

Development and Testing of a Miniaturized Platform for Photoplethysmography




Abstract
:1. Introduction
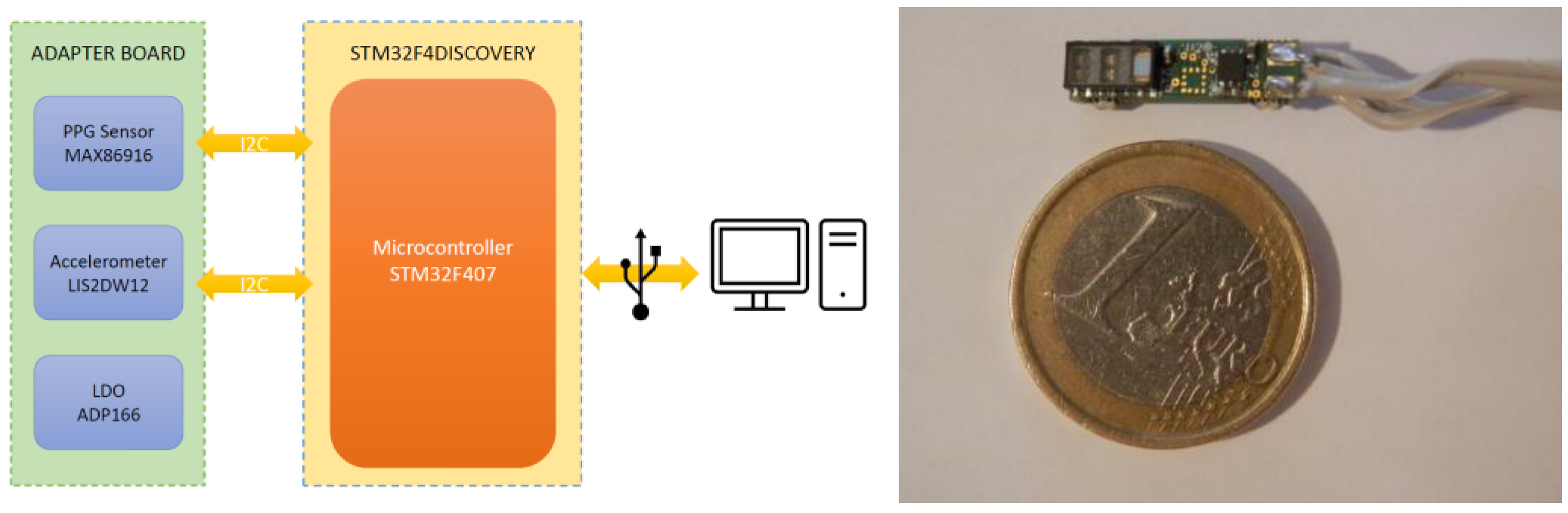
2. System Description
2.1. Hardware
- LED supply current
- LED pulse width
- Integration time of the ADC
- ADC full-scale range
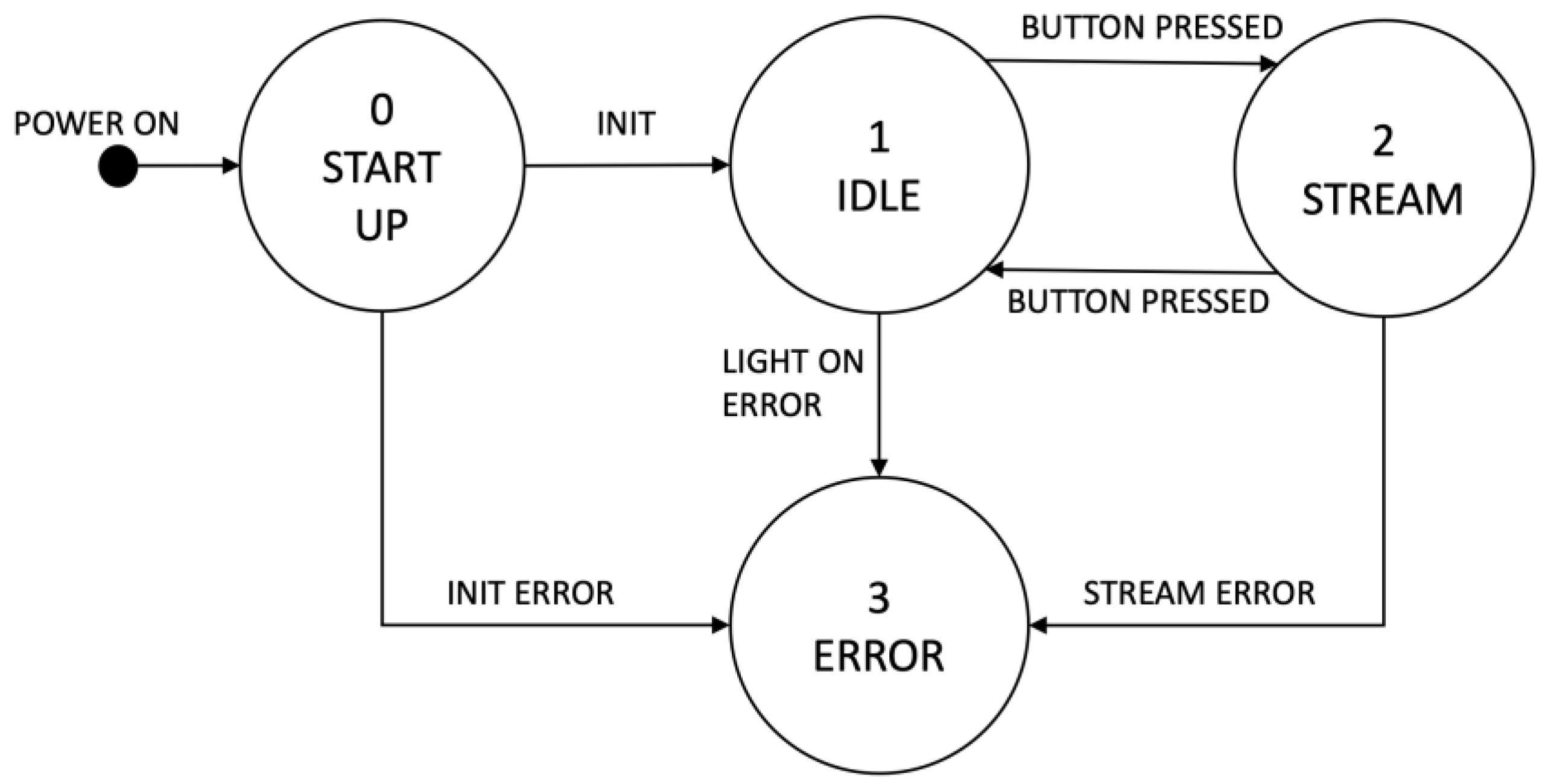
2.2. Firmware
- Start-up: the system initialization is performed in this state. The I2C, USB peripherals and GPIO pins required for operation are configured. Subsequently, the PPG sensor on the adapter board is checked to verify communication. If an error is identified, the system moves into the Error state. At the end of the start-up, the system moves to the Idle state.
- Idle: the system waits for the USER button to be pressed. This action generates an interrupt for the microcontroller, which turns on the PPG sensor and moves the system into the Stream state.
- Stream: in this state, the system acquires data from the PPG sensor and transmits them to a PC connected via the USB interface. These two operations (reading and sending data) are performed periodically thanks to an interrupt which is triggered every 10 ms. Therefore, the data frequency is 100 Hz. If an error occurs in the I2C or in the USB communication, the system moves into the Error state.
- Error: in this state all operations are disabled and the only way to recover the sensor is to reset the board.

3. System Characterization
3.1. Signal Quality Indexes
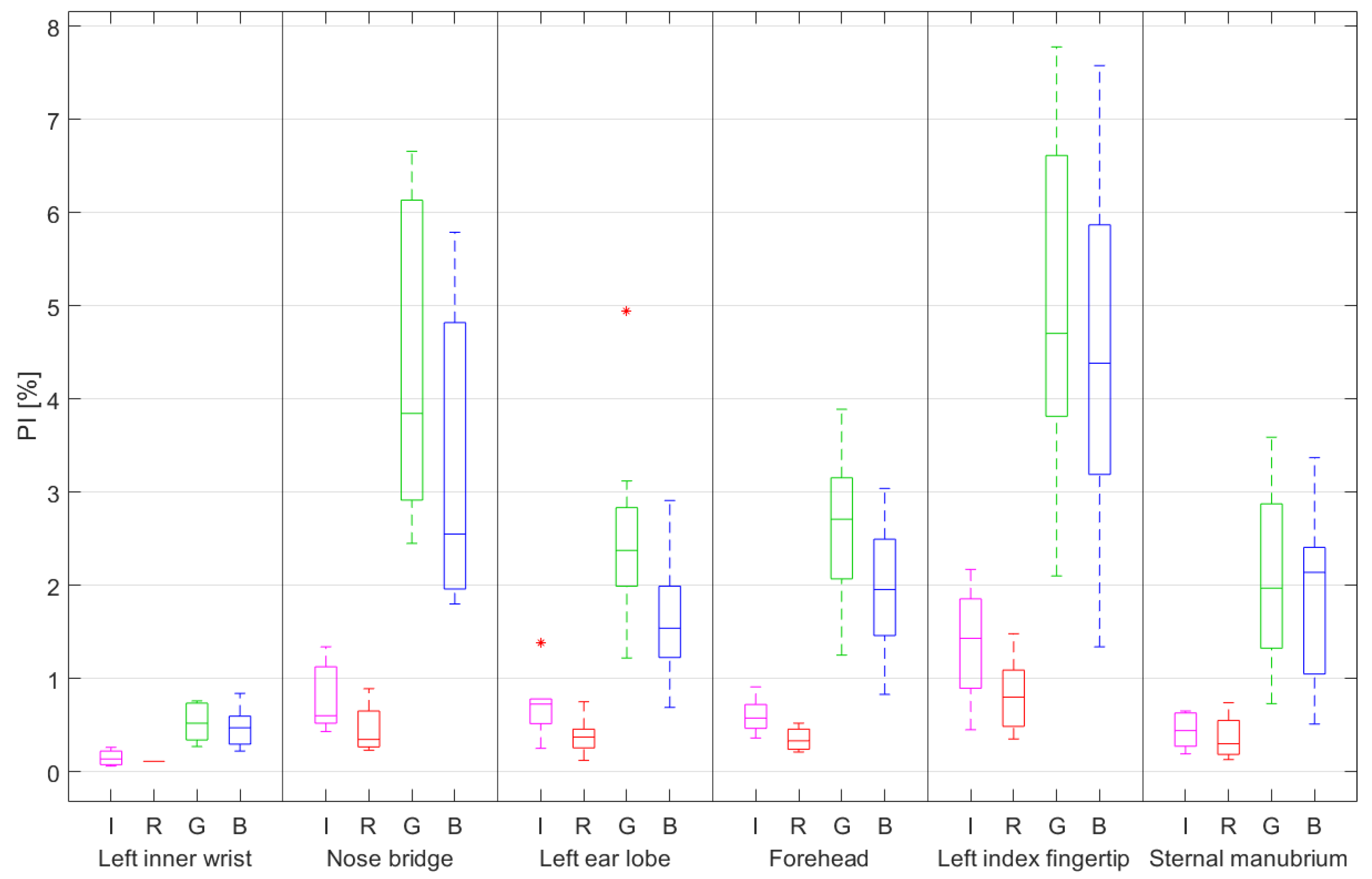
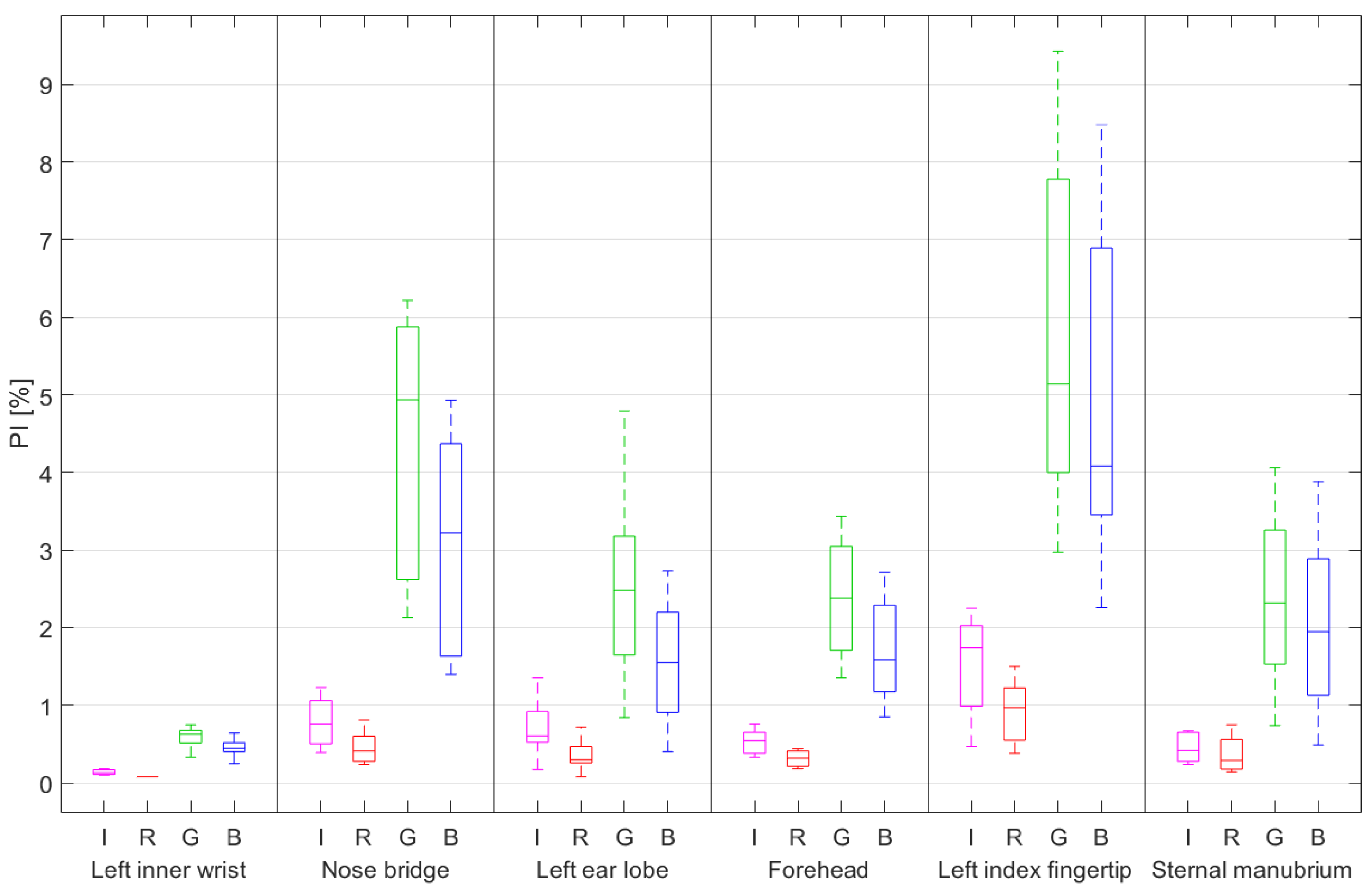
- Perfusion Index (PI): is probably the most-used signal quality index for evaluating the quality of PPG signals. The perfusion index is the ratio of the pulsatile component of the blood to the static component. It is defined as:
- Skewness: is a statistical measure of the symmetry of a distribution density. It is defined as:
- Kurtosis: is a statistical measure used to describe the distribution of observed data around the mean. It provides information about the queues of a distribution and is defined as follows:
- Signal-to-Noise ratio (SNR): is a measure that compares the signal level with that of the background noise. There are different methods to define this metric. One possible definition is based on the comparison of the signal’s variance and the noise’s variance:
- Entropy: identifies how much the probability density of the signal differs from the uniform distribution and is defined as:
- Relative power: is a measurement in the frequency domain. Since most of the systolic and diastolic wave energy is concentrated in the frequency range 1–2.25 Hz, the ratio between the power spectral density (PSD) in this band and that of the entire signal (0–8 Hz) provides a measure of the quality of the acquisition. It is defined as:
3.2. Measurement Protocol
- Fix the adapter board on the measurement site, with the subject in a stable position and at rest. For all the body locations an adhesive medical tape was used to hold the adapter board in place.
- Turn on the PPG module, waiting at least 10 s for stabilization of the PPG signal.
- Start recording for 60 s.
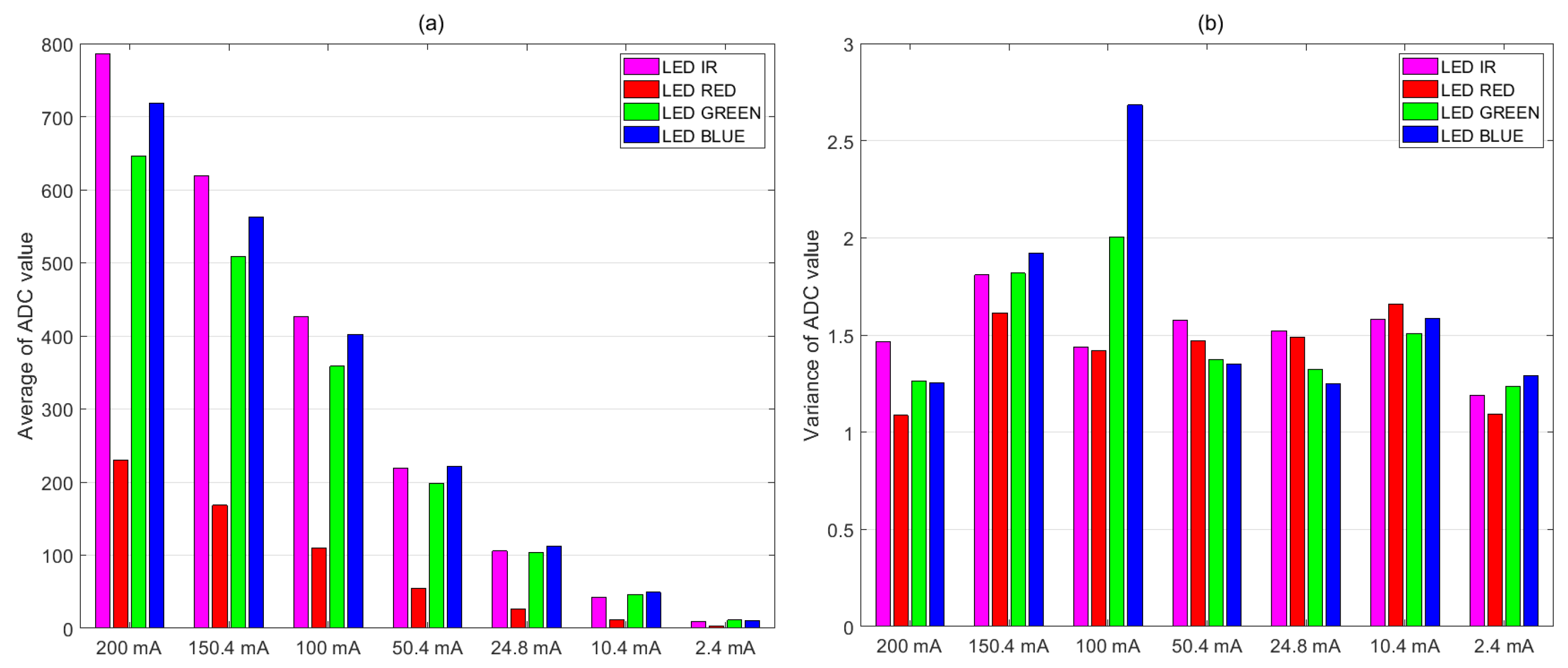
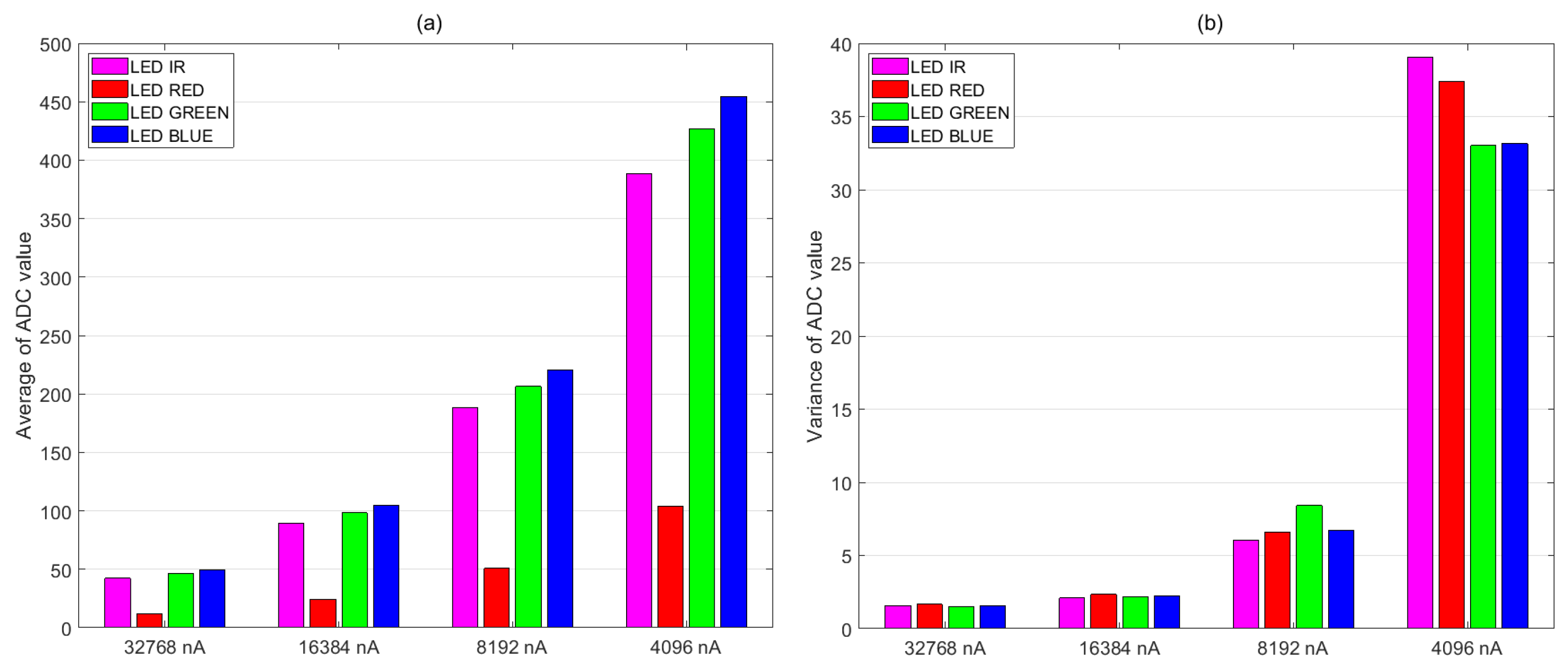
3.3. Optimization of the PPG Sensor Settings
- Supply current of the LEDs.
- Full-scale value of the ADC.
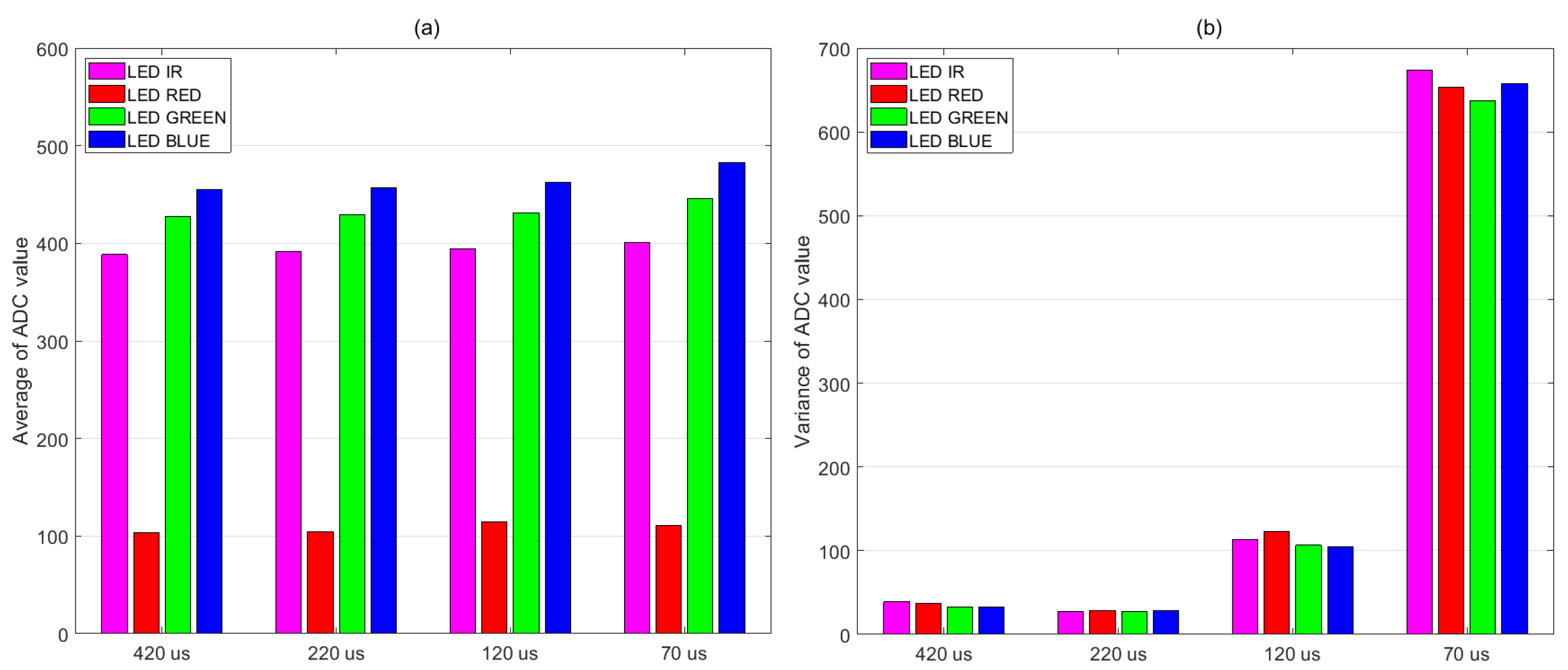
- LED pulse width and ADC integration time.
3.4. Measurement Location
- Forehead
- Left ear lobe
- Left index fingertip
- Left inner wrist
- Sternal manubrium
- Nose bridge
4. Discussion of the Measurement Results
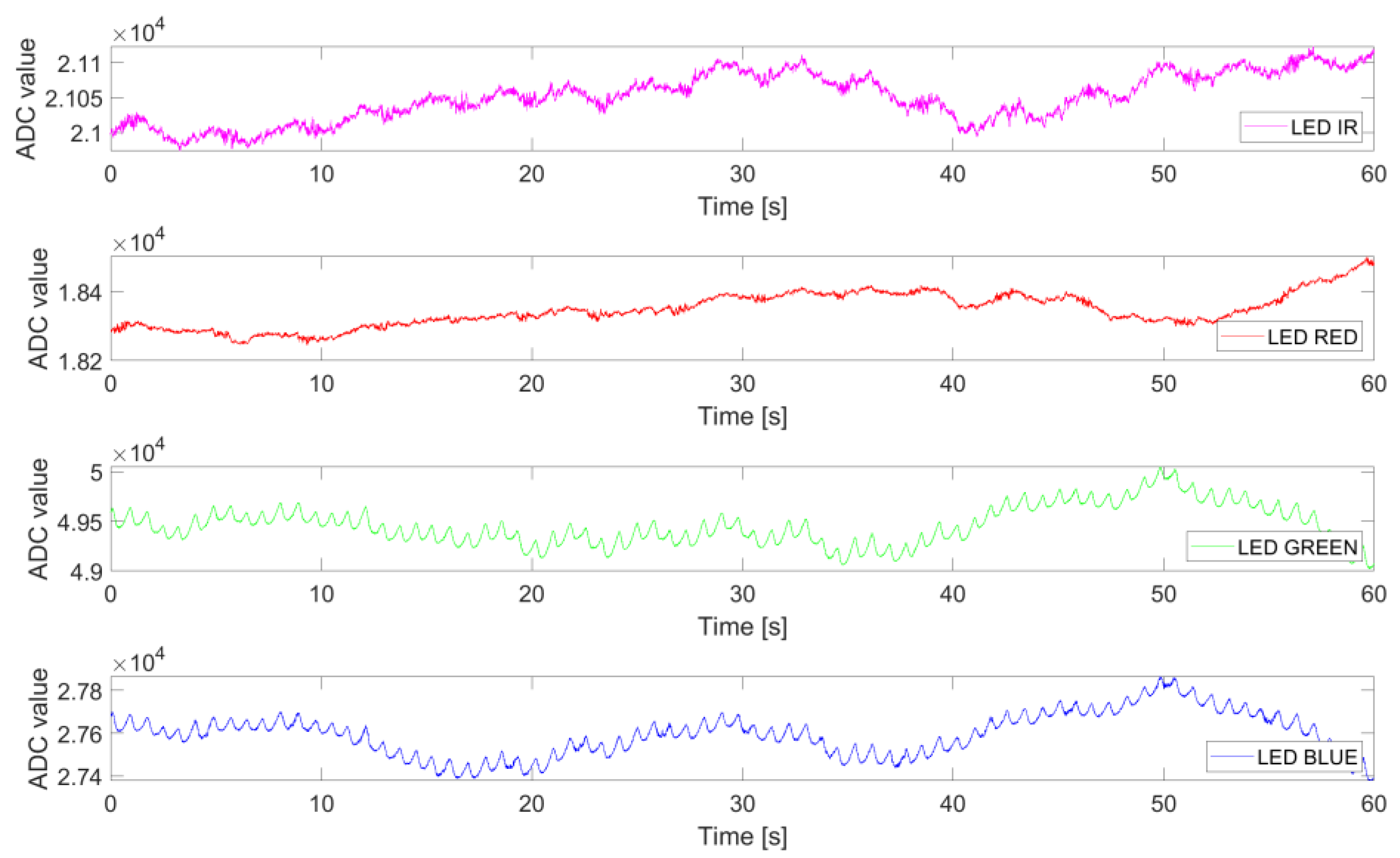
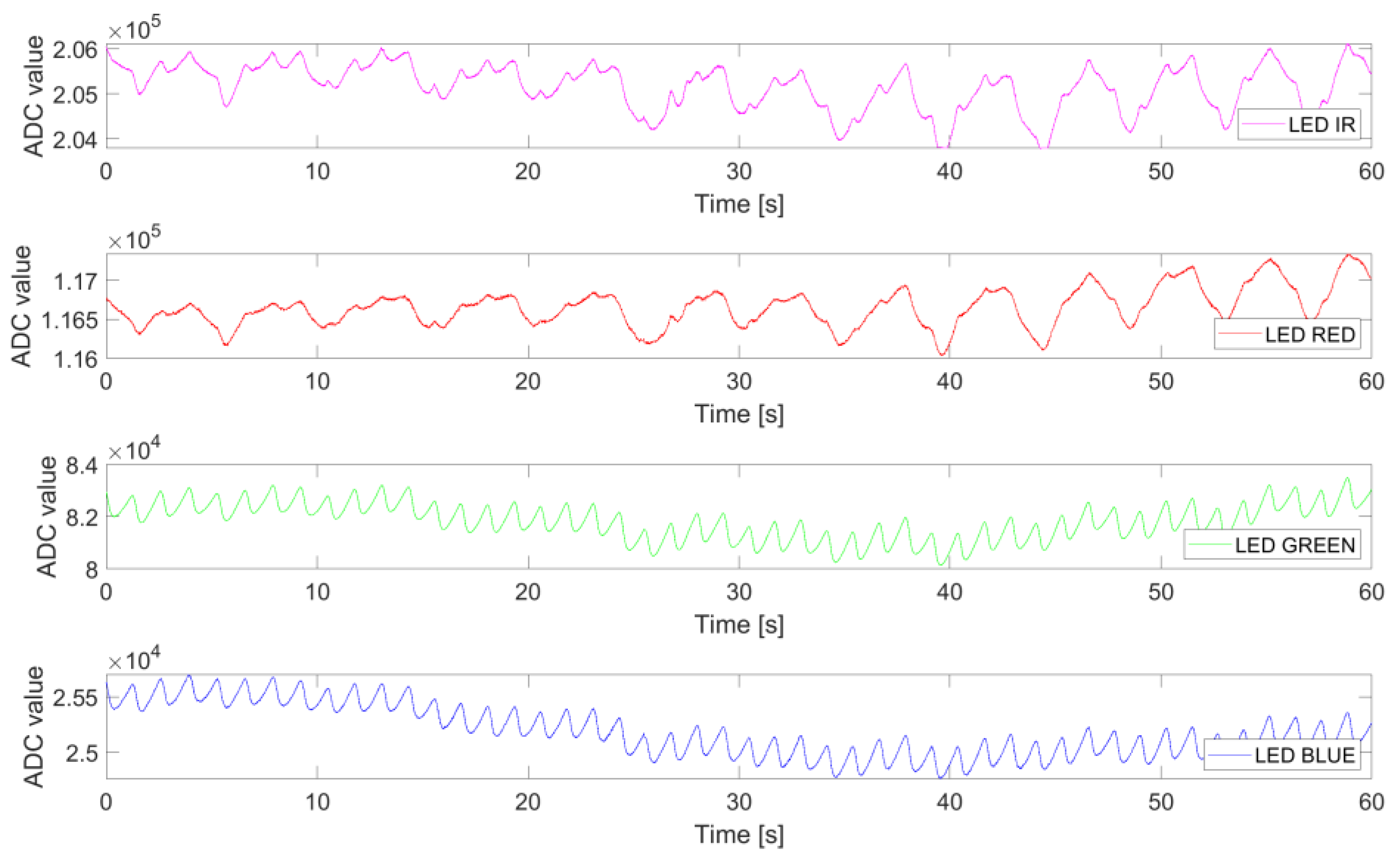
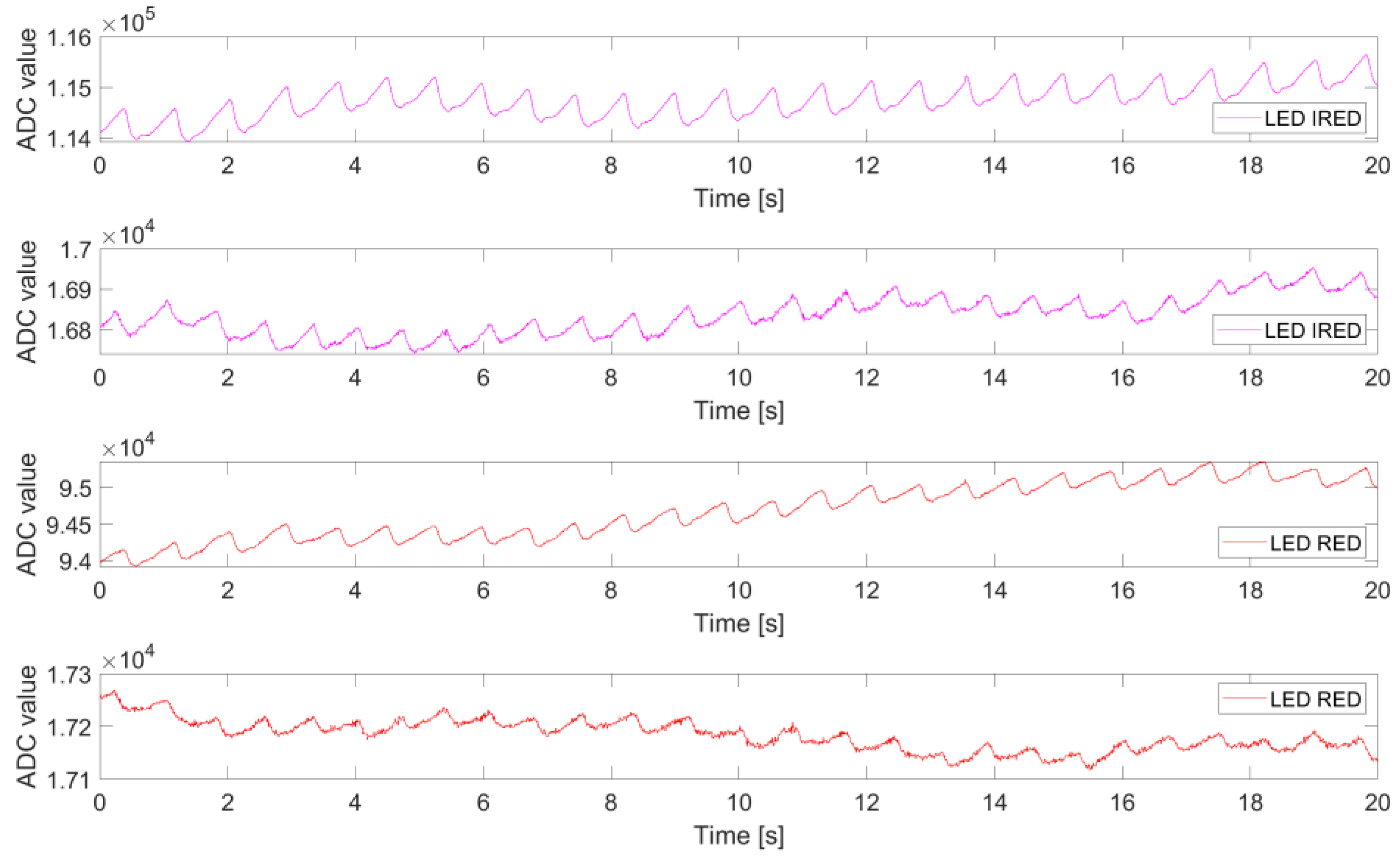
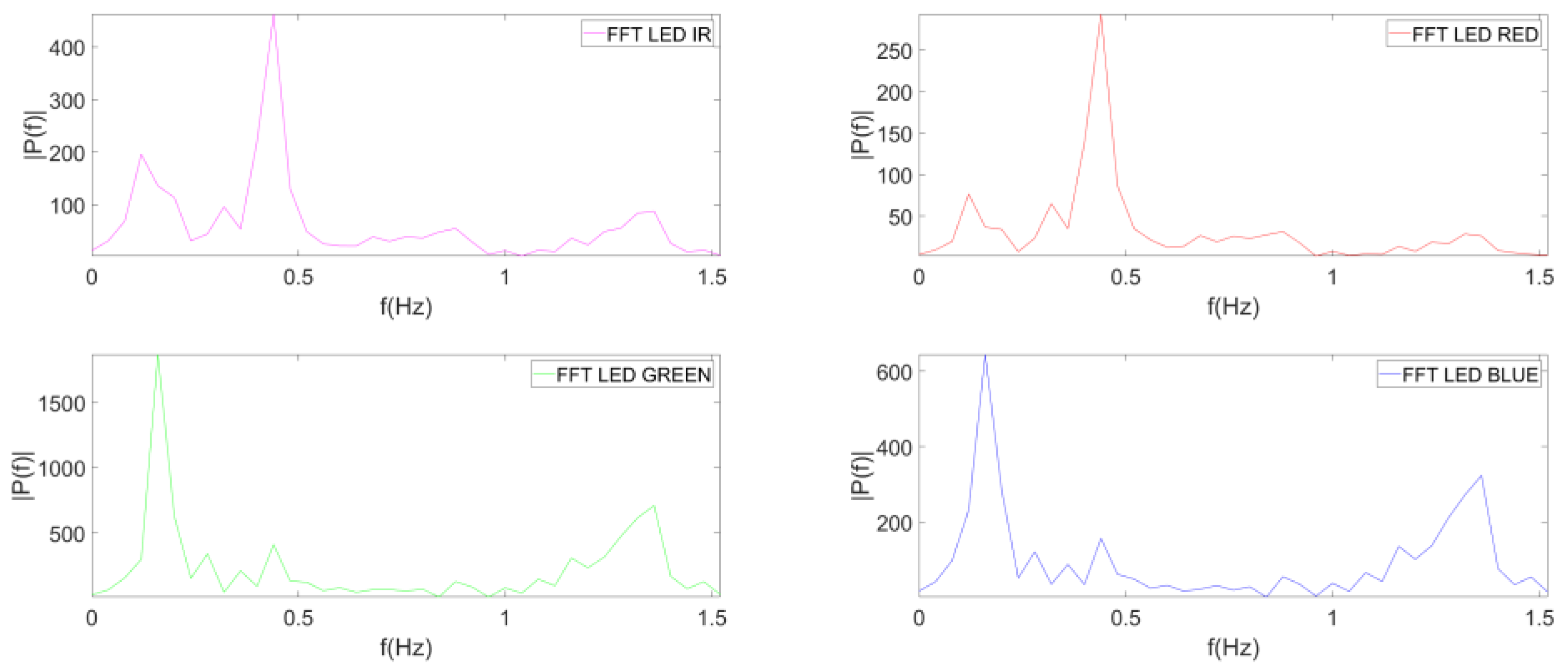
4.1. Analysis of PPG Signals for Different Measurement Sites
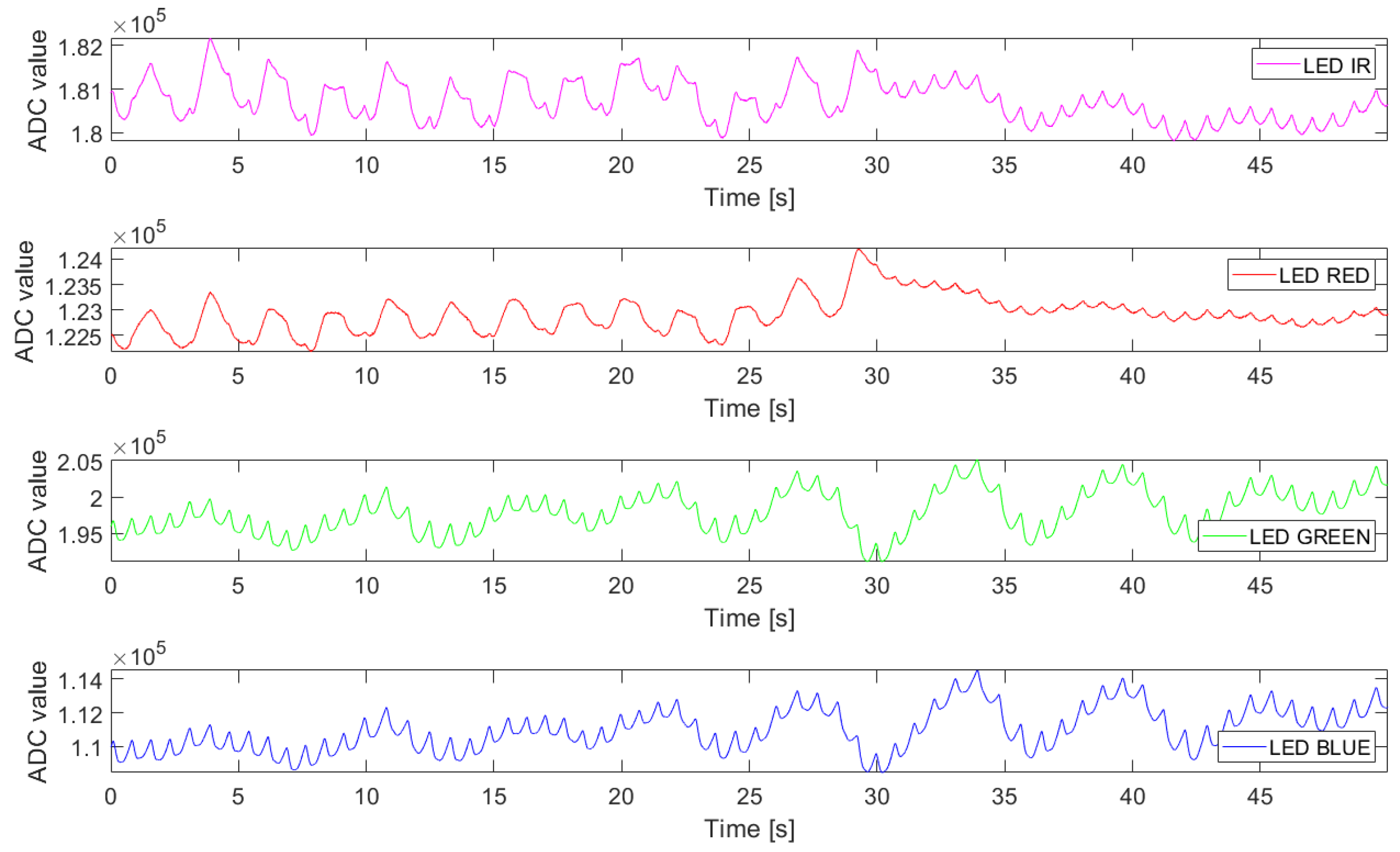
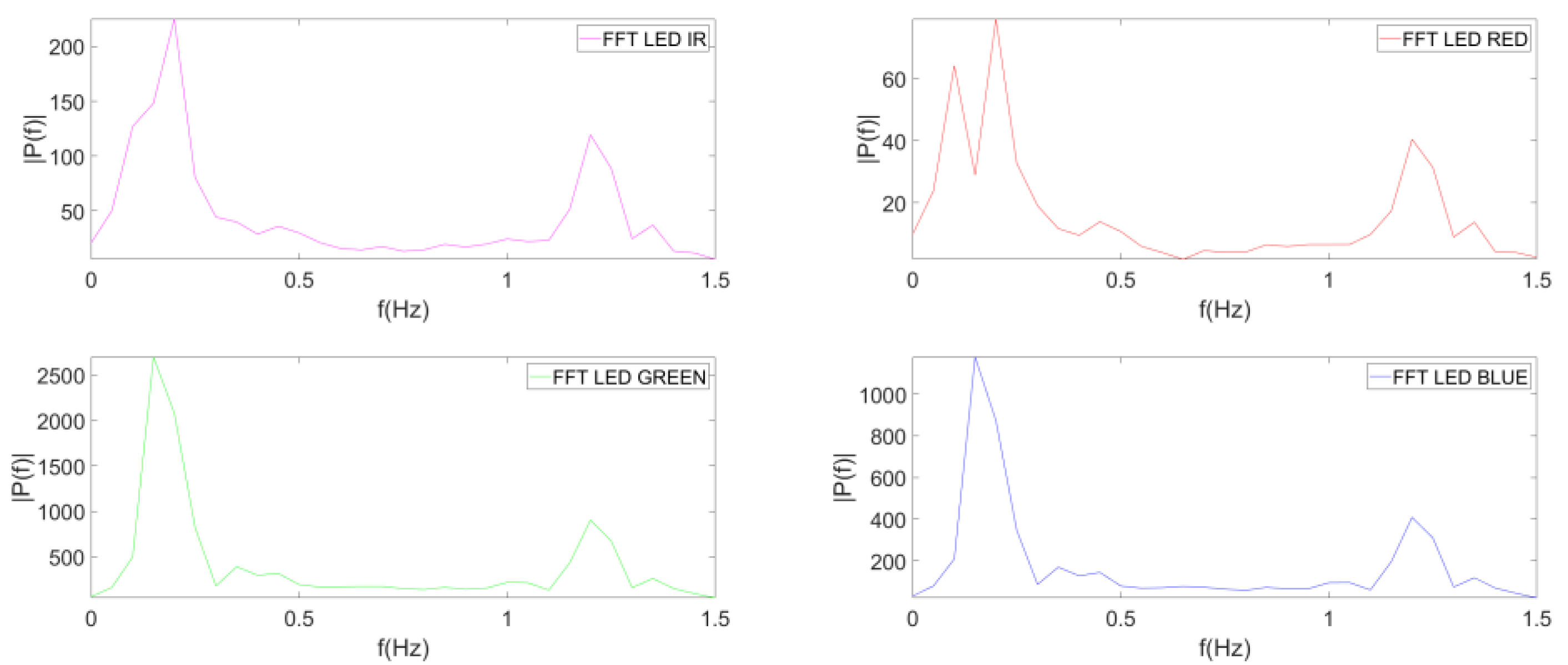
4.2. Analysis of PPG Signals from Manubrium during Apnea
4.3. Noise Analysis of the MAX86916
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Aymen, A.A.; Shelley, K.H. Photoplethysmography. Best Pract. Res. Clin. Anaesthesiol. 2014, 28, 395–406. [Google Scholar] [CrossRef]
- Tamura, T. Current progress of photoplethysmography and SPO2 for health monitoring. Biomed. Eng. Lett. 2019, 9, 21–36. [Google Scholar] [CrossRef] [PubMed]
- Wukitsch, M.W. Pulse oximetry: Historical review and Ohmeda functional analysis. Int. J. Clin. Monit. Comput. 1987, 4, 161–166. [Google Scholar] [CrossRef] [PubMed]
- Meada, Y.; Sekine, M.; Tamura, T. The advantage of green reflected photoplethysmograph. J. Med. Syst. 2011, 35, 829–834. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.; Matsumura, K.; Yamakoshi, K.-I.; Rolfe, P.; Tanaka, S.; Yamakoshi, T. Comparison between red, green and blue light reflection photoplethysmography for heart rate monitoring during motion. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Osaka, Japan, 3–7 July 2013; pp. 1724–1727. [Google Scholar] [CrossRef]
- Shchelkanova, E.; Shchelkanov, A.; Shchapova, L.; Shibata, T. An Exploration of Blue PPG Signal Using a Novel Color Sensorbased PPG System. In Proceedings of the Annual International Conference of the IEEE Engineering in Medicine and Biology Society, Montreal, QC, Canada, 20–24 July 2020; pp. 4414–4420. [Google Scholar] [CrossRef]
- Analog Devices. ADP166 Datasheet. 2014. Available online: https://www.analog.com/media/en/technical-documentation/data-sheets/ADP165_166.pdf (accessed on 3 March 2023).
- Lee, B.S. Understanding the Terms and Definitions of LDO Voltage Regulators. Technical Report October. 1999. Available online: https://www.ti.com/lit/an/slva079/slva079.pdf?ts=1627289674362 (accessed on 3 March 2023).
- Elgendi, M. Optimal signal quality index for photoplethysmogram signals. Bioengineering 2016, 3, 21. [Google Scholar] [CrossRef] [PubMed]
- Pereira, T.; Gadhoumi, K.; Ma, M.; Liu, X.; Xiao, R.; Colorado, R.A.; Keenan, K.J.; Meisel, K.; Hu, X. A Supervised Approach to Robust Photoplethysmography Quality Assessment. IEEE J. Biomed. Health Inform. 2020, 24, 649–657. [Google Scholar] [CrossRef]
- Welch, P.D. The use of Fast Fourier Transform for the estimation of power spectra: A method based on time averaging over short, modified periodograms. IEEE Trans. Audio Electroacoust. 1967, 15, 70–73. [Google Scholar] [CrossRef]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef]
- Přibil, J.; Přibilová, A.; Frollo, I. Comparative Measurement of the PPG Signal on Different Human Body Positions by Sensors Working in Reflection and Transmission Modes. Eng. Proc. 2020, 2, 69. [Google Scholar] [CrossRef]
- Kamal, A.A.; Harness, J.B.; Irving, G.; Mearns, A.J. Skin photoplethysmography: A review. Comput. Methods Programs Biomed. 1989, 28, 257–269. [Google Scholar] [CrossRef]













{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Configuration | 1 | 2 | 3 | 4 | 5 | 6 | 7 |
|---|---|---|---|---|---|---|---|
| Operation frequency [Hz] | 100 | 100 | 100 | 100 | 100 | 100 | 100 |
| Full-scale ADC [nA] | 32,768 | 16,384 | 8192 | 4096 | 4096 | 4096 | 4096 |
| LED current [mA] | 200–2 | 75–2 | 25–2 | 15–2 | 15–2 | 15–2 | 15–2 |
| Pulse width [μs] | 420 | 420 | 420 | 420 | 220 | 120 | 70 |
| ADC integration time [μs] | 400 | 400 | 400 | 400 | 200 | 100 | 50 |
| Operation mode | FLEX | FLEX | FLEX | FLEX | FLEX | FLEX | FLEX |
| Operation Frequency [Hz] | 100 |
| Full-scale ADC [nA] | 8192 |
| LED current [mA] | 10–2 |
| Pulse width [μs] | 420 |
| ADC integration time [μs] | 400 |
| Operation mode | FLEX |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Traversi, G.; Gaioni, L.; Salvetti, D. Development and Testing of a Miniaturized Platform for Photoplethysmography. Electronics 2023, 12, 2230. https://doi.org/10.3390/electronics12102230
Traversi G, Gaioni L, Salvetti D. Development and Testing of a Miniaturized Platform for Photoplethysmography. Electronics. 2023; 12(10):2230. https://doi.org/10.3390/electronics12102230
Chicago/Turabian StyleTraversi, Gianluca, Luigi Gaioni, and Davide Salvetti. 2023. "Development and Testing of a Miniaturized Platform for Photoplethysmography" Electronics 12, no. 10: 2230. https://doi.org/10.3390/electronics12102230