
Introduction of Spiritual Psychotherapy for Inpatient, Residential, and Intensive Treatment (SPIRIT) in The Netherlands: Translation and Adaptation of a Psychotherapy Protocol for Mental Health Care

 , , , , ,
, , , , ,
Abstract
:1. Introduction
2. Materials and Methods
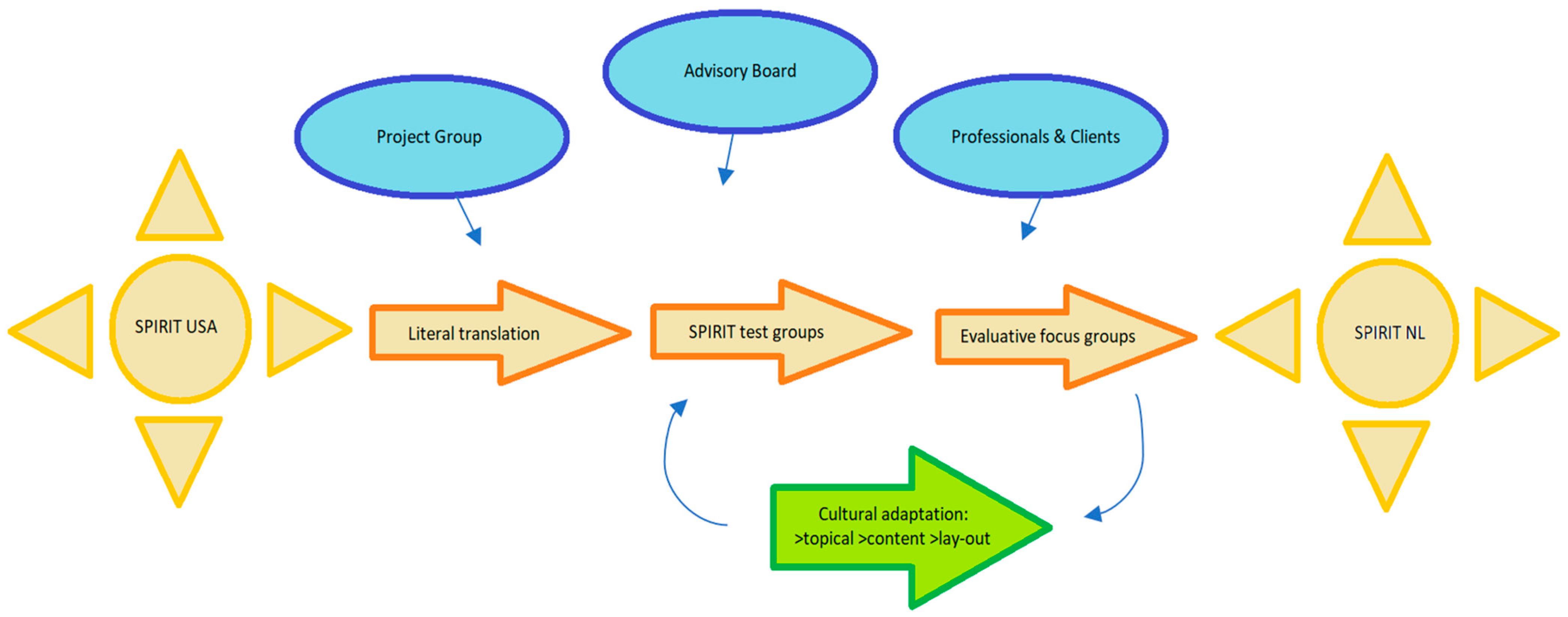
2.1. Research Design
2.2. Procedure
2.3. Analysis
3. Results
3.1. Initial Receipt
“I liked it very much. Of all the modules, I find this one the most profound. Also, to incorporate religion […] also when dealing with suicidal thoughts, and contemplating the meaning of everything, yes, faith is a significant source of strength for me. Sometimes, it’s the only thing I still derive strength from” (woman, test SPIRIT group original protocol, Christian institution).
“Why has this not yet been further disseminated?” (man, test SPIRIT group original protocol, secular institution).
3.2. Adaptation Process
3.2.1. Content
3.2.2. Topics
- Text fragment:
“Have you ever wondered how achievable life is? To what extent are you responsible for your own recovery? Are you always free to make the choices you want to make? Illness brings about a lack of freedom, where the ability to shape your own life becomes limited. Yet, you are often expected to articulate your desires. Stepping back might be beneficial. What beliefs do you hold about freedom, autonomy, and responsibility? Here, a series of questions and answers are listed. Which ones are helpful, and which ones would you prefer to let go of?”
- Text fragment:
“Every person has a need for love and the capacity to give love. Loneliness arises from not feeling seen, heard, or loved. Mental issues can result from missed love, yet they can also cause the absence of love because we may function differently than usual. Often, it is challenging to love ourselves. However, that’s a crucial key to experiencing love from others and being able to love others. Discuss the love you feel you’re missing or have missed. Identify from whom you have experienced or still experience love. Then choose one of the following texts, and consider why and how you can love yourself. Why is this important?”
- Text fragment:
“No one lives without examples. Of course, your father and mother can be examples, or quite the opposite. Others from your own neighborhood, family, or ancestry can also serve as examples, like a neighbor, grandmother or grandfather, uncle or aunt, or ancestor. Role models are often positive examples. Sometimes, they also show how not to do things and how you never want to be. Many well-known individuals are also examples for many. Often, they represent ways of dealing with difficulties and problems.”
- Text fragment:
In life, there is also loss, the letting go of what you once cherished. When you have been dealing with mental health issues for a while, undoubtedly, you have lost people or things that were important to you. Unfortunately, this aspect is often not discussed. However, taking a moment to reflect on and identify what you have lost can be helpful.
What have you lost? These can be very different things. Try to write down two significant things that you have lost for yourself. A few examples of what people might have lost due to mental health issues include the ability to pursue the career they wanted, a group member who left and never contacted them again, someone who died by suicide, dreams for the future, hope for a better future, the ability to feel and enjoy things, concentration, sleep or interest in the day.
3.2.3. Layout and Form
3.3. Secondary Receipt
“I appreciate the playfulness of the word cloud, the pinboard, and the card game. It makes it more interactive and requires participation as a group or participant to engage in thinking. It also seems to have expanded with more than just the usual philosophies, which I think will appeal to a lot of people” (patient, secular institution, adapted protocol).
“This really resonates with me” (patient, secular institution, adapted protocol).
“I often contemplate the meaning of life in my current situation” (patient focus group secular institution, adapted protocol).
“After participating in this group, I feel that my time is better spent here than in the psycho-education group twice a week” (patient, secular institution, adapted protocol).
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Akwa GGz. 2023. Generieke module Zingeving in de psychiatrische hulpverlening. [Practical guideline ‘Meaning & Spirituality in Dutch Mental Health Care’]. Available online: https://www.ggzstandaarden.nl/zorgstandaarden/zingeving-in-de-psychische-hulpverlening (accessed on 10 August 2023).
- Anbeek, Christa W. 2017. World-viewing dialogues on precarious life: The urgency of a new existential, spiritual, and ethical language in the search for meaning in vulnerable life. Essays in the Philosophy of Humanism 25: 171–85. [Google Scholar] [CrossRef]
- Anderson, Naomi, Suzanne Heywood-Everett, Najma Siddiqi, Judy Wright, Jodi Meredith, and Dean McMillan. 2015. Faith adapted psychological therapies for depression and anxiety: Systematic review and meta-analysis. Journal of Affective Disorders 176: 183–96. [Google Scholar] [CrossRef]
- Baum, Fran, Colin MacDougall, and Danielle Smith. 2006. Participatory action research. Journal of Epidemiology and Community Health 60: 854–57. [Google Scholar] [CrossRef] [PubMed]
- Bernts, Ton, and Joantine Berghuijs. 2016. God in Nederland 1966–2015 [God in the Netherlands 1966–2015]. Utrecht: Ten Have. [Google Scholar]
- Bouwhuis-Van Keulen, Annette J., Jurrijn Koelen, Liesbeth Eurelings-Bontekoe, Christien Hoekstra-Oomen, and Gerrit Glas. 2023. The evaluation of religious and spirituality-based therapy compared to standard treatment in mental health care: A multi-level meta-analysis of randomized controlled trials. Psychotherapy Research: Journal of the Society for Psychotherapy Research, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Braam, Arjan W., and Peter J. Verhagen. 2022. Levensbeschouwelijke diversiteit: Mozaïek en dynamiek. Tijdschrift voor Psychiatrie 64: 535–39. [Google Scholar] [PubMed]
- Brijan, Bernice. 2020. Existential loss in the face of mental illness: Further developing perspectives on personal recovery in mental health care. Phenomenology and Mind 18: 250–58. [Google Scholar] [CrossRef]
- Cameron, William B. 1963. Informal Sociology: A Casual Introduction to Social Thinking. New York: Random House. [Google Scholar]
- Captari, Laura E., Steven J. Sandage, and Richard A. Vandiver. 2022. Spiritually integrated psychotherapies in real-world clinical practice: Synthesizing the literature to identify best practices and future research directions. Psychotherapy 59: 307–20. [Google Scholar] [CrossRef] [PubMed]
- CBS. 2020. Religie in Nederland. Available online: https://longreads.cbs.nl/nederland-in-cijfers-2020/welk-geloof-hangen-we-aan/ (accessed on 28 November 2023).
- Cornish, Flora, Nancy Breton, Ulises Moreno-Tabarez, Jenna Delgado, Mohi Rua, Ama de-Graft Aikins, and Darrin Hodgetts. 2023. Participatory action research. Nature Reviews Methods Primers 3: 34. [Google Scholar] [CrossRef]
- Fallot, Roger D. 2007. Spirituality and religion in recovery: Some current issues. Psychiatric Rehabilitation Journal 30: 261–70. [Google Scholar] [CrossRef]
- Fitchett, George, L. A. Burton, and A. B. Sivan. 1997. The religious needs and resources of psychiatric inpatients. The Journal of Nervous and Mental Disease 185: 320–26. [Google Scholar] [CrossRef]
- Glas, Gerrit. 2003. Anxiety-Animal Reactions and the Embodiment of Meaning. In Nature and Narrative—An Introduction to the New Philosophy of Psychiatry. Edited by B. Fullord, K. Morris, J. Z. Sadler and G. Stanghellini. Oxford: Oxford University Press, pp. 231–49. [Google Scholar]
- Gonçalves, Juliane P. B., Giancarlo Lucchetti, Paulo R. Menezes, and Homero Vallada. 2015. Religious and spiritual interventions in mental health care: A systematic review and meta-analysis of randomized controlled clinical trials. Psychological Medicine 45: 2937–49. [Google Scholar] [CrossRef] [PubMed]
- Handley, Margaret A., Anuradha Gorukanti, and Adithya Cattamanchi. 2016. Strategies for implementing implementation science: A methodological overview. Emergency Medicine Journal: EMJ 33: 660–64. [Google Scholar] [CrossRef]
- Hare-Duke, Laurie, Ashleigh Charles, Mike Slade, Stefan Rennick-Egglestone, Ada Dys, and Daan Bijdevaate. 2023. Systematic review and citation content analysis of the CHIME framework for mental health recovery processes: Recommendations for developing influential conceptual frameworks. Journal of Recovery in Mental Health 6: 38–44. [Google Scholar] [CrossRef] [PubMed]
- Heinrich, Liesl M., and Eleonora Gullone. 2006. The clinical significance of loneliness: A literature review. Clinical Psychology Review 26: 695–718. [Google Scholar]
- Hem, Marit H., Elisabeth Gjerberg, Tonje L. Husum, and Reidar Pedersen. 2018. Ethical challenges when using coercion in mental healthcare: A systematic literature review. Nursing Ethics 25: 92–110. [Google Scholar] [CrossRef] [PubMed]
- Huber, Machteld, Marja van Vliet, Michele Giezenberg, Bjorn Winkens, Yvonne F. Heerkens, Pieter C. Dagnelie, and J. Anré Knottnerus. 2016. Towards a ‘patient-centred’ operationalisation of the new dynamic concept of health: A mixed methods study. BMJ Open 6: e010091. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, Caroline C., David H. Rosmarin, and Hilary Connery. 2022. Integrating Spirituality in Group Psychotherapy with First Responders: Addressing Trauma and Substance Misuse. Religions 13: 1132. [Google Scholar] [CrossRef]
- Koenig, Harold G. 2009. Research on Religion, Spirituality, and Mental Health: A Review. The Canadian Journal of Psychiatry 54: 283–91. [Google Scholar] [CrossRef] [PubMed]
- Koenig, Harold G., Michelle Pearce, Bruce Nelson, Sally Shaw, Clive Robins, Noha Daher, Harvey Jay Cohen, and Michael B. King. 2016. Effects of religious vs. standard cognitive behavioral therapy on therapeutic alliance: A randomized clinical trial. Psychotherapy Research: Journal of the Society for Psychotherapy Research 26: 365–76. [Google Scholar] [CrossRef] [PubMed]
- Kruijthoff, Dick J. 2023. Healing after Prayer, an Interdisciplinary Case Study. Ph.D. thesis, Research and Graduation Internal, Vrije Universiteit Amsterdam, Amsterdam, The Netherlands. [Google Scholar] [CrossRef]
- La Cour, Peter, and Niels C. Hvidt. 2010. Research on meaning-making and health in secular society: Secular, spiritual and religious existential orientations. Social Science & Medicine (1982) 71: 1292–99. [Google Scholar] [CrossRef]
- Lucchetti, Giancarlo, Rodrigo M. Bassi, and Alessandra L. Lucchetti. 2013. Taking spiritual history in clinical practice: A systematic review of instruments. Explore 9: 159–70. [Google Scholar] [CrossRef] [PubMed]
- Lukoff, David, Francis Lu, and Robert Turner. 1992. Toward a more culturally sensitive DSM-IV. Psychoreligious and psychospiritual problems. The Journal of Nervous and Mental Disease 180: 673–82. [Google Scholar] [CrossRef] [PubMed]
- Moreira-Almeida, Alexander, Avdesh Sharma, Bernard Janse van Rensburg, Peter J. Verhagen, and Cristopher C. H. Cook. 2016. WPA Position Statement on Spirituality and Religion in Psychiatry. World Psychiatry 15: 87–88. [Google Scholar] [CrossRef] [PubMed]
- Paas, Stefan. 2012. Religious Consciousness in a Post-Christian Culture: J.H. Bavinck’s Religious Consciousness and Christian Faith (1949), Sixty Years Later. Journal of Reformed Theology 6: 35–55. [Google Scholar] [CrossRef]
- Pargament, Kenneth I., and James W. Lomax. 2013. Understanding and addressing religion among people with mental illness. World Psychiatry 12: 26–32. [Google Scholar] [CrossRef] [PubMed]
- Pargament, Kenneth I., Harold G. Koenig, and Lilian M. Perez. 2000. The many methods of religious coping: Development and initial validation of the RCOPE. Journal of Clinical Psychology 56: 519–43. [Google Scholar] [CrossRef]
- Park, Crystal L. 2005. Religion as a Meaning-Making Framework in Coping with Life Stress. Journal of Social Issues 61: 707–29. [Google Scholar] [CrossRef]
- Poole, Rob. 2020. The sacred versus the secular in UK psychiatry. BJPsych Advances 26: 285. [Google Scholar] [CrossRef]
- Poole, Rob, and Robert Higgo. 2011. Spirituality and the threat to therapeutic boundaris in psychiatric practice. Mental Health Religion & Culture 14: 19–29. [Google Scholar] [CrossRef]
- Rosmarin, David H., Sarah Salcone, David G. Harper, and Brent Forester. 2021. Predictors of Patients’ Responses to Spiritual Psychotherapy for Inpatient, Residential, and Intensive Treatment (SPIRIT). Psychiatric Services 72: 507–13. [Google Scholar] [CrossRef]
- Rosmarin, David H., Sarah Salcone, David Harper, and Brent P. Forester. 2019. Spiritual Psychotherapy for Inpatient, Residential, and Intensive Treatment. American Journal of Psychotherapy 72: 75–83. [Google Scholar] [CrossRef]
- Santiago, Pia N., and Terry L. Gall. 2016. Acceptance and Commitment Therapy as a Spiritually Integrated Psychotherapy. Counseling and Values 61: 239–54. [Google Scholar] [CrossRef]
- Schaap-Jonker, Hanneke. 2022. How Clinical Psychology of Religion Can Support Mental Health: An Ecological–Existential View, Illustrated by the Case of Shame. Religions 13: 1009. [Google Scholar] [CrossRef]
- Theobald, Sally, Neal Brandes, Margaret Gyapong, Sameh El-Saharty, Enola Proctor, Theresa Diaz, Samuel Wanji, Soraya Elloker, Joanna Raven, Helen Elsey, and et al. 2018. Implementation research: New imperatives and opportunities in global health. The Lancet 392: 2214–28. [Google Scholar] [CrossRef] [PubMed]
- Thrash, Todd M., and Andrew J. Elliot. 2003. Inspiration as a psychological construct. Journal of Personality and Social Psychology 84: 871–89. [Google Scholar] [CrossRef] [PubMed]
- van Bruggen, Vincent, Joël Vos, Gerben Westerhof, Ernst Bohlmeijer, and Gerrit Glas. 2015. Systematic review of anxiety instruments. Journal of Humanistic Psychology 55: 173–201. [Google Scholar] [CrossRef]
- VanderWeele, Tyler J. 2017. Religion and health: A synthesis. Spirituality and Religion within the Culture of Medicine: From Evidence to Practice 419: 357–401. [Google Scholar]
- van Nieuw Amerongen-Meeuse, Joke C., Hanneke Schaap-Jonker, Gerlise Westerbroek, Christa Anbeek, and Arjan W. Braam. 2020. Conversations and Beyond: Religious/Spiritual Care Needs Among Clinical Mental Health Patients in the Netherlands. The Journal of Nervous and Mental Disease 208: 524–32. [Google Scholar] [CrossRef] [PubMed]
- Yalom, Irvin D. 1980. Existential Psychotherapy. New York: Basic Books. [Google Scholar]


{kind=link}
| Total Project Group | Advisory Board | Caregiver Evaluations | Patient Focus Groups | Working Group | |
|---|---|---|---|---|---|
| Members | Multidisciplinary group: psychologists, psychiatrists, nurses, clients, spiritual counselers, academics | Prof. Dr. Arjan Braam Prof. Dr. Peter J. Verhagen Prof. Dr. Hanneke Schaap-Jonker Prof. Dr. Rogier Hoenders Dr. David H. Rosmarin | Caregivers providing test SPIRIT groups | Patients of Christian and secular institutions | Two spiritual counselors Nurse specialist Psychiatrist Researcher |
| N | 10–15 | 3–5 | 2–3 | 4–6 per group | 5 |
| Meetings | 23 June 2022 18 October 2022 27 March 2023 8 May 2023 30 August 2023 | 8 July 2022 12 September 2022 14 November 2022 27 November 2023 | 10 February 2023 30 March 2023 | 11 April 2023 23 June 2023 30 November 2023 | 5 July 2023 13 September 2023 11 November 2023 |
| SPIRIT USA | SPIRIT NL |
|---|---|
| (1) Philosophical beliefs and reframes | (1) Philosophical beliefs and reframes |
| (2) Meaning and coping in treatment | (2) Meaning and coping in treatment |
| (3) Spiritual/religious struggles | (3) Spiritual/religious and meaning struggles |
| (4) Inspiring verses | (4) Inspiring verses from |
| …philosophical/humanistic views (a) | |
| …Judeo-Christian views (b) | |
| …Buddhist views (c) | |
| …Islamic views (d) | |
| …Hindu views (e) | |
| (5) Meditating on the Psalms | (5) Autonomy, responsibility, and liberty |
| (6) The power of prayer | (6) Loneliness and belonging |
| (7) Forgiveness | (7) Inspiring persons in the past and present |
| (8) The power of meditation and prayer | |
| (9) Grief and loss | |
| (10) Releasing and forgiveness |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Nieuw Amerongen, J.C.; Ouwehand, E.; Graaf, N.d.; van Parijs, L.; Schaap-Jonker, H.; Braam, A.W.; Verhagen, P.J.; Rosmarin, D.H.; van den Brink, B. Introduction of Spiritual Psychotherapy for Inpatient, Residential, and Intensive Treatment (SPIRIT) in The Netherlands: Translation and Adaptation of a Psychotherapy Protocol for Mental Health Care. Religions 2024, 15, 253. https://doi.org/10.3390/rel15030253
van Nieuw Amerongen JC, Ouwehand E, Graaf Nd, van Parijs L, Schaap-Jonker H, Braam AW, Verhagen PJ, Rosmarin DH, van den Brink B. Introduction of Spiritual Psychotherapy for Inpatient, Residential, and Intensive Treatment (SPIRIT) in The Netherlands: Translation and Adaptation of a Psychotherapy Protocol for Mental Health Care. Religions. 2024; 15(3):253. https://doi.org/10.3390/rel15030253
Chicago/Turabian Stylevan Nieuw Amerongen, Joke C., Eva Ouwehand, Nienke de Graaf, Linda van Parijs, Hanneke Schaap-Jonker, Arjan W. Braam, Peter J. Verhagen, David H. Rosmarin, and Bart van den Brink. 2024. "Introduction of Spiritual Psychotherapy for Inpatient, Residential, and Intensive Treatment (SPIRIT) in The Netherlands: Translation and Adaptation of a Psychotherapy Protocol for Mental Health Care" Religions 15, no. 3: 253. https://doi.org/10.3390/rel15030253