, R.; Esposito, S. The management of paediatric functional abdominal pain disorders: Latest evidence. Pediatr. Drugs 2018, 20, 235–247. [Google Scholar] [CrossRef] [Green Version]
- Chzhen, Y.; Howarth, C.; Main, G. Deprivation and intra-family conflict: Children as agents in the Family Stress Model. J. Marriage Fam. 2022, 84, 121–140. [Google Scholar] [CrossRef]
- Levy, E.I.; Lemmens, R.; Vandenplas, Y.; Devreker, T. Functional constipation in children: Challenges and solutions. Pediatr. Health Med. Ther. 2017, 8, 19. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Oshima, T.; Miwa, H. Definition and Prevalence. In Functional Dyspepsia; Tominaga, K., Kusunok, H., Eds.; Springer: Singapore, 2018; pp. 3–14. [Google Scholar] [CrossRef]
- Choi, Y.J.; Park, Y.S.; Kim, N.; Kim, Y.S.; Lee, S.M.; Lee, D.H.; Jung, H.C. Gender differences in ghrelin, nociception genes, psychological factors and quality of life in functional dyspepsia. World J. Gastroenterol. 2017, 23, 8053. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.E.; Kim, N.; Lee, J.Y.; Park, K.S.L.; Shin, J.E.; Nam, K.; Kim, H.J.; Song, H.J.; Joo, Y.E.; Myung, D.S.; et al. Prevalence and risk factors of functional dyspepsia in health check-up population: A nationwide multicenter prospective study. J. Neurogastroenterol. Motil. 2018, 24, 603. [Google Scholar] [CrossRef]
- Hosseini-Asl, M.K.; Taherifard, E.; Mousavi, M.R. The effect of a short-term physical activity after meals on gastrointestinal symptoms in individuals with functional abdominal bloating: A randomized clinical trial. J. Gastroenterol. Hepatol. 2021, 14, 59. [Google Scholar]
- Azmy, D.J.; Qualia, C.M. Review of abdominal migraine in children. J. Gastroenterol. Hepatol. 2020, 16, 632. [Google Scholar]
- Saps, M.; Velasco-Benitez, C.A.; Langshaw, A.H.; Ramírez-Hernández, C.R. Prevalence of functional gastrointestinal disorders in children and adolescents: Comparison between Rome III and Rome IV criteria. J. Pediatr. 2018, 199, 212–216. [Google Scholar] [CrossRef]
- Davis, A.; Bryant, J.H. Cyclic Vomiting Syndrome. In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2022. [Google Scholar]
- Kovacic, K.; Sood, M.; Venkatesan, T. Cyclic vomiting syndrome in children and adults: What is new in 2018? Curr. Gastroenterol. Rep. 2018, 20, 46. [Google Scholar] [CrossRef]
- Rajindrajith, S.; Devanarayana, N.M.; Crispus Perera, B.J. Rumination syndrome in children and adolescents: A school survey assessing prevalence and symptomatology. BMC Gastroenterol. 2012, 12, 163. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Murray, H.B.; Juarascio, A.S.; Di Lorenzo, C.; Drossman, D.A.; Thomas, J.J. Diagnosis and treatment of rumination syndrome: A critical review. Am. J. Gastroenterol. 2019, 114, 562. [Google Scholar] [CrossRef]
- Oswari, H.; Alatas, F.S.; Hegar, B.; Cheng, W.; Pramadyani, A.; Benninga, M.A.; Rajindrajith, S. Aerophagia study in Indonesia: Prevalence and association with family-related stress. J. Clin. Gastroenterol. 2021, 55, 772–777. [Google Scholar] [CrossRef] [PubMed]
- Devanarayana, N.M.; Adhikari, C.; Pannala, W.; Rajindrajith, S. Prevalence of functional gastrointestinal diseases in a cohort of Sri Lankan adolescents: Comparison between Rome II and Rome III criteria. J. Trop. Pediatr. 2011, 57, 34–39. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Variables | Categories | Frequency in Sample | Percentage in Sample (%) |
|---|---|---|---|
| Age | 12–13 years | 147 | 38.2 |
| 14–15 years | 166 | 43.1 | |
| 16 years and above | 72 | 18.7 | |
| Gender | Male | 87 | 22.6 |
| Female | 298 | 77.4 | |
| Grade of Study | 6th grade | 13 | 3.4 |
| 7th grade | 120 | 31.2 | |
| 8th grade | 78 | 45.2 | |
| 9–10th grade | 174 | 45.2 | |
| City of Residence | Rawalpindi | 196 | 50.9 |
| Islamabad | 189 | 49.1 | |
| School Area | Rural | 110 | 28.6 |
| Urban | 275 | 71.4 | |
| Family Members | 1–6 members | 260 | 67.5 |
| 7–12 members | 105 | 27.3 | |
| 13–18 members | 17 | 4.4 | |
| 19 or more members | 3 | 0.8 | |
| Family Type | Joint | 142 | 36.9 |
| Nuclear | 243 | 63.1 | |
| Father’s Occupation | Business/self-employed | 138 | 35.8 |
| Government job | 68 | 17.7 | |
| Private job | 155 | 40.3 | |
| Retired/unemployed | 13 | 3.4 | |
| Late | 11 | 2.9 | |
| Mother’s Occupation | Housewife | 344 | 89.4 |
| Employed | 36 | 9.4 | |
| Late | 5 | 1.3 | |
| Income | Less than 50,000/- | 175 | 45.5 |
| 50,000/- –100,000/- | 125 | 32.5 | |
| More than 100,000/- | 85 | 22.1 | |
| Parent’s Marital Status | Married | 363 | 94.3 |
| Separated/divorced | 10 | 2.6 | |
| Widowed | 12 | 3.1 | |
| Family History of Gastrointestinal Issues | Yes | 173 | 44.9 |
| No | 212 | 55.1 | |
| Dining Out Frequency | Once a week | 143 | 37.1 |
| Once every 2 weeks | 59 | 15.3 | |
| Once a month | 75 | 19.5 | |
| Every 2 months | 108 | 28.1 | |
| Bringing Home Lunch | Everyday | 99 | 25.7 |
| Every other day | 25 | 6.5 | |
| Once a week | 50 | 13 | |
| Less than once a week | 211 | 54.8 | |
| Engaging in Sports/Physical Activity | Everyday | 145 | 37.7 |
| Every other day | 41 | 10.6 | |
| Once a week | 119 | 30.9 | |
| Less than once a week | 80 | 20.8 |
| Consumption Frequencies | |||||
|---|---|---|---|---|---|
| Never n (%) | Less than Once a Week n(%) | Once a Week n(%) | 2–3 Times a Week n (%) | 4–6 Times a Week n(%) | Everyday n(%) |
| Cereals | |||||
| 0 (0) | 17 (4.4) | 131 (34) | 195 (50.6) | 40 (10.4) | 2 (0.5) |
| Fruits | |||||
| 3 (0.8) | 57 (14.8) | 120 (31.2) | 115 (29.9) | 55 (14.3) | 35 (9.1) |
| Vegetables | |||||
| 8 (2.1) | 129 (33.5) | 161 (41.8) | 65 (16.9) | 14 (3.6) | 8 (2.1) |
| Meat and Meat Compounds | |||||
| 2 (0.5) | 92 (23.9) | 166 (43.1) | 90 (23.4) | 22 (5.7) | 13 (3.4) |
| Pulses and Legumes | |||||
| 26 (6.8) | 112 (29.1) | 141 (36.6) | 73 (19.0) | 26 (6.8) | 7 (1.9) |
| Dairy and Dairy Products | |||||
| 3 (0.8) | 65 (16.9) | 93 (24.2) | 118 (30.6) | 70 (18.2) | 36 (9.4) |
| Snacks | |||||
| 0 (0) | 32 (8.3) | 76 (19.7) | 122 (31.7) | 107 (27.8) | 48 (12.5) |
| Beverages | |||||
| 2 (0.5) | 30 (7.8) | 96 (24.9) | 127 (33) | 93 (24.2) | 37 (9.6) |
| FGID Absent n (%) | FGID Present n (%) |
|---|---|
| Post-prandial Distress Syndrome | |
| 366 (95.1) | 19 (4.9) |
| Epigastric Pain | |
| 344 (89.4) | 41 (10.6) |
| Irritable Bowel Syndrome | |
| 289 (75.1) | 96 (24.9) |
| Abdominal Migraine | |
| 382 (99.2) | 3 (0.8) |
| Functional Abdominal Pain | |
| 236 (61.3) | 149 (38.7) |
| Functional Constipation | |
| 331 (86) | 54 (14) |
| Functional Nausea | |
| 321 (83.4) | 64 (16.6) |
| Functional Vomiting | |
| 383 (99.5) | 2 (0.5) |
| Adolescent Rumination Syndrome | |
| 379 (98.4) | 6 (1.6) |
| Aerophagia | |
| 381 (99) | 4 (1) |
| Variables | Categories | With Post-Prandial Distress n (%) | With Epi-Gastric Pain n (%) | With Irritable Bowel Syndrome n (%) | With Functional Abdominal Pain n (%) | With Functional Nausea n (%) | With Abdominal Migraine n (%) | With Adolescent Rumination Syndrome n (%) |
|---|---|---|---|---|---|---|---|---|
| Age | 12–13 years | 10 (52.6) | 16 (39.0) | 38 (39.6) | 66 (44.3) | 27 (42.2) | 1 (33.3) | 1 (16.7) |
| 14–15 years | 6 (31.6) | 16 (39.0) | 34 (35.4) | 65 (43.6) | 26 (40.6) | 1 (33.3) | 2 (33.3) | |
| 16 years and above | 3 (15.8) | 9 (22.0) | 24 (25.0) | 18 (12.1) | 11 (17.2) | 1 (33.3) | 3 (50.0) | |
| p-value | 0.43 | 0.80 | 0.10 | 0.01 * | 0.76 | 0.59 | 0.13 | |
| Gender | Male | 3 (15.8) | 16 (39.0) | 10 (10.4) | 47 (31.5) | 12 (18.8) | 0 (0.0) | 2 (33.3) |
| Female | 16 (84.2) | 25 (61.0) | 86 (89.6) | 102 (68.5) | 52 (81.3) | 3 (100.0) | 4 (66.7) | |
| p-value | 0.58 | 0.008 * | 0.001 * | 0.001 * | 0.42 | 1.00 | 0.52 | |
| Number of Family Members | 1–6 members | 14 (73.7) | 25 (61.0) | 60 (62.5) | 104 (69.8) | 47 (73.4) | 2 (66.7) | 4 (66.7) |
| 7–12 members | 4 (21.1) | 14 (34.1) | 26 (27.1) | 38 (25.5) | 11 (17.2) | 1 (33.3) | 2 (33.3) | |
| 13–18 members | 1 (5.3) | 1 (2.4) | 9 (9.4) | 6 (4.0) | 6 (9.4) | 0 (0.0) | 0 (0.0) | |
| 19 or more members | 0 (0) | 1 (2.4) | 1 (1.0) | 1 (0.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| p-value | 0.73 | 0.31 | 0.05 * | 0.91 | 0.04 * | 1.00 | 1.00 | |
| Income | Less than 50,000/- | 6 (31.6) | 9 (22.0) | 41 (42.7) | 74 (49.7) | 25 (39.1) | 1 (33.3) | 1 (16.7) |
| 50,000/- to 100,000/- | 4 (21.1) | 16 (39.0) | 33 (34.4) | 47 (31.5) | 25 (39.1) | 2 (66.7) | 3 (50.0) | |
| More than 100,000/- | 9 (47.4) | 16 (39.0) | 22 (22.9) | 28 (18.8) | 14 (21.9) | 0 (0.0) | 2 (33.3) | |
| p-value | 0.04 * | 0.002 * | 0.82 | 0.33 | 0.42 | 0.60 | 0.36 | |
| Dining Out Frequency | Once a week | 8 (42.1) | 17 (41.5) | 36 (37.5) | 54 (36.2) | 19 (29.7) | 3 (100.0) | 2 (33.3) |
| Once every 2 weeks | 3 (15.8) | 12 (29.3) | 17 (17.7) | 23 (15.4) | 9 (14.1) | 0 (0.0) | 2 (33.3) | |
| Once a month | 2 (10.5) | 6 (14.6) | 18 (18.8) | 31 (20.8) | 17 (26.9) | 0 (0.0) | 2 (33.3) | |
| Every 2 months | 6 (31.6) | 6 (14.6) | 25 (26.0) | 41 (27.5) | 19 (29.7) | 0 (0.0) | 0 (0.0) | |
| p-value | 0.79 | 0.02 * | 0.87 | 0.96 | 0.35 | 0.31 | 0.30 | |
| Bringing Home Lunch | Everyday | 6 (31.6) | 5 (12.2) | 24 (25.0) | 47 (31.5) | 17 (26.6) | 1 (33.3) | 1 (16.7) |
| Every other day | 0 (0.0) | 1 (2.4) | 9 (9.4) | 12 (8.1) | 1 (1.6) | 0 (0.0) | 1 (16.7) | |
| Once a week | 0 (0.0) | 9 (22.0) | 13 (13.5) | 17 (11.4) | 9 (14.1) | 2 (66.7) | 0 (0.0) | |
| Less than once a week | 13 (68.4) | 26 (63.4) | 50 (52.1) | 73 (49.0) | 37 (57.8) | 0 (0.0) | 4 (66.7) | |
| p-value | 0.204 | 0.04 * | 0.60 | 0.10 | 0.36 | 0.04 * | 0.54 | |
| Engaging in Sports/Physical Activity | Everyday | 4 (21.1) | 5 (12.2) | 30 (31.3) | 75 (50.3) | 21 (32.8) | 1 (33.3) | 2 (33.3) |
| Every other day | 1 (5.3) | 1 (2.4) | 11 (11.5) | 15 (10.1) | 10 (15.6) | 0 (0.0) | 2 (33.3) | |
| Once a week | 4 (21.1) | 9 (22.0) | 26 (27.1) | 34 (22.8) | 19 (29.7) | 1 (33.3) | 2 (33.3) | |
| Less than once a week | 10 (52.6) | 26 (63.4) | 29 (30.2) | 25 (16.8) | 14 (21.9) | 1 (33.3) | 0 (0.0) | |
| p-value | 0.01 * | 0.83 | 0.05 * | 0.001 * | 0.50 | 1.00 | 0.23 | |
| Fruits Consumption | Never | 0 (0.0) | 0 (0.0) | 1 (1.0) | 1 (0.7) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Less than once a week | 8 (42.1) | 5 (12.2) | 15 (15.6) | 25 (16.8) | 10 (15.6) | 0 (0.0) | 0 (0.0) | |
| Once a week | 7 (36.9) | 8 (19.5) | 31 (32.3) | 45 (30.2) | 21 (32.8) | 1 (33.3) | 3 (50.0) | |
| 2–3 times a week | 1 (5.3) | 13 (31.7) | 29 (30.2) | 41 (27.5) | 20 (31.3) | 2 (66.7) | 3 (50.0) | |
| 4–6 times a week | 3 (15.8) | 9 (22.0) | 12 (12.5) | 18 (12.1) | 5 (7.8) | 0 (0.0) | 0 (0.0) | |
| everyday | 0 (0.0) | 6 (14.6) | 8 (8.3) | 19 (12.8) | 8 (12.5) | 0 (0.0) | 0 (0.0) | |
| p-value | 0.007 * | 0.28 | 0.98 | 0.33 | 0.56 | 0.91 | 0.56 | |
| Vegetables consumption | Never | 0 (0.0) | 0 (0.0) | 2 (2.1) | 4 (2.7) | 1 (1.6) | 0 (0.0) | 0 (0.0) |
| Less than once a week | 11 (57.9) | 11 (26.8) | 34 (35.4) | 55 (36.9) | 29 (45.3) | 1 (33.3) | 3 (50.0) | |
| Once a week | 5 (26.3) | 21 (51.2) | 37 (38.5) | 58 (38.9) | 27 (42.2) | 2 (66.7) | 3 (50.0) | |
| 2–3 times a week | 1 (5.3) | 6 (14.6) | 18 (18.8) | 22 (14.8) | 5 (7.8) | 0 (0.0) | 0 (0.0) | |
| 4–6 times a week | 0 (0.0) | 3 (7.3) | 4 (4.2) | 5 (3.4) | 2 (3.1) | 0 (0.0) | 0 (0.0) | |
| everyday | 2 (10.5) | 0 (0.0) | 1 (1.0) | 5 (3.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | |
| p-value | 0.03 * | 0.46 | 0.92 | 0.49 | 0.11 | 1.00 | 0.18 | |
| Pulses and lentil consumption | Never | 3 (15.8) | 3 (7.3) | 3 (3.1) | 17 (11.4) | 2 (6.3) | 0 (0.0) | 1 (16.7) |
| Less than once a week | 5 (26.3) | 13 (31.7) | 25 (26.0) | 40 (26.8) | 19 (29.7) | 1 (33.3) | 0 (0.0) | |
| Once a week | 9 (47.4) | 15 (36.6) | 37 (38.5) | 56 (37.6) | 27 (42.2) | 0 (0.0) | 1 (16.7) | |
| 2–3 times a week | 1 (5.3) | 8 (19.5) | 21 (21.9) | 22 (14.8) | 11 (17.2) | 1 (33.3) | 2 (33.3) | |
| 4–6 times a week | 1 (5.3) | 0 (0.0) | 8 (8.3) | 11 (7.4) | 2 (3.1) | 1 (33.3) | 2 (33.3) | |
| everyday | 0 (0.0) | 2 (4.9) | 1 (1.0) | 3 (2.0) | 1 (1.6) | 0 (0.0) | 0 (0.0) | |
| p-value | 0.35 | 0.26 | 0.31 | 0.05 * | 0.85 | 0.20 | 0.05 * | |
| Beverages consumption | Never | 0 (0.0) | 1 (2.4) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) | 0 (0.0) |
| Less than once a week | 1 (5.3) | 3 (7.3) | 7 (7.3) | 13 (8.7) | 1 (1.6) | 0 (0.0) | 0 (0.0) | |
| Once a week | 9 (47.4) | 5 (12.2) | 22 (22.9) | 40 (26.8) | 15 (23.4) | 1 (33.3) | 0 (0.0) | |
| 2–3 times a week | 4 (21.1) | 18 (43.9) | 37 (38.5) | 43 (28.9) | 22 (34.4) | 0 (0.0) | 2 (33.3) | |
| 4–6 times a week | 5 (26.3) | 11 (26.8) | 22 (22.9) | 34 (22.8) | 16 (25.0) | 0 (0.0) | 4 (66.7) | |
| everyday | 0 (0.0) | 3 (7.3) | 8 (8.3) | 8 (12.8) | 10 (15.6) | 2 (66.7) | 0 (0.0) | |
| p-value | 0.23 | 0.12 | 0.87 | 0.35 | 0.18 | 0.04 * | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Malik, Z.I.; Umer, M.F.; Ali, K.N.; Kawish, A.B.; Arshed, M.; Zofeen, S.; Farid, A. Functional Gastrointestinal Diseases and Dietary Practices among Pakistani Children—A Schools Based Cross-Sectional Study. Diseases 2022, 10, 103. https://doi.org/10.3390/diseases10040103
Malik ZI, Umer MF, Ali KN, Kawish AB, Arshed M, Zofeen S, Farid A. Functional Gastrointestinal Diseases and Dietary Practices among Pakistani Children—A Schools Based Cross-Sectional Study. Diseases. 2022; 10(4):103. https://doi.org/10.3390/diseases10040103
Chicago/Turabian StyleMalik, Zoha Imtiaz, Muhammad Farooq Umer, Khizar Nabeel Ali, Ayesha Babar Kawish, Muhammad Arshed, Shumaila Zofeen, and Awais Farid. 2022. "Functional Gastrointestinal Diseases and Dietary Practices among Pakistani Children—A Schools Based Cross-Sectional Study" Diseases 10, no. 4: 103. https://doi.org/10.3390/diseases10040103