1. Introduction
Arrhythmia is a critical condition, and nurses should be prepared for emergencies relating to it [
1]. In an emergency, healthcare providers must be sufficiently skilled to establish and share common knowledge in order to make informed decisions; however, multiple health professionals may have different priorities, thus training for optimal interprofessional interactions would ensure the best patient outcome by providing fast but accurate care in a cooperative manner [
2]. Knowing the importance of such issues, organizations such as the American Heart Association, Canadian Cardiovascular Society, and European Society of Cardiology [
3,
4] have provided guidelines for optimal care. These guidelines are best used when patient data are well collected and analyzed comprehensively, enabling care teams to arrive at an optimal decision [
5].
Findings from meta-analyses indicate that simulation-based learning is far more effective than traditional theory-based learning, improving competency and problem-solving ability [
3,
6]. Currently, high-fidelity simulators have been widely used in nursing schools to focus on reproducing symptoms of illnesses so that students can learn how to care for individual patients [
3]. A high-fidelity simulator is a computerized whole-body mannequin that can be programmed to provide dynamic physiological feedback and realistic responses [
7]. High fidelity alone, however, does not sufficiently build a clinical situation where diverse health professionals are able to collaborate in a large range of hospital environments.
“Team-based simulation (TBS)” has been introduced to foster collaborative teamwork and mimic possible challenges that may be encountered while working together with colleagues [
7,
8,
9]. TBS is aimed at establishing a collaborative learning environment in which students become proficient and actively participate in learning team care for complex health problems [
9]. Although the benefits of TB—which include improvements in learners’ knowledge, problem-solving skills, and critical thinking skills [
8]—have been well recognized, current nursing simulation-based education is subject to potential limitations and questions concerning the full engagement of all students involved. Due to high teacher–student ratios and spatial deficits, four to five students generally make up a group, a number that is unlikely to allow the necessary decision-making and interactions required between members [
10].
2. Methods
2.1. Simluation Intervention
The smart glass-based TBS consisted of four parts: (1) lecture, (2) students developing an algorithm for patient care, (3) team-based training, and (4) evaluation. Participants participated in a lecture for electrocardiogram (EKG) analysis, medication, and nursing care for patients with arrhythmia (
Table 2). Two scenarios of arrhythmia were introduced, and students were tasked with building a step-by-step algorithm including a decision-making process. Two scenarios of patients with arrhythmia (A-fib and paroxysmal supraventricular tachycardia) who were admitted for emergency care were used. The framework of the 15-h simulation was developed based on a previous study [
32] that included seven nursing skills and four to five incidents where students were required to perform nursing practice and make clinical decisions. Since the majority of students had little previous experience using smart glasses, instructions regarding this cooperation system were provided prior to simulation education.
Given the learning objective, which was to improve the ability to practice safe and quality care, the current simulation was designed to administer nursing interventions directly to a high-fidelity simulator; optimal clinical decisions for patients with arrythmia were taken as a team. In each scenario, there were four students in one group: two students played the role of remote supporters, who were in charge of sharing information with two bedside workers for optimal decision-making. Students were provided opportunities for repetitive training using augmented reality (AR), with the option to fix their algorithm. Four teams participated in the experience at a time; participants in three teams observed the performance of the team performing the simulation to correct their algorithm or practice communication and nursing skills for their simulation.
Participants exchanged their roles and completed one of two scenarios as remote supporters. Each scenario comprised five tasks, and a team was required to make five decisions. Depending on the capacity and teamwork, an individual scenario was run for 20–25 min. The duration was shortened as the participants repeated the practice.
Using checklists, each participant’s performance was assessed in terms of accuracy and adequacy of skill performance and decision-making process. The participants were provided a questionnaire regarding their experience with smart glass and overall simulation on completion of the TBS.
2.2. Development
Our system was composed of a trainee-side wearable system, supporter-side desktop system, and a network server (
Figure 1). The trainee-side wearable system comprised a GG, Bluetooth earphones, and a small mirror attached to the GG. The GG had a front camera, Bluetooth audio, and a touchpad. The supporter-side desktop system consisted of a desktop computer and headset, video conferencing application program to monitor the trainee, and image transmission program for sharing image files.
The trainee-side wearable system transmitted real-time video and audio captured from the trainee’s field of view through the GG, and received audio and image transmitted from the supporter-side system. We used Google Glass Enterprise Edition 2 (Glass EE2; Android Oreo 8.1). The supporter-side desktop system received the trainee’s video and enabled voice communication. We also developed software that could transmit images and text required for training by accessing the web RTC server using Google Chrome.
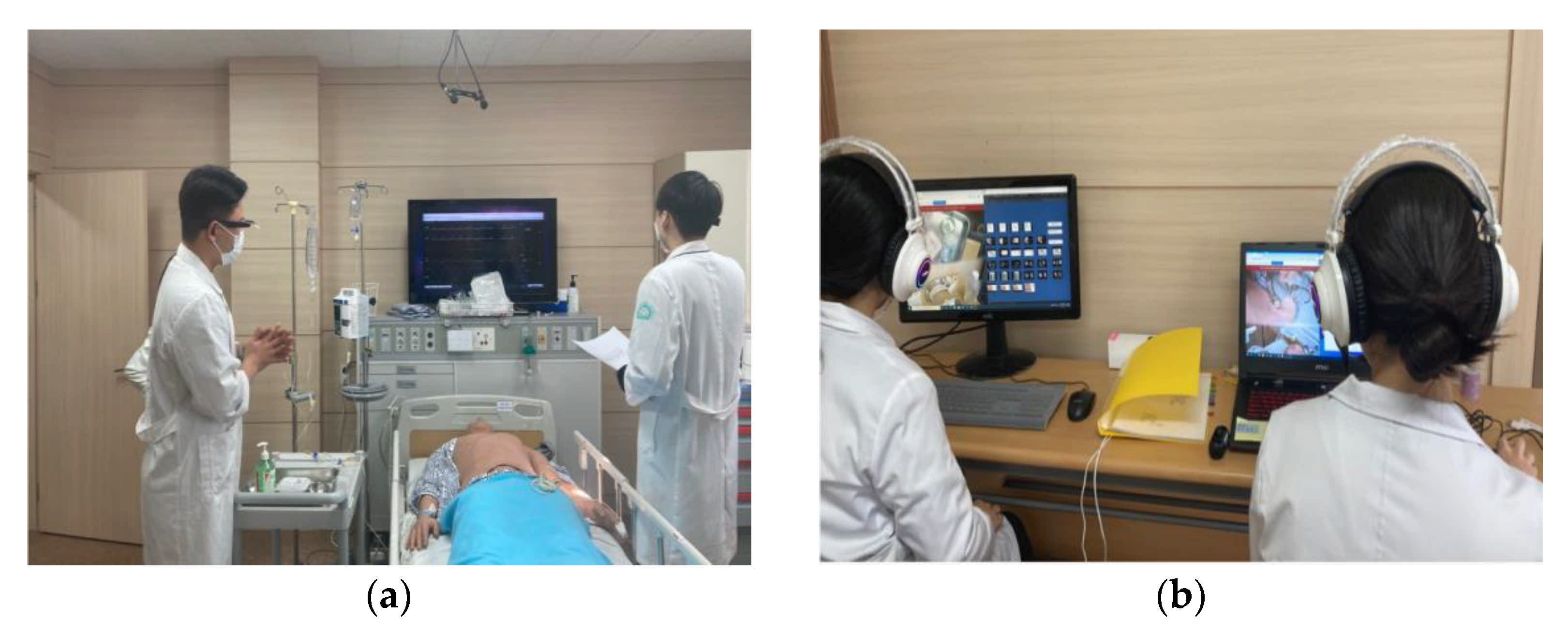
Our system was installed in two simulation rooms: the emergency intensive care and emergency support units (
Figure 2). The two trainees in the emergency intensive care unit wore a trainee-side wearable system and a high-fidelity patient simulator. The two remote supporters in the emergency support unit sat at the supporter-side desktop system. The supporters were able to use two desktop application programs: the image guide and the monitoring system. The image guide delivered selected images to the corresponding trainees and transmitted real-time video from the smart glasses to the supporter monitor.
The system supported one-way video communication and two-way audio communication, along with image and text message transmission. The video captured by the camera mounted on the trainee’s smart glass was transmitted to the supporter’s desktop through the webRTC server. While the supporter was able to attach a camera and transmit video, it was not transmitted to the trainee because the supporter’s appearance was not relevant to the simulation. The voice signal was acquired from the microphones in the trainee’s GlassEE2 and the headset worn by the supporter. Both voices were audible to each speaker. Trainees used Bluetooth earphones because several people were in the same room as them, while the supporters used headsets. The supporter sent images and text messages to help the trainee, which appeared on the display of the GlassEE2.
We developed a network-based data transmission program that transmitted images and text messages from the supporter system to the trainee system. It was developed using Unity3D (ver. 2018.3.14f1) for visualization on the desktop side, and a User Datagram Protocol socket was used for fast multi-party data transmission. If the supporter clicked on the image required by the trainee, the image was delivered to the trainee’s GlassEE2. The program also had a text box where the supporter could write a message to the trainee; when the supporter wrote a text message, it immediately appeared on the trainee’s GG and disappeared after a few seconds. The following procedure was set out for trainees and supporters participating in the experiment:
2.3. High-Fidelity Simulator
The METIman [
33] is a life-like human simulator that physically represents patients. With clinical features including breathing, pulse, heart and lung sounds, various scenarios of adults with heart disease can be simulated. Not only does the simulator show physical symptoms, but the monitor connected to the simulator displays associated signs (e.g., vital signs).
2.4. Sample
The study population included nursing students who attended a baccalaureate nursing program at a university located in J district, Korea. Thirty-two participants were recruited. After excluding one incomplete survey, data from 31 participants were used for statistical analysis. The purpose of this study was explained to all study participants and written informed consent was obtained.
2.5. Instrument
2.5.1. Usability
The instrument developed by Ingrassia et al. [
29] was used to evaluate feasibility and acceptability of the system. We revised the questionnaire according to the design and purpose of this study. The survey consisted of 54 questions spanning six categories: user input (12 items), system output (6 items), system usability (17 items), fidelity (8 items), immersivity (4 items), and likability (7 items). Using a 5-point Likert scale, the study participants provided ratings from 1 (strongly disagree) to 5 (strongly agree). There were four additional questions in which study participants rated their overall level of satisfaction from 1 (very dissatisfied) to 4 (very satisfied) regarding the smart glasses device, ease of use, system output, and smart glass-based simulation.
2.5.2. Attitudes towards the Interprofessional Health Care Team
The Attitudes Towards Interprofessional Health Care Teams Scale developed by Heinemann et al. [
34] and modified by Curran et al. [
35] was used to evaluate the effectiveness of the educational program. This scale consists of 14 items that include quality of care, time constraints, and teamwork among health professionals. This scale uses a 5-point Likert scale with values ranging from “strongly disagree” (1) to “strongly agree” (5).
2.5.3. Learning Satisfaction
Satisfaction with the education program was measured using the questionnaire used by Ji and Chung [
36]. A 5-point Likert scales was used, ranging from “not at all satisfied” (1) to “very satisfied” (5). A higher score indicated a higher level of satisfaction with the education program.
2.5.4. Essay Questionnaire
An essay questionnaire was used that asked the following seven qualitative questions to obtain in-depth information about user perceptions of the smart glass-based simulation education:
“How did you find the smart glass-based emergency simulation in general?”
“Was this program easy to use? What are the points that you thought needed further improvement?”
“Were there any difficulties or constraints when operating the system?”
“Do you think this smart glass-based simulation education would be useful for your future practice?”
“Do you think the smart glass would be useful in the clinical environment?”
“What are the components that require additional technical efforts for active application and continuous use of these smart glasses?”
“Please add any other comment on this program.”
2.6. Statistical Analysis
Statistical analysis was performed using the IBM SPSS Statistics version 25.0 (IBM Corp, Armonk, NY, USA) [
37]. For data analysis, frequency, percentage, mean, and standard deviation were calculated.
4. Discussion
The present study evaluated the usability and feasibility of adopting smart glasses for training of nursing skills and interprofessional interactions in emergency arrhythmia situations. The findings in this study indicate that participants attempted to use various features of the smart glasses to be actively engaged in team working and clinical decision-making to provide the best nursing care. The results of the current study provide evidence of the great potential for smart glasses in clinical settings and interprofessional interactions.
A majority of the students perceived TBS using smart glasses as a new, exciting, and interesting method for learning. This is in line with previous studies that have reported the incorporation of high-tech devices into education as promoting great interest among this digitally native generation [
38]. Given the clear roles within the simulation (bedside trainees or remote supporters), chances for participants to take part in team communication were greater, with greater responsibility on the remote supporters.
Among the subscales of attitudes toward interprofessional healthcare teams, the scores for the “quality of care” subscale were greater than those for the others. This could be related to the purpose of smart glass as a means of information sharing and interprofessional interactions that are intended to produce the best patient outcomes. Bedside trainees were connected to the remote supporter constantly and felt less bothered seeking for external help, which users found to be a helpful means of potentially addressing communication breakdown. Most features of the smart glasses are actually meant for a seamless flow of teamwork [
39], which be advantageous in emergency care settings where efficient and accurate interprofessional interactions are key to improved patient outcomes.
Generally, the users responded positively regarding the GG itself, expressing good feasibility for long-term use with a low level of physical discomfort experienced. One explanation may be that the weight of the GG EE2 is 46 g, which is relatively lighter than other smart glasses (65–350 g) [
40]. However, no previous studies have clearly reported wearability and comfortability of the GG; thus, further comparison studies could contribute to the physical design of wearable devices.
Interestingly, the discomfort experienced by some users was mostly related to the accessories, and only a few participants from previous studies had complaints regarding the physical aspects of the GG (short battery life, heavy weight, etc.) [
21,
22]. We used Bluetooth earphones and mirrors to compensate for the defects of the smart glasses, which users found to be superfluous. There was consistent frustration expressed by individuals wearing glasses, reporting discomfort due to the double-layering of glasses. Although one of the reasons why the GG was chosen was its lens-free design, it would be better to seek other smart glass solutions.
The findings of this study reveal that the participants were least satisfied with the system output, asking for better resolution and bigger screens. Wearable assistive technologies have different intended uses, environments, and trade-offs [
41,
42] as those in this study. In clinical settings, assistive devices should enable the wearer to seamlessly perform the clinical workflows of the main task, benefit from the hands-free potential of the device, and maintain sterile conditions [
43]. The small display of the GG limits the wearer’s peripheral vision and multitasking capabilities [
44] in terms of focus and attention to clinical tasks and workflows. In this study, we observed that the use of unfamiliar devices by inexperienced users within a tense situation could aggravate the difficulties related to the display; thus, it is suggested that sufficient time be provided for users to become accustomed to new devices.
The perceived usefulness of smart glass-based TBS for future clinical practice was high among the study participants. The current system was designed to focus on the exchange of information between remote supporters and bedside trainees, informing them of the high risks of medical errors from unskilled care providers [
45]; the participants of this study found the smart glasses to be of great use for interprofessional teamwork. Previous studies have also demonstrated that risk signs in patients were better detected when sharing patient monitoring via smart glasses [
43]. In addition, the smart glass was widely used as a supportive system for skill training, and a potential benefit to using these glasses in healthcare settings was identified in previous studies involving CPR [
46] and nursing skill training [
16]. When provided guidance via the smart glasses, trainees were able to improve their performances and achieve higher competency and success rates compared to those trained without smart glasses.
The participants reported low complexity of the simulation program, but some users complained of low compliance. Delayed audio was reported as an important concern that should be resolved. A previous study identified the requirements of low-latency applications for virtual reality (latency = 1 ms) and tele-surgery (1–10 ms) [
47]. Although there were concerns over network issue, this is an area where technology is growing rapidly. Therefore, the development additional smart glass-based interventions for education and clinical use is worthwhile.
Further consideration of user-centered interfaces may be the key to success in future system development. The principles of user-friendly interface design include an understanding the intended users and their needs [
48]. Users recommended the additional incorporation of visual status indicators due to the degree of uncertainty related to communication that was experienced within the current system. As this system was designed for use in emergency care settings, it is necessary to minimize the cognitive effort required to verify the actions of users.
Future Implications
Overall, the AR system used in this study achieved good usability and likability; users agreed on the potential of this innovative technology in nursing education and clinical practice. Considering the continuous progress in terms of technology, the introduction of new technology at an undergraduate level could foster an innovative and progressive atmosphere in future practice. Quality of care would benefit from the use of cutting edge technologies.
Unsatisfactory responses were generally related to user input, and mainly related to user comprehension of the system and ability to operate the device. In simulation education, no matter how easy it is to use the system, a task to which users are unaccustomed (and new methods of information delivery within an emergency scenario) may result in perceived complexity. At certain times, it is necessary to adapt oneself to new devices; putting individuals in complex situations with new devices may result in them having a negative impression towards the device. Nevertheless, when applying communication systems to clinical practice, the devices should not be distracting to the health professionals. Improvements reflecting user feedback are key to the successful implications of new technology in healthcare.
The user response regarding system output showed that understanding the target user is necessary for the system developer. The lack of integrity of the current system should be improved. When developing systems for clinical use, misleading users with wrong or inadequate information could lead to negative consequences related to patient safety. A multidisciplinary approach with various stakeholders will help further refine the system and ultimately lead to an optimal system for interprofessional interaction via smart glass in clinical settings.


 ,
, 




{kind=link}
{kind=link}
{kind=link}
{kind=link}