High-Rise Apartments and Urban Mental Health—Historical and Contemporary Views

 , ,
, ,
Abstract
:1. Introduction
1.1. History
1.2. Living Conditions
2. The Contribution of Stress and Social Well-Being to Mental Health Problems
2.1. Stress and Mental Health
2.2. Mental Health and High-Rise Living
2.2.1. Floor Level
2.2.2. Street and Surroundings
2.3. Thematic Review
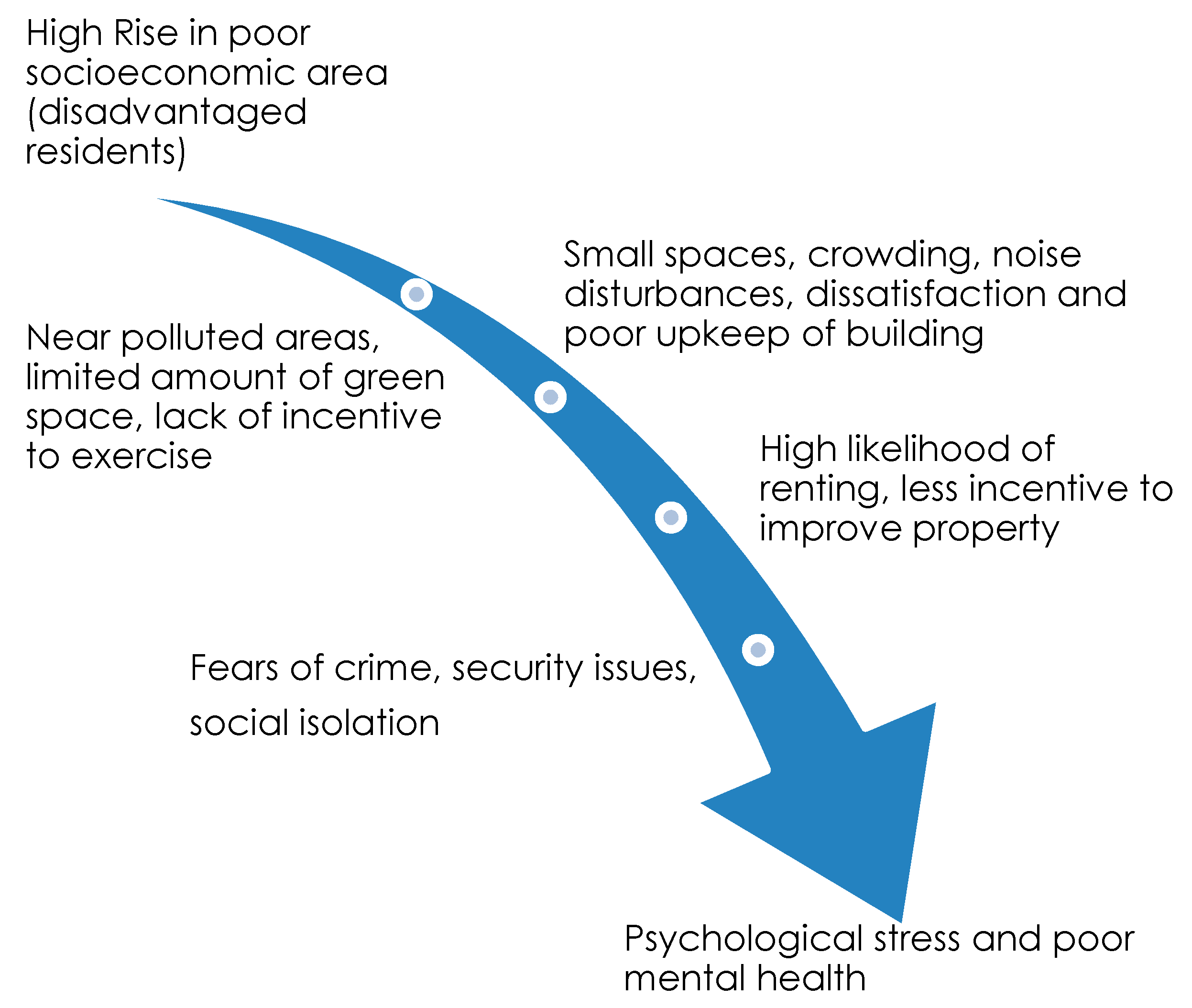
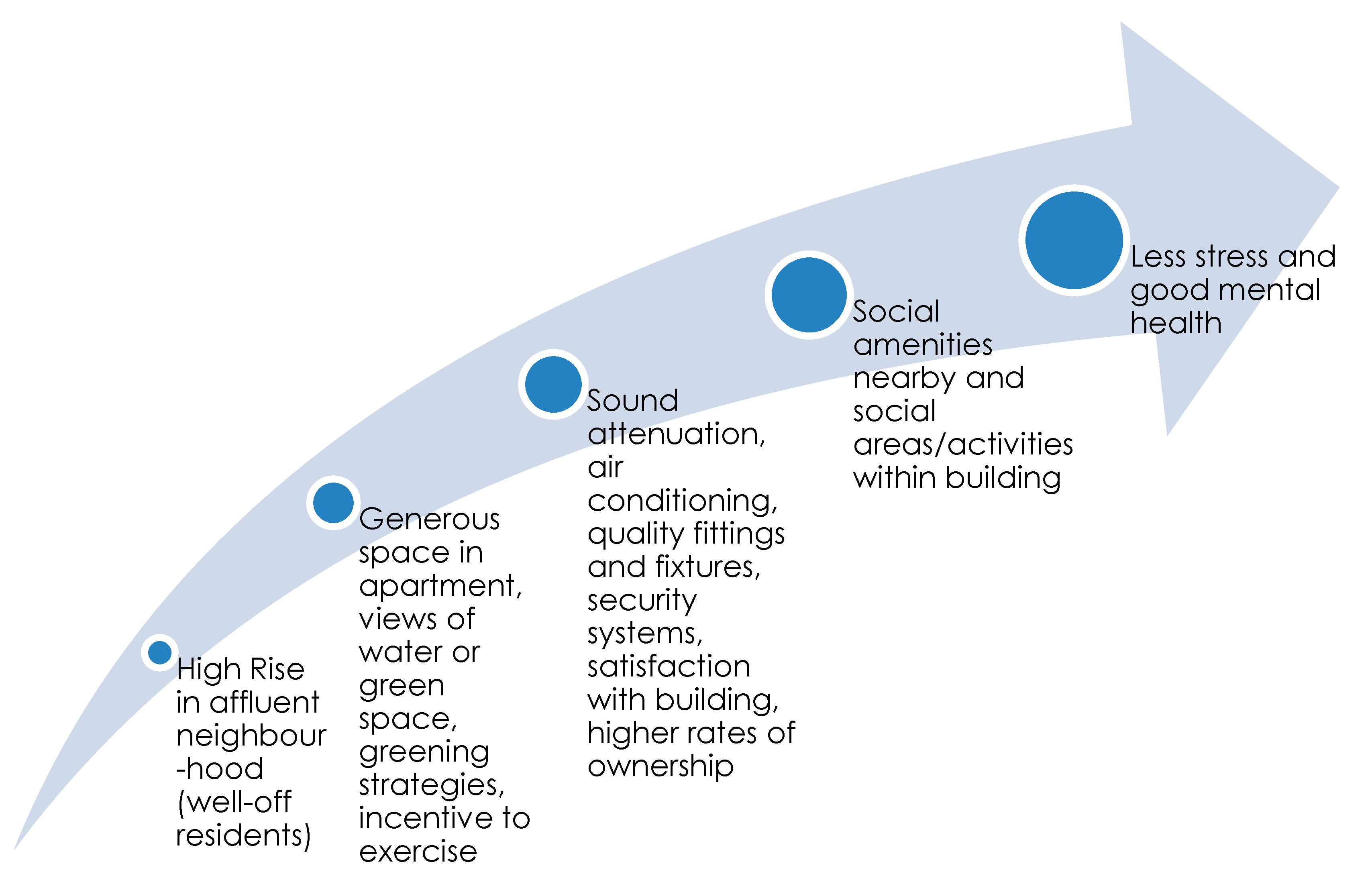
3. Proposed Causal Sequences
4. Housing Interventions to Increase Wellbeing
4.1. Relocation
4.2. Green Space
5. Further Research
6. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Appendix A. Investigation of Literature

{kind=link}
{kind=link}
| A GRADE | B GRADE | C GRADE | D GRADE |
|---|---|---|---|
| contains a comparison between high-rise and low-rise | contains a comparison between high-rise and mid-rise | contains a comparison between high-rise floor levels | contains high-rise data only |
| Reference and Study Design | Grade | Sampling Method | Type of Housing | Subject’s Age, Gender and Ethnicity | Number of People | Health Specialty | Findings of Note |
|---|---|---|---|---|---|---|---|
| [41] Random Assignment | A | Doctor’s Records | Flats vs. houses | Women with medical issues (first consults) from the United Kingdom/Canada | 1500 | Mental/Psychoneurotic | Social isolation of women in flats |
| [53] Cross-sectional | A | Survey | High-rise vs. low-rise | Public housing residents (United States) | 915 | Alienation | Significantly higher levels of alienation in high rise buildings |
| [54] Cross-sectional | A | Survey | High-rise vs. two stories with a garden | Women (United Kingdom) | 69/43 | Neuroticism and Medical Doctor (MD) visits | House dwellers had fewer neurotic scores and fewer visits to MD with nervous disorders |
| [56] Cross-sectional | A | Survey | High-rise vs. low-rise v. houses | Women (United Kingdom) | 75 | Psychological problems | More loneliness and depression complaints from women in high-rises |
| [55] Cross-sectional | A | Survey | Flats vs. houses | British and Canadian servicemen’s wives | 169 | Depression | Women living in houses had less depression than those living in flats |
| [45] Cross-sectional | A | Survey | Flats vs. houses | British and Canadian servicemen’s wives | 167/167 | Psychiatric illness | Neurotic personalities living in flats more likely to experience psychiatric illness than stable personalities in flats. No similar difference in house dwellers |
| [42] Cross-sectional | A, C | Psychiatric Screening Survey | High-rise Floor 5+ v. Floors 1–4 vs. detached homes | Random adults from a health centre (Glasgow, Scotland) | 964 | Mental symptoms | People on the 5th floor or above had twice the number of mental symptoms as those on lower floors (or in other types of housing) |
| [48] Cross-sectional | A | Survey | High-rise vs. low-rise dormitories | Students (2nd-year freshmen) in the United States | 110 | Social interaction/social support | High rise dwellers found to have less social support and less socially involved |
| [43] Cross-sectional | A, C | Survey | Eight types of public housing Inc. high-rise | Public housing residents, Canada | 442 | Psychological strain | Floor level predicts higher levels of emotional strain for women |
| [49] Cross-sectional | A | Survey | High-rise vs. detached homes | Canada | 87 | Social interaction | Residents of detached homes had more contact with neighbours |
| [50] Random assignment | A | Survey | High-rise (14 stories) vs. low-rise (three stories) | Adults, mostly of Puerto Rican or African American descent | 60 | Psychological distress, social support | Greater social overload, less social networks, less attachment to the community |
| [13] Longitudinal | A | Survey | High-rise vs. detached homes | Women | Unknown | Depression | Fewer symptoms of depression after moving out of high-rise |
| [59] Cross-sectional | A | Survey | Multi-family dwellings vs. single family dwellings. | Canadian families | 560 | Psychiatric problems | More psychiatric problems amongst men in multi-family housing, no difference in women |
| [37] Cross-sectional | D | Self-reported survey | Eight types of housing area | Adults, local authority housing, United Kingdom | 674 (383 households) | Psychological distress | Symptoms most prevalent in ‘difficult to let’ housing—location rather than type |
| [51] Cross-sectional | A | Survey | High-rise vs. low-rise owned apartments | Women, Israel | 344 | Social interaction | High-rise dwellers encountered more people, and more who were strangers |
| [57] Cross-sectional | A | Survey | High-rise vs. detached homes | Elderly men and women, South Africa | 600 | Psychological distress | High rise residents in low SES areas experienced more psychological distress |
| [52] Cross-sectional | A, B | Survey | High-rise v. mid-rise vs. low-rise | Adults, children and elderly, China | 503 | Mental health | More social contact with neighbours in low rise v. mid-rise and high-rise |
| [58] | D | Survey | High-rise | Elderly men, India | 100 | Mental health | Residents failed to cope with the stress produced by living in high-rise buildings |
| [47] Cross-sectional | A | Survey | High-rise vs. detached homes | Adults in four socio-economically disadvantaged sites in Melbourne, Australia | 1199 | Perceptions of neighbourhood factors that influence health | Residents of high-rise towers were more likely than other residents to nominate proximal aspects of the neighbourhood as having a perceived negative influence on health. |
| [60] Random Assignment | A | Interview | High-rise vs. detached homes | Gautreaux Program—Mothers and children, Chicago, United States | 100 | Sense of efficacy (control) | Residents who moved out of high-rises into detached homes reported a greater sense of efficacy including freedom from fear. |
| [18] Cross-sectional | A | Survey with interview | 14 social housing areas, high-rise to low-rise | Glasgow, United Kingdom | 1392 high rise/1848 houses | Residential, social, psychosocial | Poor social outcomes in high rise flats (for all factors), some psychosocial outcomes worse in high rise flats. |
| [28] Cross-sectional | A, C | Survey | High-rise of four floors and above, Comparison of floors 1–15 | Census data, Switzerland | 1,500,015 (160,629 high rise buildings) | Mortality | Mortality from all causes higher in ground floor dwellers. Suicide by jumping increased on higher floors at a rate of 0.41%. |
| [40] Cross-sectional | D | Self-reported Survey. Interview, Focus Groups | High-rise | Auckland, New Zealand | 429 Surveys, 30 interviews, four focus groups | Social isolation | The experience and expression of social isolation was consistent across all age groups, with highest correlation between functional social isolation and “being student”, and older adults (60+ years), length of tenure in current apartment and length of time residents have lived in the inner-city. |
| [44] Cross-sectional | A | Self-reported Survey | High-rise vs. low-rise | Census data and Belgium Register, Belgium | 2,998,227 Male 3,104,593 Female | Self-rated health | Residents’ worse self-rated health in high-rise buildings can be explained by the strong demographic and socioeconomic segregation between high- and low-rise buildings in Belgium. A weak, but robust positive curvilinear relationship between floor level and self-rated health within high-rise buildings. |
References
- Gifford, R. The Consequences of living in high-rise buildings. Archit. Sci. Rev. 2007, 50, 2–17. [Google Scholar] [CrossRef]
- Mridha, M. Living in an apartment. J. Environ. Psychol. 2015, 43, 42–54. [Google Scholar] [CrossRef]
- Goldenhagen, S.W. Sarah Williams Goldhagen on Architecture: Living High. Available online: https://newrepublic.com/article/103329/highrise-skyscraper-woha-gehry-pritzker-architecture-megalopolis (accessed on 20 July 2019).
- Gellman, E. Robert Taylor Homes. In The Electronic Encyclopedia of Chicago; University of Chicago Press: Chicago, IL, USA, 2005. [Google Scholar]
- Flanagan, S. Black Men March for Peace in one of America’s Most Violent Housing Projects. JET, 2 May 1994. [Google Scholar]
- Wener, R.; Carmalt, H. Environmental psychology and sustainability in high-rise structures. Technol. Soc. 2006, 28, 157–167. [Google Scholar] [CrossRef]
- Nethercote, M.; Horne, R. Ordinary vertical urbanisms: City apartments and the everyday geographies of high-rise families. Environ. Plan. A 2016, 48, 1581–1598. [Google Scholar] [CrossRef]
- The History of Sydney: Inter-War Architecture. Available online: http://www.visitsydneyaustralia.com.au/history-11-interwar.html (accessed on 20 July 2019).
- Roodman, D.M.; Lenssen, N.K.; Peterson, J.A. A Building Revolution: How Ecology and Health Concerns Are Transforming Construction; Worldwatch Institute: Washington, DC, USA, 1995. [Google Scholar]
- Fincher, R. Is high-rise housing innovative? Developers’ contradictory narratives of high-rise housing in Melbourne. Urban Stud. 2007, 44, 631–649. [Google Scholar] [CrossRef]
- Appold, S.; Yuen, B. Families in Flats, Revisited. Urban Stud. 2007, 44, 569. [Google Scholar] [CrossRef]
- Evans, G.W.; Wells, N.M.; Moch, A. Housing and mental health: A review of the evidence and a methodological and conceptual critique. J. Soc. Issues 2003, 59, 475–500. [Google Scholar] [CrossRef]
- Littlewood, J.; Tinker, A. Families in Flats; HMSO: London, UK, 1981.
- Ng, C.F. Living and working in tall buildings: Satisfaction and perceived benefits and concerns of occupants. Front. Built Environ. 2017, 3, 70. [Google Scholar] [CrossRef]
- Yau, Y. Does high-rise residential building design shape antisocial behaviour? Prop. Manag. 2018, 36, 483–503. [Google Scholar] [CrossRef] [Green Version]
- Buys, L.; Miller, E. Residential satisfaction in inner urban higher-density Brisbane, Australia: Role of dwelling design, neighbourhood and neighbours. J. Environ. Plan. Manag. 2012, 55, 319–338. [Google Scholar] [CrossRef]
- Lee, H.J.; Carucci Goss, R.; Beamish, J.O. Influence of lifestyle on housing preferences of multifamily housing residents. Hous. Soc. 2007, 34, 11–30. [Google Scholar] [CrossRef]
- Kearns, A.; Whitley, E.; Mason, P.; Bond, L. Living the high life? Residential, social and psychosocial outcomes for high-rise occupants in a deprived context. Hous. Stud. 2012, 27, 97–126. [Google Scholar] [CrossRef]
- Australian Bureau of Statistics. 2016 Census Community Profiles; Australian Bureau of Statistics: Canberra, Australia, 2016.
- Cappon, D. Mental health in the hi-rise. Ekistics 1972, 196, 192–195. [Google Scholar]
- Council on Tall Buildings and Urban Habitat. Tall buildings and urban habitat: Cities in the third millennium. In Proceedings of the 6th World Congress of the Council on Tall Buildings and Urban Habitat, Melbourne, VIC, Australia, 26 February–2 March 2001; Taylor & Francis: London, UK, 2005. [Google Scholar]
- Seo, J.K. Housing Policy and Urban Sustainable Development: Evaluating the Process of High-rise Apartment Development in Korea. Urban Policy Res. 2016, 34, 330–342. [Google Scholar] [CrossRef]
- IFLA. Disconnect from nature is apparent in high-rise apartment dwellers—How can we bring nature to apartment buildings? In Proceedings of the IFLA World Congress, Singapore, 18–21 July 2018. [Google Scholar]
- Astell-Burt, T.; Feng, X. Investigating ‘place effects’ on mental health: Implications for population-based studies in psychiatry. Epidemiol. Psychiatr. Sci. 2015, 24, 27–37. [Google Scholar] [CrossRef] [PubMed]
- Christian, H.; Bauman, A.; Epping, J.N.; Levine, G.N.; McCormack, G.; Rhodes, R.E.; Richards, E.; Rock, M. Encouraging dog walking for health promotion and disease prevention. Am. J. Lifestyle Med. 2018, 12, 233–243. [Google Scholar] [CrossRef] [PubMed]
- Toohey, A.M.; McCormack, G.R.; Doyle-Baker, P.K.; Adams, C.L.; Rock, M.J. Dog-walking and sense of community in neighborhoods: Implications for promoting regular physical activity in adults 50 years and older. Health Place 2013, 22, 75–81. [Google Scholar] [CrossRef] [PubMed]
- Westgarth, C.; Christian, H.; Christley, R. How might we increase physical activity through dog walking? A comprehensive review of dog walking correlates. Int. J. Behav. Nutr. Phys. Act. 2014, 11, 83. [Google Scholar] [CrossRef]
- Panczak, R.; Galobardes, B.; Spoerri, A.; Zwahlen, M.; Egger, M. High life in the sky? Mortality by floor of residence in Switzerland. Eur. J. Epidemiol. 2013, 28, 453–462. [Google Scholar] [CrossRef] [Green Version]
- World Health Organisation. Connecting Global Priorities: Biodiversity and Human Health: A State of Knowledge Review; WHO: Geneva, Switzerland, 2015. [Google Scholar]
- Melis, G.; Gelormino, E.; Marra, G.; Ferracin, E.; Costa, G. The Effects of the Urban Built Environment on Mental Health: A Cohort Study in a Large Northern Italian City. Int. J. Environ. Res. Public Health 2015, 12, 14898–14915. [Google Scholar] [CrossRef]
- Tyrväinen, L.; Ojala, A.; Korpela, K.; Lanki, T.; Tsunetsugu, Y.; Kagawa, T. The influence of urban green environments on stress relief measures: A field experiment. J. Environ. Psychol. 2014, 38, 1–9. [Google Scholar] [CrossRef]
- Quick, J.C.; Spielberger, C.D. Walter Bradford Cannon: Pioneer of stress research. Int. J. Stress Manag. 1994, 1, 141–143. [Google Scholar] [CrossRef]
- Moloney, R.D.; Desbonnet, L.; Clarke, G.; Dinan, T.G.; Cryan, J.F. The microbiome: Stress, health and disease. Mamm. Genome 2014, 25, 49–74. [Google Scholar] [CrossRef] [PubMed]
- Slavich, G.M.; Irwin, M.R. From stress to inflammation and major depressive disorder: A social signal transduction theory of depression. Psychol. Bull. 2014, 140, 774–815. [Google Scholar] [CrossRef] [PubMed]
- Stigsdotter, U.K.; Ekholm, O.; Schipperijn, J.; Toftager, M.; Kamper-Jørgensen, F.; Randrup, T.B. Health promoting outdoor environments - Associations between green space, and health, health-related quality of life and stress based on a Danish national representative survey. Scand. J. Public Health 2010, 38, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Barton, J.; Pretty, J. Urban ecology and human health and wellbeing. Urban Ecol. 2010, 12, 202–229. [Google Scholar]
- McCarthy, P.; Byrne, D.; Harrison, S.; Keithley, J. Housing type, housing location and mental health. Soc. Psychiatry 1985, 20, 125–130. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, I.; Lavalette, M. After Grenfell Tower. Crit. Radic. Soc. Work 2017, 5, 265–267. [Google Scholar] [CrossRef]
- Alexander, C.; Ishikawa, S.; Silverstein, M. A Pattern Language: Towns, Buildings, Construction; Oxford University Press: New York, NY, USA, 1977. [Google Scholar]
- Chile, L.; Black, X.; Neill, C. Experience and expression of social isolation by inner-city high-rise residents. Hous. Care Support 2014, 17, 151–166. [Google Scholar] [CrossRef]
- Fanning, D.M. Families in flats. Br. Med J. 1967, 4, 382. [Google Scholar] [CrossRef] [PubMed]
- Hannay, D.R. Mental health and high flats. J. Chronic Dis. 1981, 34, 431–432. [Google Scholar] [CrossRef]
- Gillis, A. High-rise housing and psychological strain. J. Health Soc. Behav. 1977, 18, 418–431. [Google Scholar] [CrossRef]
- Verhaeghe, P.P.; Coenen, A.; Van de Putte, B. Is living in a high-rise building bad for your self-rated health? J. Urban Health Bull. N. Y. Acad. Med. 2016, 93, 884–898. [Google Scholar] [CrossRef]
- Moore, N.C. The personality and mental health of flat dwellers. Br. J. Psychiatry J. Ment. Sci. 1976, 128, 259–261. [Google Scholar] [CrossRef]
- Ellaway, A. You are where you live. Evidence shows that where we live has a significant impact on our mental health. Ment. Health Today 2004, 33. [Google Scholar]
- Warr, D.J.; Tacticos, T.; Kelaher, M.; Klein, H. Money, stress, jobs: Residents’ perceptions of health-impairing factors in ‘poor’ neighbourhoods. Health Place 2007, 13, 743–756. [Google Scholar] [CrossRef] [PubMed]
- Wilcox, B.L.; Holahan, C.J. Social ecology of the megadorm in university student housing. J. Educ. Psychol. 1976, 68, 453–458. [Google Scholar] [CrossRef]
- Zalot, G.; Webber, J. Cognitive complexity in the perception of neighbors. Soc. Behav. Personal. 1977, 5, 281–283. [Google Scholar] [CrossRef]
- McCarthy, D.; Saegert, S. Residential density, social overload, and social withdrawal. In Residential Crowding and Density; Aiello, J., Baum, A., Eds.; Plenum: New York, NY, USA, 1979; pp. 55–76. [Google Scholar]
- Churchman, A.; Ginsberg, Y. The image and experience of high rise housing in Israel. J. Environ. Psychol. 1984, 4, 27–41. [Google Scholar] [CrossRef]
- Levi, L.; Ekblad, S.; Changhui, C.; Yueqin, H. Housing, family function, and health in Beijing. In Perception and Evaluation of Urban Environment Quality; Bonnes, S., Ed.; United Nations Educational, Scientific and Cultural Organization Man and Biosphere Programme: Rome, Italy, 1991. [Google Scholar]
- Amick, D.J.; Kviz, F.J. Density, building type, and social integration in public housing projects. Man Environ. Syst. 1974, 4, 187–190. [Google Scholar]
- Bagley, C. The built environment as an influence on personality and social behavior: A spatial study. In Psychology and the Built Environment; Canter, D., Lee, T., Eds.; Wiley: London, UK, 1974; pp. 156–162. [Google Scholar]
- Moore, N.C. Psychiatric illness and living in flats. Br. J. Psychiatry J. Ment. Sci. 1974, 125, 500–507. [Google Scholar] [CrossRef] [PubMed]
- Richman, N. The effects of housing on pre-school children and their mothers. Dev. Med. Child Neurol. 1974, 16, 53–58. [Google Scholar] [CrossRef] [PubMed]
- Husaini, B.; Moore, S.; Castor, R. Social and psychological wellbeing of black elderly living in high-rises for the elderly. J. Gerontol. Soc. Work 1991, 16, 57–78. [Google Scholar] [CrossRef]
- Dasgupta, S.K.; Bhattacharyya, S.; Asaduzzaman, M. The impact of tall buildings on elderly residents. Bangladesh J. Psychol. 1992, 13, 7–15. [Google Scholar]
- Edwards, J.N.; Booth, A.; Edwards, P.K. Housing type, stress, and family relations. Soc. Forces 1982, 61, 241. [Google Scholar] [CrossRef]
- Rosenbaum, J.E.; Reynolds, L.; Deluca, S. How do places matter? The geography of opportunity, self-efficacy and a look inside the black box of residential mobility. Hous. Stud. 2010, 17, 71–82. [Google Scholar] [CrossRef]
- Marmot, S.M. Health in an unequal world. Lancet 2006, 368, 2081–2094. [Google Scholar] [CrossRef]
- Ulrich, R.S. Evidence-based health-care architecture. Lancet 2006, 368, S38–S39. [Google Scholar] [CrossRef]
- World Health Organisation. Urban Green Spaces and Health: A Review of Evidence; World Health Organisation: Bonn, Germany, 2017. [Google Scholar]
- Van den Berg, M.; Wendel-Vos, W.; Van Poppel, M.; Kemper, H.; Van Mechelen, W.; Maas, J. Health benefits of green spaces in the living environment: A systematic review of epidemiological studies. Urban For. Urban Green. 2015, 14, 806–816. [Google Scholar] [CrossRef]


| Key Theme | Mental Health Study Focus | High-Rise Health Outcome | References |
|---|---|---|---|
| Social wellbeing | Social isolation/less social interaction | >social isolation | Fanning [41] |
| <social support and involvement | Wilcox and Holahan [48] | ||
| <social interaction | Zalot and Webber [49] | ||
| <social networks | McCarthy and Saegert [50] | ||
| <social support | Churchman and Ginsberg [51] | ||
| <social contact | Levi, et al. [52] | ||
| >poor social outcomes | Kearns, et al. [18] | ||
| >social isolation | Chile, et al. [40] | ||
| Social wellbeing | Alienation | >feelings of alienation | Amick and Kviz [53] |
| Psychological health | Nervous disorders | >neurotic scores | Bagley [54] |
| Psychological health | Psychological problems i.e., depression | >depression | Moore [55] |
| >depression | Richman [56] | ||
| >emotional strain | Gillis [43] | ||
| >psychological distress | McCarthy and Saegert [50] | ||
| <depression after moving out | Littlewood and Tinker [13] | ||
| >psychological distress | McCarthy, et al. [37] | ||
| >psychological distress | Husaini, et al. [57] | ||
| < stress coping skills | Dasgupta, et al. [58] | ||
| >mental symptoms | Hannay [42] | ||
| >worse psychosocial outcomes | Kearns, et al. [18] | ||
| Psychological health | Suicide | >suicide by jumping on higher floors | Panczak, et al. [28] |
| Psychological health | Self-rated health | <self-rated health | Verhaeghe, et al. [44] |
| Psychiatric health | Psychiatric problems | >neurotic personalities likely to experience psychiatric illness | Moore [45] Edwards, et al. [59] |
| Sense of place | Perceptions of neighbourhood factors that influence health | >perceived negative influence | Warr, et al. [47] |
| Sense of control | Sense of efficacy (control) | >sense of efficacy after moving out | Rosenbaum, et al. [60] |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larcombe, D.-L.; van Etten, E.; Logan, A.; Prescott, S.L.; Horwitz, P. High-Rise Apartments and Urban Mental Health—Historical and Contemporary Views. Challenges 2019, 10, 34. https://doi.org/10.3390/challe10020034
Larcombe D-L, van Etten E, Logan A, Prescott SL, Horwitz P. High-Rise Apartments and Urban Mental Health—Historical and Contemporary Views. Challenges. 2019; 10(2):34. https://doi.org/10.3390/challe10020034
Chicago/Turabian StyleLarcombe, Danica-Lea, Eddie van Etten, Alan Logan, Susan L. Prescott, and Pierre Horwitz. 2019. "High-Rise Apartments and Urban Mental Health—Historical and Contemporary Views" Challenges 10, no. 2: 34. https://doi.org/10.3390/challe10020034