1. Introduction
Human dignity, an intrinsic value inherent in every individual, is a cornerstone concept in healthcare ethics. As healthcare professionals navigate diverse clinical scenarios, the principle of human dignity remains a guiding compass informing treatment modalities and patient care practices. Yet, the multifaceted and diverse interpretations of human dignity often lead to varied applications in clinical settings, creating a need for a more articulated, comprehensive understanding of the concept.
This paper endeavors to bridge this gap by exploring the religious foundations of human dignity, primarily through the lens of Eastern Orthodox Christianity. While Eastern Orthodoxy, with its particular theological emphasis on the “Image of God” and human personhood, forms the primary religious lens of this study, insights from Roman Catholicism and other Christian traditions enrich our understanding of human dignity. Our unique contribution lies in threading the rich theological tapestry of these traditions with contemporary healthcare practice in central Europe, more specifically Slovakia. This particular focus on the intersection of Eastern Orthodox Christian tradition, enriched by ideas from the Ecumenical Christian Church, and a specific geographic region presents a unique perspective that can deepen our understanding of human dignity and its application in healthcare.
Our thesis posits that the Eastern Orthodox understanding of human dignity, grounded in the concept of the “Image of God” as understood by the Eastern Orthodox tradition, offers a robust framework for interpreting and applying human dignity in healthcare. Furthermore, we propose that the integration of insights from other Christian theological sources enriches this framework, enhancing respect for patients and contributing to better healthcare outcomes, particularly for hospitalized patients. Drawing from a diversity of sources, including the Bible, writings of early Church Fathers, contemporary Eastern Orthodox theologians, perspectives from other Christian traditions, and central European healthcare policies and practices, this study presents a distinctive analysis that straddles the fields of healthcare ethics, religious studies, and central European cultural studies. It aims to stimulate a dialog among these fields, contributing to a more nuanced, integrative understanding of human dignity in healthcare.
The geographic and cultural lens that informs our perspective is the central European region, more specifically, Slovakia. The region’s unique socio-economic realities, cultural attitudes, and religious traditions have significantly influenced our perspective on dignity-conserving care. Naturally, the socio-economic realities of central Europe, shaped by considerable historical socio-political transformations, significantly impact the implementation of dignity-conserving care. Disparities within and between countries in the region affect the accessibility and quality of palliative care. In response to these challenges, we propose strategies that are not only ethically grounded but also pragmatically feasible. When it comes to understanding the concept of palliative care, we propose that while often associated with end-of-life care, palliative care is a holistic approach that aims to improve the quality of life for individuals facing serious illness. It involves managing pain and other distressing symptoms, while also addressing emotional, social, and spiritual needs.
Central European cultures are characterized by a strong sense of community and familial ties, reflected in the shared responsibility for caregiving. Recognizing this, we emphasize the inclusion of family members in the care process. Furthermore, we advocate for fostering open and respectful communication, with an awareness of the power dynamics and cultural norms that can influence these interactions. In addition, the Eastern Orthodox tradition, widely practiced in parts of central Europe, has had a significant influence on our conceptualization of human dignity and dignity-conserving care. This tradition emphasizes compassion, humility, and communal interdependence, values that have informed our proposed strategies for dignity-conserving care.
With this multifaceted context in mind, our paper offers an exploration of the theological grounding of human dignity, its operationalization in the context of healthcare, and strategies for maintaining this dignity in the patient care process. By grounding our discussion in the socio-economic, cultural, and religious realities of the region, we aim to offer a perspective on dignity-conserving care that is theoretically robust, practically relevant, and culturally sensitive.
2. Clarifying the Concept of Human Dignity
The concept of human dignity is multifaceted, emanating from an array of sources, spanning various eras, and is impacted by diverse cultural, philosophical, and religious contexts. This complex lineage of human dignity necessitates a thorough dissection to foster a comprehensive understanding of the concept, its origins, interpretations, and applications, especially within the realm of healthcare. Maintaining the dignity of the hospitalized during inpatient care is critical, as it can significantly impact their sense of self-worth and quality of life.
In its original conception, human dignity is deeply rooted in biblical and theological perspectives. In the Judeo-Christian tradition, the concept of human dignity originates from the belief that human beings are created in the ‘image and likeness of God’ (Imago Dei and Similitude Dei). This seminal idea underpins each individual’s intrinsic worth and sanctity, irrespective of their social status, physical attributes, abilities, or moral character. Over the centuries, this theological understanding has influenced legal and philosophical developments, informing various human rights doctrines and ethical theories. “If the inalienable ontological dignity of every human person—its highest value, is elevated in the image of God, then a life corresponding to dignity correlates with the concept of God’s form achieved by God’s grace by overcoming sin, gaining moral value, purity and virtue” (
Movsesyan 2016).
Simultaneously, human dignity has also been interpreted through a secular lens, with philosophers such as Immanuel Kant proposing that the inherent dignity of a person derives from their capacity for rationality and autonomy. In contemporary discourse, human dignity has become central to ethical discussions concerning respect for persons, rights, justice, and autonomy in a variety of fields, including bioethics, law, and human rights. For example, according to Shotton and Seedhouse (
Simões and Sapeta 2019), human dignity is defined as the capacity of a person to exercise their abilities or to receive help under specific conditions. Dignity is related to the dynamic interaction between circumstances and abilities. In this context, Pellegrino and Pullman define human dignity as a quality of being that deserves respect and esteem. The authors distinguish between basic dignity and personal dignity. Basic dignity is the inherent dignity of every human being that cannot be taken away. In this sense, it can be conceived of as a religious–metaphysical category. Personal dignity refers to a personal sense of value associated with personal goals and social circumstances. It is related to the self-esteem and perception of people as respected by their surroundings. It can be removed or strengthened (
Albers et al. 2011). Jacobson defines dignity in a similar way (
Jacobson 2007) when he speaks of basic (universal) dignity as the dignity of all people. Relative dignity refers to the social status of the individual. This dignity can be gained or lost (
Sagbakken 2017). Social dignity is alternatively called identity dignity. This kind of dignity is related to the dignity of oneself, self-esteem, and respect for others. There is a significant relationship between identity dignity, illness, and hospitalization, as illness can undermine the independence of individuals and pose a threat to their personal identity, which in turn adversely affects their overall dignity (
Farimah et al. 2019). A similar definition is offered by
Nordenfelt (
2014)
1 when defining the four concepts of human dignity. He claims that in the course of life, all people have universal human dignity that cannot be lost. The dignity of merit exists in degrees and is related to the position of humans in society. Dignity as a moral condition is associated with a person’s moral values and self-esteem. The fourth type of dignity is identity dignity, which is related to the human identity of a person and the integrity of their body and mind. The dignity of the identity may be impaired or taken away, for example, by the actions of others or by illness.
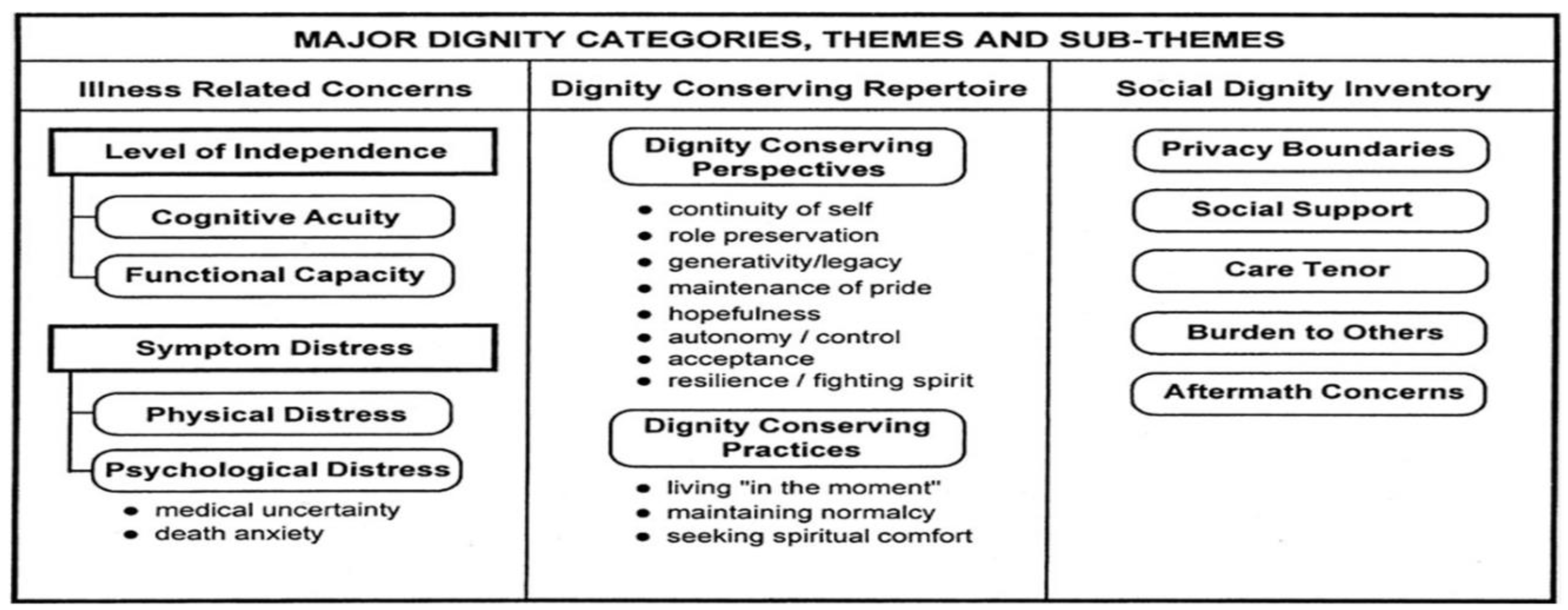
According to
Chochinov et al. (
2008), a person experiences their illness in various ways. The awareness that the disease threatens their existence can result in despair, which negatively affects the human body, psyche, and soul. The author further emphasizes the conceptual model of dignity proposed on the basis of an analysis of the hospitalized in palliative care. His attention focuses on concerns related to the disease (physical and psychological factors), personal sources of dignity, maintaining dignity (spiritual or psychological factors), and social resources (factors such as social context, challenges, positive aspects, and suffering) (
Chochinov et al. 2002).
Given the diversity of interpretations (as seen in
Scheme 1 below), we propose a typology of human dignity. It comprises three main categories: intrinsic, attributed, and inflorescent dignity. ‘Intrinsic dignity’ relates to the inherent worth of a person due to their human nature, in line with the theological perspective. ‘Attributed dignity’ refers to the value ascribed to a person based on their attributes or accomplishments, resonating with societal and cultural factors. ‘Inflorescent dignity’ encapsulates the concept of dignity as a quality that can flourish or diminish depending on the conditions of one’s life, reflecting the quality of life and healthcare perspectives.
These categories are not mutually exclusive but interact and overlap, contributing to a composite understanding of human dignity. However, it is crucial to evaluate the strengths and weaknesses of these perspectives. While intrinsic dignity underscores the equal worth of all individuals, it might risk downplaying the role of personal attributes or achievements. Attributed dignity, though honoring individual accomplishments, could potentially undermine the dignity of those less able or less accomplished. Inflorescent dignity, although highlighting the impact of external circumstances on dignity, may inadvertently neglect the enduring aspects of human worth.
In healthcare, the concept of human dignity has a fundamental role in framing ethical principles and practices. By combining the strengths of each perspective, a nuanced understanding of human dignity can be cultivated, which respects the intrinsic worth of individuals, acknowledges their unique attributes and accomplishments, and fosters conditions that allow dignity to flourish. Such a comprehensive understanding provides a robust ethical foundation for patient care and informs the core ethos of healthcare professions.
3. Understanding the Orthodox Church’s Perception of Human Dignity
Our paper focuses on the Christian religious perspectives, specifically those of Eastern Orthodox, Roman Catholic, and certain Protestant traditions, without discounting the relevance of other religious and secular understandings. The following analysis will aim to present a more nuanced understanding of this concept, highlighting the distinctions between different Christian viewpoints, while also emphasizing common ground where it exists.
The Eastern Orthodox tradition, which is the primary influence in our study, posits a holistic view of human dignity. Rooted in its interpretation of the doctrine of the ‘Imago Dei’, it emphasizes the inherent worth of every human being, an inviolable dignity bestowed by virtue of our creation in the image of God. The most commonly used characteristics of God’s image in human are logos, mind, spirit, consciousness, personality, freedom, goodness, holiness, and love (
Дyмитpaкe 2013). These are all qualities of human nature (
Lossky 1995, p. 92). They are inherent in human nature; their origin is divine, as they are not found in the non-human world. One of the greatest authorities among the church fathers, St. John Chrysostom, perceives human dignity as a gracious gift from God (
Claassens 2011). In this context, we can refer to the works of
V. N. Lossky (
1995, p. 92) or contemporary authors, such as
Дyмитpaкe (
2013) or
Papanikolaou (
2003), who offer competent and refreshing interpretations on the subject.
The Orthodox Church elucidates the concept of human dignity through the lens of Genesis 1:26 in the Bible. According to the scriptures, when God created humans in His own image and likeness, He performed His most sublime and perfect work in the history of humanity. A unique connection or bond was thus established between God and humanity, which elevated humanity’s extraordinary position. As per the biblical narrative, humans are entrusted with the significant role of being the ‘rulers’ and the crown of creation, prototypes with the potential to become like God. As interpreted by Bortkiewicz (
Bortkiewicz 2017), the act of God bestowing a name upon the first humans (i.e., Adam and Eve) signifies God’s desire for all humans to exist and live in communion with Him. This ongoing dialogue between God and humans is mediated through a conscience that identifies God’s voice as the law. This law, echoing within the conscience, embodies the culmination of love for God and fellow human beings, bearing witness to human dignity.
Echoing the words of St. Maximus the Confessor, humans are invited to partake in God’s sacred life (
Lossky 1995, p. 92). Hence, the ‘creation’ of humans ‘in God’s image’ means a kind of “communion” with divinity. Thus, ‘in the image’ does not mean a solely moral reproduction, its action is expressed by the illumination of the human mind, which gives it the ability to know God (
Дyмитpaкe 2013). Similarly, St. Gregory of Nyssa says, ‘Man is united with God,’ so that the image ‘predestines’ the human being to deification (
Дyмитpaкe 2013;
Jacobs 2009). St. Gregory of Nyssa discusses the inseparable creation of the soul and body, reflecting on their simultaneous origin (
Šip and Šipová 2015). In the theological discourse of St. Athanasius the Great, the concept of human dignity is fundamentally intertwined with the principle of homoousios (
Doйчик 2014). This principle is manifested in the doctrine of the Holy Trinity, the Divinity of Jesus Christ, and the individuality of human beings. Humans are not merely reflections of God’s image and likeness; rather, they partake in the divine through the humanity of the Word. ‘Participation’ in God’s energies gives him the opportunity to free himself from destruction and disease and to unite with God through the incarnation of His word into the human body (
Doйчик 2014). The above suggests that the static description of the image of God in humans is connected with the dynamic description of the likeness of God in humans. The notion of immortality, representing the pinnacle of the dignity of creation, emerges from the liberation of the human body from its inherent corruption and psycho-physical frailty. This liberation is made possible through the salvific presence of God’s Word within the human form (
Уcтян 2012).
It should be noted that the whole work of the Church Fathers draws attention to the fact that the image is not a regulatory or instrumental idea but a defining principle of the human being (
Дyмитpaкe 2013). Thus, patristic anthropology, as interpreted from the Eastern Orthodox perspective, argues that the human being was created as a ‘saint’ (
Perišić 2023).
The biblical text underscores facets of our present comprehension of human dignity, hinting at its universal, anthropological, and ontological dimensions. It indicates that every person holds a privileged position in the hierarchy that spans between God and the rest of creation and that all humans are equal. This privileged status bestows upon individuals a moral right and obligation of mutual respect and protection of life and implores them to exercise personal freedom and responsibility in their interactions with others (
Müller 2020).
Catholic teaching on human dignity is based on the belief that all human beings are created in the image and likeness of God. This means that all human beings have inherent and inviolable dignity, regardless of their personal attributes or circumstances. This dignity is not something that can be earned or lost; it is a gift from God. The Roman Catholic Church teaches that human dignity is grounded in our nature as rational beings. We are created with the ability to reason, to make moral choices, and to love. These capacities make us unique among all creation, and they give us special dignity. The Roman Catholic Church also teaches that human dignity is enhanced by grace. Grace is a gift from God that enables us to live in accordance with our nature and to grow in holiness. When we receive grace, we are able to overcome sin and live in a way that is pleasing to God. The Catholic understanding of human dignity is complex and nuanced. It is based on a deep understanding of human nature and on the belief that all human beings are loved and valued by God. This understanding has profound implications for the way that we treat others and for the way that we live our lives.
The Catholic understanding of human dignity is similar to the understanding of human dignity in the Eastern Orthodox tradition. Catholics also teach that all human beings are created in the image and likeness of God, and that they have inherent and inviolable dignity. However, there are also some differences between the Catholic understanding of human dignity and the understanding of human dignity in other Christian traditions. For example, the Roman Catholic Church teaches that human dignity is enhanced by grace, while other religious traditions do not (
Grisez 1997).
The Roman Catholic Church promotes human dignity mainly through its teachings, social justice work, and its charitable work. For example, the Roman Catholic Church teaches that all human beings have a right to life, and it opposes abortion and euthanasia (
Porter 1999). The Roman Catholic Church also works to promote human dignity by fighting poverty, hunger, and injustice. The Roman Catholic Church also provides charitable assistance, such as food, clothing, and shelter, to those in need (
Paul 1999).
The Protestant perspective on human dignity is a complex and diverse one. However, there are some common themes that can be found across Protestant denominations. One of the most important of these themes is the belief in sola gratia, or salvation by grace alone. This belief is based on the Protestant understanding of the Bible, which teaches that human beings are all sinners and that we cannot earn our salvation. Instead, salvation is a gift from God, given to us freely through faith in Jesus Christ.
2 The belief in sola gratia has a profound impact on the Protestant understanding of human dignity. If our salvation is not based on our own works, then it follows that our worth as human beings is not based on our own achievements or failures. We are all equal in the eyes of God, regardless of our race, gender, social status, or any other factor (
Hauerwas 1983). This unconditional dignity is a gift from God, and it is something that we should never take for granted.
The Protestant emphasis on unconditional dignity has a number of implications for how we live our lives. First, it means that we should treat all people with respect, regardless of their differences. Second, it means that we should not judge others, as we are all sinners in need of God’s grace. Third, it means that we should be humble and grateful for the gift of salvation that we have received. The Protestant perspective on human dignity is a powerful and liberating one. It reminds us that we are all equal in the eyes of God, and that our worth is not based on our own achievements or failures. This is a message that we need to hear, especially in a world that is often divided by race, gender, class, and other factors. The Protestant perspective on human dignity can help us to build a more just and compassionate world (
Wolterstorff 2008).
To enhance clarity and comparative understanding, we propose a typology that differentiates these Christian perspectives along two key axes: (i) the origin of dignity (inherent by creation versus conferred by grace); and (ii) the role of human freedom and responsibility in upholding dignity. An understanding of these Christian perspectives is crucial for gaining a broader perspective on the theological concept of human dignity. These viewpoints not only vary amongst themselves, they also provide a distinctive contrast to secular and other religious perspectives on human dignity.
To summarize this section, human life is deemed sacred because it is created in God’s image. Based on one’s ontological status and dignity, one becomes the nucleus of social interaction and activities. Each person must be regarded as a subject rather than an object or a means, at every stage of life. As social beings, people ought to respect and support each other. Through such coexistence, individuals can nurture their self-perception and their relationships with others, thereby highlighting the interdependence between societal development and personal growth (
Rumambi and Marentek 2015).
In the ensuing discussion, we will delve into the practical implications of these perspectives in healthcare practices, specifically within the context of central Europe, and more particularly Slovakia. This regional focus does not limit the relevance of our analysis; on the contrary, it allows for a more nuanced understanding of how religious concepts of human dignity are translated into real-world practices in specific cultural contexts.
4. A Theological Framing of Human Dignity in Healthcare
As we move from broad theological considerations to the more specific context of healthcare, the task is to delineate how these understandings of human dignity inform, and are shaped by, the ethical and practical aspects of patient care. The premise here is not to suggest that a religious understanding of human dignity is necessary for respectful patient care; numerous secular healthcare providers and institutions are guided by equally compelling ethical frameworks. Rather, the aim is to explore how a nuanced, theologically informed understanding of human dignity might enhance and enrich the ethical foundation of healthcare practices, especially within communities where religious beliefs and values hold significant influence.
Religious traditions have historically contributed valuable perspectives on human dignity, suffering, and the role of healthcare. These perspectives often echo and supplement secular principles of healthcare ethics, such as respect for autonomy, beneficence, non-maleficence, and justice. For instance, the Christian belief in Imago Dei underscores the intrinsic dignity and worth of each person, resonating with the principle of respect for autonomy. The call to love one’s neighbor as oneself informs the principle of beneficence. The admonition against causing harm aligns with the principle of non-maleficence, and the command to act justly corresponds with the principle of justice.
However, religious framings of human dignity can offer additional dimensions to these principles. For instance, the idea of Imago Dei does not merely affirm individual autonomy; it situates autonomy within a relational context, emphasizing the interconnectedness of human beings and their responsibilities towards each other. This understanding aligns with the growing recognition in healthcare ethics of the importance of relational autonomy, which views individuals not merely as isolated decisionmakers but as situated within a web of relationships.
Furthermore, religious traditions tend to embrace a holistic understanding of the person, acknowledging the bio-psycho-social-spiritual dimensions of human life. In this context, ‘bio-psycho-social-spiritual’ refers to a comprehensive view of the person that considers not only their biological and psychological conditions but also their social relationships and spiritual beliefs (
Baldacchino and Draper 2001). This holistic perspective aligns with the emerging patient-centered care models in healthcare, which advocate for considering the whole person, including their values, beliefs, and life circumstances, in the provision of care (
Pérez 2004). In sum, a theologically informed framing of human dignity complements (and, theologians would argue, extends) our ability to view and address ethical issues in healthcare. It can enrich our understanding of foundational ethical principles, provide a holistic view of the person, and highlight the importance of relationality and community in healthcare. Such a perspective does not replace or diminish the value of secular ethical frameworks; instead, it can complement and extend these frameworks, contributing to a more comprehensive and nuanced ethos of patient care.
5. Relating the Concept of Human Dignity to Healthcare Practices
Given the complexity and diversity of Christian perspectives on human dignity, it becomes essential to discuss how these concepts are operationalized within the realm of healthcare. Central to our thesis is the assertion that these theological viewpoints significantly inform the understanding and practices of human dignity within healthcare systems, particularly in regions where Christianity holds substantial cultural influence, such as Slovakia and broader central Europe.
In healthcare settings, the concept of human dignity often translates into a commitment to respect patients as individuals, acknowledging their intrinsic worth, and upholding their rights and freedoms. However, the theological perspectives can add a layer of depth and complexity to this understanding. For example, the Eastern Orthodox view of human dignity might inform a holistic approach to patient care, considering not just the physical but also the spiritual and psychological aspects of the individual. Similarly, a Roman Catholic perspective, deeply influenced by Thomistic philosophy, might emphasize the ethical responsibility of healthcare providers in recognizing and responding to the unique nature of each individual patient (
Grisez 1997). Furthermore, Protestant perspectives, with their emphasis on grace, might lead to an understanding of human dignity that underscores the necessity of unconditional care, irrespective of the patient’s condition or prognosis. This view could challenge certain utilitarian approaches in healthcare that might devalue individuals based on their perceived ‘utility’ or ‘quality of life’.
3These Christian perspectives on human dignity, while varying in nuances, collectively present a compelling case for a compassionate, patient-centric approach to healthcare, which respects the inherent dignity of every individual. Our aim is to explore the practical implications of these perspectives, offering a nuanced understanding that goes beyond generic appeals to ‘respect patients’ or uphold ‘human rights.’
The challenge of applying theological concepts of human dignity to healthcare practices lies in navigating the multifaceted, and sometimes conflicting, interpretations. However, by providing a comparative analysis, and examining these concepts in their specific cultural contexts, we hope to offer insights that could help practitioners and policymakers align healthcare practices with the values and beliefs of the communities they serve.
In the following paragraphs, we will delve into specific healthcare scenarios, demonstrating how these different Christian perspectives on human dignity could inform and enrich patient care practices.
Human Dignity and Patient Care: A Practical Perspective
Having laid a theoretical groundwork on the concept of human dignity and its theological framing, we now transition to examining the implications of these ideas for the practical sphere of patient care. Respect for human dignity, as it turns out, is far from being a purely theoretical concept; it manifests in numerous concrete ways in the interactions between healthcare providers and patients. This section will provide an overview of these manifestations, exploring how an understanding of human dignity can inform best practices in patient care and help address ethical dilemmas that often arise in healthcare settings.
To elucidate the role of human dignity in patient care, it is helpful to examine its relationship with other related concepts, such as quality of life, suffering, and self-esteem. These concepts often intersect with human dignity, informing its understanding and application in healthcare.
First, quality of life is a broad concept that reflects a person’s overall wellbeing and satisfaction with life, encompassing various dimensions such as physical health, psychological wellbeing, social relationships, and spiritual beliefs (
Tristán 2008). Respect for human dignity necessitates a commitment to enhance patients’ quality of life, which includes addressing not only their physical needs but also their psychological, social, and spiritual needs. This commitment is often operationalized through patient-centered care models, which emphasize individualized care, respect for a patient’s values and preferences, and the active involvement of patients in decision-making.
Next, suffering refers to the experience of distress or hardship that can result from illness or treatment. While some degree of suffering might be unavoidable in healthcare, respect for human dignity demands that healthcare providers strive to minimize unnecessary suffering and help patients cope with their suffering (
Devik et al. 2013;
Morita et al. 2014). This can be achieved through various means, including effective pain management, emotional support, spiritual care, and palliative care.
Lastly, self-esteem reflects a person’s sense of self-worth and confidence (
Rosenberg 2015). Illness and hospitalization can often impact patients’ self-esteem, due to factors such as a loss of autonomy, dependence on others, and changes in physical appearance or abilities. Upholding human dignity involves recognizing and addressing these impacts, for instance, through promoting autonomy, ensuring privacy, providing respectful care, and offering psychological support (
Haeser et al. 2012;
Entwistle et al. 2010).
In the next section, we will further explore these concepts and their implications for patient care, drawing on various sources from theology, ethics, and healthcare literature. Our goal is not to present a comprehensive or definitive account, but rather to stimulate thoughtful reflection and dialogue on these important issues.
6. Maintaining Human Dignity in the Care of Hospitalized Patients
Cuadrado proposes that the identity of human dignity during hospitalization signifies an undefined and simple quality of a human being, indicating his supremacy over other beings, irrespective of his behavior (
Cuadrado 2012).
Hervada (
1991) adds that it is the perfection or intensity of existence that corresponds to human nature and is predicted for a person concerning the existential realization of human nature. This implies that dignity is an inherent attribute that one possesses simply by existing.
Spaemann (
1988) further clarifies that dignity is a term used to delineate a specific way or quality of being, asserting that a person is a person and not an individual. Cámar asserts that the concept of a person is to possess special dignity, and despite losing certain qualities due to illness or severe suffering, the individual continues to be a being with a sense of transcendence (
Cámara 2019;
Olazabal 2020). Hence, this dignity does not rely on the somatic or psychological qualities of the person but on the fact that they are a person.
In view of the need to take seriously the dimension of transcendence of each human person, we propose the term ‘transcendental nursing care.’ Transcendental nursing care is a concept that draws upon ontological theological perspectives, and it carries significant implications for dignified care (
Cheraghi et al. 2015). In the context of this paper, we use the term ‘transcendental’ not in the philosophical sense pertaining to conditions of possibility, but rather in relation to its more common usage, denoting that which goes beyond the ordinary and aims at a higher or more spiritual level (ontologically speaking).
In nursing, the concept of ‘transcendental care’ encompasses a holistic approach, striving to address not only the physical needs of the patient but also the emotional, psychological, and spiritual dimensions. This form of care extends beyond routine clinical procedures and treatments, aiming to respect and uphold the inherent dignity of the patient. Transcendental nursing care is thus characterized by practices such as active listening, empathy, presence, comfort, and respect for the patient’s beliefs and values.
In the Eastern Orthodox tradition, the emphasis on community and interdependence provides a rich framework for this approach to care. The fundamental belief in the image and likeness of God in each person calls for a recognition of the sacred in the other, thus fostering a deep respect for the dignity and worth of the patient. This understanding guides the practice of transcendental nursing care. It demands a higher level of engagement from the caregiver, requiring not just clinical competence but also empathy, compassion, and an ability to see beyond the immediate medical condition. Such an approach to care has significant implications for the experience of the patient, potentially contributing to an enhanced sense of dignity, comfort, and well-being. Transcendental nursing care, therefore, forms a crucial component of dignity-conserving care strategies, as discussed in this paper.
By alleviating suffering and offering the best quality of life to the patient, we demonstrate respect for the patient’s autonomy. The objective of specialized medical assistance is to safeguard human dignity by taking measures to ensure respect for human rights, firmly established in international instruments such as the Universal Declaration of Human Rights, the Convention for the Protection of Human Rights and Fundamental Freedoms, the Charter of Fundamental Rights and Freedoms, and the European Charter of Patient’s Rights (which we discuss in detail below). These international legislative documents uphold and protect human dignity and promote the human right to dignified treatment of a person, especially when they are most vulnerable and at risk (
de Luca et al. 2017;
Szabo et al. 2020). The European Charter of Patient’s Rights (
Council of Europe 2002) lays out fundamental rights such as the right to preventive measures, access, information, consent, free choice, privacy and confidentiality, respect of patients’ time, observance of quality standards, safety, innovation, avoidance of unnecessary suffering and pain, and personalized treatment. These rights align with and, in some cases, expand upon the ethical imperatives embedded in our discussion of human dignity from the Eastern Orthodox theological perspective.
For instance, the Eastern Orthodox understanding of human dignity, derived from the belief in the image and likeness of God in each person, resonates strongly with the Charter’s emphasis on respect, privacy, and personalized treatment. Both frameworks call for the recognition of the inherent worth and uniqueness of each patient, necessitating an individualized, patient-centered approach to care. Similarly, the Charter’s focus on access and quality of care can be viewed as an extension of the theological emphasis on love and service, embodied in the practice of caregiving. The right to information and consent, as enshrined in the Charter, is likewise consistent with the theological understanding of human dignity that necessitates respect for individual autonomy and decision-making.
However, it is also worth noting the areas where the theological perspective might further enrich our understanding of patient rights. For instance, the concept of transcendental nursing care, discussed earlier, calls for a more holistic approach to care, addressing not just the physical but also the emotional, psychological, and spiritual needs of the patient. This is an area not explicitly covered by the Charter, highlighting the valuable contribution of the theological perspective. In short, the alignment between the theological understanding of human dignity and the principles of the European Charter of Patient’s Rights underscores the value of integrating these frameworks in our approach to healthcare. This convergence strengthens the case for a holistic, dignity-conserving approach to patient care that respects individual rights and upholds the inherent worth of each person.
Building on our discussion of human dignity’s theological framing and its interplay with the quality of life, suffering, and self-esteem, we now examine specific strategies and practices that can help maintain human dignity in the care of hospitalized patients. In doing so, we hope to provide clinicians, ethicists, and other healthcare professionals with practical guidance that is grounded in a robust understanding of human dignity.
6.1. Promoting Autonomy and Shared Decision-Making
Promoting patients’ autonomy is a key strategy for respecting human dignity. Autonomy refers to the ability to make independent decisions and control one’s own life. In healthcare, this can be fostered through shared decision-making, a process in which healthcare providers and patients collaborate to make healthcare decisions that are informed by medical evidence and aligned with the patient’s values and preferences (
Bunn et al. 2018).
6.2. Providing Person-Centered Care
Person-centered care is an approach that respects and responds to the individual needs and values of patients. It involves seeing the patient as a unique individual, not just as a patient or a diagnosis. This approach can enhance human dignity by acknowledging the intrinsic worth of each person and affirming their identity beyond their illness.
6.3. Maintaining Privacy and Confidentiality
Respecting privacy and confidentiality is another important aspect of upholding human dignity. This includes physical privacy (e.g., during medical examinations or procedures), informational privacy (e.g., maintaining confidentiality of medical records), and social privacy (e.g., respecting personal boundaries and social norms).
6.4. Addressing Spiritual Needs
Given the theological framing of human dignity, addressing spiritual needs is an integral part of dignified care. This can involve providing access to spiritual care services, accommodating religious practices, and incorporating spiritual beliefs into care planning and decision-making.
6.5. Ensuring Respectful Communication
Respectful communication is fundamental to human dignity. It involves showing empathy, listening attentively, explaining medical information in understandable terms, and respecting patients’ emotions and perspectives (
Rutter et al. 1996;
Baillie 2009).
These strategies and practices, while not exhaustive, provide a starting point for thinking about how human dignity can be upheld in the care of hospitalized patients. In the next section, we will delve deeper into the practical application of these ideas, with a specific focus on palliative care.
7. Dignity-Conserving Care in Palliative Contexts
Palliative care, given its focus on relieving suffering and enhancing the quality of life, provides a rich context for examining dignity-conserving care. Here, we will discuss specific strategies for preserving human dignity in palliative care, drawing on a wide range of sources, including clinical guidelines, empirical studies, and theological writings.
In presenting these strategies, we acknowledge the complex realities of palliative care, where respecting human dignity often involves navigating difficult ethical dilemmas and confronting deep-seated societal attitudes and practices (
de Luca et al. 2017;
Szabo et al. 2020). Nevertheless, we believe that a commitment to human dignity, informed by a nuanced understanding of the concept, can serve as a guiding principle that illuminates the path toward compassionate, ethical, and dignified palliative care.
Palliative care presents unique challenges and opportunities for dignity-conserving care. Patients facing terminal illnesses are often confronted with multifaceted suffering, encompassing physical, emotional, social, and spiritual dimensions. Their dignity might be threatened not only by the debilitating symptoms of their illnesses but also by social isolation, loss of independence, and existential distress (
Franco et al. 2019). Yet, they are also in a unique position to reflect on their lives and identities, affirm their worth, and experience profound human connections.
To navigate this complex landscape, clinicians need a nuanced and multidimensional understanding of human dignity. Drawing on our previous discussions, we suggest that this understanding should encompass the notions of inherent, attributed, and infrangible (inflorescent) dignity, informed by the Eastern Orthodox tradition, while also considering the perspectives of other Christian traditions and the broader socio-cultural context of central Europe.
Building on this understanding, we propose several strategies for dignity-conserving care in palliative contexts.
First, clinicians should aim to provide holistic and person-centered care that addresses patients’ physical, emotional, social, and spiritual needs. This could involve a range of interventions, from adequate pain and symptom management to emotional support, from facilitating meaningful human connections to addressing spiritual concerns.
For instance, let us consider the case of a 65-year-old woman suffering from advanced cancer. She is experiencing severe pain, but her distress is amplified by her feelings of loneliness and her fear of death. In this case, effective pain management is crucial for preserving her dignity. Equally important, however, are the interventions that address her emotional and spiritual suffering, such as supportive counselling, facilitating contact with her loved ones, or connecting her with a spiritual advisor.
Second, clinicians should respect and foster patients’ autonomy. This could involve shared decision-making, where patients are encouraged and supported to actively participate in decisions about their care. It could also involve efforts to uphold patients’ privacy and to preserve their sense of control, even in the face of debilitating illness.
Third, communication is a critical aspect of dignity-conserving care. Clinicians should aim to foster a climate of open, honest, and respectful communication, where patients feel heard, understood, and valued. They should listen empathetically to patients’ narratives, validate their emotions, and provide information in a clear and sensitive manner.
Fourth, clinicians should acknowledge and respect patients’ unique identities and life stories. This could involve learning about patients’ backgrounds, values, beliefs, and aspirations. It could also involve supporting patients in activities that affirm their identity and self-worth, such as life review or legacy projects (
Bolmsjo 2000).
The Eastern Orthodox tradition, with its emphasis on the value and uniqueness of each human person, can provide a rich resource for this approach. For instance, it can inspire clinicians to view each patient not merely as a case of a particular disease but as a unique person with their own story, worth, and potential. It can also encourage them to approach each encounter with patients with humility, compassion, and a deep sense of respect for their dignity.
Fifth, attention should be given to the family members of the patients (
Bolmsjo 2000), who often share the burden of the illness. Informed by the Eastern Orthodox understanding of community and mutual care, clinicians should extend their care and support to family members, addressing their needs and concerns and involving them in the care process as appropriate.
Sixth, the Eastern Orthodox tradition’s understanding of suffering and death can inform clinicians’ approach to end-of-life care. Rather than viewing death as a defeat, clinicians can learn to see it as a part of the human journey that can be approached with dignity, hope, and reverence. They can support patients in finding meaning in their suffering, preparing for death, and achieving a sense of closure and peace. In the following paragraphs, we will further elaborate on the proposed strategies for dignity-conserving care, providing more concrete examples and discussion.
7.1. Holistic and Person-Centered Care
The essence of person-centered care is to consider the person beyond their medical condition. For our hypothetical 65-year-old cancer patient, the holistic care approach would not be limited to administering pain management drugs but would extend to addressing her emotional and spiritual needs as well. A trained counselor could support her to express her feelings and fears, while a spiritual advisor could guide her to navigate existential questions and find solace in her faith.
The incorporation of family members into the healing process is also crucial. Since Eastern Orthodox tradition emphasizes familial bonds and communal interdependence, enabling the patient’s family to actively participate in care sessions (where appropriate) can significantly aid in reinforcing the patient’s sense of worth, thus strengthening their inherent dignity.
7.2. Respecting and Fostering Autonomy
Autonomy for palliative care patients, in the context of this paper, transcends the realm of making informed decisions about their medical care. While shared decision-making is indeed crucial, fostering autonomy might require creative solutions, especially when the illness significantly impairs the patient’s cognitive or physical capacities (
Entwistle et al. 2010).
For example, a terminally ill patient who was an avid gardener might find a sense of control and continuity in being able to make decisions about the upkeep of his garden, even from his hospital bed. Similarly, a former teacher might appreciate the opportunity to share her wisdom and experiences with younger generations. These seemingly small gestures can affirm patients’ self-worth, enhancing their attributed dignity.
7.3. Fostering Open and Respectful Communication
Effective communication is not merely about exchanging information, but about creating a shared understanding and fostering a human connection (
Finkelstein et al. 2015). In the context of palliative care, communication is imbued with particular significance, as patients often grapple with profound existential concerns and distressing emotions. In addition to conveying clinical information in a sensitive manner, clinicians should be prepared to listen deeply, to validate patients’ emotions, and provide emotional support. They should be aware of the power dynamics inherent in medical encounters and strive to create a communicative space where patients feel safe, respected, and valued. At the same time, clinicians should be mindful of their own emotional responses and take care of their emotional well-being. Regular debriefings and supportive supervision can provide an avenue for clinicians to express their feelings, gain emotional support, and develop their communication skills.
7.4. Acknowledging and Respecting Patients’ Unique Identities
Every patient has a unique life story, and every life story carries its dignity. Clinicians can acknowledge and affirm this dignity by taking the time to learn about their patients’ life stories, values, beliefs, and aspirations. They can support patients in expressing their identities and celebrating their lives, for example, through life reviews or legacy projects.
Importantly, this approach is not about imposing a particular narrative or identity on patients, but about helping them to reclaim and reaffirm their own narratives and identities. It requires clinicians to approach each patient with an open mind and heart, to respect their individuality, and to see beyond the stereotypes and stigma that often surround serious illnesses and dying.
7.5. Including the Family in Care
As touched upon earlier, family members play a crucial role in dignity-conserving care in the Eastern Orthodox and central European contexts. Inclusion of the family in the care process is important, as they not only provide emotional support to the patient but also hold valuable insights into the patient’s personal life and preferences. Regular family meetings and family-centered interventions, guided by a skilled clinician, can strengthen the mutual understanding and cooperation between the care team and the family, facilitate shared decision-making, and enhance the dignity and comfort of the patient.
7.6. Cultural and Spiritual Sensitivity
Cultural and spiritual sensitivity is integral to dignity-conserving care (
Eriksson 1991;
Eriksson et al. 2013). Clinicians should respect patients’ cultural beliefs and practices and be prepared to accommodate these beliefs and practices as much as is feasible in a clinical setting. This might involve facilitating access to cultural or religious resources, adjusting care plans to accommodate cultural or religious customs, and working with cultural or religious advisors to provide culturally and spiritually appropriate care (
Lavín 2002).
In the Eastern Orthodox context, spiritual care often involves accompaniment, prayer, sacraments, and guidance toward a peaceful and meaningful passage from this life to the next. The spiritual advisor, often an Orthodox priest, plays a vital role in providing this care. Yet, all members of the care team can contribute to spiritual care, for example, by showing empathy and compassion, listening to patients’ spiritual concerns, and by offering words of comfort and hope.
The strategies we have discussed are interconnected, reinforcing each other in a holistic and person-centered approach. We have sought to balance the need for detail with the risk of oversimplification, acknowledging that each strategy deserves further exploration and contextualization. Importantly, we understand dignity-conserving care as an ongoing quest, a commitment to learning and growing, and a call to honor the mystery and sanctity of life and death. We hope that our discussion has shed some light on this quest and offered some inspiration and guidance for clinicians, educators, and researchers.
We are convinced that dignity-conserving care in palliative contexts requires a comprehensive, person-centered, and compassionate approach that respects and upholds the dignity of patients. It demands not only clinical expertise but also moral sensitivity, emotional maturity, and spiritual depth. It calls for a healthcare culture that values each patient as a unique person, recognizes the sacredness of life and death, and strives to preserve and affirm human dignity in the face of suffering and dying.
8. Conclusions and Future Directions
Our study highlights the importance of a nuanced understanding of human dignity in healthcare, particularly in the care of hospitalized patients. Drawing upon an ecumenical Christian theological perspective and empirical insights from the central European context, we argue that human dignity is a multifaceted concept that involves not only inherent dignity rooted in the theological notion of being created in the ‘image of God’, but also attributed and infrangible dignity, which are shaped by individual capabilities, societal values, and interpersonal interactions.
We contend that this understanding of human dignity has profound implications for patient care. It calls for an approach that not only respects patients’ autonomy and privacy but also acknowledges their unique identities, addresses their spiritual needs, and fosters respectful communication. In palliative care contexts, this approach can guide clinicians in navigating difficult ethical dilemmas and fostering a culture of dignity-conserving care.
However, our study also points to several areas for future research. For instance, while we have focused on Christian theological perspectives, more research is needed to explore how human dignity is understood in other religious traditions and how these understandings might inform healthcare practices. Similarly, while we have drawn upon empirical insights from the central European context, further research is needed to examine how cultural, political, and socio-economic factors might shape understandings and practices of human dignity in different geographical regions. Furthermore, more empirical research is needed to understand how the strategies and practices we have outlined can be effectively implemented in different healthcare settings and how they might impact patient outcomes. For instance, future studies could explore how shared decision-making or person-centered care approaches might enhance perceived dignity among hospitalized patients or how spiritual care interventions might influence patient quality of life and dignity in palliative-care contexts.
Finally, we call for more interdisciplinary dialogue and collaboration among theologians, ethicists, clinicians, and other healthcare professionals. As our study suggests, understanding and upholding human dignity in healthcare is a complex endeavor that requires insights from various fields. By fostering such interdisciplinary dialogue, we can collectively work towards a healthcare system that truly respects and upholds the dignity of all patients.


{kind=link}
