
Nanostructured Calcium-Incorporated Surface Compared to Machined and SLA Dental Implants—A Split-Mouth Randomized Case/Double-Control Histological Human Study

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Surgical Procedure
2.3. Histological Processing
2.4. Statistical Analysis
3. Results
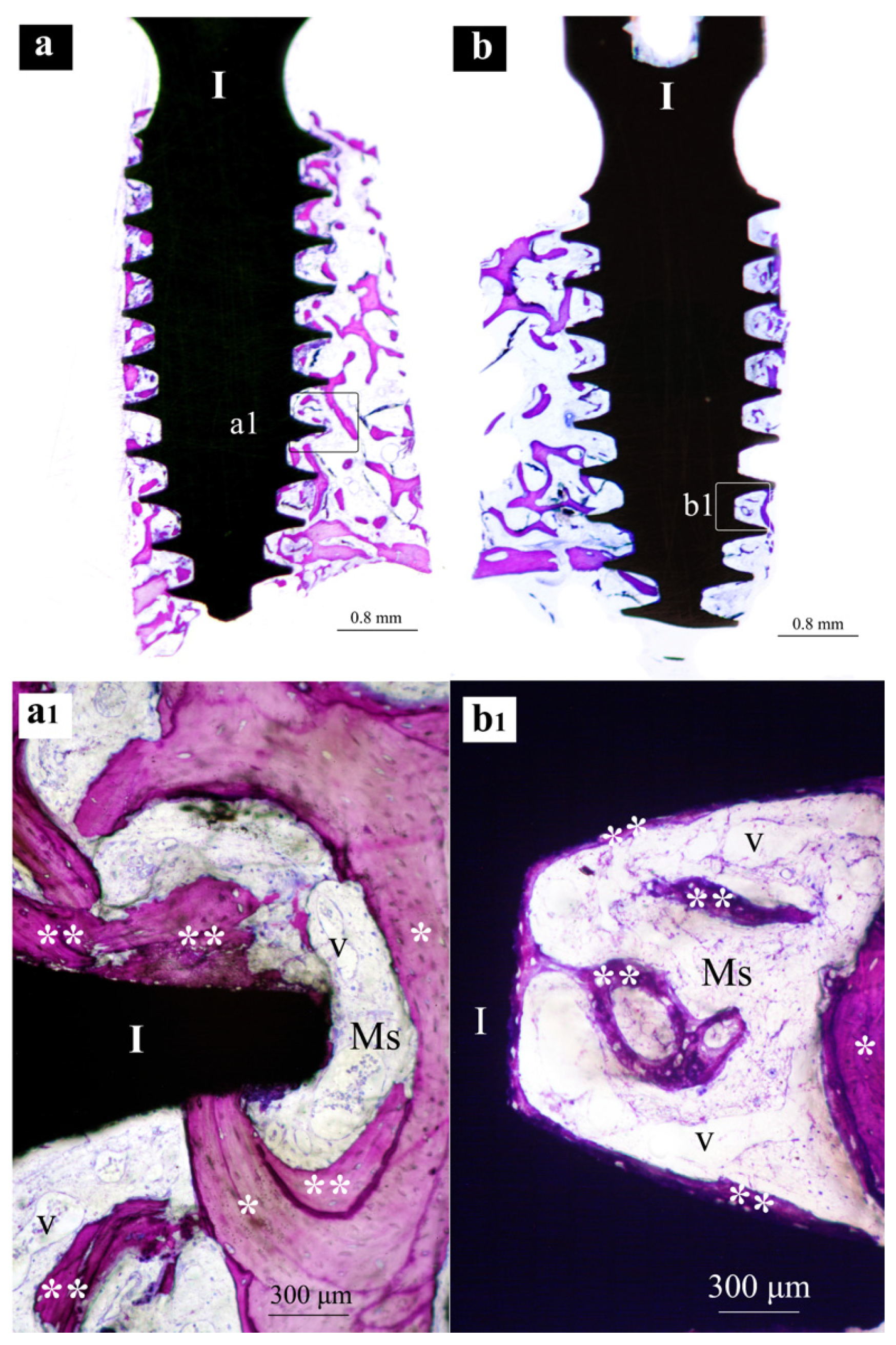
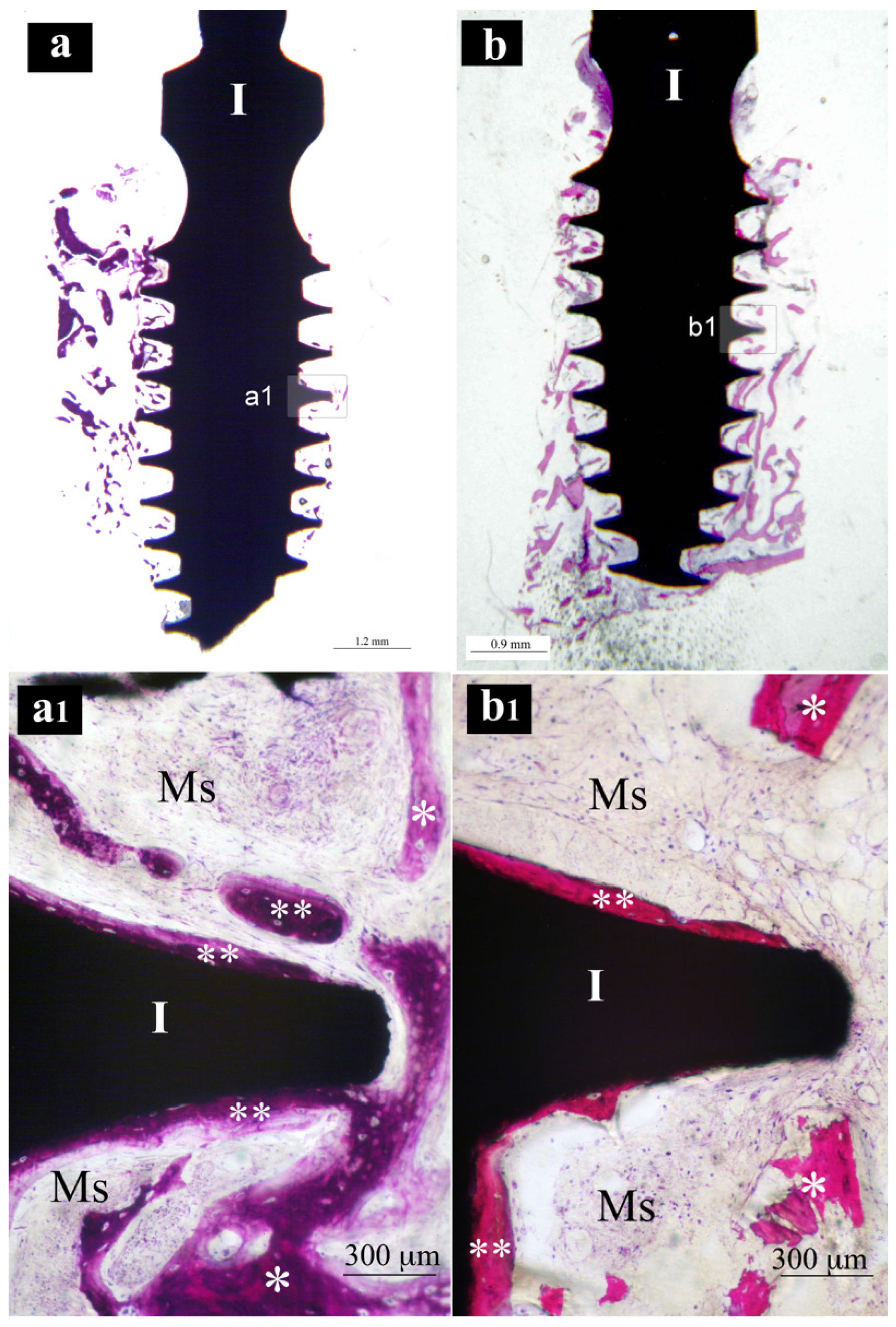
3.1. Histological
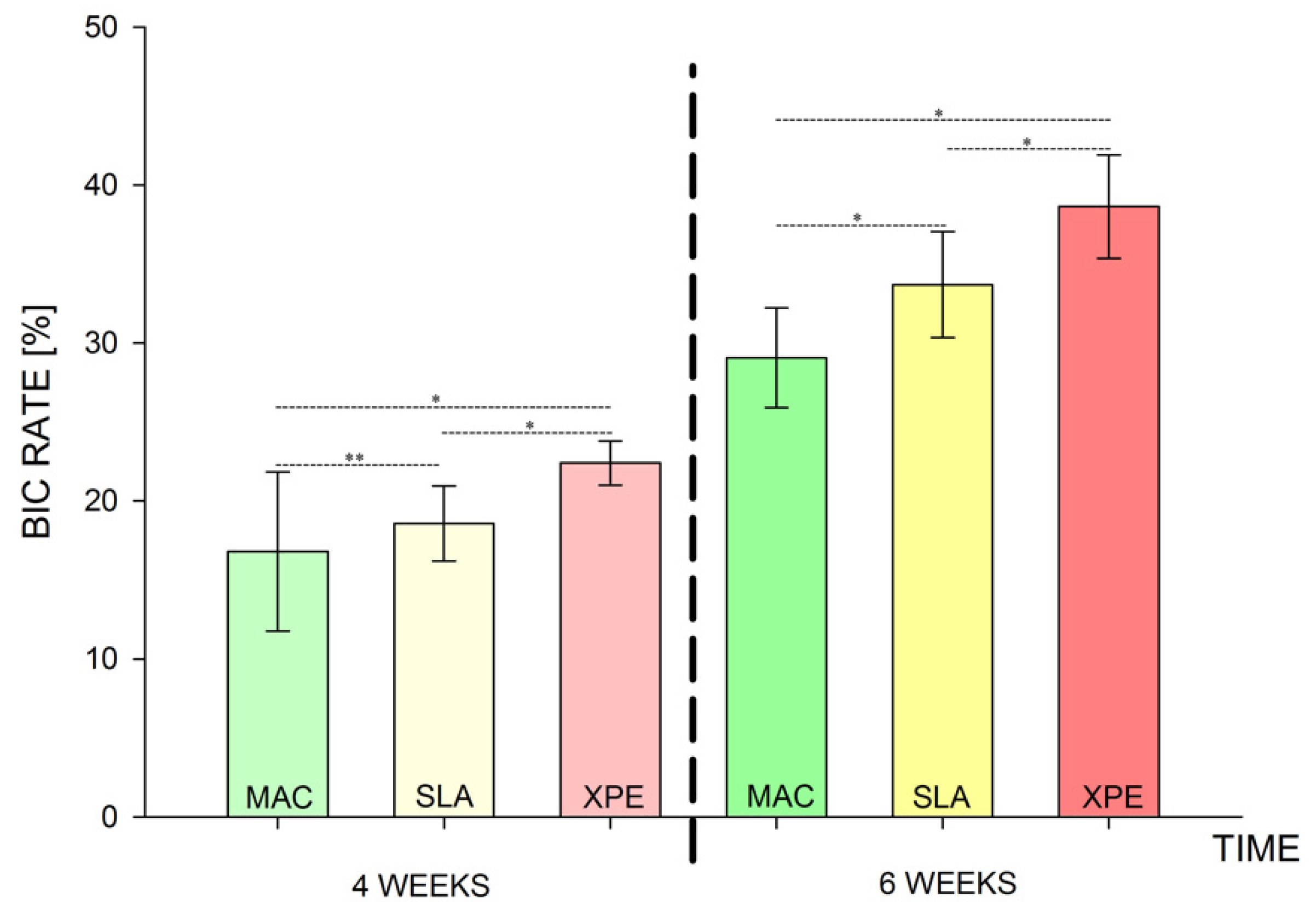
3.2. Histomorphometry
4. Discussion
5. Conclusions
- Nanostructured calcium-titanate-coated implant surfaces (XPEED®) showed higher BIC values at 4- and 6-week intervals.
- When compared to SLA and MAC surfaces, XPEED® appeared to promote bone formation around the implant very early on after placement, even in soft trabecular bone of the posterior maxilla.
- Both SLA and XPEED® surfaces showed bone formation with direct-contact osteogenesis.
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Adell, R. Tissue integrated prostheses in clinical dentistry. Int. Dent. J. 1985, 35, 259–265. [Google Scholar] [PubMed]
- Albrektsson, T.; Branemark, P.I.; Hansson, H.A.; Lindstrom, J. Osseointegrated titanium implants. Requirements for ensuring a long-lasting, direct bone-to-implant anchorage in man. Acta Orthop. Scand. 1981, 52, 155–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chrcanovic, B.R.; Albrektsson, T.; Wennerberg, A. Immediately loaded non-submerged versus delayed loaded submerged dental implants: A meta-analysis. Int. J. Oral Maxillofac. Surg. 2015, 44, 493–506. [Google Scholar] [CrossRef] [PubMed]
- Le Guehennec, L.; Soueidan, A.; Layrolle, P.; Amouriq, Y. Surface treatments of titanium dental implants for rapid osseointegration. Dent. Mater. 2007, 23, 844–854. [Google Scholar] [CrossRef] [PubMed]
- Junker, R.; Dimakis, A.; Thoneick, M.; Jansen, J.A. Effects of implant surface coatings and composition on bone integration: A systematic review. Clin. Oral Implant. Res. 2009, 20 (Suppl. 4), 185–206. [Google Scholar] [CrossRef] [PubMed]
- Dohan Ehrenfest, D.M.; Coelho, P.G.; Kang, B.S.; Sul, Y.T.; Albrektsson, T. Classification of osseointegrated implant surfaces: Materials, chemistry and topography. Trends Biotechnol. 2010, 28, 198–206. [Google Scholar] [CrossRef] [PubMed]
- Smeets, R.; Stadlinger, B.; Schwarz, F.; Beck-Broichsitter, B.; Jung, O.; Precht, C.; Kloss, F.; Grobe, A.; Heiland, M.; Ebker, T. Impact of Dental Implant Surface Modifications on Osseointegration. Biomed. Res. Int. 2016, 2016, 6285620. [Google Scholar] [CrossRef] [Green Version]
- Nicolas-Silvente, A.I.; Velasco-Ortega, E.; Ortiz-Garcia, I.; Monsalve-Guil, L.; Gil, J.; Jimenez-Guerra, A. Influence of the Titanium Implant Surface Treatment on the Surface Roughness and Chemical Composition. Materials 2020, 13, 314. [Google Scholar] [CrossRef] [Green Version]
- Demetoglu, U.; Ocak, H.; Songur, T.; Colpak, H.A. Which dental implant surface is more effective in osteointegration: RBM surface versus SLA surface. Ann. Clin. Anal. Med. 2021, 12, 736–739. [Google Scholar] [CrossRef]
- Paradowska-Stolarz, A.; Wieckiewicz, M.; Owczarek, A.; Wezgowiec, J. Natural Polymers for the Maintenance of Oral Health: Review of Recent Advances and Perspectives. Int. J. Mol. Sci. 2021, 22, 10337. [Google Scholar] [CrossRef]
- Ellingsen, J.E.; Johansson, C.B.; Wennerberg, A.; Holmen, A. Improved retention and bone-tolmplant contact with fluoride-modified titanium implants. Int. J. Oral Maxillofac. Implant. 2004, 19, 659–666. [Google Scholar]
- Buser, D.; Schenk, R.K.; Steinemann, S.; Fiorellini, J.P.; Fox, C.H.; Stich, H. Influence of surface characteristics on bone integration of titanium implants. A histomorphometric study in miniature pigs. J. Biomed. Mater. Res. 1991, 25, 889–902. [Google Scholar] [CrossRef]
- Bagno, A.; Di Bello, C. Surface treatments and roughness properties of Ti-based biomaterials. J. Mater. Sci. Mater. Med. 2004, 15, 935–949. [Google Scholar] [CrossRef] [PubMed]
- Rakic, M.; Galindo-Moreno, P.; Monje, A.; Radovanovic, S.; Wang, H.L.; Cochran, D.; Sculean, A.; Canullo, L. How frequent does peri-implantitis occur? A systematic review and meta-analysis. Clin. Oral Investig. 2018, 22, 1805–1816. [Google Scholar] [CrossRef] [PubMed]
- Fu, J.H.; Wang, H.L. Breaking the wave of peri-implantitis. Periodontol 2000 2020, 84, 145–160. [Google Scholar] [CrossRef] [PubMed]
- Chambrone, L.; Shibli, J.A.; Mercurio, C.E.; Cardoso, B.; Preshaw, P.M. Efficacy of standard (SLA) and modified sandblasted and acid-etched (SLActive) dental implants in promoting immediate and/or early occlusal loading protocols: A systematic review of prospective studies. Clin. Oral Implant. Res. 2015, 26, 359–370. [Google Scholar] [CrossRef]
- Roccuzzo, M.; Bunino, M.; Prioglio, F.; Bianchi, S.D. Early loading of sandblasted and acid-etched (SLA) implants: A prospective split-mouth comparative study. Clin. Oral Implant. Res. 2001, 12, 572–578. [Google Scholar] [CrossRef]
- Buser, D.; Belser, U.C.; Lang, N.P. The original one-stage dental implant system and its clinical application. Periodontol 2000 1998, 17, 106–118. [Google Scholar] [CrossRef]
- Cochran, D.L.; Buser, D.; ten Bruggenkate, C.M.; Weingart, D.; Taylor, T.M.; Bernard, J.P.; Peters, F.; Simpson, J.P. The use of reduced healing times on ITI implants with a sandblasted and acid-etched (SLA) surface: Early results from clinical trials on ITI SLA implants. Clin. Oral Implant. Res. 2002, 13, 144–153. [Google Scholar] [CrossRef]
- Suh, J.Y.; Jeung, O.C.; Choi, B.J.; Park, J.W. Effects of a novel calcium titanate coating on the osseointegration of blasted endosseous implants in rabbit tibiae. Clin. Oral Implant. Res. 2007, 18, 362–369. [Google Scholar] [CrossRef]
- Kubasiewicz-Ross, P.; Fleischer, M.; Pitułaj, A.; Hadzik, J.; Nawrot-Hadzik, I.; Bortkiewicz, O.; Dominiak, M.; Jurczyszyn, K. Evaluation of the three methods of bacterial decontamination on implants with three different surfaces. Adv. Clin. Exp. Med. 2020, 29, 177–182. [Google Scholar] [CrossRef] [PubMed]
- Webster, T.J.; Ejiofor, J.U. Increased osteoblast adhesion on nanophase metals: Ti, Ti6Al4V, and CoCrMo. Biomaterials 2004, 25, 4731–4739. [Google Scholar] [CrossRef] [PubMed]
- Coelho, P.G.; Jimbo, R.; Tovar, N.; Bonfante, E.A. Osseointegration: Hierarchical designing encompassing the macrometer, micrometer, and nanometer length scales. Dent. Mater. 2015, 31, 37–52. [Google Scholar] [CrossRef] [PubMed]
- Nayab, S.N.; Jones, F.H.; Olsen, I. Effects of calcium ion implantation on human bone cell interaction with titanium. Biomaterials 2005, 26, 4717–4727. [Google Scholar] [CrossRef]
- Cooper, L.F.; Zhou, Y.; Takebe, J.; Guo, J.; Abron, A.; Holmen, A.; Ellingsen, J.E. Fluoride modification effects on osteoblast behavior and bone formation at TiO2 grit-blasted c.p. titanium endosseous implants. Biomaterials 2006, 27, 926–936. [Google Scholar] [CrossRef]
- Vishwakarma, V.; Kaliaraj, G.S.; Amirtharaj Mosas, K.K. Multifunctional Coatings on Implant Materials—A Systematic Review of the Current Scenario. Coatings 2023, 13, 69. [Google Scholar] [CrossRef]
- López-Valverde, N.; Flores-Fraile, J.; Ramírez, J.M.; Macedo de Sousa, B.; Herrero-Hernández, S.; López-Valverde, A. Bioactive surfaces vs. conventional surfaces in titanium dental implants: A comparative systematic review. J. Clin. Med. 2020, 9, 2047. [Google Scholar] [CrossRef]
- Coelho, P.G.; Suzuki, M. Evaluation of an IBAD thin-film process as an alternative method for surface incorporation of bioceramics on dental implants: A study in dogs. J. Appl. Oral Sci. 2005, 13, 87–92. [Google Scholar] [CrossRef] [Green Version]
- Mendes, V.C.; Moineddin, R.; Davies, J.E. The effect of discrete calcium phosphate nanocrystals on bone-bonding to titanium surfaces. Biomaterials 2007, 28, 4748–4755. [Google Scholar] [CrossRef]
- Makary, C.; Menhall, A.; Zammarie, C.; Lombardi, T.; Lee, S.Y.; Stacchi, C.; Park, K.B. Primary Stability Optimization by Using Fixtures with Different Thread Depth According To Bone Density: A Clinical Prospective Study on Early Loaded Implants. Materials 2019, 12, 2398. [Google Scholar] [CrossRef] [Green Version]
- Park, J.W.; Suh, J.Y.; Chung, H.J. Effects of calcium ion incorporation on osteoblast gene expression in MC3T3-E1 cells cultured on microstructured titanium surfaces. J. Biomed. Mater. Res. A 2008, 86, 117–126. [Google Scholar] [CrossRef] [PubMed]
- Marconcini, S.; Giammarinaro, E.; Toti, P.; Alfonsi, F.; Covani, U.; Barone, A. Longitudinal analysis on the effect of insertion torque on delayed single implants: A 3-year randomized clinical study. Clin. Implant. Dent. Relat Res. 2018, 20, 322–332. [Google Scholar] [CrossRef] [PubMed]
- Duyck, J.; Roesems, R.; Cardoso, M.V.; Ogawa, T.; De Villa Camargos, G.; Vandamme, K. Effect of insertion torque on titanium implant osseointegration: An animal experimental study. Clin. Oral Implant. Res. 2015, 26, 191–196. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Atsumi, M.; Park, S.H.; Wang, H.L. Methods used to assess implant stability: Current status. Int. J. Oral Maxillofac. Implant. 2007, 22, 743–754. [Google Scholar]
- Choi, J.Y.; Park, J.I.; Chae, J.S.; Yeo, I.L. Comparison of micro-computed tomography and histomorphometry in the measurement of bone-implant contact ratios. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2019, 128, 87–95. [Google Scholar] [CrossRef]
- Hadzik, J.; Kubasiewicz-Ross, P.; Simka, W.; Gębarowski, T.; Barg, E.; Cieśla-Niechwiadowicz, A.; Trzcionka Szajna, A.; Szajna, E.; Gedrange, T.; Kozakiewicz, M.; et al. Fractal Dimension and Texture Analysis in the Assessment of Experimental La-ser-Induced Periodic Surface Structures (LIPSS) Dental Implant Surface—In Vitro Study Preliminary Report. Materials 2022, 15, 2713. [Google Scholar] [CrossRef]
- McCullough, J.J.; Klokkevold, P.R. The effect of implant macro-thread design on implant stability in the early post-operative period: A randomized, controlled pilot study. Clin. Oral Implant. Res. 2017, 28, 1218–1226. [Google Scholar] [CrossRef]
- Bernhardt, R.; Kuhlisch, E.; Schulz, M.C.; Eckelt, U.; Stadlinger, B. Comparison of bone-implant contact and bone-implant volume between 2D-histological sections and 3D-SRmicroCT slices. Eur. Cell Mater. 2012, 23, 237–247, discussion 247–238. [Google Scholar] [CrossRef]
- Park, Y.S.; Yi, K.Y.; Lee, I.S.; Jung, Y.C. Correlation between microtomography and histomorphometry for assessment of implant osseointegration. Clin. Oral Implant. Res. 2005, 16, 156–160. [Google Scholar] [CrossRef]
- Gasik, M.; Braem, A.; Chaudhari, A.; Duyck, J.; Vleugels, J. Titanium implants with modified surfaces: Meta-analysis of in vivo osteointegration. Mater. Sci. Eng. C Mater. Biol. Appl. 2015, 49, 152–158. [Google Scholar] [CrossRef] [Green Version]
- von Wilmowsky, C.; Moest, T.; Nkenke, E.; Stelzle, F.; Schlegel, K.A. Implants in bone: Part II. Research on implant osseointegration: Material testing, mechanical testing, imaging and histoanalytical methods. Oral Maxillofac. Surg. 2014, 18, 355–372. [Google Scholar] [CrossRef] [PubMed]
- Lian, Z.; Guan, H.; Ivanovski, S.; Loo, Y.C.; Johnson, N.W.; Zhang, H. Effect of bone to implant contact percentage on bone remodelling surrounding a dental implant. Int. J. Oral Maxillofac. Surg. 2010, 39, 690–698. [Google Scholar] [CrossRef] [PubMed]
- World Medical Association. World Medical Association Declaration of Helsinki: Ethical principles for medical research involving human subjects. JAMA 2013, 310, 2191–2194. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zita Gomes, R.; de Vasconcelos, M.R.; Lopes Guerra, I.M.; de Almeida, R.A.B.; de Campos Felino, A.C. Implant Stability in the Posterior Maxilla: A Controlled Clinical Trial. Biomed. Res. Int. 2017, 2017, 6825213. [Google Scholar] [CrossRef] [PubMed]
- Mangano, C.; Shibli, J.A.; Pires, J.T.; Luongo, G.; Piattelli, A.; Iezzi, G. Early Bone Formation around Immediately Loaded Transitional Implants Inserted in the Human Posterior Maxilla: The Effects of Fixture Design and Surface. Biomed. Res. Int. 2017, 2017, 4152506. [Google Scholar] [CrossRef]
- Romero-Millan, J.J.; Aizcorbe-Vicente, J.; Penarrocha-Diago, M.; Galindo-Moreno, P.; Canullo, L.; Penarrocha-Oltra, D. Implants in the Posterior Maxilla: Open Sinus Lift Versus Conventional Implant Placement. A Systematic Review. Int. J. Oral Maxillofac. Implant. 2019, 34, e65–e76. [Google Scholar] [CrossRef] [PubMed]
- Mangano, F.; Raspanti, M.; Maghaireh, H.; Mangano, C. Scanning Electron Microscope (SEM) Evaluation of the Interface between a Nanostructured Calcium-Incorporated Dental Implant Surface and the Human Bone. Materials 2017, 10, 1438. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rameh, S.; Menhall, A.; Younes, R. Key factors influencing short implant success. Oral Maxillofac. Surg. 2020, 24, 263–275. [Google Scholar] [CrossRef]
- Lioubavina-Hack, N.; Lang, N.P.; Karring, T. Significance of primary stability for osseointegration of dental implants. Clin. Oral Implant. Res. 2006, 17, 244–250. [Google Scholar] [CrossRef]
- Sener-Yamaner, I.D.; Yamaner, G.; Sertgoz, A.; Canakci, C.F.; Ozcan, M. Marginal Bone Loss Around Early-Loaded SLA and SLActive Implants: Radiological Follow-Up Evaluation Up to 6.5 Years. Implant. Dent. 2017, 26, 592–599. [Google Scholar] [CrossRef] [Green Version]
- Gastaldi, G.; Grusovin, M.G.; Felice, P.; Barausse, C.; Ippolito, D.R.; Esposito, M. Early loading of maxillary titanium implants with a nanostructured calcium-incorporated surface (Xpeed): 5-year results from a multicentre randomised controlled trial. Eur J Oral Implantol. 2017, 10, 415–424. [Google Scholar] [PubMed]
- Cochran, D.L.; Jackson, J.M.; Bernard, J.P.; ten Bruggenkate, C.M.; Buser, D.; Taylor, T.D.; Weingart, D.; Schoolfield, J.D.; Jones, A.A.; Oates, T.W., Jr. A 5-year prospective multicenter study of early loaded titanium implants with a sandblasted and acid-etched surface. Int. J. Oral Maxillofac. Implant. 2011, 26, 1324–1332. [Google Scholar]
- Esposito, M.; Siormpas, K.; Mitsias, M.; Bechara, S.; Trullenque-Eriksson, A.; Pistilli, R. Immediate, early (6 weeks) and delayed loading (3 months) of single implants: 4-month post-loading from a multicenter pragmatic randomised controlled trial. Eur. J. Oral Implant. 2016, 9, 249–260. [Google Scholar]
- Silva, A.S.; Martins, D.; Sá, J.; Mendes, J.M. Clinical evaluation of the implant survival rate in patients subjected to immediate implant loading protocols. Dent. Med. Probl. 2021, 58, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Grusovin, M.G.; Maghaireh, H.; Worthington, H.V. Interventions for replacing missing teeth: Different times for loading dental implants. Cochrane Database Syst. Rev. 2013, 2013, CD003878. [Google Scholar] [CrossRef] [Green Version]
- Nicolau, P.; Guerra, F.; Reis, R.; Krafft, T.; Benz, K.; Jackowski, J. 10-year outcomes with immediate and early loaded implants with a chemically modified SLA surface. Quintessence Int. 2019, 50, 114–124. [Google Scholar] [CrossRef]
- Chen, J.; Cai, M.; Yang, J.; Aldhohrah, T.; Wang, Y. Immediate versus early or conventional loading dental implants with fixed prostheses: A systematic review and meta-analysis of randomized controlled clinical trials. J. Prosthet. Dent. 2019, 122, 516–536. [Google Scholar] [CrossRef] [Green Version]
- Krawiec, M.; Olchowy, C.; Kubasiewicz-Ross, P.; Hadzik, J.; Dominiak, M. Role of implant loading time in the prevention of marginal bone loss after implant-supported restorations: A targeted review. Dent. Med. Probl. 2022, 59, 475–481. [Google Scholar] [CrossRef]
- Hao, C.P.; Cao, N.J.; Zhu, Y.H.; Wang, W. The osseointegration and stability of dental implants with different surface treatments in animal models: A network meta-analysis. Sci. Rep. 2021, 11, 13849. [Google Scholar] [CrossRef]
- Norton, M.R.; Astrom, M. The Influence of Implant Surface on Maintenance of Marginal Bone Levels for Three Premium Implant Brands: A Systematic Review and Meta-analysis. Int. J. Oral Maxillofac. Implant. 2020, 35, 1099–1111. [Google Scholar] [CrossRef]
- Oates, T.W.; Valderrama, P.; Bischof, M.; Nedir, R.; Jones, A.; Simpson, J.; Toutenburg, H.; Cochran, D.L. Enhanced implant stability with a chemically modified SLA surface: A randomized pilot study. Int. J. Oral Maxillofac. Implant. 2007, 22, 755–760. [Google Scholar]
- Traini, T.; Mangano, C.; Perrotti, V.; Caputi, S.; Coelho, P.; Piattelli, A.; Iezzi, G. Human bone reactions around implants with adverse interfacial bone strain over 20 years. J. Biomed. Mater. Res. B Appl. Biomater. 2014, 102, 1342–1352. [Google Scholar] [CrossRef]
- Iezzi, G.; Piattelli, A.; Mangano, C.; Degidi, M.; Testori, T.; Vantaggiato, G.; Fiera, E.; Frosecchi, M.; Floris, P.; Perroni, R.; et al. Periimplant Bone Response in Human-Retrieved, Clinically Stable, Successful, and Functioning Dental Implants After a Long-Term Loading Period: A Report of 17 Cases From 4 to 20 Years. Implant. Dent. 2016, 25, 380–386. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayakawa, T.; Kiba, H.; Yasuda, S.; Yamamoto, H.; Nemoto, K. A histologic and histomorphometric evaluation of two types of retrieved human titanium implants. Int. J. Periodontics Restor. Dent. 2002, 22, 164–171. [Google Scholar]
- Kozakiewicz, M.; Skorupska, M.; Wach, T. What Does Bone Corticalization around Dental Implants Mean in Light of Ten Years of Follow-Up? J. Clin. Med. 2022, 11, 3545. [Google Scholar] [CrossRef] [PubMed]
- Kozakiewicz, M. Measures of Corticalization. J. Clin. Med. 2022, 11, 5463. [Google Scholar] [CrossRef]
- Shah, F.A.; Nilson, B.; Branemark, R.; Thomsen, P.; Palmquist, A. The bone-implant interface-nanoscale analysis of clinically retrieved dental implants. Nanomedicine 2014, 10, 1729–1737. [Google Scholar] [CrossRef]
- Faeda, R.S.; do Nascimento, S.C.S.; Santos, P.L.; Boeck, R.J.N.; Sartori, R.; Margonar, R.; Marcantonio, E., Jr. Human non-decalcified histology of three dental implants 45 months under function-a case report. Int. J. Implant. Dent. 2019, 5, 33. [Google Scholar] [CrossRef] [Green Version]
- Albrektsson, T. Hard tissue implant interface. Aust. Dent. J. 2008, 53 (Suppl. S1), S34–S38. [Google Scholar] [CrossRef]
- Lang, N.P.; Salvi, G.E.; Huynh-Ba, G.; Ivanovski, S.; Donos, N.; Bosshardt, D.D. Early osseointegration to hydrophilic and hydrophobic implant surfaces in humans. Clin. Oral Implant. Res. 2011, 22, 349–356. [Google Scholar] [CrossRef]
- Stach, R.M.; Kohles, S.S. A meta-analysis examining the clinical survivability of machined-surfaced and osseotite implants in poor-quality bone. Implant. Dent. 2003, 12, 87–96. [Google Scholar] [CrossRef] [PubMed]
- Glauser, R.; Ree, A.; Lundgren, A.; Gottlow, J.; Hammerle, C.H.; Scharer, P. Immediate occlusal loading of Branemark implants applied in various jawbone regions: A prospective, 1-year clinical study. Clin. Implant. Dent. Relat Res. 2001, 3, 204–213. [Google Scholar] [CrossRef] [PubMed]
- Sayin Ozel, G.; Inan, O.; Secilmis Acar, A.; Alniacik Iyidogan, G.; Dolanmaz, D.; Yildirim, G. Stability of dental implants with sandblasted and acid-etched (SLA) and modified (SLActive) surfaces during the osseointegration period. J. Dent. Res. Dent. Clin. Dent. Prospect. 2021, 15, 226–231. [Google Scholar] [CrossRef]
- Baker, C.E.; Moore-Lotridge, S.N.; Hysong, A.A.; Posey, S.L.; Robinette, J.P.; Blum, D.M.; Benvenuti, M.A.; Cole, H.A.; Egawa, S.; Okawa, A.; et al. Bone Fracture Acute Phase Response-A Unifying Theory of Fracture Repair: Clinical and Scientific Implications. Clin. Rev. Bone Min. Metab. 2018, 16, 142–158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Raghavendra, S.; Wood, M.C.; Taylor, T.D. Early wound healing around endosseous implants: A review of the literature. Int. J. Oral Maxillofac. Implant. 2005, 20, 425–431. [Google Scholar]
- Pellegrini, G.; Francetti, L.; Barbaro, B.; Del Fabbro, M. Novel surfaces and osseointegration in implant dentistry. J. Investig. Clin. Dent. 2018, 9, e12349. [Google Scholar] [CrossRef] [PubMed]
- Abrahamsson, I.; Berglundh, T.; Linder, E.; Lang, N.P.; Lindhe, J. Early bone formation adjacent to rough and turned endosseous implant surfaces. An experimental study in the dog. Clin. Oral Implant. Res. 2004, 15, 381–392. [Google Scholar] [CrossRef]
- Buser, D.; Broggini, N.; Wieland, M.; Schenk, R.K.; Denzer, A.J.; Cochran, D.L.; Hoffmann, B.; Lussi, A.; Steinemann, S.G. Enhanced bone apposition to a chemically modified SLA titanium surface. J. Dent. Res. 2004, 83, 529–533. [Google Scholar] [CrossRef]
- Kim, H.; Choi, S.H.; Ryu, J.J.; Koh, S.Y.; Park, J.H.; Lee, I.S. The biocompatibility of SLA-treated titanium implants. Biomed. Mater. 2008, 3, 025011. [Google Scholar] [CrossRef]
- Schwarz, F.; Herten, M.; Sager, M.; Wieland, M.; Dard, M.; Becker, J. Histological and immunohistochemical analysis of initial and early osseous integration at chemically modified and conventional SLA titanium implants: Preliminary results of a pilot study in dogs. Clin. Oral Implant. Res. 2007, 18, 481–488. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Inclusion Criteria | Exclusion Criteria |
|---|---|
| Height of the residual bone crest in the programmed implant site ≥ 9 mm | Myocardial infarction within the past 6 months. |
| Thickness of the residual bone crest in the programmed implant site ≥ 7 mm. | Poorly controlled diabetes (HBA1c > 7.5%). |
| Availability, in each sector, of sufficient mesio-distal space allowing placement of 2 standard-sized implants and at least 2 mini-implants (3.5 × 8.5 mm) for retrieval. | Coagulation disorders. |
| Healed bone crest (≥3 months elapsed after extraction or tooth loss). | Radiotherapy to the head/neck area within the past two years. |
| Age > 18 years. | Present or past treatment with intravenous bisphosphonates. |
| Immunocompromised patients. | |
| Ability to examine and fully understand the study protocol. | Psychological or psychiatric problems. |
| Alcohol or drug abuse. | |
| Poor oral hygiene and motivation (full mouth plaque score > 30% and/or full mouth bleeding score > 20%). | |
| Uncontrolled periodontal disease. |
| Normality Test: Passed (p = 0.528) | |||||
|---|---|---|---|---|---|
| Equal Variance Test: Passed (p = 0.123) | |||||
| Source of Variation | DF * | SS * | MS * | F * | p |
| SURFACES | 2 | 290,982 | 145,491 | 17,956 | <0.001 |
| TIME | 1 | 1,528,390 | 1,528,390 | 188,626 | <0.001 |
| SURFACES × TIME | 2 | 17,050 | 8525 | 1052 | 0.362 |
| Residual | 29 | 234,980 | 8103 | ||
| Total | 34 | 2,481,227 | 72,977 | ||
| Power of performed test with alpha = 0.0500: for SURFACES: 1000 | |||||
| Power of performed test with alpha = 0.0500: for TIME: 1000 | |||||
| Least Square Means for SURFACES **1 | ||
|---|---|---|
| Groups* | Mean | SEM |
| SLA (n = 13) | 26,131 | 0.811 |
| XPEED® (n = 16) | 30,514 | 0.717 |
| MACHINED (n = 6) | 22,933 | 1162 |
| Least square means for TIME **2 | ||
| Groups * | Mean | SEM |
| 4W (n = 18) | 19,254 | 0.716 |
| 6W (n = 17) | 33,798 | 0.780 |
| Least square means for SURFACES × TIME **3 | ||
| Groups * | Mean | SEM |
| SLA × 4W (n = 7) | 18,562 | 1006 |
| SLA × 6W (n = 6) | 33,700 | 1273 |
| XPEED® × 4W (n = 8) | 22,400 | 0.949 |
| XPEED® × 6W (n = 8) | 38,629 | 1076 |
| MAC × 4W (n = 3) | 16,800 | 1643 |
| MAC × 6W (n = 3) | 29,067 | 1643 |
| Comparison | Diff of Means | t | Unadjusted P | Critical Level | Significant? |
|---|---|---|---|---|---|
| Comparisons for factor: SURFACES | |||||
| XPEED® vs. MAC | 7581 | 5551 | 0.00000549 | 0.017 | Yes |
| XPEED® vs. SLA | 4383 | 4047 | 0.000352 | 0.025 | Yes |
| SLA vs. MAC | 3198 | 2256 | 0.0318 | 0.050 | Yes |
| Comparisons for factor: TIME | |||||
| 6W vs. 4W | 14,544 | 13,734 | 3191 × 10−14 | 0.050 | Yes |
| Comparisons for factor: TIME within SLA | |||||
| 6W vs. 4W | 15,138 | 9328 | 0.000 | 0.050 | Yes |
| Comparisons for factor: TIME within XPEED® | |||||
| 6W vs. 4W | 16,229 | 11,313 | 0.000 | 0.050 | Yes |
| Comparisons for factor: TIME within MAC | |||||
| 6W vs. 4W | 12,267 | 5278 | 0.000 | 0.050 | Yes |
| Comparisons for factor: SURFACES within 4W | |||||
| XPEED® vs. MAC | 5600 | 2951 | 0.006 | 0.017 | Yes |
| XPEED® vs. SLA | 3837 | 2774 | 0.010 | 0.025 | Yes |
| SLA vs. MAC | 1763 | 0.915 | 0.368 | 0.050 | No |
| Comparisons for factor: SURFACES within 6W | |||||
| XPEED® vs. MAC | 9562 | 4868 | 0.000 | 0.017 | Yes |
| XPEED® vs. SLA | 4929 | 2957 | 0.006 | 0.025 | Yes |
| SLA vs. MAC | 4633 | 2229 | 0.034 | 0.050 | Yes |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Makary, C.; Menhall, A.; Lahoud, P.; An, H.-W.; Park, K.-B.; Traini, T. Nanostructured Calcium-Incorporated Surface Compared to Machined and SLA Dental Implants—A Split-Mouth Randomized Case/Double-Control Histological Human Study. Nanomaterials 2023, 13, 357. https://doi.org/10.3390/nano13020357
Makary C, Menhall A, Lahoud P, An H-W, Park K-B, Traini T. Nanostructured Calcium-Incorporated Surface Compared to Machined and SLA Dental Implants—A Split-Mouth Randomized Case/Double-Control Histological Human Study. Nanomaterials. 2023; 13(2):357. https://doi.org/10.3390/nano13020357
Chicago/Turabian StyleMakary, Christian, Abdallah Menhall, Pierre Lahoud, Hyun-Wook An, Kwang-Bum Park, and Tonino Traini. 2023. "Nanostructured Calcium-Incorporated Surface Compared to Machined and SLA Dental Implants—A Split-Mouth Randomized Case/Double-Control Histological Human Study" Nanomaterials 13, no. 2: 357. https://doi.org/10.3390/nano13020357