

PCA-Based Preprocessing for Clustering-Based Fetal Heart Rate Extraction in Non-Invasive Fetal Electrocardiograms

 , , , and
, , , and 
Abstract
:1. Introduction
2. Background
2.1. NI-fECG Fundamentals
2.2. Processing of NI-fECG
2.2.1. Wavelet Denoising
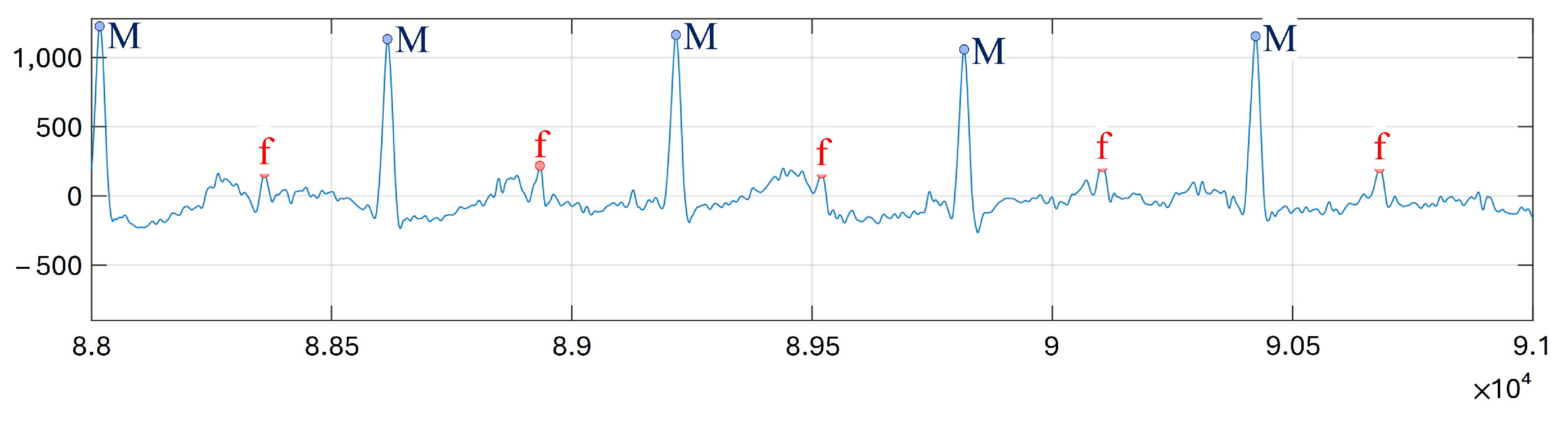
2.2.2. Clustering-Based Procedure for FHR Extraction
- Case 1: detection of two local maxima from the first local minimum, which represents candidates that are actually noise. Each of these maxima provides information about the amplitude zones corresponding to fetal RS-peaks and maternal RS-peaks. If the distance between these maxima is 35% greater than the maximum candidate amplitude, maternal candidates are larger than fetal ones and amplitudes are the selected data to be classified.
- Case 2: detection of two local maxima from the first local minimum, the distance between which is 35% less than the maximum candidate amplitude. This situation can be related to similar amplitudes for fetal and maternal RS-peaks and, thus, amplitudes multiplied by the number of samples of the candidates are the data to be classified.
- Case 3: detection of a single local maximum from the first local minimum. This situation generally corresponds again to similar amplitudes for fetal and maternal RS-peaks, and amplitudes multiplied by the number of samples of the candidates are the selected data to be classified.
2.2.3. Blind Source Separation Fundamentals
2.2.4. Principal Component Analysis (PCA)
3. Proposed Framework
3.1. Fetal ECG Datasets
- Abdominal and Direct Fetal Electrocardiogram Database (ADFECGDB) [50]: this database contains multichannel fECG recordings obtained from five different women in labor. Each recording comprises four 5 min differential signals acquired from the maternal abdomen, and the reference direct fECG registered from the fetus head. The recordings are sampled at 1 ksps with 16-bit resolution, and the signal bandwidth is 1–150 Hz. Moreover, the database includes a set of reference annotations indicating the fetal R-wave locations. The ADFECGDB will be used to train the proposed algorithm.
- Challenge 2013 Training Set A (Challenge) [53]: these data consist of one-minute fECG recordings, sampled at 1 ksps, each one including four noninvasive abdominal signals as well as the reference annotations marking fetal R-wave locations [14]. The Challenge database is used to test and validate the proposed algorithm.
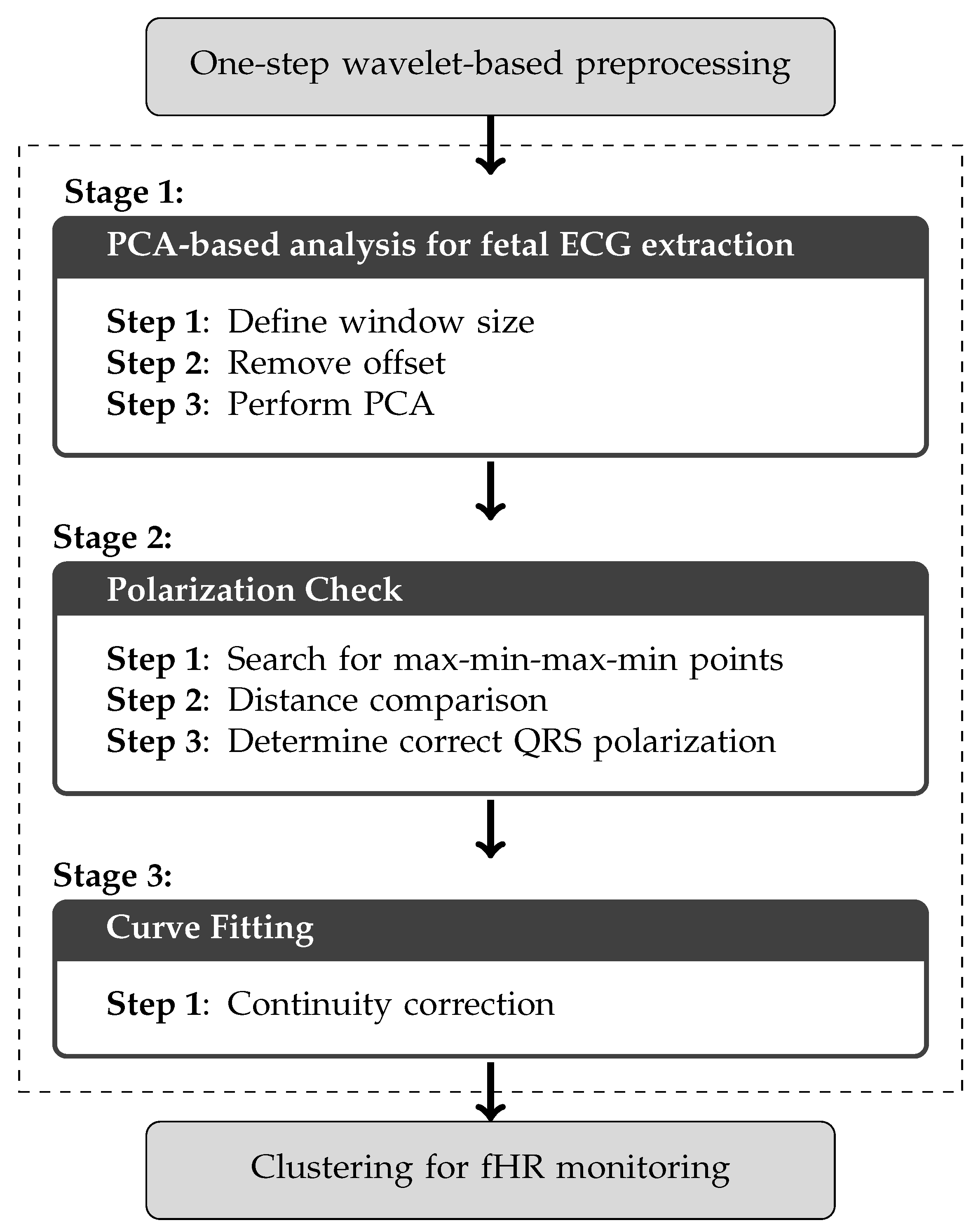
3.2. Proposed PCA-Based Framework
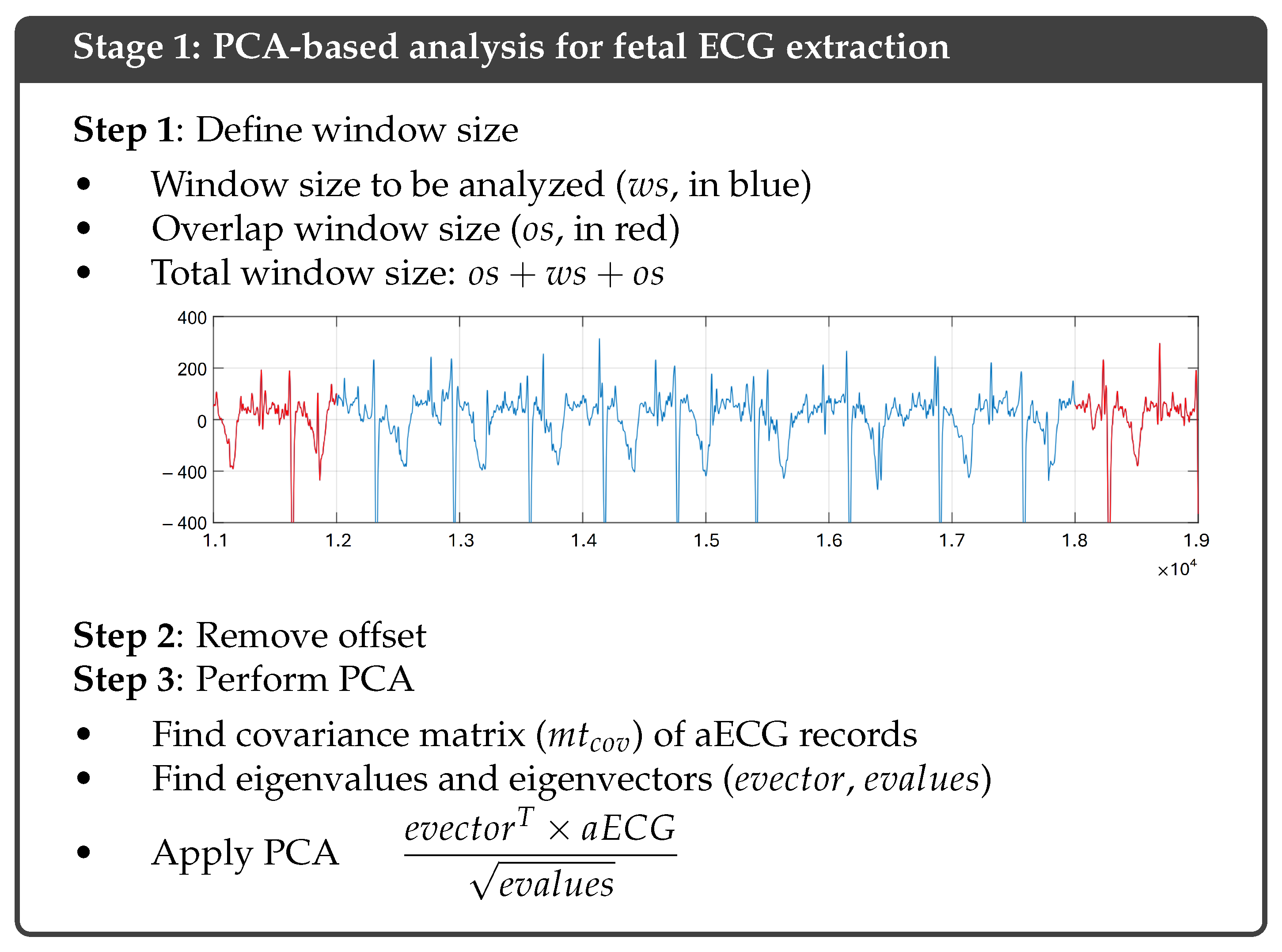
3.3. Stage 1: PCA-Based Analysis for Fetal ECG Extraction
| Algorithm 1 PCA-based analysis for fetal ECG extraction. |
|
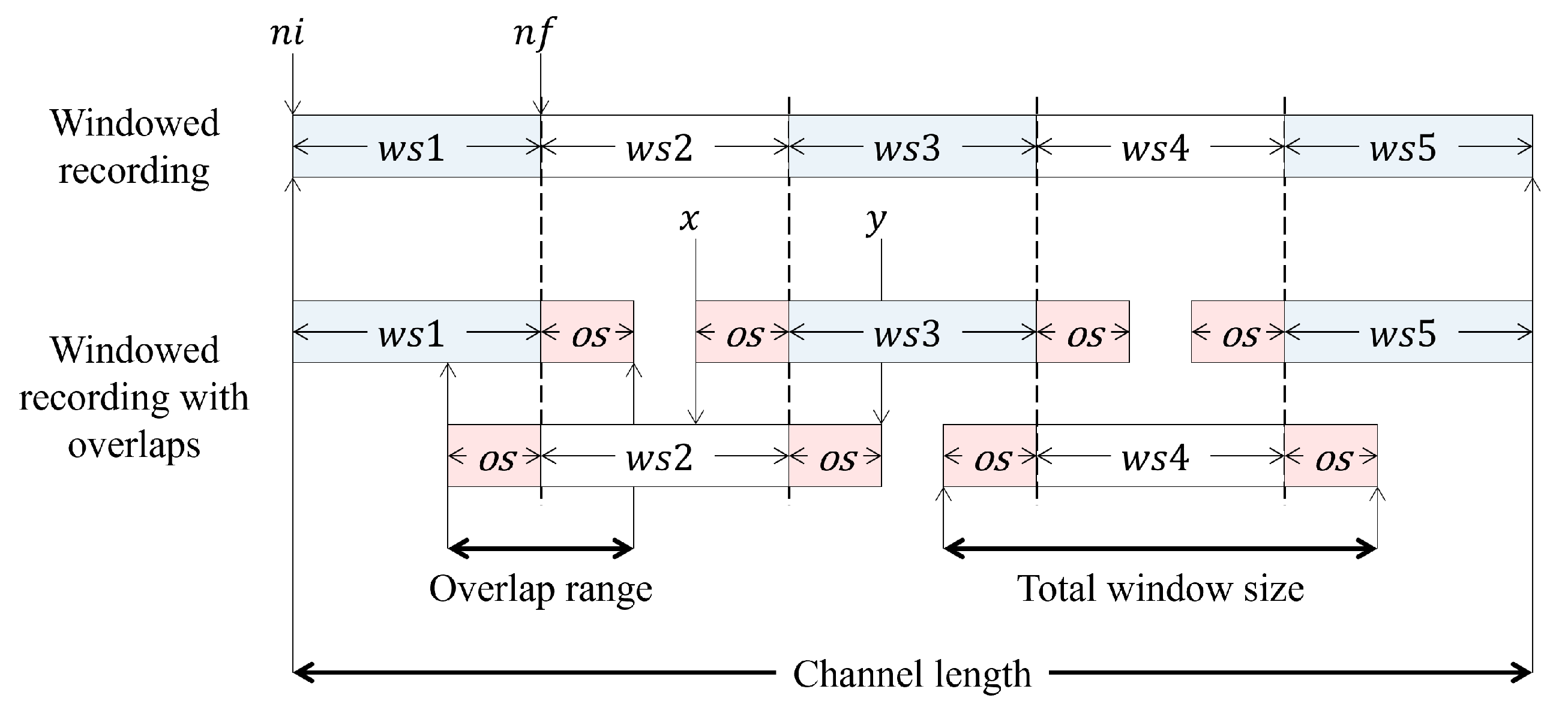
3.3.1. Step 1: Define Window Size
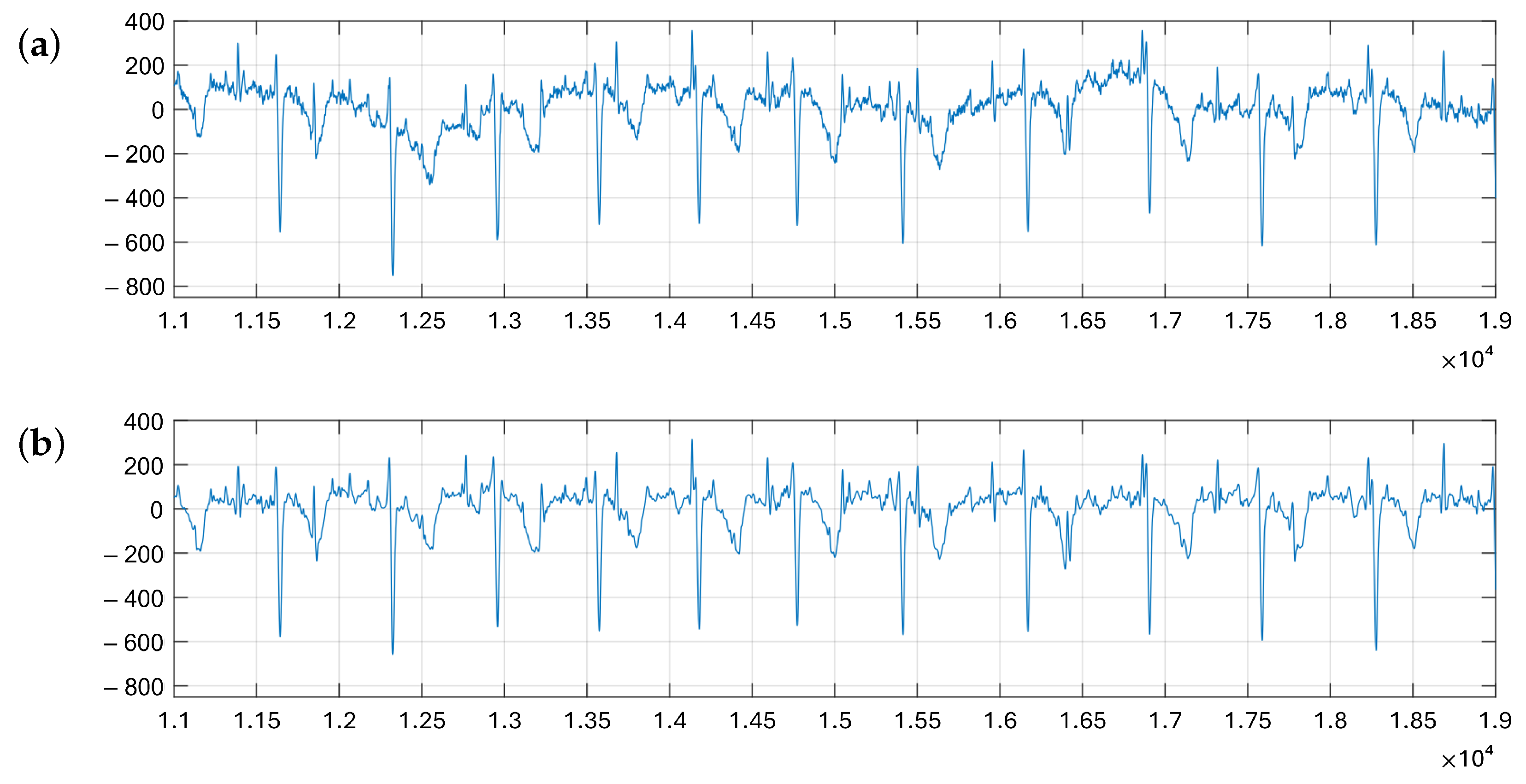
3.3.2. Step 2: Remove Offset
3.3.3. Step 3: Perform PCA
3.4. Stage 2: Polarization Check
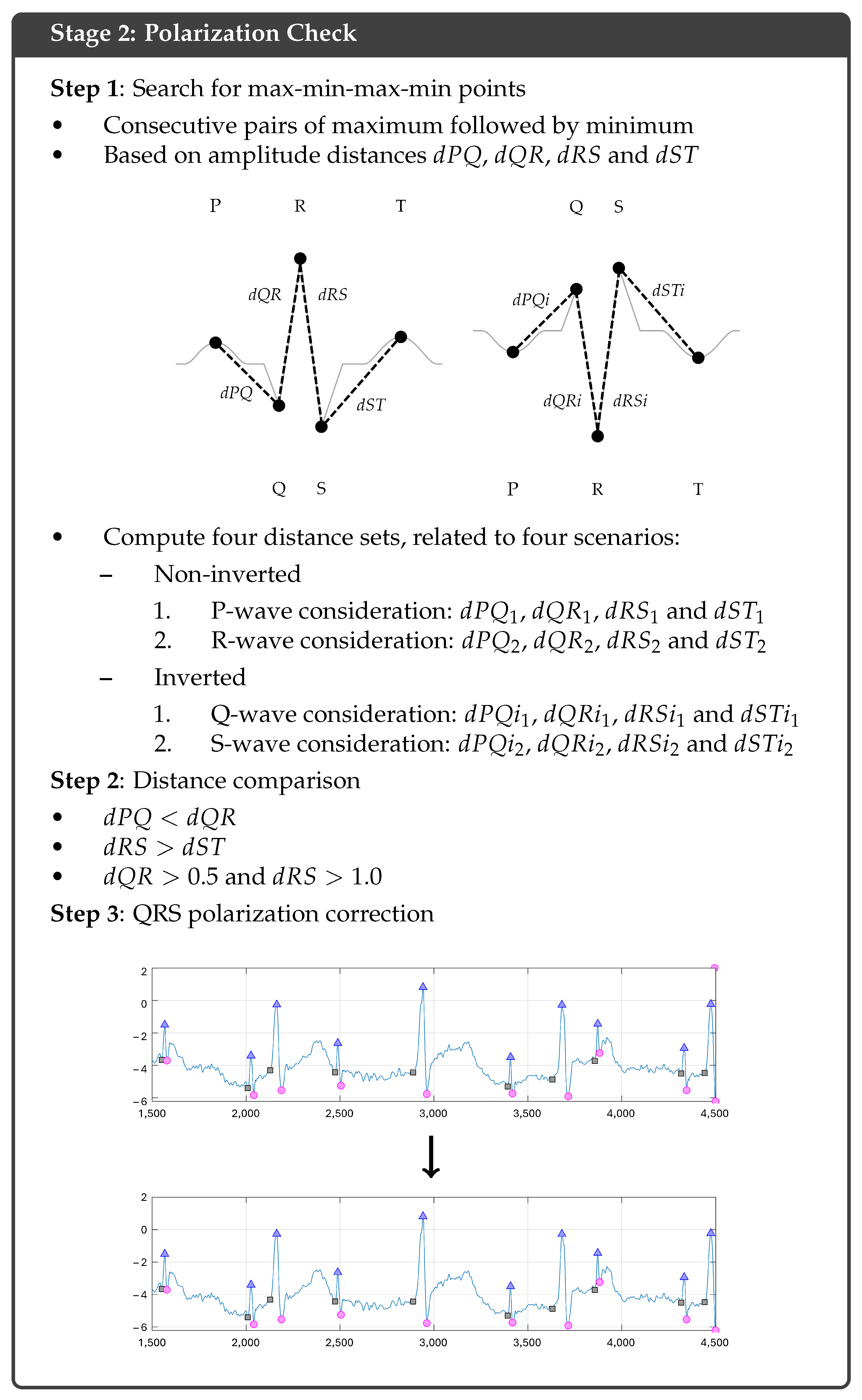
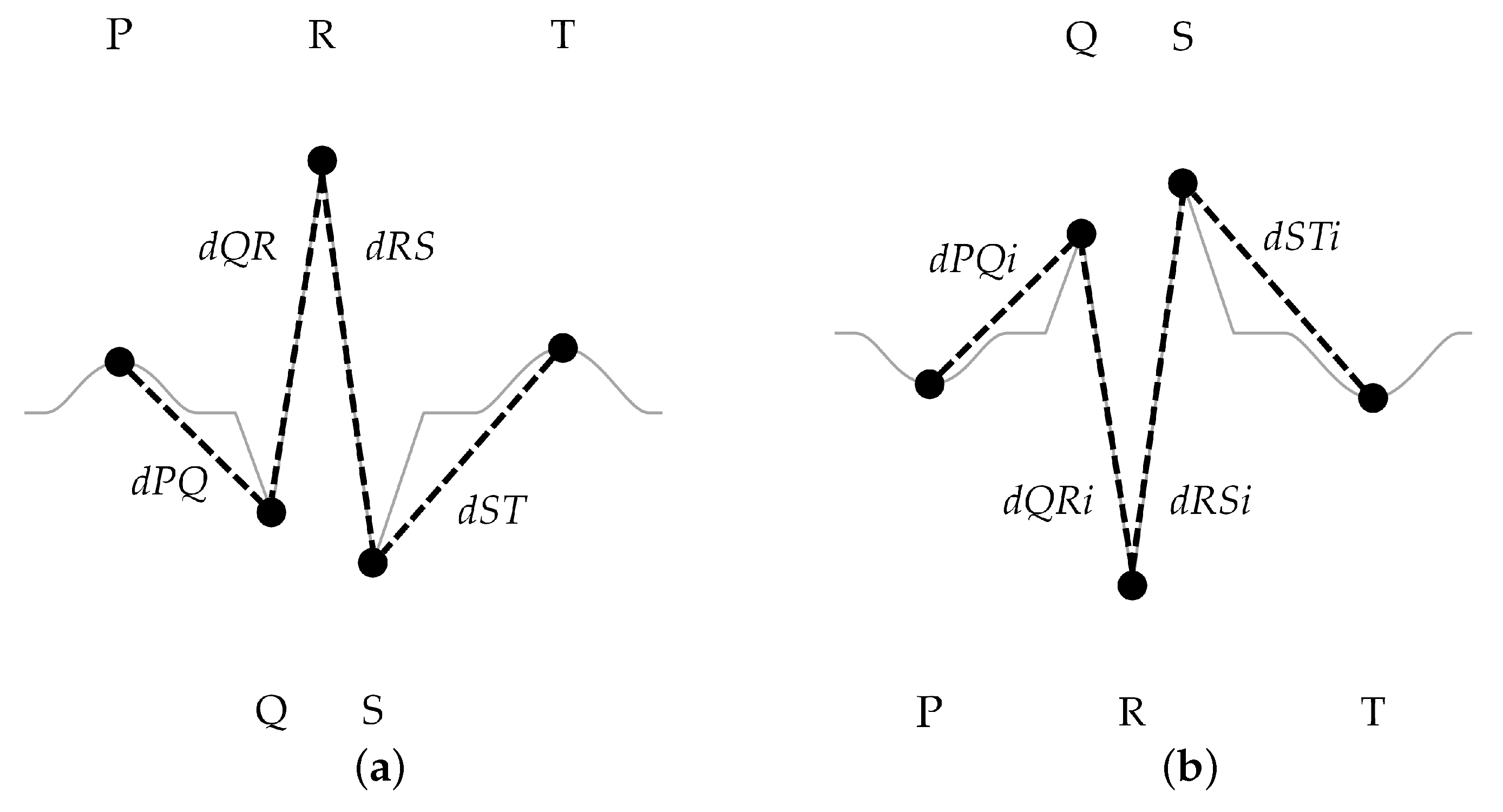
3.4.1. Step 1: Search for Max-Min-Max-Min Points
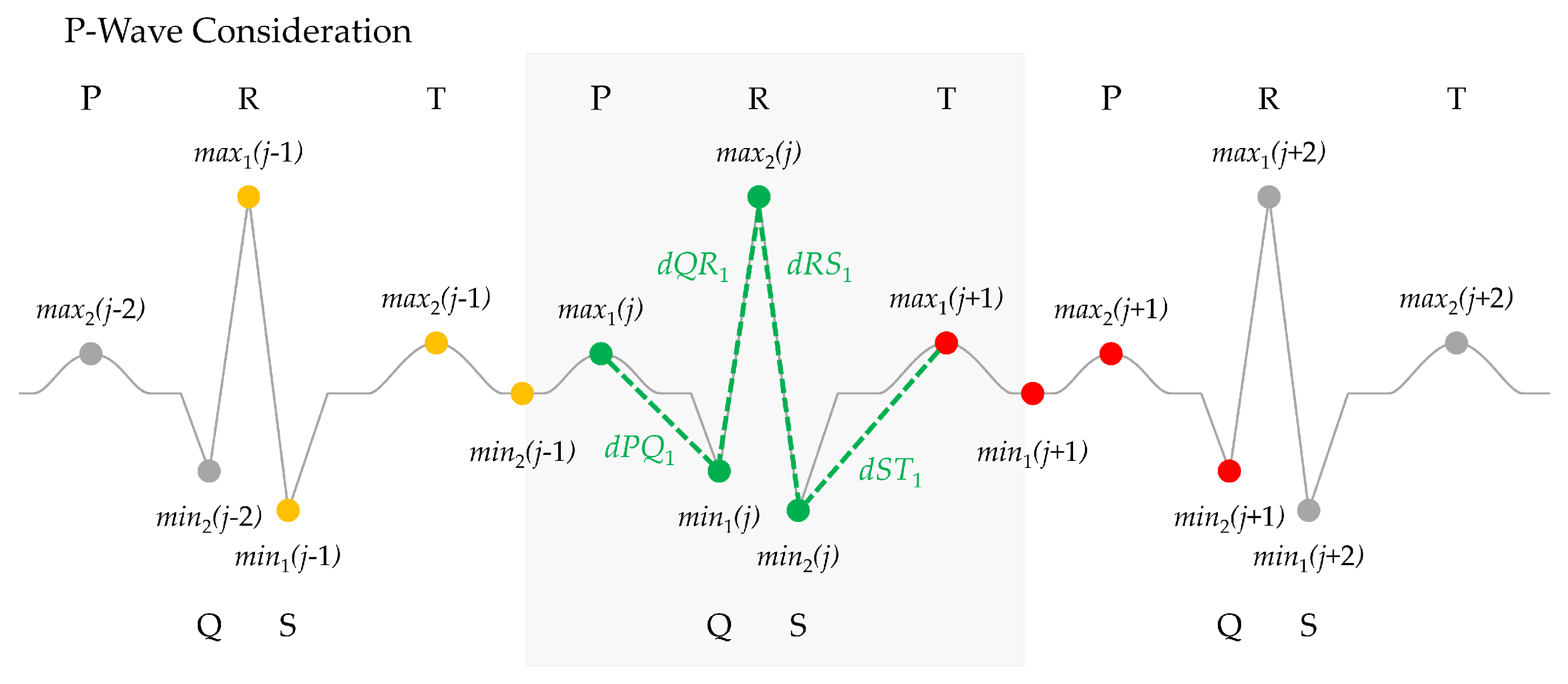
- In the first scenario, it is considered that the first maximum found is the P-wave, located at , where j is the index of the pair of maximum–minimum being evaluated, as shown in Figure 10. Thus, the next values to be found are the Q wave, located at , the R wave at , and the S wave, located at , while the T wave corresponds to the first maximum of the next group, . These allow us to define and analyze the distances , , , and as shown in Figure 10.
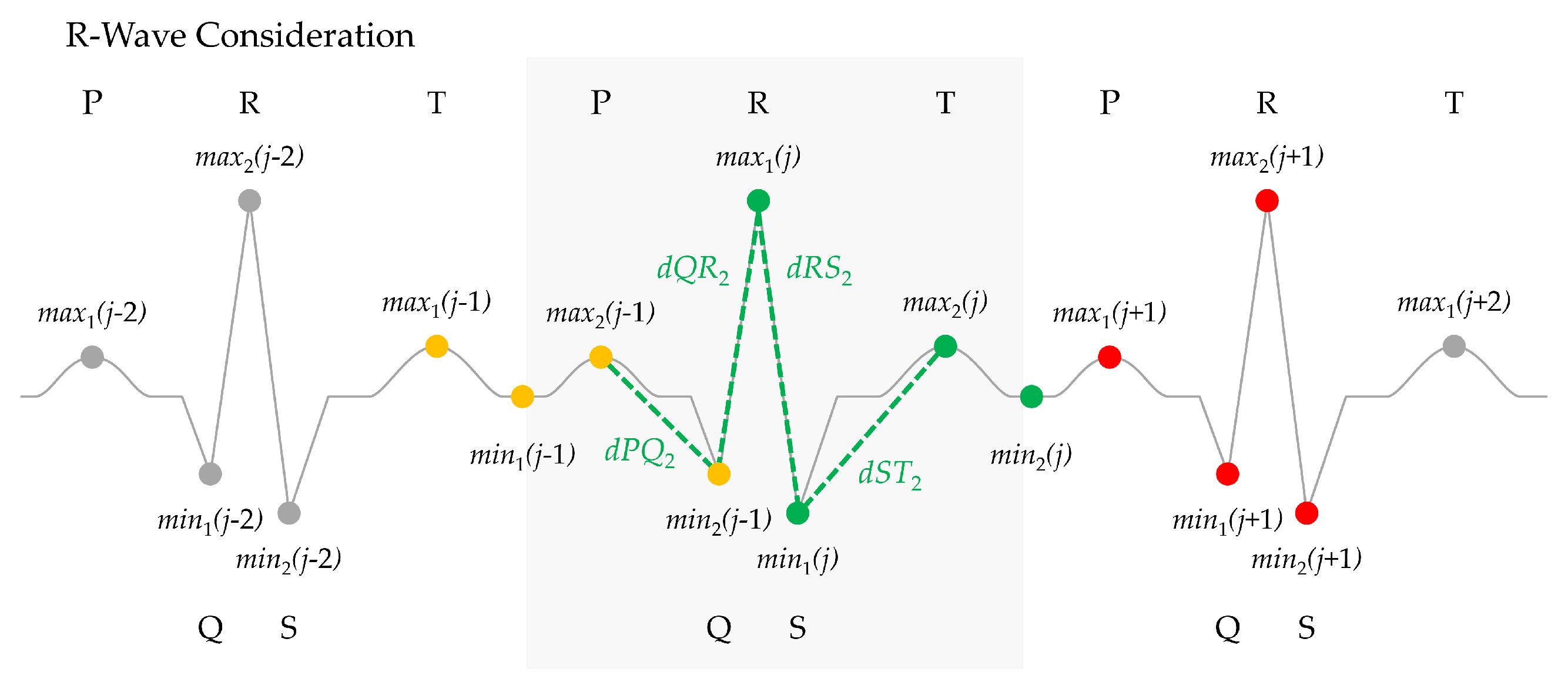
- In a second scenario, it is considered that corresponds to a R-wave, as shown in Figure 11. Thus, the set of distances , , , and can be computed as illustrated in Figure 11 using the points , which should correspond to the previous P wave, , corresponding to the Q wave, , which should match the S wave, and finally as the T wave.
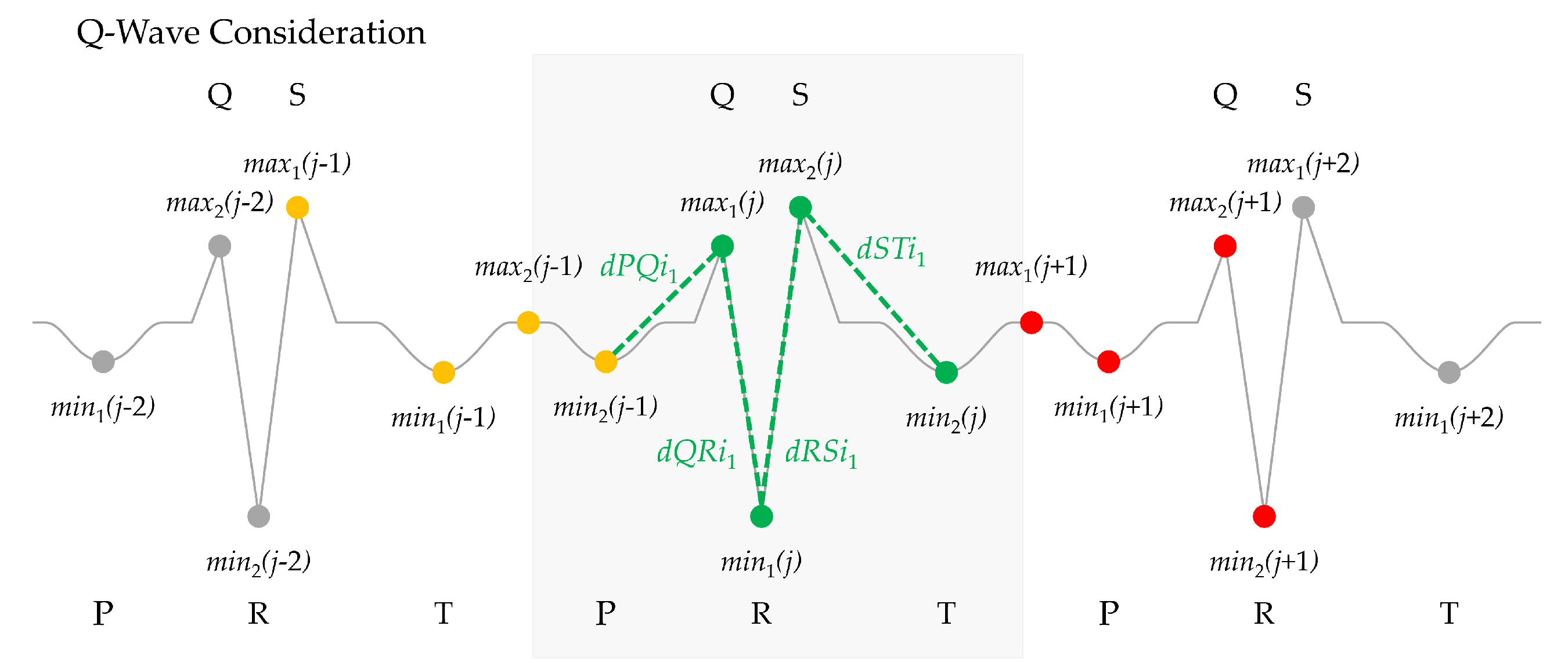
- In the case the polarity is inverted, a third scenario is possible where it is considered that the first maximum found is the Q wave at , as shown in Figure 12, where it is illustrated how the distances , , , and are obtained using the points , , , and .
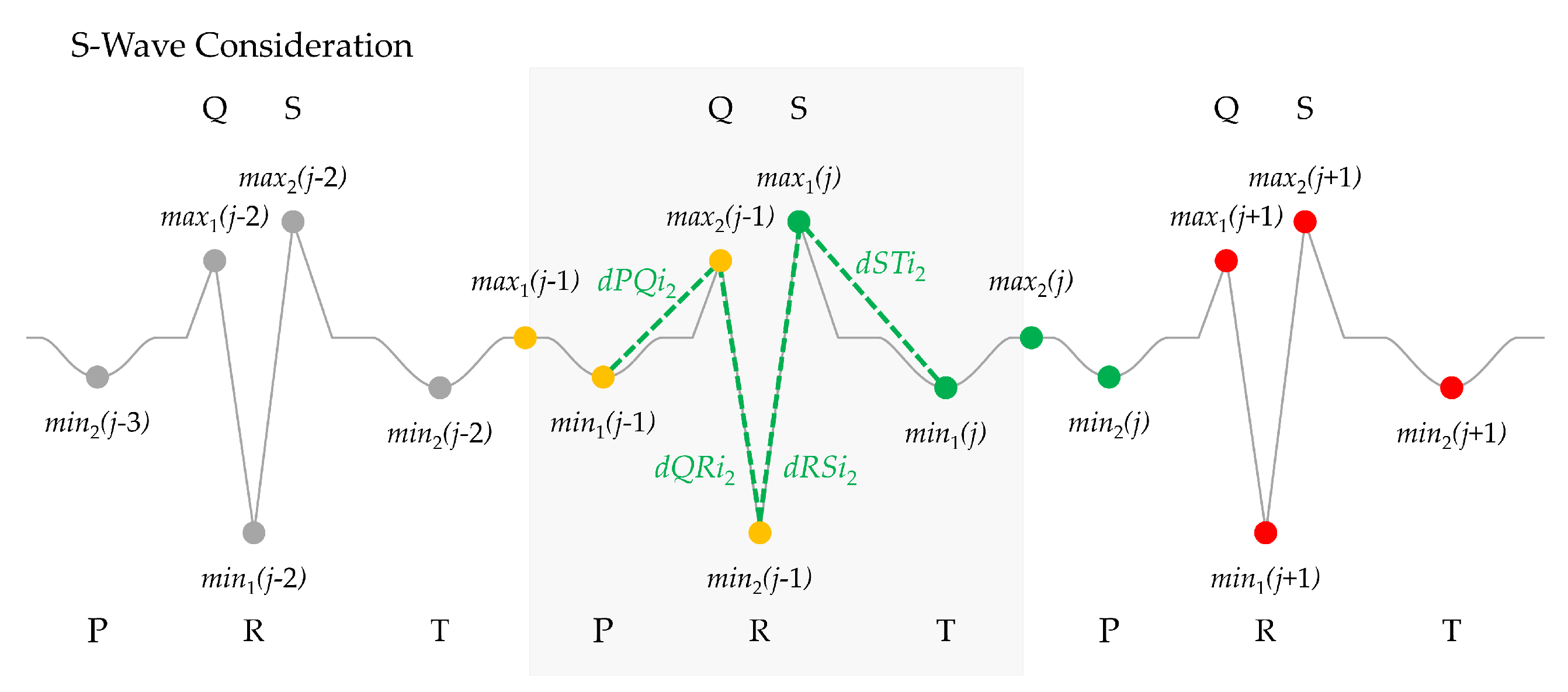
- Finally, when the polarity is inverted, a final scenario is defined in Figure 13, so corresponds to the S wave and the set of distances , , , and are computed using , , , and .
| Algorithm 2 Polarization check, step 1. |
|
3.4.2. Step 2: Distance Comparison
| Algorithm 3 Polarization check, step 2. |
|
3.4.3. Step 3: QRS Polarization Correction
| Algorithm 4 Polarization check, step 3. |
|
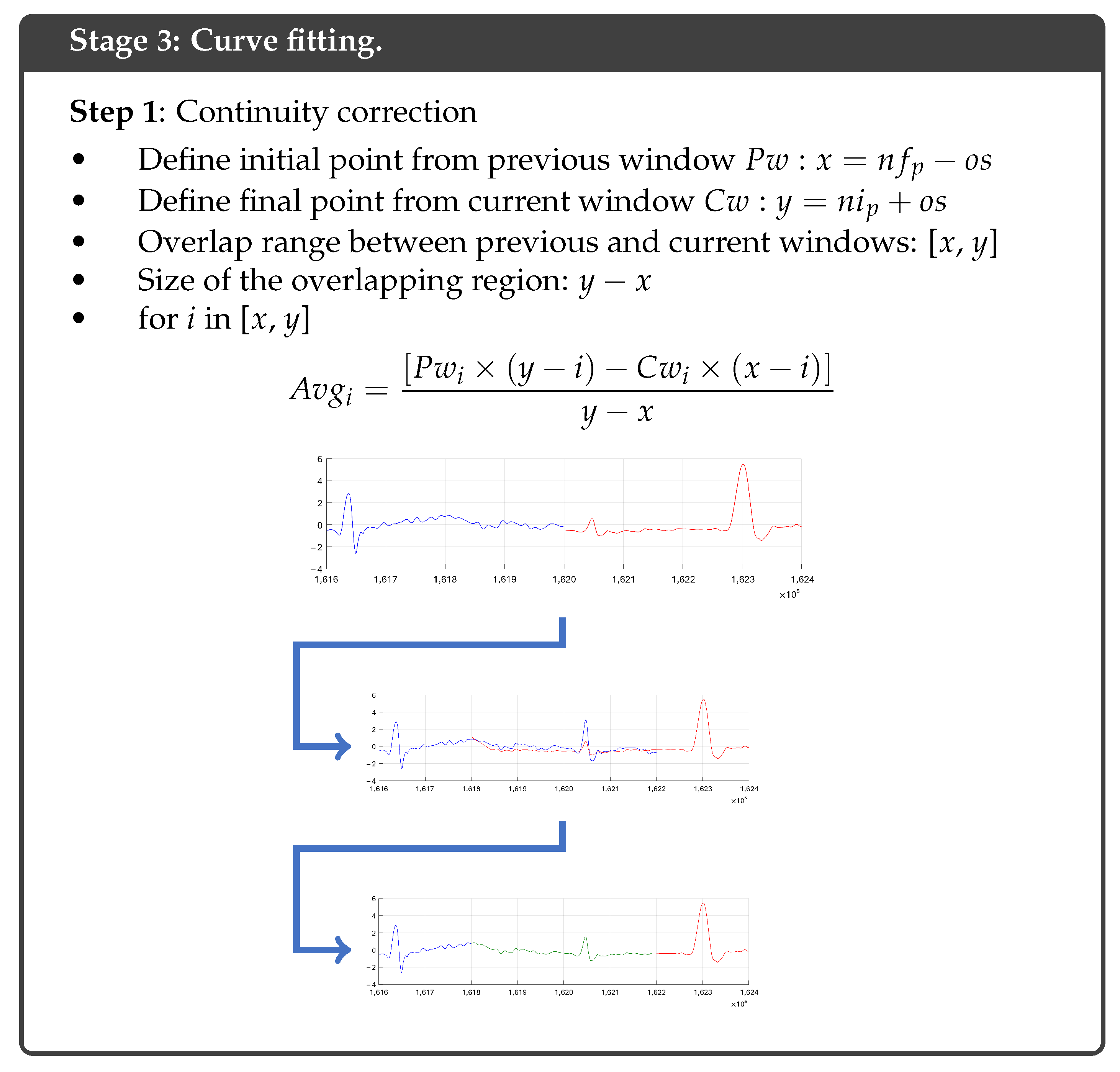
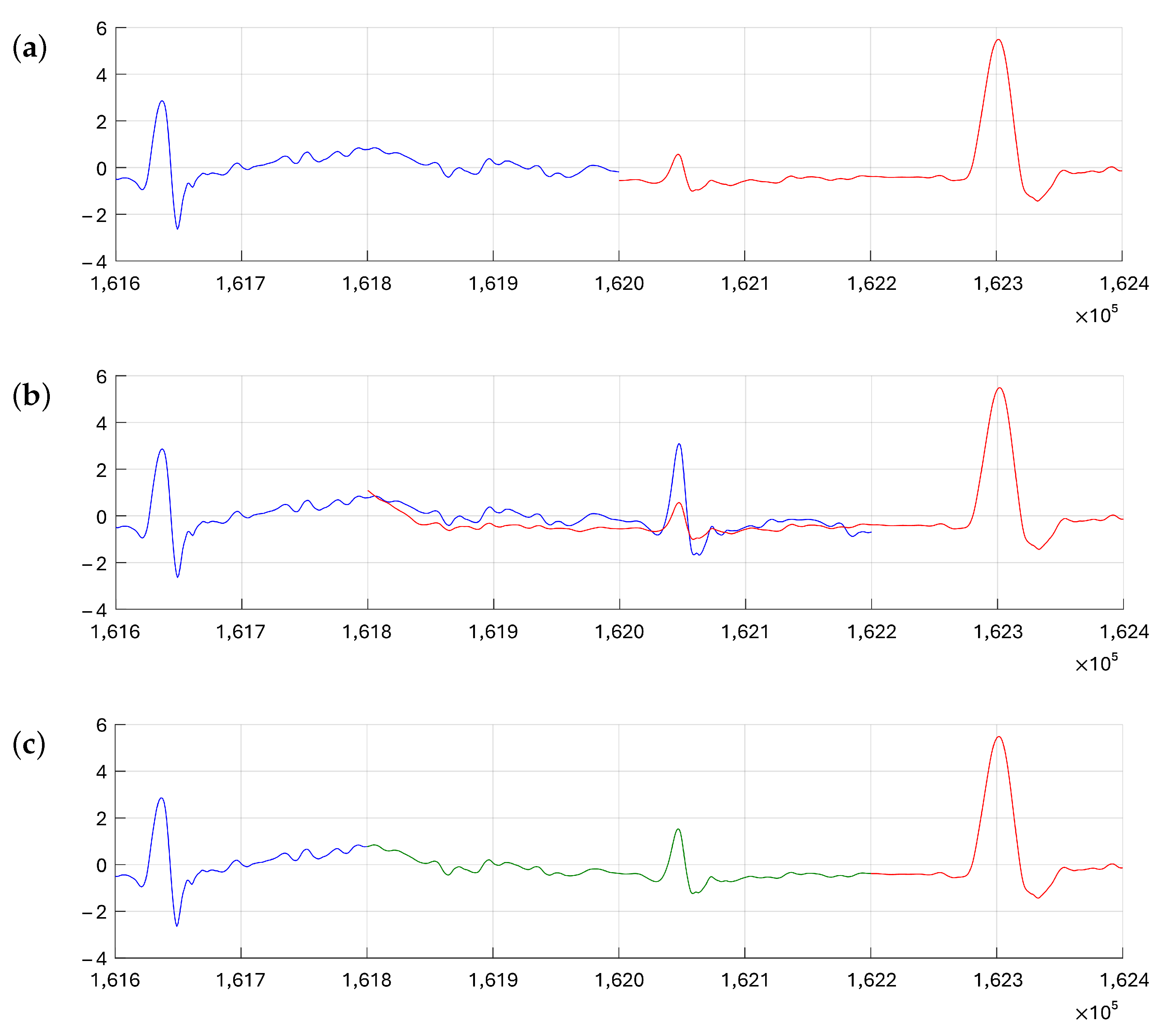
3.5. Stage 3: Curve Fitting
| Algorithm 5 Curve fitting. |
|
4. Validation and Results
4.1. Performance Metrics
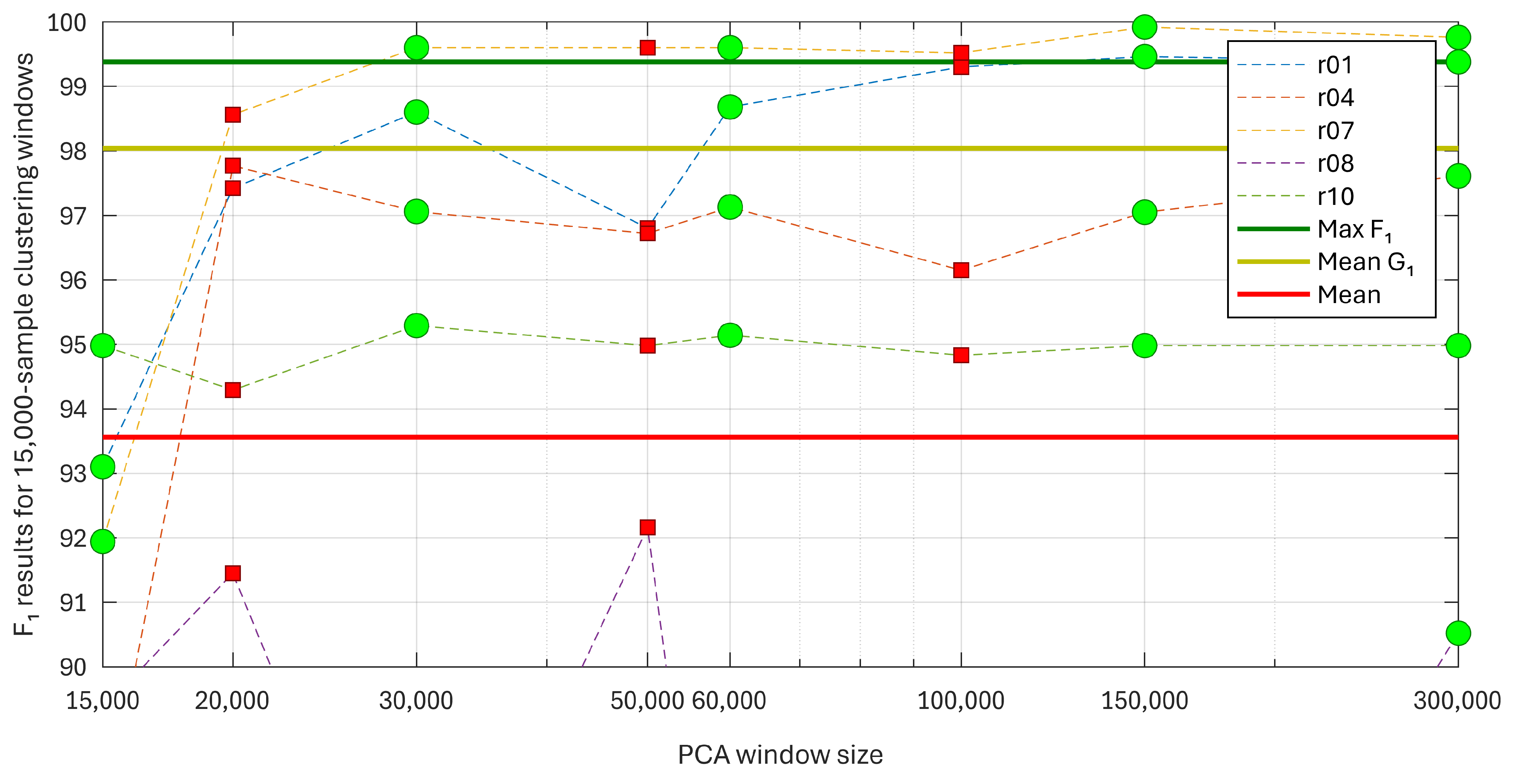
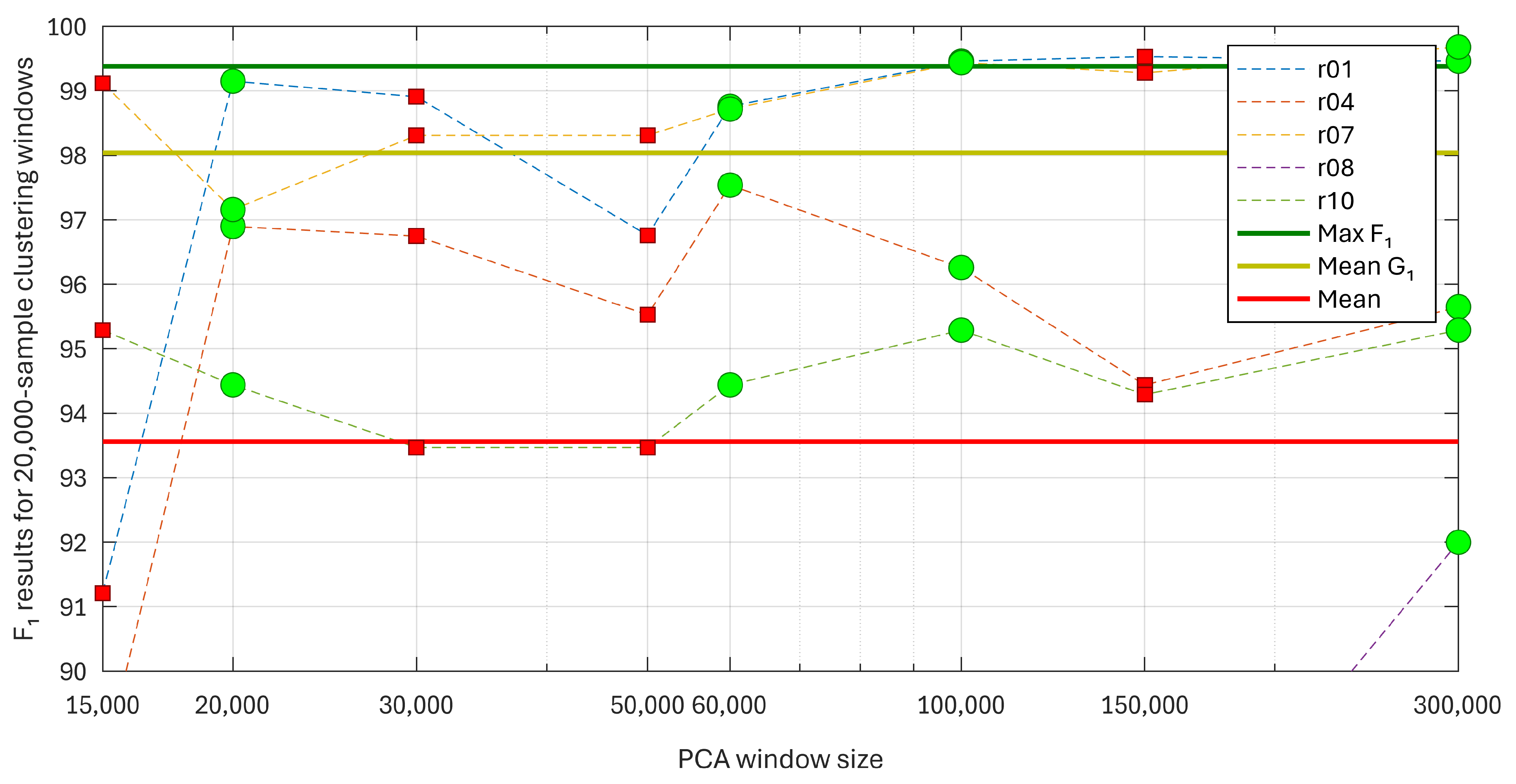
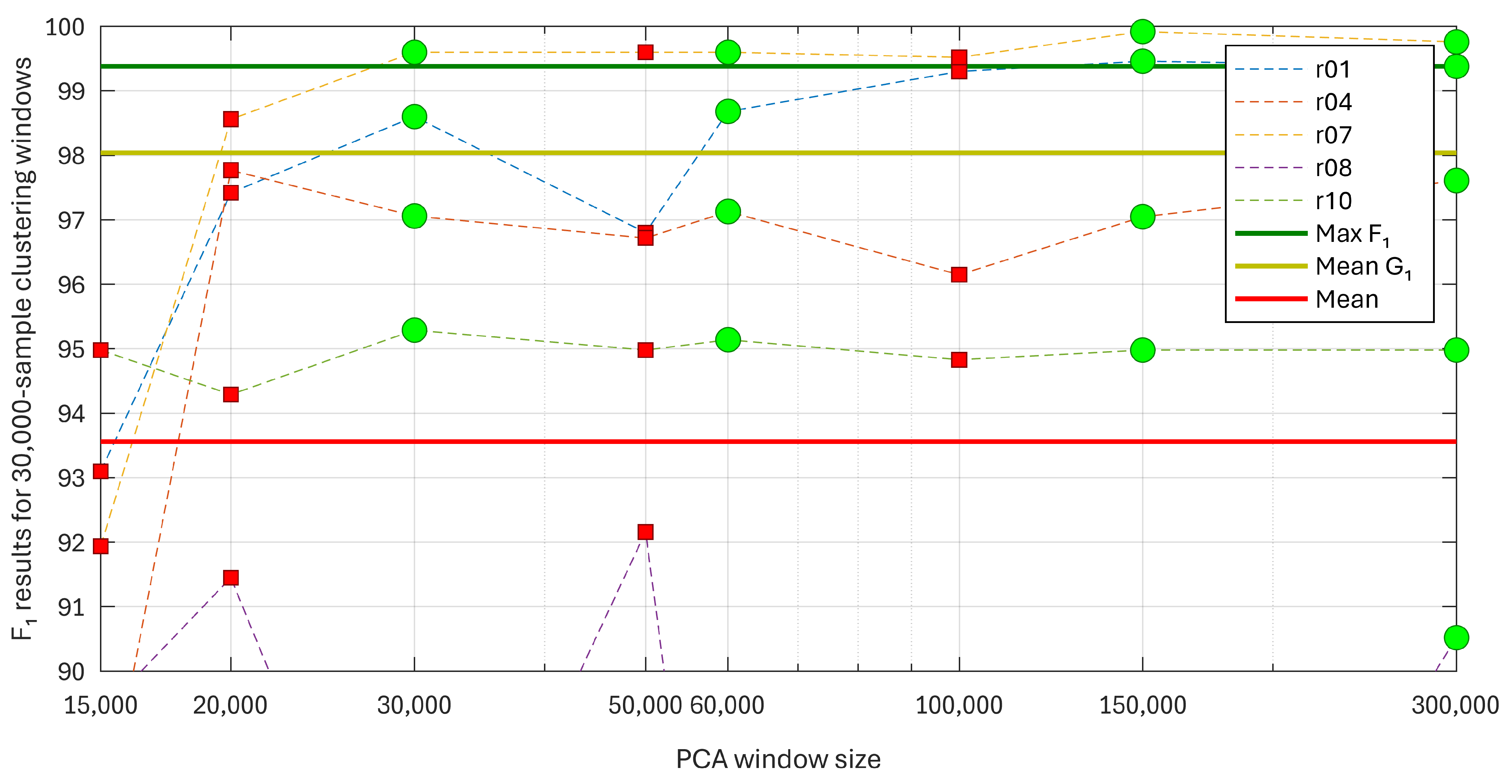
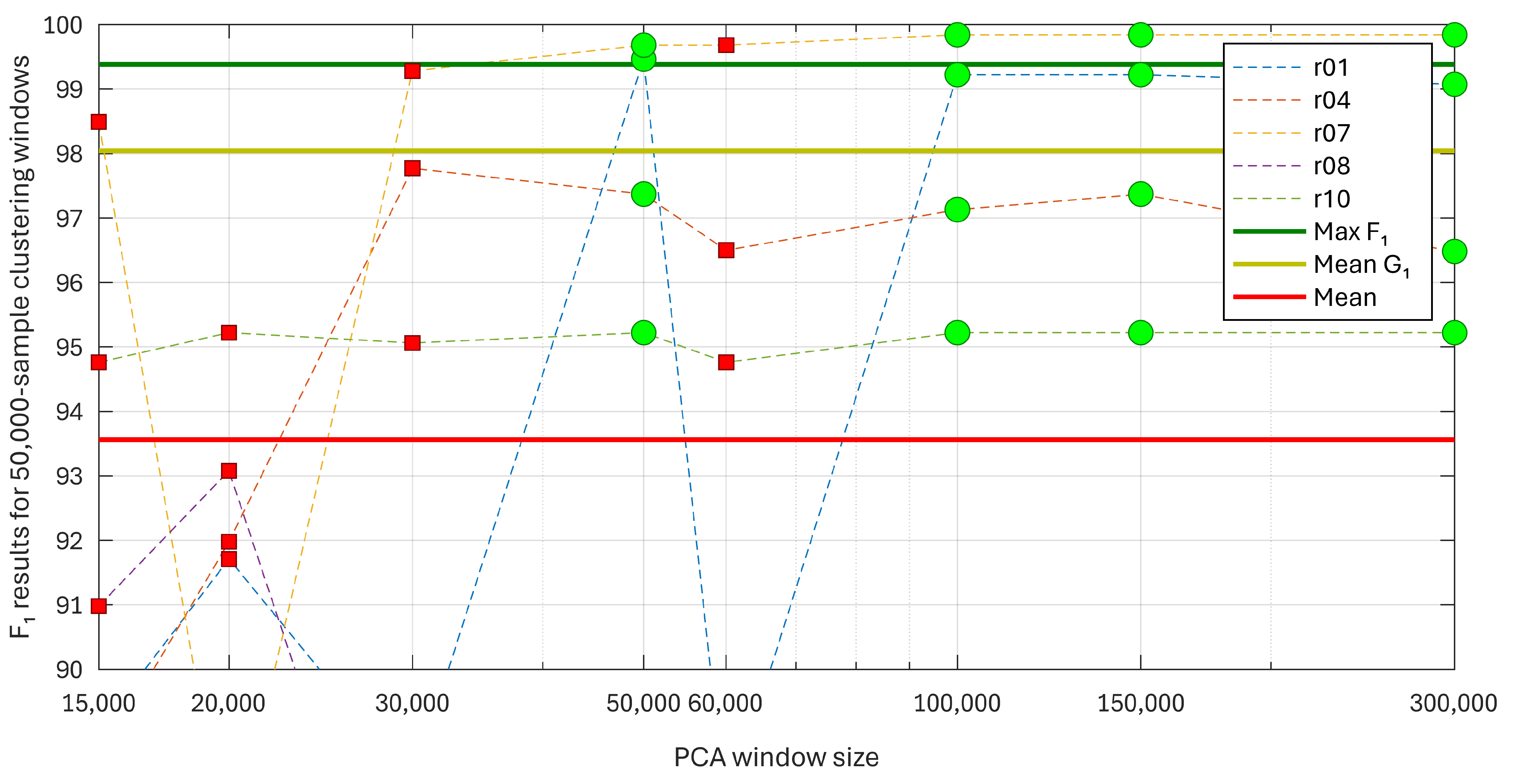
4.2. Training
4.3. Testing and Validation
5. Conclusions
Author Contributions
Funding
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Jaros, R.; Martinek, R.; Kahankova, R. Non-Adaptive Methods for Fetal ECG Signal Processing: A Review and Appraisal. Sensors 2018, 18, 3648. [Google Scholar] [CrossRef] [PubMed]
- Kahankova, R.; Martinek, R.; Jaros, R.; Behbehani, K.; Matonia, A.; Jezewski, M.; Behar, J.A. A Review of Signal Processing Techniques for Non-Invasive Fetal Electrocardiography. IEEE Rev. Biomed. Eng. 2020, 13, 51–73. [Google Scholar] [CrossRef] [PubMed]
- Blix, E.; Maude, R.; Hals, E.; Kisa, S.; Karlsen, E.; Nohr, E.A.; Jonge, A.d.; Lindgren, H.; Downe, S.; Reinar, L.M.; et al. Intermittent auscultation fetal monitoring during labour: A systematic scoping review to identify methods, effects, and accuracy. PLoS ONE 2019, 14, e0219573. [Google Scholar] [CrossRef] [PubMed]
- Cunningham, F.G.; Leveno, K.J.; Bloom, S.L.; Dashe, J.S.; Hoffman, B.L.; Casey, B.M.; Spong, C.Y. Intrapartum Assessment. In Williams Obstetrics, 26th ed.; McGraw-Hill Education: New York, NY, USA, 2022. [Google Scholar]
- Vintzileos, A.M.; Nochimson, D.J.; Guzman, E.R.; Knuppel, R.A.; Lake, M.; Schifrin, B.S. Intrapartum electronic fetal heart rate monitoring versus intermittent auscultation: A meta-analysis. Obstet. Gynecol. 1995, 85, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Ibrahim, E.A.; Al Awar, S.; Balayah, Z.H.; Hadjileontiadis, L.J.; Khandoker, A.H. A Comparative Study on Fetal Heart Rates Estimated from Fetal Phonography and Cardiotocography. Front. Physiol. 2017, 8, 764. [Google Scholar] [CrossRef] [PubMed]
- Martinek, R.; Kahankova, R.; Jaros, R.; Barnova, K.; Matonia, A.; Jezewski, M.; Czabanski, R.; Horoba, K.; Jezewski, J. Non-Invasive Fetal Electrocardiogram Extraction Based on Novel Hybrid Method for Intrapartum ST Segment Analysis. IEEE Access 2021, 9, 28608–28631. [Google Scholar] [CrossRef]
- Zeng, R.; Lu, Y.; Long, S.; Wang, C.; Bai, J. Cardiotocography signal abnormality classification using time-frequency features and Ensemble Cost-sensitive SVM classifier. Comput. Biol. Med. 2021, 130, 104218. [Google Scholar] [CrossRef] [PubMed]
- Vintzileos, A.M.; Antsaklis, A.; Varvarigos, I.; Papas, C.; Sofatzis, I.; Montgomery, J.T. A randomized trial of intrapartum electronic fetal heart rate monitoring versus intermittent auscultation. Obstet. Gynecol. 1993, 81, 899–907. [Google Scholar]
- Caliskan, E.; Cakiroglu, Y.; Corakci, A.; Ozeren, S. Reduction in caesarean delivery with fetal heart rate monitoring and intermittent pulse oximetry after induction of labour with misoprostol. J. Matern.-Fetal Neonatal Med. 2009, 22, 445–451. [Google Scholar] [CrossRef]
- Cohen, W.R.; Ommani, S.; Hassan, S.; Mirza, F.G.; Solomon, M.; Brown, R.; Schifrin, B.S.; Himsworth, J.M.; Hayes-Gill, B.R. Accuracy and reliability of fetal heart rate monitoring using maternal abdominal surface electrodes. Acta Obstet. Gynecol. Scand. 2012, 91, 1306–1313. [Google Scholar] [CrossRef]
- Liu, B.; Thilaganathan, B.; Bhide, A. Effectiveness of ambulatory non-invasive fetal electrocardiography: Impact of maternal and fetal characteristics. Acta Obstet. Gynecol. Scand. 2023, 102, 577–584. [Google Scholar] [CrossRef] [PubMed]
- Pardey, J.; Moulden, M.; Redman, C.W. A computer system for the numerical analysis of nonstress test. Am. J. Obstet. Gynecol. 2002, 186, 1095–1103. [Google Scholar] [CrossRef] [PubMed]
- Castillo, E.; Morales, D.P.; García, A.; Parrilla, L.; Ruiz, V.U.; Álvarez Bermejo, J.A. A clustering-based method for single-channel fetal heart rate monitoring. PLoS ONE 2018, 13, e0199308. [Google Scholar] [CrossRef] [PubMed]
- Mujumdar, R.; Nadar, P.; Bondre, A.P.; Kulkarni, A.; Pathak, S. Principal Component Analysis (PCA) Based Single-Channel, Non-Invasive Fetal ECG Extraction; CareNX Innovations Pvt. Ltd.: Maharashtra, India, 2019. [Google Scholar]
- Castillo, E.; Morales, D.P.; García, A.; Martínez-Martí, F.; Parrilla, L.; Palma, A.J. Noise Suppression in ECG Signals through Efficient One-Step Wavelet Processing Techniques. J. Appl. Math. 2013, 2013, e763903. [Google Scholar] [CrossRef]
- Lisenbee, N.; Tyndall, J.A. Fetal Heart Rate Monitoring. In Atlas of Emergency Medicine Procedures; Ganti, L., Ed.; Springer: New York, NY, USA, 2016; pp. 639–642. [Google Scholar] [CrossRef]
- Bin Queyam, A.; Kumar Pahuja, S.; Singh, D. Quantification of Feto-Maternal Heart Rate from Abdominal ECG Signal Using Empirical Mode Decomposition for Heart Rate Variability Analysis. Technologies 2017, 5, 68. [Google Scholar] [CrossRef]
- Barnova, K.; Martinek, R.; Jaros, R.; Kahankova, R. Hybrid Methods Based on Empirical Mode Decomposition for Non-Invasive Fetal Heart Rate Monitoring. IEEE Access 2020, 8, 51200–51218. [Google Scholar] [CrossRef]
- Apsana, S.; Suresh, M.G.; Aneesh, R.P. A novel algorithm for early detection of fetal arrhythmia using ICA. In Proceedings of the 2017 International Conference on Intelligent Computing, Instrumentation and Control Technologies (ICICICT), Kerala, India, 6–7 July 2017; pp. 1277–1283. [Google Scholar] [CrossRef]
- Abramowicz, J.S.; Barnett, S.B.; Duck, F.A.; Edmonds, P.D.; Hynynen, K.H.; Ziskin, M.C. Fetal Thermal Effects of Diagnostic Ultrasound. J. Ultrasound Med. 2008, 27, 541–559. [Google Scholar] [CrossRef]
- Castillo, E.; Morales, D.P.; Botella, G.; García, A.; Parrilla, L.; Palma, A.J. Efficient wavelet-based ECG processing for single-lead FHR extraction. Digit. Signal Process. 2013, 23, 1897–1909. [Google Scholar] [CrossRef]
- Martinek, R.; Kahankova, R.; Jezewski, J.; Jaros, R.; Mohylova, J.; Fajkus, M.; Nedoma, J.; Janku, P.; Nazeran, H. Comparative Effectiveness of ICA and PCA in Extraction of Fetal ECG From Abdominal Signals: Toward Non-invasive Fetal Monitoring. Front. Physiol. 2018, 9, 338138. [Google Scholar] [CrossRef]
- Behar, J.; Johnson, A.; Clifford, G.D.; Oster, J. A Comparison of Single Channel Fetal ECG Extraction Methods. Ann. Biomed. Eng. 2014, 42, 1340–1353. [Google Scholar] [CrossRef]
- Panigrahy, D.; Sahu, P.K. Extraction of fetal ECG signal by an improved method using extended Kalman smoother framework from single channel abdominal ECG signal. Australas. Phys. Eng. Sci. Med. 2017, 40, 191–207. [Google Scholar] [CrossRef] [PubMed]
- He, P.J.; Chen, X.M.; Liang, Y.; Zeng, H.Z. Extraction for fetal ECG using single channel blind source separation algorithm based on multi-algorithm fusion. MATEC Web Conf. 2016, 44, 01026. [Google Scholar] [CrossRef]
- Rahmati, A.; Setarehdan, S.; Araabi, B. A PCA/ICA based Fetal ECG Extraction from Mother Abdominal Recordings by Means of a Novel Data-driven Approach to Fetal ECG Quality Assessment. J. Biomed. Phys. Eng. 2017, 7, 37–50. [Google Scholar]
- Wang, Y.; Fu, Y.; He, Z. Fetal Electrocardiogram Extraction Based on Fast ICA and Wavelet Denoising. In Proceedings of the 2018 2nd IEEE Advanced Information Management, Communicates, Electronic and Automation Control Conference (IMCEC), Xi’an, China,, 25–27 May 2018; pp. 466–469. [Google Scholar] [CrossRef]
- Sutha, P.; Jayanthi, V. Fetal Electrocardiogram Extraction and Analysis Using Adaptive Noise Cancellation and Wavelet Transformation Techniques. J. Med. Syst. 2017, 42, 21. [Google Scholar] [CrossRef] [PubMed]
- Zarzoso, V.; Nandi, A. Noninvasive fetal electrocardiogram extraction: Blind separation versus adaptive noise cancellation. IEEE Trans. Biomed. Eng. 2001, 48, 12–18. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Liu, S.; Zhang, J. Extraction of Fetal ECG Signal via Adaptive Noise Cancellation Approach. In Proceedings of the 2008 2nd International Conference on Bioinformatics and Biomedical Engineering, Shanghai, China, 16–18 May May 2008; pp. 2270–2273. [Google Scholar] [CrossRef]
- Hassanpour, H.; Parsaei, A. Fetal ECG Extraction Using Wavelet Transform. In Proceedings of the 2006 International Conference on Computational Inteligence for Modelling Control and Automation and International Conference on Intelligent Agents Web Technologies and International Commerce (CIMCA’06), Sydney, NSW, Australia, 28 November–1 December 2006; p. 179. [Google Scholar] [CrossRef]
- Wu, S.; Shen, Y.; Zhou, Z.; Lin, L.; Zeng, Y.; Gao, X. Research of fetal ECG extraction using wavelet analysis and adaptive filtering. Comput. Biol. Med. 2013, 43, 1622–1627. [Google Scholar] [CrossRef] [PubMed]
- Morales, D.P.; García, A.; Castillo, E.; Meyer-Baese, U.; Palma, A.J. Wavelets for full reconfigurable ECG acquisition system. In Proceedings of the Independent Component Analyses, Wavelets, Neural Networks, Biosystems, and Nanoengineering IX. International Society for Optics and Photonics, Orlando, FL, USA, 25–29 April 2011; Volume 8058, p. 805817. [Google Scholar] [CrossRef]
- Azbari, P.G.; Mohaqeqi, S.; Gashti, N.G.; Mikaili, M. Introducing a combined approach of empirical mode decomposition and PCA methods for maternal and fetal ECG signal processing. J. Matern.-Fetal Neonatal Med. 2016, 29, 3104–3109. [Google Scholar] [CrossRef] [PubMed]
- Sameni, R.; Shamsollahi, M.; Jutten, C. Filtering Electrocardiogram Signals Using the Extended Kalman Filter. In Proceedings of the 2005 IEEE Engineering in Medicine and Biology 27th Annual Conference, Shanghai, China, 17–18 January 2005; pp. 5639–5642. [Google Scholar] [CrossRef]
- Camps-Valls, G.; Martínez-Sober, M.; Soria-Olivas, E.; Magdalena-Benedito, R.; Calpe-Maravilla, J.; Guerrero-Martínez, J. Foetal ECG recovery using dynamic neural networks. Artif. Intell. Med. 2004, 31, 197–209. [Google Scholar] [CrossRef] [PubMed]
- Behar, J.; Johnson, A.E.W.; Oster, J.; Clifford, G. An Echo State Neural Network for Foetal ECG Extraction Optimised by Random Search. In Proceedings of the Machine Learning for Clinical Data Analysis and Healthcare, NIPS Workshop 2013, Lake Tahoe, NV, USA, 9–10 December 2013; p. 5. [Google Scholar]
- Fotiadou, E.; Vullings, R. Multi-Channel Fetal ECG Denoising With Deep Convolutional Neural Networks. Front. Pediatr. 2020, 8, 508. [Google Scholar] [CrossRef]
- Meyer-Baese, U. Adaptive Systems. In Digital Signal Processing with Field Programmable Gate Arrays; Meyer-Baese, U., Ed.; Signals and Communication Technology; Springer: Berlin/Heidelberg, Germany, 2014; pp. 533–630. [Google Scholar] [CrossRef]
- Ziani, S.; El Hassouani, Y. Fetal Electrocardiogram Analysis Based on LMS Adaptive Filtering and Complex Continuous Wavelet 1-D. In Big Data and Networks Technologies; Lecture Notes in Networks and, Systems, Farhaoui, Y., Eds.; Springer: Cham, Switzerland, 2020; pp. 360–366. [Google Scholar] [CrossRef]
- Swarnalath, R.; Prasad, D.V. A Novel Technique for Extraction of FECG using Multi Stage Adaptive Filtering. J. Appl. Sci. 2010, 10, 319–324. [Google Scholar] [CrossRef]
- Ramli, D.A.; Shiong, Y.H.; Hassan, N. Blind Source Separation (BSS) of Mixed Maternal and Fetal Electrocardiogram (ECG) Signal: A comparative Study. Procedia Comput. Sci. 2020, 176, 582–591. [Google Scholar] [CrossRef]
- Madhulatha, T.S. An Overview on Clustering Methods. IOSR J. Eng. 2012, 2, 719–725. [Google Scholar] [CrossRef]
- Clifford, G.D.; Silva, I.; Behar, J.; Moody, G.B. Noninvasive Fetal ECG analysis. Physiol. Meas. 2014, 35, 1521–1536. [Google Scholar] [CrossRef] [PubMed]
- Țarălungă, D.; Gussi, I.; Strungaru, R. A New Method for Fetal Electrocardiogram Denoising Using Blind Source Separation and Empirical Mode Decomposition. Rev. Roum. Sci. Techn.–Électrotechn. Énerg. 2016, 61, 94–98. [Google Scholar]
- Kanjilal, P.; Palit, S.; Saha, G. Fetal ECG extraction from single-channel maternal ECG using singular value decomposition. IEEE Trans. Biomed. Eng. 1997, 44, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Kanjilal, P.; Saha, G. Fetal ECG extraction from single channel maternal ECG using SVD and SVR spectrum. In Proceedings of the 17th International Conference of the Engineering in Medicine and Biology Society, Montreal, QC, Canada, 20–23 September 1995; Volume 1, pp. 187–188. [Google Scholar] [CrossRef]
- Meyer-Baese, U.; Muddu, H.; Schinhaerl, S.; Kumm, M.; Zipf, P. Real-time fetal ECG system design using embedded microprocessors. In Proceedings of the Sensing and Analysis Technologies for Biomedical and Cognitive Applications 2016. International Society for Optics and Photonics, Baltimore, MD, USA, 17–21 April 2016; Volume 9871, p. 987106. [Google Scholar] [CrossRef]
- Matonia, A.; Jezewski, J.; Kupka, T.; Horoba, K.; Wrobel, J.; Gacek, A. Abdominal and Direct Fetal ECG Database . Biomed. Eng. Tech. 2012, 57, 383–394. [Google Scholar] [CrossRef]
- Goldberger, A.L.; Amaral, L.A.N.; Glass, L.; Hausdorff, J.M.; Ivanov, P.C.; Mark, R.G.; Mietus, J.E.; Moody, G.B.; Peng, C.K.; Stanley, H.E. PhysioBank, PhysioToolkit, and PhysioNet. Circulation 2000, 101, e215–e220. [Google Scholar] [CrossRef]
- Open Data Commons Public Domain Dedication and License (PDDL) v1.0—Open Data Commons: Legal Tools for Open Data. Available online: https://physionet.org/about/licenses/open-data-commons-open-database-license-v10/ (accessed on 25 March 2024).
- Silva, I.; Behar, J.A.; Sameni, R.; Tingting, Z.; Clifford, G.; Moody, G. Noninvasive Fetal ECG—The PhysioNet Computing in Cardiology Challenge. 2013. Available online: https://physionet.org/content/challenge-2013/1.0.0/ (accessed on 25 March 2024).






















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| ADFECGDB Record | ||||||
|---|---|---|---|---|---|---|
| r01 | r04 | r07 | r08 | r10 | ||
| PCA | (%) | (%) | (%) | (%) | (%) | |
| Training results derived from the proposed framework | 15,000 | 93.10 | 87.4 | 91.94 | 89.35 | 94.98 |
| 20,000 | 97.42 | 97.77 | 98.56 | 91.45 | 94.29 | |
| 30,000 | 98.60 | 97.06 | 99.60 | 84.52 | 95.29 | |
| 50,000 | 96.8 | 96.72 | 99.60 | 92.16 | 94.98 | |
| 60,000 | 98.68 | 97.13 | 99.60 | 82.59 | 95.14 | |
| 100,000 | 99.3 | 96.15 | 99.52 | 89.39 | 94.83 | |
| 150,000 | 99.46 | 97.05 | 99.92 | 82.76 | 94.98 | |
| 300,000 | 99.38 | 97.61 | 99.76 | 90.52 | 94.98 | |
| Result summary from [14] | 99.38 | 97.62 | 98.96 | 99.08 | 98.09 | |
| 98.91 | 97.41 | 97.99 | 97.86 | 98.02 | ||
| 93.39 | 95.19 | 97.99 | 89.72 | 95.95 | ||
| Discarded channels | – | 1 | 1 | – | 3 | |
| Noisy channels | 2, 3 | 3 | – | 2, 3 | 4 | |
| ADFECGDB Record | ||||||
|---|---|---|---|---|---|---|
| r01 | r04 | r07 | r08 | r10 | ||
| PCA | (%) | (%) | (%) | (%) | (%) | |
| Training results derived from the proposed framework | 15,000 | 91.21 | 88.49 | 99.12 | 88.45 | 95.29 |
| 20,000 | 99.15 | 96.90 | 97.16 | 82.39 | 94.44 | |
| 30,000 | 98.91 | 96.75 | 98.31 | 78.14 | 93.47 | |
| 50,000 | 96.76 | 95.53 | 98.31 | 85.16 | 93.47 | |
| 60,000 | 98.76 | 97.54 | 98.72 | 84.99 | 94.44 | |
| 100,000 | 99.46 | 96.26 | 99.44 | 88.68 | 95.29 | |
| 150,000 | 99.53 | 94.44 | 99.28 | 86.15 | 94.29 | |
| 300,000 | 99.46 | 95.65 | 99.68 | 92 | 95.29 | |
| Result summary from [14] | 99.38 | 97.62 | 98.96 | 99.08 | 98.09 | |
| 98.91 | 97.41 | 97.99 | 97.86 | 98.02 | ||
| 93.39 | 95.19 | 97.99 | 89.72 | 95.95 | ||
| Discarded channels | – | 1 | 1 | – | 3 | |
| Noisy channels | 2, 3 | 3 | – | 2, 3 | 4 | |
| ADFECGDB Record | ||||||
|---|---|---|---|---|---|---|
| r01 | r04 | r07 | r08 | r10 | ||
| PCA | (%) | (%) | (%) | (%) | (%) | |
| Training results derived from the proposed framework | 15,000 | 93.10 | 87.40 | 91.94 | 89.35 | 94.98 |
| 20,000 | 97.42 | 97.77 | 98.56 | 91.45 | 94.29 | |
| 30,000 | 98.6 | 97.06 | 99.60 | 84.52 | 95.29 | |
| 50,000 | 96.80 | 96.72 | 99.6 | 92.16 | 94.98 | |
| 60,000 | 98.68 | 97.13 | 99.6 | 82.59 | 95.14 | |
| 100,000 | 99.30 | 96.15 | 99.52 | 89.39 | 94.83 | |
| 150,000 | 99.46 | 97.05 | 99.92 | 82.76 | 94.98 | |
| 300,000 | 99.38 | 97.61 | 99.76 | 90.52 | 94.98 | |
| Result summary from [14] | 99.38 | 97.62 | 98.96 | 99.08 | 98.09 | |
| 98.91 | 97.41 | 97.99 | 97.86 | 98.02 | ||
| 93.39 | 95.19 | 97.99 | 89.72 | 95.95 | ||
| Discarded channels | – | 1 | 1 | – | 3 | |
| Noisy channels | 2, 3 | 3 | – | 2, 3 | 4 | |
| ADFECGDB Record | ||||||
|---|---|---|---|---|---|---|
| r01 | r04 | r07 | r08 | r10 | ||
| PCA | (%) | (%) | (%) | (%) | (%) | |
| Training results derived from the proposed framework | 15,000 | 89.06 | 88.56 | 98.49 | 90.98 | 94.76 |
| 20,000 | 91.71 | 91.98 | 86.90 | 93.08 | 95.22 | |
| 30,000 | 88.25 | 97.77 | 99.28 | 84.54 | 95.06 | |
| 50,000 | 99.46 | 97.37 | 99.68 | 89.79 | 95.22 | |
| 60,000 | 87.81 | 96.5 | 99.68 | 86.75 | 94.76 | |
| 100,000 | 99.22 | 97.13 | 99.84 | 88.17 | 95.22 | |
| 150,000 | 99.22 | 97.37 | 99.84 | 87.01 | 95.22 | |
| 300,000 | 99.07 | 96.48 | 99.84 | 89.73 | 95.22 | |
| Result summary from [14] | 99.38 | 97.62 | 98.96 | 99.08 | 98.09 | |
| 98.91 | 97.41 | 97.99 | 97.86 | 98.02 | ||
| 93.39 | 95.19 | 97.99 | 89.72 | 95.95 | ||
| Discarded channels | – | 1 | 1 | – | 3 | |
| Noisy channels | 2, 3 | 3 | – | 2, 3 | 4 | |
| ADFECGDB Record | ||||||
|---|---|---|---|---|---|---|
| r01 | r04 | r07 | r08 | r10 | ||
| PCA | (%) | (%) | (%) | (%) | (%) | |
| Training results derived from the proposed framework | 15,000 | 93.10 | 87.4 | 91.94 | 89.35 | 94.98 |
| 20,000 | 97.42 | 97.77 | 98.56 | 91.45 | 94.29 | |
| 30,000 | 98.60 | 97.06 | 99.60 | 84.52 | 95.29 | |
| 50,000 | 96.8 | 96.72 | 99.60 | 92.16 | 94.98 | |
| 60,000 | 98.68 | 97.13 | 99.60 | 82.59 | 95.14 | |
| 100,000 | 99.3 | 96.15 | 99.52 | 89.39 | 94.83 | |
| 150,000 | 99.46 | 97.05 | 99.92 | 82.76 | 94.98 | |
| 300,000 | 99.38 | 97.61 | 99.76 | 90.52 | 94.98 | |
| Result summary from [14] | 99.38 | 97.62 | 98.96 | 99.08 | 98.09 | |
| 98.91 | 97.41 | 97.99 | 97.86 | 98.02 | ||
| 93.39 | 95.19 | 97.99 | 89.72 | 95.95 | ||
| Discarded channels | – | 1 | 1 | – | 3 | |
| Noisy channels | 2, 3 | 3 | – | 2, 3 | 4 | |
| [14] (60,000-Sample Window) | PCA 15,000 | PCA 30,000 | PCA 60,000 | |||||||
|---|---|---|---|---|---|---|---|---|---|---|
| Record | Used Channels | Max (%) | Min (%) | Cluster 15,000 (%) | Cluster 15,000 (%) | Cluster 30,000 (%) | Cluster 15,000 (%) | Cluster 20,000 (%) | Cluster 30,000 (%) | Cluster 60,000 (%) |
| a03 | 1, 2, 4 | 100.00 | 96.88 | 96.47 | 96.47 | 96.47 | 96.47 | 96.47 | 96.47 | 94.94 |
| a04 | 1, 3, 4 | 99.22 | 96.88 | 96.85 | 99.23 | 99.23 | 99.23 | 99.23 | 99.23 | 99.23 |
| a05 | 1, 3, 4 | 100.00 | 97.04 | 99.61 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| a08 | 3, 4 | 100.00 | 99.21 | 72.17 | 80.87 | 99.22 | 82.55 | 97.64 | 96.06 | 98.43 |
| a12 | 1, 2 | 99.64 | 99.64 | 99.28 | 99.28 | 99.28 | 99.28 | 99.28 | 99.28 | 99.28 |
| a13 | 2, 3, 4 | 100.00 | 97.56 | 99.21 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| a14 | 1 | 97.94 | 97.94 | 90.98 | 91.80 | 96.33 | 90.98 | 85.94 | 96.33 | 97.14 |
| a20 | 2, 3 | 100.00 | 96.85 | 100.00 | 100.00 | 100.00 | 100.00 | 99.62 | 100.00 | 100.00 |
| a22 | 1, 4 | 100.00 | 100.00 | 86.34 | 96.03 | 96.41 | 96.41 | 96.41 | 96.41 | 96.41 |
| a23 | 2, 3, 4 | 98.80 | 97.58 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| a24 | 2, 3, 4 | 100.00 | 98.36 | 99.18 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| a25 | 2 | 100.00 | 100.00 | 98.39 | 98.79 | 98.79 | 98.79 | 100.00 | 98.79 | 98.79 |
| a28 | 1, 2, 3 | 98.16 | 96.95 | 96.97 | 96.97 | 96.97 | 96.97 | 96.95 | 96.05 | 96.64 |
| a35 | 1, 2, 3, 4 | 98.47 | 97.83 | 97.23 | 97.23 | 97.53 | 97.23 | 97.23 | 97.23 | 97.53 |
| a36 | 1, 2, 3, 4 | 100.00 | 98.49 | 98.20 | 98.20 | 99.10 | 98.20 | 97.89 | 99.10 | 99.40 |
| a44 | 1, 2, 3, 4 | 100.00 | 97.52 | 99.08 | 99.08 | 99.39 | 99.08 | 99.08 | 99.39 | 99.39 |
| a49 | 1, 2, 3 | 100.00 | 98.98 | 95.50 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 | 100.00 |
| a55 | 2, 3 | 96.43 | 92.75 | 40.64 | 40.64 | 38.46 | 40.64 | 38.25 | 38.46 | 38.46 |
| a61 | 2, 4 | 97.42 | 95.34 | 10.11 | 11.15 | 15.69 | 16.33 | 14.67 | 14.48 | 18.79 |
| a62 | 2, 3, 4 | 99.30 | 97.18 | 92.96 | 83.75 | 83.75 | 98.26 | 98.26 | 98.26 | 97.20 |
| a65 | 2, 4 | 97.87 | 92.53 | 94.29 | 94.29 | 82.68 | 94.29 | 78.23 | 83.27 | 83.27 |
| a66 | 3 | 94.44 | 94.44 | 90.69 | 91.50 | 92.31 | 90.16 | 92.31 | 90.08 | 90.08 |
| a67 | 4 | 91.53 | 91.53 | 87.41 | 84.13 | 87.37 | 85.09 | 92.67 | 87.68 | 91.29 |
| a69 | 1 | 94.44 | 94.44 | 80.99 | 70.92 | 75.45 | 58.52 | 66.42 | 60.97 | 62.31 |
| a70 | 1, 2 | 98.21 | 91.37 | 93.82 | 96.77 | 91.11 | 97.86 | 85.16 | 86.92 | 78.19 |
| a72 | 1, 2, 3, 4 | 100.00 | 97.58 | 98.80 | 98.80 | 99.70 | 98.80 | 98.80 | 99.70 | 98.80 |
| a15 | – | – | – | 66.37 | 65.70 | 58.54 | 73.64 | 80.69 | 94.25 | 93.44 |
| a17 | – | – | – | 68.18 | 54.55 | 92.61 | 95.75 | 96.15 | 96.15 | 96.15 |
| a19 | – | – | – | 99.21 | 98.81 | 99.21 | 99.21 | 97.62 | 99.21 | 99.21 |
| a33 | – | – | – | 93.33 | 95.41 | 95.71 | 94.66 | 94.66 | 95.71 | 94.66 |
| a37 | – | – | – | 95.71 | 96.45 | 96.06 | 98.23 | 97.16 | 97.86 | 96.77 |
| a53 | – | – | – | 71.28 | 76.09 | 94.95 | 78.62 | 79.87 | 91.58 | 92.93 |
| a58 | – | – | – | 84.06 | 83.10 | 94.96 | 84.21 | 72.92 | 95.68 | 96.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Oyarzún, L.; Castillo, E.; Parrilla, L.; Meyer-Baese, U.; García, A. PCA-Based Preprocessing for Clustering-Based Fetal Heart Rate Extraction in Non-Invasive Fetal Electrocardiograms. Electronics 2024, 13, 1264. https://doi.org/10.3390/electronics13071264
Oyarzún L, Castillo E, Parrilla L, Meyer-Baese U, García A. PCA-Based Preprocessing for Clustering-Based Fetal Heart Rate Extraction in Non-Invasive Fetal Electrocardiograms. Electronics. 2024; 13(7):1264. https://doi.org/10.3390/electronics13071264
Chicago/Turabian StyleOyarzún, Luis, Encarnación Castillo, Luis Parrilla, Uwe Meyer-Baese, and Antonio García. 2024. "PCA-Based Preprocessing for Clustering-Based Fetal Heart Rate Extraction in Non-Invasive Fetal Electrocardiograms" Electronics 13, no. 7: 1264. https://doi.org/10.3390/electronics13071264