
A Customized Efficient Deep Learning Model for the Diagnosis of Acute Leukemia Cells Based on Lymphocyte and Monocyte Images
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. The General Model of CNN
2.2. The General Model of GAN
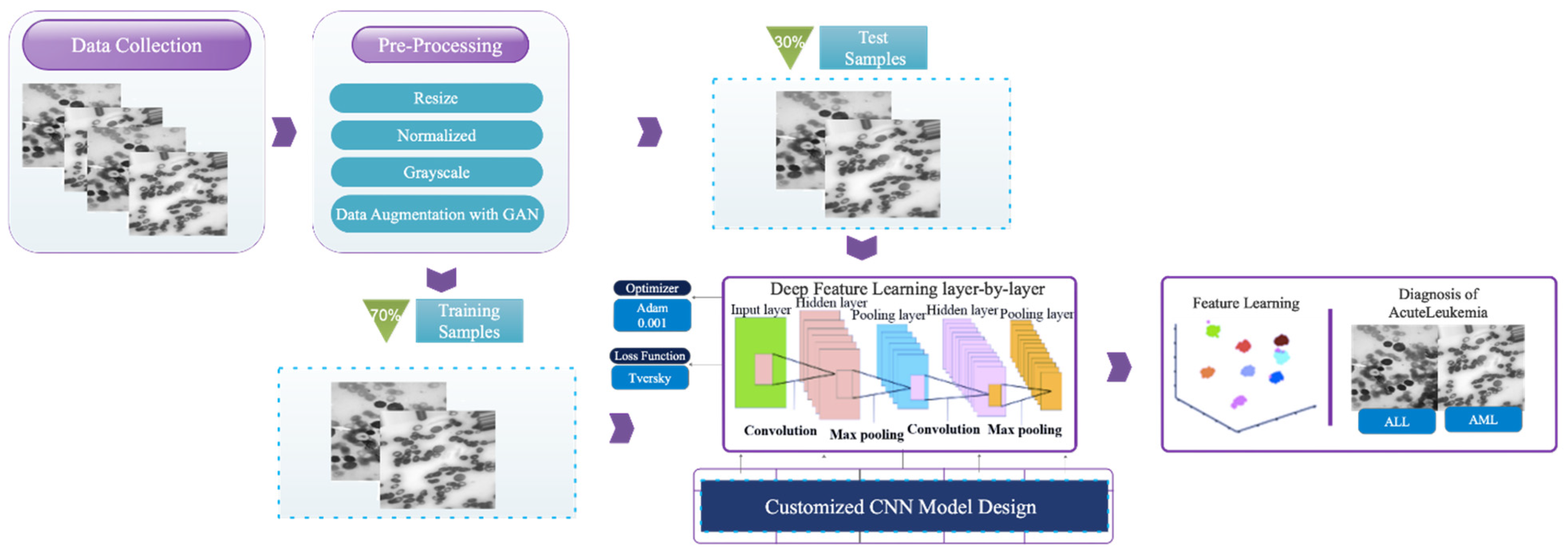
3. Proposed Framework
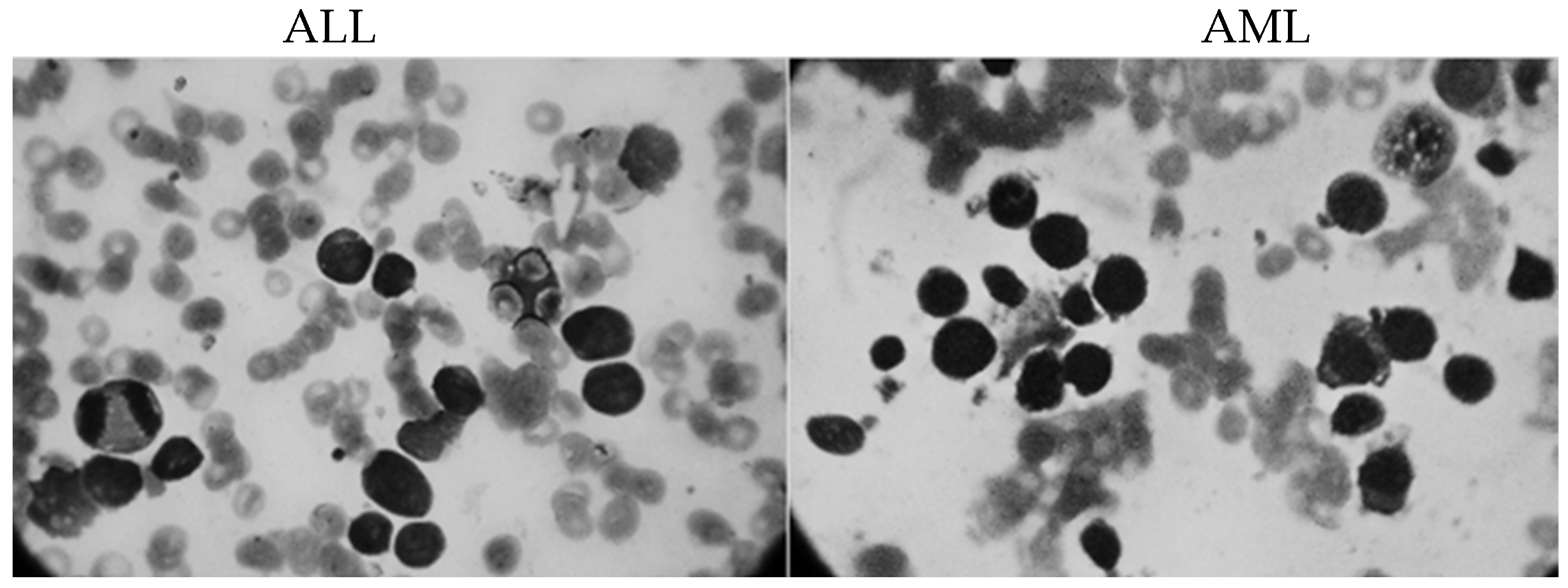
3.1. Data Collection
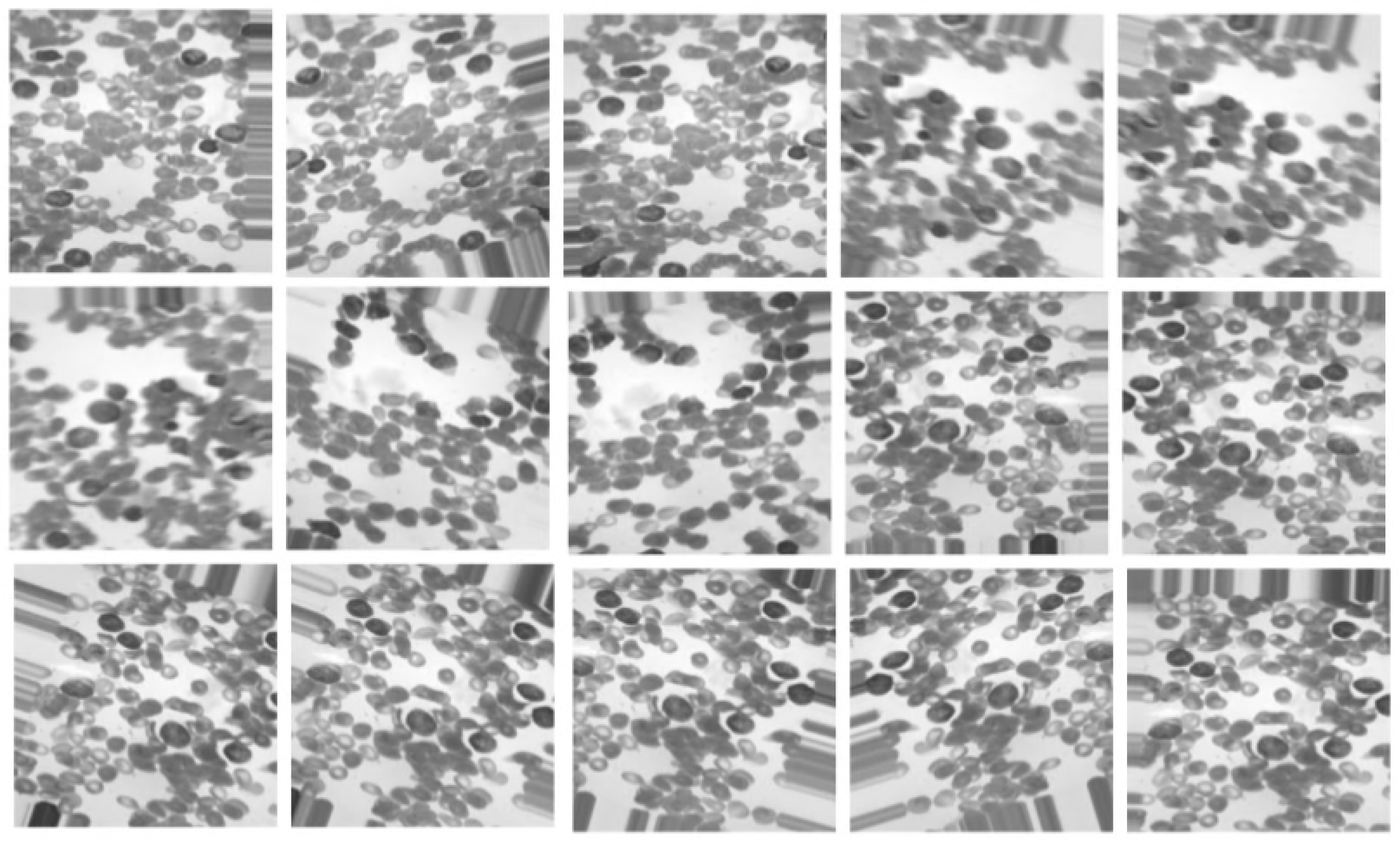
3.2. Pre-Processing
3.3. A Customized CNN Model Design
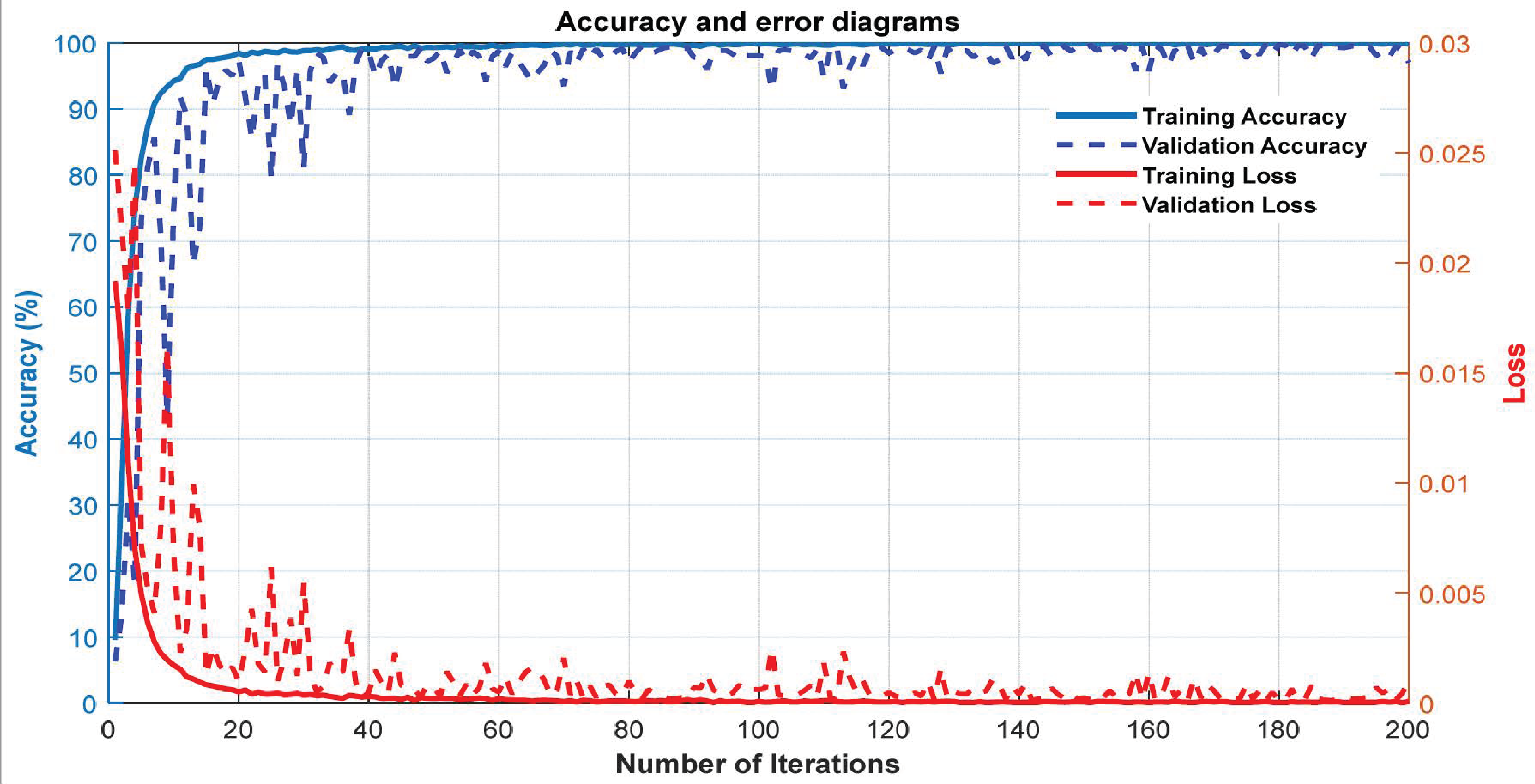
4. Experimental Results
5. Discussion
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Oskouei, V.G.; Saatlo, A.N.; Sheykhivand, S.; Farzamnia, A. In An Experimental Study: ICA-Based Sensorimotor Rhythms Detection in ALS Patients for BCI Applications. In Proceedings of the International Conference on Computer, Information Technology and Intelligent Computing (CITIC 2022), Kuala Lumpur, Malaysia, 25–27 July 2022; pp. 145–155. [Google Scholar]
- Boldú, L.; Merino, A.; Acevedo, A.; Molina, A.; Rodellar, J. A deep learning model (ALNet) for the diagnosis of acute leukaemia lineage using peripheral blood cell images. Comput. Methods Programs Biomed. 2021, 202, 105999. [Google Scholar] [CrossRef] [PubMed]
- Salah, H.T.; Muhsen, I.N.; Salama, M.E.; Owaidah, T.; Hashmi, S.K. Machine learning applications in the diagnosis of leukemia: Current trends and future directions. Int. J. Lab. Hematol. 2019, 41, 717–725. [Google Scholar] [CrossRef] [PubMed]
- El Achi, H.; Khoury, J.D. Artificial intelligence and digital microscopy applications in diagnostic hematopathology. Cancers 2020, 12, 797. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Radakovich, N.; Nagy, M.; Nazha, A. Machine learning in haematological malignancies. Lancet Haematol. 2020, 7, e541–e550. [Google Scholar] [CrossRef]
- Shouval, R.; Fein, J.A.; Savani, B.; Mohty, M.; Nagler, A. Machine learning and artificial intelligence in haematology. Br. J. Haematol. 2021, 192, 239–250. [Google Scholar] [CrossRef] [PubMed]
- Thanh, T.; Vununu, C.; Atoev, S.; Lee, S.-H.; Kwon, K.-R. Leukemia blood cell image classification using convolutional neural network. Int. J. Comput. Theory Eng. 2018, 10, 54–58. [Google Scholar] [CrossRef] [Green Version]
- Pansombut, T.; Wikaisuksakul, S.; Khongkraphan, K.; Phon-On, A. Convolutional neural networks for recognition of lymphoblast cell images. Comput. Intell. Neurosci. 2019, 2019, 7519603. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jha, K.K.; Dutta, H.S. Mutual information based hybrid model and deep learning for acute lymphocytic leukemia detection in single cell blood smear images. Comput. Methods Programs Biomed. 2019, 179, 104987. [Google Scholar] [CrossRef]
- Matek, C.; Schwarz, S.; Spiekermann, K.; Marr, C. Human-level recognition of blast cells in acute myeloid leukaemia with convolutional neural networks. Nat. Mach. Intell. 2019, 1, 538–544. [Google Scholar] [CrossRef]
- Loey, M.; Naman, M.; Zayed, H. Deep transfer learning in diagnosing leukemia in blood cells. Computers 2020, 9, 29. [Google Scholar] [CrossRef]
- Vogado, L.H.; Veras, R.M.; Araujo, F.H.; Silva, R.R.; Aires, K.R. Leukemia diagnosis in blood slides using transfer learning in CNNs and SVM for classification. Eng. Appl. Artif. Intell. 2018, 72, 415–422. [Google Scholar] [CrossRef]
- Madhloom, H.; Kareem, S.; Ariffin, H.; Zaidan, A.; Alanazi, H.; Zaidan, B. An automated white blood cell nucleus localization and segmentation using image arithmetic and automatic threshold. J. Appl. Sci. 2010, 10, 959–966. [Google Scholar] [CrossRef] [Green Version]
- Putzu, L.; Caocci, G.; Di Ruberto, C. Leucocyte classification for leukaemia detection using image processing techniques. Artif. Intell. Med. 2014, 62, 179–191. [Google Scholar] [CrossRef] [Green Version]
- Nazlibilek, S.; Karacor, D.; Ercan, T.; Sazli, M.H.; Kalender, O.; Ege, Y. Automatic segmentation, counting, size determination and classification of white blood cells. Measurement 2014, 55, 58–65. [Google Scholar] [CrossRef]
- Habibzadeh, M.; Krzyżak, A.; Fevens, T. Comparative study of shape, intensity and texture features and support vector machine for white blood cell classification. J. Theor. Appl. Comput. Sci. 2013, 7, 20–35. [Google Scholar]
- Khandekar, R.; Shastry, P.; Jaishankar, S.; Faust, O.; Sampathila, N. Automated blast cell detection for Acute Lymphoblastic Leukemia diagnosis. Biomed. Signal Process. Control 2021, 68, 102690. [Google Scholar] [CrossRef]
- Abhishek, A.; Jha, R.K.; Sinha, R.; Jha, K. Automated classification of acute leukemia on a heterogeneous dataset using machine learning and deep learning techniques. Biomed. Signal Process. Control 2022, 72, 103341. [Google Scholar] [CrossRef]
- Bibi, N.; Sikandar, M.; Ud Din, I.; Almogren, A.; Ali, S. IoMT-based automated detection and classification of leukemia using deep learning. J. Healthc. Eng. 2020, 2020, 6648574. [Google Scholar] [CrossRef]
- Rastogi, P.; Khanna, K.; Singh, V. LeuFeatx: Deep learning–based feature extractor for the diagnosis of acute leukemia from microscopic images of peripheral blood smear. Comput. Biol. Med. 2022, 142, 105236. [Google Scholar] [CrossRef]
- Dese, K.; Raj, H.; Ayana, G.; Yemane, T.; Adissu, W.; Krishnamoorthy, J.; Kwa, T. Accurate Machine-Learning-Based classification of Leukemia from Blood Smear Images. Clin. Lymphoma Myeloma Leuk. 2022, 21, e903–e914. [Google Scholar] [CrossRef]
- Chola, C.; Muaad, A.Y.; Bin Heyat, M.B.; Benifa, J.B.; Naji, W.R.; Hemachandran, K.; Mahmoud, N.F.; Samee, N.A.; Al-Antari, M.A.; Kadah, Y.M. BCNet: A Deep Learning Computer-Aided Diagnosis Framework for Human Peripheral Blood Cell Identification. Diagnostics 2022, 12, 2815. [Google Scholar] [CrossRef]
- Khaleghi, N.; Rezaii, T.Y.; Beheshti, S.; Meshgini, S.; Sheykhivand, S.; Danishvar, S. Visual Saliency and Image Reconstruction from EEG Signals via an Effective Geometric Deep Network-Based Generative Adversarial Network. Electronics 2022, 11, 3637. [Google Scholar] [CrossRef]
- Sheykhivand, S.; Yousefi Rezaii, T.; Mousavi, Z.; Meshini, S. Automatic stage scoring of single-channel sleep EEG using CEEMD of genetic algorithm and neural network. Comput. Intell. Electr. Eng. 2018, 9, 15–28. [Google Scholar]
- Sheykhivand, S.; Rezaii, T.Y.; Mousavi, Z.; Meshgini, S.; Makouei, S.; Farzamnia, A.; Danishvar, S.; Teo Tze Kin, K. Automatic Detection of Driver Fatigue Based on EEG Signals Using a Developed Deep Neural Network. Electronics 2022, 11, 2169. [Google Scholar] [CrossRef]
- Goodfellow, I.J.; Pouget-Abadie, J.; Mirza, M.; Xu, B.; Warde-Farley, D.; Ozair, S.; Courville, A.; Bengio, Y. Generative adversarial nets. In Advances in Neural Information Processing Systems; Curran: Red Hook, NY, USA, 2014; pp. 2672–2680. [Google Scholar]
- Schmidt, D.A.; Shi, C.; Berry, R.A.; Honig, M.L.; Utschick, W. Minimum mean squared error interference alignment. In Proceedings of the 2009 Forty-Third Asilomar Conference on Signals, Systems and Computers, Pacific Grove, CA, USA, 1–4 November 2009; pp. 1106–1110. [Google Scholar]
- Cortes, C.; Lawarence, N.; Lee, D.; Sugiyama, M.; Garnett, R. Advances in neural information processing systems 28. In Proceedings of the 29th Annual Conference on Neural Information Processing Systems 2015, Montreal, QC, Canada, 1–4 November 2009. [Google Scholar]
- Stefano, A.; Comelli, A. Customized efficient neural network for COVID-19 infected region identification in ct images. J. Imaging 2021, 7, 131. [Google Scholar] [CrossRef] [PubMed]
- Comelli, A.; Dahiya, N.; Stefano, A.; Vernuccio, F.; Portoghese, M.; Cutaia, G.; Bruno, A.; Salvaggio, G.; Yezzi, A. Deep learning-based methods for prostate segmentation in magnetic resonance imaging. Appl. Sci. 2021, 11, 782. [Google Scholar] [CrossRef]
- Awan, M.J.; Rahim, M.; Salim, N.; Ismail, A.; Shabbir, H. Acceleration of knee MRI cancellous bone classification on google colaboratory using convolutional neural network. Int. J. Adv. Trends Comput. Sci 2019, 8, 83–88. [Google Scholar] [CrossRef]
- Shahini, N.; Bahrami, Z.; Sheykhivand, S.; Marandi, S.; Danishvar, M.; Danishvar, S.; Roosta, Y. Automatically Identified EEG Signals of Movement Intention Based on CNN Network (End-To-End). Electronics 2022, 11, 3297. [Google Scholar] [CrossRef]
- Sheykhivand, S.; Rezaii, T.Y.; Meshgini, S.; Makoui, S.; Farzamnia, A. Developing a Deep Neural Network for Driver Fatigue Detection Using EEG Signals Based on Compressed Sensing. Sustainability 2022, 14, 2941. [Google Scholar] [CrossRef]
- Kassani, S.H.; Kassani, P.H.; Wesolowski, M.J.; Schneider, K.A.; Deters, R. A hybrid deep learning architecture for leukemic B-lymphoblast classification. In Proceedings of the 2019 International Conference on Information and Communication Technology Convergence (ICTC), Jeju, Republic of Korea, 16–18 October 2019; pp. 271–276. [Google Scholar]
- Agaian, S.; Madhukar, M.; Chronopoulos, A.T. A new acute leukaemia-automated classification system. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 2018, 6, 303–314. [Google Scholar] [CrossRef]
- Umamaheswari, D.; Geetha, S. A framework for efficient recognition and classification of acute lymphoblastic leukemia with a novel customized-KNN classifier. J. Comput. Inf. Technol. 2018, 26, 131–140. [Google Scholar] [CrossRef]
- Ahmed, N.; Yigit, A.; Isik, Z.; Alpkocak, A. Identification of leukemia subtypes from microscopic images using convolutional neural network. Diagnostics 2019, 9, 104. [Google Scholar] [CrossRef] [PubMed]
- Al-jaboriy, S.S.; Sjarif, N.N.A.; Chuprat, S.; Abduallah, W.M. Acute lymphoblastic leukemia segmentation using local pixel information. Pattern Recognit. Lett. 2019, 125, 85–90. [Google Scholar] [CrossRef]
- Patel, N.; Mishra, A. Automated leukaemia detection using microscopic images. Procedia Comput. Sci. 2015, 58, 635–642. [Google Scholar] [CrossRef] [Green Version]
- Chin Neoh, S.; Srisukkham, W.; Zhang, L.; Todryk, S.; Greystoke, B.; Peng Lim, C.; Alamgir Hossain, M.; Aslam, N. An intelligent decision support system for leukaemia diagnosis using microscopic blood images. Sci. Rep. 2015, 5, 14938. [Google Scholar] [CrossRef] [Green Version]
- Begum, A.J.; Razak, T.A. Diagnosing Leukemia from Microscopic Images Using Image Analysis and Processing Techniques. In Proceedings of the 2017 World Congress on Computing and Communication Technologies (WCCCT), Tiruchirappalli, India, 2–4 February 2017; pp. 227–230. [Google Scholar]
- Fakhouri, H.N.; Al-Sharaeh, S.H. A hybrid methodology for automation the diagnosis of leukemia based on quantitative and morphological feature analysis. Mod. Appl. Sci. 2018, 12, 56–73. [Google Scholar] [CrossRef] [Green Version]
- Rodellar, J.; Alférez, S.; Acevedo, A.; Molina, A.; Merino, A. Image processing and machine learning in the morphological analysis of blood cells. Int. J. Lab. Hematol. 2018, 40, 46–53. [Google Scholar] [CrossRef] [Green Version]
- Chollet, F. Xception: Deep learning with depthwise separable convolutions. In Proceedings of the IEEE Conference on computer Vision and Pattern Recognition, Honolulu, HI, USA, 21–26 July 2017; pp. 1251–1258. [Google Scholar]
- Carvalho, T.; De Rezende, E.R.; Alves, M.T.; Balieiro, F.K.; Sovat, R.B. Exposing computer generated images by eye’s region classification via transfer learning of VGG19 CNN. In Proceedings of the 2017 16th IEEE International Conference on Machine Learning and Applications (ICMLA), Cancun, Mexico, 18–21 December 2017; pp. 866–870. [Google Scholar]
- Tang, C.; Liu, X.; Zheng, X.; Li, W.; Xiong, J.; Wang, L.; Zomaya, A.Y.; Longo, A. DeFusionNET: Defocus blur detection via recurrently fusing and refining discriminative multi-scale deep features. IEEE Trans. Pattern Anal. Mach. Intell. 2020, 44, 955–968. [Google Scholar] [CrossRef]
- Theckedath, D.; Sedamkar, R. Detecting affect states using VGG16, ResNet50 and SE-ResNet50 networks. SN Comput. Sci. 2020, 1, 79. [Google Scholar] [CrossRef]


















{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| L | Layer Type | Activation Function | Output Shape | Size of Filter and Pooling | Strides | Number of Filters | Adding |
|---|---|---|---|---|---|---|---|
| 0–1 | Convolution2-D | Leaky ReLU | (None, 20, 112,112) | 5 × 5 | 2 | 20 | yes |
| 1–2 | Max-Pooling2-D | - | (None, 20, 56,56) | 2 × 2 | 2 | - | no |
| 2–3 | Convolution2-D | Leaky ReLU | (None, 20,56,56) | 5 × 5 | 1 | 20 | yes |
| 3–4 | Max-Pooling2-D | - | (None, 20, 28, 28) | 2 × 2 | 2 | - | no |
| 4–5 | Convolution2-D | Leaky ReLU | (None, 20, 28, 28) | 5 × 5 | 1 | 20 | yes |
| 5–6 | Max-Pooling2-D | - | (None, 20, 14, 14) | 2 × 2 | 2 | - | no |
| 6–7 | Convolution2-D | Leaky ReLU | (None, 20, 14, 14) | 5 × 5 | 1 | 20 | yes |
| 7–8 | Max-Pooling2-D | - | (None, 20, 7, 7) | 2 × 2 | 2 | - | no |
| 8–9 | Convolution2-D | Leaky ReLU | (None, 20, 7, 7) | 5 × 5 | 1 | 20 | yes |
| 9–10 | Max-Pooling2-D | (None, 20, 3, 3) | 2 × 2 | 2 | - | no | |
| 10–11 | Convolution2-D | Leaky ReLU | (None, 20, 3, 3) | 5 × 5 | 1 | 20 | yes |
| 11–12 | Flatten | - | (None, 180) | - | - | - | - |
| 12–13 | FC | Leaky ReLU | (None, 1024) | - | - | - | - |
| 13–14 | FC | Leaky ReLU | (None, 512) | - | - | - | - |
| 14–15 | FC | Leaky ReLU | (None, 128) | - | - | - | - |
| 15–16 | FC | Softmax | (None, 2) | - | - | - | - |
| References | Dataset | Classification | Methods | Accuracy |
|---|---|---|---|---|
| Putzu [14] | ALL-IDB1 | ALL | Image Processing | 92% |
| Kassanin et al. [34] | ISBI | Healthy and ALL | Customized CNN | 96.17% |
| Agaian et al. [35] | ALL-IDB1 | ALL | Cell Energy Feature with Support Vector Machine | 94% |
| Umamaheswari et al. [36] | ALL-IDB2 | ALL | Customized K-Nearest Neighbor | 96.25% |
| Ahmed et al. [37] | ALL-IDB, ASH Image Bank | Leukemia Subtypes Classification | CNN | 81.74% |
| Al-jaboriy et al. [38] | ALL-IDB1 | ALL | Genetic Algorithm and ANN | 97.07% |
| Nimesh patel et al. [39] | ALL-IDB1 | ALL | SVM | 93.57 |
| Siew chin neoh et al. [40] | ALL-IDB | ALL | SVM and MLP | 96.72 |
| Begum et al. [41] | Not revealed | Leukemia | SVM | Not revealed |
| Fakhouri et al. [42] | Online dataset | Leukemia types | SVM | Not revealed |
| Rdellar et al. [43] | Private dataset | Leukemia types | SVM | 90.3% |
| Chola et al. [22] | HPBC | Leukemia types | BCNet | 98.51%% |
| Rastogi et al. [20] | ALL-IDB2 | ALL-AML | LeuFeatx | 96.15% |
| Proposed Method | Private (ALL-AML) | ALL-AML | Customized CNN | 99.5% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ansari, S.; Navin, A.H.; Sangar, A.B.; Gharamaleki, J.V.; Danishvar, S. A Customized Efficient Deep Learning Model for the Diagnosis of Acute Leukemia Cells Based on Lymphocyte and Monocyte Images. Electronics 2023, 12, 322. https://doi.org/10.3390/electronics12020322
Ansari S, Navin AH, Sangar AB, Gharamaleki JV, Danishvar S. A Customized Efficient Deep Learning Model for the Diagnosis of Acute Leukemia Cells Based on Lymphocyte and Monocyte Images. Electronics. 2023; 12(2):322. https://doi.org/10.3390/electronics12020322
Chicago/Turabian StyleAnsari, Sanam, Ahmad Habibizad Navin, Amin Babazadeh Sangar, Jalil Vaez Gharamaleki, and Sebelan Danishvar. 2023. "A Customized Efficient Deep Learning Model for the Diagnosis of Acute Leukemia Cells Based on Lymphocyte and Monocyte Images" Electronics 12, no. 2: 322. https://doi.org/10.3390/electronics12020322