
Dynamically Adjusted and Peripheral Visualization of Reverse Optical Flow for VR Sickness Reduction

Abstract
:1. Introduction
2. Related Work
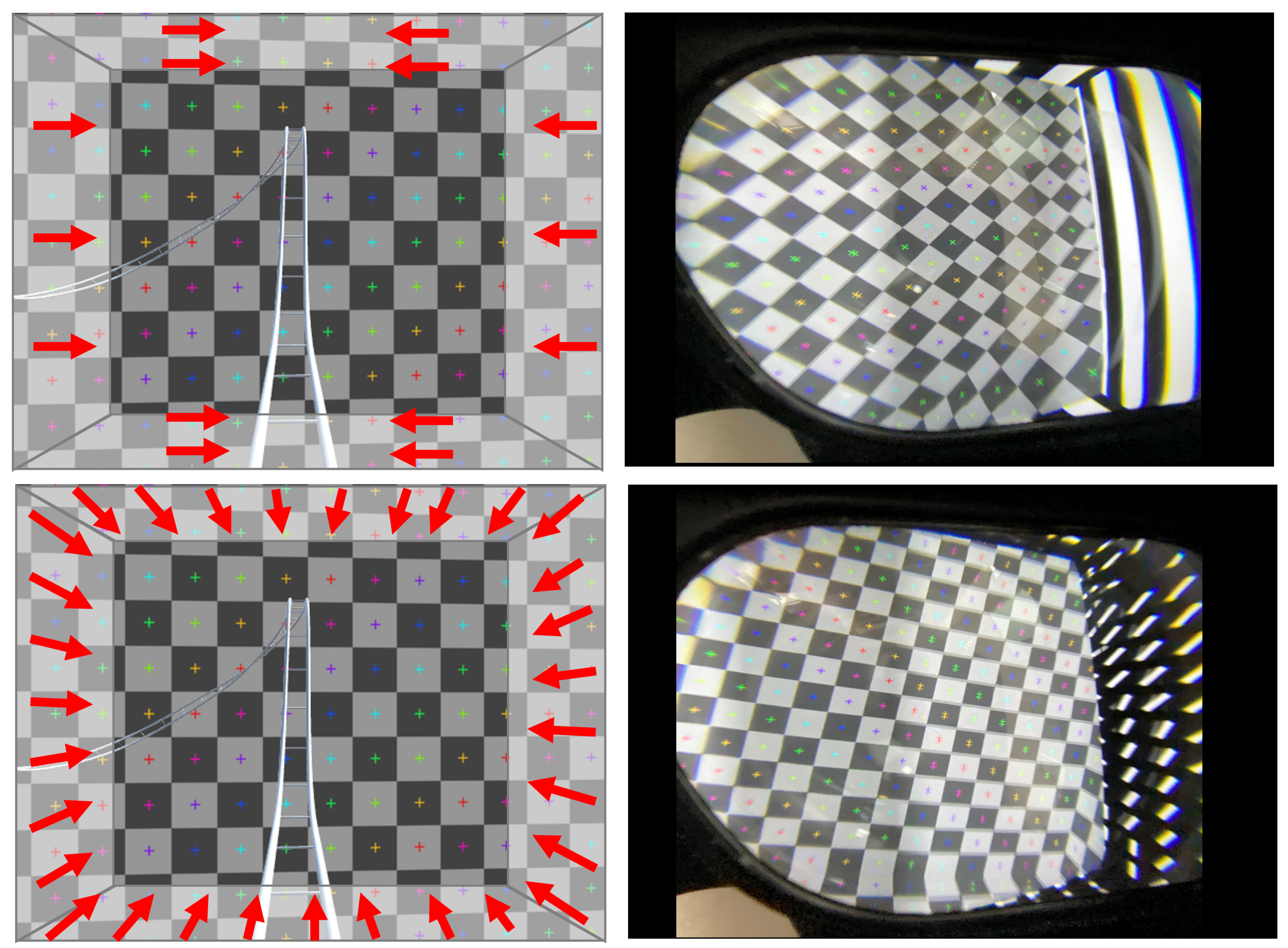
3. System Configuration: Reverse Optical Flow in the Visual Periphery
4. Pilot Experiment
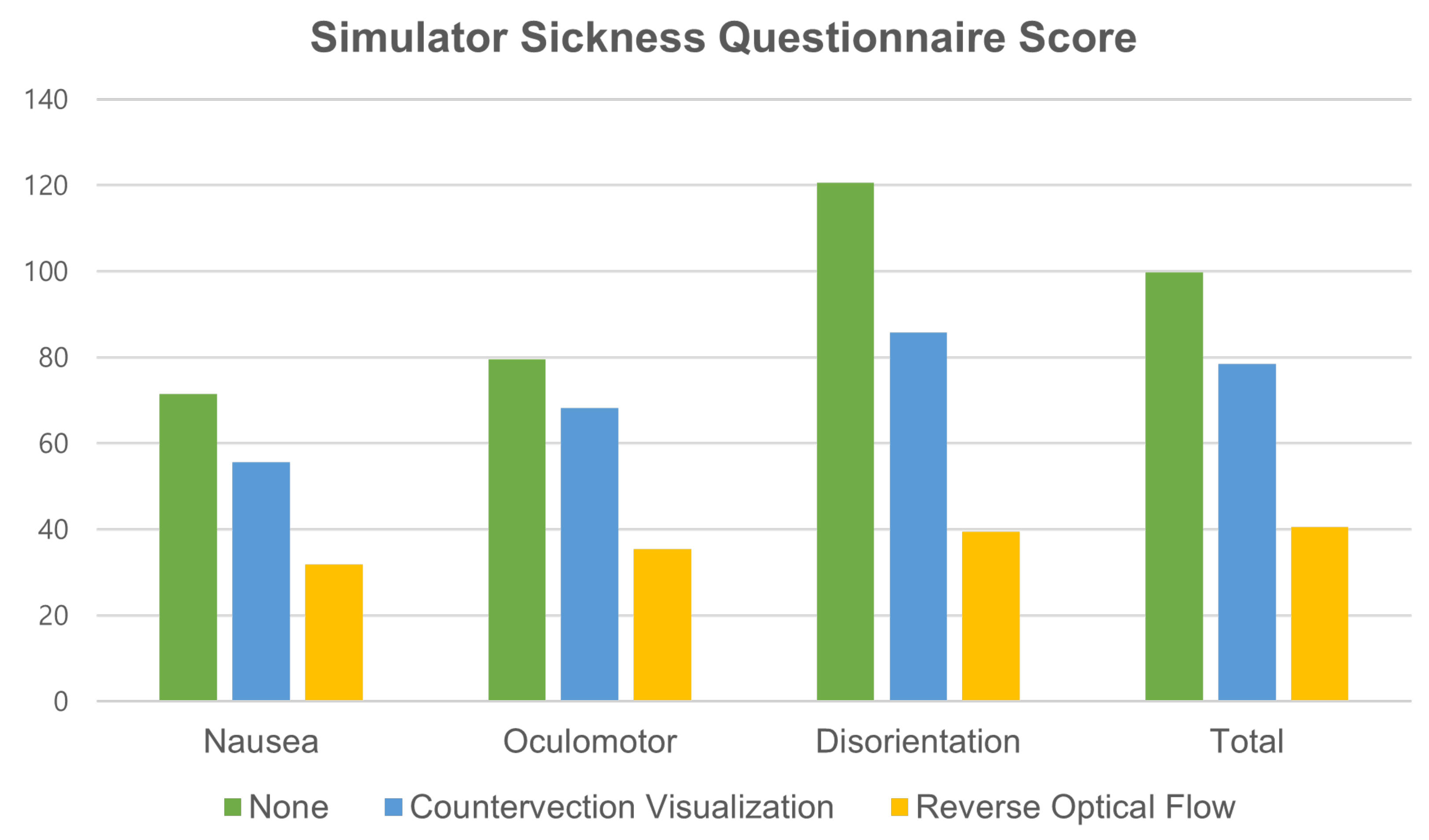
- None: The peripheral visual field was rendered black (baseline).
- Moving striped bars (CV): The peripheral visual field was rendered with a projection of rotating striped bars, situated at the top, bottom, left, and right ends of the display. This condition simulated a previous study [2].
- Reverse optical flow (RO): The peripheral visual field was rendered with the reverse optical flow, as suggested in [3].
5. Main Experiment
5.1. Experimental Design
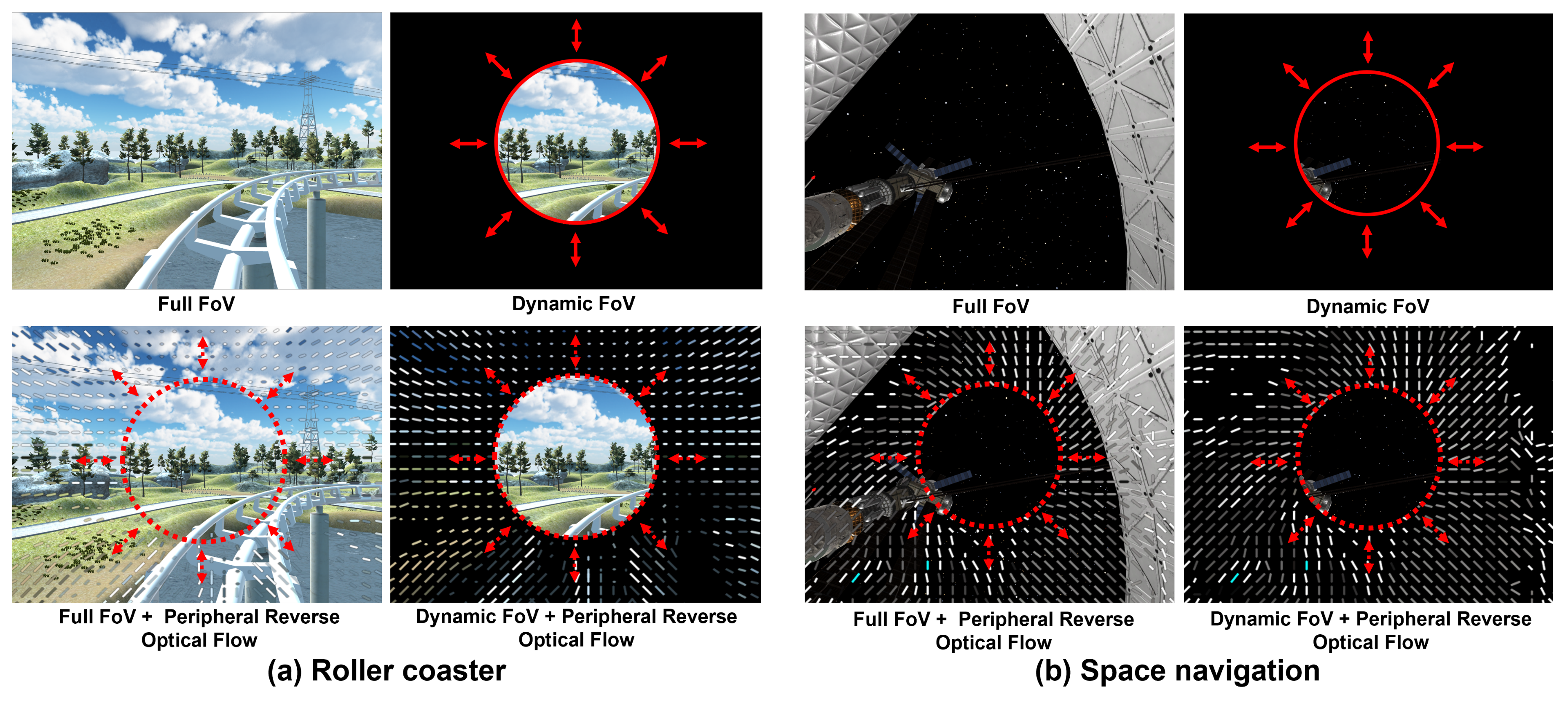
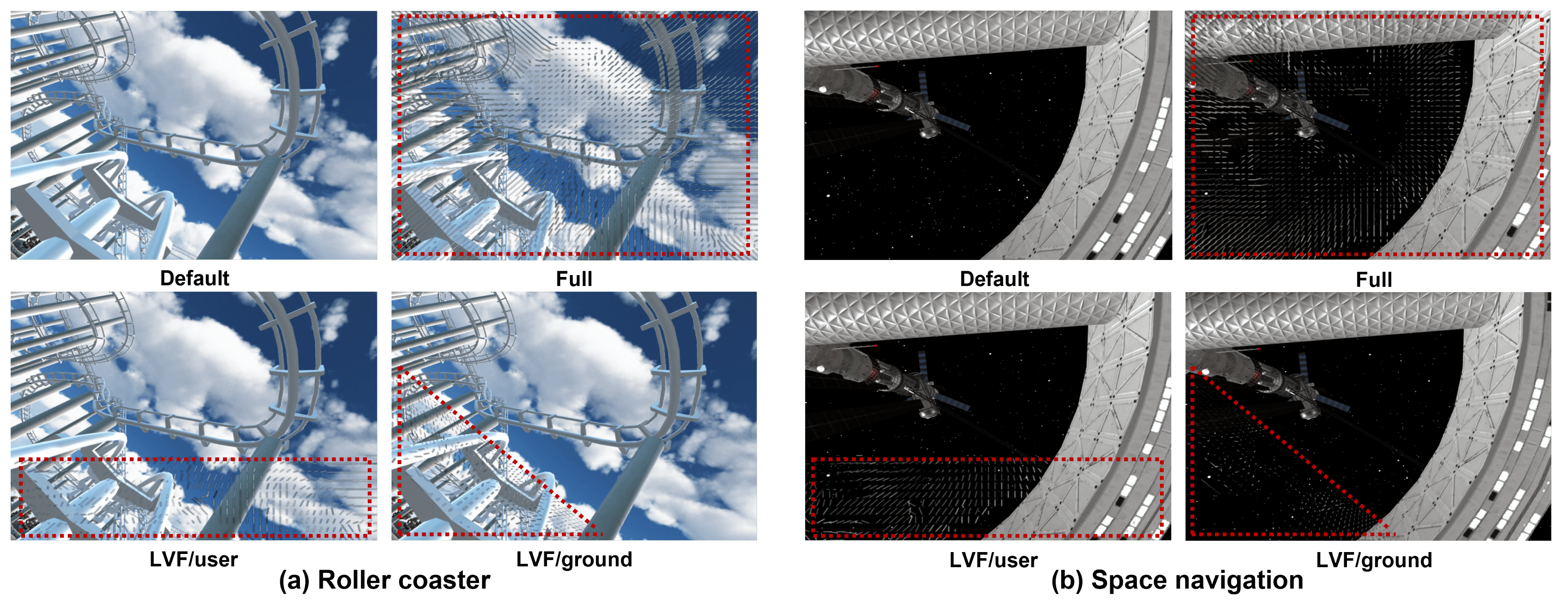
- None/full FoV (F-FoV): The content was displayed with the full FoV (baseline).
- Dynamic FoV (D-FoV): The content was displayed with the FoV adjusted according to the logic described in Section 3. The display was blacked out beyond the FoV.
- Full FoV + peripheral reverse optical flow (F-FoV+P-ROF): The content was displayed with the full FoV, but with the reverse optical flow mixed in and overlaid on the periphery. The extent of the periphery was determined by the same dynamic FoV algorithm applied in the second condition, and the reverse optical flow visualization followed the same method as proposed by [3] and in the first pilot experiment.
- Dynamic FoV + peripheral reverse optical flow (D-FoV+P-ROF): The same dynamic FoV algorithm as in the second condition was used. However, the periphery beyond the FoV was overlaid with the reverse optical flow with a blacked-out background.
5.2. Participants
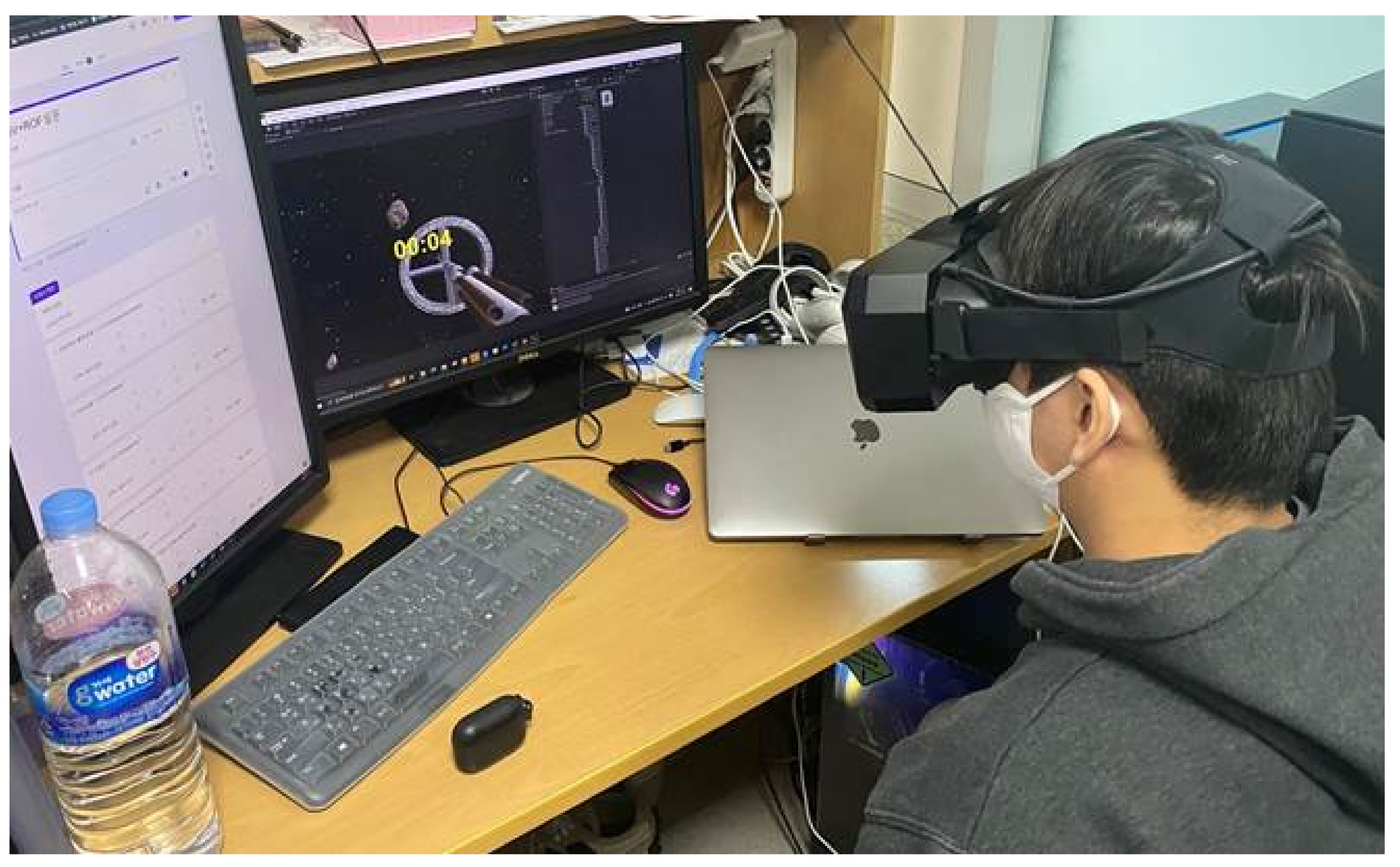
5.3. Experimental Procedure
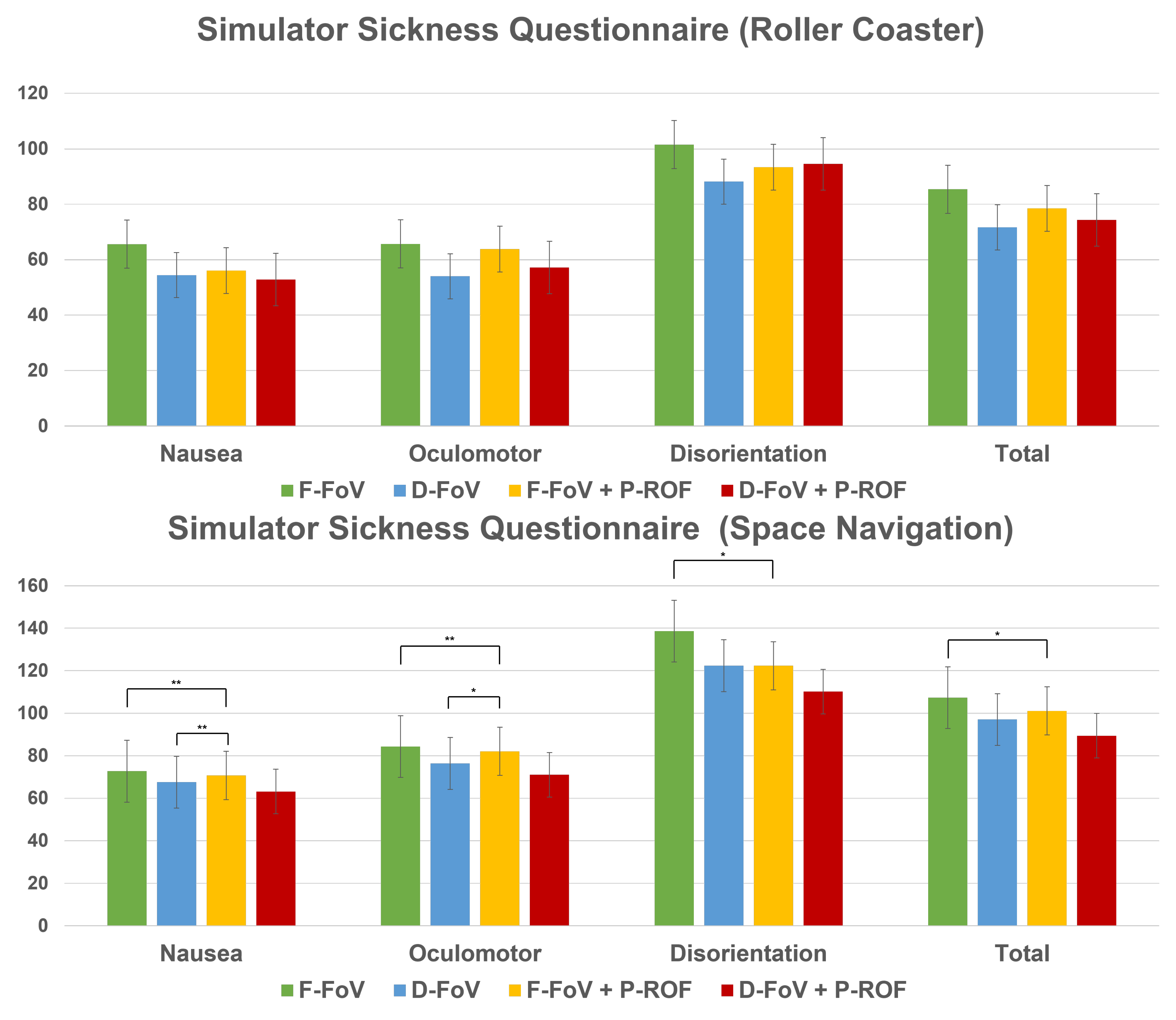
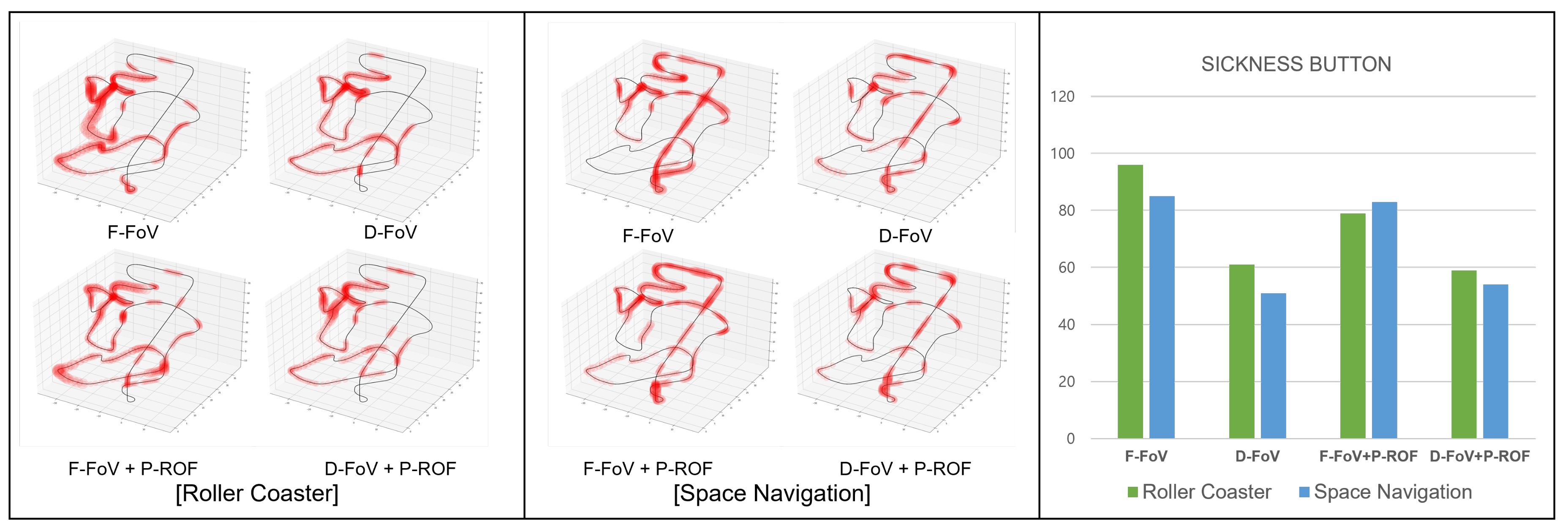
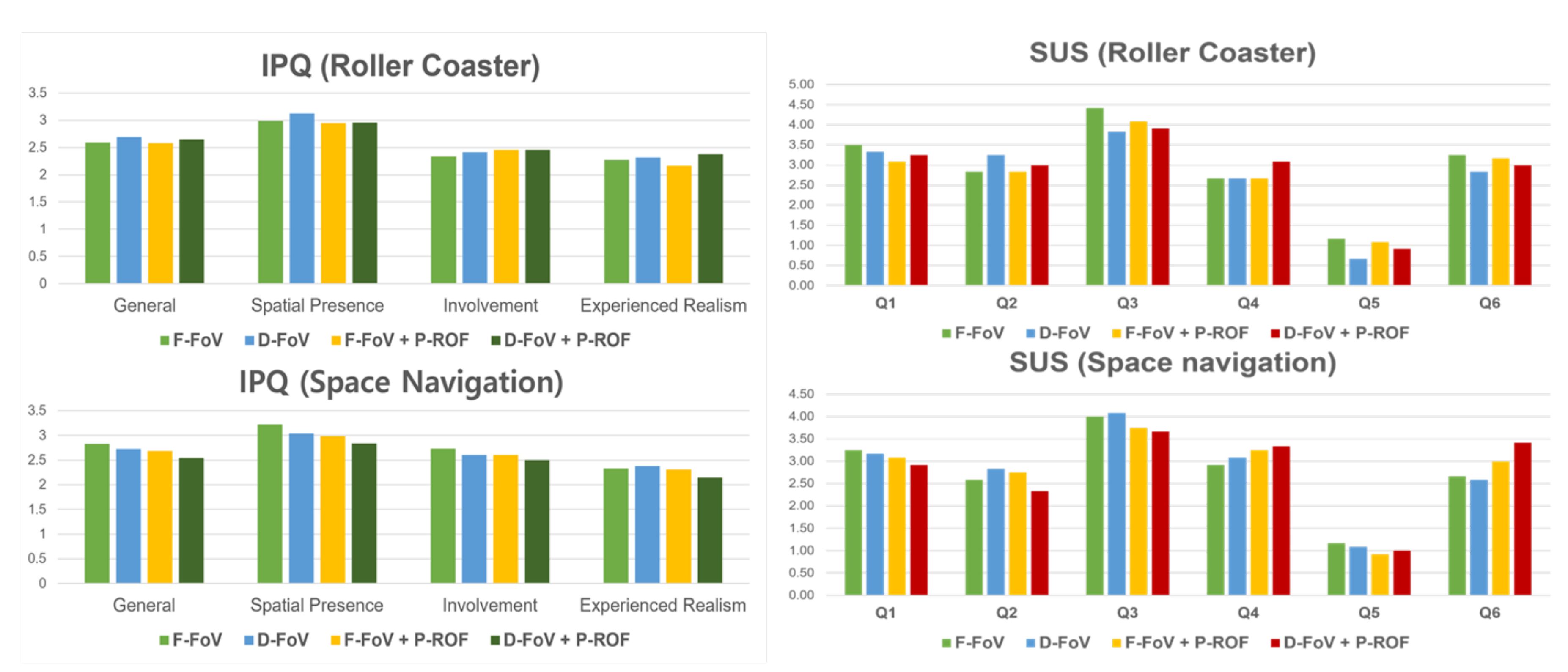
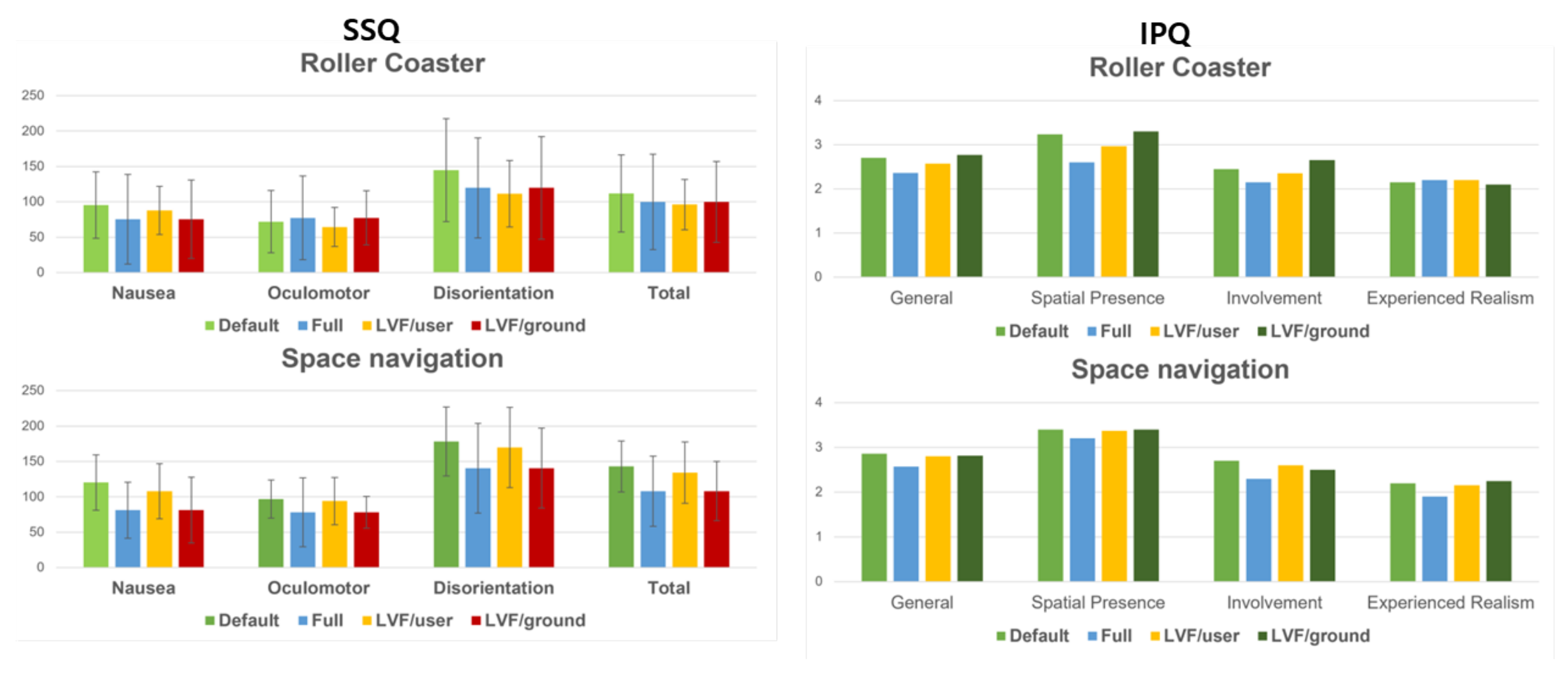
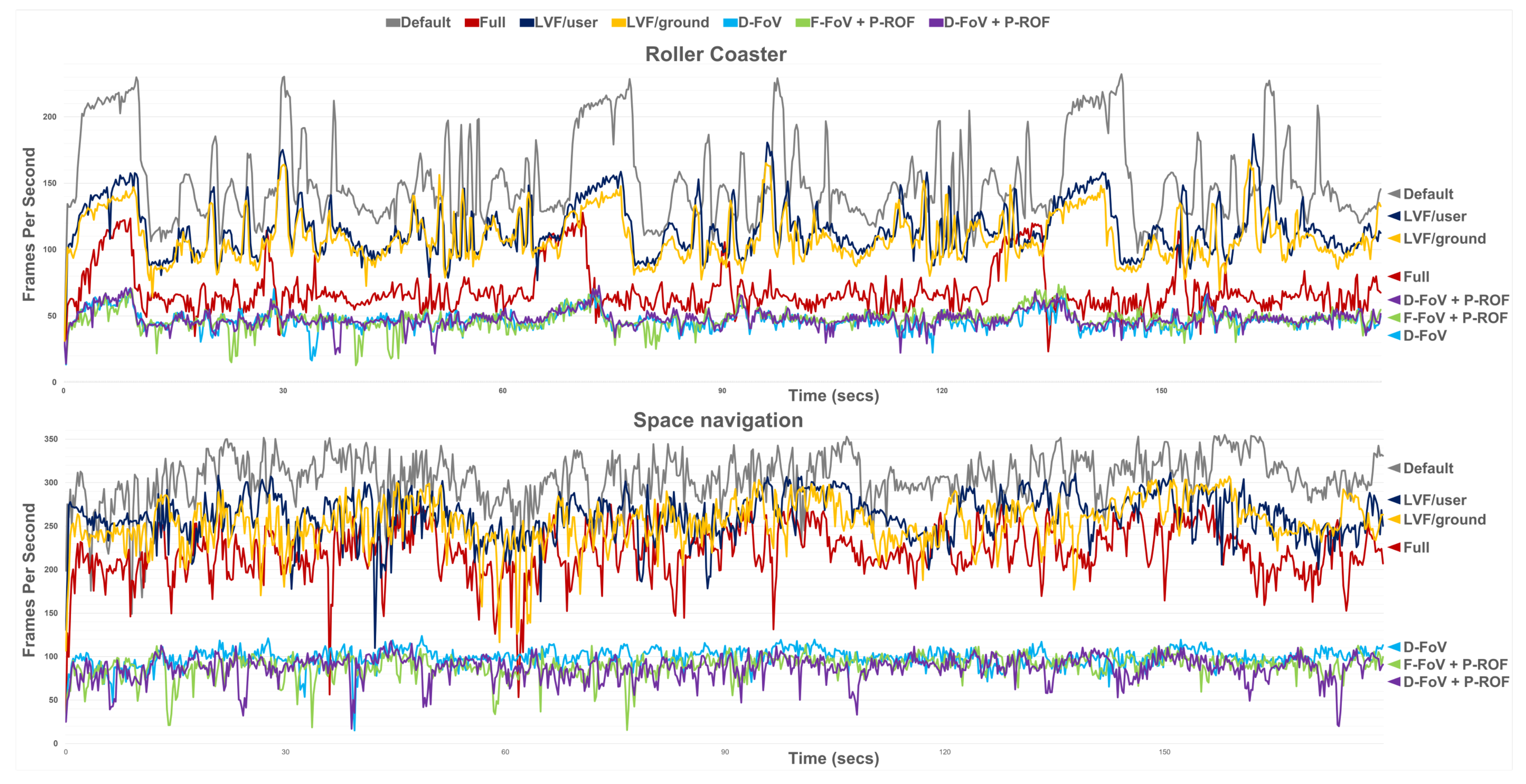
5.4. Results
6. Supplement Experiment: Restricting Reverse Optical Flow Only to Low Visual Field
7. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| VR | Virtual reality |
| FoV | Field of view |
| SSQ | Simulation sickness questionnaire |
| CV | Countervection |
| RO | Reverse optical flow |
| F-FoV | Full FoV |
| D-FoV | Dynamic FoV |
| P-ROF | Peripheral reverse optical flow |
| USD | US Dollar |
| IPQ | Igroup Presence Questionnaire |
| SUS | Slater, Usoh, and Steed |
Appendix A

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Igroup Presence Questionnaire (IPQ) | ||||
|---|---|---|---|---|
| 01. | In the computer generated world I had a sense of “being there”. | 1 (not at all) | ∼ | 7 (very much) |
| 02. | Somehow I felt that the virtual world surrounded me. | 1 (fully disagree) | ∼ | 7 (fully agree) |
| 03. | I felt like I was just perceiving pictures. | 1 (fully disagree) | ∼ | 7 (fully agree) |
| 04. | I did not feel present in the virtual space. | 1 (did not feel) | ∼ | 7 (felt present) |
| 05. | I had a sense of acting in the virtual space, rather than operating something from outside. | 1 (fully disagree) | ∼ | 7 (fully agree) |
| 06. | I felt present in the virtual space. | 1 (fully disagree) | ∼ | 7 (fully agree) |
| 07. | How aware were you of the real world surrounding while navigating in the virtual world? (i.e., sounds, room temperature, other people, etc.)? | 1 (extremely aware) | ∼ | 7 (not aware at all) |
| 08. | I was not aware of my real environment. | 1 (fully disagree) | ∼ | 7 (fully agree) |
| 09. | I still paid attention to the real environment. | 1 (fully disagree) | ∼ | 7 (fully agree) |
| 10. | I was completely captivated by the virtual world. | 1 (fully disagree) | ∼ | 7 (fully agree) |
| 11. | How real did the virtual world seem to you? | 1 (completely real) | ∼ | 7 (not real at all) |
| 12. | How much did your experience in the virtual environment seem consistent with your real world experience? | 1 (not consistent) | ∼ | 7 (very consistent) |
| 13. | How real did the virtual world seem to you? | 1 (about as real as an imagined world) | ∼ | 7 (indistinguishable from the real world) |
| 14. | The virtual world seemed more realistic than the real world. | 0 (fully disagree) | ∼ | 3 (fully agree) |
| Slater–Usoh–Steed Questionnaire (SUS) | ||||
|---|---|---|---|---|
| 01. | I had a sense of “being there” in the virtual environment | 1 (Not at all) | ∼ | 7 (Very much) |
| 02. | There were times during the experience when the virtual environment was the reality for me... | 1 (At no time) | ∼ | 7 (Almost all the time) |
| 03. | The virtual environment seems to me to be more like... | 1 (Images that I saw) | ∼ | 7 (Somewhere that I visited) |
| 04. | I had a stronger sense of... | 1 (Being elsewhere) | ∼ | 7 (Being in the virtual environment) |
| 05. | I think of the virtual environment as a place in a way similar to other places that I’ve been today... | 1 (Not at all) | ∼ | 7 (Very much so) |
| 06. | During the experience I often thought that I was really standing in the virtual environment... | 1 (Not very often) | ∼ | 7 (Very much so) |
References
- LaViola, J., Jr. A discussion of cybersickness in virtual environments. ACM Sigchi Bull. 2000, 32, 47–56. [Google Scholar]
- Xiao, R.; Benko, H. Augmenting the field-of-view of head-mounted displays with sparse peripheral displays. In Proceedings of the 2016 CHI Conference on Human Factors in Computing Systems, San Jose, CA, USA, 7–12 May 2016; pp. 1221–1232. [Google Scholar]
- Park, S.H.; Han, B.; Kim, G.J. Mixing in reverse optical flow to mitigate vection and simulation sickness in virtual reality. In Proceedings of the CHI Conference on Human Factors in Computing Systems, New Orleans, LA, USA, 29 April–5 May 2022; pp. 1–11. [Google Scholar]
- Fernandes, A.S.; Feiner, S.K. Combating VR sickness through subtle dynamic field-of-view modification. In Proceedings of the 2016 IEEE Symposium on 3D User Interfaces (3DUI), Greenville, SC, USA, 19–20 March 2016; pp. 201–210. [Google Scholar]
- Jones, J.A.; Swan II, J.E.; Bolas, M. Peripheral stimulation and its effect on perceived spatial scale in virtual environments. IEEE Trans. Vis. Comput. Graph. 2013, 19, 701–710. [Google Scholar] [CrossRef]
- Telford, L.; Frost, B. Factors affecting the onset and magnitude of linear vection. Percept. Psychophys. 1993, 53, 682–692. [Google Scholar] [CrossRef]
- Sato, T.; Seno, T.; Kanaya, H.; Hukazawa, H. The ground is more effective than the sky—The comparison of the ground and the sky in effectiveness for vection. In Proceedings of the ASIAGRAPH 2007, Shanghai, China, 15–17 November 2007; pp. 103–108. [Google Scholar]
- Budhiraja, P.; Miller, M.R.; Modi, A.K.; Forsyth, D. Rotation blurring: Use of artificial blurring to reduce cybersickness in virtual reality first person shooters. arXiv 2017, arXiv:1710.02599. [Google Scholar]
- Wienrich, C.; Weidner, C.K.; Schatto, C.; Obremski, D.; Israel, J.H. A virtual nose as a rest-frame-the impact on simulator sickness and game experience. In Proceedings of the 2018 10th International Conference on Virtual Worlds and Games for Serious Applications (VS-Games), Würzburg, Germany, 5–7 September 2018; pp. 1–8. [Google Scholar]
- Cao, Z. The Effect of Rest Frames on Simulator Sickness Reduction. Ph.D. Thesis, Duke University, Durham, NC, USA, 2017. [Google Scholar]
- Gibson, J.J. The Perception of the Visual World; Houghton Mifflin: Boston, MA, USA, 1950. [Google Scholar]
- Fujii, Y.; Seno, T. The effect of optical flow motion direction on vection strength. i-Perception 2020, 11, 2041669519899108. [Google Scholar]
- Fujimoto, K.; Ashida, H. Roles of the Retinotopic and Environmental Frames of Reference on Vection. Front. Virtual Real. 2020, 1, 581920. [Google Scholar]
- D’Avossa, G.; Kersten, D. Evidence in Human Subjects for Independent Coding of Azimuth and Elevation for Direction of Heading from Optic Flow. Vis. Res. 1996, 36, 2915–2924. [Google Scholar]
- Carrasco, M.W.P.; Yeshurun, Y. Covert attention increases spatial resolution with or without masks: Support for signal enhancement. J. Vis. 2002, 2, 4. [Google Scholar] [CrossRef]
- Zito, G.A.; Cazzoli, D.; Müri, R.M.; Mosimann, U.P.; Nef, T. Behavioral Differences in the Upper and Lower Visual Hemifields in Shape and Motion Perception. Front. Behav. Neurosci. 2016, 10, 128. [Google Scholar]
- Amenedo, E.; Pazo-Alvarez, P.; Cadaveira, F. Vertical asymmetries in pre-attentive detection of changes in motion direction. Int. J. Psychophysiol. 2007, 64, 184–189. [Google Scholar]
- Previc, F. Functional specialization in the lower and upper visual fields in humans: Its ecological origins and neurophysiological implications. Behav. Brain Sci. 1990, 13, 519–542. [Google Scholar] [CrossRef]
- Hemmerich, W.; Keshavarz, B.; Hecht, H. Visually induced motion sickness on the horizon. Front. Virtual Real. 2020, 1, 582095. [Google Scholar]
- Wilkinson, M.; Brantley, S.; Feng, J. A Mini Review of Presence and Immersion in Virtual Reality. Proc. Hum. Factors Ergon. Soc. Annu. Meet. 2021, 65, 1099–1103. [Google Scholar] [CrossRef]
- Heeter, C. Being There: The Subjective Experience of Presence. Presence Teleoperators Virtual Environ. 1992, 2, 262–271. [Google Scholar]
- Azarby, S.; Rice, A. Understanding the Effects of Virtual Reality System Usage on Spatial Perception: The Potential Impacts of Immersive Virtual Reality on Spatial Design Decisions. Sustainability 2022, 14, 10326. [Google Scholar] [CrossRef]
- Slater, M. Measuring Presence: A Response to the Witmer and Singer Presence Questionnaire. Presence 1999, 8, 560–565. [Google Scholar]
- Witmer, B.G.; Singer, M.J. Measuring Presence in Virtual Environments: A Presence Questionnaire. Presence 1998, 7, 225–240. [Google Scholar] [CrossRef]
- Berkman, M.I.; Akan, E. Presence and Immersion in Virtual Reality. In Encyclopedia of Computer Graphics and Games; Lee, N., Ed.; Springer International Publishing: Cham, Switzerland, 2019; pp. 1–10. [Google Scholar]
- Hvass, J.; Larsen, O.; Vendelbo, K.; Nilsson, N.; Nordahl, R.; Serafin, S. Visual realism and presence in a virtual reality game. In Proceedings of the 2017 3DTV Conference: The True Vision—Capture, Transmission and Display of 3D Video (3DTV-CON), Copenhagen, Denmark, 7–9 June 2017; pp. 1–4. [Google Scholar]
- Lin, J.W.; Duh, H.; Parker, D.; Abi-Rached, H.; Furness, T. Effects of field of view on presence, enjoyment, memory, and simulator sickness in a virtual environment. In Proceedings of the Proceedings IEEE Virtual Reality 2002, Orlando, FL, USA, 24–28 March 2002; pp. 164–171. [Google Scholar]
- Schubert, T.; Friedmann, F.; Regenbrecht, H. The experience of presence: Factor analytic insights. Presence Teleoperators Virtual Environ. 2001, 10, 266–281. [Google Scholar] [CrossRef]
- Usoh, M.; Catena, E.; Arman, S.; Slater, M. Using presence questionnaires in reality. Presence 2000, 9, 497–503. [Google Scholar] [CrossRef]
- Unity. 2022. Available online: https://unity.com (accessed on 5 February 2023).
- Lucas, B.D.; Kanade, T. An iterative image registration technique with an application to stereo vision. In Proceedings of the IJCAI’81: 7th International Joint Conference on Artificial Intelligence, Vancouver, BC, Canada, 24–28 August 1981; Volume 81. [Google Scholar]
- Kennedy, R.S.; Lane, N.E.; Berbaum, K.S.; Lilienthal, M.G. Simulator sickness questionnaire: An enhanced method for quantifying simulator sickness. Int. J. Aviat. Psychol. 1993, 3, 203–220. [Google Scholar]
- Golding, J.F. Motion sickness susceptibility questionnaire revised and its relationship to other forms of sickness. Brain Res. Bull. 1998, 47, 507–516. [Google Scholar] [CrossRef]
- Kim, W.; Lee, S.; Bovik, A.C. VR sickness versus VR presence: A statistical prediction model. IEEE Trans. Image Process. 2020, 30, 559–571. [Google Scholar] [CrossRef]
- Wang, Y.; Chardonnet, J.R.; Merienne, F. VR sickness prediction for navigation in immersive virtual environments using a deep long short term memory model. In Proceedings of the 2019 IEEE Conference on Virtual Reality and 3D User Interfaces (VR), Osaka, Japan, 23–27 March 2019; pp. 1874–1881. [Google Scholar]
- Hell, S.; Argyriou, V. Machine learning architectures to predict motion sickness using a virtual reality rollercoaster simulation tool. In Proceedings of the 2018 IEEE International Conference on Artificial Intelligence and Virtual Reality (AIVR), Taichung, Taiwan, 10–12 December 2018; pp. 153–156. [Google Scholar]
- Islam, R.; Desai, K.; Quarles, J. Cybersickness Prediction from Integrated HMD’s Sensors: A Multimodal Deep Fusion Approach using Eye-tracking and Head-tracking Data. In Proceedings of the 2021 IEEE International Symposium on Mixed and Augmented Reality (ISMAR), Bari, Italy, 4–8 October 2021; pp. 31–40. [Google Scholar]










| Roller Coaster | Space Navigation | |
|---|---|---|
| Nausea | 0.7292 (0.4338) | 0.0007 (6.129) * |
| Oculomotor | 0.6313 (0.5773) | 0.0047 (4.6028) * |
| Disorientation | 0.9326 (0.1449) | 0.0146 (3.6903) * |
| Total | 0.7874 (0.3524) | 0.0307 (3.0945) * |
| Roller Coaster | Space Navigation | ||||||||
|---|---|---|---|---|---|---|---|---|---|
| N | O | D | T | N | O | D | T | ||
| F-FoV | D-FoV | 0.7766 | 0.6458 | 0.8999 | 0.7458 | 0.893 | 0.8999 | 0.8999 | 0.8999 |
| F-FoV | F-FoV + P-ROF | 0.8488 | 0.8999 | 0.8999 | 0.8999 | 0.0010 * | 0.0052 * | 0.0135 * | 0.0317 * |
| F-FoV | D-FoV + P-ROF | 0.7045 | 0.8177 | 0.8999 | 0.8493 | 0.1653 | 0.2631 | 0.2694 | 0.4081 |
| D-FoV | F-FoV + P-ROF | 0.8999 | 0.7489 | 0.8999 | 0.8999 | 0.0080 * | 0.0265 * | 0.0813 | 0.0997 |
| D-FoV | D-FoV + P-ROF | 0.8999 | 0.8999 | 0.8999 | 0.8999 | 0.5086 | 0.566 | 0.6463 | 0.6735 |
| F-FoV + P-ROF | D-FoV + P-ROF | 0.8999 | 0.8999 | 0.8999 | 0.8999 | 0.2424 | 0.3995 | 0.572 | 0.5952 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kim, S.; Kim, G.J. Dynamically Adjusted and Peripheral Visualization of Reverse Optical Flow for VR Sickness Reduction. Electronics 2023, 12, 861. https://doi.org/10.3390/electronics12040861
Kim S, Kim GJ. Dynamically Adjusted and Peripheral Visualization of Reverse Optical Flow for VR Sickness Reduction. Electronics. 2023; 12(4):861. https://doi.org/10.3390/electronics12040861
Chicago/Turabian StyleKim, Songmin, and Gerard J. Kim. 2023. "Dynamically Adjusted and Peripheral Visualization of Reverse Optical Flow for VR Sickness Reduction" Electronics 12, no. 4: 861. https://doi.org/10.3390/electronics12040861