
Mean Platelet Volume as a Predictor of COVID-19 Severity: A Prospective Cohort Study in the Highlands of Peru


 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
2.2. Study Population
2.3. Definition and Clinical Results
2.4. Statistical Analysis
3. Results
4. Discussion
4.1. Main Results
4.2. Comparison with Previous Studies
4.3. Interpretation of Findings
4.4. Relevance in Clinical Practice
4.5. Limitations and Strengths
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China: Summary of a Report of 72,314 Cases from the Chinese Center for Disease Control and Prevention. JAMA 2020, 323, 1239–1242. [Google Scholar] [CrossRef] [PubMed]
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Ozder, A. A novel indicator predicts 2019 novel coronavirus infection in subjects with diabetes. Diabetes Res. Clin. Pract. 2020, 166, 108294. [Google Scholar] [CrossRef]
- Paliogiannis, P.; Zinellu, A.; Scano, V.; Mulas, G.; De Riu, G.; Pascale, R.M.; Arru, L.B.; Carru, C.; Pirina, P.; Mangoni, A.A.; et al. Laboratory test alterations in patients with COVID-19 and non COVID-19 interstitial pneumonia: A preliminary report. J. Infect. Dev. Ctries. 2020, 14, 685–690. [Google Scholar] [CrossRef] [PubMed]
- Yun, H.; Sun, Z.; Wu, J.; Tang, A.; Hu, M.; Xiang, Z. Laboratory data analysis of novel coronavirus (COVID-19) screening in 2510 patients. Clin. Chim. Acta 2020, 507, 94–97. [Google Scholar] [CrossRef]
- Vélez, J.L. ¿El volumen medio plaquetario es un predictor de mortalidad en pacientes sépticos?: Revisión de la literatura. Rev. Med. Herediana 2018, 29, 116–120. [Google Scholar] [CrossRef]
- Ittermann, T.; Feig, M.A.; Petersmann, A.; Radke, D.; Greinacher, A.; Völzke, H.; Thiele, T. Mean platelet volume is more important than age for defining reference intervals of platelet counts. PLoS ONE 2019, 14, e0213658. [Google Scholar] [CrossRef] [Green Version]
- Noris, P.; Melazzini, F.; Balduini, C.L. New roles for mean platelet volume measurement in the clinical practice? Platelets 2016, 27, 607–612. [Google Scholar] [CrossRef]
- Gasparyan, A.Y.; Ayvazyan, L.; Mikhailidis, D.P.; Kitas, G.D. Mean platelet volume: A link between thrombosis and inflammation? Curr. Pharm. Des. 2011, 17, 47–58. [Google Scholar] [CrossRef]
- Tajarernmuang, P.; Phrommintikul, A.; Limsukon, A.; Pothirat, C.; Chittawatanarat, K. The Role of Mean Platelet Volume as a Predictor of Mortality in Critically Ill Patients: A Systematic Review and Meta-Analysis. Crit. Care Res. Pract. 2016, 2016, 4370834. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bergoli, L.C.C.; Castanho, E.S.; Gonçalves, S.C.; Wainstein, R.V.; Piardi, D.; Araújo, G.; Mossmann, M.; Krepsky, A.M.; Wainstein, M.V. Mean Platelet Volume as a Predictor of Major Cardiovascular Outcomes and Final Coronary Flow in Patients Undergoing Primary Percutaneous Coronary Intervention. Rev. Bras. Cardiol. Invasiva 2014, 22, 240–244. [Google Scholar] [CrossRef] [Green Version]
- Zampieri, F.G.; Ranzani, O.T.; Sabatoski, V.; de Souza, H.P.; Barbeiro, H.; da Neto, L.M.C.; Park, M.; da Silva, F.P. An increase in mean platelet volume after admission is associated with higher mortality in critically ill patients. Ann. Intensiv. Care 2014, 4, 20. [Google Scholar] [CrossRef] [PubMed]
- Bommenahalli Gowda, S.; Gosavi, S.; Ananda Rao, A.; Shastry, S.; Raj, S.C.; Menon, S.; Suresh, A.; Sharma, A. Prognosis of COVID-19: Red Cell Distribution Width, Platelet Distribution Width, and C-Reactive Protein. Cureus 2021, 13, e13078. [Google Scholar] [CrossRef] [PubMed]
- Accinelli, R.A.; Leon-Abarca, J.A. At High Altitude COVID-19 Is Less Frequent: The Experience of Peru. Arch. Bronconeumol. 2020, 56, 760–761. [Google Scholar] [CrossRef] [PubMed]
- Zubieta-Calleja, G.; Merino-Luna, A.; Zubieta-DeUrioste, N.; Armijo-Subieta, N.F.; Soliz, J.; Arias-Reyes, C.; Escalante-Kanashiro, R.; Carmona-Suazo, J.A.; López-Bascope, A.; Calle-Aracena, J.M.; et al. Re: “Mortality Attributed to COVID-19 in High-Altitude Populations” by Woolcott and Bergman. High Alt. Med. Biol. 2021, 22, 102–104. [Google Scholar] [CrossRef] [PubMed]
- Ballaz, S.J.; Pulgar-Sánchez, M.; Chamorro, K.; Fernández-Moreira, E.; Ramírez, H.; Mora, F.X.; Fors, M. Common laboratory tests as indicators of COVID-19 severity on admission at high altitude: A single-center retrospective study in Quito (ECUADOR). Clin. Chem. Lab. Med. 2021, 59, e326–e329. [Google Scholar] [CrossRef]
- Woolcott, O.O.; Bergman, R.N. Mortality Attributed to COVID-19 in High-Altitude Populations. High Alt. Med. Biol. 2020, 21, 409–416. [Google Scholar] [CrossRef] [PubMed]
- Yue, H.; Bai, X.; Wang, J.; Yu, Q.; Liu, W.; Pu, J.; Wang, X.; Hu, J.; Xu, D.; Li, X.; et al. Clinical characteristics of coronavirus disease 2019 in Gansu province, China. Ann. Palliat. Med. 2020, 9, 1404–1412. [Google Scholar] [CrossRef]
- Prokop, M.; Van Everdingen, W.; van Rees Vellinga, T.; Quarles van Ufford, H.; Stöger, L.; Beenen, L.; Geurts, B.; Gietema, H.; Krdzalic, J.; Schaefer-Prokop, C.; et al. CO-RADS–A categorical CT assessment scheme for patients with suspected COVID-19: Definition and evaluation. Radiology 2020, 296, E97–E104. [Google Scholar] [CrossRef]
- COVID-19 Clinical Management: Living Guidance. Available online: https://www.who.int/publications-detail-redirect/WHO-2019-nCoV-clinical-2021-1 (accessed on 18 November 2021).
- Xiong, S.; Liu, L.; Lin, F.; Shi, J.; Han, L.; Liu, H.; He, L.; Jiang, Q.; Wang, Z.; Fu, W.; et al. Clinical characteristics of 116 hospitalized patients with COVID-19 in Wuhan, China: A single-centered, retrospective, observational study. BMC Infect. Dis. 2020, 20, 787. [Google Scholar] [CrossRef] [PubMed]
- Şan, İ.; Gemcioğlu, E.; Davutoğlu, M.; Çatalbaş, R.; Karabuğa, B.; Kaptan, E.; Erden, A.; Küçükşahin, O.; Ateş, İ.; Karaahmetoğlu, S.; et al. Which hematological markers have predictive value as early indicators of severe COVID-19 cases in the emergency department? Turk. J. Med. Sci. 2021, 51, 2810–2821. [Google Scholar] [CrossRef] [PubMed]
- Lanini, S.; Montaldo, C.; Nicastri, E.; Vairo, F.; Agrati, C.; Petrosillo, N.; Scognamiglio, P.; Antinori, A.; Puro, V.; Di Caro, A.; et al. COVID-19 disease-Temporal analyses of complete blood count parameters over course of illness, and relationship to patient demographics and management outcomes in survivors and non-survivors: A longitudinal descriptive cohort study. PLoS ONE 2020, 15, e0244129. [Google Scholar] [CrossRef] [PubMed]
- Ouyang, S.M.; Zhu, H.Q.; Xie, Y.N.; Zou, Z.S.; Zuo, H.M.; Rao, Y.W.; Liu, X.Y.; Zhong, B.; Chen, X. Temporal changes in laboratory markers of survivors and non-survivors of adult inpatients with COVID-19. BMC Infect. Dis. 2020, 20, 952. [Google Scholar] [CrossRef]
- Wang, H.; Xing, Y.; Yao, X.; Li, Y.; Huang, J.; Tang, J.; Zhu, S.; Zhang, Y.; Xiao, J. Retrospective Study of Clinical Features of COVID-19 in Inpatients and Their Association with Disease Severity. Med. Sci. Monit. Int. Med. J. Exp. Clin. Res. 2020, 26, e927674. [Google Scholar] [CrossRef]
- Tian, S.; Zhu, X.; Sun, X.; Wang, J.; Zhou, Q.; Wang, C.; Chen, L.; Li, S.; Xu, J. A Prognostic Model to Predict Recovery of COVID-19 Patients Based on Longitudinal Laboratory Findings. Virol. Sin. 2020, 35, 811–819. [Google Scholar] [CrossRef]
- Lin, S.; Mao, W.; Zou, Q.; Lu, S.; Zheng, S. Associations between hematological parameters and disease severity in patients with SARS-CoV-2 infection. J. Clin. Lab. Anal. 2021, 35, e23604. [Google Scholar] [CrossRef]
- Mertoglu, C.; Huyut, M.T.; Arslan, Y.; Ceylan, Y.; Coban, T.A. How do routine laboratory tests change in coronavirus disease 2019? Scand. J. Clin. Lab. Investig. 2021, 81, 24–33. [Google Scholar] [CrossRef]
- Han, Y.; Zhang, H.; Mu, S.; Wei, W.; Jin, C.; Tong, C.; Song, Z.; Zha, Y.; Xue, Y.; Gu, G. Lactate dehydrogenase, an independent risk factor of severe COVID-19 patients: A retrospective and observational study. Aging 2020, 12, 11245–11258. [Google Scholar] [CrossRef]
- Xu, P.P.; Tian, R.H.; Luo, S.; Zu, Z.Y.; Fan, B.; Wang, X.M.; Xu, K.; Wang, J.T.; Zhu, J.; Shi, J.C.; et al. Risk factors for adverse clinical outcomes with COVID-19 in China: A multicenter, retrospective, observational study. Theranostics 2020, 10, 6372–6383. [Google Scholar] [CrossRef]
- Joyce, K.E.; Weaver, S.R.; Lucas, S.J.E. Geographic components of SARS-CoV-2 expansion: A hypothesis. J. Appl. Physiol. 2020, 129, 257–262. [Google Scholar] [CrossRef] [PubMed]
- Seclén, S.N.; Nunez-Robles, E.; Yovera-Aldana, M.; Arias-Chumpitaz, A. Incidence of COVID-19 infection and prevalence of diabetes, obesity, and hypertension according to altitude in Peruvian population. Diabetes Res. Clin. Pract. 2020, 169, 108463. [Google Scholar] [PubMed]
- COVID-19 en el Perú-Ministerio del Salud. Available online: https://covid19.minsa.gob.pe/sala_situacional.asp (accessed on 7 November 2021).
- Yildiz, H.; Castanares-Zapatero, D.; Pierman, G.; Pothen, L.; De Greef, J.; Nana, F.A. Validation of Neutrophil-to-Lymphocyte Ratio Cut-off Value Associated with High In-Hospital Mortality in COVID-19 Patients. Int. J. Gen. Med. 2021, 14, 5111–5117. [Google Scholar] [CrossRef] [PubMed]
- Knight, S.R.; Ho, A.; Pius, R.; Buchan, I.; Carson, G.; Drake, T.M.; Dunning, J.; Fairfield, C.J.; Gamble, C.; Green, C.A.; et al. Risk stratification of patients admitted to hospital with covid-19 using the ISARIC WHO Clinical Characterization Protocol: Development and validation of the 4C Mortality Score. BMJ 2020, 370, m3339. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | n (Missing Values) | n = 64 |
|---|---|---|
| Demographics | ||
| Gender | 0 | |
| Female | 33 (51.6%) | |
| Male | 31 (48.4%) | |
| Age (years) | 0 | 48.5 (39–64.5) * |
| Duration of disease (days) | 0 | 7 (6−7) * |
| Body mass index | 3 | |
| Normal | 9 (14.8%) | |
| Overweight | 30 (49.2%) | |
| Obesity | 22 (36.1%) | |
| Comorbidities | ||
| Diabetes | 0 | 2 (3.1%) |
| Arterial hypertension | 0 | 5 (7.8%) |
| Chronic pulmonary disease | 0 | 4 (6.3) |
| Signs and symptoms on admission | ||
| Heart rate (beats/min) | 0 | 82.6 (± 14.10) |
| Oxygen saturation (%) | 0 | 90.3 (± 3.63) |
| Fever t > 38.3 °C | 1 | 45 (71%) |
| Dyspnea | 1 | 42 (67%) |
| Chest pain | 1 | 46 (73%) |
| Headache | 1 | 39 (62%) |
| Cough | 1 | 38 (60%) |
| Odynophagia | 1 | 23 (37%) |
| Diarrhea | 1 | 19 (30%) |
| Rhinorrhea | 1 | 24 (38%) |
| Admission Laboratory | ||
| Hemoglobin (g/dL) | 0 | 16.25 (15.31–17.45) * |
| WBC count (109/L) | 0 | 6.73 (5.25–8.98) * |
| Lymphocytes (109/L) | 0 | 1.32 (0.82–2.10) * |
| Platelets (109/L) | 0 | 225 (175–271) * |
| Mean platelet volume (fL) | 1 | 9.63 (± 0.84) |
| Lactate dehydrogenase (IU/L) | 3 | 477 (404–566) * |
| Creatinine (mg/dl) | 1 | 0.84 (0.75–1.05) * |
| AST (U/L) | 2 | 43 (29–59.5) * |
| ALT (U/L) | 1 | 60.6 (35–90) * |
| Bilirubin T (mg/dL) | 10 | 0.6 (4–9) * |
| Alkaline Phosphatase (IU/L) | 13 | 231 (190–344) * |
| Prothrombin time (sec) | 9 | 13.76 (± 1.1) |
| Arterial oxygen pressure | 4 | 65.2 (58.45–74) * |
| PaO2/FiO2 | 4 | 276.5 (257–296.5) * |
| Images | ||
| CT scan (phase) | 11 | 53 |
| Progressive | 32 (60%) | |
| Consolidative | 11 (21%) | |
| Normal | 10(19%) | |
| % Compromised | 30% (8 Y 40) | |
| % Ground glass | 20.64 +/− 16.87 | |
| Variables | Non-Severe n 47 (73.4%) | Severe n 17 (26.6%) | p Value | Statistical Test |
|---|---|---|---|---|
| Gender | 0.003 | X2 test | ||
| Female | 28 (84.8%) | 5 (15.2%) | ||
| Male | 19 (61.3%) | 12 (38.7%) | ||
| Age (years) | 44 (36–65) | 55 (47–63) | 0.04 | Mann–Whitney–U test |
| Time of disease (days) | 7 (5–7) | 7 (6–7) | 0.99 | Mann–Whitney–U test |
| Body mass index | 0.48 | Fisher’s exact test | ||
| Normal | 6 (66.7%) | 3 (33.3%) | ||
| Overweight | 23 (69.7%) | 10 (30.3%) | ||
| Obesity | 16 (84.2%) | 3 (15.8%) | ||
| Signs and symptoms on admission | ||||
| Heart rate (beats/min) | 80.5 (+/−14.2) | 88.3 (+/−12.7) | 0.05 | Student’s t-test |
| Oxygen saturation (%) | 90.6 (+/−3.81) | 89.5 (+/−3.04) | 0.32 | Student’s t-test |
| Fever t > 38.3 °C | 32 (71.1%) | 13 (28.9%) | 0.78 | Fisher’s exact test |
| Dyspnea | 30 (71.4%) | 12 (28.8%) | 0.68 | X2 test |
| Chest pain | 34 (73.9%) | 12 (26.1%) | 0.76 | Fisher’s exact test |
| Headache | 32 (82.1%) | 7 (18%) | 0.04 | X2 test |
| Cough | 26 (68.4%) | 12 (31.6%) | 0.31 | X2 test |
| Odynophagia | 18 (78.3%) | 5 (21.7%) | 0.48 | X2 test |
| Diarrhea | 14 (73.7%) | 5 (26.3%) | 0.94 | X2 test |
| Rhinorrhea | 18 (75%) | 6 (25%) | 0.78 | X2 test |
| Admission Laboratory | ||||
| Hemoglobin (g/dL) | 16 (14.9–17.3) | 16.8 (16.2–17.6) | 0.16 | Mann–Whitney–U test |
| WBC count (109/L) | 6.52 (5.2–9) | 7.67 (5.6–8.7) | 0.65 | Mann–Whitney–U test |
| Lymphocytes (109/L) | 1.48 (0.9–2.2) | 1.10 (0.8–1.4) | 0.07 | Mann–Whitney–U test |
| Platelets (109/L) | 235 (169–299) | 212 (182–228) | 0.34 | Mann–Whitney–U test |
| Mean platelet volume (fL) | 9.5 (+/–0.81) | 10 (+/–0.85) | 0.02 | Student’s t-test |
| Lactate dehydrogenase (IU/L) | 472 (390–561) | 491 (423–569) | 0.79 | Mann–Whitney–U test |
| Creatinine (mg/dL) | 0.83 (0.75–1.01) | 0.93 (0.8–1.05) | 0.39 | Mann–Whitney–U test |
| AST (U/L) | 41 (27–55) | 56 (43–77) | 0.02 | Mann–Whitney–U test |
| ALT (U/L) | 58 (31–90) | 65 (58–85) | 0.33 | Mann–Whitney–U test |
| Bilirubin T (mg/dL) | 0.6 (0.5–0.9) | 0.65 (0.4–0.8) | 0.70 | Mann–Whitney–U test |
| Alkaline Phosphatase (IU/L) | 241 (198–344) | 212.5 (185–309) | 0.57 | Mann–Whitney–U test |
| Prothrombin time | 13.69 (±1.50) | 14.08 (±0.86) | 0.43 | Student’s t-test |
| Arterial oxygen pressure | 67.8 (59.4–77) | 60.2 (56.5–65.4) | 0.11 | Mann–Whitney–U test |
| PaO2/FiO2 | 283 (260–304) | 269 (252–278) | 0.15 | Mann–Whitney–U test |
| Images | ||||
| CT scan (phase) | 0.09 | Fisher’s exact test | ||
| Progressive | 21 (65.6%) | 11 (34.4%) | ||
| Consolidative | 7 (63.6%) | 4 (36.4%) | ||
| Normal | 10 (100%) | 0 (0%) | ||
| % Compromised | 22.7 (+/−18.6) | 41.9 (+/−17.1) | 0.001 | Student’s t-test |
| % Ground glass | 16.6 (+/−15.3) | 30.9 (+/−16.9) | 0.004 | Student’s t-test |
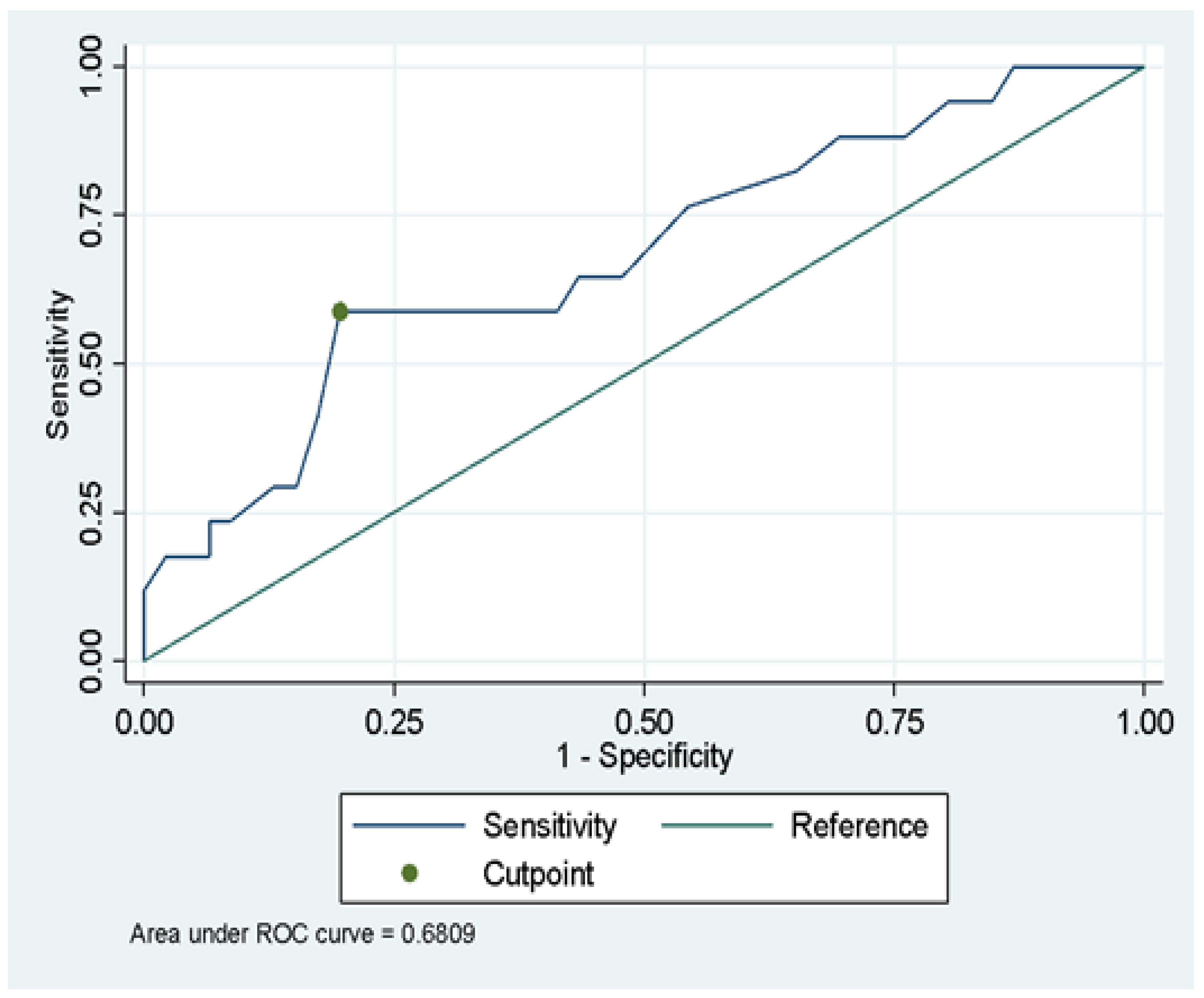
| Variable | AUC (IC95%) | Cut-Off Point | Youden Index | Sensitivity | Specificity | AUC | LR+ | LR− | PPV | NPV |
|---|---|---|---|---|---|---|---|---|---|---|
| MPV | 0.68(0.53–0.84) | 10.15 | 0.39 | 0.59 | 0.80 | 0.70 | 2.95 | 0.51 | 0.53 | 0.84 |
| Variables | Bivariate Analysis | Multiple Regression Analysis * | ||||
|---|---|---|---|---|---|---|
| RR | 95% CI | p | RR | 95% CI | p | |
| Gender | ||||||
| Female | Ref. | |||||
| Male | 2.55 | 1.01–6.46 | 0.048 | 2.7 | 1.07–6.79 | 0.035 |
| Age | ||||||
| Age in years | 1.02 | 1.00–1.05 | 0.024 | 1.03 | 1.01–1.06 | 0.009 |
| Mean platelet volume | ||||||
| <10.15 | Ref. | |||||
| ≥10.15 | 3.31 | 1.47–7.43 | 0.004 | 2.93 | 1.38–6.23 | 0.005 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Quispe-Pari, J.F.; Gonzales-Zamora, J.A.; Munive-Dionisio, J.; Castro-Contreras, C.; Villar-Astete, A.; Kong-Paravicino, C.; Vilcapoma-Balbin, P.; Hurtado-Alegre, J. Mean Platelet Volume as a Predictor of COVID-19 Severity: A Prospective Cohort Study in the Highlands of Peru. Diseases 2022, 10, 22. https://doi.org/10.3390/diseases10020022
Quispe-Pari JF, Gonzales-Zamora JA, Munive-Dionisio J, Castro-Contreras C, Villar-Astete A, Kong-Paravicino C, Vilcapoma-Balbin P, Hurtado-Alegre J. Mean Platelet Volume as a Predictor of COVID-19 Severity: A Prospective Cohort Study in the Highlands of Peru. Diseases. 2022; 10(2):22. https://doi.org/10.3390/diseases10020022
Chicago/Turabian StyleQuispe-Pari, Jhosef Franck, Jose Armando Gonzales-Zamora, Judith Munive-Dionisio, Cristhian Castro-Contreras, Abelardo Villar-Astete, Cesar Kong-Paravicino, Pierina Vilcapoma-Balbin, and Jorge Hurtado-Alegre. 2022. "Mean Platelet Volume as a Predictor of COVID-19 Severity: A Prospective Cohort Study in the Highlands of Peru" Diseases 10, no. 2: 22. https://doi.org/10.3390/diseases10020022