
Efficacy of Nanofiber Sheets Incorporating Lenvatinib in a Hepatocellular Carcinoma Xenograft Model

 , , , , , , ,
, , , , , , ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Fabrication of Electrospun PCL Nanofiber Sheets
2.2. Drug Release Profile
2.3. Cell Lines and Reagents
2.4. Animals
2.5. Treatment of Subcutaneous Tumor Models
2.6. Peritoneal Metastasis Tumor Therapy in Mice
2.7. Histological Examination
2.8. Quantification of the Serum Lenvatinib Levels
2.9. Statistical Analysis
3. Results
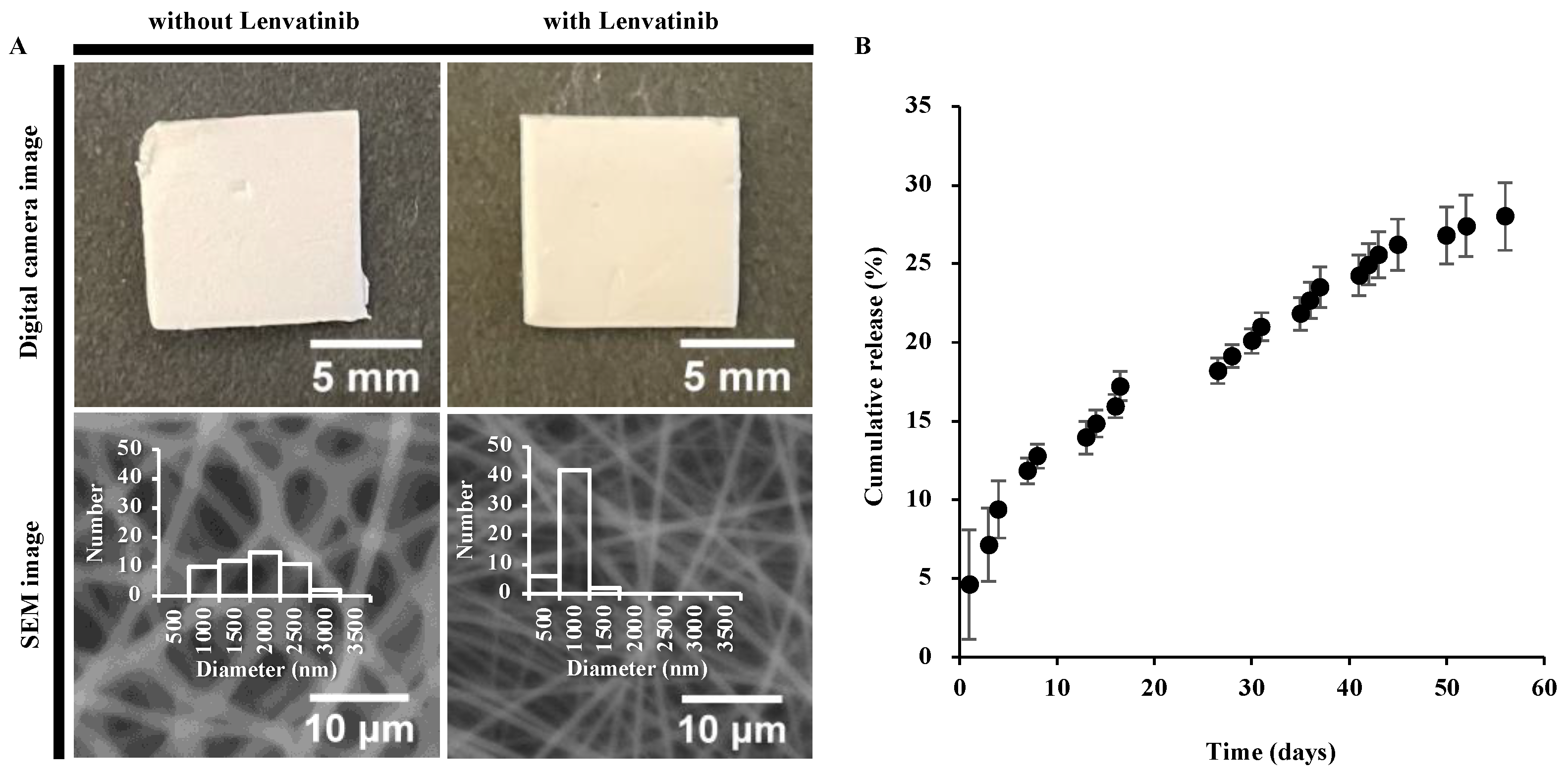
3.1. PCL Nanofiber Sheets Release Lenvatinib in a Sustainable Manner
3.2. Nanofibrous Sheets Incorporating Lenvatinib Exhibited Antitumor Effects
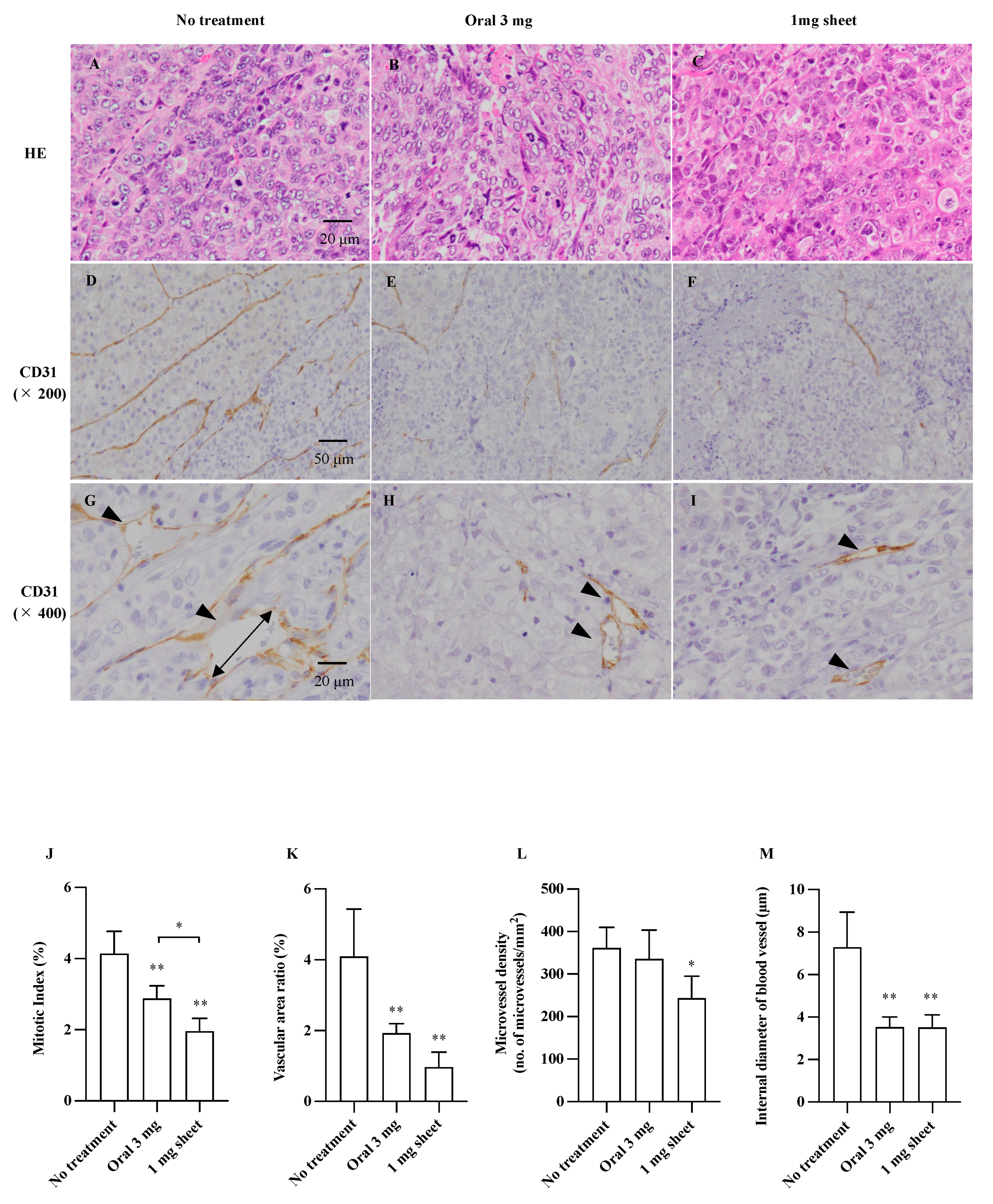
3.3. Histopathological Analysis
3.4. Lenvatinib Sheets Maintain the Serum Drug Level
3.5. The Antitumor Effect of Lenvatinib Sheets in Different Insertion Positions
3.6. Lenvatinib Sheets Improved Survival in a Mouse Peritoneal Seeding Model
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| AE | Adverse effects |
| DDS | Drug delivery system |
| H&E | Hematoxylin and eosin |
| HCC | Hepatocellular carcinoma |
| MI | Mitotic index |
| MVD | Microvessel density |
| PBS | Phosphate-buffered saline |
| VEGF | Vascular endothelial growth factor |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Kelley, R.K.; Villanueva, A.; Singal, A.G.; Pikarsky, E.; Roayaie, S.; Lencioni, R.; Koike, K.; Zucman-Rossi, J.; Finn, R.S. Hepatocellular carcinoma. Nat. Rev. Dis. Primers 2021, 7, 6. [Google Scholar] [CrossRef] [PubMed]
- Llovet, J.M.; Ricci, S.; Mazzaferro, V.; Hilgard, P.; Gane, E.; Blanc, J.-F.; De Oliveira, A.C.; Santoro, A.; Raoul, J.-L.; Forner, A.; et al. Sorafenib in advanced hepatocellular carcinoma. N. Engl. J. Med. 2008, 359, 378–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, A.-L.; Kang, Y.-K.; Chen, Z.; Tsao, C.-J.; Qin, S.; Kim, J.S.; Luo, R.; Feng, J.; Ye, S.; Yang, T.-S.; et al. Efficacy and safety of sorafenib in patients in the Asia-Pacific region with advanced hepatocellular carcinoma: A phase III randomised, double-blind, placebo-controlled trial. Lancet Oncol. 2009, 10, 25–34. [Google Scholar] [CrossRef]
- Kudo, M.; Finn, R.S.; Qin, S.; Han, K.-H.; Ikeda, K.; Piscaglia, F.; Baron, A.; Park, J.-W.; Han, G.; Jassem, J.; et al. Lenvatinib versus sorafenib in first-line treatment of patients with unresectable hepatocellular carcinoma: A randomised phase 3 non-inferiority trial. Lancet 2018, 391, 1163–1173. [Google Scholar] [CrossRef] [Green Version]
- Finn, R.S.; Qin, S.; Ikeda, M.; Galle, P.R.; Ducreux, M.; Kim, T.-Y.; Kudo, M.; Breder, V.; Merle, P.; Kaseb, A.O.; et al. Atezolizumab plus bevacizumab in unresectable hepatocellular carcinoma. N. Engl. J. Med. 2020, 382, 1894–1905. [Google Scholar] [CrossRef]
- Eso, Y.; Marusawa, H. Novel approaches for molecular targeted therapy against hepatocellular carcinoma. Hepatol. Res. 2018, 48, 597–607. [Google Scholar] [CrossRef]
- Ikeda, K.; Kudo, M.; Kawazoe, S.; Osaki, Y.; Ikeda, M.; Okusaka, T.; Tamai, T.; Suzuki, T.; Hisai, T.; Hayato, S.; et al. Phase 2 study of lenvatinib in patients with advanced hepatocellular carcinoma. J. Gastroenterol. 2017, 52, 512–519. [Google Scholar] [CrossRef] [Green Version]
- Handa, M.; Beg, S.; Shukla, R.; Barkat, M.A.; Choudhry, H.; Singh, K.K. Recent advances in lipid-engineered multifunctional nanophytomedicines for cancer targeting. J. Control. Release 2021, 340, 48–59. [Google Scholar] [CrossRef]
- Subbiah, V.; Grilley-Olson, J.E.; Combest, A.J.; Sharma, N.; Tran, R.H.; Bobe, I.; Osada, A.; Takahashi, K.; Balkissoon, J.; Camp, A.; et al. Phase Ib/II trial of NC-6004 (nanoparticle cisplatin) plus gemcitabine in patients with advanced solid tumors. Clin. Cancer Res. 2018, 24, 43–51. [Google Scholar] [CrossRef] [Green Version]
- Takahashi, S.; Karayama, M.; Takahashi, M.; Watanabe, J.; Minami, H.; Yamamoto, N.; Kinoshita, I.; Lin, C.-C.; Im, Y.-H.; Achiwa, I.; et al. Pharmacokinetics, safety, and efficacy of trastuzumab deruxtecan with concomitant ritonavir or itraconazole in patients with HER2-expressing advanced solid tumors. Clin. Cancer Res. 2021, 27, 5771–5780. [Google Scholar] [CrossRef] [PubMed]
- Tang, L.; He, S.; Yin, Y.; Liu, H.; Hu, J.; Cheng, J.; Wang, W. Combination of nanomaterials in cell-based drug delivery systems for cancer treatment. Pharmaceutics 2021, 13, 1888. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.M.; Patel, M.; Patel, R. PLGA core-shell nano/microparticle delivery system for biomedical application. Polymers 2021, 13, 3471. [Google Scholar] [CrossRef] [PubMed]
- Hou, J.; Li, C.; Cheng, L.; Guo, S.; Zhang, Y.; Tang, T. Study on hydrophilic 5-fluorouracil release from hydrophobic poly(ε-caprolactone) cylindrical implants. Drug Dev. Ind. Pharm. 2011, 37, 1068–1075. [Google Scholar] [CrossRef] [PubMed]
- Niiyama, E.; Uto, K.; Lee, C.M.; Sakura, K.; Ebara, M. Hyperthermia nanofiber platform synergized by sustained release of paclitaxel to improve antitumor efficiency. Adv. Healthc. Mater. 2019, 8, 1900102. [Google Scholar] [CrossRef] [PubMed]
- Gholipour Kanani, A.; Bahrami, S.H. Effect of changing solvents on poly(-caprolactone) nanofibrous webs morphology. J. Nanomater. 2011, 2011, 724153. [Google Scholar] [CrossRef] [Green Version]
- Niiyama, E.; Uto, K.; Lee, C.M.; Sakura, K.; Ebara, M. Alternating magnetic field-triggered switchable nanofiber mesh for cancer thermo-chemotherapy. Polymers 2018, 10, 1018. [Google Scholar] [CrossRef] [Green Version]
- Miyamura, S.; Iwahashi, T.; Sayanagi, J.; Hirai, Y.; Okada, K.; Oka, K.; Niiyama, E.; Uto, K.; Ebara, M.; Yoshikawa, H.; et al. A nanofiber sheet incorporating vitamin B12 promotes nerve regeneration in a rat neurorrhaphy model. Plast. Reconstr. Surg. Glob. Open 2019, 7, e2538. [Google Scholar] [CrossRef]
- Niiyama, E.; Uto, K.; Ebara, M. Electrospun PCL-PCL polyblend nanofibers with high- and low-molecular weight for controlled degradation. Chem. Lett. 2019, 48, 623–626. [Google Scholar] [CrossRef]
- Matsuki, M.; Hoshi, T.; Yamamoto, Y.; Ikemori-Kawada, M.; Minoshima, Y.; Funahashi, Y.; Matsui, J. Lenvatinib inhibits angiogenesis and tumor fibroblast growth factor signaling pathways in human hepatocellular carcinoma models. Cancer Med. 2018, 7, 2641–2653. [Google Scholar] [CrossRef]
- Matsuki, M.; Adachi, Y.; Ozawa, Y.; Kimura, T.; Hoshi, T.; Okamoto, K.; Tohyama, O.; Mitsuhashi, K.; Yamaguchi, A.; Matsui, J.; et al. Targeting of tumor growth and angiogenesis underlies the enhanced antitumor activity of lenvatinib in combination with everolimus. Cancer Sci. 2017, 108, 763–771. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Iwai, H.; Utsunomiya, K.; Kono, Y.; Kobayashi, Y.; Van Bui, D.; Sawada, S.; Yun, Y.; Mitani, A.; Kondo, N.; et al. Combination therapy with lenvatinib and radiation significantly inhibits thyroid cancer growth by uptake of tyrosine kinase inhibitor. Exp. Cell Res. 2021, 398, 112390. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Tanaka, H.; Ebara, M.; Uto, K.; Matsuoka, H.; Nishimoto, S.; Okada, K.; Murase, T.; Yoshikawa, H. Electrospun nanofiber sheets incorporating methylcobalamin promote nerve regeneration and functional recovery in a rat sciatic nerve crush injury model. Acta Biomater. 2017, 53, 250–259. [Google Scholar] [CrossRef] [PubMed]
- Ishigami, H.; Fujiwara, Y.; Fukushima, R.; Nashimoto, A.; Yabusaki, H.; Imano, M.; Imamoto, H.; Kodera, Y.; Uenosono, Y.; Amagai, K.; et al. Phase III trial comparing intraperitoneal and intravenous paclitaxel plus S-1 versus cisplatin plus S-1 in patients with gastric cancer with peritoneal metastasis: PHOENIX-GC trial. J. Clin. Oncol. 2018, 36, 1922–1929. [Google Scholar] [CrossRef] [PubMed]
- Tamai, T.; Hayato, S.; Hojo, S.; Suzuki, T.; Okusaka, T.; Ikeda, K.; Kumada, H. Dose finding of lenvatinib in subjects with advanced hepatocellular carcinoma based on population pharmacokinetic and exposure–response analyses. J. Clin. Pharmacol. 2017, 57, 1138–1147. [Google Scholar] [CrossRef] [PubMed]
- Nagahama, M.; Ozeki, T.; Suzuki, A.; Sugino, K.; Niioka, T.; Ito, K.; Miura, M. Association of lenvatinib trough plasma concentrations with lenvatinib-induced toxicities in Japanese patients with thyroid cancer. Med. Oncol. 2019, 36, 39. [Google Scholar] [CrossRef]
- Low, S.S.; Lim, C.N.; Yew, M.; Chai, W.S.; Low, L.E.; Manickam, S.; Tey, B.T.; Show, P.L. Recent ultrasound advancements for the manipulation of nanobiomaterials and nanoformulations for drug delivery. Ultrason. Sonochem. 2021, 80, 105805. [Google Scholar] [CrossRef]
- Zhao, W.; Zhao, Y.; Wang, Q.; Liu, T.; Sun, J.; Zhang, R. Remote light-responsive nanocarriers for controlled drug delivery: Advances and perspectives. Small 2019, 15, e1903060. [Google Scholar] [CrossRef]
- Hornok, V. Serum albumin nanoparticles: Problems and prospects. Polymers 2021, 13, 3759. [Google Scholar] [CrossRef]
- Wang-Gillam, A.; Li, C.-P.; Bodoky, G.; Dean, A.; Shan, Y.-S.; Jameson, G.; Macarulla, T.; Lee, K.-H.; Cunningham, D.; Blanc, J.F.; et al. Nanoliposomal irinotecan with fluorouracil and folinic acid in metastatic pancreatic cancer after previous gemcitabine-based therapy (NAPOLI-1): A global, randomised, open-label, phase 3 trial. Lancet 2016, 387, 545–557. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 2 Weeks | 4 Weeks | 8 Weeks |
|---|---|---|
| 14.85 ± 0.86% | 19.15 ± 0.73% | 28.02 ± 2.15% |
| Tumor Volume (mm3) | Aspartate Transaminase (IU/L) | Lactate Dehydrogenase (IU/L) | ||
|---|---|---|---|---|
| Day 7 | Day 14 | Day 14 | Day 14 | |
| No treatment | 1102 ± 138 | 2049 ± 313 | 182 ± 89 | 1417 ± 864 |
| Oral 3 mg | 0787 ± 128 | 0780 ± 111 | 115 ± 20 | 0608 ± 117 |
| 1 mg sheet | 354 ± 55 | 375 ± 54 | 090 ± 26 | 0441 ± 197 |
| 2 mg sheet | 344 ± 38 | 315 ± 67 | — | — |
| Mitotic Index | Vascular Area Ratio | Microvessel Density (mm2) | Internal Diameter of Vessels (μm) | |
|---|---|---|---|---|
| No treatment | 4.14 ± 0.63% | 4.10 ± 1.34% | 362 ± 48 | 7.29 ± 1.64 |
| Oral 3 mg | 2.88 ± 0.36% | 1.92 ± 0.26% | 336 ± 68 | 3.53 ± 0.47 |
| 1 mg sheet | 1.96 ± 0.36% | 0.97 ± 0.43% | 243 ± 52 | 3.52 ± 0.60 |
| Tumor Volume (mm3) | ||
|---|---|---|
| Day 7 | Day 14 | |
| Control | 1233 ± 333 | 2003 ± 327 |
| Direct | 247 ± 61 | 377 ± 41 |
| Peripheral | 340 ± 67 | 431 ± 67 |
| Contralateral | 256 ± 62 | 397 ± 48 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yoshida, T.; Kaibori, M.; Fujisawa, N.; Ishizuka, M.; Sumiyama, F.; Hatta, M.; Kosaka, H.; Matsui, K.; Suzuki, K.; Akama, T.O.; et al. Efficacy of Nanofiber Sheets Incorporating Lenvatinib in a Hepatocellular Carcinoma Xenograft Model. Nanomaterials 2022, 12, 1364. https://doi.org/10.3390/nano12081364
Yoshida T, Kaibori M, Fujisawa N, Ishizuka M, Sumiyama F, Hatta M, Kosaka H, Matsui K, Suzuki K, Akama TO, et al. Efficacy of Nanofiber Sheets Incorporating Lenvatinib in a Hepatocellular Carcinoma Xenograft Model. Nanomaterials. 2022; 12(8):1364. https://doi.org/10.3390/nano12081364
Chicago/Turabian StyleYoshida, Terufumi, Masaki Kaibori, Nanami Fujisawa, Mariko Ishizuka, Fusao Sumiyama, Masahiko Hatta, Hisashi Kosaka, Kosuke Matsui, Kensuke Suzuki, Tomoya O. Akama, and et al. 2022. "Efficacy of Nanofiber Sheets Incorporating Lenvatinib in a Hepatocellular Carcinoma Xenograft Model" Nanomaterials 12, no. 8: 1364. https://doi.org/10.3390/nano12081364