
A Biodegradable Flexible Micro/Nano-Structured Porous Hemostatic Dental Sponge
 , , , and
, , , and
Abstract
:1. Introduction

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sponge Brand | Producer | Applications | Ref. |
|---|---|---|---|
| Gelfoam® | Pharmacia & Upjohn Co., Kalamazoo, MI, USA | Dental | [14] |
| Gelita-Spon® | Invotec International, Inc, Jacksonville, FL, USA | Dental, nasal, sinus surgery, or any other surgical procedure | [14] |
| SPONGOSTAN TM | Johnson & Johnson, Ferrosan, Søborg, Denmark | Dental | [27] |
| SURGIFOAM® | Ethicon, Somerville, NJ, USA | Dental, Oral Surgery | [27] |
| Gelatamp | Roeko-Coltène/Whaledent, Langenau, Germany | Dental, Oral Surgery | [28] |
2. Materials and Methods
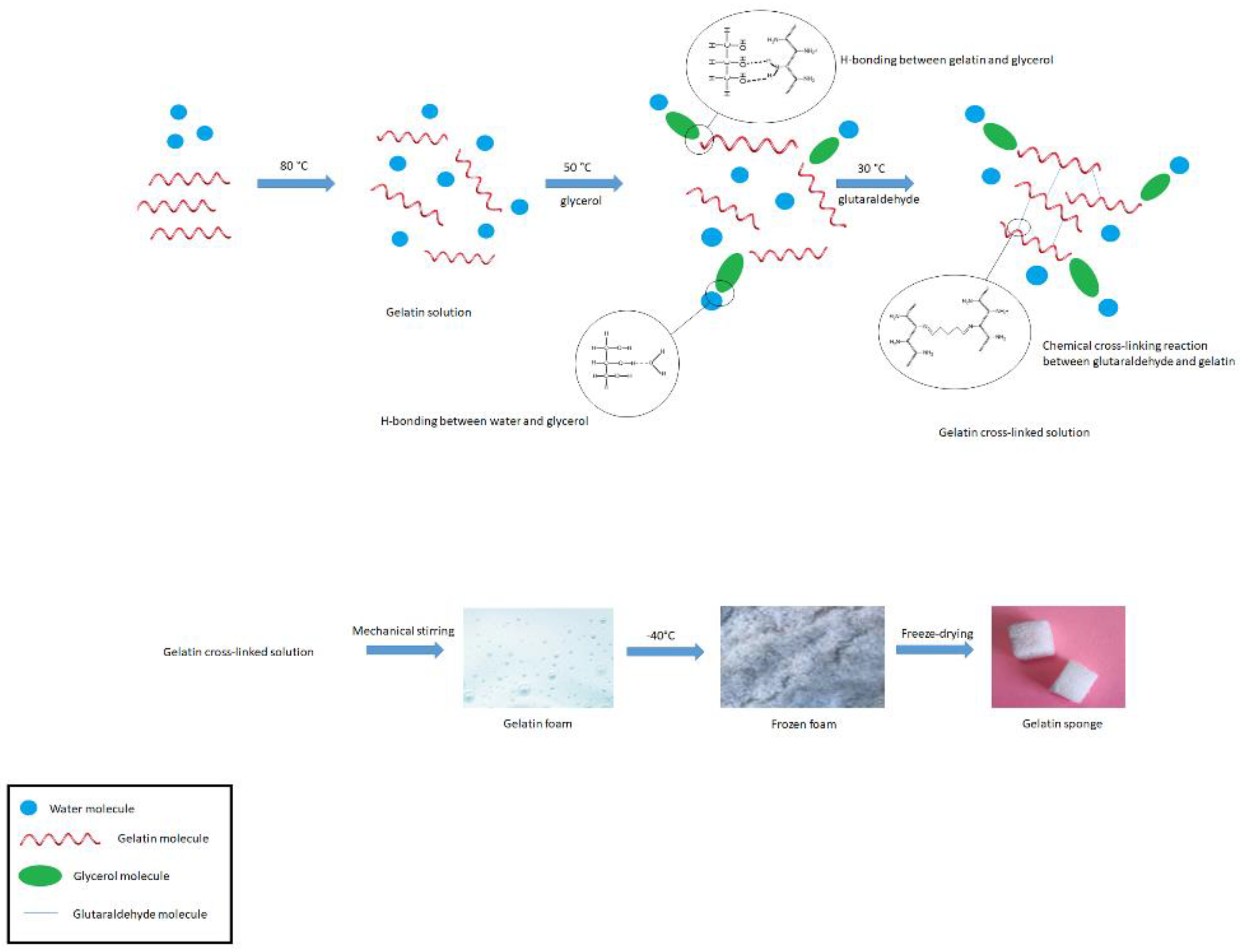
2.1. Preparation of Sponge
2.2. Physicochemical and Physicomechanical Characterization
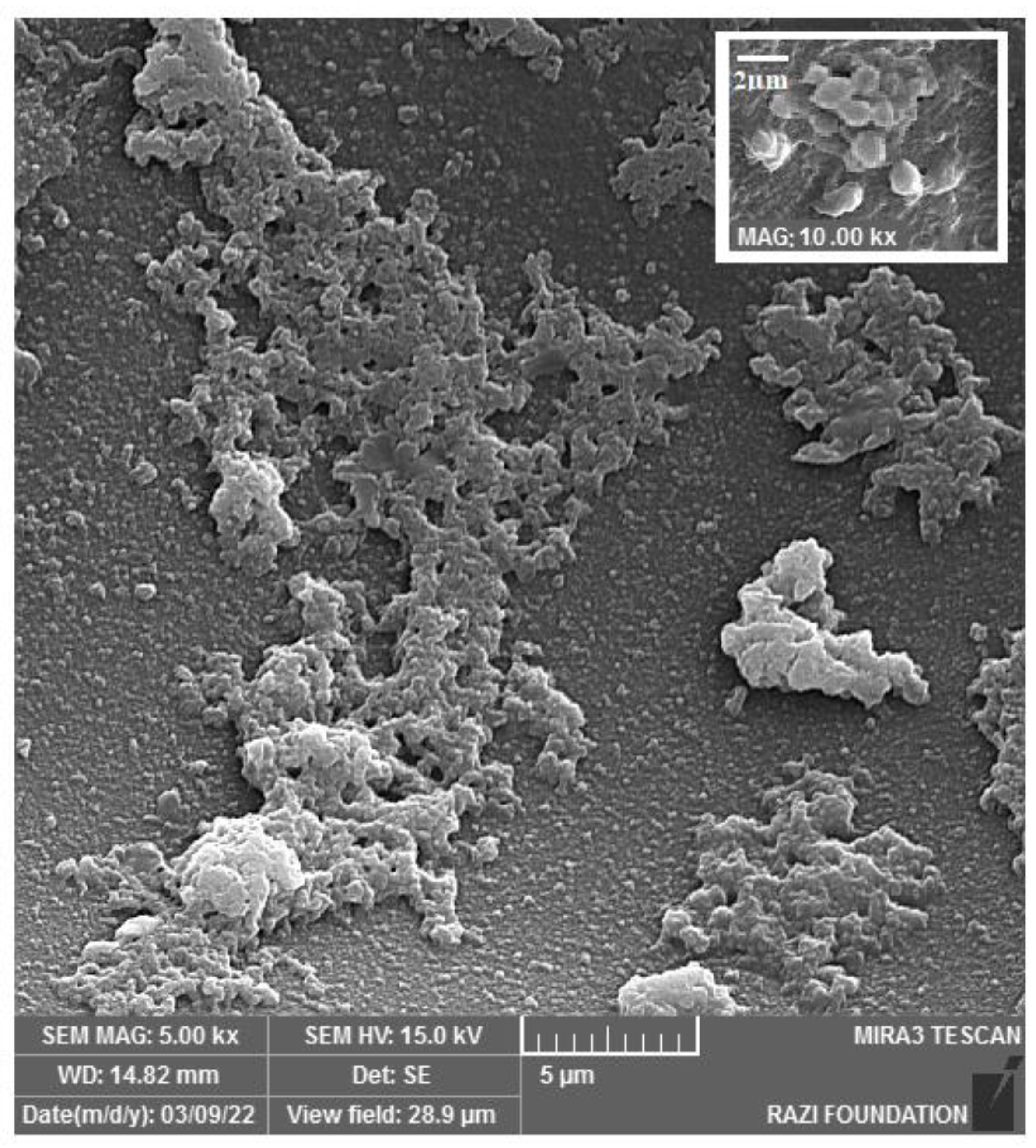
2.2.1. Sponge Structure and Morphology
2.2.2. Identification of the Functional Groups
2.2.3. Identification of Crystallinity State
2.2.4. Tensile Strength Determination
2.2.5. The Specific Surface Area, Total Pore Volume, and Porosity
2.2.6. Volume Expansion
2.2.7. Degradation Test
2.3. Biocompatibility Assay
2.3.1. Cellular Cytotoxicity
2.3.2. Hemolysis Test
2.4. Function Evaluation Tests
2.4.1. Blood Absorption Test and Swelling Percentage
2.4.2. Blood Standard Prothrombin and Partial Thromboplastin Time
2.4.3. Blood Clotting Time (BCT)
2.4.4. Blood Clotting Index (BCI)
2.4.5. Fibrin Formation Process
2.4.6. Platelet Adhesion Test
2.4.7. Clinical Assessment
3. Results and Discussion
3.1. Physicochemical and Physicomechanical Characterization
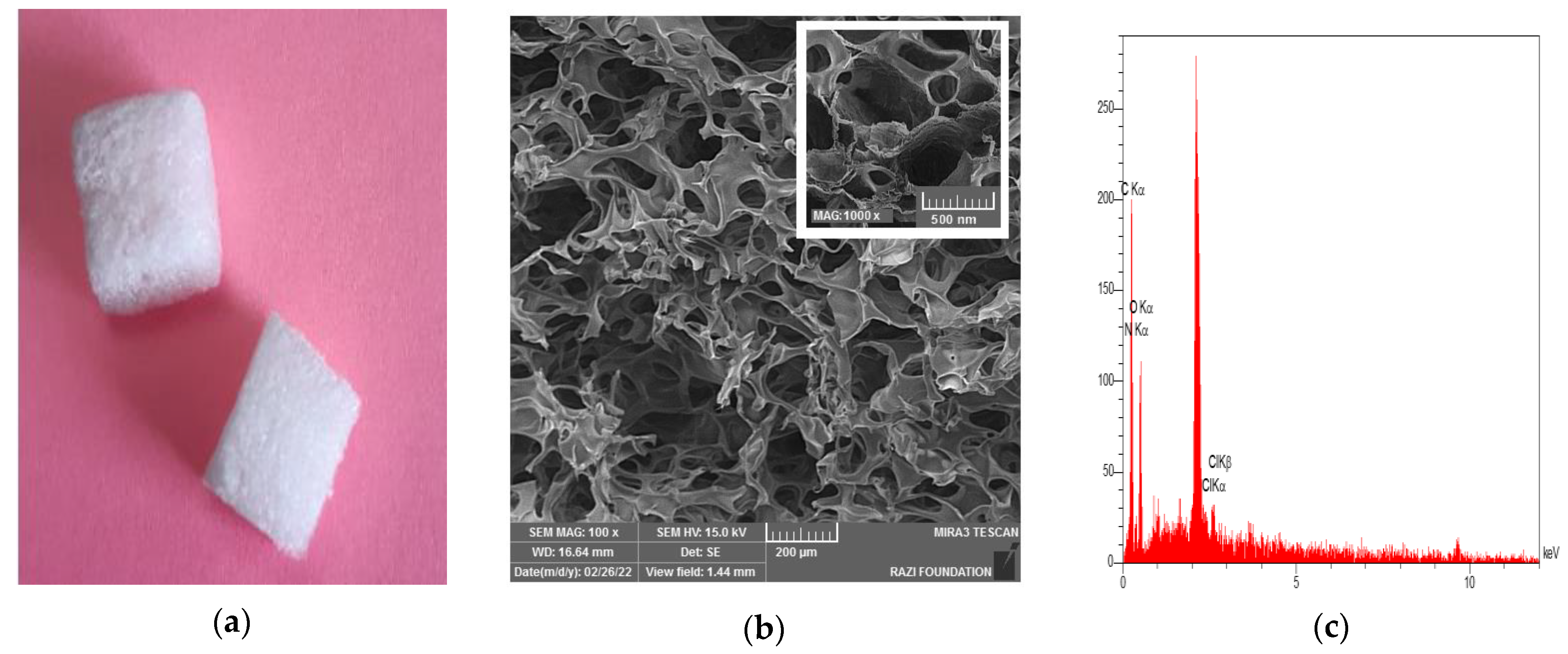
3.1.1. Sponge Structure and Morphology
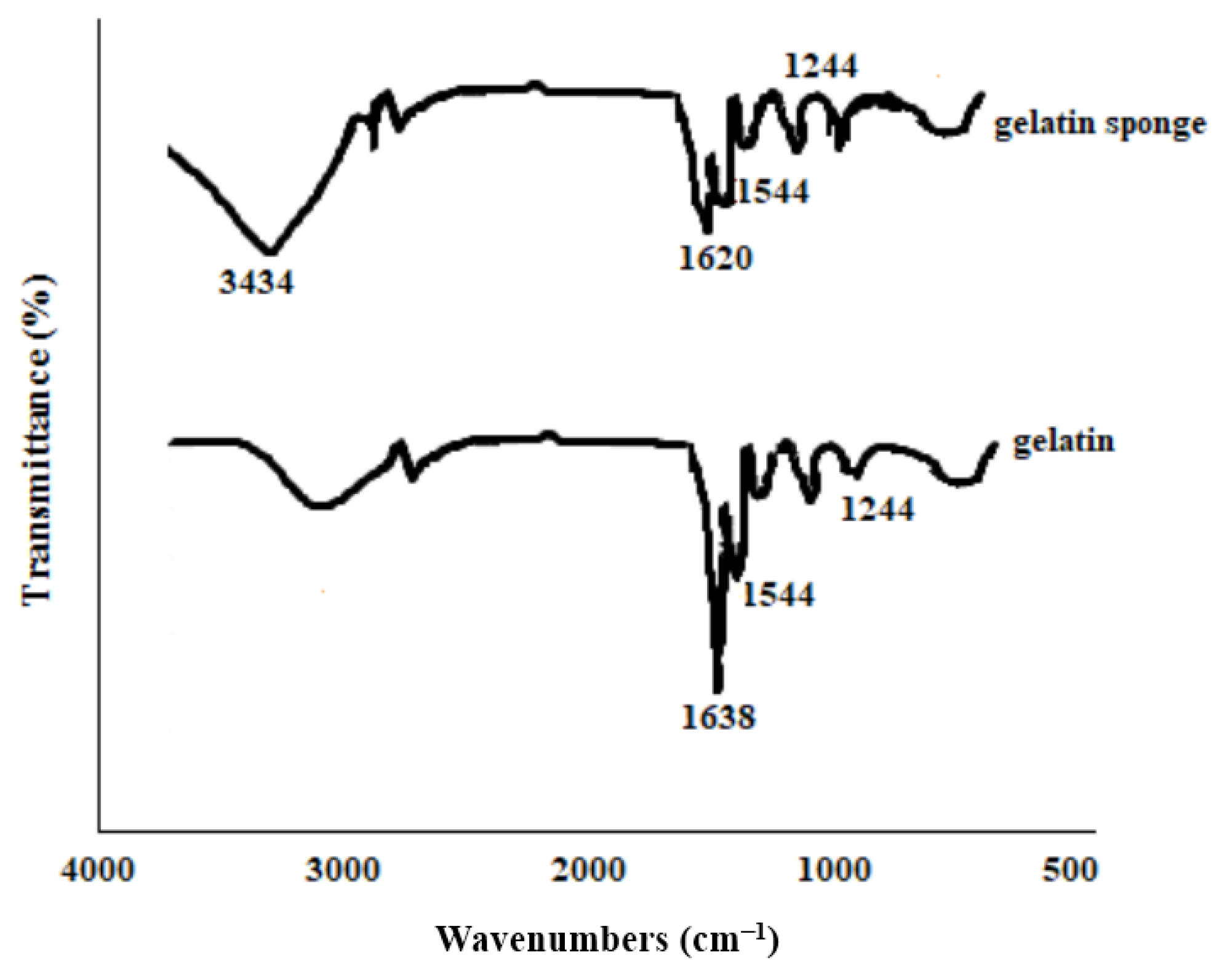
3.1.2. Identification of the Functional Groups
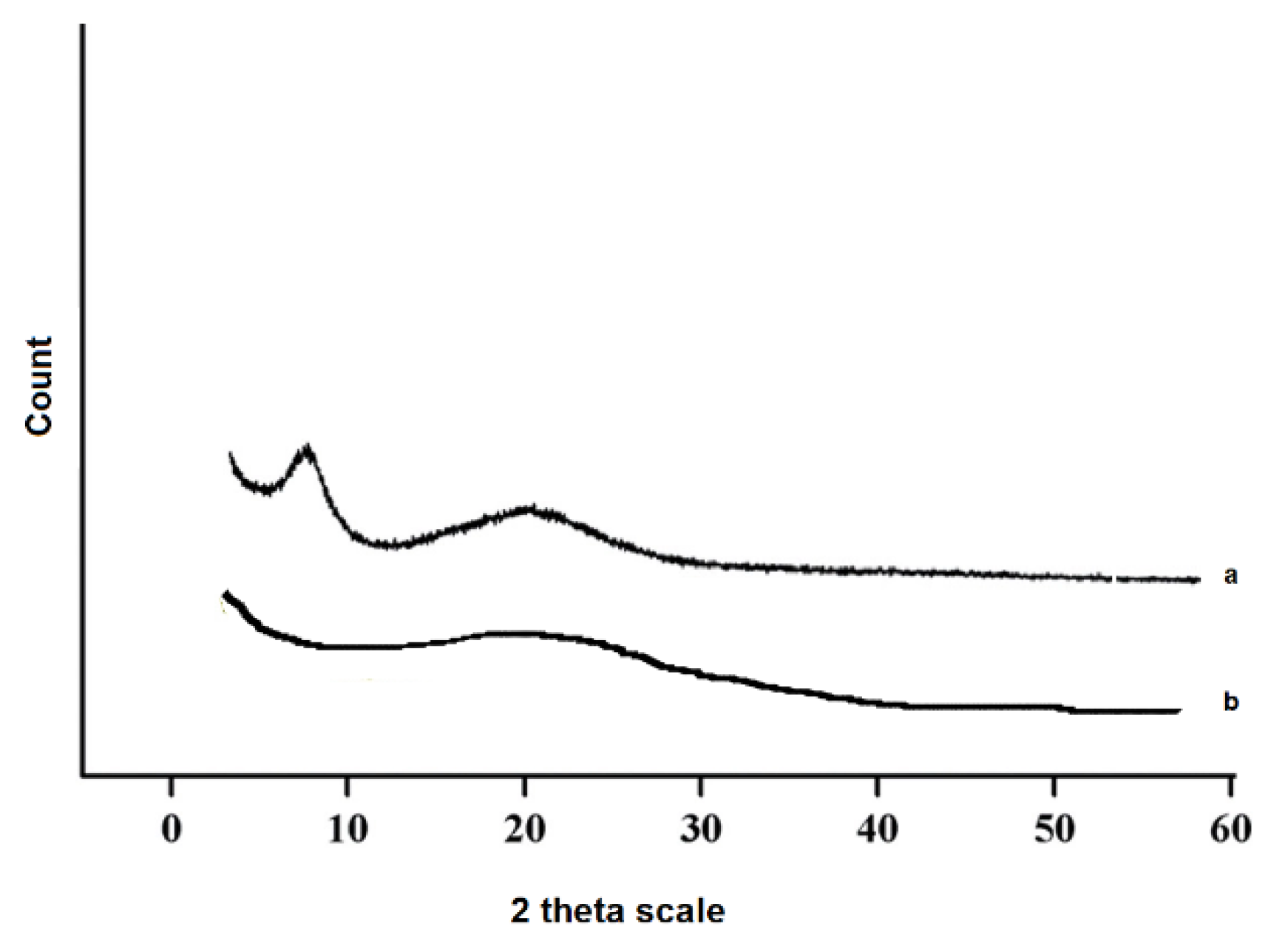
3.1.3. Identification of Crystallinity State
3.1.4. Tensile Strength Determination
3.1.5. The Specific Surface Area, Total Pore Volume, and the Porosity
3.1.6. Volume Expansion and Density Determination
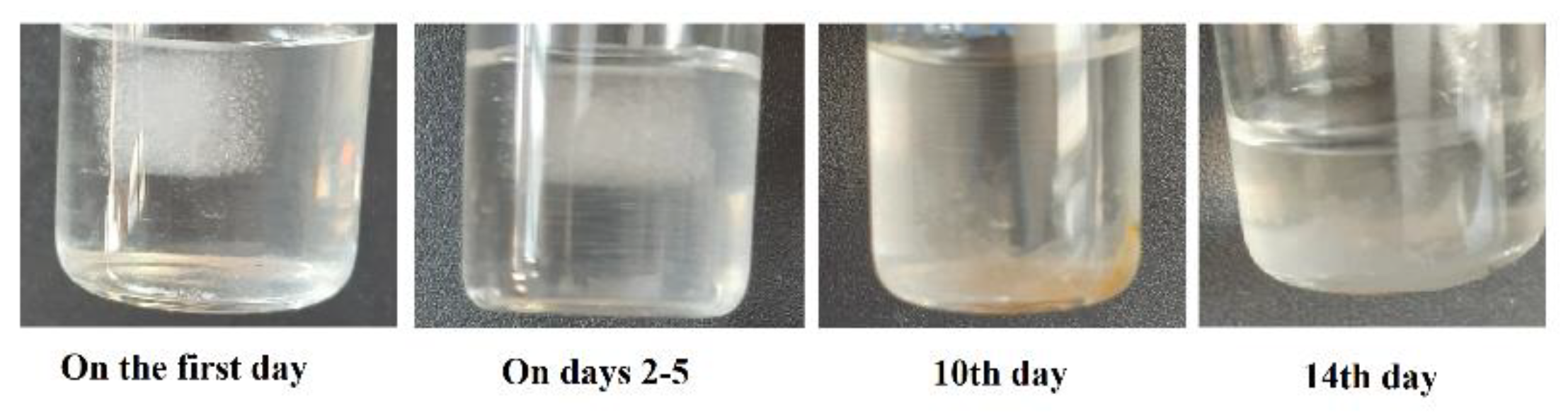
3.1.7. Degradation Test
3.2. Biocompatibility Assay
3.2.1. Cytotoxicity
3.2.2. Hemolysis Test
3.3. Function Evaluation Tests
3.3.1. Blood Absorption and Swelling Percentage
3.3.2. Blood Standard Prothrombin and Partial Thromboplastin Time
3.3.3. CT Coagulation Time
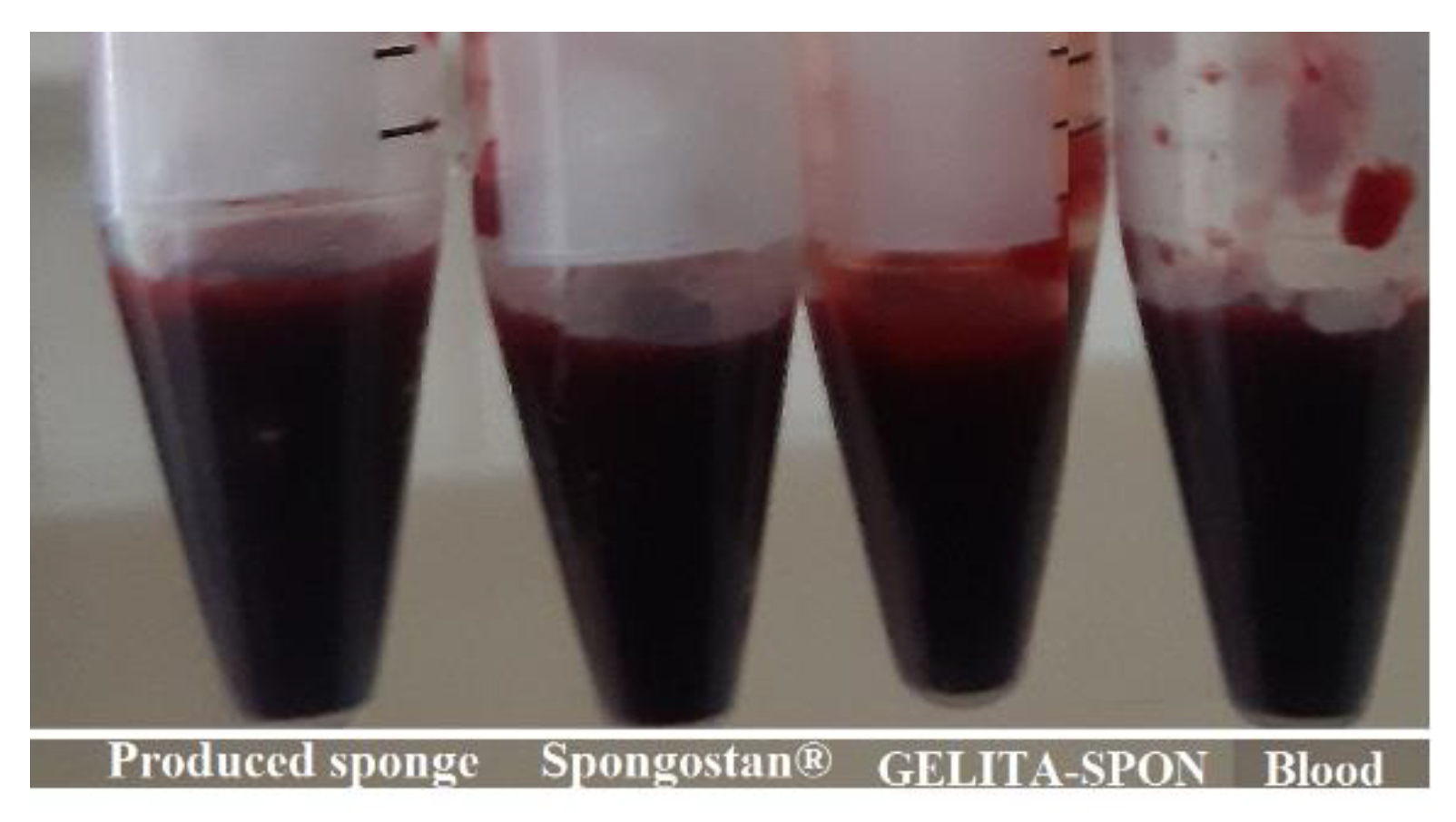
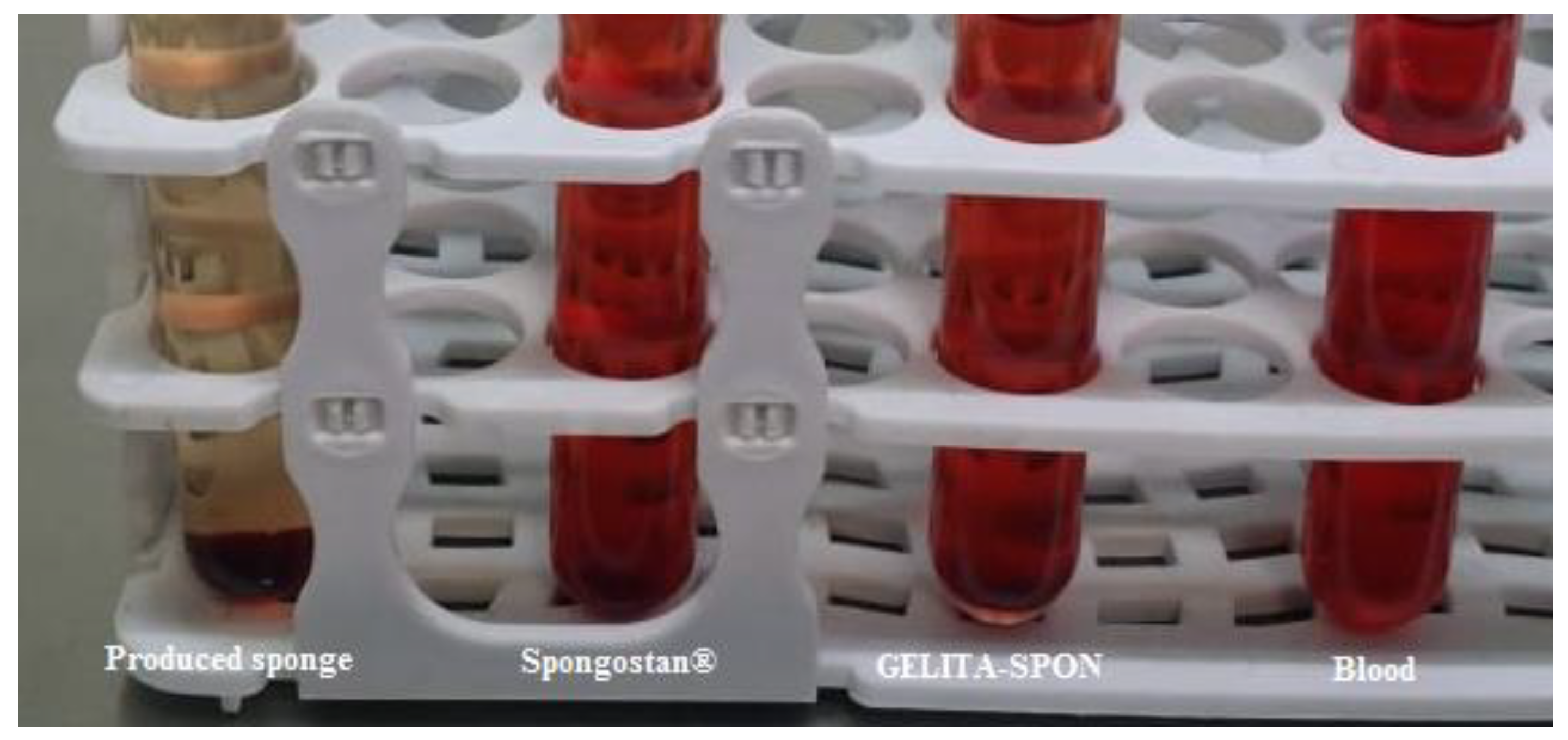
3.3.4. Blood Clotting Index (BCI)
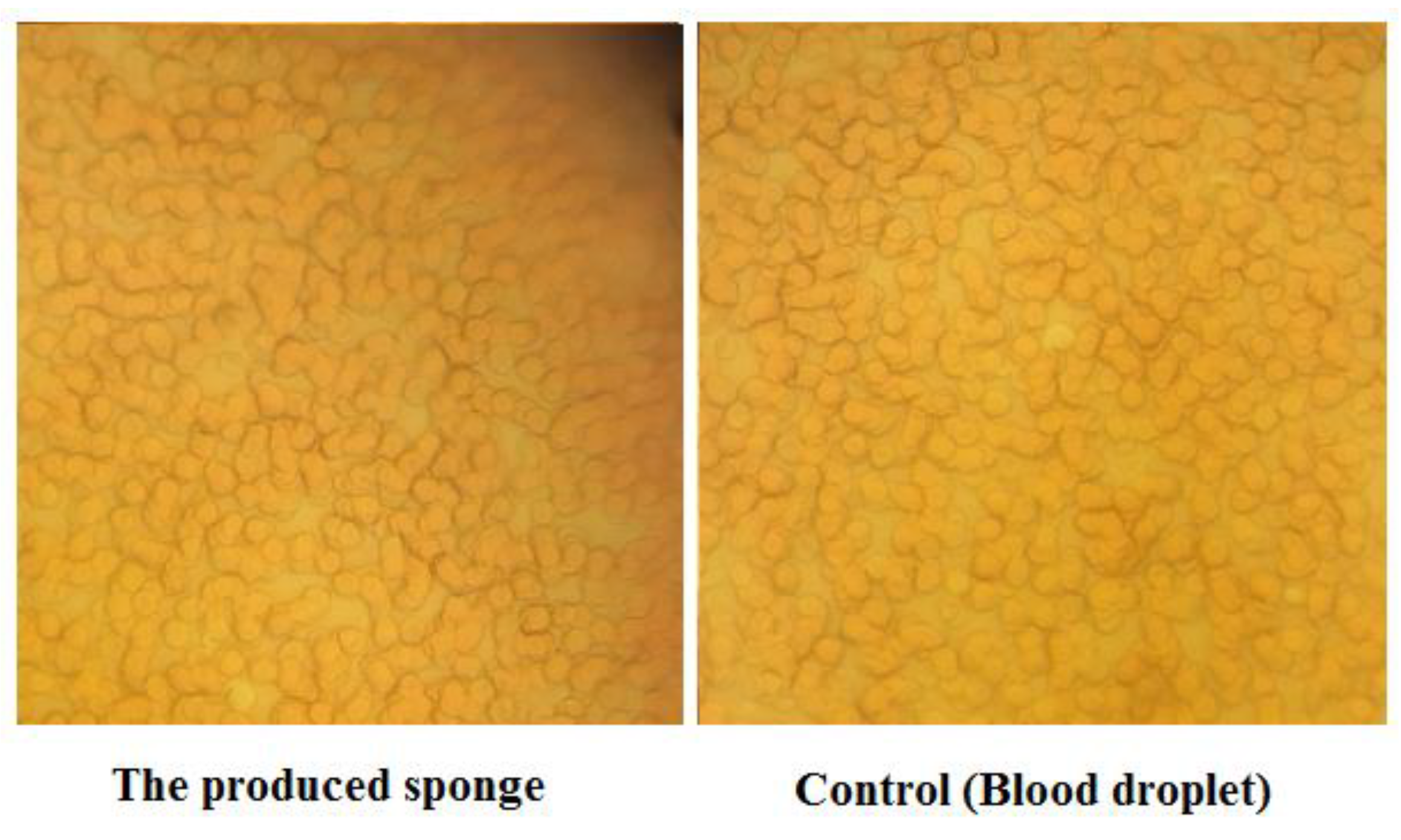
3.3.5. Platelet Adhesion Test
3.3.6. Fibrin Formation Process
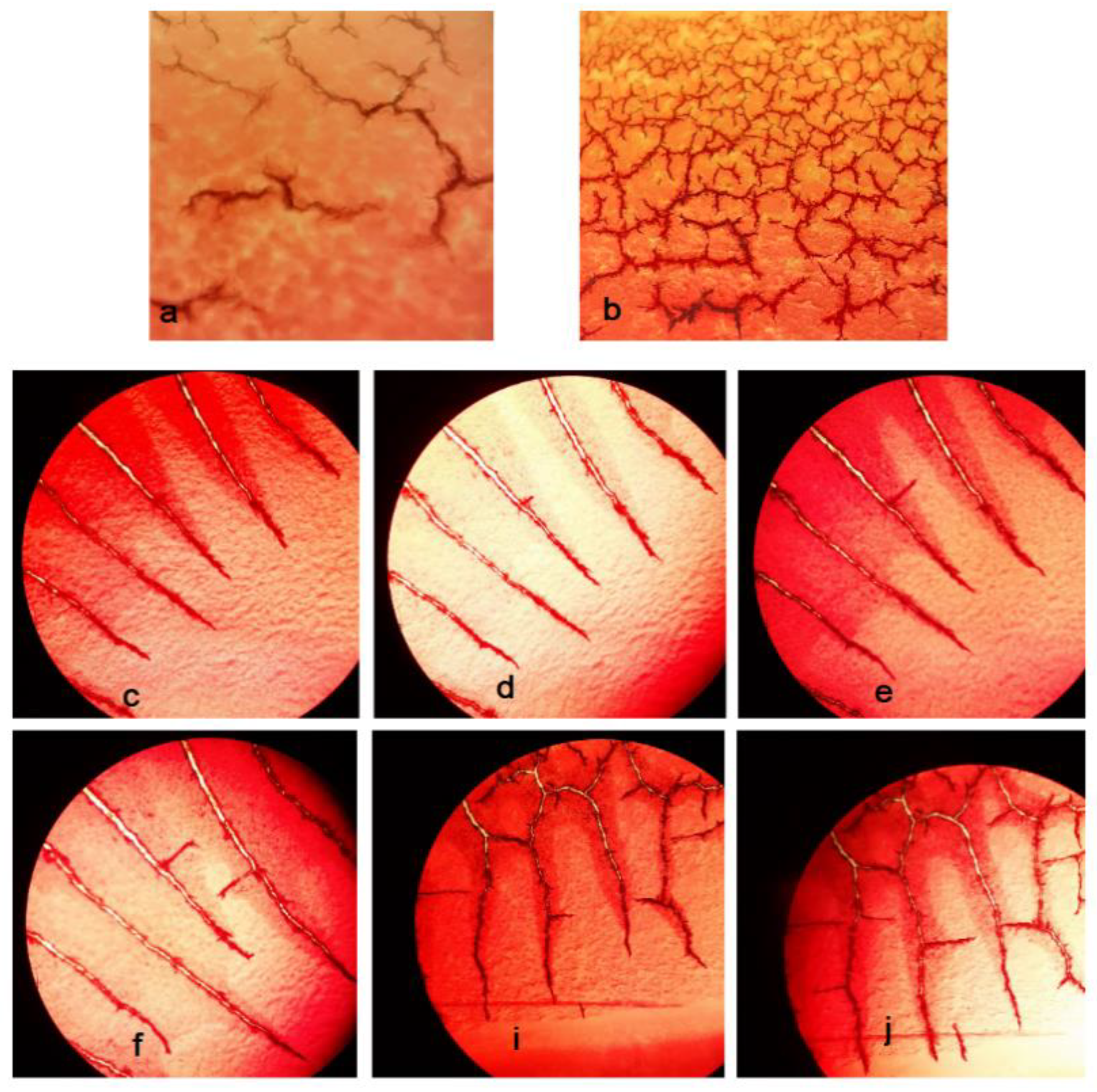
3.3.7. Clinical Assessment
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Guo, B.; Dong, R.; Liang, Y.; Li, M. Haemostatic materials for wound healing applications. Nat. Rev. Chem. 2021, 5, 773–791. [Google Scholar] [CrossRef]
- Wang, L.; Li, W.; Qu, Y.; Wang, K.; Lv, K.; He, X.; Qin, S. Preparation of Super Absorbent and Highly Active Fish Collagen Sponge and its Hemostatic Effect in vivo and in vitro. Front. Bioeng. Biotechnol. 2022, 10, 862532. [Google Scholar] [CrossRef] [PubMed]
- Tomizawa, Y. Clinical benefits and risk analysis of topical hemostats: A review. J. Artif. Organs 2005, 8, 137–142. [Google Scholar] [CrossRef] [PubMed]
- Aziz, O.; Athanasiou, T.; Darzi, A. Haemostasis using a ready-to-use collagen sponge coated with activated thrombin and fibrinogen. Surg. Technol. Online 2005, 14, 35–40. [Google Scholar]
- Sun, H.; Lv, L.; Bai, Y.; Yang, H.; Zhou, H.; Li, C.; Yang, L. Nanotechnology-enabled materials for hemostatic and anti-infection treatments in orthopedic surgery. Int. J. Nanomed. 2018, 13, 8325. [Google Scholar] [CrossRef]
- Huang, Y.; Cheng, W.; JMH, Y.; Gao, S.; Li, D. A Preparation Method of Regenerated Cellulose Hemostatic Material with Surface Nanostructure. CN Patent 102,912,622A, 2013. [Google Scholar]
- Xi, G.; Liu, W.; Chen, M.; Li, Q.; Hao, X.; Wang, M.; Yang, X.; Feng, Y.; He, H.; Shi, C.; et al. Polysaccharide-based lotus seedpod surface-like porous microsphere with precise and controllable micromorphology for ultrarapid hemostasis. ACS Appl. Mater. Interfaces 2019, 11, 46558–46571. [Google Scholar] [CrossRef] [PubMed]
- Xue, J.; Wu, T.; Dai, Y.; Xia, Y. Electrospinning and electrospun nanofibers: Methods, materials, and applications. Chem. Rev. 2019, 119, 5298–5415. [Google Scholar] [CrossRef] [PubMed]
- Zheng, W.; Chen, C.; Zhang, X.; Wen, X.; Xiao, Y.; Li, L.; Xu, Q.; Fu, F.; Diao, H.; Liu, X. Layer-by-layer coating of carboxymethyl chitosan-gelatin-alginate on cotton gauze for hemostasis and wound healing. Surf. Coat. Technol. 2021, 406, 126644. [Google Scholar] [CrossRef]
- Al-Mofty, S.E.-D.; Karaly, A.H.; Sarhan, W.A.; Azzazy, H.M. Multifunctional Hemostatic PVA/Chitosan Sponges Loaded with Hydroxyapatite and Ciprofloxacin. ACS Omega 2022, 7, 13210–13220. [Google Scholar] [CrossRef]
- Dowd, F.J.; Yagiela, J.A.; Johnson, B.; Mariotti, A.; Neidle, E.A. Pharmacology and Therapeutics for Dentistry-E-Book; Elsevier Health Sciences: Amsterdam, The Netherlands, 2010. [Google Scholar]
- Ibne Mahbub, M.S.; Sultana, T.; Gwon, J.-G.; Lee, B.-T. Fabrication of thrombin loaded TEMPO-oxidized cellulose nanofiber-gelatin sponges and their hemostatic behavior in rat liver hemorrhage model. J. Biomater. Sci. Polym. Ed. 2022, 33, 499–516. [Google Scholar] [CrossRef] [PubMed]
- di Lena, F. Hemostatic polymers: The concept, state of the art and perspectives. J. Mater. Chem. B 2014, 2, 3567–3577. [Google Scholar] [CrossRef] [PubMed]
- Mann, A.; Tighe, B.J. Wound healing studies and interfacial phenomena: Use and relevance of the corneal model. In Advanced Wound Repair Therapies; Elsevier: Amsterdam, The Netherlands, 2011; pp. 284–320. [Google Scholar]
- Nagraj, S.K.; Prashanti, E.; Aggarwal, H.; Lingappa, A.; Muthu, M.S.; Krishanappa, S.K.K.; Hassan, H. Interventions for treating post-extraction bleeding. Cochrane Database Syst. Rev. 2018, CD011930. [Google Scholar]
- Howe, N.; Cherpelis, B. Obtaining rapid and effective hemostasis: Part I. Update and review of topical hemostatic agents. J. Am. Acad. Dermatol. 2013, 69, 659.e1–e17. [Google Scholar] [CrossRef]
- McCormick, N.J.; Moore, U.J.; Meechan, J.G. Haemostasis part 1: The management of post-extraction haemorrhage. Dent. Updat. 2014, 41, 290–296. [Google Scholar] [CrossRef] [PubMed]
- Traver, M.A.; Assimos, D.G. New generation tissue sealants and hemostatic agents: Innovative urologic applications. Rev. Urol. 2006, 8, 104. [Google Scholar] [PubMed]
- Guralnick, W.C.; Berg, L. Gelfoam in oral surgery: A report of two hundred fifty cases. Oral Surg. Oral Med. Oral Pathol. 1948, 1, 632–639. [Google Scholar] [CrossRef]
- Amin, K.; Khor, W.S.; Rosich-Medina, A.; Beale, V. Alveolar bone grafting: Donor site review of 100 consecutive cases in cleft lip and palate. Cleft Palate-Craniofacial J. 2017, 54, 137–141. [Google Scholar] [CrossRef]
- Zhang, W.; Yelick, P.C. Vital pulp therapy—Current progress of dental pulp regeneration and revascularization. Int. J. Dent. 2010, 2010, 856087. [Google Scholar] [CrossRef]
- Volpe, S.; Di Girolamo, M.; Pagliani, P.; Zicari, S.; Sennerby, L. Osteotome-Induced Blood Clot and Subsequent Bone Formation with the Use of Collagen Sponge for Integration of Single Dental Implants into the Atrophied Posterior Maxilla: A Retrospective Follow-Up of 36 Implants after 5 to 13 years. Int. J. Dent. 2022, 2022, 6594279. [Google Scholar] [CrossRef]
- Al-obaidi, M.; Alhamdani, F.; Alalawi, H.; Alhamdani, F. Evaluation of Bone around Dental Implants with Sinus Lift Using Gelfoam Augmentation. South Asian Res. J. Oral Dent. Sci. 2021, 3, 108–118. [Google Scholar]
- Kim, J.-C.; Choi, S.-S.; Wang, S.-J.; Kim, S.-G. Minor complications after mandibular third molar surgery: Type, incidence, and possible prevention. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2006, 102, e4–e11. [Google Scholar] [CrossRef] [PubMed]
- Noroozi, A.-R.; Philbert, R.F. Modern concepts in understanding and management of the “dry socket” syndrome: Comprehensive review of the literature. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. Endodontology 2009, 107, 30–35. [Google Scholar] [CrossRef] [PubMed]
- Pal, U.S.; Singh, B.P.; Verma, V. Comparative evaluation of zinc oxide eugenol versus gelatin sponge soaked in plasma rich in growth factor in the treatment of dry socket: An initial study. Contemp. Clin. Dent. 2013, 4, 37–41. [Google Scholar] [CrossRef] [PubMed]
- Kobatake, K.; Mita, K.; Kato, M. Effect on hemostasis of an absorbable hemostatic gelatin sponge after transrectal prostate needle biopsy. Int. Braz J Urol 2015, 41, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Piry, P.; Esmaeeli Sari, A.; Mahdipour, A.; Asayesh, H. The effect of using Gelatamp on pain and gingival bleeding after tooth extraction: A randomize clinical trial. Qom Univ. Med. Sci. J. 2018, 12, 10–18. [Google Scholar] [CrossRef]
- Valenta, C.; Auner, B.G. The use of polymers for dermal and transdermal delivery. Eur. J. Pharm. Biopharm. 2004, 58, 279–289. [Google Scholar] [CrossRef]
- Lu, B.; Wang, T.; Li, Z.; Dai, F.; Lv, L.; Tang, F.; Yu, K.; Liu, J.; Lan, G. Healing of skin wounds with a chitosan–gelatin sponge loaded with tannins and platelet-rich plasma. Int. J. Biol. Macromol. 2016, 82, 884–891. [Google Scholar] [CrossRef]
- Ghosh, T.; Deveswaran, R.; Murahari, M.; Bharath, S. Development and Characterization of Copper Cross-Linked Freeze-Dried Bioscaffolds for Potential Wound Healing Activity. J. Pharm. Innov. 2022, 1–11. [Google Scholar] [CrossRef]
- Musa, A.; Ahmad, M.B.; Hussein, M.Z.; Saiman, M.I.; Sani, H.A. Effect of gelatin-stabilized copper nanoparticles on catalytic reduction of methylene blue. Nanoscale Res. Lett. 2016, 11, 438. [Google Scholar] [CrossRef]
- Cai, B.; Chen, L.; Luo, J. Synthesis and characterization of bis-(O-vanillin) benzoic imine Schiff base. J. Nanjing For. Univ. 2011, 35, 91–94. [Google Scholar]
- Liu, Y.; Huang, X.; Guo, P.; Liao, X.; Shi, B. Skin collagen fiber-based radar absorbing materials. Chin. Sci. Bull. 2011, 56, 202–208. [Google Scholar] [CrossRef]
- Wahab, R.A.; Elias, N.; Abdullah, F.; Ghoshal, S.K. On the taught new tricks of enzymes immobilization: An all-inclusive overview. React. Funct. Polym. 2020, 152, 104613. [Google Scholar] [CrossRef]
- Tengroth, C.; Gasslander, U.; Andersson, F.O.; Jacobsson, S.P.J. Cross-linking of gelatin capsules with formaldehyde and other aldehydes: An FTIR spectroscopy study. Pharm. Dev. Technol. 2005, 10, 405–412. [Google Scholar] [CrossRef] [PubMed]
- Ramasubramaniam, S.; Govindarajan, C.; Nasreen, K.; Sudha, P. Removal of cadmium (II) ions from aqueous solution using chitosan/starch polymer blend. Interfaces 2014, 21, 95–109. [Google Scholar] [CrossRef]
- Cheng, S.; Wang, W.; Li, Y.; Gao, G.; Zhang, K.; Zhou, J.; Wu, Z. Cross-linking and film-forming properties of transglutaminase-modified collagen fibers tailored by denaturation temperature. Food Chem. 2019, 271, 527–535. [Google Scholar] [CrossRef]
- Liu, F.; Majeed, H.; Antoniou, J.; Li, Y.; Ma, Y.; Yokoyama, W.; Ma, J.; Zhong, F. Tailoring physical properties of transglutaminase-modified gelatin films by varying drying temperature. Food Hydrocoll. 2016, 58, 20–28. [Google Scholar] [CrossRef]
- Qu, W.; Häkkinen, R.; Allen, J.; D’Agostino, C.; Abbott, A.P. Globular and fibrous proteins modified with deep eutectic solvents: Materials for drug delivery. Molecules 2019, 24, 3583. [Google Scholar] [CrossRef]
- Long, H.; Ma, K.; Xiao, Z.; Ren, X.; Yang, G. Preparation and characteristics of gelatin sponges crosslinked by microbial transglutaminase. PeerJ 2017, 5, e3665. [Google Scholar] [CrossRef] [PubMed]
- Li, X.; Zhang, H.; He, L.; Chen, Z.; Tan, Z.; You, R.; Wang, D. Flexible nanofibers-reinforced silk fibroin films plasticized by glycerol. Compos. Part B Eng. 2018, 152, 305–310. [Google Scholar] [CrossRef]
- Rafienia, M.; Imani, R.; Hojjati Emami, S.; Rabbani, M.; Kabiri, M. Synthesis and characterization of biodegradable hemostat gelatin sponge for surgery application. Iran. J. Pharm. Sci. 2008, 4, 193–200. [Google Scholar]
- Tropp, J.; Rivnay, J. Design of biodegradable and biocompatible conjugated polymers for bioelectronics. J. Mater. Chem. C 2021, 9, 13543–13556. [Google Scholar] [CrossRef]
- Singh, B.; Pal, L. Sterculia crosslinked PVA and PVA-poly (AAm) hydrogel wound dressings for slow drug delivery: Mechanical, mucoadhesive, biocompatible and permeability properties. J. Mech. Behav. Biomed. Mater. 2012, 9, 9–21. [Google Scholar] [CrossRef]
- Seyfert, U.T.; Biehl, V.; Schenk, J. In vitro hemocompatibility testing of biomaterials according to the ISO 10993-4. Biomol. Eng. 2002, 19, 91–96. [Google Scholar] [CrossRef]
- Xie, X.; Li, D.; Chen, Y.; Shen, Y.; Yu, F.; Wang, W.; Yuan, Z.; Morsi, Y.; Wu, J.; Mo, X. Conjugate electrospun 3D gelatin nanofiber sponge for rapid hemostasis. Adv. Healthc. Mater. 2021, 10, 2100918. [Google Scholar] [CrossRef] [PubMed]
- Fang, Y.; Xu, Y.; Wang, Z.; Zhou, W.; Yan, L.; Fan, X.; Liu, H. 3D porous chitin sponge with high absorbency, rapid shape recovery, and excellent antibacterial activities for noncompressible wound. Chem. Eng. J. 2020, 388, 124169. [Google Scholar] [CrossRef]
- Fan, X.; Li, Y.; Li, N.; Wan, G.; Ali, M.A.; Tang, K. Rapid hemostatic chitosan/cellulose composite sponge by alkali/urea method for massive haemorrhage. Int. J. Biol. Macromol. 2020, 164, 2769–2778. [Google Scholar] [CrossRef] [PubMed]
- González, A.; Avivar, J.; Maya, F.; Palomino Cabello, C.; Turnes Palomino, G.; Cerdà, V. In-syringe dispersive μ-SPE of estrogens using magnetic carbon microparticles obtained from zeolitic imidazolate frameworks. Anal. Bioanal. Chem. 2017, 409, 225–234. [Google Scholar] [CrossRef]
- Liu, W.; Yang, C.; Gao, R.; Zhang, C.; Ou-Yang, W.; Feng, Z.; Zhang, C.; Pan, X.; Huang, P.; Kong, D.; et al. Polymer Composite Sponges with Inherent Antibacterial, Hemostatic, Inflammation-Modulating and Proregenerative Performances for Methicillin-Resistant Staphylococcus aureus-Infected Wound Healing. Adv. Healthc. Mater. 2021, 10, 2101247. [Google Scholar] [CrossRef] [PubMed]
- He, Y.; Zhao, W.; Dong, Z.; Ji, Y.; Li, M.; Hao, Y.; Zhang, D.; Yuan, C.; Deng, J.; Zhao, P.; et al. A biodegradable antibacterial alginate/carboxymethyl chitosan/Kangfuxin sponges for promoting blood coagulation and full-thickness wound healing. Int. J. Biol. Macromol. 2021, 167, 182–192. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Guan, J.; Wu, J.; Ding, S.; Yang, J.; Zhang, J.; Dong, A.; Deng, L. N-alkylated chitosan/graphene oxide porous sponge for rapid and effective hemostasis in emergency situations. Carbohydr. Polym. 2019, 219, 405–413. [Google Scholar] [CrossRef]
- Mahmoodzadeh, A.; Moghaddas, J.; Jarolmasjed, S.; Kalan, A.E.; Edalati, M.; Salehi, R. Biodegradable cellulose-based superabsorbent as potent hemostatic agent. Chem. Eng. J. 2021, 418, 129252. [Google Scholar] [CrossRef]
- Wan, Y.; Han, J.; Cheng, F.; Wang, X.; Wang, H.; Song, Q.; He, W. Green preparation of hierarchically structured hemostatic epoxy-amine sponge. Chem. Eng. J. 2020, 397, 125445. [Google Scholar] [CrossRef]
- Wang, L.; Zhong, Y.; Qian, C.; Yang, D.; Nie, J.; Ma, G. A natural polymer-based porous sponge with capillary-mimicking microchannels for rapid hemostasis. Acta Biomater. 2020, 114, 193–205. [Google Scholar] [CrossRef]
- Periayah, M.H.; Halim, A.S.; Saad, A.Z.M. Mechanism action of platelets and crucial blood coagulation pathways in hemostasis. Int. J. Hematol. Oncol. Stem Cell Res. 2017, 11, 319. [Google Scholar]
- Liu, C.; Liu, X.; Liu, C.; Wang, N.; Chen, H.; Yao, W.; Sun, G.; Song, Q.; Qiao, W. A highly efficient, in situ wet-adhesive dextran derivative sponge for rapid hemostasis. Biomaterials 2019, 205, 23–37. [Google Scholar] [CrossRef] [PubMed]
- Davalos, D.; Akassoglou, K. Fibrinogen as a key regulator of inflammation in disease. Semin. Immunopathol. 2011, 34, 43–62. [Google Scholar] [CrossRef] [PubMed]
- Guralnick, W.C. Absorbable gelatin sponge and thrombin in oral surgery. Am. J. Orthod. Oral Surg. 1946, 32, 792–794. [Google Scholar] [CrossRef]











| Specific Surface (m2/g) | Pore Radius (nm) | Total Pore Volume (cm3) | Porosity (%) |
|---|---|---|---|
| 5.3 | 120 | 0.63 | 63 |
| Group | The Number of Used Sterile Gauze (Mean Number) | The Total Weight of Absorbed Blood by Sterile Gauze (g/g) |
|---|---|---|
| Test | 2.4 ± 0.48 | 2.67 ± 1.17 |
| Control | 2.6 ± 0.48 | 4.27 ± 0.49 |
| t-test p-value | 0.39 | 0.0015 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sharifi, S.; Maleki Dizaj, S.; Ahmadian, E.; Karimpour, A.; Maleki, A.; Memar, M.Y.; Ghavimi, M.A.; Dalir Abdolahinia, E.; Goh, K.W. A Biodegradable Flexible Micro/Nano-Structured Porous Hemostatic Dental Sponge. Nanomaterials 2022, 12, 3436. https://doi.org/10.3390/nano12193436
Sharifi S, Maleki Dizaj S, Ahmadian E, Karimpour A, Maleki A, Memar MY, Ghavimi MA, Dalir Abdolahinia E, Goh KW. A Biodegradable Flexible Micro/Nano-Structured Porous Hemostatic Dental Sponge. Nanomaterials. 2022; 12(19):3436. https://doi.org/10.3390/nano12193436
Chicago/Turabian StyleSharifi, Simin, Solmaz Maleki Dizaj, Elham Ahmadian, Alireza Karimpour, Abdollah Maleki, Mohammad Yousef Memar, Mohammad Ali Ghavimi, Elaheh Dalir Abdolahinia, and Khang Wen Goh. 2022. "A Biodegradable Flexible Micro/Nano-Structured Porous Hemostatic Dental Sponge" Nanomaterials 12, no. 19: 3436. https://doi.org/10.3390/nano12193436