Emerging Nano- and Micro-Technologies Used in the Treatment of Type-1 Diabetes

 ,
,
Abstract
:1. Introduction
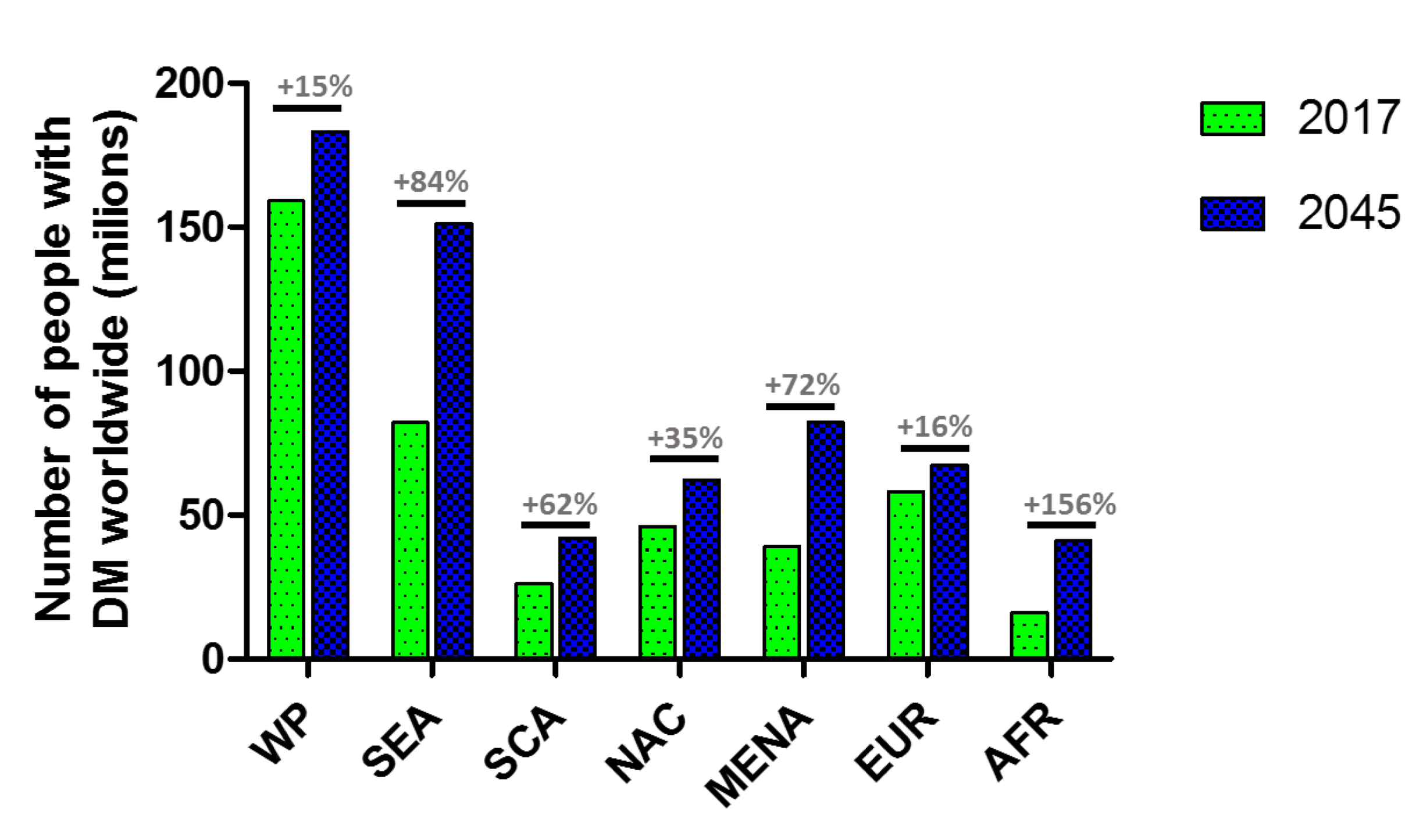
1.1. Diabetes Mellitus
1.2. Insulin
2. Platforms for Carrying Insulin
2.1. Nano-Scale Carriers
2.2. Micro-Scale Carriers
3. Platforms for Transdermal Delivery of Insulin
4. Platforms That Can Modulate Insulin Delivery
4.1. Glucose Oxidase-Based System
4.2. Glucose-Binding Protein-Based System
4.3. Phenilboronic Acid-Based System
5. Platforms to Accommodate or Protect Cell-Based Therapies for Insulin Release
5.1. Three-Dimensional (3D) Porous Bioscaffolds
5.2. Encapsulation Devices
6. Future Directions and Conclusions
Funding
Conflicts of Interest
References
- Ogurtsova, K.; da Rocha Fernandes, J.; Huang, Y.; Linnenkamp, U.; Guariguata, L.; Cho, N.H.; Cavan, D.; Shaw, J.; Makaroff, L.E. IDF Diabetes Atlas: Global estimates for the prevalence of diabetes for 2015 and 2040. Diabetes Res. Clin. Pract. 2017, 128, 40–50. [Google Scholar] [CrossRef] [Green Version]
- Zimmet, P.; Alberti, K.; Shaw, J. Global and societal implications of the diabetes epidemic. Nature 2001, 414, 782. [Google Scholar] [CrossRef]
- Cho, N.; Shaw, J.; Karuranga, S.; Huang, Y.; da Rocha Fernandes, J.; Ohlrogge, A.; Malanda, B. IDF Diabetes Atlas: Global estimates of diabetes prevalence for 2017 and projections for 2045. Diabetes Res. Clin. Pract. 2018, 138, 271–281. [Google Scholar] [CrossRef] [PubMed]
- Association, A.D. 2. Classification and diagnosis of diabetes: Standards of medical care in diabetes—2018. Diabetes Care 2018, 41, S13–S27. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Perera, M.J.; Reina, S.A.; Elfassy, T.; Potter, J.E.; Alvarez, D.S.; Simon, M.A.; Isasi, C.R.; Stuebe, A.M.; Schneiderman, N.; Llabre, M.M. Gestational diabetes and cardiovascular risk factors and disease in US Hispanics/Latinas in the Hispanic Community Health Study/Study of Latinos (HCHS/SOL). Women Health 2019, 59, 481–495. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, G. Insulin and insulin resistance. Clin. Biochem. Rev. 2005, 26, 19. [Google Scholar]
- Dodson, G.; Steiner, D. The role of assembly in insulin’s biosynthesis. Curr. Opin. Struct. Biol. 1998, 8, 189–194. [Google Scholar] [CrossRef]
- Hirsch, I.B. Insulin analogues. N. Engl. J. Med. 2005, 352, 174–183. [Google Scholar] [CrossRef]
- Moini, J. Epidemiology of Diabetes; Elsevier: Amsterdam, The Netherlands, 2019. [Google Scholar]
- Homko, C.; Deluzio, A.; Jimenez, C.; Kolaczynski, J.W.; Boden, G. Comparison of insulin aspart and lispro: Pharmacokinetic and metabolic effects. Diabetes Care 2003, 26, 2027–2031. [Google Scholar] [CrossRef] [Green Version]
- Lepore, M.; Pampanelli, S.; Fanelli, C.; Porcellati, F.; Bartocci, L.; Di Vincenzo, A.; Cordoni, C.; Costa, E.; Brunetti, P.; Bolli, G.B. Pharmacokinetics and pharmacodynamics of subcutaneous injection of long-acting human insulin analog glargine, NPH insulin, and ultralente human insulin and continuous subcutaneous infusion of insulin lispro. Diabetes 2000, 49, 2142–2148. [Google Scholar] [CrossRef] [Green Version]
- Orban, J.-C.; Van Obberghen, E.; Ichai, C. Acute Complications of Diabetes. In Metabolic Disorders and Critically Ill Patients; Springer: Berlin/Heidelberg, Germany, 2018; pp. 341–363. [Google Scholar]
- Control, D.; Group, C.T.R. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N. Engl. J. Med. 1993, 329, 977–986. [Google Scholar]
- Shi, J.; Votruba, A.R.; Farokhzad, O.C.; Langer, R. Nanotechnology in drug delivery and tissue engineering: From discovery to applications. Nano Lett. 2010, 10, 3223–3230. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bobo, D.; Robinson, K.J.; Islam, J.; Thurecht, K.J.; Corrie, S.R. Nanoparticle-based medicines: A review of FDA-approved materials and clinical trials to date. Pharm. Res. 2016, 33, 2373–2387. [Google Scholar] [CrossRef] [PubMed]
- Rahiman, S.; Tantry, B.A. Nanomedicine current trends in diabetes management. J. Nanomed. Nanotechol. 2012, 3, 1000137. [Google Scholar] [CrossRef] [Green Version]
- DiSanto, R.M.; Subramanian, V.; Gu, Z. Recent advances in nanotechnology for diabetes treatment. Wiley Interdiscip. Rev. Nanomed. Nanobiotechnology 2015, 7, 548–564. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Agnihotri, S.A.; Mallikarjuna, N.N.; Aminabhavi, T.M. Recent advances on chitosan-based micro-and nanoparticles in drug delivery. J. Control. Release 2004, 100, 5–28. [Google Scholar] [CrossRef]
- Lin, Y.-H.; Chen, C.-T.; Liang, H.-F.; Kulkarni, A.R.; Lee, P.-W.; Chen, C.-H.; Sung, H.-W. Novel nanoparticles for oral insulin delivery via the paracellular pathway. Nanotechnology 2007, 18, 105102. [Google Scholar] [CrossRef]
- Cui, F.; Qian, F.; Zhao, Z.; Yin, L.; Tang, C.; Yin, C. Preparation, characterization, and oral delivery of insulin loaded carboxylated chitosan grafted poly (methyl methacrylate) nanoparticles. Biomacromolecules 2009, 10, 1253–1258. [Google Scholar] [CrossRef]
- Takeuchi, H.; Yamamoto, H.; Niwa, T.; Hino, T.; Kawashima, Y. Enteral absorption of insulin in rats from mucoadhesive chitosan-coated liposomes. Pharm. Res. 1996, 13, 896–901. [Google Scholar] [CrossRef]
- Al-Remawi, M.; Elsayed, A.; Maghrabi, I.; Hamaidi, M.; Jaber, N. Chitosan/lecithin liposomal nanovesicles as an oral insulin delivery system. Pharm. Dev. Technol. 2017, 22, 390–398. [Google Scholar] [CrossRef]
- Makadia, H.K.; Siegel, S.J. Poly lactic-co-glycolic acid (PLGA) as biodegradable controlled drug delivery carrier. Polymers 2011, 3, 1377–1397. [Google Scholar] [CrossRef] [PubMed]
- Pridgen, E.M.; Alexis, F.; Kuo, T.T.; Levy-Nissenbaum, E.; Karnik, R.; Blumberg, R.S.; Langer, R.; Farokhzad, O.C. Transepithelial transport of Fc-targeted nanoparticles by the neonatal fc receptor for oral delivery. Sci. Transl. Med. 2013, 5, ra167–ra213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jain, A.; Jain, S.K. L-Valine appended PLGA nanoparticles for oral insulin delivery. Acta Diabetol. 2015, 52, 663–676. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Sun, M.; Zheng, A.; Cao, D.; Bi, Y.; Sun, J. Preparation and characterization of insulin-loaded bioadhesive PLGA nanoparticles for oral administration. Eur. J. Pharm. Sci. 2012, 45, 632–638. [Google Scholar] [CrossRef] [PubMed]
- Tao, A.J.; Cun, D.M.; Zhang, L.Q.; Shi, K. Preparation of insulin loaded PLGA-Hp55 nanoparticles for oral delivery. J. Pharm. Sci. 2007, 96, 421–427. [Google Scholar]
- Kisel, M.; Kulik, L.; Tsybovsky, I.; Vlasov, A.; Vorob’Yov, M.; Kholodova, E.; Zabarovskaya, Z. Liposomes with phosphatidylethanol as a carrier for oral delivery of insulin: Studies in the rat. Int. J. Pharm. 2001, 216, 105–114. [Google Scholar] [CrossRef]
- Mohanraj, V.J.; Barnes, T.J.; Prestidge, C.A. Silica nanoparticle coated liposomes: A new type of hybrid nanocapsule for proteins. Int. J. Pharm. 2010, 392, 285–293. [Google Scholar] [CrossRef]
- Iwanaga, K.; Ono, S.; Narioka, K.; Kakemi, M.; Morimoto, K.; Yamashita, S.; Namba, Y.; Oku, N. Application of surface-coated liposomes for oral delivery of peptide: Effects of coating the liposome’s surface on the GI transit of insulin. J. Pharm. Sci. 1999, 88, 248–252. [Google Scholar] [CrossRef]
- Schwartz, S.; Geho, B.; Rosenberg, L.; Lau, J. Single-blind, placebo-controlled, dose-ranging trial of oral HDV-insulin in patients with type 2 diabetes mellitus. Diabetes 2008, 57, A127. [Google Scholar]
- Keservani, R.K.; Sharma, A.K.; Kesharwani, R.K. Novel Approaches for Drug Delivery; IGI Global: Hershey, PA, USA, 2016. [Google Scholar]
- Kohane, D.S. Microparticles and nanoparticles for drug delivery. Biotechnol. Bioeng. 2007, 96, 203–209. [Google Scholar] [CrossRef]
- Kohane, D.S.; Lipp, M.; Kinney, R.C.; Anthony, D.C.; Louis, D.N.; Lotan, N.; Langer, R. Biocompatibility of lipid-protein-sugar particles containing bupivacaine in the epineurium. J. Biomed. Mater. Res. 2002, 59, 450–459. [Google Scholar] [CrossRef] [PubMed]
- Kohane, D.S.; Tse, J.Y.; Yeo, Y.; Padera, R.; Shubina, M.; Langer, R. Biodegradable polymeric microspheres and nanospheres for drug delivery in the peritoneum. J. Biomed. Mater. Res. A 2006, 77, 351–361. [Google Scholar] [CrossRef] [PubMed]
- Hinds, K.D.; Campbell, K.M.; Holland, K.M.; Lewis, D.H.; Piché, C.A.; Schmidt, P.G. PEGylated insulin in PLGA microparticles. In vivo and in vitro analysis. J. Control. Release 2005, 104, 447–460. [Google Scholar] [CrossRef] [PubMed]
- Primavera, R.; Magnone, M.; Di Mascolo, D.; Zocchi, E.; DE Pascale, A.; Decuzzi, P. Controlled Release of Insulin Granules from PLGA Microparticles for Glucose Modulation in Diabetes. Am. Diabetes Assoc. 2018, 67. [Google Scholar] [CrossRef]
- Cheng, J.; Teply, B.A.; Jeong, S.Y.; Yim, C.H.; Ho, D.; Sherifi, I.; Jon, S.; Farokhzad, O.C.; Khademhosseini, A.; Langer, R.S. Magnetically responsive polymeric microparticles for oral delivery of protein drugs. Pharm. Res. 2006, 23, 557–564. [Google Scholar] [CrossRef]
- Zhang, Y.; Wei, W.; Lv, P.; Wang, L.; Ma, G. Preparation and evaluation of alginate–chitosan microspheres for oral delivery of insulin. Eur. J. Pharm. Biopharm. 2011, 77, 11–19. [Google Scholar] [CrossRef]
- Zhang, N.; Li, J.; Jiang, W.; Ren, C.; Li, J.; Xin, J.; Li, K. Effective protection and controlled release of insulin by cationic β-cyclodextrin polymers from alginate/chitosan nanoparticles. Int. J. Pharm. 2010, 393, 213–219. [Google Scholar] [CrossRef]
- Nur, M.; Vasiljevic, T. Insulin Inclusion into a Tragacanth Hydrogel: An Oral Delivery System for Insulin. Materials 2018, 11, 79. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Tabata, Y.; Morimoto, K. Aminated gelatin microspheres as a nasal delivery system for peptide drugs: Evaluation of in vitro release and in vivo insulin absorption in rats. J. Control. Release 2006, 113, 31–37. [Google Scholar] [CrossRef]
- Emisphere Technologies, Inc. Emisphere’s Press Release (October 6, 2006) on Additional Clinical Data from Phase 2 Oral Insulin Trial. 6 October 2006. Available online: http://www.emisphere.com (accessed on 15 February 2009).
- Wajcberg, E.; Miyazaki, Y.; Triplitt, C.; Cersosimo, E.; DeFronzo, R.A. Dose-response effect of a single administration of oral hexyl-insulin monoconjugate 2 in healthy nondiabetic subjects. Diabetes Care 2004, 27, 2868–2873. [Google Scholar] [CrossRef] [Green Version]
- Iyer, H.; Khedkar, A.; Verma, M.; Krishnamurthy, S.; Anand, A. A Dose Escalation Study of IN-105 (Insulin Analogue) Tablets in Type 2 Diabetes Mellitus Subjects. Diabetes 2009, 58, A117. [Google Scholar]
- Angelo, R.; Rousseau, K.; Grant, M.; Leone-Bay, A.; Richardson, P. Technosphere® insulin: Defining the role of technosphere particles at the cellular level. J. Diabetes Sci. Technol. 2009, 3, 545–554. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Food and Drug Administration. FDA Approves Afrezza to Treat Diabetes. 2014. Available online: https://www.thepharmaletter.com/article/fda-approves-mannkind-s-afrezza-to-treat-diabetes (accessed on 27 June 2014).
- Hamishehkar, H.; Emami, J.; Najafabadi, A.R.; Gilani, K.; Minaiyan, M.; Hassanzadeh, K.; Mahdavi, H.; Koohsoltani, M.; Nokhodchi, A. Pharmacokinetics and pharmacodynamics of controlled release insulin loaded PLGA microcapsules using dry powder inhaler in diabetic rats. Biopharm. Drug Dispos. 2010, 31, 189–201. [Google Scholar] [CrossRef] [PubMed]
- Edwards, D.A.; Hanes, J.; Caponetti, G.; Hrkach, J.; Ben-Jebria, A.; Eskew, M.L.; Mintzes, J.; Deaver, D.; Lotan, N.; Langer, R. Large porous particles for pulmonary drug delivery. Science 1997, 276, 1868–1872. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Oh, Y.J.; Lee, S.K.; Lee, K.Y. Facile control of porous structures of polymer microspheres using an osmotic agent for pulmonary delivery. J. Control. Release 2010, 146, 61–67. [Google Scholar] [CrossRef]
- Suzuki, Y.; Yamaguchi, T. Effects of hyaluronic acid on macrophage phagocytosis and active oxygen release. Agents Actions 1993, 38, 32–37. [Google Scholar] [CrossRef]
- Prestwich, G.D.; Vercruysse, K.P. Therapeutic applications of hyaluronic acid and hyaluronan derivatives. Pharm. Sci. Technol. Today 1998, 1, 42–43. [Google Scholar] [CrossRef]
- Surendrakumar, K.; Martyn, G.; Hodgers, E.; Jansen, M.; Blair, J. Sustained release of insulin from sodium hyaluronate based dry powder formulations after pulmonary delivery to beagle dogs. J. Control. Release 2003, 91, 385–394. [Google Scholar] [CrossRef]
- Narayan, R.J. Transdermal delivery of insulin via microneedles. J. Biomed. Nanotechnol. 2014, 10, 2244–2260. [Google Scholar] [CrossRef]
- Gerstel, M.S.; Place, V.A. Drug Delivery Device. U.S. Patent 3,964,482, 22 June 1976. [Google Scholar]
- Bariya, S.H.; Gohel, M.C.; Mehta, T.A.; Sharma, O.P. Microneedles: An emerging transdermal drug delivery system. J. Pharm. Pharmacol. 2012, 64, 11–29. [Google Scholar] [CrossRef]
- Martanto, W.; Davis, S.P.; Holiday, N.R.; Wang, J.; Gill, H.S.; Prausnitz, M.R. Transdermal delivery of insulin using microneedles in vivo. Pharm. Res. 2004, 21, 947–952. [Google Scholar] [CrossRef] [PubMed]
- Migalska, K.; Morrow, D.I.; Garland, M.J.; Thakur, R.; Woolfson, A.D.; Donnelly, R.F. Laser-engineered dissolving microneedle arrays for transdermal macromolecular drug delivery. Pharm. Res. 2011, 28, 1919–1930. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Jin, M.-N.; Quan, Y.-S.; Kamiyama, F.; Katsumi, H.; Sakane, T.; Yamamoto, A. The development and characteristics of novel microneedle arrays fabricated from hyaluronic acid, and their application in the transdermal delivery of insulin. J. Control. Release 2012, 161, 933–941. [Google Scholar] [CrossRef] [PubMed]
- Ling, M.-H.; Chen, M.-C. Dissolving polymer microneedle patches for rapid and efficient transdermal delivery of insulin to diabetic rats. Acta Biomater. 2013, 9, 8952–8961. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.D.; Kim, M.; Yang, H.; Lee, K.; Jung, H. Droplet-born air blowing: Novel dissolving microneedle fabrication. J. Control. Release 2013, 170, 430–436. [Google Scholar] [CrossRef]
- Nordquist, L.; Roxhed, N.; Griss, P.; Stemme, G. Novel microneedle patches for active insulin delivery are efficient in maintaining glycaemic control: An initial comparison with subcutaneous administration. Pharm. Res. 2007, 24, 1381–1388. [Google Scholar] [CrossRef]
- Norman, J.J.; Brown, M.R.; Raviele, N.A.; Prausnitz, M.R.; Felner, E.I. Faster pharmacokinetics and increased patient acceptance of intradermal insulin delivery using a single hollow microneedle in children and adolescents with type 1 diabetes. Pediatric Diabetes 2013, 14, 459–465. [Google Scholar] [CrossRef]
- Mo, R.; Jiang, T.; Di, J.; Tai, W.; Gu, Z. Emerging micro-and nanotechnology based synthetic approaches for insulin delivery. Chem. Soc. Rev. 2014, 43, 3595–3629. [Google Scholar] [CrossRef]
- Reichard, P.; Nilsson, B.-Y.; Rosenqvist, U. The effect of long-term intensified insulin treatment on the development of microvascular complications of diabetes mellitus. N. Engl. J. Med. 1993, 329, 304–309. [Google Scholar] [CrossRef]
- Brogden, R.N.; Heel, R. Human insulin. Drugs 1987, 34, 350–371. [Google Scholar] [CrossRef]
- Brownlee, M.; Cerami, A. A glucose-controlled insulin-delivery system: Semisynthetic insulin bound to lectin. Science 1979, 206, 1190–1191. [Google Scholar] [CrossRef] [PubMed]
- Russell, S.J.; El-Khatib, F.H.; Sinha, M.; Magyar, K.L.; McKeon, K.; Goergen, L.G.; Balliro, C.; Hillard, M.A.; Nathan, D.M.; Damiano, E.R. Outpatient glycemic control with a bionic pancreas in type 1 diabetes. N. Engl. J. Med. 2014, 371, 313–325. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Webber, M.J.; Anderson, D.G. Smart approaches to glucose-responsive drug delivery. J. Drug Target. 2015, 23, 651–655. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ravaine, V.; Ancla, C.; Catargi, B. Chemically controlled closed-loop insulin delivery. J. Control. Release 2008, 132, 2–11. [Google Scholar] [CrossRef] [PubMed]
- Veiseh, O.; Tang, B.C.; Whitehead, K.A.; Anderson, D.G.; Langer, R. Managing diabetes with nanomedicine: Challenges and opportunities. Nat. Rev. Drug Discov. 2015, 14, 45. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ferri, S.; Kojima, K.; Sode, K. Review of Glucose Oxidases and Glucose Dehydrogenases: A Bird’s Eye View of Glucose Sensing Enzymes; SAGE Publications: New York, NY, USA, 2011. [Google Scholar]
- Zhao, L.; Wang, L.; Zhang, Y.; Xiao, S.; Bi, F.; Zhao, J.; Gai, G.; Ding, J. Glucose oxidase-based glucose-sensitive drug delivery for diabetes treatment. Polymers 2017, 9, 255. [Google Scholar] [CrossRef]
- Kim, M.Y.; Kim, J. Chitosan microgels embedded with catalase nanozyme-loaded mesocellular silica foam for glucose-responsive drug delivery. ACS Biomater. Sci. Eng. 2017, 3, 572–578. [Google Scholar] [CrossRef]
- Gu, Z.; Aimetti, A.A.; Wang, Q.; Dang, T.T.; Zhang, Y.; Veiseh, O.; Cheng, H.; Langer, R.S.; Anderson, D.G. Injectable nano-network for glucose-mediated insulin delivery. Acs Nano 2013, 7, 4194–4201. [Google Scholar] [CrossRef]
- Hu, X.; Yu, J.; Qian, C.; Lu, Y.; Kahkoska, A.R.; Xie, Z.; Jing, X.; Buse, J.B.; Gu, Z. H2O2-responsive vesicles integrated with transcutaneous patches for glucose-mediated insulin delivery. ACS Nano 2017, 11, 613–620. [Google Scholar] [CrossRef] [Green Version]
- Wang, J.; Ye, Y.; Yu, J.; Kahkoska, A.R.; Zhang, X.; Wang, C.; Sun, W.; Corder, R.D.; Chen, Z.; Khan, S.A. Core–Shell Microneedle Gel for Self-Regulated Insulin Delivery. ACS Nano 2018, 12, 2466–2473. [Google Scholar] [CrossRef]
- Yu, J.; Qian, C.; Zhang, Y.; Cui, Z.; Zhu, Y.; Shen, Q.; Ligler, F.S.; Buse, J.B.; Gu, Z. Hypoxia and H2O2 dual-sensitive vesicles for enhanced glucose-responsive insulin delivery. Nano Lett. 2017, 17, 733–739. [Google Scholar] [CrossRef] [PubMed]
- Volpatti, L.R.; Matranga, M.A.; Cortinas, A.B.; Delcassian, D.; Daniel, K.B.; Langer, R.; Anderson, D.G. Glucose-Responsive Nanoparticles for Rapid and Extended Self-Regulated Insulin Delivery. ACS Nano 2019, 14, 488–497. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Chu, M.K.; Gordijo, C.R.; Abbasi, A.Z.; Chen, K.; Adissu, H.A.; Löhn, M.; Giacca, A.; Plettenburg, O.; Wu, X.Y. Microfabricated microporous membranes reduce the host immune response and prolong the functional lifetime of a closed-loop insulin delivery implant in a type 1 diabetic rat model. Biomaterials 2015, 47, 51–61. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.X.; Li, J.; Zhang, T.; Amini, M.A.; He, C.; Lu, B.; Ahmed, T.; Lip, H.; Rauth, A.M.; Wu, X.Y. Importance of integrating nanotechnology with pharmacology and physiology for innovative drug delivery and therapy–an illustration with firsthand examples. Acta Pharm. Sin. 2018, 39, 825. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sharon, N.; Lis, H. Lectins: Cell-agglutinating and sugar-specific proteins. Science 1972, 177, 949–959. [Google Scholar] [CrossRef] [PubMed]
- Yin, R.; Tong, Z.; Yang, D.; Nie, J. Glucose and pH dual-responsive concanavalin A based microhydrogels for insulin delivery. Int. J. Biol. Macromol. 2011, 49, 1137–1142. [Google Scholar] [CrossRef]
- Sato, K.; Kodama, D.; Endo, Y.; Anzai, J.-I. Preparation of insulin-containing microcapsules by a layer-by-layer deposition of concanavalin A and glycogen. J. Nanosci. Nanotechnol. 2009, 9, 386–390. [Google Scholar] [CrossRef]
- Ballerstadt, R.; Evans, C.; McNichols, R.; Gowda, A. Concanavalin A for in vivo glucose sensing: A biotoxicity review. Biosens. Bioelectron. 2006, 22, 275–284. [Google Scholar] [CrossRef]
- Krug, A.W.; Visser, S.A.; Tsai, K.; Kandala, B.; Fancourt, C.; Thornton, B.; Morrow, L.; Kaarsholm, N.C.; Bernstein, H.S.; Stoch, S.A.; et al. Clinical Evaluation of MK-2640: An Insulin Analog with Glucose-Responsive Properties. Clin. Pharmacol. Ther. 2019, 105, 417–425. [Google Scholar] [CrossRef]
- Fang, H.; Kaur, G.; Wang, B. Progress in boronic acid-based fluorescent glucose sensors. J. Fluoresc. 2004, 14, 481–489. [Google Scholar] [CrossRef]
- Bull, S.D.; Davidson, M.G.; Van den Elsen, J.M.; Fossey, J.S.; Jenkins, A.T.A.; Jiang, Y.-B.; Kubo, Y.; Marken, F.; Sakurai, K.; Zhao, J. Exploiting the reversible covalent bonding of boronic acids: Recognition, sensing, and assembly. Acc. Chem. Res. 2012, 46, 312–326. [Google Scholar] [CrossRef] [PubMed]
- Kataoka, K.; Hisamitsu, I.; Sayama, N.; Okano, T.; Sakurai, Y.J.T. Novel sensing system for glucose based on the complex formation between phenylborate and fluorescent diol compounds. J. Biochem. 1995, 117, 1145–1147. [Google Scholar] [CrossRef] [PubMed]
- Springsteen, G.; Wang, B. A detailed examination of boronic acid–diol complexation. Tetrahedron 2002, 58, 5291–5300. [Google Scholar] [CrossRef]
- Zhang, C.; Losego, M.D.; Braun, P.V. Hydrogel-based glucose sensors: Effects of phenylboronic acid chemical structure on response. Chem. Mater. 2013, 25, 3239–3250. [Google Scholar] [CrossRef] [Green Version]
- Wang, B.; Ma, R.; Liu, G.; Li, Y.; Liu, X.; An, Y.; Shi, L. Glucose-responsive micelles from self-assembly of poly (ethylene glycol)-b-poly (acrylic acid-co-acrylamidophenylboronic acid) and the controlled release of insulin. Langmuir 2009, 25, 12522–12528. [Google Scholar] [CrossRef]
- Ma, R.; Yang, H.; Li, Z.; Liu, G.; Sun, X.; Liu, X.; An, Y.; Shi, L. Phenylboronic acid-based complex micelles with enhanced glucose-responsiveness at physiological pH by complexation with glycopolymer. Biomacromolecules 2012, 13, 3409–3417. [Google Scholar] [CrossRef]
- Kim, H.; Kang, Y.J.; Kang, S.; Kim, K.T. Monosaccharide-responsive release of insulin from polymersomes of polyboroxole block copolymers at neutral pH. J. Am. Chem. Soc. 2012, 134, 4030–4033. [Google Scholar] [CrossRef]
- Zhao, Y.; Trewyn, B.G.; Slowing, I.I.; Lin, V.S.-Y. Mesoporous silica nanoparticle-based double drug delivery system for glucose-responsive controlled release of insulin and cyclic AMP. J. Am. Chem. Soc. 2009, 131, 8398–8400. [Google Scholar] [CrossRef] [Green Version]
- Yu, J.; Wang, J.; Zhang, Y.; Chen, G.; Mao, W.; Ye, Y.; Kahkoska, A.R.; Buse, J.B.; Langer, R.; Gu, Z. Glucose-responsive insulin patch for the regulation of blood glucose in mice and minipigs. Nat. Biomed. Eng. 2020, 1–8. [Google Scholar] [CrossRef]
- Niclauss, N.; Meier, R.; Bédat, B.; Berishvili, E.; Berney, T. Beta-cell replacement: Pancreas and islet cell transplantation. In Novelties in Diabetes; Karger Publishers: Basel, Switzerland, 2016; Volume 31, pp. 146–162. [Google Scholar]
- Procurement, O.; Network, T. Scientific Registry of Transplant Recipients (SRTR). In OPTN/SRTR 2010 Annual Data Report; Department of Health and Human Services, Health Resources and Services Administration, Healthcare Systems Bureau, Division of Transplantation: Rockville, MD, USA, 2011; Volume 12, pp. 1–156. [Google Scholar]
- Farney, A.C.; Sutherland, D.E.; Opara, E.C. Evolution of islet transplantation for the last 30 years. Pancreas 2016, 45, 8–20. [Google Scholar] [CrossRef]
- Stratta, R.J.; Farney, A.C.; Rogers, J.; Orlando, G. Immunosuppression for pancreas transplantation with an emphasis on antibody induction strategies: Review and perspective. Expert Rev. Clin. Immunol. 2014, 10, 117–132. [Google Scholar] [CrossRef] [PubMed]
- Shapiro, A.J.; Ricordi, C.; Hering, B.J.; Auchincloss, H.; Lindblad, R.; Robertson, R.P.; Secchi, A.; Brendel, M.D.; Berney, T.; Brennan, D.C. International trial of the Edmonton protocol for islet transplantation. N. Engl. J. Med. 2006, 355, 1318–1330. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ryan, E.A.; Paty, B.W.; Senior, P.A.; Bigam, D.; Alfadhli, E.; Kneteman, N.M.; Lakey, J.R.; Shapiro, A.M.J. Five-year follow-up after clinical islet transplantation. Diabetes 2005, 54, 2060–2069. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Balamurugan, A.; Naziruddin, B.; Lockridge, A.; Tiwari, M.; Loganathan, G.; Takita, M.; Matsumoto, S.; Papas, K.; Trieger, M.; Rainis, H. Islet product characteristics and factors related to successful human islet transplantation from the Collaborative Islet Transplant Registry (CITR) 1999–2010. Arab. Archaeol. Epigr. 2014, 14, 2595–2606. [Google Scholar] [CrossRef] [PubMed]
- Farney, A.; Najarian, J.; Nakhleh, R.; Lloveras, G.; Field, M.; Gores, P.; Sutherland, D. Autotransplantation of dispersed pancreatic islet tissue combined with total or near-total pancreatectomy for treatment of chronic pancreatitis. Surgery 1991, 110, 427–437, discussion 437–429. [Google Scholar] [PubMed]
- Sakata, N.; Egawa, S.; Motoi, F.; Mikami, Y.; Ishida, M.; Aoki, T.; Ottomo, S.; Fukuyama, S.; Rikiyama, T.; Katayose, Y.J. Institutional indications for islet transplantation after total pancreatectomy. J. Hepato-Biliary-Pancreat. Surg. 2008, 15, 488–492. [Google Scholar] [CrossRef]
- Jindal, R.M.; Ricordi, C.; Shriver, C.D. Autologous pancreatic islet transplantation for severe trauma. N. Engl. J. Med. 2010, 362, 1550. [Google Scholar] [CrossRef] [Green Version]
- Thakor, A.S.; Sangha, B.S.; Ho, S.G.; Warnock, G.L.; Meloche, M.; Liu, D.M. Percutaneous autologous pancreatic islet cell transplantation for traumatic pancreatic injury. J. Clin. Endocrinol. Metab. 2015, 100, 1230–1233. [Google Scholar] [CrossRef] [Green Version]
- Ricordi, C.; Tzakis, A.G.; Carroll, P.B.; Zeng, Y.; Rilo, H.L.R.; Alejandro, R.; Shapiro, R.; Fung, J.J.; Demetris, A.J.; Mintz, D.H. Human islet isolation and allotransplantation in 22 consecutive cases. Transplantation 1992, 53, 407. [Google Scholar] [CrossRef] [Green Version]
- Elliott, R.B.; Escobar, L.; Tan, P.L.; Muzina, M.; Zwain, S.; Buchanan, C. Live encapsulated porcine islets from a type 1 diabetic patient 9.5 yr after xenotransplantation. Xenotransplantation 2007, 14, 157–161. [Google Scholar] [CrossRef]
- Hering, B.J.; Walawalkar, N. Pig-to-nonhuman primate islet xenotransplantation. Transpl. Immunol. 2009, 21, 81–86. [Google Scholar] [CrossRef] [PubMed]
- Hering, B.J.; Clarke, W.R.; Bridges, N.D.; Eggerman, T.L.; Alejandro, R.; Bellin, M.D.; Chaloner, K.; Czarniecki, C.W.; Goldstein, J.S.; Hunsicker, L.G. Phase 3 trial of transplantation of human islets in type 1 diabetes complicated by severe hypoglycemia. Diabetes Care 2016, 39, 1230–1240. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Vacanti, J.P.; Langer, R. Tissue engineering: The design and fabrication of living replacement devices for surgical reconstruction and transplantation. Lancet 1999, 354, S32–S34. [Google Scholar] [CrossRef]
- de Vos, P.; Hamel, A.F.; Tatarkiewicz, K. Considerations for successful transplantation of encapsulated pancreatic islets. Diabetologia 2002, 45, 159–173. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chaikof, E.L. Engineering and material considerations in islet cell transplantation. Annu. Rev. Biomed. Eng. 1999, 1, 103–127. [Google Scholar] [CrossRef] [PubMed]
- Merani, S.; Toso, C.; Emamaullee, J.; Shapiro, A.M.J. Optimal implantation site for pancreatic islet transplantation. BJS 2008, 95, 1449–1461. [Google Scholar] [CrossRef]
- Mellgren, A.; Landström, A.S.; Petersson, B.; Andersson, A. The renal subcapsular site offers better growth conditions for transplanted mouse pancreatic islet cells than the liver or spleen. Diabetologia 1986, 29, 670–672. [Google Scholar] [CrossRef]
- Juang, J.-H.; Hsu, B.-S.; Kuo, C.-H. Islet transplantation at subcutaneous and intramuscular sites. Transplant. Proc. 2005, 37, 3479–3481. [Google Scholar] [CrossRef]
- Berman, D.M.; O’Neil, J.J.; Coffey, L.C.; Chaffanjon, P.C.; Kenyon, N.M.; Ruiz, P., Jr.; Pileggi, A.; Ricordi, C.; Kenyon, N.S. Long-term survival of nonhuman primate islets implanted in an omental pouch on a biodegradable scaffold. Arab. Archaeol. Epigr. 2009, 9, 91–104. [Google Scholar] [CrossRef] [Green Version]
- Echeverri, G.; McGrath, K.; Bottino, R.; Hara, H.; Dons, E.; Van Der Windt, D.; Ekser, B.; Casu, A.; Houser, S.; Ezzelarab, M. Endoscopic gastric submucosal transplantation of islets (ENDO-STI): Technique and initial results in diabetic pigs. Arab. Archaeol. Epigr. 2009, 9, 2485–2496. [Google Scholar] [CrossRef]
- Blomeier, H.; Zhang, X.; Rives, C.; Brissova, M.; Hughes, E.; Baker, M.; Powers, A.C.; Kaufman, D.B.; Shea, L.D.; Lowe, W.L., Jr. Polymer scaffolds as synthetic microenvironments for extrahepatic islet transplantation. Transplantation 2006, 82, 452. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daoud, J.T.; Petropavlovskaia, M.S.; Patapas, J.M.; Degrandpré, C.E.; DiRaddo, R.W.; Rosenberg, L.; Tabrizian, M. Long-term in vitro human pancreatic islet culture using three-dimensional microfabricated scaffolds. Biomaterials 2011, 32, 1536–1542. [Google Scholar] [CrossRef] [PubMed]
- Feng, B.; Jinkang, Z.; Zhen, W.; Jianxi, L.; Jiang, C.; Jian, L.; Guolin, M.; Xin, D. The effect of pore size on tissue ingrowth and neovascularization in porous bioceramics of controlled architecture in vivo. Biomed. Mater. 2011, 6, 015007. [Google Scholar] [CrossRef] [PubMed]
- Dufour, J.M.; Rajotte, R.V.; Zimmerman, M.; Rezania, A.; Kin, T.; Dixon, D.E.; Korbutt, G.S. Development of an ectopic site for islet transplantation, using biodegradable scaffolds. Tissue Eng. 2005, 11, 1323–1331. [Google Scholar] [CrossRef]
- Jiang, K.; Weaver, J.D.; Li, Y.; Chen, X.; Liang, J.; Stabler, C.L. Local release of dexamethasone from macroporous scaffolds accelerates islet transplant engraftment by promotion of anti-inflammatory M2 macrophages. Biomaterials 2017, 114, 71–81. [Google Scholar] [CrossRef]
- Brady, A.-C.; Martino, M.M.; Pedraza, E.; Sukert, S.; Pileggi, A.; Ricordi, C.; Hubbell, J.A.; Stabler, C.L. Proangiogenic hydrogels within macroporous scaffolds enhance islet engraftment in an extrahepatic site. Tissue Eng. Part A 2013, 19, 2544–2552. [Google Scholar] [CrossRef] [Green Version]
- Yap, W.T.; Salvay, D.M.; Silliman, M.A.; Zhang, X.; Bannon, Z.G.; Kaufman, D.B.; Lowe, W.L., Jr.; Shea, L.D. Collagen IV-modified scaffolds improve islet survival and function and reduce time to euglycemia. Tissue Eng. Part A 2013, 19, 2361–2372. [Google Scholar] [CrossRef] [Green Version]
- Jalili, R.B.; Moeen Rezakhanlou, A.; Hosseini-Tabatabaei, A.; Ao, Z.; Warnock, G.L.; Ghahary, A. Fibroblast populated collagen matrix promotes islet survival and reduces the number of islets required for diabetes reversal. J. Cell. Physiol. 2011, 226, 1813–1819. [Google Scholar] [CrossRef]
- Mao, G.-H.; Chen, G.-A.; Bai, H.-Y.; Song, T.-R.; Wang, Y.-X. The reversal of hyperglycaemia in diabetic mice using PLGA scaffolds seeded with islet-like cells derived from human embryonic stem cells. Biomaterials 2009, 30, 1706–1714. [Google Scholar] [CrossRef]
- Sakata, N.; Sumi, S.; Yoshimatsu, G.; Goto, M.; Egawa, S.; Unno, M. Encapsulated islets transplantation: Past, present and future. World J. Gastrointest. Pathophysiol. 2012, 3, 19. [Google Scholar] [CrossRef]
- Jones, K.S.; Sefton, M.V.; Gorczynski, R.M. In vivo recognition by the host adaptive immune system of microencapsulated xenogeneic cells. Transplantation 2004, 78, 1454–1462. [Google Scholar] [CrossRef] [PubMed]
- Hayashi, H.; Inoue, K.; Aung, T.; Tun, T.; Yuanjun, G.; Wending, W.; Shinohara, S.; Kaji, H.; Doi, R.; Setoyama, H. Application of a novel B cell line MIN6 to a mesh-reinforced polyvinyl alcohol hydrogel tube and three-layer agarose microcapsules: An in vitro study. Cell Transplant. 1996, 5, S65–S69. [Google Scholar] [CrossRef]
- Lee, J.I.; Nishimura, R.; Sakai, H.; Sasaki, N.; Kenmochi, T. A newly developed immunoisolated bioartificial pancreas with cell sheet engineering. Cell Transplant. 2008, 17, 51–59. [Google Scholar] [CrossRef] [PubMed]
- Beck, J.; Angus, R.; Madsen, B.; Britt, D.; Vernon, B.; Nguyen, K.T. Islet encapsulation: Strategies to enhance islet cell functions. Tissue Eng. 2007, 13, 589–599. [Google Scholar] [CrossRef]
- Lim, F.; Sun, A.M. Microencapsulated islets as bioartificial endocrine pancreas. Science 1980, 210, 908–910. [Google Scholar] [CrossRef]
- Opara, E.C.; McQuilling, J.P.; Farney, A.C. Microencapsulation of pancreatic islets for use in a bioartificial pancreas. In Organ Regeneration; Springer: Berlin/Heidelberg, Germany, 2013; pp. 261–266. [Google Scholar]
- Hall, K.K.; Gattás-Asfura, K.M.; Stabler, C.L. Microencapsulation of islets within alginate/poly (ethylene glycol) gels cross-linked via Staudinger ligation. Acta Biomater. 2011, 7, 614–624. [Google Scholar] [CrossRef] [Green Version]
- Goosen, M.F.; O’Shea, G.M.; Gharapetian, H.M.; Chou, S.; Sun, A.M. Optimization of microencapsulation parameters: Semipermeable microcapsules as a bioartificial pancreas. Biotechnol. Bioeng. 1985, 27, 146–150. [Google Scholar] [CrossRef]
- Lembert, N.; Wesche, J.; Petersen, P.; Zschocke, P.; Enderle, A.; Planck, H.; Ammon, H. Macroencapsulation of rat islets without alteration of insulin secretion kinetics. Exp. Clin. Endocrinol. Diabetes 2001, 109, 116–119. [Google Scholar] [CrossRef]
- Inoue, K.; Fujisato, T.; Gu, Y.; Burczak, K.; Sumi, S.; Kogire, M.; Tobe, T.; Uchida, K.; Nakai, I.; Maetani, S. Experimental hybrid islet transplantation: Application of polyvinyl alcohol membrane for entrapment of islets. Pancreas 1992, 7, 562–568. [Google Scholar] [CrossRef]
- Aung, T.; Kogire, M.; Inoue, K.; Fujisato, T.; Gu, Y.; Burczak, K.; Shinohara, S.; Mitsuo, M.; Maetani, S.; Ikada, Y. Insulin release from a bioartificial pancreas using a mesh reinforced polyvinyl alcohol hydrogel tube. An in vitro study. ASAIO J. 1993, 39, 93–96. [Google Scholar] [CrossRef]
- Miyamoto, M.; Inoue, K.; Gu, Y.; Tun, T.; Cui, W.; Fujiwara, I.; Ohyanagi, H.; Hayashi, H.; Yamazaki, T.; Setoyama, H. Improved large-scale isolation of breeder porcine islets: Possibility of harvesting from nonheart-beating donor. Cell Transplant. 1998, 7, 397–402. [Google Scholar] [CrossRef] [PubMed]
- Sakurai, T.; Satake, A.; Sumi, S.; Inoue, K.; Nagata, N.; Tabata, Y.; Miyakoshi, J. The efficient prevascularization induced by fibroblast growth factor 2 with a collagen-coated device improves the cell survival of a bioartificial pancreas. Pancreas 2004, 28, e70–e79. [Google Scholar] [CrossRef] [PubMed]
- Qi, M.; Gu, Y.; Sakata, N.; Kim, D.; Shirouzu, Y.; Yamamoto, C.; Hiura, A.; Sumi, S.; Inoue, K. PVA hydrogel sheet macroencapsulation for the bioartificial pancreas. Biomaterials 2004, 25, 5885–5892. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Soon-Shiong, P. Treatment of type I diabetes using encapsulated islets. Adv. Drug Deliv. Rev. 1999, 35, 259–270. [Google Scholar] [CrossRef]
- Calafiore, R.; Basta, G.; Luca, G.; Lemmi, A.; Racanicchi, L.; Mancuso, F.; Montanucci, M.; Brunetti, P. Standard technical procedures for microencapsulation of human islets for graft into nonimmunosuppressed patients with type 1 diabetes mellitus. Transplant. Proc. 2006, 38, 1156–1157. [Google Scholar] [CrossRef]
- Tuch, B.E.; Keogh, G.W.; Williams, L.J.; Wu, W.; Foster, J.L.; Vaithilingam, V.; Philips, R. Safety and viability of microencapsulated human islets transplanted into diabetic humans. Diabetes Care 2009, 32, 1887–1889. [Google Scholar] [CrossRef] [Green Version]
- MacKenzie, D.A.; Hullett, D.A.; Sollinger, H.W. Xenogeneic transplantation of porcine islets: An overview. Transplantation 2003, 76, 887–891. [Google Scholar] [CrossRef]
- Rayat, G.R.; Rajotte, R.V.; Korbutt, G.S. Potential application of neonatal porcine islets as treatment for type 1 diabetes: A review. Ann. N. Y. Acad. Sci. 1999, 875, 175–188. [Google Scholar] [CrossRef]
- Ito, T.; Itakura, S.; Todorov, I.; Rawson, J.; Asari, S.; Shintaku, J.; Nair, I.; Ferreri, K.; Kandeel, F.; Mullen, Y. Mesenchymal stem cell and islet co-transplantation promotes graft revascularization and function. Transplantation 2010, 89, 1438–1445. [Google Scholar] [CrossRef]
- Pepper, A.R.; Gala-Lopez, B.; Pawlick, R.; Merani, S.; Kin, T.; Shapiro, A.J. A prevascularized subcutaneous device-less site for islet and cellular transplantation. Nat. Biotechnol. 2015, 33, 518. [Google Scholar] [CrossRef]
- Song, W.; Chiu, A.; Wang, L.-H.; Schwartz, R.E.; Li, B.; Bouklas, N.; Bowers, D.T.; An, D.; Cheong, S.H.; Flanders, J.A. Engineering transferrable microvascular meshes for subcutaneous islet transplantation. Nat. Commun. 2019, 10, 4602–4612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tomei, A.A.; Manzoli, V.; Fraker, C.A.; Giraldo, J.; Velluto, D.; Najjar, M.; Pileggi, A.; Molano, R.D.; Ricordi, C.; Stabler, C.L. Device design and materials optimization of conformal coating for islets of Langerhans. Proc. Natl. Acad. Sci. USA 2014, 111, 10514–10519. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schneider, S.; Feilen, P.J.; Slotty, V.; Kampfner, D.; Preuss, S.; Berger, S.; Beyer, J.; Pommersheim, R. Multilayer capsules: A promising microencapsulation system for transplantation of pancreatic islets. Biomaterials 2001, 22, 1961–1970. [Google Scholar] [CrossRef]
- Prausnitz, M.R.; Elias, P.M.; Franz, T.J.; Schmuth, M.; Tsai, J.-C.; Menon, G.K.; Holleran, W.M.; Feingold, K.R. Skin barrier and transdermal drug delivery. Dermatology 2012, 3, 2065–2073. [Google Scholar]
- Mitragotri, S.; Blankschtein, D.; Langer, R. Ultrasound-mediated transdermal protein delivery. Science 1995, 269, 850–853. [Google Scholar] [CrossRef]
- Di, J.; Price, J.; Gu, X.; Jiang, X.; Jing, Y.; Gu, Z. Ultrasound-triggered regulation of blood glucose levels using injectable nano-network. Adv. Healthc. Mater. 2014, 3, 811–816. [Google Scholar] [CrossRef] [Green Version]
- Di, J.; Yu, J.; Wang, Q.; Yao, S.; Suo, D.; Ye, Y.; Pless, M.; Zhu, Y.; Jing, Y.; Gu, Z. Ultrasound-triggered noninvasive regulation of blood glucose levels using microgels integrated with insulin nanocapsules. Nano Res. 2017, 10, 1393–1402. [Google Scholar] [CrossRef]
- Stanley, S.A.; Gagner, J.E.; Damanpour, S.; Yoshida, M.; Dordick, J.S.; Friedman, J.M. Radio-wave heating of iron oxide nanoparticles can regulate plasma glucose in mice. Science 2012, 336, 604–608. [Google Scholar] [CrossRef] [Green Version]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Insulin Variants | Onset of Action | Peak of Action | Duration of Action | References |
|---|---|---|---|---|
| Rapid-acting Insulin Lispro Aspart | 5–15 min | 1–2 h | 4–5 h | [10] |
| Short-acting Insulin Regular | 30–60 min | 2–5 h | 5–8 h | [8] |
| Intermediate-acting Insulin NPH | 1–2 h | 4–8 h | 10–20 h | [11] |
| Long-acting Insulin Detemir Glargine | 1–2h | Relatively flat | 14–24 h | [11] |
| Platforms for Carrying Insulin | Advantages | Disadvantages | References |
|---|---|---|---|
| Nano-scale carrier |
|
| [15,20,21,22,23,24,25,26,27,28,29,30] |
| Micro-scale carrier |
|
| [33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,50,51,52,53] |
| Microneedle |
|
| [54,55,56,57,58,59,60,61,62] |
| Glucose-Sensing Molecules | Advantages | Disadvantages | References |
|---|---|---|---|
| Glucose oxidase-based sensor | High glucose specificity | Slow response rates Susceptible to oxygen and pH fluctuations | [72,79] |
| Phenylboronic-based sensor | Structurally very versatile Rapid response rates High stability | Lack of glucose specificity | [90,91,92] |
| ConA or glucose binding protein sensor | High glucose specificity Rapid response rates | Instability Host immune response High cost | [83,84,87] |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Primavera, R.; Kevadiya, B.D.; Swaminathan, G.; Wilson, R.J.; De Pascale, A.; Decuzzi, P.; Thakor, A.S. Emerging Nano- and Micro-Technologies Used in the Treatment of Type-1 Diabetes. Nanomaterials 2020, 10, 789. https://doi.org/10.3390/nano10040789
Primavera R, Kevadiya BD, Swaminathan G, Wilson RJ, De Pascale A, Decuzzi P, Thakor AS. Emerging Nano- and Micro-Technologies Used in the Treatment of Type-1 Diabetes. Nanomaterials. 2020; 10(4):789. https://doi.org/10.3390/nano10040789
Chicago/Turabian StylePrimavera, Rosita, Bhavesh D Kevadiya, Ganesh Swaminathan, Rudilyn Joyce Wilson, Angelo De Pascale, Paolo Decuzzi, and Avnesh S Thakor. 2020. "Emerging Nano- and Micro-Technologies Used in the Treatment of Type-1 Diabetes" Nanomaterials 10, no. 4: 789. https://doi.org/10.3390/nano10040789