
Role of Melatonin in Bone Remodeling around Titanium Dental Implants: Meta-Analysis
by
 , ,
, ,
Nansi López-Valverde
1 ,
,
Beatriz Pardal-Peláez
1,
Antonio López-Valverde
1,* and
Juan Manuel Ramírez
2 1
Department of Surgery, Instituto de Investigación Biomédica de Salamanca (IBSAL), University of Salamanca, 37007 Salamanca, Spain
2
Department of Morphological Sciences, University of Cordoba, Avenida Meneéndez Pidal S/N, 14071 Cordoba, Spain
*
Author to whom correspondence should be addressed.
Coatings 2021, 11(3), 271; https://doi.org/10.3390/coatings11030271
Submission received: 15 January 2021
/
Revised: 15 February 2021
/
Accepted: 20 February 2021
/
Published: 25 February 2021
(This article belongs to the Special Issue Bioactive Coatings for Implantable Devices)
Abstract
:The theory, known as the “brain-bone axis” theory, involves the central nervous system in bone remodeling. The alteration of the nervous system could lead to abnormal bone remodeling. Melatonin produced by the pineal gland is a hormone that is characterized by its antioxidant properties. The aim of this meta-analysis was to examine the role of melatonin in the growth of new bone around titanium dental implants in vivo. A manual search of the PubMed and Web of Science databases was conducted to identify scientific studies published until November 2020. We included randomized clinical trials (RCTs) and animal studies where melatonin was used with titanium implants. Fourteen studies met the inclusion criteria. Quality was assessed using the Jadad scale and SYRCLE’s risk of bias tool. Our meta-analysis revealed that the use of melatonin during implant placement improves bone-to-implant contact percentages in animals (difference of means, random effects: 9.59 [95% CI: 5.53–13.65]), reducing crestal bone loss in humans (difference in means, random effects: −0.55 [95% CI: 1.10–0.00]). In animals, titanium implants using melatonin increase bone-to-implant contact surface 2–6 weeks after their placement and reduce crestal bone loss in humans following six months. The results of this meta-analysis should be taken with caution, due to the small samples and the large heterogeneity among studies.
1. Introduction
The first description of osseointegration was provided by Brånemark and colleagues [1] more than 50 years ago, and to date, this process still remains unexplored. One of the theories posed in recent years, referred to as the “brain-bone axis theory” by certain authors [2], has drawn particular interest. It suggests the involvement of the sympathetic nervous system (SNS) in bone remodeling, claiming the need for the autonomic nervous system to be undamaged in order to contribute to the maintenance of healthy bone tissue, with its alteration leading to possible anomalies in bone remodeling [3,4]. This remodeling process would be mainly controlled by neurotransmitters (noradrenaline, serotonin and dopamine), and growth hormones secreted by the pituitary gland could stimulate osteoblast and osteoclast proliferation, which plays a crucial part in the bone formation-destruction balance [5,6].
It has been proven that the group of glucose-sensing neurons in the hypothalamic arcuate nucleus makes control of the skeleton by the brain possible [7], and that long-term use of certain central nervous depressant drugs causes a reduction in bone mass that results in osteoporosis, and therefore in high rates of dental implant failure in patients under treatment with such drugs [8].
The biofunctionalization of a certain biomaterial consists of modifying the physicochemical characteristics of its surface, which improves a body’s biological response when it comes into contact with it, despite the fact that there are other factors that influence the creation of an adequate surface bone-implant contact, such as bone quality or proper surgical technique [9,10,11].
In recent decades, different techniques to improve titanium (Ti) surface topography and promote osseointegration have been developed, since Ti surfaces have no antioxidant properties and the cells that grow on the surface may be under permanent oxidative stress [12]. Current research is focused on obtaining surfaces that may achieve better and faster osseointegration through morphological or biochemical modification [13,14].
Melatonin (MT) (Melatonin, N-acetyl 5-methoxytriptamine) is a hormone that is mainly synthetized in the pineal gland. It is regarded as a relevant mediator of angiogenesis and bone formation due to its antioxidant effects, its production being precisely modulated under the influence of the hypothalamus [15,16,17]. Previous studies have assessed its anti-inflammatory properties, as well as its relevant role in peri-implant bone formation [18,19,20,21], all due to its extraordinary capacity to destroy reactive oxygen species [22]. In this regard, the benefits of its topical application on post-extraction sockets and before dental surgery to prevent bisphosphonate-related osteonecrosis have also been noted [23]. However, it should be noted that despite this knowledge, the clinical application of antioxidant therapies and surface biofunctionalization in this respect to enhance dental-implant surgery is very limited.
The purpose of our study was to carry out a systematic review of the literature related to bone growth and remodeling around Ti dental implants, combined with MT.
2. Materials and Methods
Eligible studies were selected according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) guidelines for systematic reviews and meta-analysis [24] (Table S1, Checklist).
2.1. Protocol
The Population, Intervention, Comparison and Outcome framework (PICO) was used as a basis to formulate the research question, which was: “The inclusion of melatonin in dental implant surgery: does it influence osseointegration?”.
(P) Participants: the subjects received endo-bone implant placement. (I) Interventions: implants including melatonin. (C) Control: implants without melatonin. (O) Outcome: Bone-to-Implant Contact (BIC) (in animal studies) and Marginal Bone Level (MBL) in randomized clinical trials (RCTs).
2.2. Data Sources and Search Strategy
The PubMed and Web of Science electronic databases were searched for findings published in the last 15 years until November 2020. The search terms used were: “titanium dental implants AND melatonin surface”; “melatonin AND dental implants”; and “melatonin AND dental implants AND bone formation”. The Boolean operator “AND” was used to combine the searches.
2.3. Inclusion and Exclusion Criteria
The inclusion criteria for the study selection were:
- Randomized clinical trials and animal studies on Ti implants, with and without the incorporation of melatonin.
- Randomized clinical trials and animal studies that reported bone-implant contact percentages, with and without the incorporation of melatonin.
- Studies with a minimum of six implants/group.
The exclusion criteria for the study selection were:
- In vitro studies.
- Narrative and systematic reviews.
- Clinical cases.
- Studies that assessed the effectiveness of melatonin in bone regeneration without including dental implants, duplicates and those that failed to meet the inclusion criteria.
2.4. Data Extraction and Analysis
Those articles that failed to address the research question were removed. The correponding titles and abstracts of the eligible articles were taken, and two reviewers (NL-V and AL-V) separately drew up a selection of them. The reviewers discussed and solved the discrepancies over the choice of articles that arose. The full versions of the chosen articles were then obtained for review and inclusion.
2.5. Risk of Bias (RoB) of the Selected Articles
The methodology of the scientific evidence gathered in the selected studies was assessed using SYRCLE’s risk of bias tool (an adapted version of the Cochrane RoB tool, with specific biases in animal studies) [25].
2.6. Quality of the Reports of the Selected Articles
This assessment was based on the provided ARRIVE (Animal Research: Reporting of In Vivo Experiments) guidelines [26], with a total of 23 items. The reviewers, N.L.-V. and A.L.-V., allocated each item a score of 0 (not reported) or 1 (reported), including an overall inventory of all the selected studies.
2.7. Quality of the Reports of the Included Randomized Clinical Trials
The assessment was carried out using the Jadad scale [27], which reveals the methodological quality of a study based on how it describes randomization, blinding and dropouts (withdrawals). The scale goes from 0 to 5, with a score of ≤2 meaning poor quality and a score of ≥3 meaning that the report meets high quality standards.
2.8. Statistical Analysis
The meta-analysis was conducted using the RevMan 5 program (Review Manager (RevMan) [Computer program]. Version 5.4. Copenhagen, Denmark: The Nordic Cochrane Centre, The Cochrane Collaboration, London, UK, 2014). Animal studies were assessed for BIC [28,29,30] between 2 and 6 weeks after placement, and crestal bone loss or MBL of implants was assessed in RCTs 6 months after placement [31,32]. Mean difference (MD) and standard deviation (SD) were used for the assessment of continuous variables (BIC and crestal bone loss), weighting by inverse variance with a 95% confidence interval (CI). The threshold for statistical significance was established at p < 0.05. Heterogeneity was assessed by calculating I2 and Chi-square, using a random effects model in both cases. The sensitivity analysis was conducted by excluding one study at a time to check whether there were changes in the results. A funnel plot graph was used to assess publication bias.
3. Results
3.1. Characteristics of the Studies
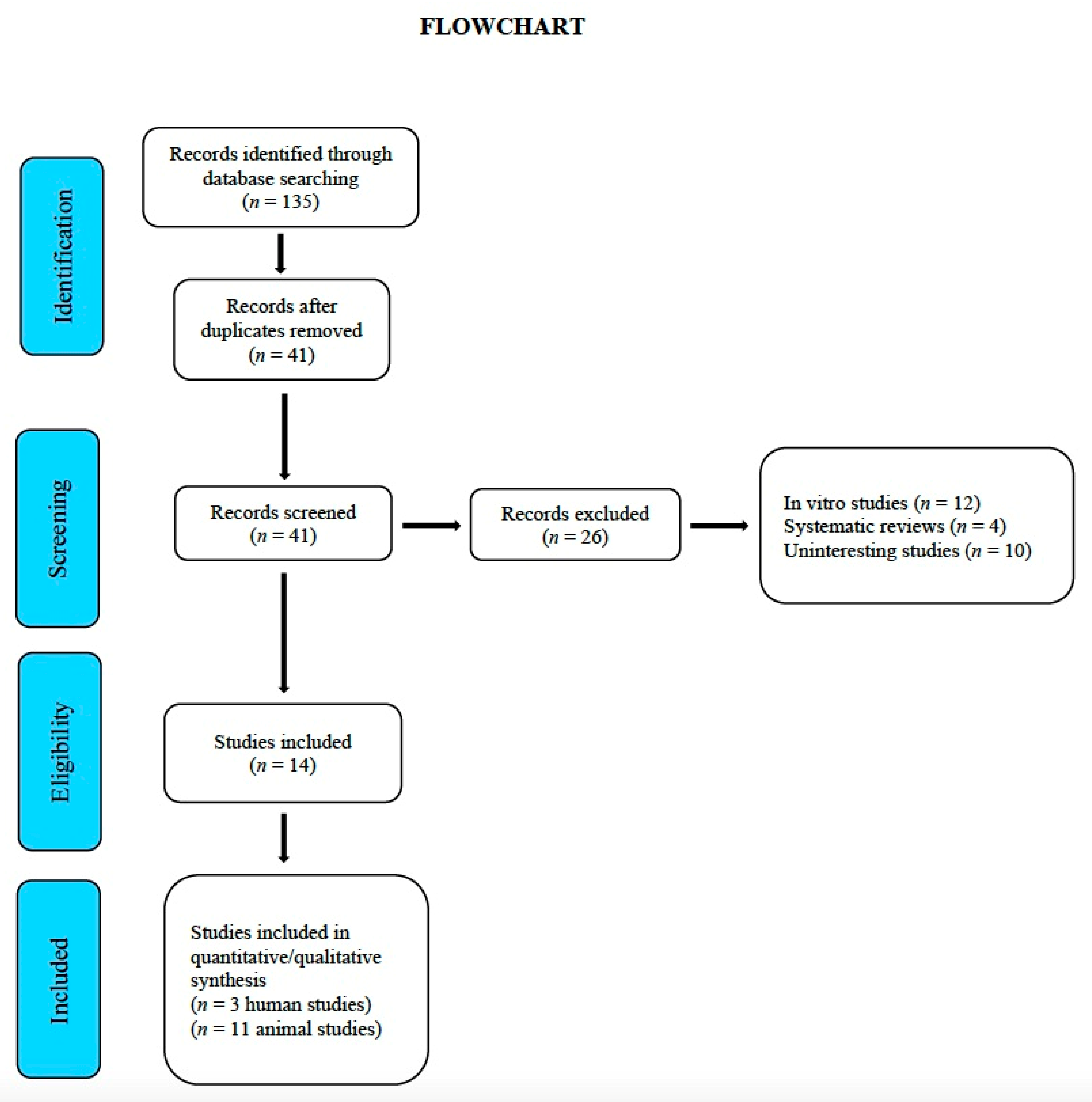
Until November 2020, a total of 135 studies were identified for subsequent assessment by the reviewers. After a first screening, 41 duplicate studies were removed. In a second screening, 26 studies that did not clearly meet the inclusion criteria, and were therefore considered inadequate, were removed (Figure 1, Flowchart). Table 1 provide the evaluation of the ARRIVE criteria in animal studies. Table 2 and Table 3 provide a general description of the details corresponding to the RCTs and experimental animal studies, respectively. Table 4 provides the Jadad quality score in RCTs.
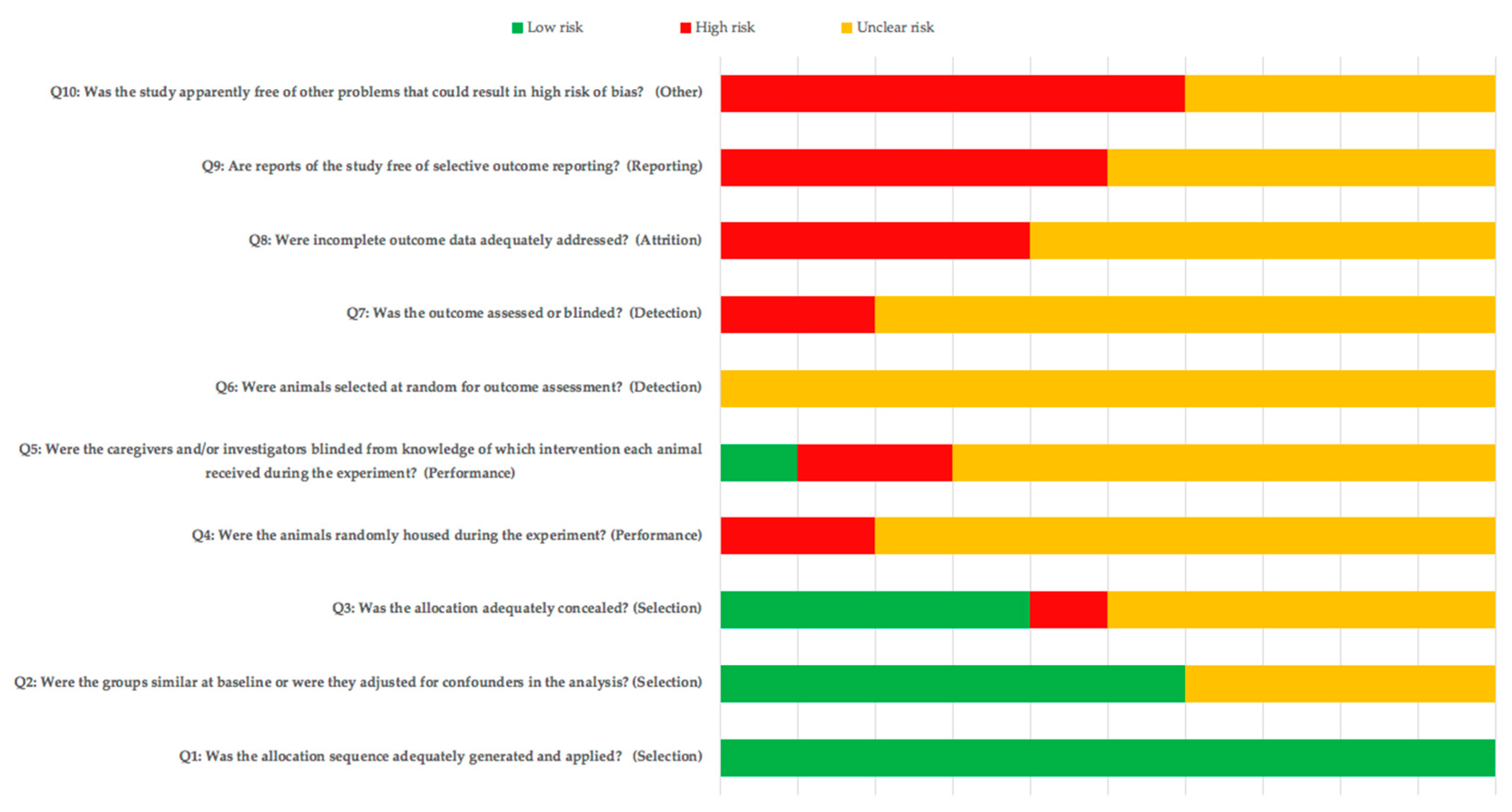
3.2. Risk of Bias and Quality Assessment of Animals Included Studies
The risk of bias assessment results for the animal studies are shown in Figure 2. Although allocation to blinding was mentioned in several articles, the lack of information resulted in a high and unclear risk of bias for most of the items. The ARRIVE checklist criteria for the animal studies [26] included are shown in Table 1. The mean score of the studies was 16.36 ± 0.88. All the studies provided adequate information in terms of title, abstract, introduction, ethical declaration, species, surgical procedure, assessment of results and statistical analysis. None of the studies reported items 5 (Reasons for animal models), 19 (3Rs, Replace, Reduce and Refine), 20 (Adverse events), 21 (Study limitations) or 22 (Generalization/applicability).
3.3. Methodological Quality of the Included Randomized Studies
The mean score of the studies was 3.3 ± 1.2. Two of the included studies [44,46] scored ≥3; the study by Hazzaa et al. [45] obtained the lowest score (Table 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Table 4.
Jadad quality score of randomized controlled trial, included in the meta-analysis.
| Study and Year | Randomization | Blinding | Dropouts | Total Score |
|---|---|---|---|---|
| Hazzaa et al., 2020. [44] | 3 | 0 | 0 | 3 |
| Hazzaa et al., 2019. [45] | 1 | 0 | 0 | 2 |
| El-Gammal et al., 2016. [46] | 3 | 1 | 1 | 5 |
Each study was assigned a score of 0–5; Mode value: 3.3 ± 1.2 (Mean value and standard deviation).
3.4. Meta-Analysis Results
The meta-analysis for bone-implant contact was carried out between 2 and 6 weeks after implant placement in animal studies [34,35,36,37,39,41,42,43], while that of crestal bone loss was performed six months after placement in RCTs [44,45,46].
Three animal studies were excluded from the quantitative analysis: that by Palin et al. [33], as it did not measure bone-implant contact; the study by Muñoz et al. [38], which combined melatonin with growth hormone; and the study conducted by Calvo-Guirado et al. in 2010 [40], where melatonin was combined with pig bone.
Heterogeneity in the results was very high (I2 = 96%; Chi-square = 193.87; 95% CI), which is why a random effects model was chosen, assuming that the differences among studies were due to heterogeneity, and that the effect of small studies on the result of the meta-analysis was relevant. The results of the sensitivity analysis did not suggest the exclusion of any study to be the cause for heterogeneity, the latter being always above 90%; however, it appeared to be the cause for significant changes in the direction or size of the effect. Since in this case the large effect size suggested a positive result (higher percentage of bone-implant contact), the forest plot’s labels were inverted.
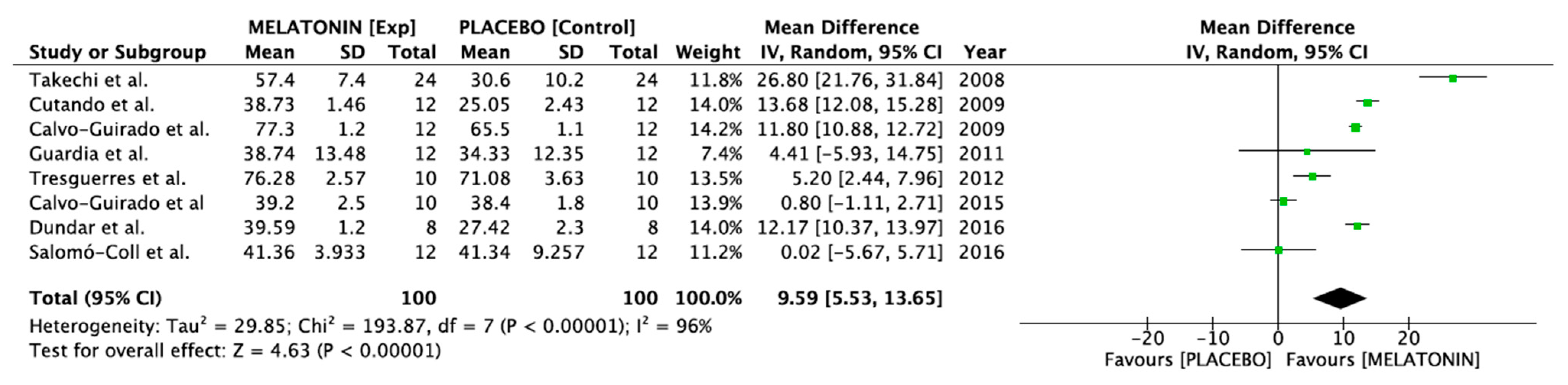
The study of the forest plot (Figure 3) revealed no significant differences between the two groups (melatonin vs. placebo) in the studies of Guardia et al. [39], Calvo-Guirado et al. en 2015 [36] and Salomó-Coll et al. [34], since confidence intervals at 95% overlap and cross the line of no effect. In the remaining studies [33,35,37,38,40,41,42,43], the experimental group (melatonin) achieves significantly better results than the placebo group. There were also no noticeable differences among studies, since the confidence intervals of the selected studies overlap, except in the case of Takechi et al. [43], where results were more favorable to melatonin than in the other studies.
The meta-analysis revealed that treatment with melatonin is associated with greater contact between the implant’s surface and the bone in the assessment carried out between 2 and 6 months after implant placement (difference in means, random effects: 9.59 [95% CI: 5.53–13.65]).
As regards RCTs, three studies [44,45,46] assessed crestal bone loss 6 months after placement were selected.
Heterogeneity was high (I2 = 95%; Chi-square = 41, 50; 95% CI), so a random effects model was chosen, assuming that the differences among studies were due to heterogeneity rather than chance. The study of the forest plot (Figure 4) revealed that the difference between the two study groups (melatonin vs. placebo) was not significant in the study by El-Gammal et al. [46], while in the two studies by Hazzaa et al. [44,45], the experimental group (melatonin) achieved better results than the placebo group.
The meta-analysis also proved that, after 6 months, the implants placed in the experimental group (melatonin) presented less marginal bone loss than those placed in the control group (difference in means, random effects: −0.55 [95% CI: 1.10–0.00]). The load increase in the study by El-Gammal et al. [46] led to a widening of the confidence interval for the overall effect size. Nevertheless, because of the small size of the sample and the large heterogeneity among studies, the results of this meta-analysis should be taken with caution.
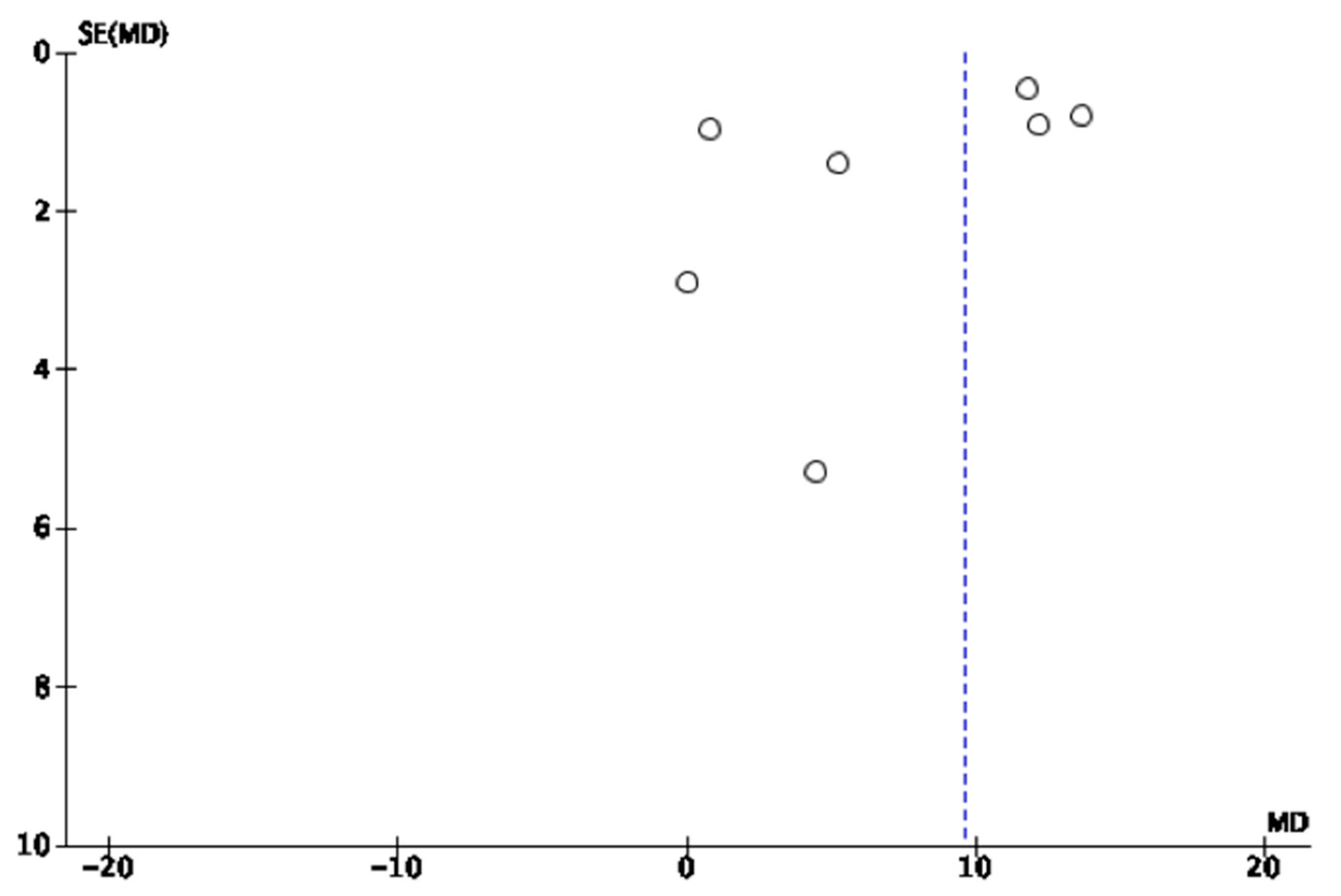
3.5. Publication Bias and Heterogeneity
The experimental studies show graphical signs of publication bias, as can be observed in the Funnel Plot (Figure 5).
4. Discussion
The purpose of this study was to explore the role of MT in bone growth and remodeling around Ti dental implants, both in RCTs and in experimental animal trials.
Bone remodeling involves hormones, cytokines, growth factors and other molecules [47], with MT being one of the hormones that modulates bone formation and absorption.
Certain studies have reported that MT stimulates the osteogenic activity of bone tissue, increasing human osteoblast differentiation in vitro and inducing the formation of cortical bone in mice in [48].
The relationship between MT and bone metabolism has been demonstrated in several studies [37,41,45], with evidence of its effect as a precursor of bone cells in rat bone marrow [49]. Koyama and colleagues [50] were the first to prove that the administration of MT in young rats during their growth period increased spongy bone mass and inhibited bone resorption. If such findings were to be confirmed using adult animals with no endogenous MT, they could be useful to explain the concept of osseointegration. Satomura and colleagues proved that MT accelerates osteoblastic differentiation in humans and rodents, suggesting its possible application as pharmaceutical agent to promote bone regeneration [51]. Nevertheless, in an in vitro study on the effect of melatonin on adipogenesis and osteogenesis in human mesenchymal stem cells, Zhang and colleagues [52] reported an early increase in adhesion and proliferation but found no differences in extended culture periods.
The experimental studies included in our meta-analysis [34,35,36,37,39,41,42,43] show the beneficial effects of MT as regards bone regeneration around Ti dental implants, be it topically applied on implant beds [34,37,39,41,42], coating the implant [35,36], or injected around the implants at the time of placement [43]. However, although certain studies reported a reduction in osteoclastogenesis [53] when topically applied to the alveolar socket after extraction prior to surgery [23], Cobo-Vázquez and colleagues [54], in a pilot study using a sample of 10 patients, found no differences regarding bone density when MT was applied to post-extraction alveolar sockets of retained mandibular third molars. According to our systematic review, Tresguerres and colleagues [37] presented the most thorough histological results, reporting changes in the cortical and medullary regions, and a larger amount of trabecular tissue in contact with the implants in the group treated with MT. The remaining studies only reported histomorphometric results [34,35,36,39,40,42,43].
Current studies regard the skeleton as a true endocrine organ controlled by the hypothalamus [55]. Protein degradation mediated by the ubiquitin-proteasome pathway is essential to regulate the balance between bone formation and bone resorption through certain signal transduction pathways, which regulate the activity of mature osteoblasts and osteoclasts [56].
Apart from contributing to synchronize biological rhythms and its antioxidant and inflammatory effects, among others, MT has immunomodulatory effects and induces apoptosis [57]. However, the role of MT in the formation of new bone is not fully defined, its reduction being regarded as proportional to skeletal maturation and with contraindications concerning its function, such as the fact that certain individuals with different defects in osteoblast function are at a greater risk for osteosarcoma. Conversely, MT can improve the normal functions of osteoblasts, and would therefore play a protective role against bone cancer [58,59].
Because of the ethical implications associated with histopathological examinations, the RCTs included in our meta-analysis exclusively reported macroscopic and radiologic results; nevertheless, the reduced number of included studies prevented an adequate and conclusive meta-analysis. Moreover, the study by Hazzaa and colleagues [45] presented certain limitations in its design and in how it was conducted, such as group randomization, implant location, reason for removal, demographic characteristics of the participants and the degree to which they balanced between groups that reduce the reliability of its results [60]. Nonetheless, our meta-analysis found that MT stimulates the formation of new bone and increases bone density around Ti dental implants, although it presented serious limitations, mainly associated with the heterogeneity among the selected studies and the scarcity of RCTs. On the other hand, there were significant discrepancies among animal studies regarding measurement of the parameters of bone surface in contact with the implant, as had been observed in the radiologic measurements in the RCTs. There were also major differences regarding the amounts, preparation, forms of application, concentrations and application timing of MT. Another important limitation was that none of the included studies considered factors such as bone quality or the surgical technique used—these factors would provide biases in obtaining results.
The study by Takechi and colleagues [43], which is consistent with that of Satomura and colleagues [51], was the only one where melatonin was used systemically (intraperitoneal, 100 mg/Kg weight) until the animals were sacrificed (4 weeks after implant placement): this form of administration and dosage conflicts with those used by the other authors included in the review [33,34,35,36,37,38,39,40,41,42,43]. The systemic administration of MT requires large doses of the drug, which increases the possibility of side effects; therefore, the topical application of MT is preferred over its systemic administration [61]. This same discrepancy in form of administration and dosage could be observed in the RCTs, while Hazzaa and colleagues and El-Gammal and colleagues [44,46] used MT in the form of topical gel, in doses of 1.2 mg., and Hazzaa and colleagues [45] used it in powder form, not specifying the dosage. Hence, there is no consensus as to the best route of administration for this molecule, and the dosage required to achieve the desired effect.
5. Conclusions
Bearing in mind the limitations of most of the studies, all of those included in this meta-analysis reported that the topical application of MT on the ostectomy site at the time of implant placement can induce greater bone-to-implant contact, as well as greater bone mass and density around Ti dental implants, especially in the earliest stages of healing, thus favoring osseointegration. Nevertheless, to clearly confirm such affirmations, further research using broader, well-designed samples with long-term monitoring and standardized protocols for application, MT dosage and assessment of bone parameters is required; all with the purpose of ensuring predictable and reliable outcomes.
Supplementary Materials
The following are available online at https://www.mdpi.com/2079-6412/11/3/271/s1, Table S1: PRISMA Checklist.
Author Contributions
Study concept, N.L.-V. and A.L.-V.; literature search, N.L.-V. and J.M.R.; data analysis, B.P.-P.; drafting of the manuscript, N.L.-V. and A.L.-V.; critical revision of the manuscript, A.L.-V. and J.M.R. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| MT | Melatonin |
| Ti | Titanium |
| RCTs | Randomized Clinical Trials |
| BIC | Bone Implant Contact |
| MLB | Marginal Bone Loss |
| BD | Bone Density |
| PPD | Pre-Implant Probing Depth |
| PIST | Peri-Implant Soft Tissue |
| GI | Gingival Index |
| MPD | Mesial Probing Depth |
| DDP | Distal Probing Depth |
| ABG | Autogenous Bone Graft |
References
- Brånemark, P.I.; Adell, R.; Breine, U.; Hansson, B.O.; Lindström, J.; Ohlsson, A. Intra-osseous anchorage of dental prostheses. I. Experimental studies. Scand. J. Plast. Reconstr. Surg. 1969, 3, 81–100. [Google Scholar]
- Naveau, A.; Shinmyouzu, K.; Moore, C.; Avivi-Arber, L.; Jokerst, J.; Koka, S. Etiology and Measurement of Peri-Implant Crestal Bone Loss (CBL). J. Clin. Med. 2019, 8, 166. [Google Scholar] [CrossRef] [Green Version]
- He, J.-Y.; Zheng, X.-F.; Jiang, L.-S. Autonomic control of bone formation: Its clinical relevance. Handb. Clin. Neurol. 2013, 117, 161–171. [Google Scholar] [PubMed]
- He, J.-Y.; Jiang, L.-S.; Dai, L.-Y. The Roles of the Sympathetic Nervous System in Osteoporotic Diseases: A Review of Experimental and Clinical Studies. Ageing Res. Rev. 2011, 10, 253–263. [Google Scholar]
- Olney, R.C. Regulation of bone mass by growth hormone. Med. Pediatric Oncol. 2003, 41, 228–234. [Google Scholar] [CrossRef] [PubMed]
- López-Valverde, N.; Flores-Fraile, J.; López-Valverde, A. The Unknown Process Osseointegration. Biology 2020, 9, 168. [Google Scholar] [CrossRef] [PubMed]
- Shi, H.; Sorrell, J.E.; Clegg, D.J.; Woods, S.C.; Seeley, R.J. The Roles of Leptin Receptors on POMC Neurons in the Regulation of Sex-Specific Energy Homeostasis. Physiol. Behav. 2010, 11, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Gupta, B.; Acharya, A.; Pelekos, G.; Gopalakrishnan, D.; Kolokythas, A. Selective serotonin reuptake inhibitors and dental implant failure-a significant concern in elders? Gerodontology 2017, 34, 505–507. [Google Scholar] [CrossRef]
- Pellegrino, G.; Grande, F.; Ferri, A.; Pisi, P.; Gandolfi, M.G.; Marchetti, C. Three-Dimensional Radiographic Evaluation of the Malar Bone Engagement Available for Ideal Zygomatic Implant Placement. Methods Protoc. 2020, 3, 52. [Google Scholar] [CrossRef] [PubMed]
- Buser, D.; Sennerby, L.; De Bruyn, H. Modern implant dentistry based on osseointegration: 50 years of progress, current trends and open questions. Periodontology 2017, 73, 7–21. [Google Scholar] [CrossRef]
- Piatelli, A. Bone Response to Dental Implant Materials, 1st ed.; Woodhead Publishing: Cambridge, UK, 2016. [Google Scholar]
- Iwai-Yoshida, M.; Shibata, Y.; Wurihan; Suzuki, D.; Fujisawa, N.; Tanimoto, Y.; Kamijo, R.; Maki, K.; Miyazaki, T. Antioxidant and osteogenic properties of anodically oxidized titanium. J. Mech. Behav. Biomed. Mater. 2012, 13, 230–236. [Google Scholar] [CrossRef]
- Coelho, P.G.; Granjeiro, J.M.; Romanos, G.E.; Suzuki, M.; Silva, N.R.F.; Cardaropoli, G.; Thompson, V.P.; Lemons, J.E. Basic research methods and current trends of dental implant surfaces. J. Biomed. Mater. Res. Part B Appl. Biomater. 2009, 88, 579–596. [Google Scholar] [CrossRef]
- López-Valverde, N.; Flores-Fraile, J.; Ramírez, J.M.; Sousa, B.M.; Herrero-Hernández, S.; López-Valverde, A. Bioactive Surfaces vs. Conventional Surfaces in Titanium Dental Implants: A Comparative Systematic Review. J. Clin. Med. 2020, 9, 2047. [Google Scholar] [CrossRef]
- Ramírez-Fernández, M.P.; Calvo-Guirado, J.L.; Maté Sánchez de-Val, J.E.; Delgado-Ruiz, R.A.; Negri, B.; Pardo-Zamora, G.; Peñarrocha, D.; Barona, C.; Granero, J.M.; Alcaraz-Baños, M. Melatonin promotes angiogenesis during repair of bone defects: A radiological and histomorphometric study in rabbit tibiae. Clin. Oral Investig. 2013, 17, 147–158. [Google Scholar]
- Tordjman, S.; Chokron, S.; Delorme, R.; Charrier, A.; Bellissant, E.; Jaafari, N.; Fougerou, C. Melatonin: Pharmacology, Functions and Therapeutic Benefits. Curr. Neuropharmacol. 2017, 15, 434–443. [Google Scholar] [CrossRef] [PubMed]
- Amaral, F.G.D.; Cipolla-Neto, J. A brief review about melatonin, a pineal hormone. Arch. Endocrinol. Metab. 2018, 62, 472–479. [Google Scholar] [CrossRef] [Green Version]
- Najafi, M.; Shirazi, A.; Motevaseli, E.; Rezaeyan, A.H.; Salajegheh, A.; Rezapoor, S. Melatonin as an anti-inflammatory agent in radiotherapy. Inflammopharmacology 2017, 25, 403–413. [Google Scholar] [CrossRef]
- Mauriz, J.L.; Collado, P.S.; Veneroso, C.; Reiter, R.J.; González-Gallego, J. A review of the molecular aspects of melatonin’s anti-inflammatory actions: Recent insights and new perspectives. J. Pineal Res. 2013, 54, 1–14. [Google Scholar] [CrossRef]
- Liu, J.; Huang, F.; He, H.W. Melatonin effects on hard tissues: Bone and tooth. Int. J. Mol. Sci. 2013, 14, 10063–10074. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Salomó-Coll, O.; de Maté-Sánchez, J.E.V.; Ramírez-Fernandez, M.P.; Hernández-Alfaro, F.; Gargallo-Albiol, J.; Calvo-Guirado, J.L. Osseoinductive elements around immediate implants for better osteointegration: A pilot study in foxhound dogs. Clin. Oral Implants Res. 2018, 29, 1061–1069. [Google Scholar] [CrossRef] [PubMed]
- Manchester, L.C.; Coto-Montes, A.; Boga, J.A.; Andersen, L.P.H.; Zhou, Z.; Galano, A.; Vriend, J.; Tan, D.X.; Reiter, R.J. Melatonin: An ancient molecule that makes oxygen metabolically tolerable. J. Pineal Res. 2015, 59, 403–419. [Google Scholar] [CrossRef] [PubMed]
- Rodríguez-Lozano, F.J.; García-Bernal, D.; de los Ros-Roca, M.; del Carmen Algueró, M.; Oñate-Sánchez, R.E.; Camacho-Alonso, F.; Moraleda, J.M. Cytoprotective effects of melatonin on zoledronic acid-treated human mesenchymal stem cells in vitro. J. Craniomaxillofac. Surg. 2015, 43, 855–862. [Google Scholar] [CrossRef]
- Hutton, B.; Ferrán Catalá-López, F.; Moher, D. The PRISMA statement extension for systematic reviews incorporating network meta-analysis: PRISMA-NMA. Med. Clin. 2016, 16, 262–266. [Google Scholar] [CrossRef] [PubMed]
- Hooijmans, C.R.; Rovers, M.M.; de Vries, R.B.; Leenaars, M.; Ritskes-Hoitinga, M.; Langendam, M.W. SYRCLE’s risk of bias tool for animal studies. BMC Med. Res. Methodol. 2014, 14, 43. [Google Scholar] [CrossRef] [Green Version]
- Stadlinger, B.; Pourmand, P.; Locher, M.C.; Schulz, M.C. Systematic review of animal models for the study of implant integration, assessing the influence of material, surface and design. J. Clin. Periodontol. 2012, 39, 28–36. [Google Scholar] [CrossRef]
- Jadad, A.R.; Moore, R.A.; Carroll, D.; Jenkinson, C.; Reynolds, D.J.; Gavaghan, D.J.; McQuay, H.J. Assessing the quality of reports of randomized clinical trials: Is blinding necessary? Control Clin. Trials 1996, 17, 1–12. [Google Scholar] [CrossRef]
- Degidi, M.; Perrotti, V.; Piattelli, A.; Iezzi, G. Mineralized bone-implant contact and implant stability quotient in 16 human implants retrieved after early healing periods: A histologic and histomorphometric evaluation. Int. J. Oral Maxillofac. Implant. 2010, 25, 45–48. [Google Scholar]
- Bornstein, M.M.; Valderrama, P.; Jones, A.A.; Wilson, T.G.; Seibl, R.; Cochran, D.L. Bone apposition around two different sandblasted and acid-etched titanium implant surfaces: A histomorphometric study in canine mandibles. Clin. Oral Implant. Res. 2008, 19, 233–241. [Google Scholar] [CrossRef]
- Froum, S.J.; Simon, H.; Cho, S.C.; Elian, N.; Rohrer, M.D.; Tarnow, D.P. Histologic evaluation of bone-implant contact of immediately loaded transitional implants after 6 to 27 months. Int. J. Oral Maxillofac. Implant. 2005, 20, 54–60. [Google Scholar]
- Cosola, S.; Marconcini, S.; Boccuzzi, M.; Menchini-Fabris, G.B.; Covani, U.; Peñarrocha-Diago, M.; Peñarrocha-Oltra, D. Radiological Outcomes of Bone-Level and Tissue-Level Dental Implants: Systematic Review. Int. J. Environ. Res. Public Health 2020, 17, 6920. [Google Scholar] [CrossRef] [PubMed]
- Laurell, L.; Lundgren, D. Marginal bone level changes at dental implants after 5 years in function: A meta-analysis. Clin. Implant. Dent. Relat. Res. 2011, 13, 19–28. [Google Scholar] [CrossRef] [PubMed]
- Palin, L.P.; Polo, T.O.B.; Batista, F.R.; Gomes-Ferreira, P.H. Garcia Junior, I.R.; Rossi, A.C.; Freire, A.; Faverani, L.P.; Sumida, D.H.; Okamoto, R. Daily melatonin administration improves osseointegration in pinealectomized rats. J. Appl. Oral Sci. 2018, 26, e20170470. [Google Scholar] [CrossRef] [Green Version]
- Salomó-Coll, O.; Maté-Sánchez de Val, J.E.; Ramírez-Fernández, M.P.; Satorres-Nieto, M.; Gargallo-Albiol, J.; Calvo-Guirado, J.L. Osseoinductive elements for promoting osseointegration around immediate implants: A pilot study in the foxhound dog. Clin. Oral Implant. Res. 2016, 27, e167–e175. [Google Scholar] [CrossRef] [PubMed]
- Dundar, S.; Yaman, F.; Saybak, A.; Ozupek, M.F.; Toy, V.E.; Gul, M.; Ozercan, I.H. Evaluation of Effects of Topical Melatonin Application on Osseointegration of Dental Implant: An Experimental Study. J. Oral Implantol. 2016, 42, 386–389. [Google Scholar] [CrossRef]
- Calvo-Guirado, J.L.; Aguilar Salvatierra, A.; Gargallo-Albiol, J.; Delgado-Ruiz, R.A.; Maté Sanchez, J.E.; Satorres-Nieto, M. Zirconia with laser-modified microgrooved surface vs. titanium implants covered with melatonin stiulates bone formation. Experimental study in tibia rabbits. Clin. Oral Implant. Res. 2015, 26, 1421–1429. [Google Scholar] [CrossRef]
- Tresguerres, I.F.; Clemente, C.; Blanco, L.; Khraisat, A.; Tamimi, F.; Tresguerres, J.A. Effects of local melatonin application on implant osseointegration. Clin. Implant. Dent. Relat. Res. 2012, 14, 395–399. [Google Scholar] [CrossRef]
- Muñoz, F.; López-Peña, M.; Miño, N.; Gómez-Moreno, G.; Guardia, J.; Cutando, A. Topical application of melatonin and growth hormone accelerates bone healing around dental implants in dogs. Clin. Implant. Dent. Relat. Res. 2012, 14, 226–235. [Google Scholar] [CrossRef] [PubMed]
- Guardia, J.; Gómez-Moreno, G.; Ferrera, M.J.; Cutando, A. Evaluation of effects of topic melatonin on implant surface at 5 and 8 weeks in Beagle dogs. Clin. Implant. Dent. Relat. Res. 2011, 13, 262–268. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; Gómez-Moreno, G.; López-Marí, L.; Guardia, J.; Marínez-González, J.M.; Barone, A.; Tresguerres, I.F.; Paredes, S.D.; Fuentes-Breto, L. Actions of melatonin mixed with collagenized porcine bone versus porcine bone only on osteointegration of dental implants. J. Pineal Res. 2010, 48, 194–203. [Google Scholar] [CrossRef] [PubMed]
- Calvo-Guirado, J.L.; Gómez-Moreno, G.; Barone, A.; Cutando, A.; Alcaraz-Baños, M.; Chiva, F.; López-Marí, L.; Guardia, J. Melatonin plus porcine bone on discrete calcium deposit implant surface stimulates osteointegration in dental implants. J. Pineal Res. 2009, 47, 164–172. [Google Scholar] [CrossRef] [PubMed]
- Cutando, A.; Gómez-Moreno, G.; Arana, C.; Muñoz, F.; Lopez-Peña, M.; Stephenson, J.; Reiter, R.J. Melatonin stimulates osteointegration of dental implants. J. Pineal Res. 2008, 45, 174–179. [Google Scholar] [CrossRef] [PubMed]
- Takechi, M.; Tatehara, S.; Satomura, K.; Fujisawa, K.; Nagayama, M. Effect of FGF-2 and melatonin on implant bone healing: A histomorphometric study. J. Mater. Sci. Mater. Med. 2008, 19, 2949–2952. [Google Scholar] [CrossRef]
- Hazzaa, H.H.A.; Shawki, N.A.; Abdelaziz, L.M.; Shoshan, H.S. Early Loading of Dental Implant Grafted with Autogenous Bone Alone or Combined with Melatonin Gel: A Randomized Clinical Trial. Austin J. Dent. 2020, 7, 1137. [Google Scholar]
- Hazzaa, H.H.A.; El-Kilani, N.S.; Elsayed, S.A.; Abd El Massieh, P.M. Evaluation of Immediate Implants Augmented with Autogenous Bone/Melatonin Composite Graft in the Esthetic Zone: A Randomized Controlled Trial. J. Prosthodont. 2019, 28, e637–e642. [Google Scholar] [CrossRef]
- El-Gammal, M.Y.; Salem, A.S.; Anees, M.M.; Tawfik, M.A. Clinical and Radiographic Evaluation of Immediate Loaded Dental Implants with Local Application of Melatonin: A Preliminary Randomized Controlled Clinical Trial. J. Oral Implantol. 2016, 42, 119–125. [Google Scholar] [CrossRef]
- Ostrowska, Z.; Kos-Kudla, B.; Nowak, M.; Swietochowska, E.; Marek, B.; Gorski, J.; Kajdaniuk, D.; Wolkowska, K. The relationship between bone metabolism, melatonin and other hormones in sham-operated and pinealectomized rats. Endocr. Regul. 2003, 37, 211–224. [Google Scholar] [PubMed]
- Roth, J.A.; Kim, B.G.; Lin, W.L.; Cho, M.I. Melatonin promotes osteoblast differentiation and bone formation. J. Biol. Chem. 1999, 274, 22041–22047. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Witt-Enderby, P.; Radio, N.M.; Doctor, J.S.; Davis, V.L. Therapeutic treatments potentially mediated by melatonin receptors: Potential clinical uses in the prevention of osteoporosis, cancer and as an adjuvant therapy. J. Pineal Res. 2006, 41, 297–305. [Google Scholar] [CrossRef] [PubMed]
- Koyama, H.; Nakade, O.; Takada, Y.; Kaku, T.; Lau, K.H. Melatonin at pharmacologic doses increases bone mass by suppressing resorption through down-regulation of the RANKL-mediated osteoclast formation and activation. J. Bone Miner. Res. 2002, 17, 1219–1229. [Google Scholar] [CrossRef]
- Satomura, K.; Tobiume, S.; Tokuyama, R.; Yamasaki, Y.; Kudoh, K.; Maeda, E.; Nagayama, M. Melatonin at pharmacological doses enhances human osteoblastic differentiation in vitro and promotes mouse cortical bone formation in vivo. J. Pineal Res. 2007, 42, 231–239. [Google Scholar] [CrossRef] [PubMed]
- Zhang, L.; Su, P.; Xu, C.; Chen, C.; Liang, A.; Du, K.; Peng, Y.; Huang, D. Melatonin inhibits adipogenesis and enhances osteogenesis of human mesenchymal stem cells by suppressing PPARγ expression and enhancing Runx2 expression. J. Pineal Res. 2010, 49, 364–372. [Google Scholar] [CrossRef] [PubMed]
- Cutando, A.; López-Valverde, A.; Gómez-de-Diego, R.; Arias-Santiago, S.; de Vicente-Jiménez, J. Effect of gingival application of melatonin on alkaline and acid phosphatase, osteopontin and osteocalcin in patients with diabetes and periodontal disease. Med. Oral Patol. Oral Cir. Bucal 2013, 18, e657–e663. [Google Scholar] [CrossRef] [PubMed]
- Cobo-Vázquez, C.; Fernández-Tresguerres, I.; Ortega-Aranegui, R.; López-Quiles, J. Effects of local melatonin application on post-extraction sockets after third molar surgery. A pilot study. Med. Oral Patol. Oral Cir. Bucal 2014, 19, e628–e633. [Google Scholar] [CrossRef] [PubMed]
- Tyrovola, J.B. The “Mechanostat” Principle and the Osteoprotegerin-OPG/RANKL/RANK System PART II. The Role of the Hypothalamic-Pituitary Axis. J. Cell Biochem. 2017, 118, 962–966. [Google Scholar] [CrossRef] [PubMed]
- Vriend, J.; Reiter, R.J. Melatonin, bone regulation and the ubiquitin-proteasome connection: A review. Life Sci. 2016, 145, 152–160. [Google Scholar] [CrossRef]
- Carlberg, C. Gene regulation by melatonin. Ann. N. Y. Acad. Sci. 2000, 917, 387–396. [Google Scholar] [CrossRef]
- Gupta, D. How important is the pineal gland in children? In Advances in Pineal Research; Reiter, R.J., Pang, S.F., Eds.; John Libbey: London, UK, 1989; pp. 291–297. [Google Scholar]
- Lu, K.H.; Su, S.C.; Lin, C.W.; Hsieh, Y.H.; Lin, Y.C.; Chien, M.H.; Reiter, R.J.; Yang, S.F. Melatonin attenuates osteosarcoma cell invasion by suppression of c-c motif chemokine ligand 24 through inhibition of the c-jun n-terminal kinase pathway. J. Pineal Res. 2018, 65, e12507. [Google Scholar] [CrossRef]
- Brignardello-Petersen, R. Melatonin as an adjunct to autogenous bone grafts may result in small benefits in probing depth, marginal bone loss, and gingival index of sites with immediate implants. J. Am. Dent. Assoc. 2018, 149, e85. [Google Scholar] [CrossRef]
- Xiao, L.; Lin, J.; Chen, R.; Huang, Y.; Liu, Y.; Bai, J.; Ge, G.; Shi, X.; Chen, Y.; Shi, J.; et al. Sustained Release of Melatonin from GelMA Liposomes Reduced Osteoblast Apoptosis and Improved Implant Osseointegration in Osteoporosis. Oxid. Med. Cell. Longev. 2020, 2020, 6797154. [Google Scholar] [CrossRef]
Figure 1.
Flowchart.

Figure 2.
SYRCLE’s risk of bias tool.

Figure 3.
Forest plot for the meta-analysis of animal studies assessing bone-implant contact between 2 to 6 weeks after placement, taking the mean difference as the effect size index, weighting by inverse variance and assuming a random effects model. CI = Confidence Interval.
Figure 3.
Forest plot for the meta-analysis of animal studies assessing bone-implant contact between 2 to 6 weeks after placement, taking the mean difference as the effect size index, weighting by inverse variance and assuming a random effects model. CI = Confidence Interval.

Figure 4.
Forest plot for the meta-analysis of the human clinical trials assessing crestal bone loss 6 months after placement, taking the mean difference as the effect size index, weighting by inverse variance and assuming a random effects model. CI = Confidence Interval.
Figure 4.
Forest plot for the meta-analysis of the human clinical trials assessing crestal bone loss 6 months after placement, taking the mean difference as the effect size index, weighting by inverse variance and assuming a random effects model. CI = Confidence Interval.

Figure 5.
Funnel plot for animal studies. The asymmetry proves publication bias.

Table 1.
Checklist of ARRIVE criteria reported by the included studies.
| Studies | Palin et al., 2018 [33] | Salomó-Coll et al., 2016 [34] | Dundar et al., 2016 [35] | Calvo-Guirado et al., 2015 [36] | Tresguerres et al., 2012 [37] | Muñoz et al., 2012 [38] | Guardia et al., 2011 [39] | Calvo-Guirado et al., 2010 [40] | Calvo-Guirado et al., 2009 [41] | Cutando et al., 2008 [42] | Takechi et al., 2008 [43] |
|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. Title | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Abstract | – | – | – | – | – | – | – | – | – | – | – |
| 2. Species | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 3. Key finding | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Introduction | – | – | – | – | – | – | – | – | – | – | – |
| 4. Bankground | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 5. Reasons for animal models | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 6. Objectives | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Methods | – | – | – | – | – | – | – | – | – | – | – |
| 7. Ethical statement | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 8. Study design | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 9. Experimentalprocedures | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 10. Experimentalanimals | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 11. Accommodation and handling of animals | 0 | 1 | 0 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 0 |
| 12. Sample size | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 13. Assignment of animals to experimental groups | 1 | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 0 | 0 | 0 |
| 14. Anaesthesia | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 15. Stadistical methods | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Results | – | – | – | – | – | – | – | – | – | – | – |
| 16. Experimental results | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 17. Results and estimation | 0 | 1 | 0 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| Discussion | – | – | – | – | – | – | – | – | – | – | – |
| 18. Interpretation and Scientific implications | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 | 1 |
| 19. 3Rs reported | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 20. Adverse events | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 21. Study limitations | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 |
| 22.Generalization/applicability | 0 | 0 | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 0 | 0 |
| 23. Funding | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 0 | 0 | 1 | 1 |
| Total Score | 15 | 17 | 15 | 17 | 16 | 16 | 18 | 17 | 16 | 17 | 16 |
Mode Value: 16.36 ± 0.88 (Mean value and standard deviation); Each item was allocated a score of “0” (not reported) or “1” (reported). The total score of each of the included studies was also recorded.
Table 2.
Characteristics of randomized clinical trials (RCTs).
| Study, Year | Participants Number | Interventions Number | Implants Number | Outcomes | Test Group p-Values | Conclusions |
|---|---|---|---|---|---|---|
| Hazzaa et al., 2020. [44]. | 23 | 46 sites for dental implants. | 46 |
| p = 0.000 | The combined use of ABG with MLN is a promising alternative for early loading. |
| Hazzaa et al., 2019. [45]. | 26 | 26 sites for dental implants. | 52 |
| p = 0.001 | Application of melatonin with ABG around immediate implants is a valuable option for replacing missing teeth in the esthetic zone in terms of soft and hard tissues. |
| El-Gammal et al., 2016. [46]. | 14 | 14 sites for dental implants. | 14 | Periotest; MPD; DPD; and MBL | p = 0.2 | The topical application of melatonin could be a good treatment option for dental implants in the posterior maxilla. |
MBL (Marginal Bone Loss); BD (Bone Density); PPD (Pre-implant Probing Depth); PIST (Peri-implant soft tissue); GI (Gingival Index); MPD (Mesial Probing Depth); DDP (Distal Probing Depth); ABG (Autogenous Bone Graft); MT (Melatonin).
Table 3.
Characteristics of Animal Studies.
| Studies, Year | Animals | Melatonin Administration Form | Implants Number | Implantation Sites | Tracing (Weeks) | Conclusions |
|---|---|---|---|---|---|---|
| Palin et al., 2018 [33] | Rat model | Melatonin in saline solution; orally | 36 | Tibia | 60 days | The use of melatonin restores the bone repair process during the osseointegration phase. |
| Salomó-Coll et al., 2016 [34] | American foxhound dog model | Implants submerged in melatonin at 5% in solution | 36 | Jaw, premolars area | 12 weeks | Topical applications of melatonin to implants placed immediately after extraction improved osseointegration and reduced bone resorption. |
| Dúndar et al., 2016 [35] | New Zealand rabbit model | Locally (powder melatonin) into the dental implant socket before implant placement | 24 | Tibia | 4 weeks | Local melatonin administration at the osteotomy site during surgical implant insertion may stimulate more BIC. |
| Calvo-Guirado et al., 2015 [36] | New Zealand rabbit model | Local application of melatonin (Titanium dental implant with melatonin doping surface) | 20 | Tibia | 1 week and 4 weeks | The use of melatonin improves the formation of new bone around the implants. |
| Tresguerres et al., 2012 [37] | New Zealand rabbit model | 3 mg of melatonin administered locally at the osteoctomy site as a lyophilizate powder before implant placement | 20 | Jaw, molars area | 4 weeks | Local melatonin administered in the osteoctomy site at the time of implant placement may induce more trabecular bone to implant contact and more trabecular area density. |
| Muñoz et al., 2012 [38] | Beagle dog model | Topical administration. Prior to implanting, a layer of 1.2 mg lyophilized powdered melatonin was applied to the bone hole | 48 | Jaw, premolars area. | 2, 5 and 8 weeks | Melatonin has stimulating effects on osteogenesis and enhances the formation of new bone around titanium implants in the early stages of healing. |
| Guardia et al., 2011 [39] | Beagle dog model | Prior to implanting, a layer of 1.2 mg lyophilized powdered melatonin was applied to the bone hole | 48 | Jaw, premolars and molars area | 5 and 8 weeks | Melatonin may bring about a reduction in bone resorption and an increase in bone mass because of its repression of osteoclast activation. |
| Calvo-Guirado et al., 2010 [40] | Beagle dog model | Implants covered with 5 mg lyophilized powdered melatonin | 36 | Femur | 2 and 4 weeks | Melatonin-coated implants increase BIC and reduce crestal bone loss. |
| Calvo-Guirado et al., 2009 [41] | Beagle dog model | Prior to implanting, a layer of 5 mg lyophilized powdered melatonin was applied to the bone hole | 24 | Jaw, premolars area | 2, 4 and 12 weeks | Melatonin increases BIC and reduces crestal bone loss. |
| Cutando et al., 2008 [42] | Beagle dog model | Topical administration. Prior to implanting, a layer of 1.2 mg lyophilized powdered melatonin was applied to the bone hole | 48 | Jaw, premolars area | 2 weeks | Topical application of melatonin may act as a biomimetic agent in the placement of endoosseous dental implants. |
| Takechi et al., 2008 [43] | Rat model | Locally injected around the implant sites 5 days after implantation | 48 | Tibia | 4 weeks | Melatonin has effects on osteogenesis and enhances the formation of new bone around titanium implants. |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
López-Valverde, N.; Pardal-Peláez, B.; López-Valverde, A.; Ramírez, J.M. Role of Melatonin in Bone Remodeling around Titanium Dental Implants: Meta-Analysis. Coatings 2021, 11, 271. https://doi.org/10.3390/coatings11030271
AMA Style
López-Valverde N, Pardal-Peláez B, López-Valverde A, Ramírez JM. Role of Melatonin in Bone Remodeling around Titanium Dental Implants: Meta-Analysis. Coatings. 2021; 11(3):271. https://doi.org/10.3390/coatings11030271
Chicago/Turabian StyleLópez-Valverde, Nansi, Beatriz Pardal-Peláez, Antonio López-Valverde, and Juan Manuel Ramírez. 2021. "Role of Melatonin in Bone Remodeling around Titanium Dental Implants: Meta-Analysis" Coatings 11, no. 3: 271. https://doi.org/10.3390/coatings11030271
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.