
Development of Lateral Flow Immunochromatographic Test for Rapid Detection of SARS-CoV-2 Virus Antigens in Clinical Specimens

 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Nucleocapsid Protein (NP) and Spike Protein (S) of SARS- CoV-2
2.2. Preparation of Monospecific Antibodies against NP in Rabbits
2.3. Preparation of Monospecific Antibodies against S Protein in Goats
2.4. Purification of Immunoglobulin of Rabbit and Goat Antibodies Using Caprylic Acid
2.5. Preparation of Nanogold Particles of 40 nm Diameter Size
2.6. Conjugation of Nanogold Particles with Purified Rabbit IgG Specific to SARS-CoV-2 Nucleoprotein
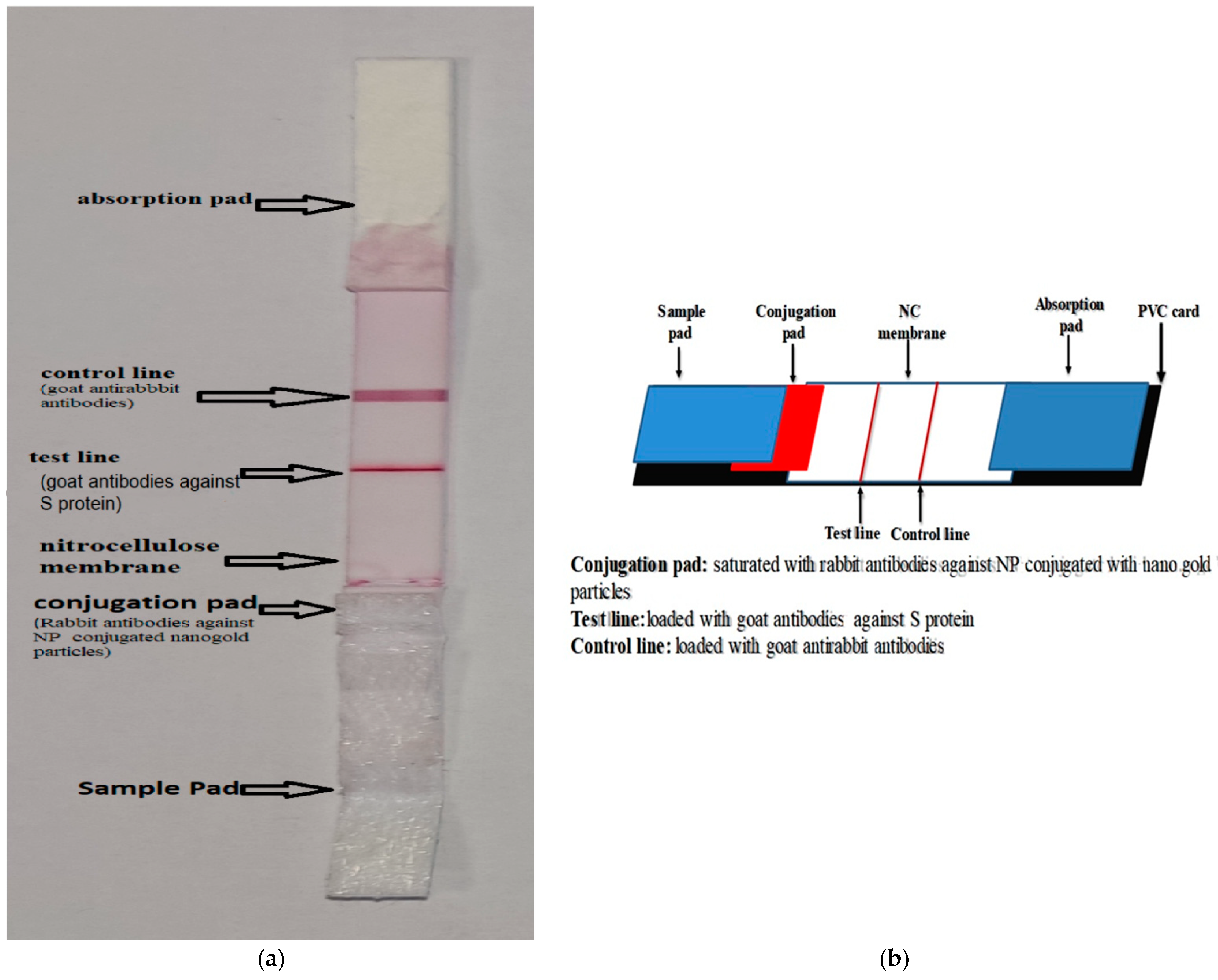
2.7. Dispensing of the Prepared SARS-CoV-2 NP-Specific Rabbit IgG Conjugated Nanogold Particles and Non-Conjugated SARS-CoV-2 Spike Protein Specific Goat IgG in the Nitrocellulose Membrane and the Conjugation Pad
2.8. Specificity Testing Using Other Viral Strains
2.9. Cross-Reactivity and Interfering Substances
2.10. Sensitivity Testing of Developed LFI-COVID-19 Antigen
2.11. Determination of Sensitivity, Specificity and Accuracy of the Prepared LFI COVID-19 Antigen as Compared with RT-qPCR Commercial Kit
2.12. Ethical Approval
3. Results
3.1. Gold Nanoparticle Measuring
3.2. Sensitivity Testing
3.3. Specificity Testing
3.4. Cross-Reactivity and Interfering Substances
3.5. The Relative Sensitivity, Specificity and Accuracy of LFI COVID-19 Antigen Test Compared with RT-qPCR Commercial Kit
4. Discussion
5. Conclusions
6. Limitations
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Diao, K.; Han, P.; Pang, T.; Li, Y.; Yang, Z. HRCT imaging features in representative imported cases of 2019 novel coronavirus pneumonia. Precis. Clin. Med. 2020, 3, 9–13. [Google Scholar] [CrossRef] [Green Version]
- Wu, F.; Zhao, S.; Yu, B.; Chen, Y.-M.; Wang, W.; Song, Z.-G.; Hu, Y.; Tao, Z.-W.; Tian, J.-H.; Pei, Y.-Y. A new coronavirus associated with human respiratory disease in China. Nature 2020, 579, 265–269. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lv, L.; Li, G.; Chen, J.; Liang, X.; Li, Y. Comparative genomic analysis revealed specific mutation pattern between human coronavirus SARS-CoV-2 and Bat-SARS-CoV RaTG13. bioRxiv 2020. [Google Scholar] [CrossRef] [Green Version]
- Abousenna, M.S. Alignment of SARS-CoV-2 in comparison with other coronaviruses. J. Life Sci. Biomed 2020, 10, 17–20. [Google Scholar] [CrossRef]
- Al-Awaida, W.J.; Jawabrah, A.B.; Swedan, S.; Nimer, R.; Alzoughool, F.; Al-Ameer, H.J.; Al Tamam, S.E.; Alashqar, R.; Al bawareed, O.; Gushchina, Y.; et al. Correlates of SARS-CoV-2 Variants on Deaths, Case Incidence and Case Fatality Ratio among the Continents for the Period of 1 December 2020 to 15 March 2021. Genes 2021, 12, 1061. [Google Scholar] [CrossRef]
- Weekly Operational Update on COVID-19 Issue No. 81. WHO. Coronavirus Disease (2019). 2021. Available online: https://www.who.int/publications/m/item/weekly-operational-update-on-covid-19 (accessed on 23 November 2021).
- Yang, P.; Wang, X. COVID-19: A new challenge for human beings. Cell. Mol. Immunol. 2020, 17, 555–557. [Google Scholar] [CrossRef] [Green Version]
- Cui, F.; Zhou, H.S. Diagnostic methods and potential portable biosensors for coronavirus disease 2019. Biosens. Bioelectron. 2020, 165, 112349. [Google Scholar] [CrossRef]
- Larremore, D.B.; Wilder, B.; Lester, E.; Shehata, S.; Burke, J.M.; Hay, J.A.; Tambe, M.; Mina, M.J.; Parker, R. Test sensitivity is secondary to frequency and turnaround time for COVID-19 screening. Sci. Adv. 2021, 7, eabd5393. [Google Scholar] [CrossRef]
- COVID-19 Target Product Profiles for Priority Diagnostics to Support Response to the COVID-19 Pandemic v.1.0. Available online: https://www.who.int/publications/m/item/covid-19-target-product-profiles-for-priority-diagnostics-to-support-response-to-the-covid-19-pandemic-v.0.1 (accessed on 2 May 2022).
- La Marca, A.; Capuzzo, M.; Paglia, T.; Roli, L.; Trenti, T.; Nelson, S.M. Testing for SARS-CoV-2 (COVID-19): A systematic review and clinical guide to molecular and serological in-vitro diagnostic assays. Reprod. Biomed. Online 2020, 41, 483–499. [Google Scholar] [CrossRef]
- Mistry, D.A.; Wang, J.Y.; Moeser, M.E.; Starkey, T.; Lee, L.Y.W. A systematic review of the sensitivity and specificity of lateral flow devices in the detection of SARS-CoV-2. BMC Infect. Dis. 2021, 21, 828. [Google Scholar] [CrossRef]
- Guglielmi, G. Fast coronavirus tests: What they can and can’t do. Nature 2020, 585, 496–498. [Google Scholar] [CrossRef]
- Abousenna, M.S.; Sayed, R.H.; Darwish, D.M.; Saad, M.A. Sensitivity of lateral flow technique for evaluation of inactivated rift valley fever virus vaccine in comparison with serum neutralization test. World Vet. J. 2020, 10, 165–169. [Google Scholar] [CrossRef]
- Shaimaa, A.E.; Latif, A.A.; Sayed, R.H.; Jakeen, K.E. Develop of Lateral Flow Immunochromatographic Test and PCR for Detection of Salmonella Enteritidis in Poultry Farm. Inter. J. Vet. Sci. 2018, 7, 153–158. [Google Scholar]
- Bergmann-Leitner, E.S.; Mease, R.M.; Duncan, E.H.; Khan, F.; Waitumbi, J.; Angov, E. Evaluation of immunoglobulin purification methods and their impact on quality and yield of antigen-specific antibodies. Malar. J. 2008, 7, 129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Di Nardo, F.; Chiarello, M.; Cavalera, S.; Baggiani, C.; Anfossi, L. Ten years of lateral flow immunoassay technique applications: Trends, challenges and future perspectives. Sensors 2021, 21, 5185. [Google Scholar] [CrossRef]
- Ge, L.; Wang, D.; Lian, F.; Zhao, J.; Wang, Y.; Zhao, Y.; Zhang, L.; Wang, J.; Song, X.; Li, J.; et al. Lateral Flow Immunoassay for Visible Detection of Human Brucellosis Based on Blue Silica Nanoparticles. Front. Vet. Sci. 2021, 8, 771341. [Google Scholar] [CrossRef]
- Mohamed, M.M.; Abdelaziz, W.R.; Sayed, R.H.; Shasha, F.A.; Ali, A.F. Gold nanoparticles based assay for rapid detection of caseous lymphadenitis in sheep. Adv. Anim. Vet. Sci. 2021, 9, 709–714. [Google Scholar] [CrossRef]
- Ki, M. Task Force for 2019-nCoV. Epidemiologic characteristics of early cases with 2019 novel coronavirus (2019-nCoV) disease in Korea. Epidemiol. Health 2020, 42, e2020007. [Google Scholar] [CrossRef]
- Rahban, M.; Stanek, A.; Hooshmand, A.; Khamineh, Y.; Ahi, S.; Kazim, S.N.; Ahmad, F.; Muronetz, V.; Abousenna, M.S.; Zolghadri, S.; et al. Infection of Human Cells by SARS-CoV-2 and Molecular Overview of Gastrointestinal, Neurological, and Hepatic Problems in COVID-19 Patients. J. Clin. Med. 2021, 10, 4802. [Google Scholar] [CrossRef]
- Hsieh, W.-Y.; Lin, C.-H.; Lin, T.-C.; Lin, C.-H.; Chang, H.-F.; Tsai, C.-H.; Wu, H.-T.; Lin, C.-S. Development and Efficacy of Lateral Flow Point-of-Care Testing Devices for Rapid and Mass COVID-19 Diagnosis by the Detections of SARS-CoV-2 Antigen and Anti-SARS-CoV-2 Antibodies. Diagnostics 2021, 11, 1760. [Google Scholar] [CrossRef]
- Vann, M. COVID-19 Tests Can Spot Variants, Lab Companies Insist (9 February 2021). Available online: http://abcnewsradioonline.com/health-news/covid-19-tests-can-spot-variants-lab-companies-insist.html (accessed on 10 May 2022).
- Mertens, P.; De Vos, N.; Martiny, D.; Jassoy, C.; Mirazimi, A.; Cuypers, L.; Van den Wijngaert, S.; Monteil, V.; Melin, P.; Stoffels, K. Development and potential usefulness of the COVID-19 Ag Respi-Strip diagnostic assay in a pandemic context. Front. Med. 2020, 7, 225. [Google Scholar] [CrossRef] [PubMed]
- Liu, D.; Wu, F.; Cen, Y.; Ye, L.; Shi, X.; Huang, Y.; Fang, S.; Ma, L. Comparative research on nucleocapsid and spike glycoprotein as the rapid immunodetection targets of COVID-19 and establishment of immunoassay strips. Mol. Immunol. 2021, 131, 6–12. [Google Scholar] [CrossRef]
- Bachman, C.M.; Grant, B.D.; Anderson, C.E.; Alonzo, L.F.; Garing, S.; Byrnes, S.A.; Rivera, R.; Burkot, S.; Ball, A.; Stafford, J.W.; et al. Clinical validation of an open-access SARS-CoV-2 antigen detection lateral flow assay, compared to commercially available assays. PLoS ONE 2021, 16, e0256352. [Google Scholar] [CrossRef]
- Biby, A.; Wang, X.; Liu, X.; Roberson, O.; Henry, A.; Xia, X. Rapid testing for coronavirus disease 2019 (COVID-19). MRS Commun. 2022, 12, 12–23. [Google Scholar] [CrossRef] [PubMed]
- FDA. EUA Authorized Serology Test Performance. 2021. Available online: https://www.fda.gov/medical-devices/coronavirus-disease-2019-covid-19-emergencyuse-authorizations-medical-devices/eua-authorized-serology-test-performance (accessed on 10 May 2022).
- FDA. Potential for False Positive Results with Antigen Tests for Rapid Detection of SARS-CoV-2—Letter to Clinical Laboratory Staff and Health Care Providers. 2020. Available online: https://www.fda.gov/medical-devices/letters-healthcare-providers/potential-false-positive-results-antigen-tests-rapid-detection-sars-cov-2-letter-clinical-laboratory (accessed on 10 May 2022).
- Wise, J. COVID-19: Lateral flow tests miss over half of cases, Liverpool pilot data show. BMJ 2020, 371, m4848. [Google Scholar] [CrossRef] [PubMed]
- Flower, B.; Brown, J.C.; Simmons, B.; Moshe, M.; Frise, R.; Penn, R.; Kugathasan, R.; Petersen, C.; Daunt, A.; Ashby, D.; et al. Clinical and laboratory evaluation of SARS-CoV-2 lateral flow assays for use in a national COVID-19 seroprevalence survey. Thorax 2020, 75, 1082–1088. [Google Scholar] [CrossRef]
- Brooks, Z.C.; Das, S. COVID-19 Testing: Impact of Prevalence, Sensitivity, and Specificity on Patient Risk and Cost. Am. J. Clin. Pathol. 2020, 154, 575–584. [Google Scholar] [CrossRef]
- Brenner, H.; Gefeller, O. Variation of sensitivity, specificity, likelihood ratios and predictive values with disease prevalence. Stat. Med. 1997, 16, 981–991. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Method | 108 | 107 | 106 | 105 | 104 | 103 | 102 | 10 |
|---|---|---|---|---|---|---|---|---|
| LFI COVID-19 antigen | +ve | +ve | +ve | +ve | +ve | Weak positive | −ve | −ve |
| RT-qPCR | +ve (Ct20.3) | +ve (Ct23.7) | +ve (Ct26.5) | +ve (Ct29.5) | +ve (Ct31.1) | +ve (Ct33.4) | +ve (Ct37.1) | +ve (38.3) * |
| A * | ||||
|---|---|---|---|---|
| Method | RT-qPCR | Total Results | ||
| LFI COVID-19 antigen | Results | Positive | Negative | |
| positive | 35 (True +ve) | 3 (False +ve) | ||
| Negative | 2 (False −ve) | 160 (True −ve) | ||
| Total results | 37 | 163 | 200 | |
| B | ||||
| Sample | Sensitivity (%) | Specificity (%) | Accuracy (%) | |
| SARS-CoV-2 virus | 95% | 98% | 97% | |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sayed, R.H.; Abousenna, M.S.; Elsaady, S.A.; Soliman, R.; Saad, M.A. Development of Lateral Flow Immunochromatographic Test for Rapid Detection of SARS-CoV-2 Virus Antigens in Clinical Specimens. Nanomaterials 2022, 12, 2477. https://doi.org/10.3390/nano12142477
Sayed RH, Abousenna MS, Elsaady SA, Soliman R, Saad MA. Development of Lateral Flow Immunochromatographic Test for Rapid Detection of SARS-CoV-2 Virus Antigens in Clinical Specimens. Nanomaterials. 2022; 12(14):2477. https://doi.org/10.3390/nano12142477
Chicago/Turabian StyleSayed, Rafik Hamed, Mohamed Samy Abousenna, Shaimaa Abdelall Elsaady, Rafik Soliman, and Mohamed Ahmed Saad. 2022. "Development of Lateral Flow Immunochromatographic Test for Rapid Detection of SARS-CoV-2 Virus Antigens in Clinical Specimens" Nanomaterials 12, no. 14: 2477. https://doi.org/10.3390/nano12142477