
Applying Collective Intelligence in Health Recommender Systems for Smoking Cessation: A Comparison Trial

 , , ,
, , ,
Abstract
:1. Introduction
Related Works
2. Materials and Methods
2.1. Design
2.2. Interventions
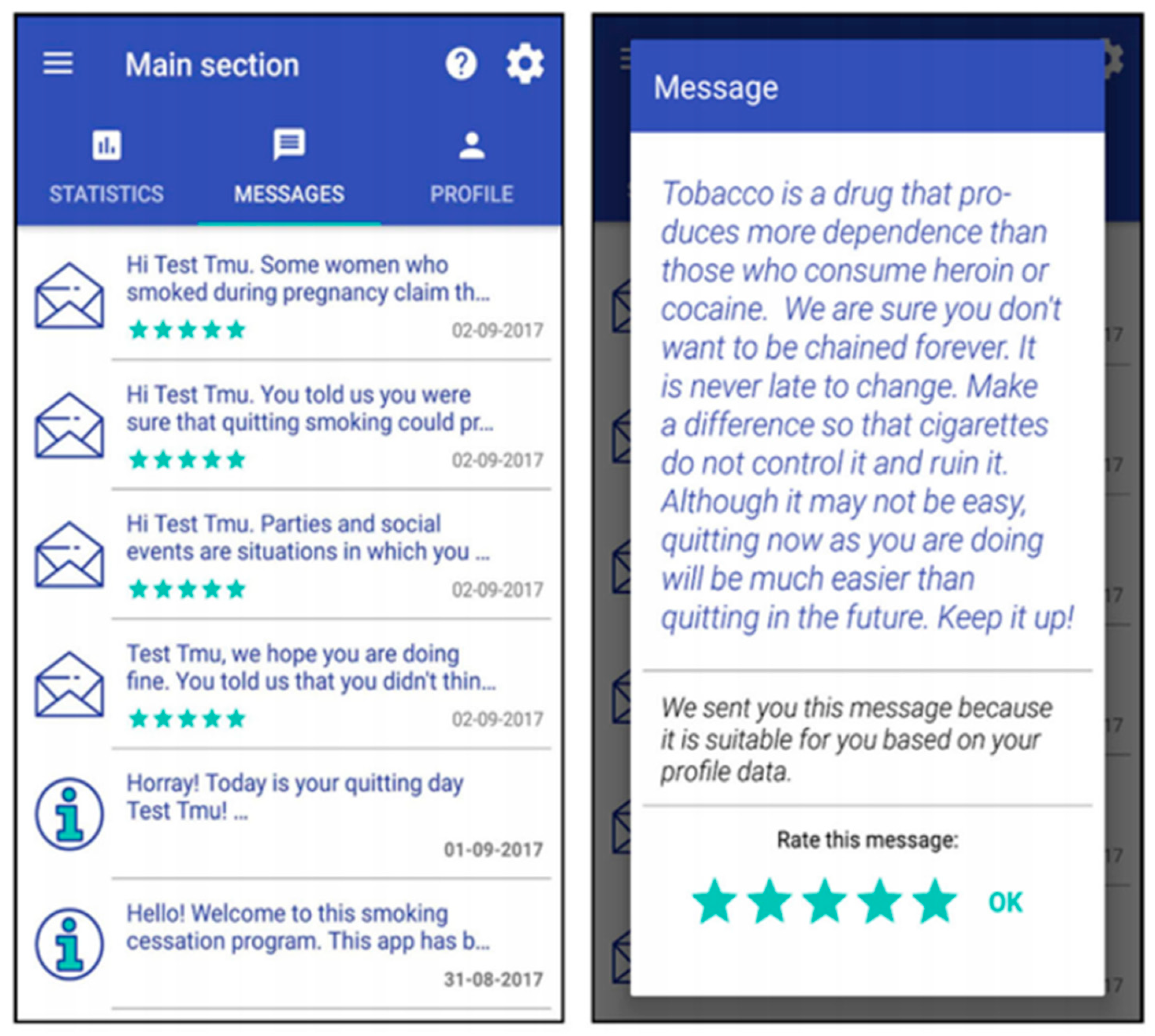
2.2.1. Messages
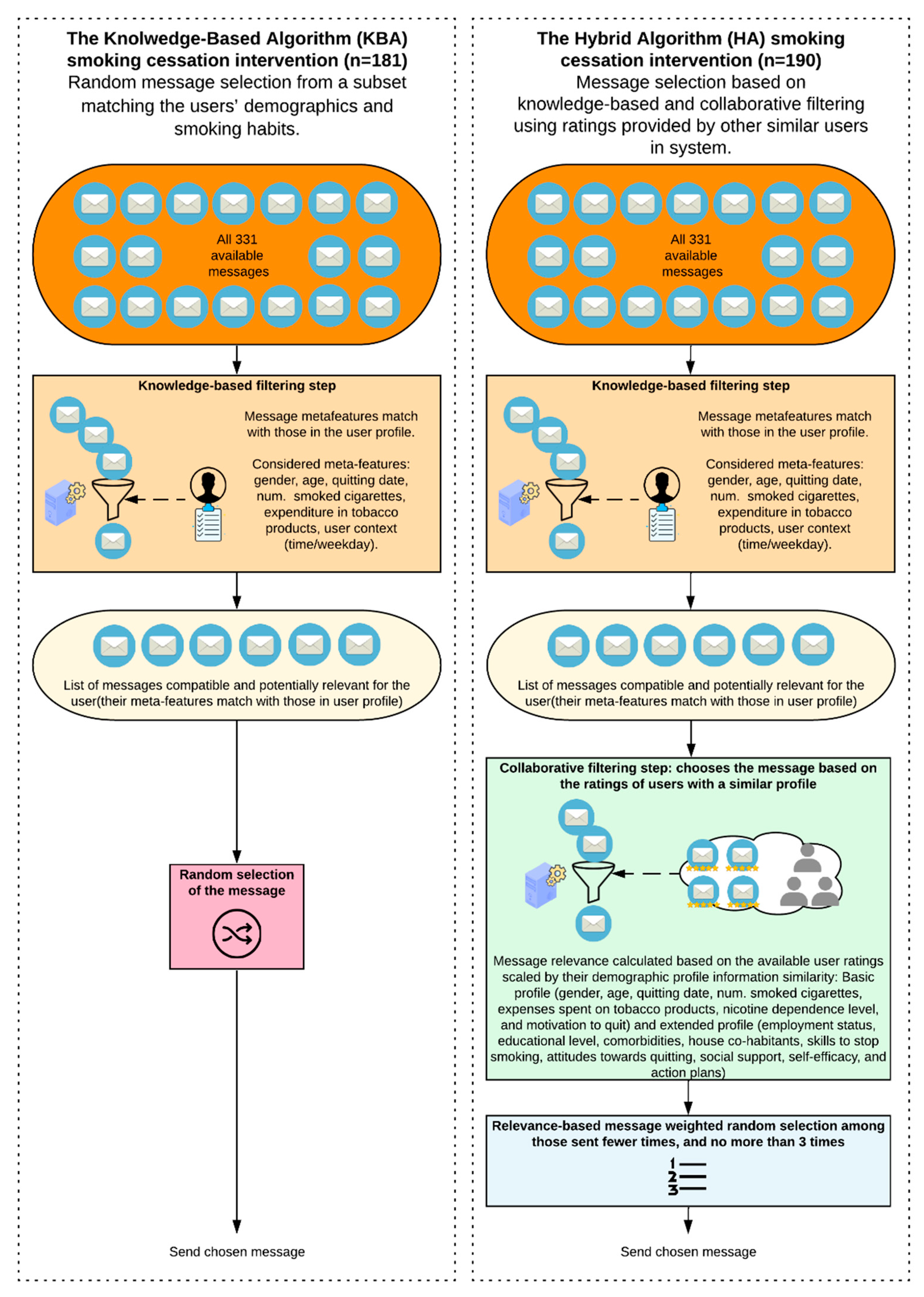
2.2.2. Knowledge-Based Algorithm (KBA) System
2.2.3. Hybrid Algorithm (HA) System
2.3. Participants and Recruitment
2.4. Measurements
2.4.1. Demographics
2.4.2. Outcomes
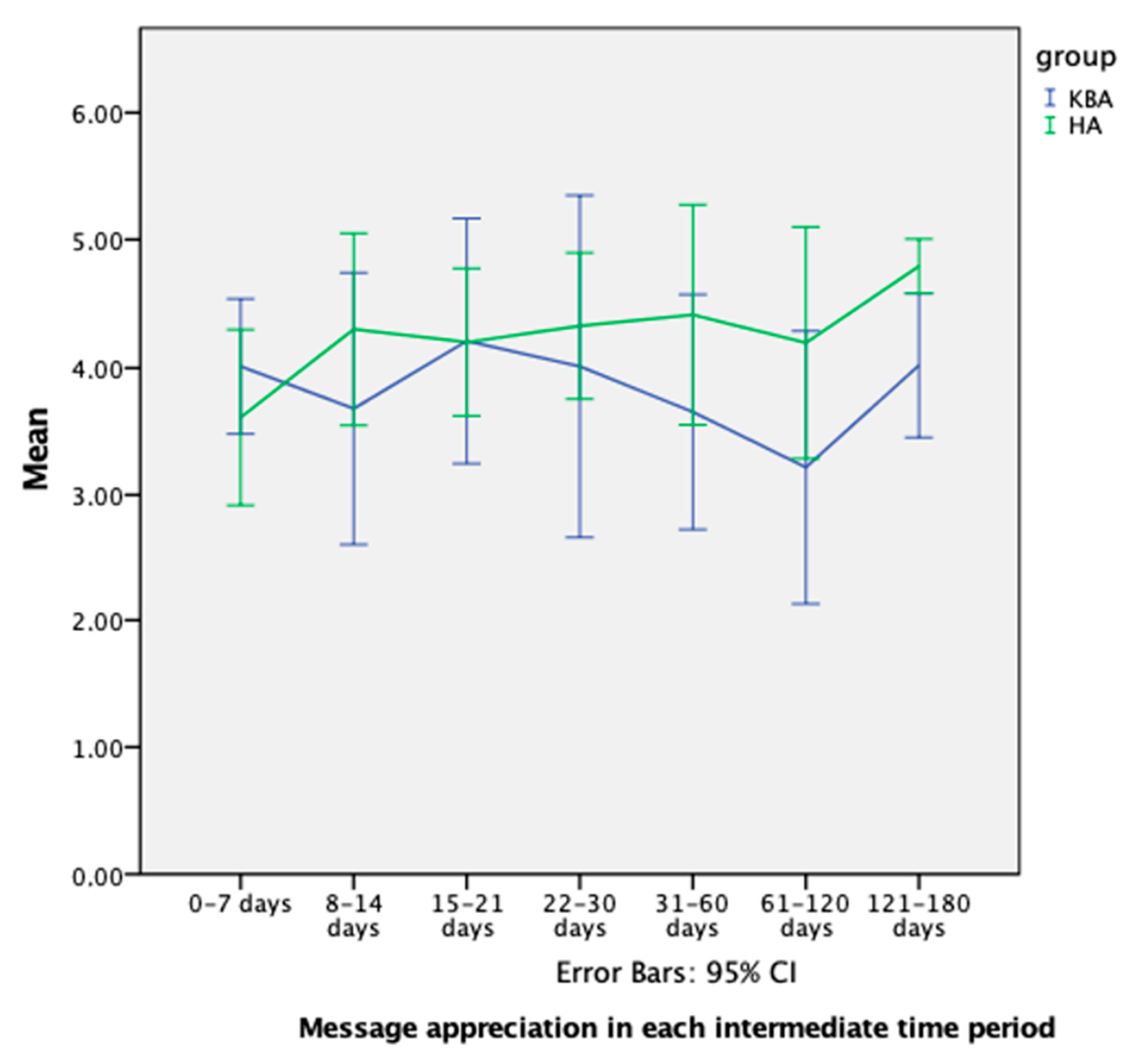
Message Appreciation
Engagement with the System
Smoking Behaviors
2.5. Statistical Analysis
- dropout in terms of no longer sending message ratings,
- dropout in terms of no longer sending abstinence reports, and
- dropout in terms of no longer being active on the app.
- gender,
- nicotine dependence levels (low, medium, high),
- motivation level (low and medium-low, medium-high, and high),
- age (born after 1965 versus born on, or before, 1965),
- employment situation (employed versus unemployed),
- and completion of the extended profile (yes versus no).
3. Results
3.1. Description of the Sample and Involvement Level
3.2. Dropout Analysis
3.3. Overview of Outcomes
3.3.1. Message Appreciation Results
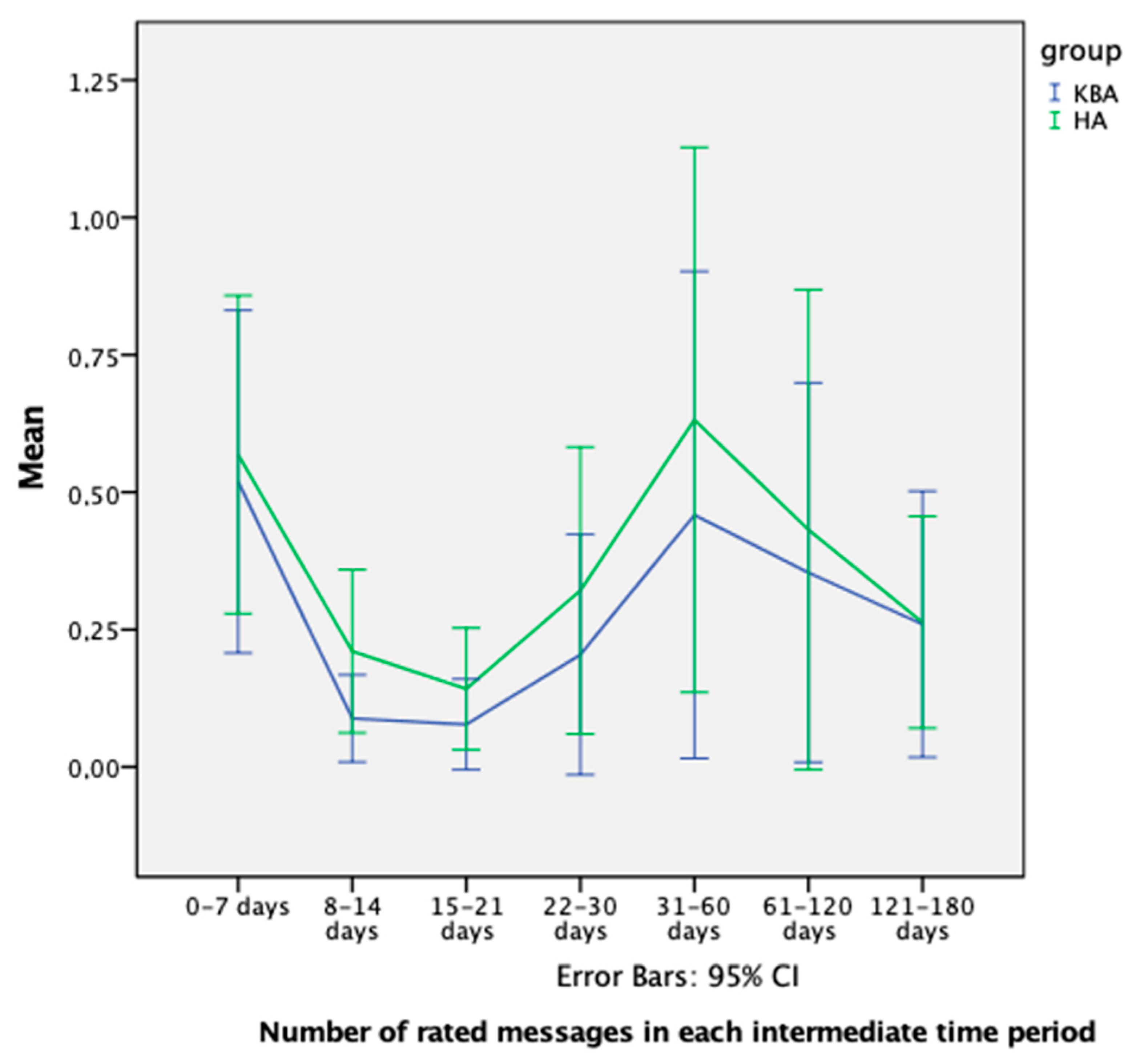
3.3.2. Engagement Results
Number of Rated Messages
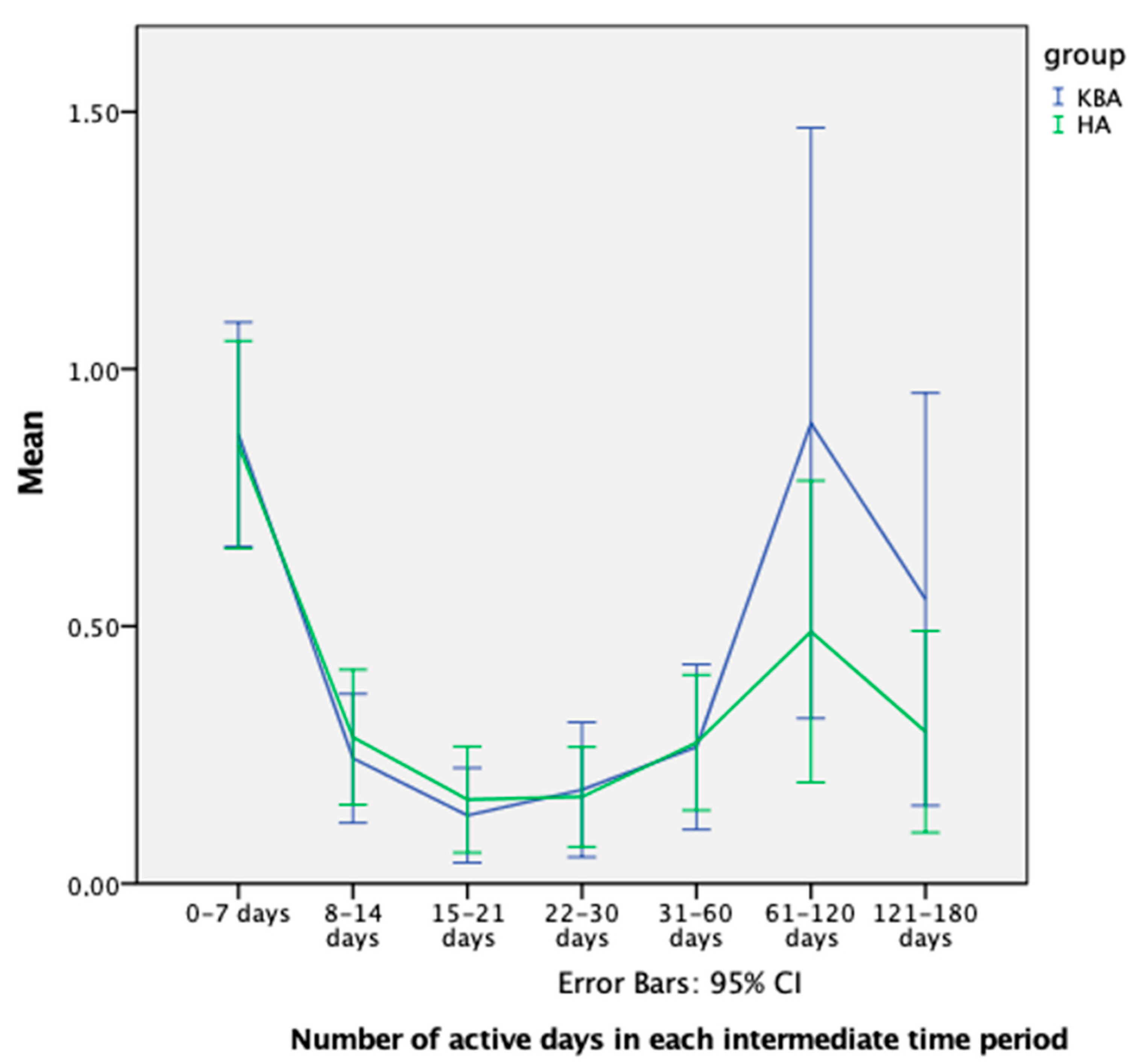
Number of Active Days
Number of Quitting Attempts
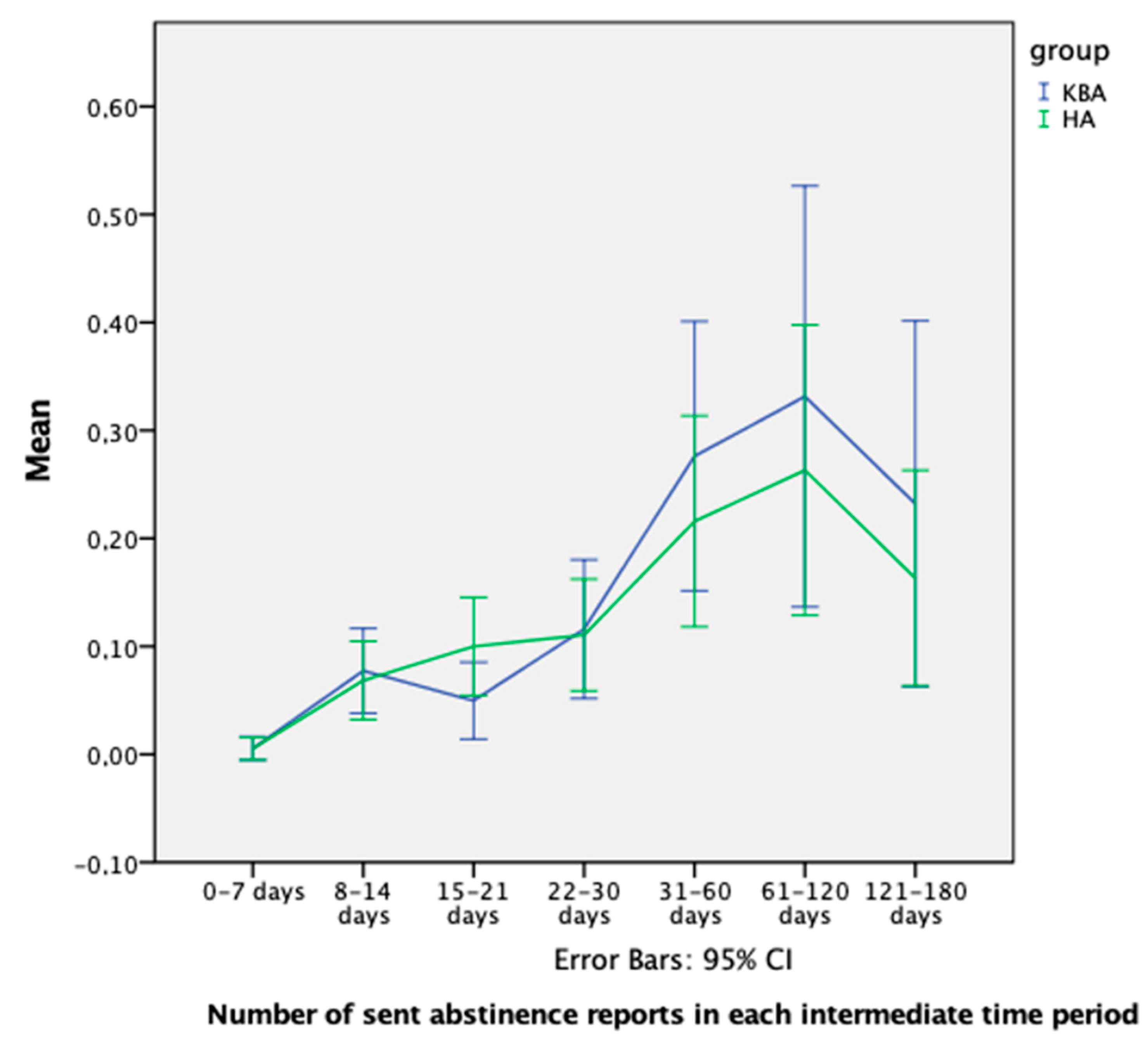
Number of Abstinence Reports
3.3.3. Smoking Cessation Results
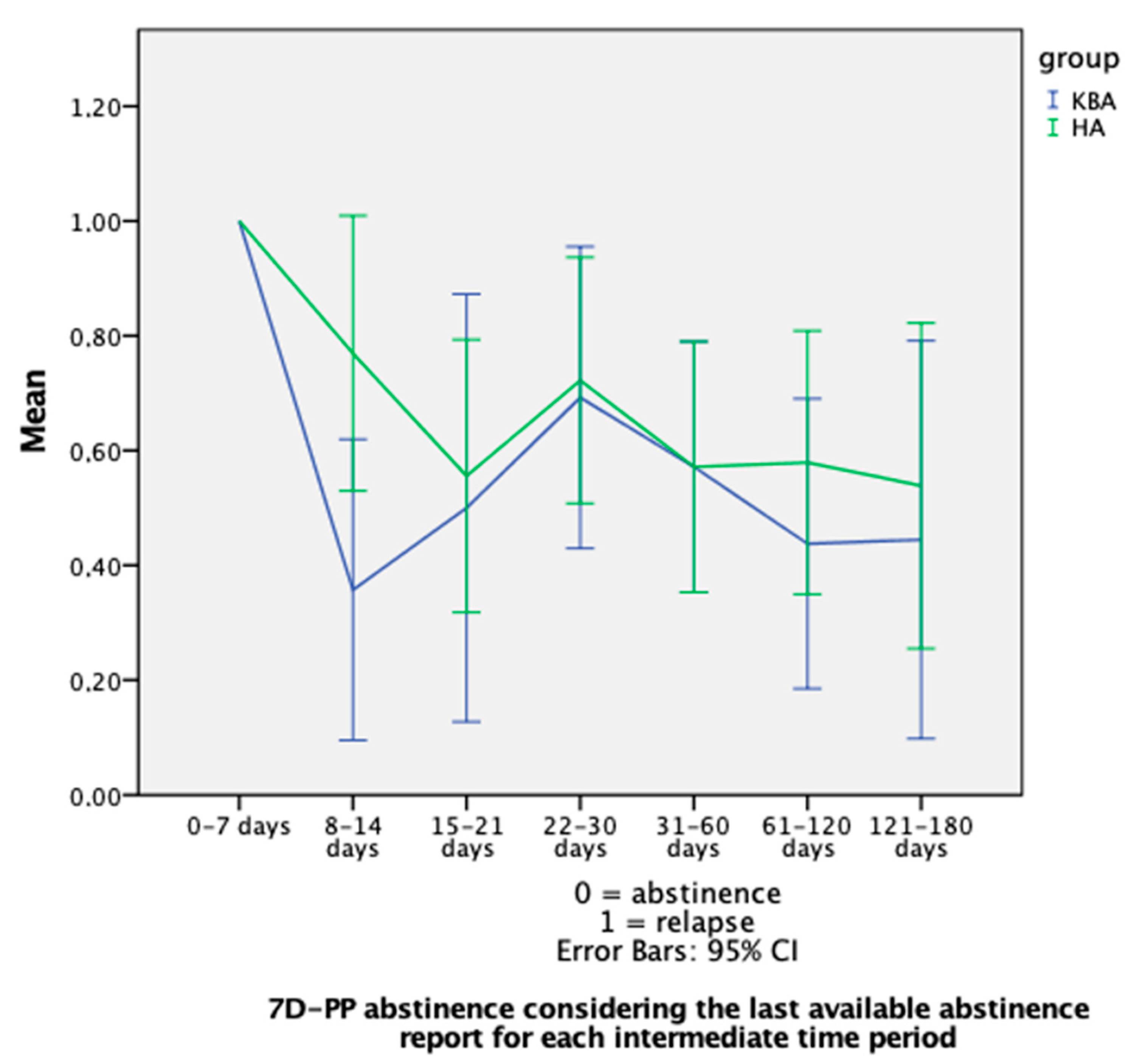
7D-PP Abstinence: Analysis on Available Data
7D-PP Abstinence: Sensitivity Analysis under a Pessimistic Scenario
4. Discussion
4.1. Main Findings
4.1.1. Message Appreciation
4.1.2. Engagement
4.1.3. Smoking Cessation
4.2. Additional Considerations
4.3. Limitations
- 1.
- The HRSs considered all users’ feedback for computing recommendations. This implies that the feedback provided by one group affected the generation of recommendations for the other. This design decision was taken to reduce the cold start effect.
- 2.
- Between 22 May and 6 June 2018, and between 1 and 6 August 2018, there was a server service interruption that prevented users from registering the app and receiving messages.
- 3.
- We could not verify the smoking status self-reports. Self-reports may provide a valid estimation of cessation rates as they were used in several previous studies [132]. The Society for Research on Nicotine and Tobacco Subcommittee on Biochemical Verification considered the use of biochemical validation unnecessary in studies with limited face-to-face contact [133]. However, the use of bogus-pipeline procedures [134], or some biochemical verification methods, would have improved the validity of the smoking status reports [135]. Also, the pessimistic scenario analysis we conducted, intending to follow a conservative approach, may not have accurately reflected the actual behavior of the participants. Also, this study may have suffered from errors derived from some users’ difficulties in accurately recalling their behaviors, as Ramo et al. previously reflected on for an anonymous survey about smoking behaviors [136].
- 4.
- We considered the last status for the abstinence report as the value for each time interval. This way of measuring smoking cessation results hampered direct comparisons with previous studies.
- 5.
- In this effectiveness study, smokers could report by self-chosen times, resulting in the fact that we could not assess all data for all participants at one specific time (e.g., smoking cessation status after 1 month).
- 6.
- It is conceivable that specific subgroup effects could have occurred in our analyses, requiring more sophisticated models with more two-way (or even three-way) interactions to explain our results. However, due to the sparsity of the collected data, these more sophisticated models could not be applied.
- 7.
- 8.
- Persuasion profile meta-features to determine what recommendation style (e.g., authority shown in the message, the reflected consensus stated in the message, the message sender liking perception, etc.) [138,139] would persuade participants the most, were not considered. Such types of meta-features could have added extra personalization power to the HRS without needing the participants to complete additional questions in their user profile.
4.4. Recommendations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Brug, J.; Glanz, K.; Van Assema, P.; Kok, G.; Van Breukelen, G.J. The impact of computer-tailored feedback and iterative feedback on fat, fruit, and vegetable intake. Health Educ. Behav. 1998, 25, 517–531. [Google Scholar] [CrossRef] [PubMed]
- Strecher, V.J. Computer-tailored smoking cessation materials: A review and discussion. Patient Educ. Couns. 1999, 36, 107–117. [Google Scholar] [CrossRef]
- De Vries, H.; Brug, J. Computer-tailored interventions motivating people to adopt health promoting behaviours: Introduction to a new approach. Patient Educ. Couns. 1999, 36, 99–195. [Google Scholar] [PubMed]
- Brug, J.; Oenema, A.; Campbell, M. Past, present, and future of computer-tailored nutrition education. Am. J. Clin. Nutr. 2003, 77, 1028S–1034S. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dijkstra, A. The psychology of tailoring-ingredients in computer-tailored persuasion. Soc. Personal. Psychol. Compass 2008, 2, 765–784. [Google Scholar] [CrossRef]
- Enwald, H.P.K.; Huotari, M.-L.A. Preventing the obesity epidemic by second generation tailored health communication: An interdisciplinary review. J. Med. Internet Res. 2010, 12, e24. [Google Scholar] [CrossRef]
- Ghalibaf, A.K.; Nazari, E.; Gholian-Aval, M.; Tara, M. Comprehensive overview of computer-based health information tailoring: A systematic scoping review. BMJ Open 2019, 9, e021022. [Google Scholar] [CrossRef]
- Kreuter, M.; Farrell, D.; Olevitch, L.; Brennan, L. Tailored Health Messages: Customizing Communication with Computer Technology; Lewrence Erlbaum: Mahwah, NJ, USA, 1999. [Google Scholar]
- Kroeze, W.; Werkman, A.; Brug, J. A systematic review of randomized trials on the effectiveness of computer-tailored education on physical activity and dietary behaviors. Ann. Behav. Med. 2006, 31, 205–223. [Google Scholar] [CrossRef]
- Neville, L.M.; O’Hara, B.; Milat, A. Computer-tailored physical activity behavior change interventions targeting adults: A systematic review. Int. J. Behav. Nutr. Phys. Act. 2009, 6, 30. [Google Scholar] [CrossRef] [Green Version]
- Krebs, P.; Prochaska, J.O.; Rossi, J.S. A meta-analysis of computer-tailored interventions for health behavior change. Prev. Med. 2010, 51, 214–221. [Google Scholar] [CrossRef] [Green Version]
- Cheung, K.L.; Wijnen, B.; de Vries, H. A review of the theoretical basis, effects, and cost effectiveness of online smoking cessation interventions in the Netherlands: A mixed-methods approach. J. Med. Internet Res. 2017, 19, e230. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, A.; De Vries, H.; Roijackers, J.; van Breukelen, G. Tailoring information to enhance quitting in smokers with low motivation to quit: Three basic efficacy questions. Health Psychol. 1998, 17, 513. [Google Scholar] [CrossRef]
- Glasgow, R.; Christiansen, S.M.; Kurz, D.; King, D.K.; Woolley, T.; Faber, A.J.; Estabrooks, P.A.; Strycker, L.; Toobert, D.; Dickman, J. Engagement in a diabetes self-management website: Usage patterns and generalizability of program use. J. Med. Internet Res. 2011, 13, e9. [Google Scholar] [CrossRef] [PubMed]
- Schneider, F.; van Osch, L.; Schulz, D.N.; Kremers, S.P.; de Vries, H. The influence of user characteristics and a periodic email prompt on exposure to an internet-delivered computer-tailored lifestyle program. J. Med. Internet Res. 2012, 14, e40. [Google Scholar] [CrossRef] [PubMed]
- Bennett, G.G.; Glasgow, R.E. The delivery of public health interventions via the Internet: Actualizing their potential. Annu. Rev. Public Health 2009, 30, 273–292. [Google Scholar] [CrossRef] [PubMed]
- Kreps, G.L.; Neuhauser, L. New directions in eHealth communication: Opportunities and challenges. Patient Educ. Couns. 2010, 78, 329–336. [Google Scholar] [CrossRef]
- Sadasivam, R.S.; Cutrona, S.L.; Kinney, R.L.; Marlin, B.M.; Mazor, K.M.; Lemon, S.C.; Houston, T.K. Collective-intelligence recommender systems: Advancing computer tailoring for health behavior change into the 21st century. J. Med. Internet Res. 2016, 18, e42. [Google Scholar] [CrossRef]
- Kaptein, M.; Eckles, D. Selecting effective means to any end: Futures and ethics of persuasion profiling. In Proceedings of the International Conference on Persuasive Technology, 2010, Copenhagen, Denmark, 7–10 June 2010; pp. 82–93. [Google Scholar]
- Noar, S.M.; Benac, C.N.; Harris, M.S. Does tailoring matter? Meta-analytic review of tailored print health behavior change interventions. Psychol. Bull. 2007, 133, 673. [Google Scholar] [CrossRef] [Green Version]
- Lederman, R.; Smith, S.; Dreyfus, S.; Alzougool, B. Tailoring patient information to encourage patient engagement. Int. J. Netw. Virtual Organ. 2016, 16, 191–203. [Google Scholar] [CrossRef]
- Strecher, V.J.; McClure, J.B.; Alexander, G.L.; Chakraborty, B.; Nair, V.N.; Konkel, J.M.; Greene, S.M.; Collins, L.M.; Carlier, C.C.; Wiese, C.J. Web-based smoking-cessation programs: Results of a randomized trial. Am. J. Prev. Med. 2008, 34, 373–381. [Google Scholar] [CrossRef] [Green Version]
- Spittaels, H.; De Bourdeaudhuij, I.; Brug, J.; Vandelanotte, C. Effectiveness of an online computer-tailored physical activity intervention in a real-life setting. Health Educ. Res. 2007, 22, 385–396. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morrison, L.; Moss-Morris, R.; Michie, S.; Yardley, L. Optimizing engagement with I nternet-based health behaviour change interventions: Comparison of self-assessment with and without tailored feedback using a mixed methods approach. Br. J. Health Psychol. 2014, 19, 839–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schäfer, H.; Hors-Fraile, S.; Karumur, R.P.; Calero Valdez, A.; Said, A.; Torkamaan, H.; Ulmer, T.; Trattner, C. Towards health (aware) recommender systems. In Proceedings of the 2017 International Conference on Digital Health, London, UK, 2–5 July 2017; pp. 157–161. [Google Scholar]
- Hors-Fraile, S.; Malwade, S.; Luna-Perejon, F.; Amaya, C.; Civit, A.; Schneider, F.; Bamidis, P.; Syed-Abdul, S.; Li, Y.-C.; De Vries, H. Opening the Black Box: Explaining the Process of Basing a Health Recommender System on the I-Change Behavioral Change Model. IEEE Access 2019, 7, 176525–176540. [Google Scholar] [CrossRef]
- Pu, P.; Chen, L.; Hu, R. Evaluating recommender systems from the user’s perspective: Survey of the state of the art. User Modeling User-Adapt. Interact. 2012, 22, 317–355. [Google Scholar] [CrossRef]
- Hors-Fraile, S.; Rivera-Romero, O.; Schneider, F.; Fernandez-Luque, L.; Luna-Perejon, F.; Civit-Balcells, A.; de Vries, H. Analyzing recommender systems for health promotion using a multidisciplinary taxonomy: A scoping review. Int. J. Med. Inform. 2018, 114, 143–155. [Google Scholar] [CrossRef]
- De Vries, H. An integrated approach for understanding health behavior; the I-change model as an example. Psychol. Behav. Sci. Int. J. 2017, 2, 555–585. [Google Scholar] [CrossRef] [Green Version]
- Gunawardana, A.; Shani, G. Evaluating recommender systems. In Recommender Systems Handbook; Springer: Berlin/Heidelberg, Germany, 2015; pp. 265–308. [Google Scholar]
- Said, A.; Tikk, D.; Stumpf, K.; Shi, Y.; Larson, M.A.; Cremonesi, P. Recommender Systems Evaluation: A 3D Benchmark. In Proceedings of the RUE@ RecSys, Dublin, Ireland, 9–13 September 2012; pp. 21–23. [Google Scholar]
- Herlocker, J.L.; Konstan, J.A.; Terveen, L.G.; Riedl, J.T. Evaluating collaborative filtering recommender systems. ACM Trans. Inf. Syst. (TOIS) 2004, 22, 5–53. [Google Scholar] [CrossRef]
- Valdez, A.C.; Ziefle, M.; Verbert, K.; Felfernig, A.; Holzinger, A. Recommender systems for health informatics: State-of-the-art and future perspectives. In Machine Learning for Health Informatics; Springer: Berlin/Heidelberg, Germany, 2016; pp. 391–414. [Google Scholar]
- Jander, A.; Crutzen, R.; Mercken, L.; Candel, M.; de Vries, H. Effects of a web-based computer-tailored game to reduce binge drinking among Dutch adolescents: A cluster randomized controlled trial. J. Med. Internet Res. 2016, 18, e29. [Google Scholar] [CrossRef] [Green Version]
- Bingham, C.R.; Barretto, A.I.; Walton, M.A.; Bryant, C.M.; Shope, J.T.; Raghunathan, T.E. Efficacy of a web-based, tailored, alcohol prevention/intervention program for college students: Initial findings. J. Am. Coll. Health 2010, 58, 349–356. [Google Scholar] [CrossRef]
- Martinez-Montilla, J.M.; Mercken, L.; de Vries, H.; Candel, M.; Lima-Rodríguez, J.S.; Lima-Serrano, M. A web-based, computer-tailored intervention to reduce alcohol consumption and binge drinking among Spanish adolescents: Cluster randomized controlled trial. J. Med. Internet Res. 2020, 22, e15438. [Google Scholar] [CrossRef] [Green Version]
- Brug, J.; Steenhuis, I.; van Assema, P.; de Vries, H. The impact of a computer-tailored nutrition intervention. Prev. Med. 1996, 25, 236–242. [Google Scholar] [CrossRef] [PubMed]
- Springvloet, L.; Lechner, L.; de Vries, H.; Candel, M.J.; Oenema, A. Short-and medium-term efficacy of a Web-based computer-tailored nutrition education intervention for adults including cognitive and environmental feedback: Randomized controlled trial. J. Med. Internet Res. 2015, 17, e23. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rawl, S.M.; Skinner, C.S.; Perkins, S.M.; Springston, J.; Wang, H.-L.; Russell, K.M.; Tong, Y.; Gebregziabher, N.; Krier, C.; Smith-Howell, E. Computer-delivered tailored intervention improves colon cancer screening knowledge and health beliefs of African-Americans. Health Educ. Res. 2012, 27, 868–885. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van der Aalst, C.M.; de Koning, H.J.; van den Bergh, K.A.; Willemsen, M.C.; van Klaveren, R.J. The effectiveness of a computer-tailored smoking cessation intervention for participants in lung cancer screening: A randomised controlled trial. Lung Cancer 2012, 76, 204–210. [Google Scholar] [CrossRef]
- Smeets, T.; Brug, J.; de Vries, H. Effects of tailoring health messages on physical activity. Health Educ. Res. 2008, 23, 402–413. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Vries, H.; Logister, M.; Krekels, G.; Klaasse, F.; Servranckx, V.; van Osch, L. Internet-based computer tailored feedback on sunscreen use. J. Med. Internet Res. 2012, 14, e48. [Google Scholar] [CrossRef]
- Smit, E.S.; Evers, S.M.; de Vries, H.; Hoving, C. Cost-effectiveness and cost-utility of Internet-based computer tailoring for smoking cessation. J. Med. Internet Res. 2013, 15, e57. [Google Scholar] [CrossRef]
- Smit, E.S.; de Vries, H.; Hoving, C. Effectiveness of a Web-based multiple tailored smoking cessation program: A randomized controlled trial among Dutch adult smokers. J. Med. Internet Res. 2012, 14, e82. [Google Scholar] [CrossRef] [Green Version]
- Stanczyk, N.E.; Crutzen, R.; Bolman, C.; Muris, J.; de Vries, H. Influence of delivery strategy on message-processing mechanisms and future adherence to a Dutch computer-tailored smoking cessation intervention. J. Med. Internet Res. 2013, 15, e28. [Google Scholar] [CrossRef]
- Elfeddali, I.; de Vries, H.; Bolman, C.; Pronk, T.; Wiers, R.W. A randomized controlled trial of Web-based Attentional Bias Modification to help smokers quit. Health Psychol. 2016, 35, 870. [Google Scholar] [CrossRef]
- Etter, J.-F.; Perneger, T.V. Effectiveness of a computer-tailored smoking cessation program: A randomized trial. Arch. Intern. Med. 2001, 161, 2596–2601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Starke, A.D.; Trattner, C. Promoting Healthy Food Choices Online: A Case for Multi-List Recommender Systems. In Proceedings of the ACM IUI 2021 Workshops, College Station, TX, USA, 14–17 April 2021. [Google Scholar]
- Starke, A.; Asotic, E.; Trattner, C. “Serving Each User”: Supporting Different Eating Goals Through a Multi-List Recommender Interface. In Proceedings of the Fifteenth ACM Conference on Recommender Systems, New York, NY, USA, 27 September–1 October 2021; pp. 124–132. [Google Scholar]
- Musto, C.; Trattner, C.; Starke, A.; Semeraro, G. Towards a knowledge-aware food recommender system exploiting holistic user models. In Proceedings of the 28th ACM Conference on User Modeling, Adaptation and Personalization, Genoa, Italy, 12–18 July 2020; pp. 333–337. [Google Scholar]
- Pecune, F.; Callebert, L.; Marsella, S. A Recommender System for Healthy and Personalized Recipes Recommendations. In Proceedings of the HealthRecSys@ RecSys, New York, NY, USA, 27 September–1 October 2020; pp. 15–20. [Google Scholar]
- Chavan, P.; Thoms, B.; Isaacs, J. A Recommender System for Healthy Food Choices: Building a Hybrid Model for Recipe Recommendations using Big Data Sets; AIS Electronic Library; Available online: https://aisel.aisnet.org/hicss-54/hc/wellness_management/2/ (accessed on 5 January 2021).
- Elahi, M.; Ge, M.; Ricci, F.; Fernández-Tobías, I.; Berkovsky, S.; Massimo, D. Interaction Design in a Mobile Food Recommender System. In Proceedings of the IntRS@ RecSys, Vienna, Austria, 16–20 September 2015; pp. 49–52. [Google Scholar]
- Gómez-del-Río, N.; González-González, C.S.; Toledo-Delgado, P.A.; Muñoz-Cruz, V.; García-Peñalvo, F. Health promotion for childhood obesity: An approach based on self-tracking of data. Sensors 2020, 20, 3778. [Google Scholar] [CrossRef]
- Elsweiler, D.; Harvey, M.; Ludwig, B.; Said, A. Bringing the “healthy” into Food Recommenders. In Proceedings of the DMRS, 2015, Bolzano, Italy, 22–23 October 2015; pp. 33–36. [Google Scholar]
- Tran, T.N.T.; Atas, M.; Felfernig, A.; Stettinger, M. An overview of recommender systems in the healthy food domain. J. Intell. Inf. Syst. 2018, 50, 501–526. [Google Scholar] [CrossRef]
- Zenun Franco, R. Online recommender system for personalized nutrition advice. In Proceedings of the Eleventh ACM Conference on Recommender Systems, 2017, Como, Italy, 31 August 2017; pp. 411–415. [Google Scholar]
- Ribeiro, D.; Machado, J.; Ribeiro, J.; Vasconcelos, M.J.M.; Vieira, E.F.; de Barros, A.C. SousChef: Mobile Meal Recommender System for Older Adults. In Proceedings of the ICT4AgeingWell, Porto, Portugal, 28–29 April 2017; pp. 36–45. [Google Scholar]
- Kuanr, M.; Mohapatra, P.; Piri, J. Health recommender system for cervical cancer prognosis in women. In Proceedings of the 2021 6th International Conference on Inventive Computation Technologies (ICICT), Lalitpur, Nepal, 20–22 July 2021; pp. 673–679. [Google Scholar]
- Ammar, N.; Bailey, J.E.; Davis, R.L.; Shaban-Nejad, A. Using a Personal Health Library–Enabled mHealth Recommender System for Self-Management of Diabetes Among Underserved Populations: Use Case for Knowledge Graphs and Linked Data. JMIR Form. Res. 2021, 5, e24738. [Google Scholar] [CrossRef] [PubMed]
- Rohani, D.A.; Quemada Lopategui, A.; Tuxen, N.; Faurholt-Jepsen, M.; Kessing, L.V.; Bardram, J.E. MUBS: A personalized recommender system for behavioral activation in mental health. In Proceedings of the 2020 CHI Conference on Human Factors in Computing Systems, Honolulu, HI, USA, 25–30 April 2020; pp. 1–13. [Google Scholar]
- Hors-Fraile, S.; Benjumea, F.J.N.; Hernández, L.C.; Ruiz, F.O.; Fernandez-Luque, L. Design of two combined health recommender systems for tailoring messages in a smoking cessation app. arXiv 2016, arXiv:1608.07192. [Google Scholar]
- Carrasco-Hernandez, L.; Jódar-Sánchez, F.; Núñez-Benjumea, F.; Conde, J.M.; González, M.M.; Civit-Balcells, A.; Hors-Fraile, S.; Parra-Calderón, C.L.; Bamidis, P.D.; Ortega-Ruiz, F. A Mobile Health Solution Complementing Psychopharmacology-Supported Smoking Cessation: Randomized Controlled Trial. JMIR mHealth uHealth 2020, 8, e17530. [Google Scholar] [CrossRef]
- Sadasivam, R.S.; Borglund, E.M.; Adams, R.; Marlin, B.M.; Houston, T.K. Impact of a collective intelligence tailored messaging system on smoking cessation: The Perspect randomized experiment. J. Med. Internet Res. 2016, 18, e285. [Google Scholar] [CrossRef] [Green Version]
- Chen, J.; Houston, T.K.; Faro, J.M.; Nagawa, C.S.; Orvek, E.A.; Blok, A.C.; Allison, J.J.; Person, S.D.; Smith, B.M.; Sadasivam, R.S. Evaluating the use of a recommender system for selecting optimal messages for smoking cessation: Patterns and effects of user-system engagement. BMC Public Health 2021, 21, 1749. [Google Scholar] [CrossRef]
- Pincay, J.; Terán, L.; Portmann, E. Health recommender systems: A state-of-the-art review. In Proceedings of the 2019 Sixth International Conference on eDemocracy & eGovernment (ICEDEG), Quito, Ecuador, 24–26 April 2019; pp. 47–55. [Google Scholar]
- Cheung, K.L.; Durusu, D.; Sui, X.; de Vries, H. How recommender systems could support and enhance computer-tailored digital health programs: A scoping review. Digital Health 2019, 5, 1–19. [Google Scholar] [CrossRef] [Green Version]
- Su, J.; Guan, Y.; Li, Y.; Chen, W.; Lv, H.; Yan, Y. Do recommender systems function in the health domain: A system review. arXiv 2020, arXiv:2007.13058. [Google Scholar]
- Ferretto, L.R.; Cervi, C.R.; de Marchi, A.C.B. Recommender systems in mobile apps for health a systematic review. In Proceedings of the 2017 12th Iberian Conference on Information Systems and Technologies (CISTI), Lisbon, Portugal, 14–17 June 2017; pp. 1–6. [Google Scholar]
- Prajapati, J.; Brahmbhatt, K.N. A Systematic Literature Review on Health Recommender Systems. In Proceedings of the International e-Conference on Intelligent Systems and Signal Processing, Hanoi, Vietnam, 19–20 March 2022; pp. 557–572. [Google Scholar]
- De Croon, R.; Van Houdt, L.; Htun, N.N.; Štiglic, G.; Abeele, V.V.; Verbert, K. Health Recommender Systems: Systematic Review. J. Med. Internet Res. 2021, 23, e18035. [Google Scholar] [CrossRef] [PubMed]
- Hors-Fraile, S.; Malwade, S.; Spachos, D.; Fernandez-Luque, L.; Su, C.-T.; Jeng, W.-L.; Syed-Abdul, S.; Bamidis, P.; Li, Y.-C.J. A recommender system to quit smoking with mobile motivational messages: Study protocol for a randomized controlled trial. Trials 2018, 19, 618. [Google Scholar] [CrossRef] [PubMed]
- Bamidis, P.D.; Paraskevopoulos, E.; Konstantinidis, E.; Spachos, D.; Billis, A. Multimodal e-health services for smoking cessation and public health: The smokefreebrain project approach. In Proceedings of the MEDINFO 2017: Precision Healthcare through Informatics: Proceedings of the 16th World Congress on Medical and Health Informatics, Hangzhou, China, 31 January 2018; p. 5. [Google Scholar]
- Abroms, L.C.; Whittaker, R.; Free, C.; Van Alstyne, J.M.; Schindler-Ruwisch, J.M. Developing and pretesting a text messaging program for health behavior change: Recommended steps. JMIR mHealth uHealth 2015, 3, e107. [Google Scholar] [CrossRef] [PubMed]
- Walsh, R.A.; Sanson-Fisher, R.W. Encouraging People to Stop Smoking; World Health Organisation: Geneva, Switzerland, 2001. [Google Scholar]
- Panday, S.; Reddy, S.P.; Ruiter, R.A.; Bergström, E.; de Vries, H. Determinants of smoking cessation among adolescents in South Africa. Health Educ. Res. 2005, 20, 586–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hoving, E.; Mudde, A.; De Vries, H. Predictors of smoking relapse in a sample of Dutch adult smokers; the roles of gender and action plans. Addict. Behav. 2006, 31, 1177–1189. [Google Scholar] [CrossRef] [PubMed]
- De Vries, H.; Eggers, S.M.; Bolman, C. The role of action planning and plan enactment for smoking cessation. BMC Public Health 2013, 13, 393. [Google Scholar] [CrossRef] [Green Version]
- Elling, J.M.; Crutzen, R.; Talhout, R.; De Vries, H. Tobacco smoking and smoking cessation in times of COVID-19. Tob. Prev. Cessat. 2020, 6, 39. [Google Scholar] [CrossRef]
- Kasten, S.; Eggers, S.; de Vries, H. The importance of self-efficacy and action planning for smoking cessation. Eur. Health Psychol. 2015, 17, 694. [Google Scholar]
- Dijkstra, A.; Vries, H.D. Self-efficacy expectations with regard to different tasks in smoking cessation. Psychol. Health 2000, 15, 501–511. [Google Scholar] [CrossRef]
- Vries, H.D.; Mudde, A.N. Predicting stage transitions for smoking cessation applying the attitude-social influence-efficacy model. Psychol. Health 1998, 13, 369–385. [Google Scholar] [CrossRef]
- De Vries, H.; Backbier, E.; Kok, G.; Dijkstra, M. The Impact of Social Influences in the Context of Attitude, Self-Efficacy, Intention, and Previous Behavior as Predictors of Smoking Onset1. J. Appl. Soc. Psychol. 1995, 25, 237–257. [Google Scholar] [CrossRef]
- Abraham, C.; Kools, M. Writing Health Communication: An Evidence-Based Guide; Sage: Ventura County, CA, USA, 2011. [Google Scholar]
- Burke, R. Knowledge-based recommender systems. Encycl. Libr. Inf. Syst. 2000, 69, 175–186. [Google Scholar]
- Çano, E.; Morisio, M. Hybrid recommender systems: A systematic literature review. Intell. Data Anal. 2017, 21, 1487–1524. [Google Scholar] [CrossRef] [Green Version]
- Herlocker, J.L.; Konstan, J.A.; Riedl, J. Explaining collaborative filtering recommendations. In Proceedings of the 2000 ACM Conference on Computer Supported Cooperative Work, Philadelphia, PA, USA, 2–6 December 2000; pp. 241–250. [Google Scholar]
- Cacioppo, J.T.; Petty, R.E.J.B.; Psychology, A.S. Effects of message repetition on argument processing, recall, and persuasion. Basic Appl. Soc. Psychol. 1989, 10, 3–12. [Google Scholar] [CrossRef]
- Heatherton, T.F.; Kozlowski, L.T.; Frecker, R.C.; Fagerstrom, K.O. The Fagerström test for nicotine dependence: A revision of the Fagerstrom Tolerance Questionnaire. Br. J. Addict. 1991, 86, 1119–1127. [Google Scholar] [CrossRef] [PubMed]
- Richmond, R.L.; Kehoe, L.A.; Webster, I.W. Multivariate models for predicting abstention following intervention to stop smoking by general practitioners. Addiction 1993, 88, 1127–1135. [Google Scholar] [CrossRef] [PubMed]
- Berkup, S.B. Working with generations X and Y in generation Z period: Management of different generations in business life. Mediterr. J. Soc. Sci. 2014, 5, 218. [Google Scholar] [CrossRef]
- Cheung, K.L.; de Ruijter, D.; Hiligsmann, M.; Elfeddali, I.; Hoving, C.; Evers, S.M.; de Vries, H. Exploring consensus on how to measure smoking cessation. A Delphi study. BMC Public Health 2017, 17, 890. [Google Scholar] [CrossRef]
- Gupta, S.K. Intention-to-treat concept: A review. Perspect. Clin. Res. 2011, 2, 109. [Google Scholar] [CrossRef]
- Cacheda, F.; Carneiro, V.; Fernández, D.; Formoso, V. Comparison of collaborative filtering algorithms: Limitations of current techniques and proposals for scalable, high-performance recommender systems. ACM Trans. Web (TWEB) 2011, 5, 1–33. [Google Scholar] [CrossRef]
- Candillier, L.; Jack, K.; Fessant, F.; Meyer, F. State-of-the-art recommender systems. In Collaborative and Social Information Retrieval and Access: Techniques for Improved User Modeling; IGI Global: Hershey, PA, USA, 2009; pp. 1–22. [Google Scholar]
- Desrosiers, C.; Karypis, G. A comprehensive survey of neighborhood-based recommendation methods. In Recommender Systems Handbook; Springer: Berlin/Heidelberg, Germany, 2011; pp. 107–144. [Google Scholar]
- Ziegler, C.-N.; McNee, S.M.; Konstan, J.A.; Lausen, G. Improving recommendation lists through topic diversification. In Proceedings of the 14th International Conference on World Wide Web, Chiba, Japan, 10–14 May 2005; pp. 22–32. [Google Scholar]
- Schafer, J.B.; Frankowski, D.; Herlocker, J.; Sen, S. Collaborative filtering recommender systems. In The Adaptive Web; Springer: Berlin/Heidelberg, Germany, 2007; pp. 291–324. [Google Scholar]
- Serrano-Guerrero, J.; Herrera-Viedma, E.; Olivas, J.A.; Cerezo, A.; Romero, F.P. A google wave-based fuzzy recommender system to disseminate information in University Digital Libraries 2.0. Inf. Sci. 2011, 181, 1503–1516. [Google Scholar] [CrossRef]
- Porcel, C.; Tejeda-Lorente, A.; Martínez, M.; Herrera-Viedma, E. A hybrid recommender system for the selective dissemination of research resources in a technology transfer office. Inf. Sci. 2012, 184, 1–19. [Google Scholar] [CrossRef]
- Pu, P.; Chen, L.; Hu, R. A user-centric evaluation framework for recommender systems. In Proceedings of the Fifth ACM Conference on Recommender Systems, Chicago, IL, USA, 23–27 October 2011; pp. 157–164. [Google Scholar]
- Torous, J.; Nicholas, J.; Larsen, M.E.; Firth, J.; Christensen, H. Clinical review of user engagement with mental health smartphone apps: Evidence, theory and improvements. Evid.-Based Ment. Health 2018, 21, 116–119. [Google Scholar] [CrossRef] [PubMed]
- Sandborg, J.; Henriksson, P.; Larsen, E.; Lindqvist, A.-K.; Rutberg, S.; Söderström, E.; Maddison, R.; Löf, M. Participants’ Engagement and Satisfaction With a Smartphone App Intended to Support Healthy Weight Gain, Diet, and Physical Activity During Pregnancy: Qualitative Study Within the HealthyMoms Trial. JMIR mHealth uHealth 2021, 9, e26159. [Google Scholar] [CrossRef] [PubMed]
- Dovaliene, A.; Piligrimiene, Z.; Masiulyte, A. Factors influencing customer engagement in mobile applications. Eng. Econ. 2016, 27, 205–212. [Google Scholar] [CrossRef] [Green Version]
- Ahmadian, S.; Ahmadian, M.; Jalili, M. A deep learning based trust-and tag-aware recommender system. Neurocomputing 2021, in press. [CrossRef]
- Arnold, C.L.; Davis, T.C.; Berkel, H.J.; Jackson, R.H.; Nandy, I.; London, S. Smoking status, reading level, and knowledge of tobacco effects among low-income pregnant women. Prev. Med. 2001, 32, 313–320. [Google Scholar] [CrossRef]
- Fakir, S.E.; Serhier, Z.; Berraho, M.; Elrhazi, K.; Tachfouti, N.; Slama, K.; Nejjari, C. Knowledge and perceptions of smoking according to income level in Morocco. Am. J. Health Promot. 2011, 25, 387–391. [Google Scholar] [CrossRef]
- Kaye, L.; Gondalia, R.; Remmelink, E.; Su, J.; Thompson, A.; Barrett, M. Impact of Socioeconomic Status on the Relationship Between Smartphone App Engagement and Adherence Among Patients with Asthma. In B102. Caring for Lung Diseases in Underserved and Vulnerable Populations; American Thoracic Society: New York, NY, USA, 2020; p. A4281. [Google Scholar]
- Crafoord, M.-T.; Fjell, M.; Sundberg, K.; Nilsson, M.; Langius-Eklöf, A. Engagement in an Interactive App for Symptom Self-Management during Treatment in Patients With Breast or Prostate Cancer: Mixed Methods Study. J. Med. Internet Res. 2020, 22, e17058. [Google Scholar] [CrossRef]
- Garnett, C.; Perski, O.; Tombor, I.; West, R.; Michie, S.; Brown, J. Predictors of engagement, response to follow up, and extent of alcohol reduction in users of a smartphone app (Drink Less): Secondary analysis of a factorial randomized controlled trial. JMIR mHealth uHealth 2018, 6, e11175. [Google Scholar] [CrossRef]
- Zheng, Y.; Mobasher, B.; Burke, R. Similarity-based context-aware recommendation. In Proceedings of the International Conference on Web Information Systems Engineering, Amsterdam, The Netherlands, 20–24 October 2015; pp. 431–447. [Google Scholar]
- Guo, G.; Zhang, J.; Yorke-Smith, N. A novel Bayesian similarity measure for recommender systems. In Proceedings of the IJCAI, Beijing, China, 3–9 August 2013; pp. 2619–2625. [Google Scholar]
- Sarwar, B.; Karypis, G.; Konstan, J.; Riedl, J. Analysis of recommendation algorithms for e-commerce. In Proceedings of the 2nd ACM Conference on Electronic Commerce, Minneapolis, MN, USA, 17–20 October 2000; pp. 158–167. [Google Scholar]
- Ahmadian, M.; Ahmadi, M.; Ahmadian, S. A Reliable Deep Representation Learning to Improve Trust-aware Recommendation Systems. Expert Syst. Appl. 2022, 197, 116697. [Google Scholar] [CrossRef]
- Nelson, D.B.; Partin, M.R.; Fu, S.S.; Joseph, A.M.; An, L.C. Why assigning ongoing tobacco use is not necessarily a conservative approach to handling missing tobacco cessation outcomes. Nicotine Tob. Res. 2009, 11, 77–83. [Google Scholar] [CrossRef]
- Blankers, M.; Smit, E.S.; van der Pol, P.; de Vries, H.; Hoving, C.; van Laar, M. The missing= smoking assumption: A fallacy in internet-based smoking cessation trials? Nicotine Tob. Res. 2016, 18, 25–33. [Google Scholar] [CrossRef] [PubMed]
- Westmaas, J.L.; Bontemps-Jones, J.; Hendricks, P.S.; Kim, J.; Abroms, L.C. Randomised controlled trial of stand-alone tailored emails for smoking cessation. Tob. Control 2018, 27, 136–146. [Google Scholar] [CrossRef] [PubMed]
- Regmi, K.; Kassim, N.; Ahmad, N.; Tuah, N.A. Effectiveness of mobile apps for smoking cessation: A review. Tob. Prev. Cessat. 2017, 3, 12. [Google Scholar] [CrossRef] [Green Version]
- Bricker, J.B.; Mull, K.E.; Kientz, J.A.; Vilardaga, R.; Mercer, L.D.; Akioka, K.J.; Heffner, J.L. Randomized, controlled pilot trial of a smartphone app for smoking cessation using acceptance and commitment therapy. Drug Alcohol Depend. 2014, 143, 87–94. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ubhi, H.K.; Michie, S.; Kotz, D.; Wong, W.C.; West, R. A mobile app to aid smoking cessation: Preliminary evaluation of SmokeFree28. J. Med. Internet Res. 2015, 17, e17. [Google Scholar] [CrossRef] [Green Version]
- Iacoviello, B.M.; Steinerman, J.R.; Klein, D.B.; Silver, T.L.; Berger, A.G.; Luo, S.X.; Schork, N.J. Clickotine, a personalized smartphone app for smoking cessation: Initial evaluation. JMIR mHealth uHealth 2017, 5, e56. [Google Scholar] [CrossRef]
- Meyer, C.; Ulbricht, S.; Baumeister, S.E.; Schumann, A.; Rüge, J.; Bischof, G.; Rumpf, H.J.; John, U. Proactive interventions for smoking cessation in general medical practice: A quasi-randomized controlled trial to examine the efficacy of computer-tailored letters and physician-delivered brief advice. Addiction 2008, 103, 294–304. [Google Scholar] [CrossRef]
- Te Poel, F.; Bolman, C.; Reubsaet, A.; de Vries, H. Efficacy of a single computer-tailored e-mail for smoking cessation: Results after 6 months. Health Educ. Res. 2009, 24, 930–940. [Google Scholar] [CrossRef] [Green Version]
- Karumur, R.P.; Nguyen, T.T.; Konstan, J.A. Personality, user preferences and behavior in recommender systems. Inf. Syst. Front. 2018, 20, 1241–1265. [Google Scholar] [CrossRef]
- Willemse, B.J.P.C.; Kaptein, M.C.; Hasaart, F. Developing Effective Methods for Electronic Health Personalization: Protocol for Health Telescope, a Prospective Interventional Study. JMIR Res. Protoc. 2020, 9, e16471. [Google Scholar] [CrossRef] [PubMed]
- Kennedy-Martin, T.; Curtis, S.; Faries, D.; Robinson, S.; Johnston, J. A literature review on the representativeness of randomized controlled trial samples and implications for the external validity of trial results. Trials 2015, 16, 495. [Google Scholar] [CrossRef] [Green Version]
- Harper, F.M.; Konstan, J.A. The movielens datasets: History and context. Acm Trans. Interact. Intell. Syst. (TiiS) 2015, 5, 1–19. [Google Scholar] [CrossRef]
- Sahoo, A.K.; Pradhan, C.; Barik, R.K.; Dubey, H. DeepReco: Deep learning based health recommender system using collaborative filtering. Computation 2019, 7, 25. [Google Scholar] [CrossRef] [Green Version]
- Rivero-Rodriguez, A.; Konstantinidis, S.T.; Sánchez-Bocanegra, C.L.; Fernández-Luque, L. A health information recommender system: Enriching YouTube health videos with Medline Plus information by the use of SnomedCT terms. In Proceedings of the 26th IEEE International Symposium on Computer-Based Medical Systems, Porto, Portugal, 20–22 June 2013; pp. 257–261. [Google Scholar]
- Bocanegra, C.L.S.; Ramos, J.L.S.; Rizo, C.; Civit, A.; Fernandez-Luque, L. HealthRecSys: A semantic content-based recommender system to complement health videos. BMC Med. Inform. Decis. Mak. 2017, 17, 63. [Google Scholar]
- Hors-Fraile, S.; Schneider, F.; Fernandez-Luque, L.; Luna-Perejon, F.; Civit, A.; Spachos, D.; Bamidis, P.; de Vries, H. Tailoring motivational health messages for smoking cessation using an mHealth recommender system integrated with an electronic health record: A study protocol. BMC Public Health 2018, 18, 698. [Google Scholar] [CrossRef]
- Hutton, H.E.; Wilson, L.M.; Apelberg, B.J.; Avila Tang, E.; Odelola, O.; Bass, E.B.; Chander, G. A systematic review of randomized controlled trials: Web-based interventions for smoking cessation among adolescents, college students, and adults. Nicotine Tob. Res. 2011, 13, 227–238. [Google Scholar] [CrossRef] [Green Version]
- Benowitz, N.; Jacob, P.; Ahijevych, K.; Jarvis, M.; Hall, S.; LeHouezec, J.; Hansson, A.; Lichtenstein, E.; Henningfield, J.; Tsoh, J. SRNT Subcommittee on Biochemical Verification. Biochemical verification of tobacco use and cessation. Nicotine Tob. Res. 2002, 4, 149–159. [Google Scholar] [CrossRef] [Green Version]
- Stanczyk, N.; de Vries, H.; Candel, M.; Muris, J.; Bolman, C. Effectiveness of video-versus text-based computer-tailored smoking cessation interventions among smokers after one year. Prev. Med. 2016, 82, 42–50. [Google Scholar] [CrossRef] [Green Version]
- Patrick, D.L.; Cheadle, A.; Thompson, D.C.; Diehr, P.; Koepsell, T.; Kinne, S. The validity of self-reported smoking: A review and meta-analysis. Am. J. Public Health 1994, 84, 1086–1093. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramo, D.E.; Hall, S.M.; Prochaska, J.J. Reliability and validity of self-reported smoking in an anonymous online survey with young adults. Health Psychol. 2011, 30, 693. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Knijnenburg, B.P.; Willemsen, M.C.; Gantner, Z.; Soncu, H.; Newell, C. Explaining the user experience of recommender systems. User Modeling User-Adapt. Interact. 2012, 22, 441–504. [Google Scholar] [CrossRef] [Green Version]
- Kaptein, M.; Eckles, D. Heterogeneity in the effects of online persuasion. J. Interact. Mark. 2012, 26, 176–188. [Google Scholar] [CrossRef]
- Kaptein, M.; Markopoulos, P.; De Ruyter, B.; Aarts, E. Personalizing persuasive technologies: Explicit and implicit personalization using persuasion profiles. Int. J. Hum.-Comput. Stud. 2015, 77, 38–51. [Google Scholar] [CrossRef] [Green Version]
- Smith, A.L.; Chapman, S.; Dunlop, S.M. What do we know about unassisted smoking cessation in Australia? A systematic review, 2005–2012. Tob. Control 2015, 24, 18–27. [Google Scholar] [CrossRef]
- Hughes, J.R.; Keely, J.; Naud, S. Shape of the relapse curve and long-term abstinence among untreated smokers. Addiction 2004, 99, 29–38. [Google Scholar] [CrossRef]
- Moore, D.; Aveyard, P.; Connock, M.; Wang, D.; Fry-Smith, A.; Barton, P. Effectiveness and safety of nicotine replacement therapy assisted reduction to stop smoking: Systematic review and meta-analysis. BMJ 2009, 338, b1024. [Google Scholar] [CrossRef] [Green Version]
- Shiffman, S.; Rolf, C.N.; Hellebusch, S.J.; Gorsline, J.; Gorodetzky, C.W.; Chiang, Y.K.; Schleusener, D.S.; Marino, M.E.D. Real-world efficacy of prescription and over-the-counter nicotine replacement therapy. Addiction 2002, 97, 505–516. [Google Scholar] [CrossRef] [Green Version]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Message Meta-Features | |||||||
|---|---|---|---|---|---|---|---|
| Potentially Compatible Messages | Age Group | Gender | Number of Daily Smoked Cigarettes | Weekly Expenditure | Quitting Date | Context | |
| Message A | Young | Male | High | Only for mornings | No (Not matching in age group & weekly expenditure) | ||
| Message B | <10 | Less than 15 days ago | Only for weekends | Yes | |||
| Message C | Old | Female | >20 | Only for evenings | No (Not matching in age group, gender, and number of smoked cigarettes) | ||
| Message D | Middle-aged | High | Only for mornings | Yes | |||
| Message E | Male | 10–20 | Low | No (Not matching in number of daily smoked cigarettes) | |||
| Message F | More than 30 days ago | No (Not matching in quitting date) | |||||
| Message G | Female | Less than 7 days ago | No (Not matching in gender, and quitting date) | ||||
| Specific meta-features for the target user profile | Middle-aged | Male | <10 | Low | 9 days ago | No restrictions | |
| Variable | Total (n = 371) | KBA (n = 181) | HA (n = 190) | Test Statistics p-Value |
|---|---|---|---|---|
| Mean age, years (SD, CV) | 36.90 (10.21, 0.28) | 37.71 (10.78, 0.29) | 36.13 (9.60, 0.27) | F(1369) = 2.229 p = 0.136 |
| Generation distribution: Percentage younger (no.) | 92.7% (344) | 90.6% (64) | 94.7% (180) | χ2 = 2.34 * p = 0.13/p = 0.16 |
| Gender: Percentage male (no.) | 78.2% (290) | 76.8% (139) | 79.5% (151) | χ2 = 0.39 * p = 0.53/p = 0.62 |
| Mean nicotine dependence score (SD, CV) | 5.13 (2.59, 0.50) | 5.08 (2.69, 0.53) | 5.17 (2.50, 0.48) | F(1386) = 0.13 p = 0.77 |
| Mean motivation to quit score (SD, CV) | 7.54 (1.91. 0.25) | 7.54 (2.03, 0.27) | 7.55 (1.80, 0.24) | F(1369) = 0.01 p = 0.93 |
| Employment status: Percentage employed (no.) | 83.0% (308) | 83.4% (151) | 82.6% (157) | χ2 = 0.04 * p = 0.83/p = 0.89 |
| Profile completion: Percentage completed (no.) | 43.9% (163) | 42.0% (76) | 45.8% (87) | χ2 = 0.54 * p = 0.46/p = 0.47 |
| Appreciation Variable | Regression Coefficient of HRS (Coding: KBA = 0, HA= 1) | Test Statistic | p-Value | Odds Ratio | 95% Confidence Interval for Effect Size |
|---|---|---|---|---|---|
| Message ratings | 0.818 | F(1129) = 0.869 | 0.353 | 2.265 | (0.399, 12.85) |
| Engagement Variable | Regression Coefficient of HRS (Coding: KBA = 0, HA = 1) | Test Statistic | p-Value | Incidence Rate Ratio | 95% Confidence Interval for Effect Size |
|---|---|---|---|---|---|
| Number of rated messages | −0.036 | F(1233) = 0.021 | 0.884 | 0.965 | (0.595, 1.565) |
| Number of active days | −0.258 | F(1440) = 4.112 | 0.043 | 0.773 | (0.602, 0.992) |
| Number of abstinence reports | −0.403 | F(1421) = 11.702 | 0.001 | 0.710 | (0.530, 0.843) |
| Number of quitting attempts | 0.105 | χ2(1) = 1.190 | 0.275 | 1.111 | (0.920, 1.340) |
| Smoking Cessation Variable | Regression Coefficient of HRS (Coding: KBA = 0, HA = 1) | Test Statistic | p-Value | Odds Ratio | 95% Confidence Interval for Effect Size |
|---|---|---|---|---|---|
| 7D-PP reports: available data (on last report available in each time interval) | −0.474 | χ2(1) = 2.383 | 0.123 | 0.623 | (0.341, 1.138) |
| 7D-PP reports: available data (on last report available from 0–180 days period) | −1.010 | χ2(1) = 5.162 | 0.023 | 0.364 | (0.151, 0.880) |
| 7D-PP reports: pessimistic scenario (on last report available in each time interval) | −0.044 | χ2(1) = 0.037 | 0.847 | 0.957 | (0.610, 1.501) |
| 7D-PP reports: pessimistic scenario (on last report available from 0–180 days period) | −0.301 | χ2(1) = 0.732 | 0.392 | 0.740 | (0.371, 1.478) |
| Taxonomy aspect | Element | KBA | HA |
|---|---|---|---|
| Domain | Therapeutic area | Smoking cessation | Smoking cessation |
| Target population | Current smokers willing to quit, speaking Mandarin Chinese | Current smokers willing to quit, speaking Mandarin Chinese | |
| Type of recommendation (items) | Text messages | Text messages | |
| Device interface | Android and iPhone mobile app | Android and iPhone mobile app | |
| Tailoring | Yes | Yes | |
| Country | Taiwan | Taiwan | |
| Methodology and procedures | Used metrics to assess performance | Self-reported smoking abstinence (7-day point prevalence), message appreciation, engagement (number of quitting attempts, number of rated messages, number of abstinence reports, number of days active in the app) | Self-reported smoking abstinence (7-day point prevalence), message appreciation, engagement (number of quitting attempts, number of rated messages, number of abstinence reports, number of days active in the app) |
| Number of test users | 181 | 190 | |
| Effectiveness on patients | Yes | Yes | |
| Success percentage | 7-day point prevalence: 3.4%- of 48.8% Message appreciation: 3.835/5 Mean number of: quitting attempts = 1.43, rated message = 3.59, abstinence reports = 1.1, days active in the app = 2.74 | 7-day point prevalence: 3.3–37.9% Message appreciation: 4.185/5 Mean number of: quitting attempts = 1.71, rated messages = 4.31, abstinence reports = 0.7, days active in the app: = 1.99 | |
| Duration of total intervention | 6 months | 6 months | |
| Number of sessions | Minimum: 1 (Maximum: 50 (estimated) | Minimum: 1 (Maximum: 50 (estimated) | |
| Electronic Health Record connection | No | No | |
| Cost-effectiveness | Not analyzed | Not analyzed | |
| Health promotion theoretical factors and behavior change theories | Attitude | Yes | Yes |
| Social influence | Yes | Yes | |
| Self-efficacy | Yes | Yes | |
| Action and Coping planning | Yes | Yes | |
| Supporting identity change | Yes | Yes | |
| Rewarding | Yes | Yes | |
| Advising on changing routines | Yes | Yes | |
| Advising on coping | Yes | Yes | |
| Advising on medication use | No | No | |
| Technical aspects | Recommendation interface | Top-N (N = 1) | Top-N (N = 1) |
| Recommendation technology | Attribute-based recommendations | Attribute-based recommendations + People-to-People correlation | |
| Finding recommendations | Selection options + request recommendation list | Selection options + request recommendation list | |
| Initial profile representation techniques | Manual | Manual | |
| Profile presentation technique | User-item feature matrix | User-item feature matrix, history-based model, user-item rating matrix, demographic features | |
| Profile learning technique | Not necessary | Not necessary | |
| Relevant feedback | Not necessary | Explicit feedback | |
| Profile adaptation technique | Manual | Manual | |
| Information filtering method | Knowledge-based | Hybrid: knowledge-based + demographic filtering | |
| User-profile item matching technique | Not applicable | Nearest neighbor (Pearson), Find similar users |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Hors-Fraile, S.; Candel, M.J.J.M.; Schneider, F.; Malwade, S.; Nunez-Benjumea, F.J.; Syed-Abdul, S.; Fernandez-Luque, L.; de Vries, H. Applying Collective Intelligence in Health Recommender Systems for Smoking Cessation: A Comparison Trial. Electronics 2022, 11, 1219. https://doi.org/10.3390/electronics11081219
Hors-Fraile S, Candel MJJM, Schneider F, Malwade S, Nunez-Benjumea FJ, Syed-Abdul S, Fernandez-Luque L, de Vries H. Applying Collective Intelligence in Health Recommender Systems for Smoking Cessation: A Comparison Trial. Electronics. 2022; 11(8):1219. https://doi.org/10.3390/electronics11081219
Chicago/Turabian StyleHors-Fraile, Santiago, Math J. J. M. Candel, Francine Schneider, Shwetambara Malwade, Francisco J. Nunez-Benjumea, Shabbir Syed-Abdul, Luis Fernandez-Luque, and Hein de Vries. 2022. "Applying Collective Intelligence in Health Recommender Systems for Smoking Cessation: A Comparison Trial" Electronics 11, no. 8: 1219. https://doi.org/10.3390/electronics11081219