
Three-Dimensional Point Cloud Reconstruction Method of Cardiac Soft Tissue Based on Binocular Endoscopic Images


Abstract
:1. Introduction
2. Related Work
2.1. Binocular Stereo Vision Camera Calibration
2.2. Stereo Endoscope Vision and 3D Reconstruction
3. Dataset
4. Method
4.1. Joint Calibration Algorithm
4.2. Binocular Endoscope Image Matching Algorithm
- (1)
- Construct new left and right images. The gray values of all pixels corresponding to each color channel are 0. That is, a 0 matrix of is constructed.
- (2)
- Use internal parameter matrices of the two endoscopes obtained from the calibration to construct a standard internal parameter matrix . Moreover, use the obtained internal parameters to backproject the pixel coordinates to the corresponding endoscope coordinate system, as shown in Equation (7).
- (3)
- Employ the acquired external parameters to derive the rotation matrix pertaining to the coordinate systems of the two endoscopes. Subsequently, the coordinates of the identified points in the two endoscopic systems are inversely rotated, yielding their original coordinates in the two endoscopic coordinate systems. Use and to multiply the resulting coordinate points to the left. Then take the corresponding value of the -axis as the reference object and normalize its coordinate value.
- (4)
- Substitute the calibrated distortion coefficients of the two endoscopes and the coordinate values obtained in the previous step into the distortion model. Obtain X and Y-axis components when there is non-linear distortion.
- (5)
- Combine the results obtained in the previous step. The inherent internal parameters of both endoscopes are utilized to calculate the pixel coordinates of the corresponding points in the original images.
- (6)
- Use the bilinear interpolation algorithm and the obtained color values of the four pixels around the pixel coordinates in both original images to interpolate the corresponding pixels in the new images. When the interpolation of all pixels is completed, both corrected images are obtained.
4.3. Three-Dimensional Reconstruction of Spatial Points
4.4. Point Cloud Surface Reconstruction
4.4.1. Preprocessing of Point Cloud Data
4.4.2. Surface Reconstruction
- (1)
- Judge whether the cardinality of the set exceeds the predefined threshold. If the cardinality exceeds the threshold, divide it into two subsets, and then execute steps (2) and (3). If it is less than the set threshold, execute step (4).
- (2)
- Combine the two subsets separately.
- (3)
- Merge the subdivision results of the two subsets and execute step (5).
- (4)
- Execute the incremental algorithm to obtain the subdivision results.
- (5)
- Return the subdivision result.
5. Experiment and Results
5.1. Endoscope Parameter Calibration
- (1)
- Obtain the template image: position the calibration template before the binocular camera and rotate the calibration template. During each rotation of the calibration template, both cameras simultaneously take pictures. Part of the image obtained with the left camera is shown in Figure 7a.
- (2)
- Corner coordinate acquisition: considering that the edge part of the checkerboard calibration template is blurred due to the printing quality, the corner points of the edge part are discarded. Four points are manually selected (A, B, C, D). The straight line formed by the 11 corner points closest to the connecting line A and B is the X axis, and the straight line formed by the 7 corner points closest to the connecting line A and D is the Y axis. Then the Harris corner detection algorithm extracts the corner points’ pixel coordinates in the area surrounded by the connecting line between these points, as shown in Figure 7b. The corner points are extracted locally and displayed magnified. Human beings observe the presence of errors, and the corners with errors are corrected artificially.
- (3)
- Setting up the world coordinate system: for all template images, the corner points in the top left corner are chosen as the reference origin of the world coordinate system. The first row of corner points, both horizontally and vertically, represent the X-axis and Y-axis. All corner points are on the plane, so it is possible to derive all corner points’ coordinates. The coordinates of all corners on the template are consistent in different world coordinate systems.
- (4)
- Following the aforementioned monocular calibration approach, the individual calibration operations for the left and right cameras are successfully conducted. The resulting calibration parameters for both cameras are provided in Table 2.
- (5)
- Using the external parameters for both cameras obtained in the previous step, as presented in Table 3, the external parameters of the binocular camera system are accessed employing the prescribed solution. Consequently, the calibration process is concluded.
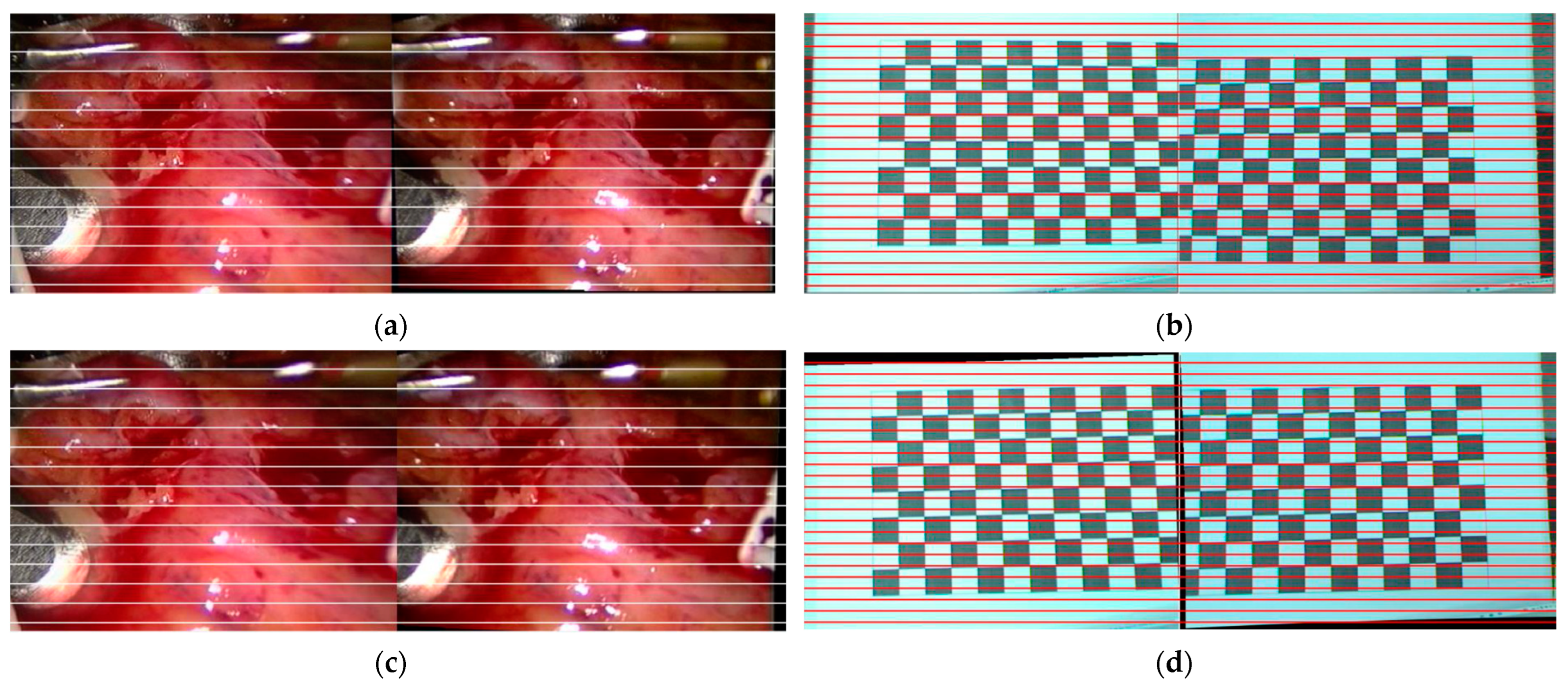
5.2. Binocular Endoscope Image Matching
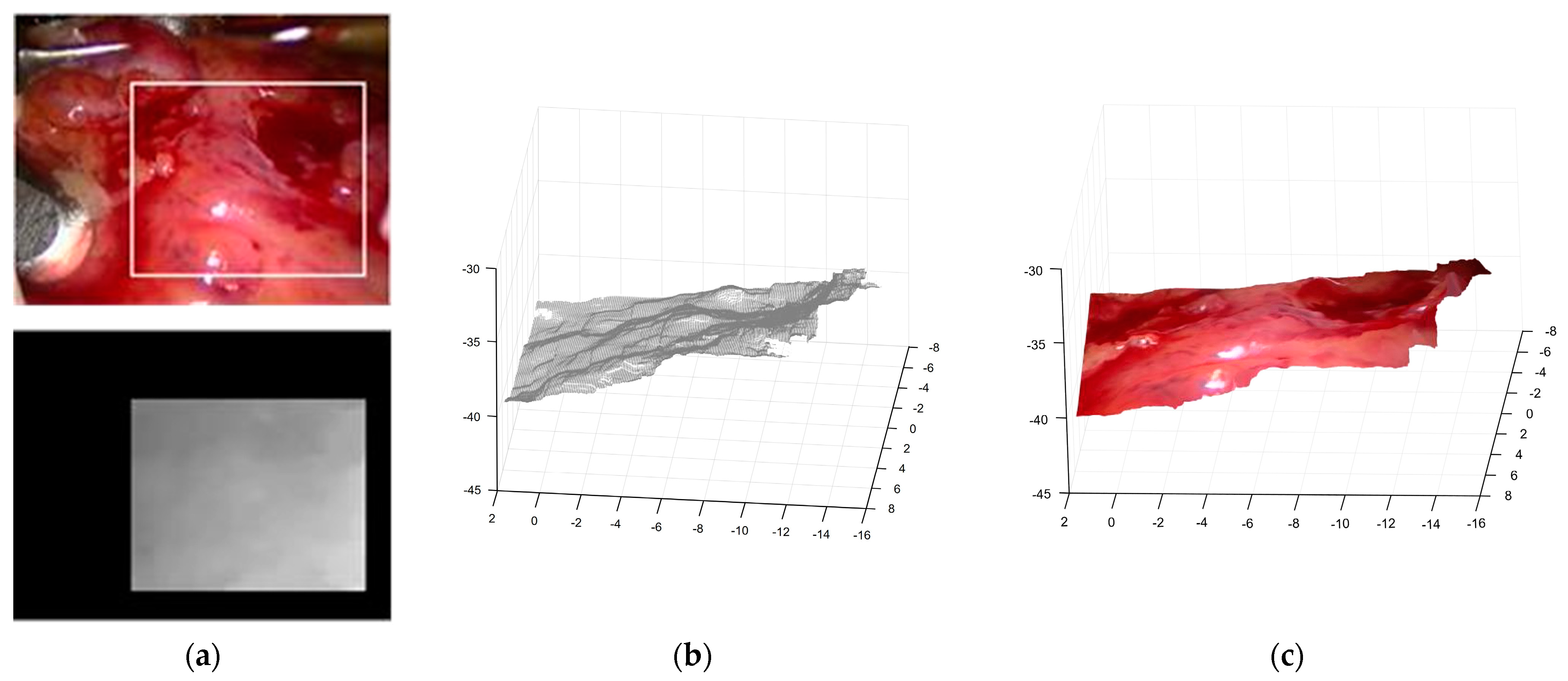
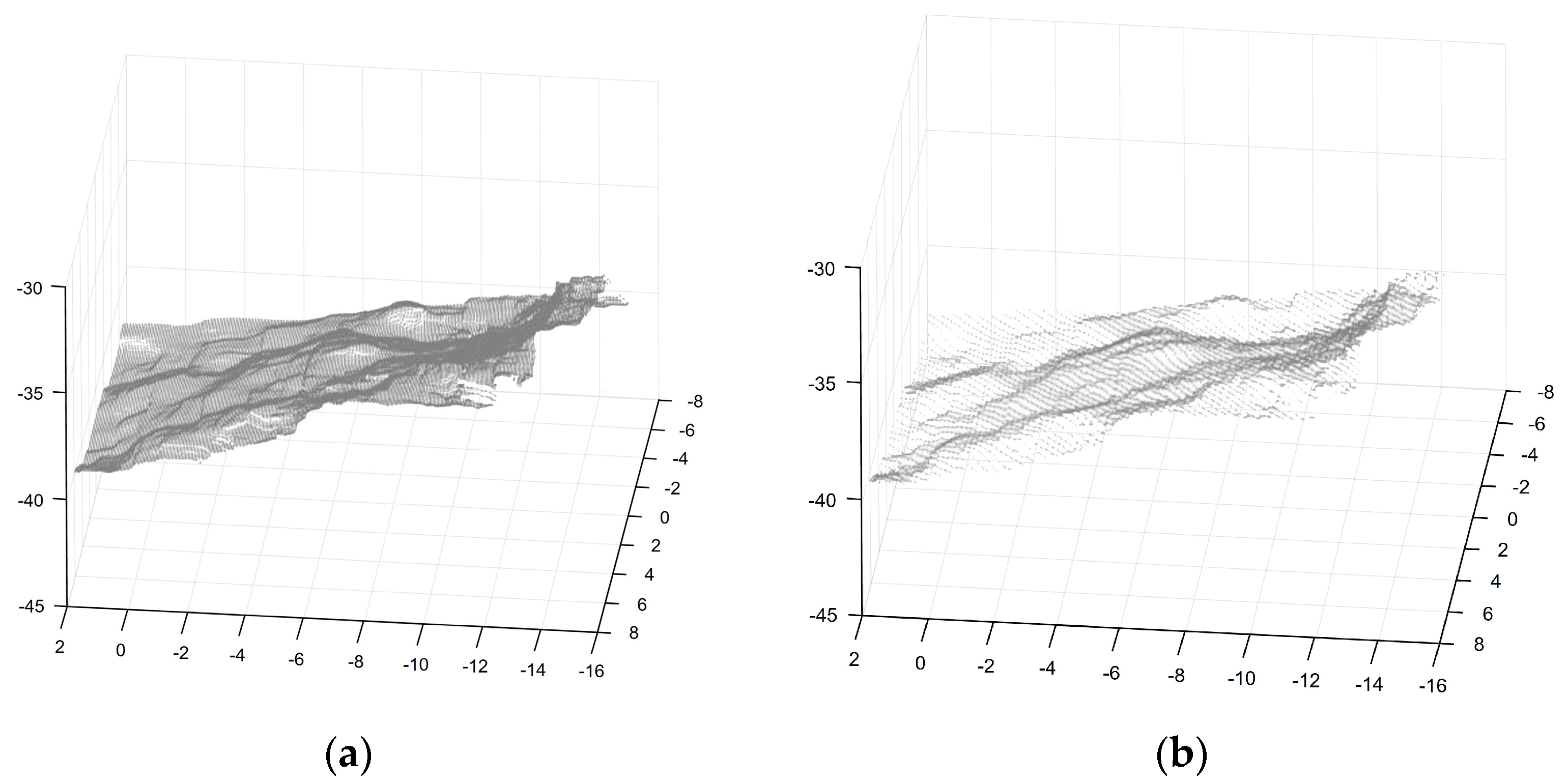
5.3. Three-Dimensional Reconstruction of Cardiac Soft Tissue Surface
6. Discussion
7. Conclusions
Author Contributions
Funding
Data Availability Statement
Conflicts of Interest
References
- Marr, D.; Poggio, T.; Hildreth, E.C.; Grimson, W.E.L. A computational theory of human stereo vision. In From the Retina to the Neocortex: Selected Papers of David Marr; Vaina, L., Ed.; Birkhäuser Boston: Boston, MA, USA, 1991; pp. 263–295. [Google Scholar] [CrossRef]
- Ji, Y.; Li, Y.; Sun, X.; Yan, S.; Guo, N. Stereo matching algorithm based on binocular vision. In Proceedings of the 2020 7th International Forum on Electrical Engineering and Automation (IFEEA), Hefei, China, 25–27 September 2020; pp. 843–847. [Google Scholar] [CrossRef]
- Lu, S.; Yang, J.; Yang, B.; Yin, Z.; Liu, M.; Yin, L.; Zheng, W. Analysis and Design of Surgical Instrument Localization Algorithm. Comput. Model. Eng. Sci. 2023, 137, 669–685. [Google Scholar] [CrossRef]
- Zhang, Y.-J. Camera calibration. In 3-D Computer Vision: Principles, Algorithms and Applications; Springer: Berlin/Heidelberg, Germany, 2023; pp. 37–65. [Google Scholar] [CrossRef]
- Tang, Y.; Liu, S.; Deng, Y.; Zhang, Y.; Yin, L.; Zheng, W. An improved method for soft tissue modeling. Biomed. Signal Process. Control. 2021, 65, 102367. [Google Scholar] [CrossRef]
- Dang, W.; Xiang, L.; Liu, S.; Yang, B.; Liu, M.; Yin, Z.; Yin, L.; Zheng, W. A Feature Matching Method based on the Convolutional Neural Network. J. Imaging Sci. Technol. 2023, 67, 1–11. [Google Scholar] [CrossRef]
- Lu, S.; Liu, S.; Hou, P.; Yang, B.; Liu, M.; Yin, L.; Zheng, W. Soft Tissue Feature Tracking Based on DeepMatching Network. CMES Comput. Model. Eng. Sci. 2023, 136, 363–379. [Google Scholar]
- Han, R.; Yan, H.; Ma, L. Research on 3D Reconstruction methods Based on Binocular Structured Light Vision. J. Phys. Conf. Ser. 2021, 1744, 032002. [Google Scholar] [CrossRef]
- Liu, X.; Zheng, W.; Mou, Y.; Li, Y.; Yin, L. Microscopic 3D reconstruction based on point cloud data generated using defocused images. Meas. Control. 2021, 54, 1309–1318. [Google Scholar] [CrossRef]
- Zhu, J.; Lyu, L.; Xu, Y.; Liang, H.; Zhang, X.; Ding, H.; Wu, Z. Intelligent Soft Surgical Robots for Next-Generation Minimally Invasive Surgery. Adv. Intell. Syst. 2021, 3, 2100011. [Google Scholar] [CrossRef]
- Hardner, M.; Docea, R.; Schneider, D. Guided Calibration of Medical Stereo Endoscopes. Int. Arch. Photogramm. Remote Sens. Spatial Inf. Sci. 2022, XLIII-B2-2022, 679–686. [Google Scholar] [CrossRef]
- Edwards, P.J.E.; Psychogyios, D.; Speidel, S.; Maier-Hein, L.; Stoyanov, D. SERV-CT: A disparity dataset from cone-beam CT for validation of endoscopic 3D reconstruction. Med. Image Anal. 2022, 76, 102302. [Google Scholar] [CrossRef]
- Huo, J.; Zhou, C.; Yuan, B.; Yang, Q.; Wang, L. Real-Time Dense Reconstruction with Binocular Endoscopy Based on StereoNet and ORB-SLAM. Sensors 2023, 23, 2074. [Google Scholar] [CrossRef]
- Davies, M.; Stuart, M.B.; Hobbs, M.J.; McGonigle, A.J.; Willmott, J.R. Image correction and In situ spectral calibration for low-cost, smartphone hyperspectral imaging. Remote Sens. 2022, 14, 1152. [Google Scholar] [CrossRef]
- Suganyadevi, S.; Seethalakshmi, V.; Balasamy, K. A review on deep learning in medical image analysis. Int. J. Multimed. Inf. Retr. 2022, 11, 19–38. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z. A flexible new technique for camera calibration. IEEE Trans. Pattern Anal. Mach. Intell. 2000, 22, 1330–1334. [Google Scholar] [CrossRef]
- Lü, X.; Meng, L.; Long, L.; Wang, P. Comprehensive improvement of camera calibration based on mutation particle swarm optimization. Measurement 2022, 187, 110303. [Google Scholar] [CrossRef]
- Miyawaki, T.; Endo, K. Optical path length self-calibration method based on form measured surface data. Precis. Eng. 2022, 77, 360–364. [Google Scholar] [CrossRef]
- Barone, F.; Marrazzo, M.; Oton, C.J. Camera calibration with weighted direct linear transformation and anisotropic uncertainties of image control points. Sensors 2020, 20, 1175. [Google Scholar] [CrossRef]
- Kwon, Y.-H. A non-linear camera calibration algorithm: Direct Solution Method. In Proceedings of the ISBS-Conference Proceedings Archive, Beijing, China, 22–27 August 2005; p. 142. [Google Scholar]
- Gee, T.; Delmas, P.; Stones-Havas, N.; Sinclair, C.; Mark, W.V.D.; Li, W.; Friedrich, H.; Gimel’farb, G. Tsai camera calibration enhanced. In Proceedings of the 2015 14th IAPR International Conference on Machine Vision Applications (MVA), Tokyo, Japan, 18–22 May 2015; pp. 435–438. [Google Scholar] [CrossRef]
- Kumar, A.; Wang, Y.-Y.; Wu, C.-J.; Liu, K.-C.; Wu, H.-S. Stereoscopic visualization of laparoscope image using depth information from 3D model. Comput. Methods Programs Biomed. 2014, 113, 862–868. [Google Scholar] [CrossRef]
- Luo, H.; Yin, D.; Zhang, S.; Xiao, D.; He, B.; Meng, F.; Zhang, Y.; Cai, W.; He, S.; Zhang, W.; et al. Augmented reality navigation for liver resection with a stereoscopic laparoscope. Comput. Methods Programs Biomed. 2020, 187, 105099. [Google Scholar] [CrossRef]
- Wang, Y.; Long, Y.; Fan, S.H.; Dou, Q. Neural Rendering for Stereo 3D Reconstruction of Deformable Tissues in Robotic Surgery. In Proceedings of the Medical Image Computing and Computer Assisted Intervention—MICCAI 2022, Singapore, 18–22 September 2022; pp. 431–441. [Google Scholar] [CrossRef]
- Zicheng, L.; He, Y.; Hongya, W.; Liang, C.; Quan, Z. Research Progress in 3D-reconstruction Based Imaging Analysis in Partial Solid Pulmonary Nodule. Chin. J. Lung Cancer 2022, 25, 124–129. [Google Scholar]
- Wu, Z.; Guo, W.; Chen, Z.; Wang, H.; Li, X.; Zhang, Q. Three-dimensional shape and deformation measurement on complex structure parts. Sci. Rep. 2022, 12, 7760. [Google Scholar] [CrossRef]
- Zenteno, O.; Trinh, D.-H.; Treuillet, S.; Lucas, Y.; Bazin, T.; Lamarque, D.; Daul, C. Optical biopsy mapping on endoscopic image mosaics with a marker-free probe. Comput. Biol. Med. 2022, 143, 105234. [Google Scholar] [CrossRef] [PubMed]
- Bao, J.; Jing, J.; Zhang, W.; Liu, C.; Gao, T. A corner detection method based on adaptive multi-directional anisotropic diffusion. Multimed. Tools Appl. 2022, 81, 28729–28754. [Google Scholar] [CrossRef]
- Han, Z.; Zhang, L. Modeling and Calibration of a Galvanometer-Camera Imaging System. IEEE Trans. Instrum. Meas. 2022, 71, 1–9. [Google Scholar] [CrossRef]
- Xuechun, W.; Liang, W.; Fuqing, D. Calibration for light field cameras based on fixed point constraint of spatial plane homography. Opt. Express 2022, 30, 24968–24983. [Google Scholar] [CrossRef]
- Lang, J.; Mao, J.; Liang, R. Non-horizontal target measurement method based on monocular vision. Syst. Sci. Control. Eng. 2022, 10, 443–458. [Google Scholar] [CrossRef]
- Wang, D.; Hu, L.-L. Improved Feature Stereo Matching Method Based on Binocular Vision. Acta Electonica Sin. 2022, 50, 157. [Google Scholar] [CrossRef]
- Mehedi, I.M.; Rao, K.P.; Alotaibi, F.M.; Alkanfery, H.M. Intelligent Wireless Capsule Endoscopy for the Diagnosis of Gastrointestinal Diseases. Diagnostics 2023, 13, 1445. [Google Scholar] [CrossRef]
- Boese, A.; Wex, C.; Croner, R.; Liehr, U.B.; Wendler, J.J.; Weigt, J.; Walles, T.; Vorwerk, U.; Lohmann, C.H.; Friebe, M.; et al. Endoscopic Imaging Technology Today. Diagnostics 2022, 12, 1262. [Google Scholar] [CrossRef]
- Xi, L.; Zhao, Y.; Chen, L.; Gao, Q.H.; Tang, W.; Wan, T.R.; Xue, T. Recovering dense 3D point clouds from single endoscopic image. Comput. Methods Programs Biomed. 2021, 205, 106077. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Parameter | Expression |
|---|---|
| Right and left parameter matrix | |
| Radial distortion and tangential distortion | |
| External parameters (rotation matrix and translation vector) |
| Parameter | Left Camera | Right Camera |
|---|---|---|
| Focal length ] | [911.7311, 912.0249] | [911.5704, 911.5454] |
| Principal point | (337.9437, 251.4144) | (326.3726, 280.5231) |
| Non-vertical factor γ | 0.4986 | −0.3069 |
| Distortion coefficient k | [−0.1062, 0.1594, −5.2870 × 10−4, 8.6057 × 10−4] | [−0.0990, 0.1218, −7.0641 × 10−4, 4.7172 × 10−4] |
| Parameter | Result |
|---|---|
| Rotation matrix R | |
| Translation vector T |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Tian, J.; Ma, B.; Lu, S.; Yang, B.; Liu, S.; Yin, Z. Three-Dimensional Point Cloud Reconstruction Method of Cardiac Soft Tissue Based on Binocular Endoscopic Images. Electronics 2023, 12, 3799. https://doi.org/10.3390/electronics12183799
Tian J, Ma B, Lu S, Yang B, Liu S, Yin Z. Three-Dimensional Point Cloud Reconstruction Method of Cardiac Soft Tissue Based on Binocular Endoscopic Images. Electronics. 2023; 12(18):3799. https://doi.org/10.3390/electronics12183799
Chicago/Turabian StyleTian, Jiawei, Botao Ma, Siyu Lu, Bo Yang, Shan Liu, and Zhengtong Yin. 2023. "Three-Dimensional Point Cloud Reconstruction Method of Cardiac Soft Tissue Based on Binocular Endoscopic Images" Electronics 12, no. 18: 3799. https://doi.org/10.3390/electronics12183799