
Effects of Autologous Bone Marrow Mesenchymal Stem Cells and Platelet-Rich Plasma on Bone Regeneration and Osseointegration of a Hydroxyapatite-Coated Titanium Implant

 , , , , and
, , , , and
Abstract
:1. Introduction
1.1. Titanium Implants
1.2. Bone Marrow Mesenchymal Stem Cells and Platelet Rich Plasma
2. Material and Methods
2.1. In Vivo Study
2.2. Bone Marrow Stromal Cells (BMSCs)
2.3. Platelet-Rich Plasma (PRP) Gel
2.4. Growth Factor Measurements
2.5. Histology and Histomorphometry
2.6. Statistical Analyses
3. Results
3.1. Growth Factor Measurements
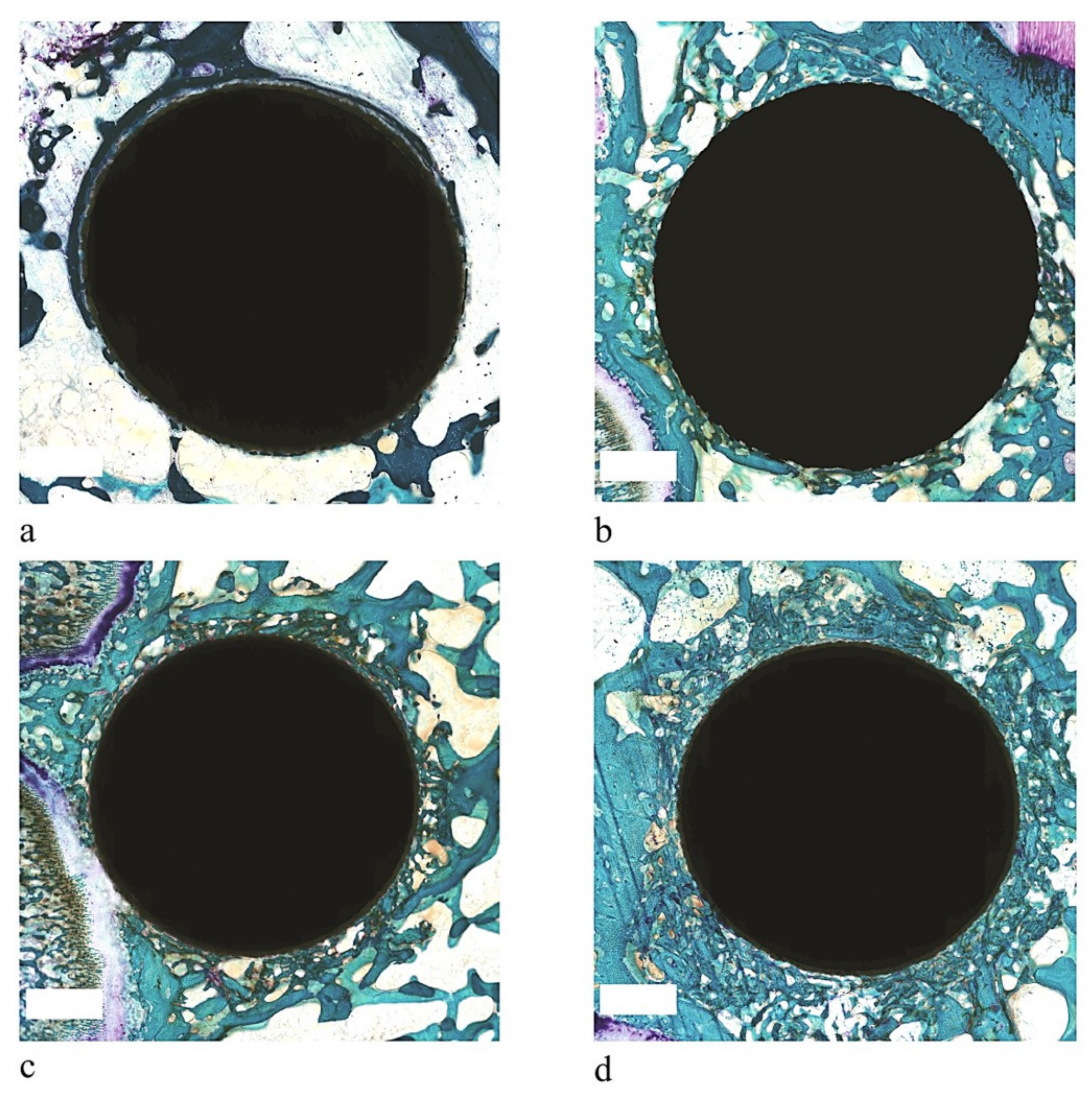
3.2. Histology
3.3. Histomorphometry
4. Discussion
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Kirmanidou, Y.; Sidira, M.; Drosou, M.-E.; Bennani, V.; Bakopoulou, A.; Tsouknidas, A.; Michailidis, N.; Michalakis, K. New Ti-Alloys and Surface Modifications to Improve the Mechanical Properties and the Biological Response to Orthopedic and Dental Implants: A Review. BioMed Res. Int. 2016, 2016, 1–21. [Google Scholar] [CrossRef] [Green Version]
- Liu, X.; Chu, P.K.; Ding, C. Surface modification of titanium, titanium alloys, and related materials for biomedical applications. Mater. Sci. Eng. R Rep. 2004, 47, 49–121. [Google Scholar] [CrossRef] [Green Version]
- Hartmann, E.S.; Köhler, M.I.; Huber, F.; Redeker, J.I.; Schmitt, B.; Schmitt-Sody, M.; Summer, B.; Fottner, A.; Jansson, V.; Mayer-Wagner, S. Factors regulating bone remodeling processes in aseptic implant loosening. J. Orthop. Res. 2017, 35, 248–257. [Google Scholar] [CrossRef] [Green Version]
- Overmann, A.L.; Aparicio, C.; Richards, J.T.; Mutreja, I.; Fischer, N.G.; Wade, S.M.; Potter, B.K.; Davis, T.A.; Bechtold, J.E.; Forsberg, J.A.; et al. Orthopaedic osseointegration: Implantology and future directions. J. Orthop. Res. 2019, 38, 1445–1454. [Google Scholar] [CrossRef]
- Ahn, T.K.; Lee, D.H.; Kim, T.; Jang, G.C.; Choi, S.; Oh, J.B.; Ye, G.; Lee, S. Modification of Titanium Implant and Titanium Dioxide for Bone Tissue Engineering. In Novel Biomaterials for Regenerative Medicine; Chun, H.J., Park, K., Kim, C.-H., Khang, G., Eds.; Springer: Singapore, 2018; Volume 1077, pp. 355–368. [Google Scholar]
- Heimann, R.B. Osseoconductive and Corrosion-Inhibiting Plasma-Sprayed Calcium Phosphate Coatings for Metallic Medical Implants. Metals 2017, 7, 468. [Google Scholar] [CrossRef] [Green Version]
- Lombardi, A.V.; Berend, K.R.; Mallory, T.H. Hydroxyapatite-coated Titanium Porous Plasma Spray Tapered Stem: Experience at 15 to 18 Years. Clin. Orthop. Relat. Res. 2006, 453, 81–85. [Google Scholar] [CrossRef] [PubMed]
- Fu, T.; Li, H.; Sun, J.; Li, G.; Li, W.; Zhang, H. Facile hydrothermal synthesis of TiO2–CaP nano-films on Ti6Al4V alloy. Trans. Nonferrous Met. Soc. China 2015, 25, 1122–1127. [Google Scholar] [CrossRef]
- Fini, M.; Filardo, G.; Tschon, M.; Pischedda, M.; Pacorini, A.; Kon, E.; Giardino, R. Regenerative medicine for the treatment of musculoskeletal overuse injuries in competition horses. Int. Orthop. 2011, 35, 1569–1576. [Google Scholar] [CrossRef] [Green Version]
- Weibrich, G.; Hansen, T.; Kleis, W.; Buch, R.; Hitzler, W.E. Effect of platelet concentration in platelet-rich plasma on peri-implant bone regeneration. Bone 2004, 34, 665–671. [Google Scholar] [CrossRef] [PubMed]
- Jensen, T.B.; Rahbek, O.; Overgaard, S.; Søballe, K. Platelet rich plasma and fresh frozen bone allograft as enhancement of implant fixation an experimental study in dogs. J. Orthop. Res. 2004, 22, 653–658. [Google Scholar] [CrossRef] [PubMed]
- Roldán, J.; Jepsen, S.; Miller, J.; Freitag, S.; Rueger, D.C.; Açil, Y.; Terheyden, H. Bone formation in the presence of platelet-rich plasma vs. bone morphogenetic protein-7. Bone 2004, 34, 80–90. [Google Scholar] [CrossRef] [PubMed]
- Mazor, Z.; Peleg, M.; Garg, A.K.; Luboshitz, J. Platelet-Rich Plasma for Bone Graft Enhancement in Sinus Floor Augmentation With Simultaneous Implant Placement: Patient Series Study. Implant. Dent. 2004, 13, 65–72. [Google Scholar] [CrossRef] [PubMed]
- Fontana, S.; Olmedo, D.G.; Linares, J.A.; Guglielmotti, M.B.; Crosa, M.E. Effect of Platelet-Rich Plasma on the Peri-implant Bone Response::An Experimental Study. Implant Dent. 2004, 13, 73–78. [Google Scholar] [CrossRef]
- Yin, D.; Wang, Z.; Gao, Q.; Sundaresan, R.; Parrish, C.; Yang, Q.; Krebsbach, P.H.; Lichtler, A.C.; Rowe, D.W.; Hock, J.; et al. Determination of the Fate and Contribution of Ex Vivo Expanded Human Bone Marrow Stem and Progenitor Cells for Bone Formation by 2.3ColGFP. Mol. Ther. 2009, 17, 1967–1978. [Google Scholar] [CrossRef] [PubMed]
- Jäger, M.; Hernigou, P.; Zilkens, C.; Herten, M.; Li, X.; Fischer, J.; Krauspe, R. Cell therapy in bone healing disorders. Orthop. Rev. 2010, 2, e20. [Google Scholar] [CrossRef] [Green Version]
- Livingston, T.L.; Gordon, S.; Archambault, M.; Kadiyala, S.; McIntosh, K.; Smith, A.; Peter, S.J. Mesenchymal stem cells combined with biphasic calcium phosphate ceramics promote bone regeneration. J. Mater. Sci. Mater. Electron. 2003, 14, 211–218. [Google Scholar] [CrossRef] [PubMed]
- Mankani, M.H.; Kuznetsov, S.A.; Robey, P.G. Formation of hematopoietic territories and bone by transplanted human bone marrow stromal cells requires a critical cell density. Exp. Hematol. 2007, 35, 995–1004. [Google Scholar] [CrossRef]
- Fang, D.; Seo, B.-M.; Liu, Y.; Sonoyama, W.; Yamaza, T.; Zhang, C.; Wang, S.; Shi, S. Transplantation of Mesenchymal Stem Cells Is an Optimal Approach for Plastic Surgery. Stem Cells 2007, 25, 1021–1028. [Google Scholar] [CrossRef]
- Stanovici, J.; Le Nail, L.-R.; Brennan, M.Á.; Vidal, L.; Trichet, V.; Rosset, P.; Layrolle, P. Bone regeneration strategies with bone marrow stromal cells in orthopaedic surgery. Curr. Res. Transl. Med. 2016, 64, 83–90. [Google Scholar] [CrossRef]
- Brennan, M.Á.; Renaud, A.; Amiaud, J.; Rojewski, M.T.; Schrezenmeier, H.; Heymann, D.; Trichet, V.; Layrolle, P. Pre-clinical studies of bone regeneration with human bone marrow stromal cells and biphasic calcium phosphate. Stem Cell Res. Ther. 2014, 5, 114. [Google Scholar] [CrossRef] [Green Version]
- Dong, Y.; Chen, X.; Hong, Y. Tissue-Engineered Bone Formation In Vivo for Artificial Laminae of the Vertebral Arch Using β-Tricalcium Phosphate Bioceramics Seeded With Mesenchymal Stem Cells. Spine 2013, 38, E1300–E1306. [Google Scholar] [CrossRef]
- Hernigou, P.; Poignard, A.; Beaujean, F.; Rouard, H. Percutaneous Autologous Bone-Marrow Grafting for NonunionsInfluence of the Number and Concentration of Progenitor Cells. J. Bone Jt. Surg. Am. Vol. 2005, 87, 1430–1437. [Google Scholar] [CrossRef]
- Schottel, P.C.; Warner, S.J. Role of Bone Marrow Aspirate in Orthopedic Trauma. Orthop. Clin. N. Am. 2017, 48, 311–321. [Google Scholar] [CrossRef]
- Lieberman, J.R.; Daluiski, A.; Einhorn, T.A. The role of growth factors in the repair of bone. J. Bone Jt. Surg. Am. Vol. 2002, 84, 1032–1044. [Google Scholar] [CrossRef]
- Tschon, M.; Fini, M.; Giardino, R.; Filardo, G.; Dallari, D.; Torricelli, P.; Martini, L.; Giavaresi, G.; Kon, E.; Maltarello, M.C.; et al. Lights and shadows concerning platelet products for musculoskeletal regeneration. Front. Biosci. 2011, E3, 96–107. [Google Scholar] [CrossRef] [Green Version]
- Cole, B.J.; Seroyer, S.T.; Filardo, G.; Bajaj, S.; Fortier, L.A. Platelet-Rich Plasma: Where Are We Now and Where Are We Going? Sports Health A Multidiscip. Approach 2010, 2, 203–210. [Google Scholar] [CrossRef]
- Salamanna, F.; Veronesi, F.; Maglio, M.; Della Bella, E.; Sartori, M.; Fini, M. New and Emerging Strategies in Platelet-Rich Plasma Application in Musculoskeletal Regenerative Procedures: General Overview on Still Open Questions and Outlook. BioMed Res. Int. 2015, 2015, 1–24. [Google Scholar] [CrossRef] [PubMed]
- Veronesi, F.; Fini, M.; Sartori, M.; Parrilli, A.; Martini, L.; Tschon, M. Pulsed electromagnetic fields and platelet rich plasma alone and combined for the treatment of wear-mediated periprosthetic osteolysis: An in vivo study. Acta Biomater. 2018, 77, 106–115. [Google Scholar] [CrossRef]
- Heldin, C.-H.; Westermark, B. PDGF-like growth factors in autocrine stimulation of growth. J. Cell. Physiol. 1987, 133, 31–34. [Google Scholar] [CrossRef] [PubMed]
- Andrew, J.G.; Hoyland, J.A.; Freemont, A.J.; Marsh, D.R. Platelet-derived growth factor expression in normally healing human fractures. EMC Cardiol. Angéiologie 1995, 16, 455–460. [Google Scholar] [CrossRef]
- Crane, J.L.; Cao, X. Bone marrow mesenchymal stem cells and TGF-β signaling in bone remodeling. J. Clin. Investig. 2014, 124, 466–472. [Google Scholar] [CrossRef] [Green Version]
- Barry, F.; Boynton, R.E.; Liu, B.; Murphy, J.M. Chondrogenic Differentiation of Mesenchymal Stem Cells from Bone Marrow: Differentiation-Dependent Gene Expression of Matrix Components. Exp. Cell Res. 2001, 268, 189–200. [Google Scholar] [CrossRef]
- Gerber, H.-P.; Vu, T.H.; Ryan, A.M.; Kowalski, J.; Werb, Z.; Ferrara, N. VEGF couples hypertrophic cartilage remodeling, ossification and angiogenesis during endochondral bone formation. Nat. Med. 1999, 5, 623–628. [Google Scholar] [CrossRef] [PubMed]
- Maes, C.; Stockmans, I.; Moermans, K.; Van Looveren, R.; Smets, N.; Carmeliet, P.; Bouillon, R.; Carmeliet, G. Soluble VEGF isoforms are essential for establishingepiphyseal vascularization and regulating chondrocyte development and survival. J. Clin. Investig. 2004, 113, 188–199. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Wright, V.; Usas, A.; Gearhart, B.; Shen, H.-C.; Cummins, J.; Huard, J. Synergistic enhancement of bone formation and healing by stem cell–expressed VEGF and bone morphogenetic protein-4. J. Clin. Investig. 2002, 110, 751–759. [Google Scholar] [CrossRef] [PubMed]
- Peng, H.; Usas, A.; Olshanski, A.; Ho, A.M.; Gearhart, B.; Cooper, G.M.; Huard, J. VEGF Improves, Whereas sFlt1 Inhibits, BMP2-Induced Bone Formation and Bone Healing Through Modulation of Angiogenesis. J. Bone Miner. Res. 2005, 20, 2017–2027. [Google Scholar] [CrossRef] [PubMed]
- Oryan, A.; Alidadi, S.; Moshiri, A. Platelet-rich plasma for bone healing and regeneration. Expert Opin. Biol. Ther. 2015, 16, 213–232. [Google Scholar] [CrossRef]
- Eskan, M.A.; Greenwell, H.; Hill, M.; Morton, D.; Vidal, R.; Shumway, B.; Girouard, M.-E. Platelet-Rich Plasma–Assisted Guided Bone Regeneration for Ridge Augmentation: A Randomized, Controlled Clinical Trial. J. Periodontol. 2014, 85, 661–668. [Google Scholar] [CrossRef] [PubMed]
- Liebig, B.E.; Kisiday, J.D.; Bahney, C.S.; Ehrhart, N.P.; Goodrich, L.R. The platelet-rich plasma and mesenchymal stem cell milieu: A review of therapeutic effects on bone healing. J. Orthop. Res. 2020, 38, 2539–2550. [Google Scholar] [CrossRef]
- Kasten, P.; Vogel, J.; Geiger, F.; Niemeyer, P.; Luginbühl, R.; Szalay, K. The effect of platelet-rich plasma on healing in critical-size long-bone defects. Biomaterials 2008, 29, 3983–3992. [Google Scholar] [CrossRef]
- Yamada, Y.; Ueda, M.; Naiki, T.; Takahashi, M.; Hata, K.-I.; Nagasaka, T. Autogenous Injectable Bone for Regeneration with Mesenchymal Stem Cells and Platelet-Rich Plasma: Tissue-Engineered Bone Regeneration. Tissue Eng. 2004, 10, 955–964. [Google Scholar] [CrossRef]
- Qi, Y.; Niu, L.; Zhao, T.; Shi, Z.; Di, T.; Feng, G.; Li, J.; Huang, Z. Combining mesenchymal stem cell sheets with platelet-rich plasma gel/calcium phosphate particles: A novel strategy to promote bone regeneration. Stem Cell Res. Ther. 2015, 6, 1–16. [Google Scholar] [CrossRef] [Green Version]
- Yu, T.; Pan, H.; Hu, Y.; Tao, H.; Wang, K.; Zhang, C. Autologous platelet-rich plasma induces bone formation of tissue-engineered bone with bone marrow mesenchymal stem cells on beta-tricalcium phosphate ceramics. J. Orthop. Surg. Res. 2017, 12, 178. [Google Scholar] [CrossRef] [Green Version]
- Kitoh, H.; Kitakoji, T.; Tsuchiya, H.; Katoh, M.; Ishiguro, N. Transplantation of culture expanded bone marrow cells and platelet rich plasma in distraction osteogenesis of the long bones. Bone 2007, 40, 522–528. [Google Scholar] [CrossRef] [PubMed]
- Filho Cerruti, H.; Kerkis, I.; Kerkis, A.; Tatsui, N.H.; da Costa Neves, A.; Bueno, D.F.; Da Silva, M.C.P. Allogenous Bone Grafts Improved by Bone Marrow Stem Cells and Platelet Growth Factors: Clinical Case Reports. Artif. Organs 2007, 31, 268–273. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, S.; Tsuchiya, S.; Hirakawa, A.; Kato, K.; Ando, M.; Mizuno, M.; Osugi, M.; Okabe, K.; Katagiri, W.; Hibi, H. Design of a Randomized Controlled Clinical Study of tissue-engineered osteogenic materials using bone marrow-derived mesenchymal cells for Maxillomandibular bone defects in Japan: The TEOM study protocol. BMC Oral Health 2019, 19, 1–8. [Google Scholar] [CrossRef] [Green Version]
- Tobita, M.; Uysal, C.A.; Guo, X.; Hyakusoku, H.; Mizuno, H. Periodontal tissue regeneration by combined implantation of adipose tissue-derived stem cells and platelet-rich plasma in a canine model. Cytotherapy 2013, 15, 1517–1526. [Google Scholar] [CrossRef]
- Yamada, Y.; Nakamura, S.; Ueda, M.; Ito, K. Osteotome technique with injectable tissue-engineered bone and simultaneous implant placement by cell therapy. Clin. Oral Implant. Res. 2011, 24, 468–474. [Google Scholar] [CrossRef] [PubMed]
- Kasper, G.; Mao, L.; Geißler, S.; Draycheva, A.; Trippens, J.; Kühnisch, J.; Tschirschmann, M.; Kaspar, K.; Perka, C.; Duda, G.N.; et al. Insights into Mesenchymal Stem Cell Aging: Involvement of Antioxidant Defense and Actin Cytoskeleton. Stem Cells 2009, 27, 1288–1297. [Google Scholar] [CrossRef] [PubMed]
- Geissler, S.; Textor, M.; Kühnisch, J.; Könnig, D.; Klein, O.; Ode, A.; Pfitzner, T.; Adjaye, J.; Kasper, G.; Duda, G.N. Functional Comparison of Chronological and In Vitro Aging: Differential Role of the Cytoskeleton and Mitochondria in Mesenchymal Stromal Cells. PLoS ONE 2012, 7, e52700. [Google Scholar] [CrossRef] [Green Version]
- Yukata, K.; Xie, C.; Li, T.-F.; Takahata, M.; Hoak, D.; Kondabolu, S.; Zhang, X.; Awad, H.A.; Schwarz, E.M.; Beck, C.A.; et al. Aging periosteal progenitor cells have reduced regenerative responsiveness to bone injury and to the anabolic actions of PTH 1-34 treatment. Bone 2014, 62, 79–89. [Google Scholar] [CrossRef] [Green Version]
- D’Ippolito, G.; Schiller, P.C.; Ricordi, C.; Roos, B.A.; Howard, G.A. Age-Related Osteogenic Potential of Mesenchymal Stromal Stem Cells from Human Vertebral Bone Marrow. J. Bone Miner. Res. 1999, 14, 1115–1122. [Google Scholar] [CrossRef]
- Lu, C.; Hansen, E.; Sapozhnikova, A.; Hu, D.; Miclau, T.; Marcucio, R.S. Effect of age on vascularization during fracture repair. J. Orthop. Res. 2008, 26, 1384–1389. [Google Scholar] [CrossRef] [Green Version]
- Checa, S.; Hesse, B.; Roschger, P.; Aido, M.; Duda, G.N.; Raum, K.; Willie, B.M. Skeletal maturation substantially affects elastic tissue properties in the endosteal and periosteal regions of loaded mice tibiae. Acta Biomater. 2015, 21, 154–164. [Google Scholar] [CrossRef]
- Aido, M.; Kerschnitzki, M.; Hoerth, R.; Checa, S.; Spevak, L.; Boskey, A.L.; Fratzl, P.; Duda, G.N.; Wagermaier, W.; Willie, B.M. Effect of in vivo loading on bone composition varies with animal age. Exp. Gerontol. 2015, 63, 48–58. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, T.W.; Muschler, G.F. Bone graft materials. An overview of the basic science. Clin. Orthop. Relat. Res. 2000, 371, 10–27. [Google Scholar] [CrossRef]
- Veronesi, F.; Giavaresi, G.; Tschon, M.; Borsari, V.; Aldini, N.N.; Fini, M. Clinical Use of Bone Marrow, Bone Marrow Concentrate, and Expanded Bone Marrow Mesenchymal Stem Cells in Cartilage Disease. Stem Cells Dev. 2013, 22, 181–192. [Google Scholar] [CrossRef]
- Gobbi, A.; Fishman, M. Platelet-rich Plasma and Bone Marrow–derived Mesenchymal Stem Cells in Sports Medicine. Sports Med. Arthrosc. Rev. 2016, 24, 69–73. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vogel, J.P.; Szalay, K.; Geiger, F.; Kramer, M.; Richter, W.; Kasten, P. Platelet-rich plasma improves expansion of human mesenchymal stem cells and retains differentiation capacity andin vivobone formation in calcium phosphate ceramics. Platelets 2006, 17, 462–469. [Google Scholar] [CrossRef] [PubMed]
- Yun, J.-H.; Han, S.-H.; Choi, S.-H.; Lee, M.-H.; Lee, S.-J.; Song, S.U.; Oh, N. Effects of bone marrow-derived mesenchymal stem cells and platelet-rich plasma on bone regeneration for osseointegration of dental implants: Preliminary study in canine three-wall intrabony defects. J. Biomed. Mater. Res. Part B Appl. Biomater. 2014, 102, 1021–1030. [Google Scholar] [CrossRef]
- Rodrigues, M.; Griffith, L.G.; Wells, A. Growth factor regulation of proliferation and survival of multipotential stromal cells. Stem Cell Res. Ther. 2010, 1, 1–12. [Google Scholar] [CrossRef] [Green Version]
- Hua, P.; Liu, J.-Y.; Tao, J.; Yang, S.-R. Application and Progress of Combined Mesenchymal Stem Cell Transplantation in the Treatment of Ischemic Cardiomyopathy. BioMed Res. Int. 2015, 2015, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wiafe, B.; Metcalfe, P.D.; Adesida, A.B. Stem Cell Therapy: Current Applications and Potential for Urology. Curr. Urol. Rep. 2015, 16, 77. [Google Scholar] [CrossRef] [PubMed]
- Rubio-Azpeitia, E.; Andia, I. Partnership between platelet-rich plasma and mesenchymal stem cells: In vitro experi-ence. Muscles Ligaments Tendons J. 2014, 4, 52–62. [Google Scholar] [CrossRef] [PubMed]
- Lana, J.F.S.D.; da Fonseca, L.F.; Macedo, R.D.R.; Mosaner, T.; Murrell, W.; Kumar, A.; Purita, J.; de Andrade, M.A.P. Platelet-rich plasma vs bone marrow aspirate concentrate: An overview of mechanisms of action and orthobiologic synergistic effects. World J. Stem Cells 2021, 13, 155–167. [Google Scholar] [CrossRef] [PubMed]




{kind=link}
{kind=link}
{kind=link}
| GFs | Plasma | iPRP | aPRP |
|---|---|---|---|
| TGF-β1 (ng/mL) | 52 ± 13 | 175 ± 28 a | 401 ± 174 b,c |
| PDGF-AB (ng/mL) | 8 ± 1 | 28 ± 6 | 116 ± 34 b,c |
| VEGF (ng/mL) | 230 ± 23 | 382 ± 75 d | 817 ± 74 b,c |
| IL-1β (mg/mL) | 0.8 ± 0.2 | 1.3 ± 0.5 | 6.0 ± 1.0 b,c |
| Parameters | Implants | |||
|---|---|---|---|---|
| Ti-HA | Ti-HA + PRP | Ti-HA + BMSC | Ti-HA + BMSC + PRP | |
| BIC (%) | 53.7 ± 2.5 | 51.2 ± 7.0 | 61.6 ± 1.4 | 71.5 ± 2.0 * |
| BV/TV (%) | 51.6 ± 0.2 | 64.1 ± 3.7 * | 67.8 ± 1.3 ** | 79.3 ± 3.3 *** |
| Os.V/BV (%) | 0.4 ± 0.1 | 1.0 ± 0.1 * | 1.1 ± 0.4 * | 2.5 ± 0.3 * |
| Os.S/BS (%) | 1.4 ± 0.7 | 2.8 ± 0.6 | 5.4 ± 1.0 * | 21.9 ± 4.7 ** |
| Os.Th (μm) | 6.8 ± 2.8 | 14.2 ± 1.1 | 13.5 ± 3.5 | 17.2 ± 1.3 * |
| N.Ob/BS (n/mm2) | 14.6 ± 6.0 | 40.7 ± 2.4 * | 32.1 ± 1.7 * | 59.0 ± 7.8 *, ** |
| Parameters | Implants | |||
|---|---|---|---|---|
| Ti-HA | Ti-HA + PRP | Ti-HA + BMSC | Ti-HA + BMSC + PRP | |
| BIC (%) | 55.6 ± 2.1 | 63.3 ± 5.3 | 65. 6 ± 4.2 | 81.7 ± 2.5 *** |
| BV/TV (%) | 52.9 ± 0.6 | 68.8 ± 0.4 ** | 71.5 ± 2.0 ** | 85.3 ± 4.4 ***, ** |
| Os.V/BV (%) | 0.1 ± 0.0 | 0.6 ± 0.0 *** | 0.5 ± 0.1 ** | 0.6 ± 0.1 *** |
| Os.S/BS (%) | 0.9 ± 0.1 | 5.2 ± 0.3 * | 6.6 ± 1.8 * | 5.7 ± 1.6 ** |
| Os.Th (μm) | 2.9 ± 4.4 | 9.9 ± 0.2 | 9.2 ± 1.0 | 11.8 ± 1.5 ** |
| N.Ob/BS (n/mm2) | 6.3 ± 2.9 | 36.9 ± 0.1 | 28.9 ± 0.6 | 50.7 ± 4.9 ***, ** |
| MAR (μm/day) | 1.4 ± 0.3 | 2.4 ± 0.2 *** | 2.5 ± 0.1 *** | 3.0 ± 0.4 ***, * |
| BFR/BS (μm2/μm3/day) | 0.6 ± 0.1 | 1.6 ± 0.4 ** | 1.7 ± 0.1 ** | 3.3 ± 0.6 *** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salamanna, F.; Del Piccolo, N.; Sartori, M.; Giavaresi, G.; Martini, L.; Di Sante, G.; Stagni, C.; Dallari, D.; Fini, M. Effects of Autologous Bone Marrow Mesenchymal Stem Cells and Platelet-Rich Plasma on Bone Regeneration and Osseointegration of a Hydroxyapatite-Coated Titanium Implant. Coatings 2021, 11, 840. https://doi.org/10.3390/coatings11070840
Salamanna F, Del Piccolo N, Sartori M, Giavaresi G, Martini L, Di Sante G, Stagni C, Dallari D, Fini M. Effects of Autologous Bone Marrow Mesenchymal Stem Cells and Platelet-Rich Plasma on Bone Regeneration and Osseointegration of a Hydroxyapatite-Coated Titanium Implant. Coatings. 2021; 11(7):840. https://doi.org/10.3390/coatings11070840
Chicago/Turabian StyleSalamanna, Francesca, Nicolandrea Del Piccolo, Maria Sartori, Gianluca Giavaresi, Lucia Martini, Giuseppe Di Sante, Cesare Stagni, Dante Dallari, and Milena Fini. 2021. "Effects of Autologous Bone Marrow Mesenchymal Stem Cells and Platelet-Rich Plasma on Bone Regeneration and Osseointegration of a Hydroxyapatite-Coated Titanium Implant" Coatings 11, no. 7: 840. https://doi.org/10.3390/coatings11070840