
Determinants of Post-COVID-19 Conditions among SARS-CoV-2-Infected Patients in Saudi Arabia: A Web-Based Cross-Sectional Study


 , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Sampling Strategy
2.3. Study Tool
2.4. Statistical Analysis
3. Results
3.1. Demographic Characteristics
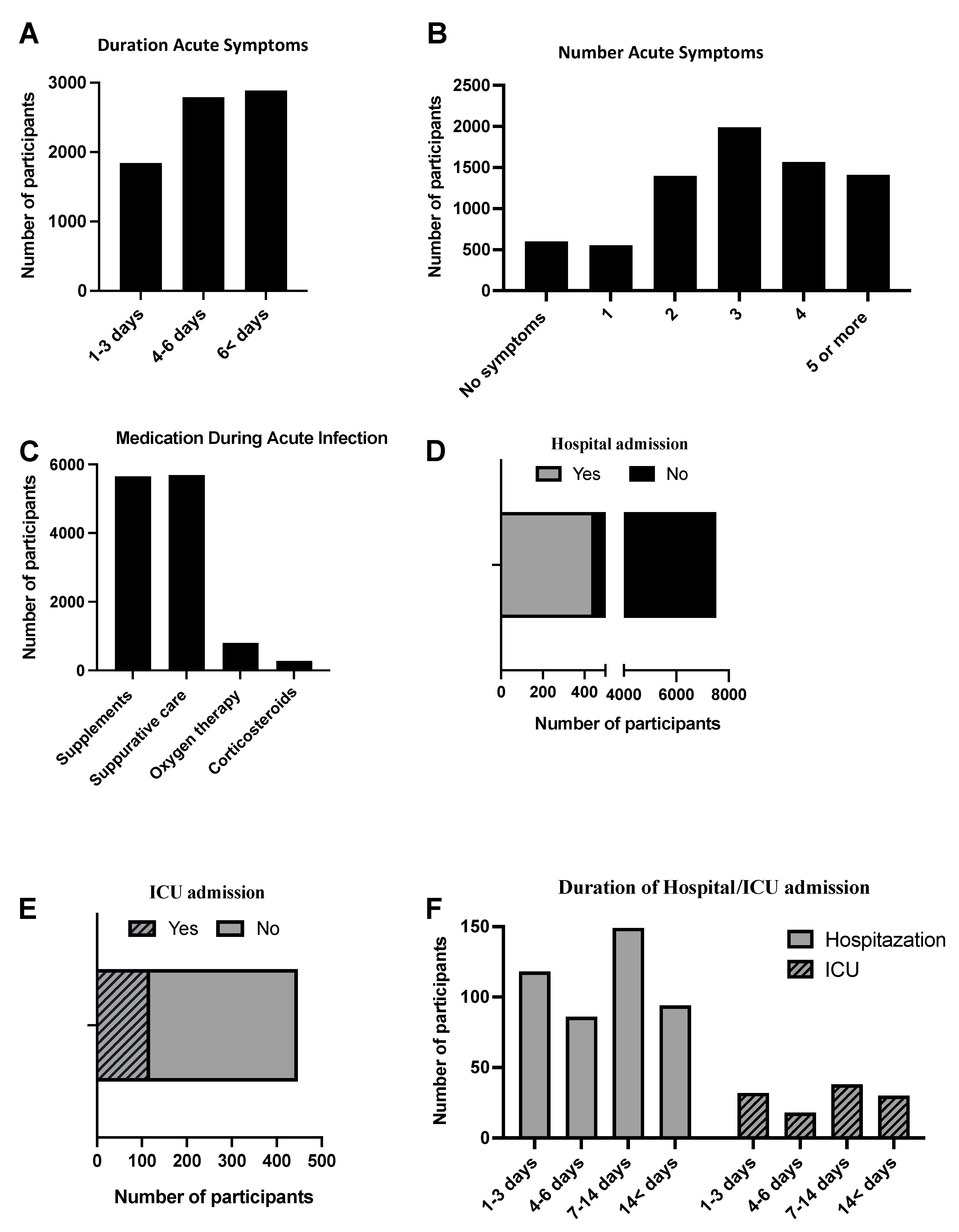
3.2. Characteristics of Acute COVID-19 among the Saudi Population
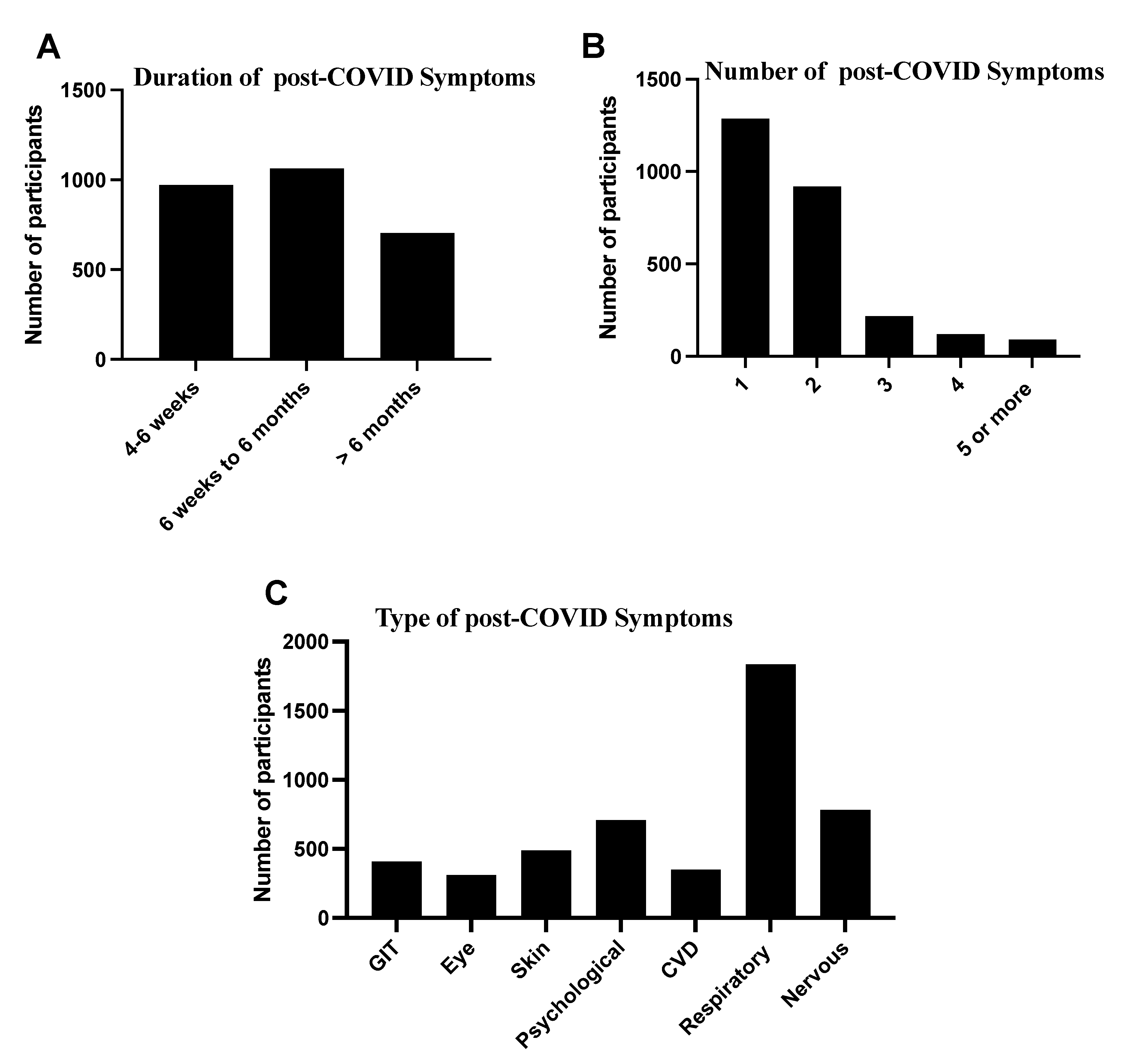
3.3. Characteristics and Risk Factors of Post-COVID-19 Conditions in the Saudi Population
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Hu, B.; Guo, H.; Zhou, P.; Shi, Z.L. Characteristics of SARS-CoV-2 and COVID-19. Nat. Rev. Microbiol. 2021, 19, 141–154. [Google Scholar] [CrossRef] [PubMed]
- Cascella, M.; Rajnik, M.; Aleem, A.; Dulebohn, S.C.; Di Napoli, R. Features, Evaluation, and Treatment of Coronavirus (COVID-19). In StatPearls; StatPearls Publishing: Treasure Island, FL, USA, 2021. [Google Scholar]
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA 2020, 324, 782–793. [Google Scholar] [CrossRef]
- CDC. Post-COVID Conditions: National Center for Immunization and Respiratory Diseases (NCIRD). 2021. Available online: https://www.cdc.gov/coronavirus/2019-ncov/long-term-effects/index.html (accessed on 1 July 2021).
- Raveendran, A.V.; Jayadevan, R.; Sashidharan, S. Long COVID: An overview. Diabetes Metab. Syndr. 2021, 15, 869–875. [Google Scholar] [CrossRef] [PubMed]
- Vehar, S.; Boushra, M.; Ntiamoah, P.; Biehl, M. Post-acute sequelae of SARS-CoV-2 infection: Caring for the ‘long-haulers’. Cleve. Clin. J. Med. 2021, 88, 267–272. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, M.; Nel, J.; Blumberg, L.; Madhi, S.A.; Dryden, M.; Stevens, W.; Venter, F.W.D. Long-COVID: An evolving problem with an extensive impact. S. Afr. Med. J. 2020, 111, 10–12. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Garrigues, E.; Janvier, P.; Kherabi, Y.; Le Bot, A.; Hamon, A.; Gouze, H.; Doucet, L.; Berkani, S.; Oliosi, E.; Mallart, E.; et al. Post-discharge persistent symptoms and health-related quality of life after hospitalization for COVID-19. J. Infect. 2020, 81, e4–e6. [Google Scholar] [CrossRef]
- Huang, C.; Huang, L.; Wang, Y.; Li, X.; Ren, L.; Gu, X.; Kang, L.; Guo, L.; Liu, M.; Zhou, X.; et al. 6-month consequences of COVID-19 in patients discharged from hospital: A cohort study. Lancet 2021, 397, 220–232. [Google Scholar] [CrossRef]
- Castanares-Zapatero, D.; Chalon, P.; Kohn, L.; Dauvrin, M.; Detollenaere, J.; Maertens de Noordhout, C.; Primus-de Jong, C.; Cleemput, I.; Van den Heede, K. Pathophysiology and mechanism of long COVID: A comprehensive review. Ann. Med. 2022, 54, 1473–1487. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention. Long COVID. Available online: https://www.cdc.gov/nchs/covid19/pulse/long-covid.htm (accessed on 24 August 2021).
- Naing, N.N. Determination of sample size. Malays J. Med. Sci. 2003, 10, 84–86. [Google Scholar]
- Peghin, M.; Palese, A.; Venturini, M.; De Martino, M.; Gerussi, V.; Graziano, E.; Bontempo, G.; Marrella, F.; Tommasini, A.; Fabris, M. Post-COVID-19 symptoms 6 months after acute infection among hospitalized and non-hospitalized patients. Clin. Microbiol. Infect. 2021, 27, 1507–1513. [Google Scholar] [CrossRef] [PubMed]
- Galal, I.; Hussein, A.A.M.; Amin, M.T.; Saad, M.M.; Zayan, H.E.E.; Abdelsayed, M.Z.; Moustafa, M.M.; Ezzat, A.R.; Helmy, R.E.; Abd_Elaal, H.K. Determinants of persistent post-COVID-19 symptoms: Value of a novel COVID-19 symptom score. Egypt. J. Bronchol. 2021, 15, 10. [Google Scholar] [CrossRef]
- Thompson, E.J.; Williams, D.M.; Walker, A.J.; Mitchell, R.E.; Niedzwiedz, C.L.; Yang, T.C.; Huggins, C.F.; Kwong, A.S.F.; Silverwood, R.J.; Di Gessa, G.; et al. Long COVID burden and risk factors in 10 UK longitudinal studies and electronic health records. Nat. Commun. 2022, 13, 3528. [Google Scholar] [CrossRef] [PubMed]
- Pazukhina, E.; Andreeva, M.; Spiridonova, E.; Bobkova, P.; Shikhaleva, A.; El-Taravi, Y.; Rumyantsev, M.; Gamirova, A.; Bairashevskaia, A.; Petrova, P.; et al. Prevalence and risk factors of post-COVID-19 condition in adults and children at 6 and 12 months after hospital discharge: A prospective, cohort study in Moscow (StopCOVID). BMC Med. 2022, 20, 244. [Google Scholar] [CrossRef]
- Nalbandian, A.; Sehgal, K.; Gupta, A.; Madhavan, M.V.; McGroder, C.; Stevens, J.S.; Cook, J.R.; Nordvig, A.S.; Shalev, D.; Sehrawat, T.S.; et al. Post-acute COVID-19 syndrome. Nat. Med. 2021, 27, 601–615. [Google Scholar] [CrossRef]
- Ahmed, H.; Patel, K.; Greenwood, D.C.; Halpin, S.; Lewthwaite, P.; Salawu, A.; Eyre, L.; Breen, A.; O’Connor, R.; Jones, A.; et al. Long-term clinical outcomes in survivors of severe acute respiratory syndrome and Middle East respiratory syndrome coronavirus outbreaks after hospitalisation or ICU admission: A systematic review and meta-analysis. J. Rehabil. Med. 2020, 52, jrm00063. [Google Scholar] [CrossRef]
- Lan, L.; Xu, D.; Ye, G.; Xia, C.; Wang, S.; Li, Y.; Xu, H. Positive RT-PCR Test Results in Patients Recovered From COVID-19. JAMA 2020, 323, 1502–1503. [Google Scholar] [CrossRef] [Green Version]
- Tay, M.Z.; Poh, C.M.; Renia, L.; MacAry, P.A.; Ng, L.F.P. The trinity of COVID-19: Immunity, inflammation and intervention. Nat. Rev. Immunol. 2020, 20, 363–374. [Google Scholar] [CrossRef]
- Forte, G.; Favieri, F.; Tambelli, R.; Casagrande, M. COVID-19 Pandemic in the Italian Population: Validation of a Post-Traumatic Stress Disorder Questionnaire and Prevalence of PTSD Symptomatology. Int. J. Environ. Res. Public Health 2020, 17, 4151. [Google Scholar] [CrossRef]
- Shabrawishi, M.; Al-Gethamy, M.M.; Naser, A.Y.; Ghazawi, M.A.; Alsharif, G.F.; Obaid, E.F.; Melebari, H.A.; Alamri, D.M.; Brinji, A.S.; Al Jehani, F.H.; et al. Clinical, radiological and therapeutic characteristics of patients with COVID-19 in Saudi Arabia. PLoS ONE 2020, 15, e0237130. [Google Scholar] [CrossRef]
- Li, L.Q.; Huang, T.; Wang, Y.Q.; Wang, Z.P.; Liang, Y.; Huang, T.B.; Zhang, H.Y.; Sun, W.; Wang, Y. COVID-19 patients’ clinical characteristics, discharge rate, and fatality rate of meta-analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef]
- Tenforde, M.W.; Self, W.H.; Adams, K.; Gaglani, M.; Ginde, A.A.; McNeal, T.; Ghamande, S.; Douin, D.J.; Talbot, H.K.; Casey, J.D. Association Between mRNA Vaccination and COVID-19 Hospitalization and Disease Severity. JAMA 2021, 326, 2043. [Google Scholar] [CrossRef]
- Braman, S.S. Postinfectious cough: ACCP evidence-based clinical practice guidelines. Chest 2006, 129, 138S–146S. [Google Scholar] [CrossRef]
- O’Neill, A. Saudi Arabia: Age Structure from 2010 to 2020. Available online: https://www.statista.com/statistics/262478/age-structure-in-saudi-arabia/ (accessed on 28 November 2021).
- Fulop, T.; Larbi, A.; Pawelec, G. Human T cell aging and the impact of persistent viral infections. Front. Immunol. 2013, 4, 271. [Google Scholar] [CrossRef] [Green Version]
- Collaboration, N.C.D.R.F. Worldwide trends in hypertension prevalence and progress in treatment and control from 1990 to 2019: A pooled analysis of 1201 population-representative studies with 104 million participants. Lancet 2021, 398, 957–980. [Google Scholar] [CrossRef]
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; et al. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res. Clin. Pract. 2019, 157, 107843. [Google Scholar] [CrossRef] [Green Version]
- Pinto, B.; Oliveira, A.; Singh, Y.; Jimenez, L.; Goncalves, A.; Ogava, R.; Creighton, R.; Peron, J.; Nakaya, H. ACE2 expression is increased in the lungs of patients with comorbidities associated with severe COVID-19. medRxiv 2020. [Google Scholar] [CrossRef]
- Brooks, S.D.; Smith, R.L.; Moreira, A.S.; Ackerman, H.C. Oral Lisinopril Raises Tissue Levels of ACE2, the SARS-CoV-2 Receptor, in Healthy Male and Female Mice. Front. Pharmacol. 2022, 13, 798349. [Google Scholar] [CrossRef]
- Fernandez-de-Las-Penas, C.; Palacios-Cena, D.; Gomez-Mayordomo, V.; Rodriuez-Jimenez, J.; Palacios-Cena, M.; Velasco-Arribas, M.; Guijarro, C.; de-la-Llave-Rincon, A.I.; Fuensalida-Novo, S.; Elvira-Martinez, C.M.; et al. Long-term post-COVID symptoms and associated risk factors in previously hospitalized patients: A multicenter study. J. Infect. 2021, 83, 237–279. [Google Scholar] [CrossRef]
- Asadi-Pooya, A.A.; Akbari, A.; Emami, A.; Lotfi, M.; Rostamihosseinkhani, M.; Nemati, H.; Barzegar, Z.; Kabiri, M.; Zeraatpisheh, Z.; Farjoud-Kouhanjani, M.; et al. Risk Factors Associated with Long COVID Syndrome: A Retrospective Study. Iran. J. Med. Sci. 2021, 46, 428–436. [Google Scholar] [CrossRef]
- Moreno-Perez, O.; Merino, E.; Leon-Ramirez, J.M.; Andres, M.; Ramos, J.M.; Arenas-Jimenez, J.; Asensio, S.; Sanchez, R.; Ruiz-Torregrosa, P.; Galan, I.; et al. Post-acute COVID-19 syndrome. Incidence and risk factors: A Mediterranean cohort study. J. Infect. 2021, 82, 378–383. [Google Scholar] [CrossRef]
- Halpin, S.J.; McIvor, C.; Whyatt, G.; Adams, A.; Harvey, O.; McLean, L.; Walshaw, C.; Kemp, S.; Corrado, J.; Singh, R.; et al. Postdischarge symptoms and rehabilitation needs in survivors of COVID-19 infection: A cross-sectional evaluation. J. Med. Virol. 2021, 93, 1013–1022. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Variable | Frequency (%) |
|---|---|
| Age | |
| Below 25 years | 3447 (45.8%) |
| 25–40 years | 2354 (31.3%) |
| 41–59 years | 1507 (20.0%) |
| 60 years and above | 212 (2.8%) |
| Gender | |
| Females | 5230 (69.5%) |
| BMI (Mean (SD) (kg/m2) | 24.0 (SD: 8.4) |
| Smoking history | |
| Non-smoker | 6290 (83.6%) |
| Ex-smoker | 351 (4.7%) |
| Smoker | 879 (11.7%) |
| Alcohol drinking (Yes) | 25 (0.3%) |
| Number of comorbidities | |
| 0 | 6083 (80.9%) |
| 1 | 975 (13.0%) |
| 2 | 303 (4.0%) |
| 3 | 111 (1.5%) |
| 4 or more | 48 (0.6%) |
| Type of comorbidities | |
| Diabetes mellitus | 455 (6.1%) |
| Hypertension | 298 (4.0%) |
| Liver diseases | 5 (0.1%) |
| Cardiovascular diseases | 68 (0.9%) |
| Chronic obstructive pulmonary diseases | 193 (2.6%) |
| Immune diseases | 77 (1.0%) |
| Psychological disorders | 134 (1.8%) |
| Obesity | 971 (12.9%) |
| Others | 370 (4.9%) |
| Chronic diseases medications use history (Yes) | 1060 (14.1%) |
| Type of chronic diseases medications | |
| Hypertension medication | 205 (2.7%) |
| Oral antidiabetic | 176 (2.3%) |
| Insulin | 64 (0.9%) |
| Combination of oral antidiabetic and insulin | 8 (0.1%) |
| Anti-hyperlipidemic agent | 47 (0.6%) |
| Aspirin | 23 (0.3%) |
| Thyroid disease medication | 89 (1.2%) |
| Inhaled corticosteroids | 29 (0.4%) |
| Gastro-protective agent | 21 (0.3%) |
| Corticosteroids | 19 (0.3%) |
| Antipsychotic agent | 9 (0.1%) |
| Variable | Odds Ratio (95% CI) |
|---|---|
| Age | |
| Below 25 years (Reference category) | 1.00 |
| 25–40 years | 1.07 (0.96–1.18) |
| 41–59 years | 1.10 (0.98–1.24) |
| 60 years and above | 1.50 (1.13–1.99) ** |
| Gender | |
| Females (Reference category) | 1.00 |
| Males | 0.72 (0.65–0.80) *** |
| BMI | |
| 24.0 kg/cm2 or lower (Reference category) | 1.00 |
| Above 24.0 kg/cm2 | 0.966 (0.86–1.06) |
| Smoking history | |
| Non-smoker (Reference category) | 1.00 |
| Ex-smoker | 0.98 (0.78–1.23) |
| Smoker | 1.00 (0.86–1.16) |
| Number of comorbidities | |
| 0 (Reference category) | 1.00 |
| 1 | 1.66 (1.31–2.10) *** |
| 2 | 1.59 (1.09–2.32) * |
| 3 | - |
| 4 or more | 2.92 (1.60–5.35) ** |
| Type of comorbidities | |
| Diabetes mellitus (Yes) | 0.89 (0.66–1.19) |
| Hypertension (Yes) | 0.81 (0.61–1.09) |
| Cardiovascular diseases (Yes) | 0.81 (0.37–1.79) |
| Chronic obstructive pulmonary diseases (Yes) | 0.95 (0.62–1.45) |
| Immune diseases (Yes) | 1.00 (0.59–1.71) |
| Obesity (Yes) | 0.66 (0.47–0.94) * |
| Psychological disorders (Yes) | 0.88 (0.50–1.55) |
| Chronic diseases medications use history | |
| No (Reference category) | 1.00 |
| Yes | 1.59 (1.39–1.82) *** |
| Length of hospital stay | |
| One–three days (Reference category) | 1.00 |
| Four–six days | 3.54 (1.33–9.43) * |
| Seven–fourteen days | 2.08 (1.09–3.98) * |
| More than fourteen days | 5.61 (2.24–14.07) *** |
| Length of ICU stay | |
| One–three days (Reference category) | 1.00 |
| Four–six days | 3.54 (1.33–9.43) * |
| Seven days and above | 3.02 (1.80–5.06) *** |
| Duration of acute symptoms | |
| 1–3 days (Reference category) | 1.00 |
| 4–6 days | 0.82 (0.74–0.91) *** |
| 7 days and above | 2.10 (1.91–2.32) *** |
| Number of acute symptoms | |
| No symptoms (Reference category) | 1.00 |
| One | 0.59 (0.48–0.72) *** |
| Two | 0.67 (0.59–0.76) *** |
| Three | 0.78 (0.70–0.88) *** |
| Four | 1.42 (1.27–1.59) *** |
| Five | - |
| Six and above | 2.61 (2.31–2.94) *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Samannodi, M.; Alwafi, H.; Naser, A.Y.; Al Qurashi, A.A.; Qedair, J.T.; Salawati, E.; Almatrafi, M.A.; Ekram, R.; Bukhari, R.I.; Dahlawi, M.; et al. Determinants of Post-COVID-19 Conditions among SARS-CoV-2-Infected Patients in Saudi Arabia: A Web-Based Cross-Sectional Study. Diseases 2022, 10, 55. https://doi.org/10.3390/diseases10030055
Samannodi M, Alwafi H, Naser AY, Al Qurashi AA, Qedair JT, Salawati E, Almatrafi MA, Ekram R, Bukhari RI, Dahlawi M, et al. Determinants of Post-COVID-19 Conditions among SARS-CoV-2-Infected Patients in Saudi Arabia: A Web-Based Cross-Sectional Study. Diseases. 2022; 10(3):55. https://doi.org/10.3390/diseases10030055
Chicago/Turabian StyleSamannodi, Mohammed, Hassan Alwafi, Abdallah Y. Naser, Abdullah A. Al Qurashi, Jumanah T. Qedair, Emad Salawati, Mohammed A. Almatrafi, Rakan Ekram, Rahaf I. Bukhari, Maryam Dahlawi, and et al. 2022. "Determinants of Post-COVID-19 Conditions among SARS-CoV-2-Infected Patients in Saudi Arabia: A Web-Based Cross-Sectional Study" Diseases 10, no. 3: 55. https://doi.org/10.3390/diseases10030055