

Transitioning to Sustainable Healthcare: Decarbonising Healthcare Clinics, a Literature Review


Independent Researcher, Brisbane, Australia
Challenges 2022, 13(2), 68; https://doi.org/10.3390/challe13020068
Submission received: 27 October 2022
/
Revised: 8 December 2022
/
Accepted: 12 December 2022
/
Published: 19 December 2022
(This article belongs to the Special Issue Planetary Health: Building the Field and Growing the Movement (Including Manuscripts 2022 Planetary Health Annual Meeting and Festival))
Abstract
:Background: Climate change is one of the largest threats to human health and well-being globally. The healthcare industry itself currently contributes to fueling the climate crisis with its emissions and material consumption. There has been much research on decarbonising hospitals ecological/carbon footprints but very limited study on ways to assist healthcare clinics in transitioning to a low-carbon healthcare system. Methods: A structured literature review was conducted, and the results analysed. Results: The literature review revealed four important areas to act upon to decarbonise a healthcare clinic most efficiently. These are: energy use, waste minimisation/management, the behaviors/attitudes of staff, and decarbonising the supply chain. Conclusions: The pooled literature reveals an evidence-based set of recommendations or guiding principles to decarbonise healthcare clinics the most effectively. To maximise operational effectiveness, how this is achieved will differ between clinics. Although this research is written with reference to Australia, these identified ini-tiatives are likely to be relatable to many other countries healthcare systems. Decarbonising health clinics will contribute to a sector-wide transition to more sustainable healthcare that will lead to improved environmental, social, economic and health outcomes.
1. Introduction
Due to increasing pressures on the global biosphere, there is pressure for industry sectors to transition to more sustainable practices, to mitigate increasing adverse impacts on environmental and human health [1,2]. The health sector has a critical role to play, both in promoting awareness of the inextricable links between human and environmental health, and by reducing its own environmental impacts [3,4]. Historically, with a primary focus on human health, the healthcare sector has been less focused on environmental health, including its own substantial and rapidly increasing environmental footprint [2]. In the context of the Australian healthcare system, the goal of this paper is to provide an overview of healthcare’s impacts on, and the opportunities to contribute to the sustainability agenda, and to inform healthcare clinics of the most efficient means that they can decarbonise.
Although the healthcare sector is a critical service provider in every country including Australia, it possesses a substantial and growing environmental footprint due to a number of factors, including global population growth, ageing populations and the rise of increasingly energy and resource-intensive medical technologies [5]. As Australia is particularly vulnerable to the effects of climate change, decarbonising the healthcare sector would yield benefits to its residents as well as the wider environment [2,6].
More recently, momentum on this subject has been increasing with various healthcare organisations acknowledging the direct link between climate change and human health and publicly demanding emissions reduction [7]. A recent example is the prestigious international medical journal The Lancet publishing a report on the connection between health and climate change, with a subtitle of ‘code red for a healthy future’ [8]. In this unprecedented editorial re-published in more than 230 medical journals, it explains that human health is being harmed by climate change, and that the effects could become worse if governments do not do more to address it [9].
Within the Australian healthcare sector, hospitals account for the majority of CO2e emissions [5]. This is largely due to their high energy usage and single-use item policies [10]. General Practitioner (GP) clinics and other medical and allied health services contribute roughly 15% of total healthcare emissions [5]. Despite this relatively small percentage, it is still important to reduce these emissions and improve environmental performance if the entire healthcare sector is to decarbonise and transition to ‘net-zero’.
As hospitals are the largest emitters in the healthcare system, there has been considerable research on improving sustainability outcomes for them [11]. There have also been many studies that have analysed healthcare emissions, waste generation and ecological footprints from a hospital perspective [4,5]. These and other studies have provided evidence-based recommendations for how to transition/decarbonise to lower emissions and reduce hospitals’ environmental footprints [7,12,13].
On the other hand, there is currently fragmented literature on healthcare clinic sustainability transitions [5,14]. The World Health Organisation (WHO) has published an evidence-based guide for helping healthcare facilities become more environmentally sustainable, however, it is not specific to healthcare clinics, especially in a developed country [15]. Overall, there is little research that addresses specific actions, challenges and opportunities that healthcare clinics may need to consider when decreasing their ecological footprints [14]. Exploring the literature shows that there is a gap in addressing healthcare clinic decarbonisation.
For the purposes of this paper, the healthcare sector can be defined as the entities responsible for delivering services that improve, maintain or restore the health of individuals [16]. ‘Healthcare clinic’ will be considered any healthcare business that provides services via a registered healthcare professional and that is not a hospital. This includes but is not limited to: GP clinics, physiotherapy clinics, nutritionist/dietitian and exercise physiologist businesses, podiatry clinics, holistic healthcare centres, chiropractic clinics, specialist consulting rooms, dentists, pharmacies, community nurse clinics, etc. Gyms and spas will be excluded from the scope of this research as they do not typically employ registered health professionals.
2. Materials and Methods
Research Methodology
Research aims
The aim of this research is to identify progress on healthcare clinics’ engagement and contribution to the wider sustainability agenda through decarbonising their activities. The second aim is to review the most important factors identified in the literature to decarbonising healthcare clinics the most efficiently and how this fits into the context of the greater sustainability narrative. The final aim is to produce a practical, evidenced-based guide or set of recommendations for healthcare clinics to assist with transitioning their businesses.
Initial scoping research was undertaken. This was exploratory in nature to identify the current state of Australian healthcare clinic sustainability research and to identify if there was a gap in the literature on decarbonising healthcare clinics.
The initial scoping search was conducted using:
- Core electronic databases (ProQuest, Scopus)
- The Curtin Library Catalogue
- Google Scholar (example: healthcare AND sustainability AND Australia returned 43,000 results since 2010) (health business AND sustainability AND Australia AND footprint returned 160 results since 2010)
The main research comprised a structured literature review. This was approached with similar rigour and attention to bias as a systematic literature review. This was in part due to the research encompassing academic and non-academic (industry) sources, due to the cross-cutting nature of the topic [17]. Search terms can be found in Table 1.
Literature search limitations
- Articles in English
- Articles from 2010 onwards
- Priority given to Australian examples/case studies if many are found.
Structured literature search was performed in:
- Core electronic databases (Connected Papers, ProQuest, Espace, Trove, Annual Reviews, Scopus, and Web of Science for sustainability research)
- The Curtin Library Catalogue
- Google Scholar
Grey literature sources
- Health industry governing bodies, e.g., Australian Medical Association (AMA), etc
- NGO publications/reports including United Nations, Green and Healthy Hospitals (GGHH), Climate and Health Alliance (CAHA), etc.
Data analysis
As part of the qualitative analysis process, articles were read critically, summarised and then grouped thematically around the various aims of this research. Information was compared using textual and content analysis [18,19]. This identified patterns and trends seen across the articles to identify factors which play roles in healthcare clinic decarbonisation and the wider transition to sustainable healthcare.
3. Background
Climate change drivers and impacts on global health
The Intergovernmental Panel on Climate Change (IPCC) and the WHO both agree that climate change poses a considerable health threat [20,21]. Concurrently, recent systematic literature reviews have found that actions across sectors to mitigate climate change have significant positive health co-benefits [22,23]. A 2021 WHO report along with an open letter signed by more than 45 million health workers from 102 countries acknowledges the interconnection between human health, our environment and the climate crisis and calls for an immediate decarbonisation of various sectors globally including energy, healthcare, transportation and agriculture [24]. The report mentions that reducing air pollution and eating more plant-based diets would save millions of deaths per year by 2050 as well as reducing environmental damage and aiding the mitigation of climate change [24,25]. It states clearly that the public health benefits from implementing ambitious climate actions far outweigh the economic costs [25].
Human health is dependent upon the health of our greater environment [13,26]. A 2021 systematic review on the health effects of climate change concluded that climate change will worsen human health, mostly through increased infectious disease, higher mortality and respiratory issues (Figure 1) [27]. Climate change has proven links to heat deaths, dehydration and kidney function loss, skin cancer, tropical infections, mental health issues, pregnancy complications, increased allergies, and heart and lung disease [9]. Additionally, as humans continue to invade further into relatively untouched wild places causing habitat destruction and deforestation, zoonotic diseases (such as COVID-19) will only increase in frequency [9].
The climate crisis not only has impacts on human lives directly, but also has the potential to disrupt whole public health systems and overwhelm health services by increasing stress on them over time [7,12]. The IPCC’s 6th Assessment Report finds that effects on physical and mental health are likely to worsen with rising global temperatures [28]. In addition, the report finds that the underlying systems that allow healthcare systems to function (including ecosystems, food production systems and economic systems) are themselves under threat from not only many of the drivers of the climate crisis but climate change itself [28]. The report notes that for Australia specifically, there will be 20–70% more days over 35 °C by 2030, increasing the risk of heat-related illnesses. To note, these warnings in the literature were issued before a global virus pandemic that has further stressed health system resources.
The healthcare sectors environmental impacts on human health
The healthcare sector including healthcare clinics, when not designed and operated with sound sustainable principles in mind, produce negative environmental and subsequent health consequences for health workers and their communities [15]. Air pollution and subsequent health conditions from particulate matter produced from fossil fuel combustion that the healthcare sector uses for material goods and energy are the major cause of short to medium term health impacts, the same emissions then go on to contribute to climate change causing further longer-term health consequences [29]. For example, in 2013, the U.S. healthcare system emitted 613 million metric tons of CO2e projected to cause between 123,000 and 388,000 disability-adjusted life-years in future health damages [29].
Healthcare’s global emissions footprint
A 2019 report by Healthcare Without Harm (HCWH) provides a comprehensive global analysis of healthcare’s environmental footprint and contribution to climate change [2]. It includes data from 43 countries (developed and developing) and identifies the main sources of healthcare emissions [2]. The report’s key findings include that healthcare’s environmental footprint makes up 4.4% of global net emissions (if the health sector were a country, it would be the 5th largest CO2e emitter). Another study that undertook comprehensive analysis of the many facets of global healthcare’s environmental impact, including its supply chain estimates a global carbon footprint of a very similar 4.6% [30].
Sources of healthcare’s climate footprint vary, the main generators are from energy consumption, transport, and the supply chain for products [2]. Emissions originating directly from healthcare facilities and healthcare owned vehicles (Scope 1) make up 17% of the sector’s global footprint [2]. Indirect emissions from purchased energy (Scope 2) account for 12% [2]. The majority of emissions, 71%, are derived from the healthcare supply chain (Scope 3) through the production, transport, and disposal of products such as food, equipment and pharmaceuticals [2].
Australian healthcare’s emissions footprint
The Australian healthcare sector is responsible for 5.1–7% of total national greenhouse gas (GHG) emissions [2,5]. The increase compared to the global average is largely due to the carbon intensity of Australia’s energy grid and the large amounts of physical waste that is generated [2,5]. A comprehensive study by Malik et al. (2018) used lifecycle analysis to assess Australia’s healthcare systems’ emissions footprint (Figure 2). The study found that the largest emitters were: public hospitals 34%, pharmaceuticals 19%, and private hospitals 10% (Figure 2) [5]. General Practitioner (GP) clinics in Australia accounted for approximately 4%, however, when combined with other community health services this made up approximately 15% of total emissions [5]. Direct (scope 1) emissions made up 10% and indirect (scope 2 and 3 including supply chain) accounted for 90% of emissions [5].
Emissions from healthcare waste
Healthcare emissions from waste are discussed separately in this section as it is prominent in the literature and a major contributor to the sector’s emissions. In this research, waste is defined as physical waste, for example product packaging, discarded objects, and used anaesthetic gases. Wasted resources from unnecessary health services or overservicing are not included in this section of the paper.
Globally, the waste the healthcare sector generates contributes to a significant proportion of its emissions footprint and produces substantial volumes of toxic pollutants as well as GHG emissions [31,32]. The WHO estimates that over half the world’s population is at risk of negative health consequences of improperly treated healthcare waste [15]. The Australian healthcare sector is similar, producing a significant amount of waste, although it is unknown how much of this originates directly from healthcare clinics [33]. The majority of healthcare waste in Australia goes to landfill or is incinerated [31,33], which results in CO2e emissions and harmful air pollutants [34,35]. A growing number of healthcare workers are concerned about this, especially since COVID-19 has increased the amounts of healthcare waste [36].
Healthcare costs and decoupling
Health systems will suffer additional rising costs from the health impacts of increasingly frequent and severe weather events [2]. Improving the health sector’s sustainability outcomes, including decarbonising its operations, will make the health sector more resilient to these increasing costs and demands [2]. As an example of the interconnectedness between emissions and healthcare costs, research has estimated that the public health cost of the Australian 2019-20 bushfires (smoke-related health impacts alone), cost almost $2 billion [37]. The ‘Climate Change and Australia’s Healthcare Systems’ report, by the Royal Australasian College of Physicians (RACP) conservatively estimates that bushfires in Australia will kill 1000 people, cost the healthcare system $69 million and the greater economy $10 billion by 2030 [38]. Decreasing healthcare clinic emissions would play a part in decoupling the Australian healthcare system’s activities from its emissions [5].
4. Results
What hospitals are doing to decarbonise
There has been a significant amount of research and literature published regarding decarbonising hospitals. This includes the need for reducing ecological footprints, the economic, social, environmental co-benefits and in some cases details of how exactly to execute these changes [11,39]. It is useful to discus and draw on the relevant parts of this knowledge to assist healthcare clinics to decarbonise.
There is momentum for hospitals in Australia and globally to reduce their ecological footprint and to decarbonise [11]. An example is more than 3000 healthcare facilities (mostly hospitals), across 18 countries joining the U.N’s ‘Race to zero’ to halve emissions by 2030 and achieve net-zero emissions before 2050 [40]. Various Australian hospitals have announced plans and targets to significantly reduce their emissions [41]. Smaller healthcare clinics can learn from some of what hospitals are undertaking to decarbonise efficiently and transition to sustainable healthcare.
A systematic review of sustainability progress for hospitals has found that most hospitals are making efforts to reduce their emissions/environmental footprints, although, there is wide variability in the extent of this [39]. Common actions to decrease emissions include building more energy efficient hospitals, changing products to those that use less energy and/or water and recycling certain waste streams [39]. It is observed that less is known about the psychology of how hospital staff use resources and travel to/from hospitals and how this affects emissions reduction [39].
Common actions used in hospitals to reduce their emissions footprint successfully fall into eight areas: more environmentally sustainable (circular economy) waste management, low carbon pharmaceuticals (including their waste management), utilising renewable energy, net-zero health buildings, zero-emission transport, sustainable food, improving health sector effectiveness (preventative health), and decarbonising supply chains including decreasing single-use items and purchasing environmentally friendly products used in hospitals [42]. Many of these initiatives are able to be scaled down and applied to a healthcare clinic level.
A feature that has assisted hospitals to decarbonise is improved sustainability metric reporting [43]. This has meant that large healthcare facilities could track, measure and improve various environmental elements, such as tonnes of waste and estimated amounts of CO2e from electricity usage [44]. More widespread, standardised and mainstream measurements and reporting are needed to achieve net-zero efficiently [44]. Healthcare clinics would benefit from an agreed-upon similar set of metrics to record and compare progress.
The above mentioned initiatives all have positive effects on the environmental, social and economic aspects of sustainability, it is noted however, that clinical decision making and preventative health measures that avoid hospital procedures in the first place are likely to reduce far more emissions and avoid excess resource use than incremental changes to operational efficiency or technology in hospitals [39]. This is where healthcare clinics can also assist in reducing the need for patient hospitalisation.
What healthcare clinics can do to decarbonise
The literature review showed that there was far less research specifically on healthcare clinic decarbonisation or ecological footprint reduction. From the limited literature, there were specific themes that emerged on what healthcare clinics can do to reduce their emissions footprint most efficiently and decarbonise their business. Four important areas of action were revealed: energy, waste, behaviours/attitudes, and procurement/supply chain. A practical guide for healthcare clinics is presented in Appendix A. These topics are discussed in detail below.
Energy
Energy use in clinics can be reduced through energy efficiency measures and behaviour change [14]. Examples of behaviour or procedural changes include; turning off computer monitors overnight, turning off lights and machines when not needed, using low-power lighting and agreeing to run air-conditioning/heating at evidence-based, comfortable temperatures (this varies upon climate but on average for every 1 °C of extra heating or cooling, 10% more energy is used) [45,46]. Utilising fans in clinics can be an effective way of reducing the amount of air-conditioning energy used as fans have extremely low energy use compared to even the most efficient air-conditioners and can lower the ‘feels-like’ temperature of a room by 3 degrees [45]. Further efficiency improvements can come in the form of purchasing more energy and water-efficient appliances [46,47].
Changing to an energy retailer with a lower emissions profile is an action healthcare clinic owners can take to decrease their clinics footprint. Owners to choose a more environmentally efficient company via comparison websites, some even claim to be carbon neutral at no extra cost to the customer (by purchasing certified carbon credits) and owning or investing in renewable electricity generation themselves. If their clinic is located within a larger building complex, then this may not be an option.
For clinics that are not within a larger complex, installing solar on the roof will decrease electricity used from Australia’s fossil-fuel intensive grid and is an attractive economic choice as the clinic is using electricity predominantly during daylight hours, maximising the use of the self-generated energy. For owners of clinics inside larger buildings, lobbying the owner of the building to install panels (perhaps with other store owners as well) is one avenue they could pursue.
Transport for staff and patients to the clinic uses energy, typically fossil fuel-run private vehicles [46]. Conducting telehealth appointments means the patient and possibly the health professional do not need to travel physically to the clinic. Utilising telehealth where appropriate can add up to significant energy emissions reductions [48]. An example is at a pre-operative evaluation centre, that utilised telehealth appointments where appropriate and reduced the facilities CO2 emissions by 31% [48].
Waste
Reducing waste from a healthcare setting has been shown to be one of the more effective measures a facility can action to help decarbonise [42]. Waste reduction has a two-fold benefit to reducing emissions, consuming less material product uses less resources and energy, and less waste means less landfill or recycling processing emissions. Minimising waste needs both supply chain transition as well as operational/behaviour change [49]. The first step in the waste hierarchy is avoiding the item to begin with [50]. Transitioning to paperless offices is an example of avoiding paper use in the first place [14]. Sourcing items made of plastic-alternative materials such as bamboo or others that can be more easily broken down and reused is an effective next step [51]. Alternatively, buying items that are made from recycled plastic and that can be recycled themselves reduces overall waste and emissions [52]. Having clinic policies in place to re-use items where possible is more advantageous than recycling but if this is not possible then recycling is the next best action [50]. Separate bins need to be provided at convenient locations in the clinic and healthcare staff need to be trained to know what goes in each bin [53,54]. Paper, plastic and glass all have established recycling streams in Australia and should be accessible by all healthcare clinics [55]. Making staff aware of the bigger picture of healthcare waste can assist in staff compliance in appropriate waste management practices [11]. In an example of a health facility composting food waste, all coffee grounds were packaged and offered to employees for their gardens or used in the facility’s’ gardens [56]. Hazardous medical waste needs to be treated in line with industry standards and legislation.
Attitude/Behaviour change
Behaviour change and improved attitudes towards sustainability could be a powerful accelerator of the changes required to decarbonise health clinics. More positive attitudes towards decarbonisation would lead to the implementation of policies at a clinic level as well as drive change in other aspects, such as pressuring supply chains and energy companies to decarbonise [57]. Healthcare professionals report an overwhelming acknowledgement of the problem of climate change, however, there is an apparent barrier to action within health professionals’ clinical persona [58,59]. To address this, it has been found that in a healthcare setting, leadership and organisational change have been required for pro-environmental behaviour change [60]. A contributor to organisational change is effective education of staff which can move healthcare professionals from sustainability awareness and concern to motivation and action [59,61]. Healthcare clinics themselves may facilitate this education by allowing and subsidising staff to access or attend education opportunities with appropriate providers such as The Sustainable Healthcare Education network [62].
Sustainable procurement
Around 70% of the global health systems emissions are from their supply chain [2]. This means that making more environmentally sustainable choices when purchasing products can add up to large decreases in a health facility’s emissions footprint. Examples include selecting ‘green’ cleaning products (such as items that are plant-based, in reusable/recycled/recyclable containers), reducing the use of single-use items, purchasing items made from a plastic alternative and sourcing products from more local manufacturers [56].
Sustainable procurement in healthcare can result in multiple co-benefits including cost reductions through more efficient product use, improving the resilience of healthcare operations from international supply shocks and driving sustainable innovation from suppliers [63].
From a practical perspective, clinic managers that are ordering stock might ask of companies they buy from:
- Does the supplier have ISO 140001 accreditation? This is the international standard for having an environmental management system for the company. Accreditation indicates that the company approaches environmental issues seriously and that the environment need not be sacrificed for financial gain [64]
- Does the company publicise its sustainability targets or measures and/or have strong performance in relation to sustainability, and emissions, water, waste and energy reduction?
- Does the supplier have a strong reputation and performance on other ethical/CSR issues?
- Is the supplier local or Indigenous/community based?
- Does the companies supply chain adhere to The Modern Slavery Act 2018?
Adopting circular economy principles where applicable for the clinics’ supply chain would help to decarbonise the healthcare sector [65]. Improved supply chain resilience and decreased ecological footprints are just two benefits from incorporating circular economy principles, such as designing out waste and pollution, keeping products and materials in use, reducing single-use products and increased extended producer responsibility [65]. A clinic example is purchasing sterile examination gloves that are made from an alternative material to regular single-use gloves that can be re-made or sterilised and used again [49]. Another example in-line with circular economy principles relevant to a healthcare business would be to partner with a company that supplies uniforms, branded clothing and PPE (Personal Protective Equipment) as a service not as a product. This would mean that the company cleans and reuses these items (where appropriate) reducing overall material use and emissions [66].
Globally, the healthcare sector represents 10% of total GDP, in the US it accounts for 18% of GDP, this means it could be a powerful actor in accelerating low-carbon and sustainable supply chains [67]. If powerful, respected healthcare governing bodies (such as the Australian Medical Association) sent clear policy signals to product suppliers that they would be transitioning to purchasing goods with reduced footprints from companies that were taking measurable steps to lower their own ecological profiles, it would assist the entire sector to decarbonise their supply chain [67].
The physical healthcare building
Healthcare buildings and their operation over time are a significant contributor to the overall emissions of the healthcare sector [68]. Changes to the physical building itself are not included in the main four sections above as it is assumed most healthcare clinics in Australia are in rented premises, often part of a larger existing building, therefore are impractical to retrofit or renovate significantly to be more energy efficient. This factor is identified as a barrier to decarbonisation as improved healthcare building energy efficiency and more robust minimum standards to buildings are included in key policy change recommendations in the Climate and Health Alliance’s National Framework for Climate and Health Strategy [6]. Healthcare facilities rank second for energy use per area in the United States, however, only 1% of buildings are registered with the industry standard Leadership Energy Environment Design (LEED) ratings and only 0.4% are accredited, much lower than other building types (Zadeh, Xuan and Shepley 2016). An Australian example of a healthcare facility that is incorporating some sustainability features to reduce its operational lifetime emissions is a large new hospital in Adelaide which will be the first in Australia to be built with no gas connection [69].
The physical healthcare building also plays a key role in the resilience of the healthcare sector against more frequent and severe weather events [70]. Well-designed, low-emission, sustainable healthcare buildings are more energy and water-efficient, produce less waste and better able to continue to operate effectively for the community through periods of extreme heat, drought, storms, floods, and power outages [70]. Research does point out that even well-designed sustainable healthcare buildings need to be managed and staffed in the correct manner to provide optimal sustainability benefits [70].
5. Discussion
Barriers to healthcare clinic decarbonisation
Apart from the complexity of the healthcare system itself being identified as a barrier to decarbonisation [10], common themes that emerged from the literature for barriers to decarbonising healthcare clinics include: a lack of government policy on sustainability issues in healthcare, a lack of finances to spend on more expensive ecologically superior products and established supply chain companies that do not sell lower footprint products, social issues such as a general lack of awareness around sustainability, generally time-poor and un-trained staff, a lack of appropriate infrastructure and managerial workplace issues.
Lack of government leadership and systemic policy change to coordinate a decarbonisation transition is a barrier [6,58]. This includes a lack of regulation, incentives and specific policy targets or guidelines [71]. Australia has national targets for reducing CO2e emissions, yet the healthcare sector itself has no such targets [5]. An international example that could be implemented in Australia is from the United Kingdom, where the health sector’s carbon footprint is measured and must decline as part of a broader, nationwide economic effort to reduce CO2e emissions [5]. Even if sustainability laws exist, a lack of law enforcement and government support can lead to low adherence to sustainability practices [72]. This means if environmental health policy is introduced it would need to be enforced in certain ways. As mentioned earlier, with healthcare workers displaying a reluctance to action decarbonisation strategies in their professional lives (compared to their personal lives), support from professional associations and industry regulators would enable a transition to accelerate [58].
A lack of finances to spend on decarbonisation initiatives is a common barrier [71]. Higher upfront cost of a ‘environmentally friendly’ product compared to the status quo product is the most commonly cited financial supply chain barrier in the literature [72]. It is established that the healthcare sector’s historic focus on economic rationalism has been shown to be a barrier to environmentally responsible behaviour also [58]. As is the case throughout our society currently, the total resources needed to manufacture and ship these products are not taken into account by their price so there is little incentive for companies to change from making low-quality plastic items [1]. Some of the financial concern for clinic owners could be addressed by education on financial savings that sustainability initiatives (SI) can bring and explanation on pay-back periods for initiatives that do have an up-front cost.
Social factors such as a lack of awareness around healthcare sustainability, a lack of knowledge around broader sustainability issues are barriers to transition [58,61]. Healthcare workers have reported finding it difficult to identify the economic benefits to implement SI [72]. This lack of education/awareness of sustainability issues and also the underestimation of the severity of their impacts extends from healthcare sector workers to the general public [72]. The fact that evidence-based environmentally sustainable practices are not mainstream among all sectors is itself a barrier to change.
Staff who feel time poor is a barrier to clinic decarbonisation. In a 2021 international survey of health professionals, a lack of time was the top reason for them not doing more professionally about climate change [59]. Overriding strategies of how to decarbonise various healthcare clinics businesses may be useful in guiding owners on where they can make the largest impacts, however, this is where solutions that are unique to each clinic will play a role in ensuring operational efficiency as well as the desired emissions/waste reduction outcomes.
A lack of training has been commonly sighted as a barrier to transition [59,61]. If staff understand the benefits of environmental sustainability for policies and operational changes it is more likely they will be executed/actioned effectively [11]. Sustainability training makes healthcare staff feel like they are part of a team and help them feel involved in a bigger picture, this also helps action sustainability changes in healthcare facilities [11].
The absence of suitable infrastructure is another crucial barrier for decarbonisation [72]. This applies to healthcare clinics as most are without appropriate healthcare waste management systems, and experience a lack of recycling options for medical devices and equipment in terms of their reusability at end-of-life [72].
Managerial issues, including lacking management support for decarbonisation initiatives and employee resistance to change are recognised barriers [71,73]. Employees can be concerned that new decarbonisation procedures will make their role more difficult [73]. Within a workplace (including healthcare), employees’ moral responsibility is reduced, meaning they are less likely to demonstrate their own sustainability values in tasks at work [73]. This means that creating a positive workplace sustainability culture and communicating to the entire healthcare team the benefits of any decarbonisation initiative is useful to achieve long-term behaviour change and the desired emissions reduction [74].
Although a complex topic, there is an argument in the literature that in healthcare (as well as many other sectors), what ultimately drives SI is still traditional business-minded cost reduction and profit maximisation [73]. If we consider the barriers identified above, several of them are directly related to corporate culture or economic cost/savings. From this perspective, it will not be easy to transition to low emissions healthcare until it is cost-effective to do so.
Opportunities/benefits to clinic decarbonisation
Apart from healthcare clinic decarbonisation contributing to existing health sector sustainability transition frameworks [6,75], other opportunities were identified in the literature review. These include, improved healthcare practitioner sustainability education/awareness, possible financial co-benefits to the clinic and improved general healthcare-climate advocacy.
As clinic decarbonisation could include improving healthcare professionals sustainability education, it will enhance their awareness and care for patients with climate-related health issues [76]. Improving health professionals education on climate change, and decarbonisation would improve action for wider sustainability agenda transitions [59]. A 2021 study found that after a short formal climate-health course there were increases in health professional’s intentions to change personal behaviours and future clinical practice [77]. Examples of sustainability education that are relevant to healthcare clinics include the integration of indigenous health knowledge within global and public health modules and the role of the natural environment in healthcare [78].
Financial co-benefits are a potential benefit to clinic decarbonisation [79]. Literature was only found on hospital-scale financial savings rather than on a smaller clinic level, however, principles such as cost savings from reducing electricity consumption can be applied to a clinic level. Examples of financial benefit include data from 327 hospitals in the US that showed in 2019 they collectively saved $68 million (USD) using SI [80]. In 2018, SI in operating rooms alone saved a median $100,000 per facility [80]. More research on direct financial savings at a clinic level from decarbonisation actions is needed.
An opportunity that may be enhanced by clinic decarbonisation is for healthcare professionals to become more prominent public leaders in climate change mitigation and adaptation. As the climate crisis is a major public health issue, healthcare professionals could advocate for environmentally sustainable change within the healthcare industry [13,59]. Healthcare professionals could lobby Governments directly on climate-health policy, they could communicate the health risks of climate change to the media and public and decarbonise their own clinics or facilities [59]. In a society where public trust in governments and experts is declining, health professionals remain highly trusted, this makes it more imperative that health professionals communicate the need for decarbonising our economy including the health sector [6,67].
Decarbonising healthcare clinics—The broader context
While conducting this literature review, several ‘bigger picture’ issues relating to the interconnectedness of healthcare, sustainability and the climate crisis were mentioned repetitively in the research. Several of them relevant to healthcare clinics and their future are important to discuss.
Increasing the effectiveness of preventative healthcare results in direct health and climate benefits including improving public health, costing taxpayers less in health spending and reduced emissions from the healthcare sector [5,23]. Plainly, the less people need to access healthcare services the less resources the sector will use. To find ways to use less resources is a base sustainability principle [81], which for the healthcare sector may be challenging to achieve when the Australian population is becoming increasingly ill and needing to access more health services [5,82].
Many industries are interconnected in wider preventative health. An example is populations consuming unhealthy food, beverages and tobacco (that all create emissions along their production path) that result in poor health requiring increased access to healthcare services which in turn increases healthcare consumption of products and creates further emissions [83]. In another example, in the US, more than 50% of healthcare resources are used on 5% of patients for chronic disease management, with the vast majority of these conditions being lifestyle and behaviour based and therefore almost completely preventable [75]. When added to the fact that globally, only 20% of people’s health and well-being is contributed to by the health sector (the other 80% is due to social, environmental and economic factors), it is clear that focusing on preventative healthcare is an efficient pathway to decarbonising the health sector [75]. As the major healthcare emissions sectors are hospitals and pharmaceuticals (in supply chain), there is an opportunity for healthcare clinics to act as community preventative healthcare actors to decrease the need for these more emissions intensive healthcare services [5].
A straightforward explanation of this principle in action comes from the dental world. In a case study of two 50-year-old individuals, patient A presents for a routine dental check up with no active oral disease and good oral health. Patient B presents with poor oral health, active oral disease, and tooth loss. Patient A has accessed effective preventative oral care through their life, practices good hygiene and makes positive lifestyle choices, this results in a much lower lifetime dental emissions profile with reduced physical travel to appointments and not needing resource intensive dental procedures [84]. Patient B has been on a very different oral health journey, with societal and behavioural factors playing a role in reduced preventative care and poor lifestyle choices resulting in a much higher dental emissions profile [84]. This highlights the interlinkages across sectors in society that can add up to increasing a person’s resource use in many sectors including their healthcare [84].
Where appropriate, when hospital-based care is not essential, community-based interventions mare be more desirable from both a patient care standpoint and an emissions standpoint. Clinic-based treatments such as Allied Health services are especially ‘low-emission’ and are often an effective non-pharmaceutical means to remedy pain and disfunction while encouraging positive long-term health measures such as increased exercise and reduced obesity [78]. Reducing pharmaceutical use and diagnostic imaging is especially efficient at decarbonising healthcare [10]. Healthcare clinics are well placed to provide evidence-based care while, where appropriate, reduce the need for higher emission treatment.
Another large issue that is related is notion of ‘low value’ healthcare. A recent Australian study points out that ’low-value’ and even ’harmful’ healthcare creates unnecessary emissions (Figure 3) [85]. Low-value care is difficult to define as it varies across health disciplines significantly but one example is ordering unnecessary pathology tests [85]. Out of the 80 million pathology tests ordered in Australia in 2020, between 10 and 40% of them were likely unnecessary [85]. Educating healthcare practitioners about ‘low-value’ care and concurrently about decarbonising healthcare could be effective means to reduce emissions [85].
Major transformational policy change is argued to be needed for truly transitioning to sustainable healthcare. Policy changes need to be interconnected to existing policies across different government departments and could include areas such as prioritising preventative health, ecosystem conservation for health, health disaster preparedness, and education and research (Figure 4) [6]. Policy changes that include healthcare supply chain may also include, mandatory life-cycle assessments of all medical items and pharmaceuticals, application of standardised sustainability performance metrics at the clinician, health facility and health sector levels, and revision of infection control standards driving non-evidence-based uptake of single-use disposable devices [86].
As part of a larger sustainability picture, finding the funds for increased healthcare spending as well as how our wider economic systems operate in reference to healthcare are practical discussion points. Current economic models often neglect to consider the significant intergenerational costs and negative impacts of emissions, resource use and pollution from the healthcare sector [1]. Although possible solutions to this are complex, some of the leading health and climate experts have called for an effective economy-wide carbon price to simultaneously achieve improvements in human health and the wider climate crisis [26]. Funding national, evidence-based preventative health campaigns have been shown to be cost effective but for complex reasons are politically difficult to execute [87]. The literature also points out that the world is spending trillions of dollars to restore the economy from the COVID-19 pandemic, but less than one in five of those dollars is expected to be used towards reducing greenhouse gas emissions, which would be an effective way of mitigating climate change as well as improving health outcomes [3]. Research has shown that the costs of emissions reduction in line with the Paris Agreement (0.5–1.3% of global GDP) are far outweighed by the health co-benefits in even the most conservative modelling [88]. According to a 2021 Lancet journal report, 65 out of 84 of the world’s most polluting countries subsidize a median of $1 billion to fossil fuel companies annually, money that could be better spent protecting and improving public health [9]. Similarly, according to research conducted by the International Monetary Fund (IMF), on average, globally, for every $1 a Government subsidies to fossil fuel companies, $10 worth of health costs are created [89]. This adds to the burden of disease and disability globally [89]. In an Australian context, in 2020-2021 the Australian Government subsidised fossil fuel companies to the tune of $10.3 billion [90]. This is essentially creating a significant amount of unnecessary health spending in an already stressed healthcare system.
The resilience of healthcare systems will be further tested as weather events become more frequent and severe (e.g., Australia’s ‘1-in-100 year floods’ could occur several times a year by 2050 [28,91]). Climate resilient healthcare systems are interconnected with public infrastructure resilience, and the physical healthcare facilities resilience [91]. To function effectively in an environment exposed to more frequent and severe extreme weather and more common and serious supply chain disruptions, healthcare systems need to leverage their political and social power [91]. Healthcare industries and governing bodies need to engage in a coordinated, systematic way with the community, decision makers and business partners to improve education, awareness and population health to attain improved healthcare resilience [91]. An example is lobbying Government for funds to install solar and battery power generation systems on healthcare facilities that can be run as backup power if needed, and floodproofing road and footpath infrastructure for improved access to a facility [15].
There are bigger picture issues surrounding healthier behaviour change. As mentioned, behaviour change toward more environmentally sustainable thinking is one of the key criteria needed to decarbonise healthcare clinics. Healthy behaviour change may also promote a global transition to a low emission, healthier planet as behaviours that favour improved health often include wider environmental and social benefits [92]. The WHO Global Action Plan for Physical Activity (2018–2030) notes that promoting physical activity will contribute to achieving 13 of the 17 SDG’s [93]. Driving less is another example, as it reduces emissions, improves personal health, improves air quality and improves community health [92].
In the broader context, a final point to discuss is how this studies findings compare to and compliment the WHO’s guide on assisting healthcare facilities to become more environmentally sustainable and climate resilient. Similarities include stating that sustainable procurement, waste minimisation and management and energy efficiency measures are key attributes to decarbonising healthcare facilities as well as making them more resilient to increasing climate related threats [15]. This study also agrees with the guide, mentioning that the various recommendations will need to be actioned in a flexible, specific way to suit the circumstances of individual healthcare facilities. Differences include a focus on healthcare clinics having an adequate municipal water supply, having adequate wastewater and sanitation facilities and reducing exposure to harmful chemicals in a healthcare setting [15]. These differences are partially due to the WHO’s report being pitched at all scales of healthcare facilities, including large hospitals, as well as taking into account healthcare facilities (including clinics) in developing countries where issues such as water and sanitation are more of an environmental sustainability concern than a country such as Australia [15]. Overall, this study compliments the WHO’s broader guide as it includes many of the same evidence-based over-arching principles healthcare clinics need to address to decarbonise, such as energy, waste and supply chain, but adds developed-country health clinic specifics to the data so more specific recommendations may be drawn.
6. Conclusions
The health sector is responsible for a considerable percentage of global (and Australian) emissions [2]. This contributes negatively to the health of the very people this industry serves [12]. Emissions are predominantly created through scope three/supply chain emissions and the majority are from hospitals [2]. The health sector also produces significant volumes of waste which contributes to harming populations and is not in line with international net-zero targets [94]. There is already considerable research on reducing hospital ecological footprints. There is far less research on decarbonising healthcare clinics [14].
From the literature, the common themes that emerged on what healthcare clinics can focus on to reduce their emissions footprint most efficiently are: energy, waste, behaviours/attitudes, and procurement/supply chain. The most popular topics that emerged from the literature for barriers to decarbonising healthcare clinics include: a lack of government policy on sustainability issues in healthcare, a lack of availability and the higher price of ecologically superior products, social issues such as a general lack of awareness around sustainability, a lack of appropriate infrastructure and managerial workplace issues. Important themes identified in the research for opportunities and benefits for clinic decarbonisation include improved sustainability education/awareness and possible financial co-benefits.
Through reviewing the literature, several complex, global challenges emerged that relate to decarbonising healthcare clinics. These included improving preventative health, transitioning economic systems to account for negative environmental externalities and the need to improve the resilience of entire healthcare sectors.
The Royal Australasian College of Physicians recommend the health sector reach net-zero by or before 2040 [38]. This includes healthcare clinics. Healthcare clinics have an opportunity and a responsibility to decarbonise and transition to more sustainable healthcare. Improved individual and population health, economic factors, social factors, and environmental effects are all outcomes of this pathway.
Funding
This research received no external funding.
Acknowledgments
The author wishes to thank and acknowledges the support and assistance from Dora Marinova and Curtin University.
Conflicts of Interest
The author declares no conflict of interest. To the best of the authors knowledge and belief this paper contains no material previously published by any other person except where due acknowledgment has been made. There was no funding of any kind involved in the creation of this paper.
Appendix A. Evidence-Based Recommendations or Guide to Assist Healthcare Clinics to Decarbonise
Initiation
First learn about decarbonising a healthcare clinic. Research healthcare clinic emissions reduction, there are many helpful resources that may be relevant to your industry/clinic circumstance. Then, appoint a passionate and educated “sustainability champion” in your healthcare team to implement, monitor and drive sustainability initiatives. Facilities with a passionate person driving transition are more likely to achieve sustainability outcomes.
Energy
Know your recent electricity usage and cost. If your circumstances allow, switch your electricity provider to one committed to decarbonisation that offers certified carbon offsetting and owns or invests in renewable energy generation.
Promote the benefits of using active transport, public transport and car-pooling/community cars to your staff/patients.
Supply Chain
This is the section of healthcare that contributes more emissions than any other. Audit clinic supplies, consumables, and sellable items. Possible criteria to track: percentage of products that do not contain plastic or are made of recycled plastic, the percentage of products that come in sustainable packaging. Alternatively, a traffic light system of green for products that exemplify sustainability, yellow for items that have some element of decarbonisation (e.g., the company selling it is trying to decrease their footprint), and red for products that make no attempt in reducing their environmental impact. You then have a base line of how your supply chain is performing.
Next, try and source items that have less plastic, higher percentages of recycled and recyclable material in the product and packaging. Try and source local products. Tell suppliers that you want these items compared to others. Make sure they are competitively priced. Express concern if not to pressure suppliers.
Waste
Try and reduce the amount of physical material that comes into your clinic. Supply appropriately sized bins at convenient areas of the clinic and train team members to recycle and compost (if appropriate in your clinics situation). Consider alternatives to single use items where appropriate.
Behaviour Change
Let your team know that the clinic will be reducing its carbon/ecological footprint, stress that this is evidence-based, will help save the clinic money, will improve the health for all staff and patients, will help the broader community in various ways and will not take up more of their time once procedures are set up.
Introduce operational procedure change after consulting staff to make them part of the solutions, highlight the simplicity, and benefits of each change. Examples include turning off electronic equipment overnight, lights when not in the room and not printing unless necessary.
Support/Learning
Complete a relevant health professional specific sustainability/climate education program, encourage and enable staff to do the same. Join relevant industry sustainability groups for support, answers to questions, and ideas. Enquire about industry standard metrics you can be monitoring so your decarbonisation efforts can be more easily quantifiable. Communicate with your health clinic’s professional governing body and ask what they are doing to support your profession to decarbonise.
Progress Monitoring
Monitor results, electricity bills, number of bags or waste to landfill bins, etc. Keep track of how much money you save each month and as this grows think about spending it on more expensive sustainability initiatives. An example is if you need to replace an old appliance, buy a high energy and water efficiency star model from a company dedicated to reducing its own footprint. If you own the building then other measures such as insulation, double glazing or solar panels could be applicable to your circumstance.
Celebrate and publicise successes. Emphasise that what you are achieving is creating a healthier community for your patients. Your website, social media and local news publications are all good avenues. This improves your reputation and trust with the community. You can inspire and motivate systemic change if others see your success/progress.
References
- Sachs, J.D.; Kroll, C.; Lafortune, G.; Fuller, G.; Woelm, F. Sustainable Development Report 2021; Cambridge University Press: Cambridge, UK, 2021. [Google Scholar]
- Karliner, J.; Slotterback, S.; Boyd, R.; Ashby, B.; Steele, K. Health Care’s Climate Footprint; Health Care Without Harm and ARUP: London, UK, 2019. [Google Scholar]
- Ebi, K.; Campbell-Lendrum, D.; Wyns, A. The 1.5 Health Report. 2018. Available online: http://climate.mohp.gov.np/downloads/The_1.5_health_Report.pdf (accessed on 2 February 2022).
- Karliner, J.; Slotterback, S.; Boyd, R.; Ashby, B.; Steele, K.; Wang, J. Health care’s climate footprint: The health sector contribution and opportunities for action. Eur. J. Public Health 2020, 30 (Suppl. S5), ckaa165-843. [Google Scholar] [CrossRef]
- Malik, A.; Lenzen, M.; McAlister, S.; McGain, F. The carbon footprint of Australian health care. Lancet Planet. Health 2018, 2, e27–e35. [Google Scholar] [CrossRef] [Green Version]
- Climate and Health Alliance CAHA. Healthy, Regenerative and Just, Framework for a National Strategy on Climate, Health and Well-being for Australia; Climate and Health Alliance: Melbourne, Australia, 2021. [Google Scholar]
- Salas, R.N.; Maibach, E.; Pencheon, D.; Watts, N.; Frumkin, H. A pathway to net zero emissions for healthcare. BMJ 2020, 371, m3785. [Google Scholar] [CrossRef]
- Romanello, M.; McGushin, A.; Di Napoli, C.; Drummond, P.; Hughes, N.; Jamart, L.; Kennard, H.; Lampard, P.; Rodriguez, B.S.; Arnell, N. The 2021 report of the Lancet Countdown on health and climate change: Code red for a healthy future. Lancet 2021, 398, 1619–1662. [Google Scholar] [CrossRef]
- Atwoli, L.; Baqui, A.H.; Benfield, T.; Bosurgi, R.; Godlee, F.; Hancocks, S.; Horton, R.; Laybourn-Langton, L.; Monteiro, C.A.; Norman, I. Call for emergency action to limit global temperature increases, restore biodiversity, and protect health: Wealthy nations must do much more, much faster. Nutr. Rev. 2021, 79, 1183–1185. [Google Scholar] [CrossRef]
- Australia DftE. Net Zero Carbon Emissions: Responsibilities, Pathways and Opportunities for Australia’s Healthcare Sector; Doctors for the Environment Australia: Melbourne, Australia, 2020. [Google Scholar]
- Lewis, T.M.A. Becoming a Climate-Friendly Hospital: Implications for Nursing Practice within the Australian Healthcare Context. 2018. Available online: https://ro.uow.edu.au/theses1/275/ (accessed on 23 January 2022).
- Watts, N.; Amann, M.; Arnell, N.; Ayeb-Karlsson, S.; Belesova, K.; Berry, H.; Bouley, T.; Boykoff, M.; Byass, P.; Cai, W. The 2018 report of the Lancet Countdown on health and climate change: Shaping the health of nations for centuries to come. Lancet 2018, 392, 2479–2514. [Google Scholar] [CrossRef]
- Eckelman, M.J.; Sherman, J.D.; MacNeill, A.J. Life cycle environmental emissions and health damages from the Canadian healthcare system: An economic-environmental-epidemiological analysis. PLoS Med. 2018, 15, e1002623. [Google Scholar] [CrossRef] [Green Version]
- Fathy, R.; Nelson, C.A.; Barbieri, J.S. Combating climate change in the clinic: Cost-effective strategies to decrease the carbon footprint of outpatient dermatologic practice. Int. J. Women’s Dermatol. 2021, 7, 107. [Google Scholar] [CrossRef]
- WHO. WHO Guidance for Climate Resilient and Environmentally Sustainable Health Care Facilities; Report No.: 9240012222; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- WHO. Health Systems: WHO Europe. 2022. Available online: https://www.euro.who.int/en/health-topics/Health-systems (accessed on 27 March 2022).
- Franklin, A.; Blyton, P. Researching Sustainability: A Guide to Social Science Methods, Practice and Engagement; Routledge: London, UK, 2013. [Google Scholar]
- McKee, A. Textual analysis. In The Media & Communications in Australia; Routledge: London, UK, 2020; pp. 31–42. [Google Scholar]
- Kyngäs, H. Qualitative Research and Content Analysis. In The Application of Content Analysis in Nursing Science Research; Springer: Geneva, Switzerland, 2020; pp. 3–11. [Google Scholar]
- WHO. Compendium of WHO and Other UN Guidance on Health and Environment; World Health Organization: Geneva, Switzerland, 2021. [Google Scholar]
- IPCC; Rogelj, J.; Shindell, D.; Jiang, K.; Fifita, S.; Forster, P.; Ginzburg, V.; Handa, C.; Kheshgi, H.; Kobayashi, S.; et al. Summary for Policymakers. In: Global Warming of 1.5 °C. An IPCC Special Report on the Impacts of Global Warming of 1.5 °C Above Pre-industrial Levels and Related global Greenhouse Gas Emission Pathways, in the Context of Strengthening the Global Response to the Threat of Climate Change, Sustainable development, and Efforts to Eradicate Poverty. 2018. Available online: https://www.ipcc.ch/sr15/ (accessed on 14 December 2021).
- Deng, H.-M.; Liang, Q.-M.; Liu, L.-J.; Anadon, L.D. Co-benefits of greenhouse gas mitigation: A review and classification by type, mitigation sector, and geography. Environ. Res. Lett. 2018, 12, 123001. [Google Scholar] [CrossRef] [Green Version]
- Gao, J.; Kovats, S.; Vardoulakis, S.; Wilkinson, P.; Woodward, A.; Li, J.; Gu, S.; Liu, X.; Wu, H.; Wang, J. Public health co-benefits of greenhouse gas emissions reduction: A systematic review. Sci. Total Environ. 2018, 627, 388–402. [Google Scholar] [CrossRef]
- Prescription, H.C. An Urgent Call for Climate Action from the Health Community Ahead of COP26. Available online: https://healthyclimateletter.net/ (accessed on 25 October 2021).
- WHO. WHO’s 10 Calls for Climate Action to Assure Sustained Recovery from COVID-19 World Health Organization. 2021. Available online: https://www.who.int/news/item/11-10-2021-who-s-10-calls-for-climate-action-to-assure-sustained-recovery-from-covid-19 (accessed on 25 October 2021).
- Al-Delaimy, W.; Ramanathan, V.; Sánchez Sorondo, M. Health of People, Health of Planet and Our Responsibility: Climate Change, Air Pollution and Health; Springer Nature: Geneva, Switzerland, 2020. [Google Scholar]
- Rocque, R.J.; Beaudoin, C.; Ndjaboue, R.; Cameron, L.; Poirier-Bergeron, L.; Poulin-Rheault, R.-A.; Fallon, C.; Tricco, A.C.; Witteman, H.O. Health effects of climate change: An overview of systematic reviews. BMJ Open 2021, 11, e046333. [Google Scholar] [CrossRef] [PubMed]
- IPCC. 6th Assessment Report (Working Group II) Climate Change 2022: Impacts, Adaptation and Vulnerability; IPCC: Geneva, Switzerland, 2022. [Google Scholar]
- Eckelman, M.J.; Huang, K.; Lagasse, R.; Senay, E.; Dubrow, R.; Sherman, J.D. Health Care Pollution And Public Health Damage In The United States: An Update: Study examines health care pollution and public health damage in the United States. Health Aff. 2020, 39, 2071–2079. [Google Scholar] [CrossRef]
- Lenzen, M.; Malik, A.; Li, M.; Fry, J.; Weisz, H.; Pichler, P.-P.; Chaves, L.S.M.; Capon, A.; Pencheon, D. The environmental footprint of health care: A global assessment. Lancet Planet. Health 2020, 4, e271–e279. [Google Scholar] [CrossRef] [PubMed]
- Chauhan, A.; Singh, A. Healthcare waste management: A state-of-the-art literature review. Int. J. Environ. Waste Manag. 2016, 18, 120–144. [Google Scholar] [CrossRef]
- Howard Frumkin, M. Health Care Waste and Climate Change. Am. J. Public Health 2021, 111, E15. [Google Scholar] [CrossRef] [PubMed]
- Hames, K. Healthcare waste disposal: An analysis of the effect of education on improving waste disposal. Healthc. Infect. 2013, 18, 110–114. [Google Scholar] [CrossRef]
- Honest, A.; Manyele, S.; Saria, J.; Mbuna, J. Assessment of air pollutant emissions from healthcare waste incinerators of different design features. Afr. J. Environ. Sci. Technol. 2020, 14, 311–328. [Google Scholar]
- Thakur, V.; Ramesh, A. Healthcare waste management research: A structured analysis and review (2005–2014). Waste Manag. Res. 2015, 33, 855–870. [Google Scholar] [CrossRef]
- Terzon, E. Australia’s Healthcare Industry Battling ‘Devastating’ Level of Waste, Nurses and Doctors Say: Australian Broadcasting Company (ABC). 2019. Available online: https://www.abc.net.au/news/2019-07-13/war-on-waste-hospital-waste-australia-recycling/11306376 (accessed on 25 October 2021).
- Mazengarb, M. Australia’s Public Health Already Being Hit by Climate Change, Professionals Say. Renew Economy. 2021. Available online: https://reneweconomy.com.au/australias-public-health-already-being-hit-by-climate-change-professionals-say/ (accessed on 4 October 2021).
- Smith, R. Australia, a Laggard in Responding to Climate Change, Produces an Impressive Report on Climate Change and Health; British Medical Journal Publishing Group: London, UK, 2021; Volume 375. [Google Scholar]
- McGain, F.; Naylor, C. Environmental sustainability in hospitals–a systematic review and research agenda. J. Health Serv. Res. Policy 2014, 19, 245–252. [Google Scholar] [CrossRef]
- Nations, U. Health Institutions Join the United Nations Race to Zero Campaign United Nations. 2021. Available online: https://unfccc.int/news/health-institutions-join-the-united-nations-race-to-zero-campaign (accessed on 31 October 2021).
- Green and Healthy Hospitals GGaH. About GGHH, (Members around the World Section). 2022. Available online: https://greenhospitals.org/about (accessed on 18 February 2022).
- Holzmueller, C.G. How Health Care Organizations Can Reduce Their Carbon Footprint. Qual. Manag. Healthc. 2021, 30, 46–48. [Google Scholar] [CrossRef]
- Tennison, I.; Roschnik, S.; Ashby, B.; Boyd, R.; Hamilton, I.; Oreszczyn, T.; Owen, A.; Romanello, M.; Ruyssevelt, P.; Sherman, J.D. Health care’s response to climate change: A carbon footprint assessment of the NHS in England. Lancet Planet. Health 2021, 5, e84–e92. [Google Scholar] [CrossRef] [PubMed]
- Hensher, M.; McGain, F. Health Care Sustainability Metrics: Building A Safer, Low-Carbon Health System: Commentary examines how to build a safer, low-carbon health system. Health Aff. 2020, 39, 2080–2087. [Google Scholar] [CrossRef] [PubMed]
- Australian Government Department of Industry; Energy and Resources Household. Heating and Cooling. 2021. Available online: https://www.energy.gov.au/households/heating-and-cooling (accessed on 4 November 2021).
- Doctor, M.G. My Green Doctor. 2022. Available online: https://mygreendoctor.org (accessed on 4 November 2021).
- Rehr, R.; Perkowitz, R. Moving Forward: A Guide for Health Professionals to Build Momentum on Climate Action; Eco America, Climate for Health: San Fransisco, CA, USA, 2019. [Google Scholar]
- Wang, E.Y.; Zafar, J.E.; Lawrence, C.M.; Gavin, L.F.; Mishra, S.; Boateng, A.; Thiel, C.L.; Dubrow, R.; Sherman, J.D. Environmental emissions reduction of a preoperative evaluation center utilizing telehealth screening and standardized preoperative testing guidelines. Resour. Conserv. Recycl. 2021, 171, 105652. [Google Scholar] [CrossRef]
- Skoog, M.; Backman, A. Replacing Waste Streams in the Healthcare Industry by Applied Technology: Developing Technology for a Circular Economy. 2020. Available online: https://www.diva-portal.org/smash/record.jsf?pid=diva2%3A1440290&dswid=8477 (accessed on 17 January 2022).
- Gertsakis, J.; Lewis, H. Sustainability and the waste management hierarchy. Retrieved Jan. 2003, 30, 2008. [Google Scholar]
- Shafqat, A.; Tahir, A.; Mahmood, A.; Tabinda, A.B.; Yasar, A.; Pugazhendhi, A. A review on environmental significance carbon foot prints of starch based bio-plastic: A substitute of conventional plastics. Biocatal. Agric. Biotechnol. 2020, 27, 101540. [Google Scholar] [CrossRef]
- Zheng, J.; Suh, S. Strategies to reduce the global carbon footprint of plastics. Nat. Clim. Change 2019, 9, 374–378. [Google Scholar] [CrossRef]
- Andrews, A.; Gregoire, M.; Rasmussen, H.; Witowich, G. Comparison of recycling outcomes in three types of recycling collection units. Waste Manag. 2013, 33, 530–535. [Google Scholar] [CrossRef] [Green Version]
- Rosenthal, S.; Linder, N. Effects of bin proximity and informational prompts on recycling and contamination. Resour. Conserv. Recycl. 2021, 168, 105430. [Google Scholar] [CrossRef]
- Australian Government DoA, Water and Environment. Investing in Australia’s Waste and Recycling Infrastructure. Available online: https://www.awe.gov.au/environment/protection/waste/how-we-manage-waste/recycling-modernisation-fund (accessed on 10 November 2021).
- Kinney, L.M. Environmental sustainability in healthcare. J. Qual. Particip. 2010, 33, 23. [Google Scholar]
- Hedlund-de Witt, A.; De Boer, J.; Boersema, J.J. Exploring inner and outer worlds: A quantitative study of worldviews, environmental attitudes, and sustainable lifestyles. J. Environ. Psychol. 2014, 37, 40–54. [Google Scholar] [CrossRef]
- Dunphy, J.L. Healthcare professionals’ perspectives on environmental sustainability. Nurs. Ethics 2014, 21, 414–425. [Google Scholar] [CrossRef] [PubMed]
- Kotcher, J.; Maibach, E.; Miller, J.; Campbell, E.; Alqodmani, L.; Maiero, M.; Wyns, A. Views of health professionals on climate change and health: A multinational survey study. Lancet Planet. Health 2021, 5, e316–e323. [Google Scholar] [CrossRef] [PubMed]
- Wilson, D. Recycling and Environmental Sustainability In the New Zealand Healthcare Setting: A Practice-led Case Study Research-Project; Auckland University of Technology: Auckland, New Zealand, 2020. [Google Scholar]
- Climate and Health Alliance CAHA. Real, Urgent & Now, Insights from Health Professionals on Climate and Health in Australia; Climate and Health Alliance: Melbourne, Australia, 2021. [Google Scholar]
- Walpole, S.C.; Barna, S.; Richardson, J.; Rother, H.-A. Sustainable healthcare education: Integrating planetary health into clinical education. Lancet Planet. Health 2019, 3, e6–e7. [Google Scholar] [CrossRef] [PubMed]
- Greenhealth, P. Sustainable Procurement Guide. 2021. Available online: https://practicegreenhealth.org/sustainableprocurementguide (accessed on 23 October 2021).
- Compliance Council. ISO 14001 Environmental Management System. 2022. Available online: https://www.compliancecouncil.com.au/standards/iso-14001-environmental-management-system (accessed on 12 March 2022).
- Ritchie, N.H. Leadership for a Climate Resilient, Net-Zero Health System: Transforming Supply Chains to the Circular Economy; Healthcare Management Forum; SAGE Publications: Los Angeles, CA, USA, 2021. [Google Scholar]
- Guldmann, E. Best Practice Examples of Circular Business Models; Danish Environmental Protection Agency: Copenhagen, Denmark, 2016. [Google Scholar]
- Healthcare WIthout Harm HCWH. 2020 Annual Report HCWH. 2020. Available online: https://noharm-uscanada.org/sites/default/files/documents-files/6649/HCWH-AnnualReport%20011221-digital_0.pdf (accessed on 1 November 2021).
- Zadeh, R.S.; Xuan, X.; Shepley, M.M. Sustainable healthcare design: Existing challenges and future directions for an environmental, economic, and social approach to sustainability. Facilities 2016, 34, 264–288. [Google Scholar]
- Parkinson, G. Look, No Gas! South Australia to Build Country’s First All-Electric Hospital Renew Economy. 2021. Available online: https://reneweconomy.com.au/look-no-gas-south-australia-to-build-countrys-first-all-electric-hospital/ (accessed on 3 November 2021).
- Corvalan, C.; Villalobos Prats, E.; Sena, A.; Campbell-Lendrum, D.; Karliner, J.; Risso, A.; Wilburn, S.; Slotterback, S.; Rathi, M.; Stringer, R. Towards Climate Resilient and Environmentally Sustainable Health Care Facilities. Int. J. Environ. Res. Public Health 2020, 17, 8849. [Google Scholar] [CrossRef]
- Alshehri, A. Advancing Sustainability: Environmental Health and Institutional Change in Healthcare Facilities; State University of New York, College of Environmental Science and Forestry: New York, NY, USA, 2016. [Google Scholar]
- Kazançoğlu, Y.; Sağnak, M.; Lafcı, Ç.; Luthra, S.; Kumar, A.; Taçoğlu, C. Big data-enabled solutions framework to overcoming the barriers to circular economy initiatives in healthcare sector. Int. J. Environ. Res. Public Health 2021, 18, 7513. [Google Scholar] [CrossRef]
- Rodriguez, R.; Svensson, G.; Høgevold, N.M.; Eriksson, D. Factors and determinants of value-and business-driven sustainability initiatives in health care organizations: Intrinsic differences and extrinsic similarities. Corp. Gov. Int. J. Bus. Soc. 2019, 19, 806–823. [Google Scholar] [CrossRef]
- Manika, D.; Gregory-Smith, D.; Wells, V.K.; Comerford, L.; Aldrich-Smith, L. Linking environmental sustainability and healthcare: The effects of an energy saving intervention in two hospitals. Int. J. Bus. Sci. Appl. Manag. 2017, 11, 32–55. [Google Scholar]
- Sherman, J.D.; McGain, F.; Lem, M.; Mortimer, F.; Jonas, W.B.; MacNeill, A.J. Net zero healthcare: A call for clinician action. BMJ 2021, 374, n1323. [Google Scholar] [CrossRef]
- Dzau, V.J.; Levine, R.; Barrett, G.; Witty, A. Decarbonizing the US Health Sector—A Call to Action. N. Engl. J. Med. 2021, 385, 2117–2119. [Google Scholar] [CrossRef]
- Gomez, J.; Goshua, A.; Pokrajac, N.; Erny, B.; Auerbach, P.; Nadeau, K.; Gisondi, M.A. Teaching medical students about the impacts of climate change on human health. J. Clim. Change Health 2021, 3, 100020. [Google Scholar] [CrossRef]
- Maric, F.; Chance-Larsen, K.; Chevan, J.; Jameson, S.; Nicholls, D.; Opsommer, E.; Perveen, W.; Richter, R.; Stanhope, J.; Stone, O. A Progress Report on Planetary Health, Environmental and Sustainability Education in Physiotherapy–Editorial; Taylor & Francis: London, UK, 2021. [Google Scholar]
- Bressler, R.D. The mortality cost of carbon. Nat. Commun. 2021, 12, 4467. [Google Scholar] [CrossRef] [PubMed]
- Practice Greenhealth. 2019 Sustainability Data. 2021. Available online: https://practicegreenhealth.org/tools-and-resources/2019-sustainability-data (accessed on 23 October 2021).
- Wheeler, S.M. Theory of Sustainability Planning. In Planning for Sustainability: Creating Livable, Equitable and Ecological Communities; Routledge: London, UK, 2013; pp. 34–52. [Google Scholar]
- Australian Bureau of Statistics, A. Health Conditions and Risks. 2021. Available online: https://www.abs.gov.au/statistics/health/health-conditions-and-risks (accessed on 16 March 2022).
- Aldakhil, A.M.; Nassani, A.A.; Abro, M.M.Q.; Zaman, K. Food-beverage-tobacco consumption, smoking prevalence, and high-technology exports influenced healthcare sustainability agenda across the globe. Environ. Sci. Pollut. Res. 2018, 25, 33249–33263. [Google Scholar] [CrossRef] [PubMed]
- Martin, N.; Mulligan, S. Environmental sustainability through good-quality oral healthcare. Int. Dent. J. 2021, 72, 26–30. [Google Scholar] [CrossRef] [PubMed]
- Barratt, A.L.; Bell, K.J.; Charlesworth, K.; McGain, F. High value health care is low carbon health care. Med. J. Aust. 2021, 216, 67–68. [Google Scholar] [CrossRef]
- Sherman, J.D.; Thiel, C.; MacNeill, A.; Eckelman, M.J.; Dubrow, R.; Hopf, H.; Lagasse, R.; Bialowitz, J.; Costello, A.; Forbes, M. The green print: Advancement of environmental sustainability in healthcare. Resour. Conserv. Recycl. 2020, 161, 104882. [Google Scholar] [CrossRef]
- White, P.; Skirrow, H.; George, A.; Memon, A. A systematic review of economic evaluations of local authority commissioned preventative public health interventions in overweight and obesity, physical inactivity, alcohol and illicit drugs use and smoking cessation in the United Kingdom. J. Public Health 2018, 40, e521–e530. [Google Scholar] [CrossRef] [Green Version]
- Markandya, A.; Sampedro, J.; Smith, S.J.; Van Dingenen, R.; Pizarro-Irizar, C.; Arto, I.; González-Eguino, M. Health co-benefits from air pollution and mitigation costs of the Paris Agreement: A modelling study. Lancet Planet. Health 2018, 2, e126–e133. [Google Scholar] [CrossRef] [Green Version]
- Health and Environment Alliance HaE. Fossil Fuel Subsidies and Health; The Health and Environment Alliance: Brussels, Belgium, 2017. [Google Scholar]
- Campbell, R.; Littleton, E.; Armistead, A. Fossil Fuel Subsidies in Australia: The Australian Institute. 2021. Available online: https://australiainstitute.org.au/report/fossil-fuel-subsidies-in-australia/ (accessed on 12 March 2022).
- Healthcare Without Harm HCWH. Climate Resilience for Health Care and Communities; 2022. Available online: https://noharm-uscanada.org/sites/defult/files/documents-files/7024/Climate-Resilience-for-Health-Care-and-Communities-Stratigies-and-Case-Studies.pdf (accessed on 9 March 2022).
- Palstam, A.; Andersson, M.; Lange, E.; Grenholm, A. A Call to Include a Perspective of Sustainable Development in Physical Therapy Research. Phys. Ther. 2021, 101, pzaa228. [Google Scholar] [CrossRef]
- WHO. More Active People for a Healthier World. Global Action Plan on Physical Activity 2018–2030; World Health Organization: Geneva, Switzerland, 2018. [Google Scholar]
- Government, V. Waste Victoria Health. 2012. Available online: https://www2.health.vic.gov.au/hospitals-and-health-services/planning-infrastructure/sustainability/waste (accessed on 21 November 2021).
Figure 1.
Impact of climate change on human health [2] (Original source: U.S. Centres for Disease Control and Prevention).
Figure 1.
Impact of climate change on human health [2] (Original source: U.S. Centres for Disease Control and Prevention).

Figure 2.
The proportion of CO2e emissions from the various categories of the Australian healthcare sector, 2014-15. (Malik, Lenzen, McAlister, McGain. Lancet Planetary Health 2018; 2:27–35).
Figure 2.
The proportion of CO2e emissions from the various categories of the Australian healthcare sector, 2014-15. (Malik, Lenzen, McAlister, McGain. Lancet Planetary Health 2018; 2:27–35).

Figure 3.
The carbon footprint of Australian health care and the share of its carbon emissions attributable to harmful, low value and effective care. (CO2e—Carbon Dioxide Equivalent). Source: [85] originally from [5]).

Figure 4.
Key areas of health policy action. From: Healthy, Regenerative and Just, Framework for a National Strategy on Climate, Health and Well-being for Australia. Climate and Health Alliance (CAHA) 2021.
Figure 4.
Key areas of health policy action. From: Healthy, Regenerative and Just, Framework for a National Strategy on Climate, Health and Well-being for Australia. Climate and Health Alliance (CAHA) 2021.


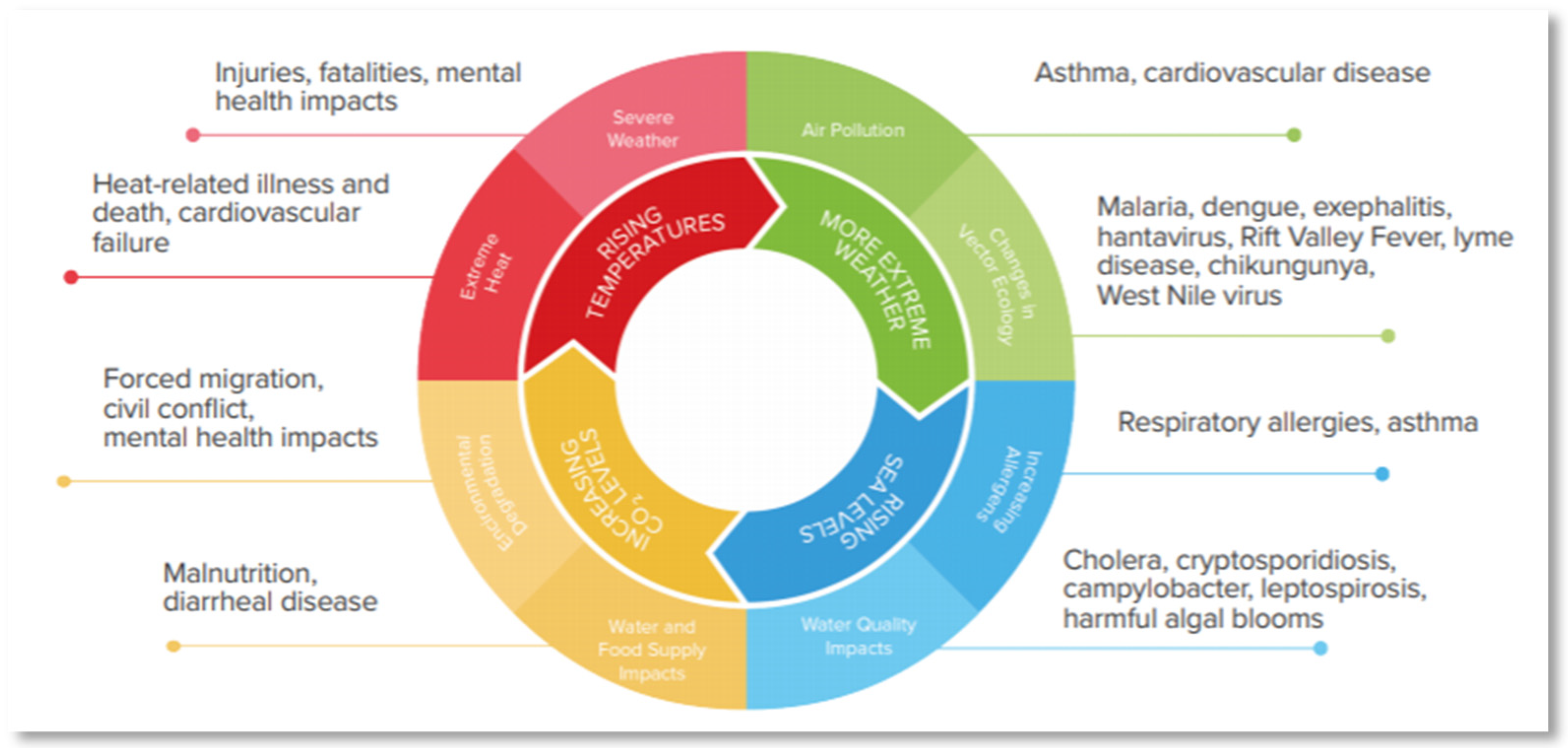{kind=link}
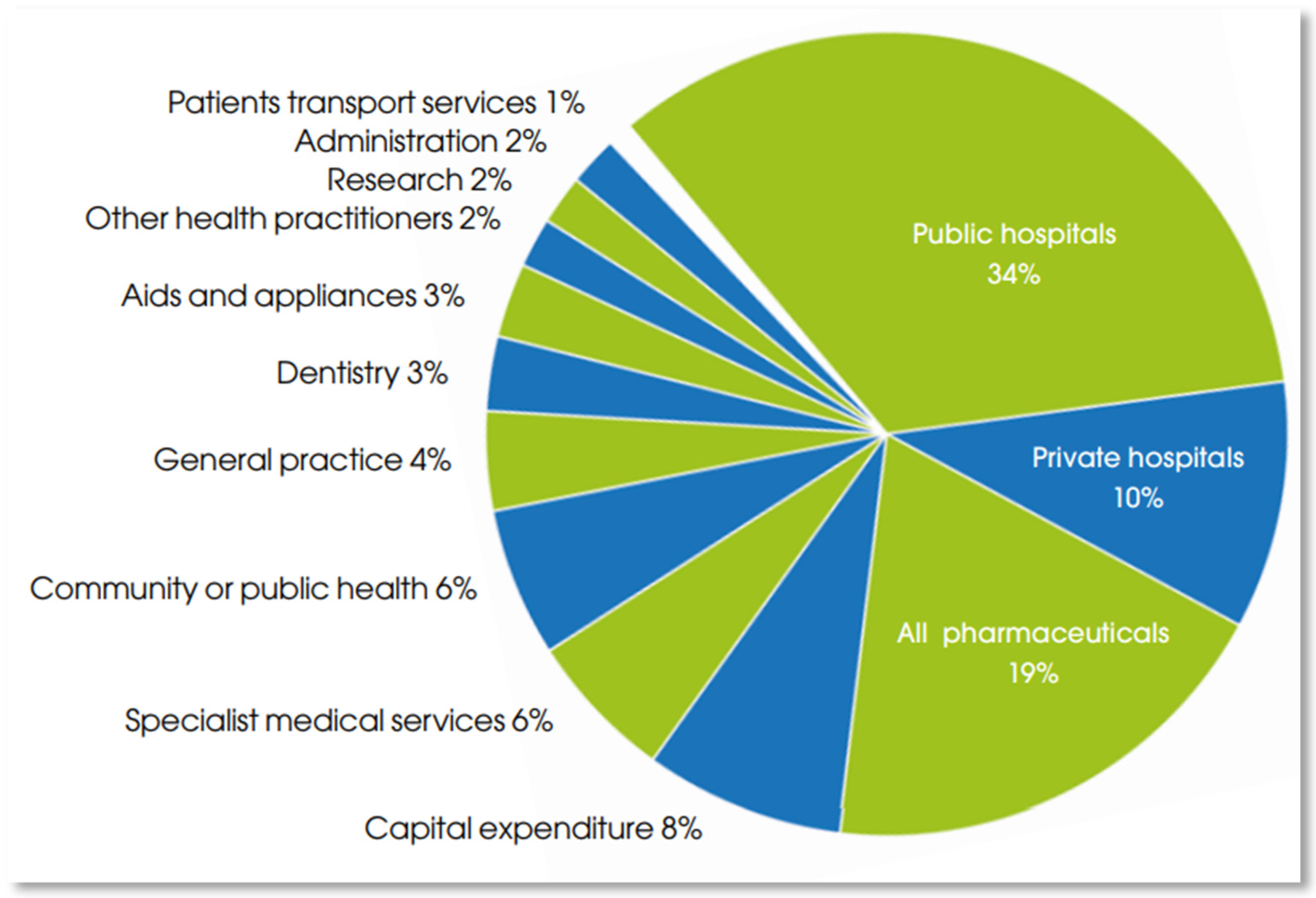{kind=link}
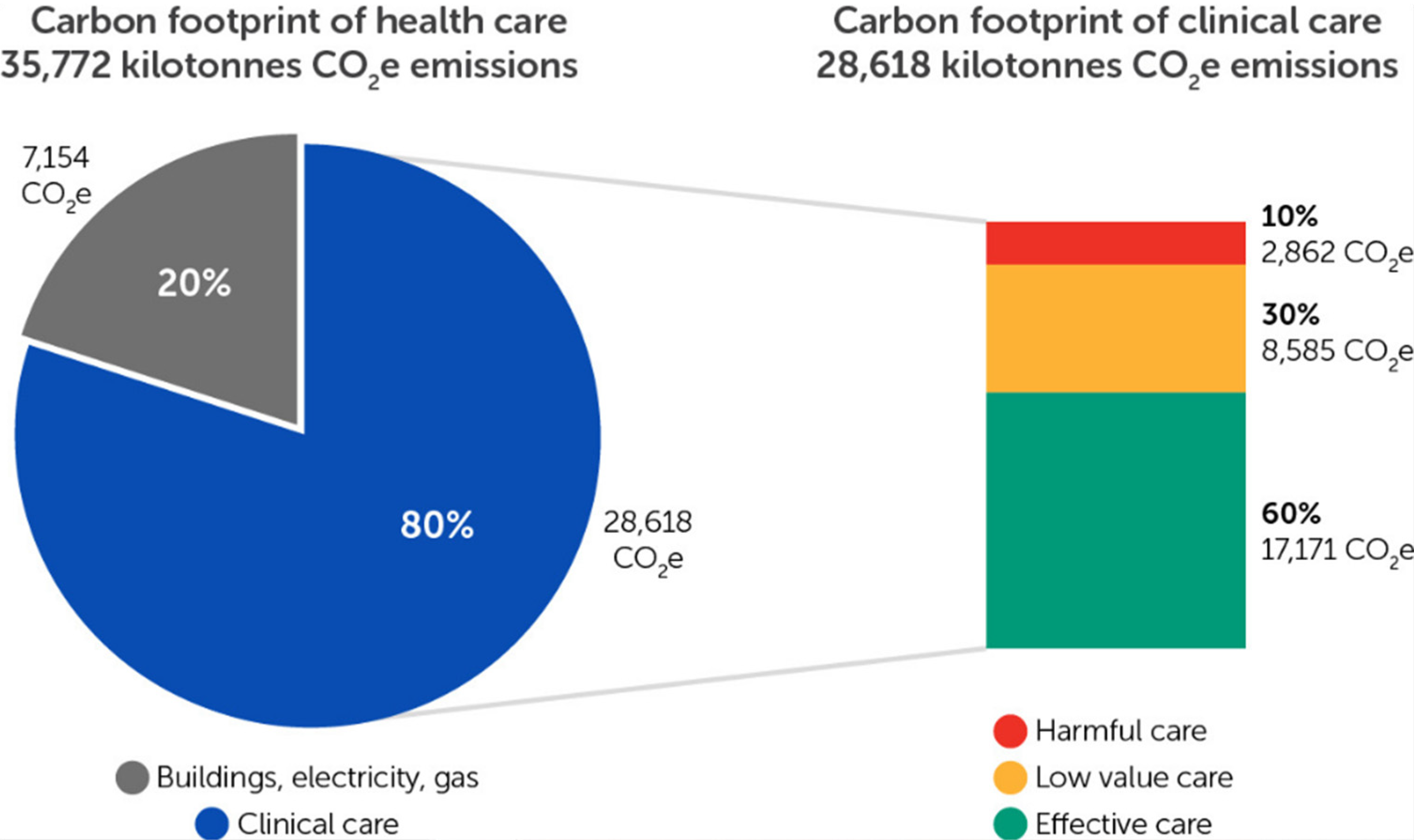{kind=link}
{kind=link}
Table 1.
Search terms used to conduct the structured literature review.
| Industry | Sustainability | Emissions | Waste |
|---|---|---|---|
| Health business | Ecological footprint/footprint | Carbon footprint | Waste |
| Small health business | Sustainability/Sustainab * | CO2 | Single use |
| Health clinic | Decarbonisation/Decarbon * | Pollution | |
| Healthcare, Health care | Net Zero, Net-Zero | Emissions | |
| Allied Health | Circular economy | ||
| Challenges/opportunities | Environment * |
* Means the program will search for that word with any ending.
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Duindam, D. Transitioning to Sustainable Healthcare: Decarbonising Healthcare Clinics, a Literature Review. Challenges 2022, 13, 68. https://doi.org/10.3390/challe13020068
AMA Style
Duindam D. Transitioning to Sustainable Healthcare: Decarbonising Healthcare Clinics, a Literature Review. Challenges. 2022; 13(2):68. https://doi.org/10.3390/challe13020068
Chicago/Turabian StyleDuindam, David. 2022. "Transitioning to Sustainable Healthcare: Decarbonising Healthcare Clinics, a Literature Review" Challenges 13, no. 2: 68. https://doi.org/10.3390/challe13020068
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.