Strategies Christian Nurses Use to Create a Healing Environment

School of Nursing, Azusa Pacific University, 901 E. Alosta Ave., Azusa, CA 91702, USA
Religions 2018, 9(11), 352; https://doi.org/10.3390/rel9110352
Submission received: 19 September 2018
/
Revised: 19 October 2018
/
Accepted: 7 November 2018
/
Published: 9 November 2018
(This article belongs to the Special Issue Selected Papers from Spirituality in Healthcare Conference 2018 “Spirituality at a Crossroads”)
{kind=link}
Abstract
:From Nightingale forward, nursing has understood that interaction of person, nurse, and environment facilitates optimal outcomes. Yet, there remains a need for research on the paradigm concept of environment and creation of a healing environment. This classical, grounded theory study aimed to identify (1) strategies Christian nurses used to create a healing environment and enhance well-being, (2) outcomes they perceived resulting from these strategies, and (3) factors they regarded as either enhancing or inhibiting the creation of the healing environments. A criterion-based, purposive sample of Christian nurses (N = 15) was interviewed between June 2013 and January 2014 until data saturation was reached. Data were analyzed using constant comparative methods in consultation with a grounded theory expert. “Charting the healing path,” the core category, consists of four phases: helping patients get better, fostering the healing environment, charting a healing path, and observing outcomes. The “charting the healing path” model informs development of the environment domain of nursing knowledge. Knowing the patient, the juncture of nurse and patient points of view, and the resultant nurse–patient partnership promote best potential outcomes to be realized incrementally during, and after, hospitalization.
1. Introduction
Nurses are the front-line caregivers in hospitalized patients’ recovery from illness. Consequently, they are purposefully engaged in healing and promotion of well-being. How nurses navigate the process of healing displays their application of nursing meta-paradigm concepts (person, nursing, environment, and health) to accomplish the goal of healing and well-being. The nurse–patient relationship is understood as the basis for transforming the patient illness experience into one of patient and family gaining knowledge and experience that fosters health. This in-hospital experience is intended to influence recovery both within and beyond the hospital as the patient returns to home and community (Young et al. 2015). Therefore, nursing influences the environment of care beyond the immediate context of hospital recovery.
While there is research on nurses’ perspectives from a particular religious background providing spiritual care (Bakir et al. 2017; Herlianita et al. 2018; Abudari et al. 2016; Pesut et al. 2009; Pfeiffer et al. 2014; Taylor et al. 2014) there is none regarding the effect of faith background on creating a healing environment. This research, which identifies and delineates the process of creating a healing environment, will describe strategies Christian nurses used in hospital settings where the nursing practice model and the hospital philosophy are jointly supportive of whole person care.
Background and Significance
From Nightingale forward, nurses have employed principles of health and hygiene embedded in nature to promote healing (Pfettscher 2010; Nightingale 1992). In addition to these Nightingale identified principles, patients need knowledge and compassionate assistance to progress in recovery.
The hospital with all its technological and organizational strangeness to patients is a known world for nurses and caregivers. Thus, the caregiving science and artistry of nurses must help set patients at ease in this setting filled with many unknowns. Nurses facilitate interaction of person (patient), nurse, and environment for optimal health outcomes (Nightingale 1992). The challenge of shaping one’s professional practice environment to be a healing, patient-centered environment includes relationships of significance, physical surroundings, and the setting in which nursing occurs. Thus, research is needed which explores how the nurse’s person and knowledge exert a profound influence in facilitating or impeding creation of a healing environment in predetermined structures and settings.
Grounded theory as methodology is based in the theoretical perspective of symbolic interactionism (SI). This perspective sensitizes the researcher to “how” participants (nurses in this case) construct and engage with the patient toward creation of a healing environment. The interactions of nurse and patient, and the meanings attached to them, invite the patient to be a full partner in choosing a path toward healing.
A limited review of literature using four health- and nursing-related search engines: Pub Med, Medline, Academic Search Premier, and Cumulative Index of Nursing and Allied Health (CINAHL) was conducted prior to study formulation and data gathering. This is consistent with classic Grounded Theory (Glaser and Strauss 1967; Glaser 1992) recommendation to not preload the study with literature-based categories or a theoretical framework (Glaser 1998). Using the search terms healing environment, well-being, nursing, nursing research, and nurses perspective, a total of 33 research studies were reviewed. It was necessary to further limit the search by adding “Not wound or bone healing” as Boolean terms.
Themes present in this review of literature (ROL) include those which explicate the relationship between nurse, patient, and environment for outcomes of healing and well-being. Nurses recognize that the human body has natural and spiritual healing capacities that can flourish when placed in an environment conducive to healing (Selanders 2010; Timmins 2011). Nurse as direct caregiver and nurse as innovator and healer were nursing roles named in this ROL. Nurse as innovator describes the nurses’ voice in design of systems and delivery of care in specific units within the system (Broyles et al. 2008). Nurse as healer is often embedded in the closely parallel concepts of caring and healing in nursing (Swanson and Wojnar 2004; Woolley et al. 2012). Themes identified were those which prioritized:
- whole person care (Bolles and Maley 2004; Watson 1999) and/or patient-centered care (Dickson et al. 2017; McCance et al. 2011; McCormack et al. 2010);
- the optimal management of nursing environments including architectural design and structure, and space and place factors which expressed value toward processes and outcomes of healing (Sakallaris et al. 2015);
- the larger organizational commitment to patient and staff well-being; and
- the above-mentioned roles of nursing, which shape practice environments of the nurse and healing environments for patients and staff.
In an overview of energy healers from many world views and practice perspectives (including Christian healers), Levin (2011) purports among all the differences that there is an overwhelming consensus that what matters for healers and healing is focus, compassion, and intention. If one possesses these three heart attitudes, regardless of the training system, the philosophical stance, or the category of healing arts practiced, healing is clearly in view. (Jarrin 2012) suggests “nursing is caring situated in space, place and time, shaped by the internal and external environment of both the nurse and the patient/client” (p. 17). The ROL suggests that the direct caregiver role, the healer role, and the innovator role of nurses deem them facilitators of a healing environment within an already built hospital structure.
The purpose of this study was to explore strategies Christian nurses used to create a healing environment for the hospitalized, non-end-of-life patient. Specific aims included identifying strategies nurses used, outcomes they perceived resulting from these strategies, and factors they regarded as either enhancing or inhibiting the creation of healing environments. Findings reflect the researcher’s attempt to answer the question, “what is the main concern of nurses in creating a healing environment?”
2. Results
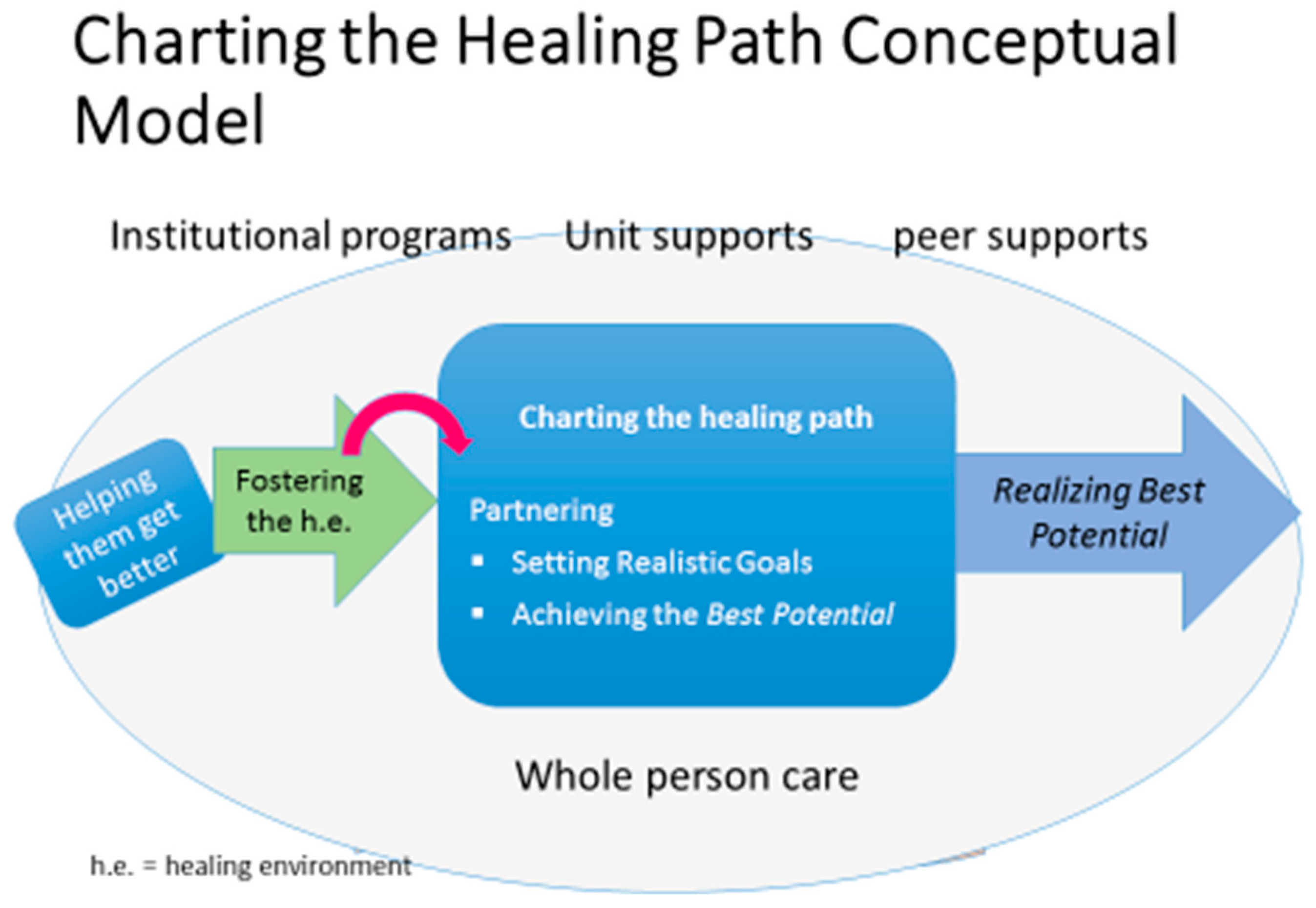
Charting the Healing Path Model (See Figure 1) gives an overview of the phases these nurses used in creation of a healing environment. The phases are described below and a case study presented which illustrates each phase with realizing the best potential as the outcome.
2.1. Helping Them Get Better
Nurses verbalized that a healing environment is one that is patient-centered, where the nurse recognizes and embraces the whole person, and communicates a compassionate presence with the patient’s best in mind. This requires the nurses to make themselves available, and assist patient and/or family to discover and gain confidence in what will help them heal. From the beginning, nurses had the vision that helping patients get better was for the purpose of returning home with the best possible recovery outcomes in their health situation. Two aspects of this helping them get better were (a) doing a baseline assessment and (b) being available to address the person wholistically. This active getting to know the person moved into the next theme of fostering a healing environment.
These Christian nurses reported that conversing with patients about the reason for their hospitalization involved asking a few intentional questions regarding their faith beliefs and practices which could influence their hospital stay. This began on admission and was augmented throughout their stay. Eight nurses did an explicit spiritual assessment. Nine of the nurses included spirituality as a part of their definition of a healing environment or well-being. Seven gave examples of integration of spiritual care without labeling it as such. Five began with a spiritually focused exemplar when asked about a specific instance of creating a healing environment.
Nurses also observed what clues were visible in the patient environment whether rosaries, readings or scriptures, family pictures, tattoos, etc. These findings offered conversational assessment of what was important and meaningful to the patient, and how they could be utilized for progress toward well-being. One middle-aged nurse (FF) with over 10 years of practice was intent on trying to find out “where the patient was coming from”. She and three other nurses (CC, JJ, PP) spoke of conversing about meanings of what they observed, including family, culture, traditions, and discerning what “is going to be helpful for them ... what matters to them?” Though comfortable with spiritual assessment questions, six nurses indicated that observational and behavioral clues were their entry to spiritual assessment. These six did not initiate further assessment, except in situations of patient distress or discouragement. Thus, nurses were evaluating, is wholeness present or lacking, and if lacking, how could they further assess. These nurses demonstrated the value of the spiritual by being intentional to access that which the patient presented as spiritual resources, or lack of them, and assess any spiritual concerns. One young night nurse (PP) described this process as stimulating patients to consider “what their support is ... and what helps them”. The breadth of spiritual strategies surfaced in 23 reported patient situations with explicit spiritual intervention.
Though spiritual assessment was not named as an explicit theme in the Charting the Healing Path model, these Christian nurses repeatedly gave exemplars of spiritual care assessment and intervention as part of their whole person care from admission to discharge. The researcher named this phenomenon as nurses having a reservoir of underlying spiritual beliefs and practices readily available to them during patient care interactions.
2.2. Fostering a Healing Environment
Getting to know the person as a unique individual and hearing a patient’s immediate concerns were open codes that summarized making connection with what was meaningful for the patient in the present, and in their larger, post-illness world. One nurse emphasized that the nurse needs to remember, and sick people need to know, the nurse is “here to take care of patients”. His message was that in the midst of all the therapies and technologies employed in the hospital, “in the end ultimately it is us [the nurse] they need, [in order] to heal and go through that process”. Glaser (1998) described this phenomenon from the researcher perspective: When the subjects, in this case nurses, know they are being listened to, they will “vent their concerns to the max” (p. 123). These nurses verified that the parallel is true for their patients: when the nurse is listening, patients know they are invited to express their concerns and most pressing needs. One senior nurse shared her strategy of getting to the bottom of things from first meeting of the patient:
Well, I usually ask them, “What’s going on?” ... I want to know where they’re at, where they’re coming from, are they afraid, are they in pain, do they have a lot of unanswered questions? ... I want to try to find out ... and just deal with that issue right off the bat so that we can get to the bottom of things ... to a lot of issues that often get missed.
Even with limitation of time, listening well without communicating a busyness or hurriedness helps move the healing process to the next identified theme: Seeing from the patient’s point of view.
A young cardiac, Spanish-speaking nurse (II) illustrated both fostering a healing environment and seeing from the patient’s point of view in sharing her faith background and tradition with a combative, resistant patient. After the shift began, another nurse requested she change patients with him as the patient refused his care and began yelling in Spanish. Nurse II agreed, began by focusing on building relationship, identifying anything they had in common, getting the patient to share some of her values and what was meaningful. In doing so, the patient talked about her orthodox Christian background. The nurse quickly identified that continuing this topic of conversation would be helpful to the patient. Thus, she shared her Christian faith and family background, which she did not usually do. However, she could see this patient would benefit from her more personal sharing.
2.3. Seeing from the Patient’s Point of View
Understanding the patient’s grasp of things, particularly the current situation, is essential for developing an individualized plan of care, and not truncating a relationship of trust and respect. These two strategies are often fluid and interchangeable. Sometimes the patient’s point of view and perspective are seen when assessing the immediate concerns. Another young cardiac nurse (DD) recalls dealing with a diabetic patient who was well known to the unit for high blood sugars and self-adjusting his insulin regime upon leaving the hospital. She describes her instinct this admission to educate versus listen to the patient’s understanding of his high blood sugars.
And so sometimes you hear things patients say and you just completely throw it out the window thinking, “you know what, like I’m the nurse here and I should know” ... but you work with them, so that you’re able to at the end of the day to teach them more because you have built their trust.
This nurse, in listening, discovered neither she nor the patient completely understood his polyuria as his rationale for self-adjusting his medication. However, his immediate concern of staff messing with his insulin regimen was key to his point of view being heard.
This same nurse, acting as the unit resource nurse for this particular shift, describes the care when one of the patient’s awaiting a new heart for transplant began to rapidly deteriorate. After many emergent interventions, in a moment of complete helplessness, she asked if they wanted to pray “because that’s all I knew to do”. The resultant 30–60 s of unimaginable peace was later described by the wife as that which changed the day, and the course of action. Though she had not done spiritual assessment with this patient, she knew they prayed and believed in God. Her intervention flowed from her own deep conviction that God was with her and a powerful resource of love and care. “I feel like He is teaching me through that, ‘I’m all you need in your time of distress.’” She acknowledged how easy it is in critical moments to forget about God and get caught in a flurry of activity. “But it takes thirty seconds to connect with God, and it makes the world of difference.” The primary nurse shortly after that prayer told nurse DD, “I’m glad you prayed with them; that helped me and gave me peace too.” The nurse affirmed the greatest blessing of joy is hers in situations like this where, “He allowed me to be there at that time.”
One intensive care nurse (ICU) nurse (KK) explained that though the healing environment is frequently focused around what’s going on physically with the patient, the patient’s perspective is essential for forming a partnership. She routinely asks the patient, “What are issues we may need to address today? What are your goals for today? You have to address their needs before you get into what you want … otherwise it seems like you’re kind of demanding.” The more intense the needs, the more challenging this forming a partnership becomes. Another nurse (BB) with only 5 years of practice recounted an example of spiritual assessment which illustrated seeing from the patient’s point of view and adding her own point of view, with the patient’s full agreement and interest to hear. After doing her initial assessment in the morning with a 93 year old suicidal man who reported no spiritual or faith ties, she made time later in the afternoon to continue her assessment. She referred to his earlier comment and continued, “you know, earlier today you said you didn’t have any spiritual beliefs ... where do you think you are going to go if you were to die today?” He stated he didn’t know where he would go. She describes herself being in close proximity, very focused, personal, and intimate with this man, and speaking softly, while many nurses would not be comfortable with this level of intervention, she told this man he could know for sure where he would go and all he had to do was pray to Jesus. He indicated interest, and so she led him in the sinner’s prayer. After a positive, peaceful response, “I went to my next patient, [in the same room] and the man said to me ‘I want to do the same thing that you did for that man.’” Surprised that the patient could have heard because of her low voice volume, she joyfully repeated the good news of Jesus as the Way to salvation and readiness for heaven, led the patient in the sinner’s prayer, and counted it a privilege to be used by God in this way.
2.4. Seeing From the Nurse’s Point of View
The first nurse interviewed (AA), when interviewed a second time, identified that something was missing in the tentative substantive theory. She looked at the strategy “seeing from the patient’s point of view” and very clearly and articulately labelled what was missing in forming a partnership with the patient as “seeing from the nurse’s point of view”. That is, “by virtue of education, experience, and caring presence the nurse now interprets the patient’s point of view and adds the nurse’s own perspective, own reservoir of knowledge and resources” (Pfeiffer 2014, p. 83). This allowed the researcher to do theoretical sampling from interviews already done, as well as yet-to-be-conducted second interviews. One night nurse explained how charting at the bedside facilitated her knowing what the patient’s needs were, even if there was no verbal dialogue. Being in the patient’s presence informed her sense of what this patient needed. Another medical-surgical nurse explained from her point of view that she knew taking pictures of the breast wound with expanders and without was a necessary step for this particular patient to come to terms with her now altered body. Seeing from both the patient’s and nurse’s point of view is indicated by the pink connecting arrow in Figure 1.
A conceptual shift occurs so the nurse is now asking “What do I have to offer that this patient needs?” Whether patients are ready to accept what the nurse has to offer is often a matter of timing and requires the nurse to hold in tension his or her own viewpoint until the patient is ready to receive it. Whether starting an IV other nurses were unable to, or after getting it started, this charge nurse (AA) insisted she was “... praying the whole way [to the patient’s room], and even when I got down there ... I was saying to myself, ‘All things are possible with God, so you got to help me with this IV, God!’” After she got it in, she said out loud, so the patient could hear, “Thank you, Jesus. ... It was important to give glory to God, to acknowledge he helped me start that IV.” This “out loud” thank you reflected the nurse’s follow through in her relationship with God and was, secondarily, a possible conversational opener if the patient chose to respond. The patient did not and the nurse was simply thankful for God’s help in her nursing care. Yet it was the nurse’s perspective that part of what she had to offer included God at work in the present situation. Whether the patient recognized it or not, did not stop her from using her belief and offering an invitation to the patient. She also emphasized the importance of not pushing the patient to respond, but attentively noted whether there was interest or not.
Nurse BB gives an experience of a patient challenging her intentional spiritual assessment, reporting to her, and later her charge nurse, being offended by these intrusive questions. Nurse BB apologized, assuring the patient she did not intend to offend [and surmised, in retrospect, that she had probably asked these questions too soon in the relationship]. As she entered the room later to pass meds, she heard the patient complaining to the charge about her “meddling in what was none of her business”. The nurse again apologized and both nurse and charge nurse valued the patient telling the truth. The charge nurse had just finished explaining that spiritual assessment is part of the nurse’s role in helping patients heal and recover. The patient felt heard, enough that she apologized later in the day, and even sought this nurse out the next day when she was assigned another nurse. This is an example of bold and honest interaction with the patient around assessment of spiritual beliefs and practices, and good conflict resolution when necessary
The nurse’s point of view was conceptualized as a bridge to partnering effectively with the patient for well-being. This bridge to partnership is illustrated by the offering of self, and resources available to strategize and chart a healing path with the patient and/or family. Nurse (FF) details an awareness of regularly knowing now is this time to act in a few short minutes to make a difference. Her patient was a 19 year old drug kingpin with bullet holes all over, under constant surveillance, and the nurse saw officers coming with the orange jumpsuit in which he would be discharged to prison. The nurse shared the process of saying “Let’s pray. Is it ok?” As the young man indicated “Yes” she began praying with her eyes closed from a ‘we’ standpoint. ... [that is] “You know we all fall short of the glory”, ...
At the end, I looked down at him and there were just tears coming down, and I looked at all the officers and their eyes were all welled up, as well. And, I knew I had seized the moment and made an impact that he was going to think about, and he’ll always probably remember that (Pfeiffer 2014, p. 109).
When the demand of care is urgent, it is seldom initiated with the luxury of time to plan one’s intervention; rather, it sometimes flows from who the nurse is: that is, from the treasure chest of character, beliefs, and practices forged together, available for emergent situations.
2.5. Charting the Healing Path
At this point in the research process, the researcher and nurse consultant had just agreed that “discovery of the healing path” was close to being a core category. However, the next three nurses interviewed talked about partnership with further nuance including vulnerability, advocacy, unknown as potential barrier [to partnership and moving forward], self-care, setting realistic goals and facilitating next levels of health or best potential. Getting this picture of the pattern and properties of partnering while using the constant comparative process helped identify the core category of charting the healing path. This category contained the substantive codes of partnering with the patient toward well-being, setting realistic goals, and facilitating best potentials. “Discovery” was indeed a part of the process, but the descriptions these nurses gave indicated a more dynamic, action-oriented process involved in partnering, setting goals, and facilitating the best potentials for the particular patient. Thus, charting the healing path became the core category with “best fit” for explaining the essence of how nurses solve their initial concern, helping patients get better.
Nurses almost always take the initiative for charting the healing path but are intentional in making it a mutual process with patient and/or family. Sharing the ongoing formation of the healing path not only gives ownership, but highlights ability, desire, and commitment (or lack) of the patient and/or family, and the treatment team to partner in reaching these realistic goals and best potentials. The ICU nurse (QQ) models her own Christian commitment to spiritual values and practices, when she cares for the Hindu ICU patient. This required her to first learn Hindu practices important to this patient and his religious community, negotiate allowances with the nurse manager, and demonstrate to her colleagues that the healing path for this patient included music with chanting, burning of incense, and the presence of four [in the room] visitors most of the day (beyond the limited visitation hours of the unit). Repeatedly, in trusting the nurse and his/her point of view, the patient can still be a full partner, even if not yet able to take initiative. The nurse adds knowledge to trust whenever possible. When what the patient values is upheld, the nurse–patient partnership can discover what is needed to move forward, a healing path can be forged, and as illustrated above, not just for the patient, but all involved as they participate in care of this patient and family.
Once a core category is identified, explanation of how all other substantive codes relate to it is necessary to confirm the selection of a core category. In this study, a memo sort allowed advocacy, vulnerability, and a readiness factor to emerge as mediators in partnering with the patient. The following patient-centered scenario will illustrate the presence of these emergent factors as the nurse navigated the patient’s need for goals with his best potential in mind.
2.6. Case Study and Realizing Best Outcomes
The ICU nurse (KK) recognized a threatening decline in her elderly patient who did not want to make decisions without family involved. As soon as family arrived, the nurse orchestrated a care team meeting (no small feat) with outcomes of a referral for pain relief, and subsequent computerized tomography (CT) scan which diagnosed a pulmonary embolus. Now anxiety about breathing was no longer obscured by pain control issues. The nurse had to repeatedly request continuous positive airway pressure (CPAP) and restate the non-rebreather, 100% O2 mask was not working. After several phone interactions, the physician ordered CPAP and “within five minutes we had his oxygen FI02 down to 70% and he was ‘satting’, like, 95 (as compared to 83 or 79 before this)”. She described feeling very, very grateful for all she was able to initiate on his behalf. In order to deal with his fear of death, the patient several times grabbed the nurse’s hand and said, “Give me a prayer. Give me a prayer.” After each prayer he would calm, breathe easier, and appear ready to continue partnering this vulnerable but competent, skilled advocate at his bedside. This nurse was aware she needed to augment the expert physical care he received with emotional and spiritual care that matched this fight for recovery. She assessed his need for courage in the situation because he had a rough road ahead, including chemotherapy. In reminding him that he was a fighter (she’d seen that in him that day), she encouraged this “I can fight this” outlook. “So, I talked to him about that kind of outlook right now ... ‘stay positive and we can do this together.’”
The nurse advocated with family, and then the care team for what the patient needed immediately, that day, that hour. She identified his readiness when he called out for prayer, and she, having never before prayed “out loud with a patient”, needed courage also, but with the patient requesting with such urgency and intensity, how could she refuse. Once she observed the results, she relaxed into forging that partnership in order to stay out in front with meeting realistic goals for that day, and facilitating his best potential. Most often the nurse initiates charting the healing path. This time the patient initiated, and the nurse was able to pull from her reservoir of Christian beliefs and practices to meet this man in his place of need. This same nurse later summarized the charting the healing path category by saying “... we need them to be active participants in their care ... when we have mutual goals we can work toward them being discharged and ... being managers of their own care.” She also acknowledged having learned, there are times when both words and presence are needed in giving spiritual care.
3. Discussion
From a classic grounded theory approach, two theoretical codes were identified that highlight the process nurses used in charting the healing path of recovery with the patient and family. The first of these, the interactive family, describes the mutually interactive commitment of shifting responsibilities to the healing path outcomes. Both nurse and patient contribute their point of view to achieve a true partnership toward best patient outcomes, with the nurse’s knowledge paving the way for next steps. The second theoretical code, the strategizing family, explains the conscious or intentional action to move the patient toward establishing the best potential for recovered health. Both of these grounded theory theoretical codes address the person–health interaction domain of nursing (Meleis 2007). The health–environment domain is background, like a stage-setting conducive to healing or not. Thus, the nurse is orchestrating a place–space–relationship context for pursuit of healing via a partnership of trust and respect (Dickson et al. 2017; Giske and Cone 2015). There are implicit and actual environment essentials present in creating a healing path.
The primary implicit essential is seen in the nurse focusing on the nurse–patient interaction, with the healing environment in view. One image which illustrates this primary implicit essential is that of a slow-motion, time-expanded handoff of a relay race baton. The nurse holds the baton as long as needed; this involves knowing the patient, building the partnership, and getting ready to transfer the baton of self-care to the patient. The nurse repeatedly made judgement calls as to patient readiness, and how long it is necessary for both to hold the baton to ensure an effective transfer. In this research, once realistic goals were set with best potentials being identified, the transfer was ready to happen. In this transfer of the baton, the second implicit essential is seen: the nurse’s intentionality about helping the patient set realistic best potentials. Now, the race can be continued successfully with the patient owning the will-to-health.
The juncture of nurse and patient points of view was a bridge to partnership and a vital link for “charting a healing path”. The nurse bringing self, and his or her perspective (nurse knowledge), to the patient creates a caring connection for healing. Here, the nurse advocates for a healing environment by care and relationship intentionality, starting with the present and charting a way forward (Giske and Cone 2015; Halldorsdottir 2008; Zoinierek 2014). As one seasoned master’s nurse said, “I listen a lot, and help that person discover what might help them heal.” (Jacobs 2013) asserts this advocacy knowledge is valuable for both research and infusing value-added practices in caring, whether from an individual or broader institutional environment. Nurses first envision the best potential for the patient and are alert and attentive for patient cues and input. Sometimes, management and administrator’s contributions influence this best potential (Young et al. 2015). A Christian nurse’s listening reflects the love of the God who knows each of his creation for the uniqueness, the gifting, the needs, and the nurse discerns what will help move this particular person forward in the healing process.
Nurses in this research described actual essentials as those that were “other-initiated efforts” toward healing. Whether nurse administrators heard from nurses or took the lead in supplying these external actions and/or programs to support healing, the environment of nurse and patient benefits. One hospital had a very important person (VIP) program where a nurse recommended by nurse management received training in meeting spiritual care needs. Nurses named programs that infuse some aspect of nature (a healing garden, real or painted nature scenes, time and place to rest with dimmed lighting and noise reduction, therapy dogs). They also identified processes that facilitated nurse–patient interaction (hourly rounding, bedside reporting, nurse zoning, provision for nurse meal and break relief, I-care cards, key words at key times) as significant contributors to creation of a healing environment. This organizational commitment to creating a healing environment shares both internal and interpersonal aspects of the Optimal Healing Environment movement (Minton and Batten 2016; Sakallaris et al. 2015; Findlay et al. 2006). It is also similar to the conceptual structure of person-centered nursing which emphasizes the care environment, person-centered processes, and outcomes possible at a personal and system-wide level (McCance et al. 2011; McCormack et al. 2010; McCormack and McCance 2006).
The nurse ensures that patient participation is significant in using these environment essentials for best patient outcomes (Dickson et al. 2017; O’Hagan et al. 2014). A Christian nurse recognizes that the whole realm of nature has power to communicate the reality of God; sometimes with words, and many times without words. Words which invite the patients to partner and own their healing path are tangible evidence of an invisible God and his desire to see humans flourish in relationship, with shared ownership and accountability for healing. Another illustration follows as the nurse, committed to distinctly Christian care, insists actions speaks louder than words.
Changing the landscape of the “possible” was part of nurses’ roles in facilitating the best potential for patients at the individual level. Here, the nurse was attentive to what was meaningful to the patient and secured the patient’s commitment to the goals of today, holding the longer-term “best potentials” in view. One cardiac-telemetry nurse described the small steps of opening the curtains (patient preferred them drawn), cajoling with humor, and getting the patient engaged in sitting up for meals, then walking to the nurses’ station. When the patient could do this, he could also walk to the window and view others playing golf. Here, the landscape of the “possible” changed for the patient: he could once again see himself playing golf. The nurse had this in view as soon as he heard the patient was a golfer and strategized step-by-step actions that would get him ready for golf (“best potential”) with recovered health.
Bridge-building and partnership happens at both the individual level, and can also happen at the larger work environment level. Thus, nursing practice can be positively impacted by a conceptual and communication model of bridge-building for a culture of care at every level of the organization. Christian nurses understand that hearing what is meaningful to the patient clarifies where they are physically and spiritually. From the Christian perspective, this demonstrates that God is near, listening, hearing, and interested, even if the patient’s desire to move forward in a healing partnership is latent at that particular point in time.
When the patient is ready, nurses partner with patients’ desire to work toward the best potential(s). Likewise, expanding nurses’ view of the “possible” allows best practice potentials to surface for their unit, section, and work environment (Aurilio 2017). Nurses have knowledge and environment savvy that can inform both a healing environment for the patient and a healing work environment for the nurse. Nurses’ perspectives can inform partnerships within nursing and beyond. These collaborative efforts could encompass a new valuing of “traditional nursing body therapies” (Benner and Wrubel 1989, p. 79) or connecting separate entities of practice and/or delivery: (Wallach 2017) e.g., nurse and patient satisfaction parameters for unit- or section-wide healing environment innovations. The possibilities seem unlimited within nursing for “charting a healing path” and impacting the health-environment domain of nursing, both of the individual patient and the nurse work environment (Paal et al. 2018). Christian nurses comprehend God as ruling over, and involved in, all the domains of the metaparadigm of nursing: person, health, nursing, and environment. Therefore, it is not surprising that one serendipitous finding was that a majority of these nurses named spiritual strategies as a part of how they created a healing environment.
4. Materials and Methods
This doctoral dissertation study was approved by the University Internal Review Board (IRB). Limited research funding was awarded by both the faculty research council of the author’s university of employment and by the school of nursing where the doctoral degree was obtained. A classical grounded theory design (Glaser 1978) was used as a general inductive approach to discover how nurses create a healing environment as the patient moves from illness toward healing and recovery. As data collection began coding, use of the constant comparative process, and data analysis happened simultaneously. This approach seeks to determine the challenge or problem as the nurse sees and understands it (Glaser 1978, 1998)
4.1. Participants
A criterion-based purposive sample design was used to identify, recruit, and interview RNs meeting the following criteria: (1) at least two years of work experience, (2) worked an average of 10 h per week or more, (3) worked primarily with adults on non-end-of-life units, (4) comprehended, read, and spoke English, and (5) declared a Christian world view. Eighteen nurses were interviewed, two were excluded because during the interview they indicated they did not share a Christian worldview (though they had indicated so verbally during interview scheduling process), and one practice interview did not meet all the study parameters. Fifteen nurse interviews were used, with no new codes in data analysis identified after interview number 12. Thus, two additional interviews were done after data saturation occurred, plus one practice interview was added at the end for its rich data.
The study participants’ average age was 36.7 years and ranged between 25 and 61 years. Seven interviewees were under 30. Three held associate degrees, nine had bachelors’ degrees, three had masters’ degrees with three others currently enrolled in a master’s program. Years in nursing ranged from 2 to 25, with an average of 7.6 years. Practice areas included acute medical/surgical units, combination of surgical or cardiac and telemetry units, intensive care units, labor and delivery, oncology and emergency department. All participants worked 12 h shifts, most working 36–40 h per week. Thirteen nurses worked day shift; two worked night shift.
4.2. Data Collection
Data collected between June 2013 and January 2014 included an ‘Information about You’ data sheet (sociodemographic data) and a semi-structured interview of 45–90 min. Consent took place at the first interview, though consent form and interview questions were sent electronically ahead of time if the nurse requested. Open-ended questions and probing questions were used to elicit nurse’s perspective, meaning, and actions taken to create a healing environment. These interviews were tape-recorded and transcribed verbatim. They were verified for accuracy before entry into NVivo (version eight), a software data management program, and then analysis began. Sample questions from the interview guide included: For you, what is well-being and what contributes to the patient’s recovery of health and well-being while here in the hospital? How do you define a healing environment? Describe how you create this healing environment. How do you do it? Tell me about a time when you created a healing environment for one of your patients. Give as much detail as you can remember.
If by the time the interview was near closure RNs had not mentioned anything related to spiritual caregiving, the researcher asked “What is your spiritual or faith-based background, and how do you express this in creating a healing environment that enhances well-being? Only one nurse had not, by the end of the interview, volunteered their faith background information and its role in the question at hand.
4.3. Data Analysis
In grounded theory, data analysis begins with no preconceived codes or concepts. On the first read, the researcher codes every concept that stands out as important (Pfeiffer 2014). Analysis also happens concurrently with ongoing data collection, coding, using constant comparative process while memoing, sorting, and writing. This facilitates comparing one incident with another for similarities and differences; and discovery of concepts, properties, and categories while interviewing participants. As themed groupings and patterns come into view, the researcher is always asking, what is the main concern of the participants? (Glaser 1998, p. 116). In this study, “helping them get better” was the initial themed grouping identified, quickly followed by “fostering the healing environment.” However, it was when second interviews began that a RN identified a structure and pattern of relationship between major categories that eventually led to identification of other main categories, a theoretical code, and emergence of a substantive theory entitled creating a healing path.
4.4. Limitations
Researcher reflexivity is always present as a potential bias in classical grounded theory. However, the constant comparative process puts data between the researcher and conclusions, and use of constant comparison and a grounded theory expert helped minimize this source of bias. Likewise, only nurses who volunteered as participants were interviewed in this study, potentially decreasing representation of Christian nurses interested in creating a healing environment. Yet interest in the topic allowed participant expertise to come forward as a baseline for understanding how Christian nurses create a healing environment. Purposive sample selection may limit the generalizability of these findings. However, within classical grounded theory, this limitation becomes a strength by which these nurses demonstrate how they solved the problem they faced: helping patients get better. Questions in the interview guide may represent some bias: these were tested and modified in mock interviews.
5. Conclusions
Christian nurses who embody the values and practice of providing wholistic patient care understand their role in creation of a healing environment as supporting the patient–health domain of nursing by “helping the patient get better.” The nurse–patient relationship was intentionally used to influence the health–environment domain. This happened when the nurse–patient points of view were merged to establish a partnership where realistic goals toward self-management could be mutually identified and worked toward. The environment of the in-hospital-present was a springboard for the beyond-the-hospital-future environment for establishing best potentials for recovery of health and well-being. These were realized when the nurse, patient, and family were successful in this transfer of understanding, and all worked together to facilitate best potential outcomes for health. While these outcomes were not always realized, nurses were quick to observe, revisit, and change strategies for charting the healing path in partnership with patient and family. Thus, the strategy for a healing environment inside the hospital has great potential to influence the ongoing environment needed for health and continued recovery outside the hospital. The Christian nurse embodies the reality that God, in Christ Jesus, is always available for partnership in the healing process. Jesus, and the nurse as his partner, have power to envision and orchestrate a healing environment infused with spirit and connection for good, beyond the human level of relationship.
Funding
This research was funded by the Azusa Pacific University Faculty Research Council grant for data collection and analysis, and by the Loma Linda University School of Nursing for dissertation completion.
Acknowledgments
I would like to thank Patricia Jones for her dedicated supervision and guidance throughout this research project. Pam Cone provided expert grounded theory consultation and mentoring from data analysis to publication.
Conflicts of Interest
The author declares no conflict of interest. The founding sponsors had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, and in the decision to publish the results.
References
- Abudari, Gassan, Hassan Hazeim, and Gilda Ginete. 2016. Caring for terminally ill Muslim patients: Lived experiences of non-Muslim nurses. Palliative & Supportive Care 14: 599–611. [Google Scholar] [CrossRef]
- Aurilio, Lisa A. 2017. Creating an Inclusive Culture for the Next Generation of Nurses. Nurse Leader 15: 315–18. [Google Scholar] [CrossRef]
- Bakir, Ercan, Sevgin Samancioglu, and Serap Parlar Kilic. 2017. Spiritual experiences of Muslim critical care nurses. Journal of Religion and Health 56: 2118–28. [Google Scholar] [CrossRef] [PubMed]
- Benner, Patricia, and Judith Wrubel. 1989. The Primacy of Care: Stress and Coping in Health and Illness. Menlo Park: Addison-Wesley. [Google Scholar]
- Bolles, Stephen, and Michael Maley. 2004. Designing relational models of collaborative integrative medicine that support healing processes. The Journal of Alternative and Complementary Medicine 10: S-61–69. [Google Scholar]
- Broyles, Gail, Georgita T. Washington, Lois W. Lowry, Beverly Gugliotta, Phyllis Eorgan, and Kathryn Wilhoit. 2008. Innovative solutions: Registered Nurses’ perceptions of the work environment before and after adult intensive care unit renovations. Dimensions of Critical Care Nursing 27: 180–88. [Google Scholar] [CrossRef] [PubMed]
- Dickson, Megan, Helen Riddell, Fiona Gilmour, and Brendan McCormack. 2017. Delivering dignified care: A realist synthesis of evidence that promotes effective listening to and learning from older people’s feedback in acute care settings. Journal of Clinical Nursing 26: 4028–38. [Google Scholar] [CrossRef] [PubMed]
- Findlay, Barbara, Katherine Smith, Michale Finch, and Sherry Loveless. 2006. Survey of Healing Environments in Hospitals: Nature and Prevalence. Available online: http://www.samueliinstitute.org/File%20Library/Our%20Research/OHE/2006PilotSurveyofHEinHospitals.pdf (accessed on 12 March 2012).
- Giske, Tove, and Pamela H. Cone. 2015. Discerning the healing path—How nurses assist patient spirituality in diverse health care settings. Journal of Clinical Nursing 24: 2926–35. [Google Scholar] [CrossRef] [PubMed]
- Glaser, Barney G. 1992. Basics of Grounded Theory Analysis. Mill Valley: Sociology Press. [Google Scholar]
- Glaser, Barney G., and Anselm L. Strauss. 1967. The Discvoery of Grounded Theory. Hawthorne: Aldine Publishing Company. [Google Scholar]
- Glaser, Barney G. 1978. Theoretical Sensitivity. Mill Valley: Sociology Press. [Google Scholar]
- Glaser, Barney G. 1998. Doing Grounded Theory: Issues and Discussions. Mill Valley: Sociology Press. [Google Scholar]
- Halldorsdottir, Sigridur. 2008. The dynamics of the nurse–patient relationship: Introduction of a synthesized theory from the patient’s perspective. Scandinavian Journal of Caring Sciences 22: 643–52. [Google Scholar] [CrossRef] [PubMed]
- Herlianita, Risa, Miaofen Yen, Ching-Huey Chen, Susan J. Fetzer, and Esther Ching-Lan Lin. 2018. Perception of spirituality and spiritual care among Muslim nurses in Indonesia. Journal of Religion and Health 57: 762–73. [Google Scholar] [CrossRef] [PubMed]
- Jacobs, Barbara Bennett. 2013. An innovative professional practice model: Adaptation of Carper’s patterns of knowing, patterns of research, and Aristotle’s intellectual virtues. Advances in Nursing Science 36: 271–88. [Google Scholar] [CrossRef] [PubMed]
- Jarrin, Olga. 2012. The integrality of situated caring in nursing and the environment. Advances in Nursing Science 35: 13–24. [Google Scholar] [CrossRef] [PubMed]
- Levin, Jeff. 2011. Energy healers: Who they are and what they do. Explore 7: 13–26. [Google Scholar] [CrossRef] [PubMed]
- McCance, Tanya, Brendan McCormack, and Jan Dewing. 2011. An exploration of person-centredness in practice. Online Journal of Issues in Nursing 16: 1. [Google Scholar] [CrossRef] [PubMed]
- McCormack, Brendan, Bengt Karlsson, Jan Dewing, and Anners Lerdal. 2010. Exploring person-centredness: A qualitative meta-synthesis of four studies. Scandinavian Journal of Caring Sciences 24: 620–34. [Google Scholar] [CrossRef] [PubMed]
- McCormack, Brendan, and Tanya V. McCance. 2006. Development of a framework for person-centred nursing. Journal of Advanced Nursing 56: 472–79. [Google Scholar] [CrossRef] [PubMed]
- Meleis, Afaf Ibrahim. 2007. Theoretical Nursing: Progress and Development, 4th ed. Philadephia: Lippincott, Williams & Wilkins. [Google Scholar]
- Minton, Claire, and Lesley Batten. 2016. Rethinking the intensive care environment: Considering nature in nursing practice. Journal of Clinical Nursing 25: 269–77. [Google Scholar] [CrossRef] [PubMed]
- Nightingale, Florence. 1992. Notes on Nursing: What It Is and What It Is Not. Philadelphia: J.B. Lippincott. [Google Scholar]
- O’Hagan, Sally, Elizabeth Manias, Catherine Elder, John Pill, Robyn Woodward-Kron, Tim McNamara, Gillian Webb, and Geoff McColl. 2014. What counts as effective communication in nursing? Evidence from nurse educators’ and clinicians’ feedback on nurse interactions with simulated patients. Journal of Advanced Nursing 70: 1344–55. [Google Scholar] [CrossRef] [PubMed]
- Paal, Piret, Kathleen Neenan, Yvonne Muldowney, Vivienne Brady, and Fiona Timmins. 2018. Spiritual leadership as an emergent solution to transform the healthcare workplace. Journal of Nursing Management 26: 335–37. [Google Scholar] [CrossRef] [PubMed]
- Pesut, Barbara, Marsha Fowler, Sheryl Reimer-Kirkham, Elizabeth J. Taylor, and Richard Sawatzky. 2009. Particularizing spirituality in points of tension: Enriching the discourse. Nursing Inquiry 16: 337–46. [Google Scholar] [CrossRef] [PubMed]
- Pfeiffer, Jane Bacon. 2014. Creating a Healing Environment: Strategies Christian Nurses Use. Ph.D. thesis, Loma Linda University, Azusa, CA, USA. [Google Scholar]
- Pfeiffer, Jane Bacon, Carla Gober, and Elizabeth Johnston Taylor. 2014. How Christian nurses converse with patients about spirituality. Journal of Clinical Nursing 23: 2886–95. [Google Scholar] [CrossRef] [PubMed]
- Pfettscher, Susan A. 2010. Florence Nightingale: Modern Nursing. In Nursing Theorists and Their Work. Edited by Martha R. Alligood and Ann M. Tomey. Maryland Heights: Mosby Elsevier. [Google Scholar]
- Sakallaris, Bonnie R, Lorissa Macallister, Megan Voss, Katherine Smith, and Wayne B Jonas. 2015. Optimal healing environments. Global Advances in Health and Medicine 4: 40–5. [Google Scholar] [CrossRef] [PubMed]
- Selanders, Louise C. 2010. The power of environmental adaptation: Florence Nightingale’s original theory for nursing practice. Journal of Holistic Nursing 28: 81–88. [Google Scholar] [CrossRef] [PubMed]
- Swanson, Kristen M., and Danuta M. Wojnar. 2004. Optimal Healing Environments in Nursing. Journal of Alternative & Complementary Medicine 10: S-43–48. [Google Scholar]
- Taylor, Elizabeth Johnston, Carla Gober Park, and Jane Bacon Pfeiffer. 2014. Nurse religiosity and spiritual care. Journal of Advanced Nursing 70: 2612–21. [Google Scholar] [CrossRef] [PubMed]
- Timmins, Fiona. 2011. Remembering the art of nursing in a technological age. Nursing In Critical Care 16: 161–63. [Google Scholar] [CrossRef] [PubMed]
- Wallach, Ari. 2017. How to Think like a Futurist. Available online: https://ideas.ted.com/three-ways-to-think-about-the-future/ (accessed on 10 March 2017).
- Watson, Jean. 1999. Postmodern Nursing and Beyond. Edinburgh: Churchill Livingstone. [Google Scholar]
- Woolley, Jennifer, Robin Perkins, Patty Laird, Jennifer Palmer, Mary Beth Schitter, Kelsie Tarter, Mindy George, Grace Atkinson, Katie McKinney, and McKenzie Woolsey. 2012. Relationship-based care: Implementing a caring, healing environment. MEDSURG Nursing 21: 179–84. [Google Scholar] [PubMed]
- Young, Jenny, Audrey Cund, Marian Renshaw, Angela Quigley, and Austyn Snowden. 2015. Improving the care of cancer patients: Holistic needs assessment. British Journal of Nursing 24: S17–20. [Google Scholar] [CrossRef] [PubMed]
- Zoinierek, Cynthia Diamond. 2014. An integrative review of knowing the patient. Journal of Nursing Scholarship 46: 3–10. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Charting the Healing Path Conceptual Model.

© 2018 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
MDPI and ACS Style
Pfeiffer, J. Strategies Christian Nurses Use to Create a Healing Environment. Religions 2018, 9, 352. https://doi.org/10.3390/rel9110352
AMA Style
Pfeiffer J. Strategies Christian Nurses Use to Create a Healing Environment. Religions. 2018; 9(11):352. https://doi.org/10.3390/rel9110352
Chicago/Turabian StylePfeiffer, Jane. 2018. "Strategies Christian Nurses Use to Create a Healing Environment" Religions 9, no. 11: 352. https://doi.org/10.3390/rel9110352
Note that from the first issue of 2016, this journal uses article numbers instead of page numbers. See further details here.