1. Introduction
Health, particularly the health of the community in the 21st century, is far more complex than the delivery of individualized healthcare and a person’s active response (
Capewell and Capewell 2018). In contrast, the effectiveness paradigm suggests treating the community in order to engage the individual in treatment that is not solely dependent on individual action and responsibility (
Capewell and Capewell 2018). Prevention and implementation of evidence-based practices (EBP) for the population’s health requires partnerships between organizations and settings whose primary mission is not health related, yet they are highly influential in the everyday lives, values, and practices of their constituents (
Raphael and Colvin 2017).
Individual actions are always submerged in and influenced by the environment (setting/surroundings) of the community. The social determinants of health (SDoH) are defined as the conditions “in which people are born, grow up, live, work, and age, that affect a wide range of health, functioning, and quality-of-life outcomes and risks” (
Raphael and Colvin 2017). These elements are essential to the assessment of a community and its perspective on community health.
This study examines the qualitative assessment data of a southern California community’s perception of its health and of barriers to improving health. The qualitative research aims to extend the initial published quantitative findings (
Pfeiffer et al. 2018). The Integrated Theory of Health Behavior Change (ITHBC) (
Ryan 2009) was adapted for the quantitative results where religious self-regulation and religious-self management behaviors contributed to one particular health outcome, healthy eating behaviors. Structural Equation Modeling (SEM) analysis conducted on N = 261 questionnaires validated the strong positive effect of religious self-regulation skills and ability on how frequently individuals engage in both organized and non-organized religious activities. Similarly, SEM confirmed a significant positive impact of religious self-management behaviors toward healthy eating behaviors. However, the likelihood of healthy food intake was reduced without the moderating effect of engagement in religious activities (self-management behaviors). This faith-related theoretical model provides an opportunity for faith-based organizations to contribute to community health promotion.
Before addressing the qualitative results, a review of upstream social determinants of health, downstream illness and disease outcomes, and facilitators of health is given. Exploration of these concepts will aid in the description of qualitative findings for this at-risk community.
1.1. Upstream Social Determinants
The Raphael article mentioned above (
Raphael and Colvin 2017) provides a framework for understanding SDoH as substantial contributors to illness or health that are beyond the control of the individual or individual lifestyle choices. Another benefit of a broader SDoH integrated approach to healthcare is the shift in focus to upstream factors that influence health versus the traditional healthcare focus on treating the downstream presentation of disease. Additionally, in the USA the 2010 Patient Protection and Affordable Care Act (PPACA, hereafter cited as the ACA) community benefit funding requires hospitals to address pre-disease and illness factors influencing health at the community level.
An explanation of upstream social determinants given by
Braveman et al. (
2011) describes these determinants as fundamental causes that flow downward and interact to produce increased health risks and negative health effects, known as illness and disease. The causal role of poor health outcomes may include lack of infrastructure and resources afforded to more affluent communities, “health related knowledge, attitudes, beliefs, or behaviors…as well as social disadvantage, risk exposure, and social inequities” (
Bharmal et al. 2015, p. 6).
Begun et al. (
2018) employ the “cliff analogy” to evaluate how SDoH interventions are addressed by hospital community health prevention efforts. These interventions move individuals and populations from the edge of the cliff, thereby reducing individual and population risk. This helps to address issues before individuals have fallen off the cliff (become ill).
Islam (
2019) asserts the everyday social and economic resources that support or detract from health are located at a mid-level between upstream policy determinants and downstream individually focused interventions.
1.2. Downstream Illness and Disease Outcomes
The Center for Disease Control and Prevention (CDC) has become increasingly concerned with
prevention of downstream illness and disease outcomes, whether biological, social, or environmental in nature (
Brownson et al. 2010).
Marmot (
2015) upholds the research findings of the WHO Commission on Social Determinants of Health—that a social gradient affecting the quality of daily life is present in factors of money, power, and distribution of resources for health. To acknowledge and tackle this social gradient and its consequent inequalities and inequities requires a change in focus, a change from downstream interventions to upstream thinking and interventions toward facilitators of healthy behaviors and outcomes.
1.3. Facilitators of Health
A healthy community is one that has the ability to improve not only the physical and social environment but also enhance the quality of life and support for community members (
Doyle et al. 2019). The community can foster four important facilitators of health: advancing social connection, community-based care, collaborative community partnerships, and the church as a community of care.
Advancing social connection. The literature supports social connection and supportive relationships as contributors to health behaviors and outcomes even if causal mechanisms and pathways are still being validated (
Amaro et al. 2021;
Holt-Lunstad et al. 2017;
Pietromonaco and Collins 2017;
Werner-Seidler et al. 2017). Advancing social connection as a public health priority is proposed as an SDoH of the same magnitude/scale with potential to reduce mortality and morbidity effects equivalent to those of diet, exercise, smoking cessation, and anger and violence reduction strategies (
Holt-Lunstad et al. 2017).
Community-based care. The care provided in a local neighborhood often influences positive health outcomes, offers hope, and provides a connection with the required resources. Three examples follow: First, for a decade and more, the Nurse-Family Partnership (
Hernández et al. 2019) has provided home visits for new moms for a period of two plus years with documented outcomes of improved physical, social, and emotional health and economic stability. Second,
DeHaven et al. (
2020) describes two decades of focused community health science work to support community-based care in South Dallas, Texas, with the goal of decreasing chronic disease and addressing SDoH in vulnerable communities. Third, community health workers (CHWs) from New Mexico have been a cultural and social bridge for health and social services in New Mexico for rural and lower socio-economic status patients and families since the 1960s (
Community Health Workers n.d., sect. 6). Informed CHWs have become navigation specialists for health and non-health sector services (
Toney et al. 2022)
Collaborative community partnerships. Collaborative partnerships within the healthcare system include the local, hospital emergency department (ED) (
Walter et al. 2021), the anchor meds/eds, those large-scale hospitals (anchor meds) or educational institutions (anchor eds) that “invest in their communities as a way of doing business” (
Resnicow et al. 2005, p. 339), and governmental public health departments. Each of these are pressed to address the SDoH of their clients, and to meet the “community benefit guidelines” of the community health needs assessment (CHNA) requirement of the ACA. Providers of health and social care outside the formalized healthcare system can range from schools to churches to civic organizations to universities and other not-for-profit groups that seek the well-being of their community. These facilitators of health must be strategically addressed with partners that have the readiness, capacity, and commitment to engage lest the community members become jaded because of good intentions with little outcome of the long-term local improvement in the community health and well-being.
The church as a community of care. Local congregations are uniquely positioned to be a community of care. Few organizations have the cadence of influence to their congregants/adherents as much as the local church. Due to the prevalent nature of their contact, influence, and direction, churches can speak into the lives of those attending regarding all types of values, including health (
Ayton et al. 2016). A local church that has the health of its congregants as a priority can speak into the open and opening values systems within the congregation. People attend their local faith communities for a myriad of reasons, but information, input, and spiritual direction and life choices are among these reasons. Fellowship, insight, and a sense of community health and well-being are other reasons as well. As such, the leaders of the faith community can seek to encourage their congregants to increase the value of health in their lives and can do this in a practical and meaningful way. Encouraging a congregation to be both a place of health and a place where people can learn about health is the goal to increase the capacity of a local church to become not only part of a continuum of care but to also become a community of care as well (
Pfeiffer et al. 2018).
With advancing social connection, community-based care, collaborative community partnerships, and the church as a community of care, there is skill, science, and perspective to address the upstream, midstream, and downstream determinants of health for all, especially the disadvantaged, at a local level.
2. Materials and Methods
The purpose of this sequential explanatory mixed method approach is to assess a Southern California community’s perception of its health and of barriers to improving health. The mixed methods approach is useful to further explain the initial quantitative results. This study is a multi-university, multidisciplinary, and CBPR project consisting of a team of researchers from a school of public health, a university school of nursing, and a local church that described member perceptions of their community and contributors/barriers to community health.
Community-based participatory research (CBPR) is a research method used with underserved and marginalized populations to assess and address the health disparities, inequities, and social and health outcomes faced by these communities (
DeHaven et al. 2020;
Dickinson et al. 2020).
Dickinson et al. (
2020) assert (CBPR) is constructed to support the “mutual contribution…by all partners with the core goal of addressing inequities in social and health outcomes faced by underserved populations and communities” (p. 51). Its design assists care providers to actively hear and partner with the local community in setting goals and developing strategic pathways toward improved health.
The aim of the project was collaboration with the neighborhood to assess its understanding of community and improve the community’s health within a one-mile radius of the local church. The church’s location was an intersection of four southern California zip codes with a diversity of racial, ethnic, and socio-economic status. The informed consent and ethical approval for this study was given by the Azusa Pacific University, study 71-16-Church.
2.1. Data
Following the quantitative assessment, focus groups were conducted (N = 21) with community members chosen in collaboration with local school administrations. School administrators helped identify key community members for focus group participation. No specific list of inclusion or exclusion criteria were given to the administrators. However, the administrators were asked to select people who lived in these four zip codes and were members of the school community who could speak on behalf of other parents. School administers provided the initial contacts and extended invitation to participate in focus groups providing a warm handoff to the researchers.
No attempt was made to systematically compare the characteristics of those who agreed to or were asked to participate with those who did not. Therefore, in this convenience sample, no direct comparisons could be made with all potential participants.
At the beginning of the meeting of the focus groups, the participants received information on the study and were reminded of the confidentiality rule. Agreement to participate in the focus group was considered to be consent and no individual identifiable data or written consents were obtained to protect the identity of the participants. Three of the four focus group interviews were conducted by the primary investigator (PI) lasting 60–75 min. The fourth, a Spanish only speaking group of moms, was conducted by a Spanish-speaking graduate nursing research assistant (RA) with a bilingual school counselor and the PI present for clarification if needed. This group met twice over 2 weeks, each time for 45–60 min. Three groups were tape recorded, one had dictation recording, and all were transcribed for data analysis. The participants were informed that the focus groups would be recorded prior to the start of the discussion. The participants were given the option to refuse participation without any negative consequences. The interview addressed the participants’ definition or understanding of community, community membership, community health, and what, in their perception, would improve the sense of community and community health. See
Table 1 for sample focus group interview questions.
2.2. Analysis
Qualitative content analysis was used to analyze the study data.
Elo and Kyngäs (
2008) assert that
Content analysis as a research method is a systematic and objective means of describing and quantifying phenomena (
Krippendorff 2018;
Downe-Wamboldt 1992;
Sandelowski 1995). It is also known as a method of analyzing documents. Content analysis allows the researcher to test theoretical issues to enhance their understanding of the data. Through content analysis, it is possible to distil words into fewer content-related categories
(p. 108)
Content analysis employs constant comparison, reflexivity, and coding and category consensus among researchers to make sense of the data and achieve rigor (
Forman and Damschroder 2007). Qualitative content analysis applied to this project involved three steps: choosing the unit of analysis, naming categories, and determining themes that help link the meanings present in these established categories (
Cho and Lee 2014).
Three analysts read and coded the first interview together to describe and distinguish similarities and differences in coding. Subsequent codes and categories were identified as each researcher independently coded the remaining three interviews and comparisons were made. In the initial analysis several major barriers were identified and their descriptions and memos were written to guide and to organize the next steps. The barriers were listed and grouped into categories that were correlated to the broad thematic review of the literature’s categories of upstream contributors, downstream results, or facilitators of health. Consensus was achieved to locate the best fit of barriers within this broad thematic framework, based on the participants’ descriptions of their concerns. Examples are given below.
Definitions of community, the role of place and information, and some factors did not fit neatly into the broad themes. Rather, a positive aspect could fit the middle level or upstream contributor and the negative component of the same element would best fit the downstream result. For example, “trust others” was repeatedly voiced as a facilitator of health at the neighborhood and the individual level, so it was merged into the category of connection. Decreased trust of others was seen as having downstream effects in both connection and fear/anxiety categories. Thus, when given the specific positive or negative description, the researchers determined the best fit with discussion until consensus was achieved.
Categories and other findings were shared with the school counsellor involved in one school’s focus groups and with the principal of the second school. Both agreed they had similar observations when they made home visits or had family appointments at the school. Other attempts at member checking were interrupted because of changes in school administration, the COVID epidemic with subsequent lock down, restricted access to the school/staff, and some moms no longer having children at that school. Further efforts to check members were abandoned.
3. Results
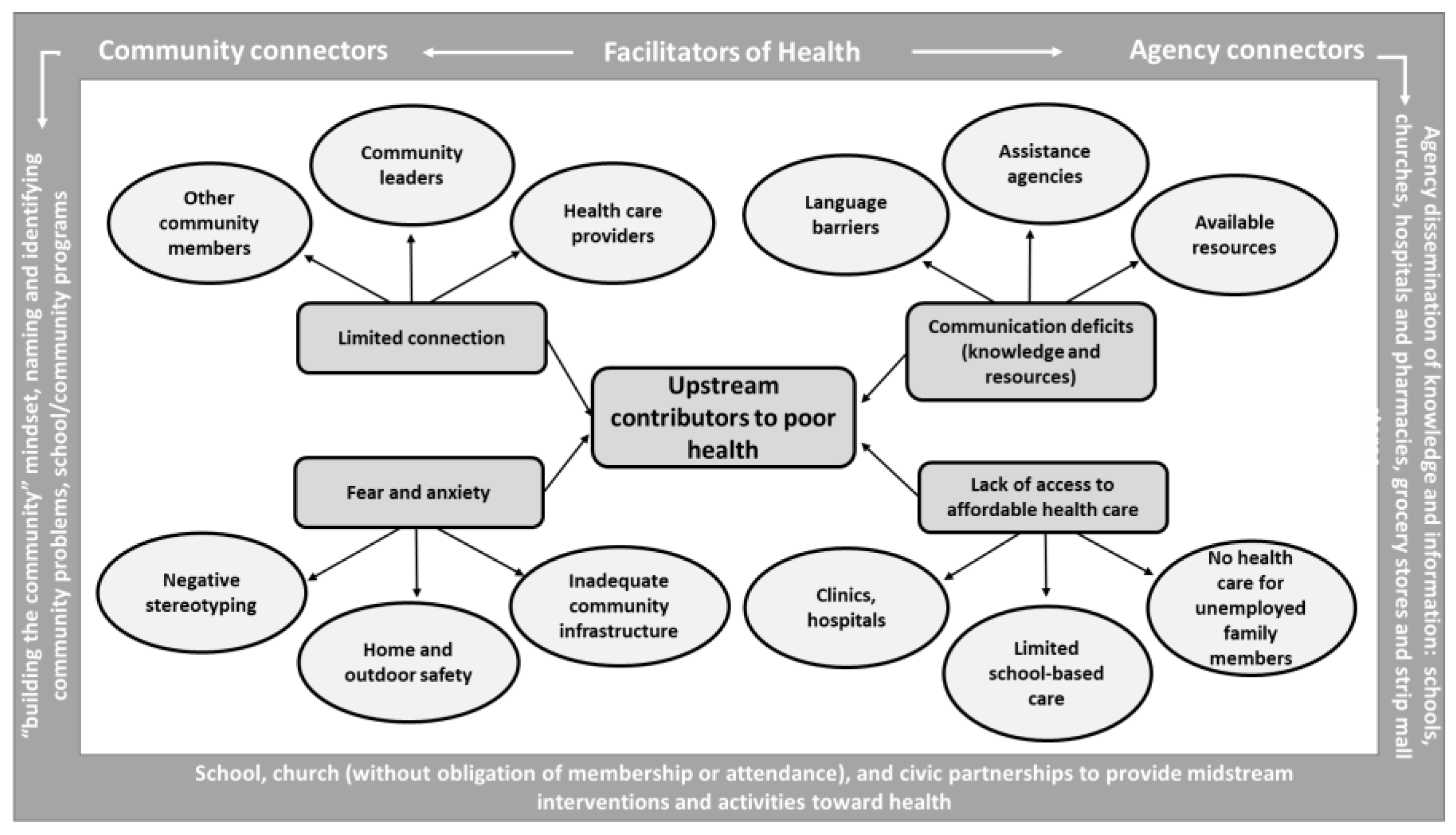
The analysis of focus group transcripts resulted in six major categories from which two were reclassified and four overarching categories of upstream contributors to lack of health and well-being were identified as 1. limited community connection—disrupted and/or decreased connectedness; 2. deficient communication—regardless of language of origin and literacy skills; 3. fear and anxiety—at both the individual and community level; and 4. inadequate access to and lack of affordable healthcare—sometimes lack of care. These upstream contributors to lack of community health reflect different snapshots of the community than the quantitative portion of the study. The emphasis of the qualitative study is the perception of the community, community health, and what contributes to or acts as a barrier to health in the community.
3.1. Limited Community Connection
The paradox of connection was experienced as participants of one group compared their sense of community in the past with the present as “everyone used to come and go away [referring to morning school drop off of children] and now we sit, get together…talk and see how the situation is and we all contribute” (participant mom). Simultaneously, these women voiced a desire for help to preserve spaces to allow more connections with neighbors; i.e., streets/areas for walking, safe passage for kids within the neighborhood, and physical health/exercise options.
Many of these former areas that encouraged connection have seen changes with small family businesses and the safety and community investment they promoted replaced by “big business and warehouse structures” that disregard the concept of connectedness within the community of the location. One participant expressed frustration at no longer being able to walk to the grocery store, stating “Now one has to drive or ride a bus,” which further hinders space and location sharing of life together. Thus, the downstream results of big business results in a sense of “other” versus neighbor, spatial and relational distance in knowing the “other,” and a guardedness which has developed toward the other.
Another contributor to the disrupted connectedness was the work schedules necessary in this low socioeconomic status (SES) area: either both parents were working, often with separate shifts, so one was always at home with the children, working nights and doing the absolute minimum of daytime activities to provide bookend support of their children’s needs, and in both of these cases, the absence of adult supportive relationships. Thus, connectivity has an economic edge, which often limits availing oneself of the resources present, however limited they are.
3.2. Deficient Communication
Deficient communication was described by participants as “an information gap,” “lack of awareness of events/activities,” and “lack of knowledge of available resources” that could have contributed positively to the needs of the family and community if they had been known. The information deficit was complicated by enclaves of people speaking only their dialect of origin. These informants interviewed from the four area codes were largely English or Spanish speakers, but they acknowledged many language groups they could not communicate with due to the absence of a common language. Lack of knowledge and lack of connection contributed to lack of health for individuals and community members, as well as the presence of fear. One mother verbalized “I’m afraid of the security of the house…worried that no one gets in to steal.” Another stated, “I’m afraid of being alone.”
3.3. Fear and Anxiety
Three aspects of the fear and anxiety participants experienced were (1) when individuals or localities were negatively labeled, (2) safety issues that were not addressed, and (3) the overburdened and, at times, unresponsive civic infrastructures of law enforcement and transportation/road repair. Application of labels to individuals as felt by these participants ranged from being labeled “a drug seeker” by the healthcare system when needing pain medication, to the “behavioral disorder or learning disabled” condition of a child by the school system, to more broad labels of illiterate, crazy, or disturbed by others in the community. Labels can assist in accessing services, and yet, they often serve to alienate, distance, or disadvantage members from the very services needed.
Two participants spoke of stigmas attached to labels, especially when mental health services are accessed, and subsequently, the person is perceived as crazy or challenged. Others described acting out behaviors seen in a group setting, i.e., a child in the school play yard or classroom is given the label of a “problem child.” Labels applied to the community included low SES, the presence of homeless or transients, a “dangerous place” to be after the 2010 area bombing incident, and presence of drug dealers and users hanging around the convenience store one block from one of the elementary schools.
Fear of physical threat or injury accompanied some explicit safety issues and were sometimes complicated by the lack of a common language. Several examples follow to illustrate this at-risk, vulnerable status. When cars are speeding on two-lane neighborhood streets without sidewalks, the fear is not only of children being hit while walking on the street, but cars veering out of control. Thus, it is no longer safe to play in one’s enclosed front yard space. When homeless or transient people are found in one’s own home, members expressed fear of a hostile, violent response, affecting themselves and the children involved, as well as lack of others to call for help. Older kids bullying younger kids in after-school environments leaves a fear of resolving the conflict for a lone adult, as well as fear of later reprisal for the child when no adult is present.
Individuals reported attempts to engage police have been unsatisfactory in terms of help or a positive outcome. Seeing unknown cars and persons in the neighborhood results in emotional fear and anxiety of “outsiders” that increases one’s sense of risk of injury or harm. These fears can grow to become pervasive and color one’s outlook on daily life. One participant stated, “There are more risks for children because they are not very safe.” This lack of safety and disrupted sense of connection was mirrored in the lack of healthcare, which is presented next.
3.4. Inadequate Access to Affordable Healthcare
Many participants expressed inadequate access to and lack of affordable healthcare. A few members with English as their language of origin described heroic efforts to locate mental and social health services only to be subjected to a looped system of assessment and care that offered no real help. One woman told of her adult daughter waiting three months to get a psychiatric evaluation of the required medication after both mother and daughter spent hours on the phone, the Internet, going to the crisis center at the county hospital, etc. Efforts like this often resulted in decreased care-seeking behaviors.
Participants also detailed a lack of time to address their own (versus their children’s) healthcare needs, in addition to lack of money and lack of access to healthcare. For their children in school, Med-i-Cal and health services were provided. However, without insurance and sometimes with insurance, care for the parent or non-employed spouse was simply not an option. Moreover, prevention was nearly always replaced with emergency care only, and often without money for the recommended treatment from the emergency room visit. One woman described going to the Emergency Room (ER) “They gave me the recipe [prescription], it was $155 for the pills, so I didn’t buy them…[then] I got the bill, $1400, so it was worst. I thought, why did I go?” Others agreed they stopped going to the ER for just such reasons. One mother, employed as a play yard monitor, talked about debilitating migraines with no insurance. The emergency room doctor ordered an MRI, but without the funds to pay for it, she went home unaided with respect to her pain with ongoing headaches. Thus, the lack of connection and communication, fear and anxiety, and lack of care or access to affordable care build on one another. These layers of distance and complexity are difficult to address in the downstream arena of illness-based healthcare.
3.5. Facilitators of Health
These community residents recognized that the city and community leaders needed a “building the community” mindset as necessary to address the deficits (think midstream) before they resulted in health problems at the downstream level. They verbalized that connection with resources and one another was vital to facilitate health for all. Identifying and naming the problem allowed the community members to “watch out for, protect one another by caring for our kids and neighbors, by reaching out to do whatever we can” said one mom. Offering “acceptance to all” in the local community, regardless of whether they could speak their language or not, was an action of inclusion they identified after being in the Tenacity Moms program, an English language specialist and school counselor led group at the local elementary school. This intervention positively affected many moms, especially Spanish speakers. It enabled them to increase their language and systems navigation skills, gain emotional and relational knowledge, learn how to help their children with homework, and find the resources and services offered.
The participants identified community agencies that could be places to disseminate information for all: schools, churches, hospitals, pharmacies, grocery stores, and strip mall stores, but the means remained a challenge. They verbalized “not everybody is able to read fliers…and even if fliers are sent home in backpacks some parents don’t read them.” Additionally, not everyone has access to the Internet or knowledge of where to find the information posted.
Church offerings were often considered suspect because of the perception of obligation for attendance or membership if their services were utilized. Many moms were surprised to learn that the church supporting this research started a free health and legal clinic midway through the research within a mile of the school for people with limited resources and access to healthcare. This was unknown to many even though a small 4 × 6 color ad was widely dispersed at the school, sent home in children’s backpacks, and handed out at the trailer park when the initial surveys for the quantitative study were administered, as well as at the time participants were initially contacted for the qualitative focus group interviews and at the actual focus group interviews.
The participants identified wanting more school and church initiatives to address sources of fear. For example, schools could address bullying with parents and kids, and churches could combat fear and stigma associated with mental health by providing places of comfort and acceptance for those with mental health and illness issues, for the homeless, and for those who perceived themselves being labeled negatively. The participants welcomed school, church, and civic partnerships to provide midstream interventions and activities toward health. See
Figure 1.
4. Discussion
The micro-level findings from these qualitative focus groups highlight the parallel disruption of connectivity, the deficiency of communication and interruption of information and knowledge, the fear and anxiety related to healthcare, and the lack of care present within the healthcare system itself and its resultant disappointed recipients of care.
de Leeuw (
2017) suggests that though the location of health is primarily outside the healthcare (or disease) sector, nonetheless, it inappropriately assumes ownership of all of health, not just the diagnosis and treatment of disease. This creates confusion for the public as they lack an understanding of the major role they have in creating and maintaining health.
Fraught with fragmentation, reproduction of power struggles, divisions and/or duplications of services in its system, and the inability to deliver quality care in the community it intends to serve, the healthcare sector is ripe for transformation. Incorporating non-health sectors (agencies whose primary purpose is not the delivery of healthcare) as key partners in the distribution of healthcare (versus disease/illness care) for the vulnerable will require integration of the best of scientific and collaborative partnerships, and an attitude of humility on the part of leaders in order to achieve health and well-being in the community (
de Sayu and Sparks 2017;
DeHaven et al. 2020).
Engaging the local neighborhood members in establishing high-priority goals and strategies for their own community health and well-being is an essential first step. Community-based participatory research and asset-based community development reinforce the involvement of local community members at every level of planning, implementation, and evaluation of the outcomes (
DeHaven et al. 2020;
Nguyen et al. 2021).
4.1. Large Anchor Institutions
Large anchor institutions (medical and educational) are crucial in facilitating connection, communication, and allocation of the inter-health system’s resources in partnership with the neighborhood, and the non-health sector’s smaller anchors in the community. Large anchor institutions have been recognized as powerful, resource-rich, and important partners when it comes to upstream health interventions and community health practices (
Koh et al. 2020). Moreover, they can often take the lead in helping all agency players provide individual and community-level navigation to address the shared goals of the local community’s health and well-being. The inter-sector provision and distribution of health to address the social gradient factors of money, power, and unfamiliarity with resources for health must tap the smaller anchors as assets already in action (
DeHaven et al. 2020). Churches, small businesses, and not-for-profit organizations are important to the ongoing health and well-being of a community; however, they can often be forgotten when addressing community health. Among the four main findings of this study, each of the areas of deficiency can be addressed by these smaller anchor organizations in profound and effective ways.
4.2. Smaller Anchor Organizations
Limited community connection can be, in part, remedied by the local businesses and faith communities that organize and play a part in the warp and woof of the community. Churches, synagogues, temples (
Chatters et al. 1998), hair salons, barber shops (
National Institute on Minority and Health Disparities 2019), and the like can be engaged in helping individuals and families navigate the health system and non-health sector, leading to increased communication and greater connectedness in the community. However, intentional effort must be made to communicate with these overlooked “little anchors” within the community. Since they do not have health as part of their mission, they are often disenfranchised from the decision-making spaces of health, just as their constituents served are commonly marginalized from the decision-making space for their own local community. There is, therefore, a parallel need for capacity building among these two groups. The missional clarity of the local faith communities allows for this kind of capacity building in a regular and impactful cadence. In addition, the relative organization of the community allows for easily accessible learning opportunities.
One need of small anchors is making a commitment to shared community-oriented goals for health with their own role identified and empowered. Another need is capacity building of vulnerable community members with the outcome of disappointment, anger, unrest, and injustice (lack of action) turned to one of linking voices and arms to be heard, to give input, and to see results. This promotes true empowerment and prevents the charity mindset of doling out services and resources without the community input of what is needed. In other words, well-meaning efforts, that meet immediate, legitimate, and individual needs remain at a distance from the community, and frequently disempower a sense of collective, collaborative, and community-based action for health (
Stoeffler et al. 2020;
Townsend et al. 2020).
In the study that concerns this article, a local church has been the initiator to find and bridge gaps and for health interventions in the communities directly surrounding its parish. The systematic approach of this faith community, as evidenced by participation in this study, shows that when taken seriously, a little anchor can begin to understand its community and make a difference. The outcome of this study, from the small anchor’s perspective, is a free, weekly health clinic to address individual needs. Free services include physical therapy, food distribution, dentistry, access to legal counsel, public health education, and prosthetics and orthotics offerings. While these services do not begin to fill all the gaps in care, communication, and connectedness, they address in part what the community wants: services in their lived neighborhood with input as to how that offering best serves the marginalized and disadvantaged, offering hope, help, and healing to those who avail themselves of these services. These services coincide with the mission of the local church to be a blessing in the community. It also coalesces community expertise through volunteerism and creates a sense of community among the caregivers. The spiritual outcomes, while not measured quantitatively, can anecdotally be said to be positive as well. Baptisms, recommitments to spiritual journeys, and continued relationships centered around growing faith can be seen at every aspect of the clinic, food distribution, shower access, and community building. The overall aggregate response from this work from both the community and the faith community is positive and builds a greater sense of community well-being.
4.3. Additional Resources
Another asset waiting to extend and multiply the sponsoring church’s free clinic, approach to health, and reach is that of community health workers (
Community Health Workers n.d.). This asset offers connection and communication among and between smaller anchors and community members. Community health workers are navigation specialists able to inform, connect, and bridge access to the health sector and the non-health sector and resources each provides for individuals and population groups (
Community Health Workers n.d.;
Page-Reeves et al. 2016). They are the local neighborhood’s, culturally competent “resource or health fair” in action and are part of the capacity and assets already at work. Community members can experience their power and voice at work making a difference, and the communication grows as the knowledge and information gap is reduced. Contiguous with this training and deployment, it is important to embrace the vulnerable community members using their network of relationships and giftings to further the trust and cohesion needed to penetrate the community with health outside the confines of the healthcare system. As
Koh et al. (
2020) suggest, building relationships with community and its members involves “willingness to commit years of time engaging key internal and external audiences because ‘change happens at the speed of trust’” (p. 134).
4.4. Integrated Theory of Change in Health Behavior
In addition to direct provision and trusted connection to heath care services, leveraging small anchors such as churches and educational entities may foster chenag in the health behavior through communicating health information via trusted sources (
Dada et al. 2022), building capacity for religiously motivated self-regulation (
Grim and Grim 2019;
Hodge et al. 2020;
Zong and Cheah 2021), and religious influence and support for the behavior change (
Brewer et al. 2019;
Lahijani et al. 2021;
Resnicow et al. 2005). The quantitative results of this study supported a modified Integrated Theory of Health Behavior Change (
Pfeiffer et al. 2018) where religious self-regulation skill and ability and religious self-management behaviors contributed to healthy eating behaviors. These qualitative results suggest that a religious institution as a trusted and connected community partner could address upstream factors contributing to poor health outcomes, helping to address issues of disconnectedness, deficient communication, and fear and anxiety, as well as connecting the community to health care (
Javed et al. 2022;
Krause and Bastida 2011;
Stoeffler et al. 2020).
While the original ITHBC theory (
Ryan 2009) was applied to care for individuals and families with chronic illness, these qualitative findings open a perception of the church and the community as entities dealing with chronic conditions. These groups may also have collective self-regulation skill and ability, and self-management behavior. This holds the possibility for the church to influence the change in health behavior at both the individual and community level. Where the church is known as a major resource for health and referral for those beyond the church both proximal and distal health behaviors may result—i.e., the undocumented know they can come to a legal clinic for help with local and immediate legal issues (proximal health outcomes) or longer-term immigration assistance (distal health outcomes). Likewise, a change in both proximal and distal health behavior happens when the church surrounds people with advanced social support and collaborative partnerships in communicating care. These are part of the ITHBC’s concept of social facilitation (
Ryan 2009). Without the moderating effects of the church as a community of care many more could be lost, alienated, and truncated in their ability to seek, much less find, needed support and assistance, access to health care, and increased connection and communication.
By coordinating the communication from large anchors and seeking community member involvement and input, smaller anchors can increase the effectiveness of communication, undermine fear through connection, and quell anxiety through education. All this empowers the community, including the marginalized and disadvantaged, to be able to move more midstream or upstream in their interventions and more local in their expression of health, and to seek answers and care earlier even if the results are longer term (
de Sayu and Sparks 2017).
The limitations of this small CBPR study were limited sustained community focus group involvement and inconsistent community informant participation. This was due in part to changing leadership at the local elementary schools and within the research team, as well as COVID-19 restrictions. Thus, the trajectory of long-term involvement in the community was modestly challenged.
5. Conclusions
This qualitative research of four zip codes within a radius of a mile from a local sponsoring church revealed the parallel needs of the local community and the health (disease) care system. Future investment of university, church, and community partnership must start with agreement and commitment to a high priority and realistic goals with markers that anticipate potential for turnover in team membership without deterring the pursuit and attainment of the goals (
de Sayu and Sparks 2017). In the future, the CBPR of post COVID-19 needs and assets can be done while identifying the community informants, anchor medical groups, and/or anchor educational institutions to give coordination to team building, identification of shared goals for the local community, and targeted capacity building of the local neighborhood. Research should be done in each aspect of the community empowerment process. Each group and organization must give priority to continuous communication with each sector, which will allow the work of trust, partnership, and accomplishment to continue and be renewed.
The analogous needs for increased connection and connectivity, communication and knowledge, and health and social care in the local area require the best of community member ownership and involvement, the best of large anchor facilitation and investment, and the full expression of the smaller anchor offerings. A commitment to this approach will provide a more just and equitable distribution of, and capacity building for, community health and well-being. Collaborative, community partnerships will serve to empower versus dole out “charity,” reinforce belief and goodwill, and create expectation with commensurate commitment on the part of each group and organization involved. An empowered community is one positioned to partner with the health sector, the non-health sector, and its community constituents in bringing health and social care to its members, thereby reducing some of the vulnerability and disadvantages present in the local community.





{kind=link}