1. A Narrative of Ageing and Spirituality: Reflections on the Ageing Journey and the Spiritual Dimension
Narrative has been woven into human history, at times being more prominent while at other times, being seemingly more hidden. Narrative, expressed through human biography, or story, is vital to human identity and flourishing. If we lose contact with our story, our identity may become diffused, we risk alienation from each other, and we may lose vital connections within our community and culture. Those who have religious faith affiliations, and particularly those of the Abrahamic faiths, will find that story connects them to their faith, and to their identities as people of faith. Story adds connection, depth, and a sense of continuity to the human journey. Story evolves over the lifespan, and yet our very individualities are diminished if we are seen only as autonomous individuals. Human beings are made for connecting with others. This need for connecting with others has been emphasised during the COVID-19 pandemic, when so many social and emotional connections have been fractured, and especially among the weakest and most vulnerable members of societies, as people have sought to halt the spread of the contagion. This has been particularly so for older and frail people, and for those with dementia. The necessary emphasis on physical and social distancing has had its most devastating effects on older adults, on those who live alone, and, most notably, on those who live in residential elder care where, often, not even their loved ones have been able to physically visit. Platforms such as Zoom may or may not have been helpful in making connections between these people. Physical care and the prevention of the spread of COVID-19 have been important; however, without spiritual nurturing, the experiences of isolation can be devastating, and the normal modes of the affirmation of narrative become weakened among those who are separated from loved ones. In such instances, older vulnerable and isolated people may fail to thrive and may become even more susceptible to losing hope and succumbing to infection. This was particularly noticeable during the lockdowns that were associated with COVID-19, but it could occur in relation to other highly infectious diseases in the future.
2. Where Does Spirituality Fit into the Narrative?: A Brief Historical Perspective
Having said that narrative is vital to our identity, and to our continuing connections with others, where then does spirituality sit in relation to narrative and identity? Could spirituality be just a modern Western invention? If we look at the past, we see that healing was part of the narrative of religion in prehistoric and biblical times; however, it seems there was no conversation about ageing, and the spiritual dimension in those times as a more holistic view of human life was seen. Such was the closer relationship between religion and healing in earlier times (
MacKinlay and Cameron 2019). Religion was closely associated with health, and with the culture and tradition that formed important ways of living. However, it seems that spirituality was not separately spoken of; it was assumed to be part of religion, which, in turn, was assumed to be part of being human. Just as spirituality was not treated separately from religion during biblical times, ageing was not addressed separately from the rest of the lifecycle during earlier millennia. The lifespan was also generally shorter than is seen today in Western countries; for example, in the time of the Kings of Israel, including David, the average life expectancy was about 46 years of age (
Knight 2014). In the Old Testament, it is said that Methuselah lived 969 years (Gen 5: 27, NRSV), although his exact age in years cannot be confirmed. His long life was certainly not the norm.
Over recent centuries, the increased perception in Western societies of religion as a private pursuit has pushed the narrative, or dialogue, of the spiritual and religious to the personal and private domain. Another important change that occurred over time was that, as societies became more complex, health and healing moved from being controlled by churches to being controlled by secular societies. Where religion previously had a role in health and healing, this was largely taken over by the state. From mid to later nineteenth century, with the rise in the research into health, it became apparent that the concentration on physical health and illness care missed something important: the religious or, for some, the spiritual dimension. The lack of spiritual care in healthcare became even more obvious from the mid-twentieth century.
2.1. What Is Spirituality, and How Are We to Understand It?
Is the spiritual dimension separate from the psychological dimension? Can the spiritual dimension be investigated by scientific means? Can we measure it? If we can’t measure it according to scientific measures, it is not science—is it? How do we study this dimension? Is it important to study? So many questions. In this article, I attempt to address just some of these questions in relation to the current knowledge of spirituality, issues regarding its definition, and how religion and spirituality connect. I will focus primarily on the spiritual dimension as it relates to ageing. I will consider the question of the differences in the understandings of the spiritual dimension between different health and ageing disciplines in their body of knowledge and their practices. Finally, I will look to the future of spirituality and ageing in terms of research opportunities for building effective practice. I begin, now, to briefly consider more recent scholarship on ageing and spirituality, before considering the relationship between the understandings of spirituality between disciplines, and how new knowledge may be used in clinical practice in health and ageing. It is also important to consider whether there is a body of knowledge of the spiritual dimension that could be transferrable across disciplines.
2.2. The View from the Twentieth Century
During the 20th century, with rapidly developing discoveries in science, particularly in the biological, psychological, and social sciences, the spiritual dimension came under increasing scrutiny. Although, in historical times, religion and health had been closely linked, with the increasing advances in science, these links were largely lost, and some in the helping professions began to ask: What about religion and spirituality? Often, these types of questions were asked by members of a discipline, such as nursing, psychology, sociology, social work, or medicine. Each discipline viewed the same questions from within their own socialisation into their profession. There was little cross fertilisation of knowledge across disciplines.
While there were earlier examples of the study of the spiritual dimension in the literature, to begin, I will take an example from nursing, where one author stands out from the others for her foundational work during the 1970s. Ruth Stoll, who was an American nurse, introduced a model of spiritual assessment, and it is worth briefly looking at her assessment questions more than 50 years later. Below are her questions, which were to be used by nurses in the assessment of the spiritual needs of their patients in clinical practice.
Stoll’s (
1979) spiritual assessment asked just four very basic and broad questions:
Is religion or God significant to you? If yes, can you describe how?
Is prayer helpful to you? What happens when you pray?
Does a God or deity function in your personal life? If yes, can you describe how?
How would you describe your God or what you worship?
These questions still remain relevant today, in 2022. A twenty-first-century article on spiritual assessment from a nursing perspective (
Harrington 2016) provided evidence of the relevance of the same questions. Harrington also unearthed the complexity and variety of spirituality definitions, as well as the growing body of evidence in the literature for the positive effects of religiousness and spirituality on health, and particularly for older people. Like Stoll, Harrington examined spiritual assessment and affirmed its importance in healthcare.
3. A Multiplicity of Voices
Nursing was not the only discipline that was studying and working within the field of spirituality. The narrative of the nature of the spiritual dimension was being told by multiple voices. Jeff Levin, with a background in epidemiology and population health, is well suited to explore the development of the research and scholarship in religion and health.
Levin (
2017) wrote an important article titled: “
For they Knew Not What It Was”: Rethinking the tacit narrative history of religion and health research.” Levin suggested that there were many misperceptions about the history and the scope of the field of religion and health (a slightly different perspective than the one that I take in this paper, since I am more particularly interested in the broad field of ageing and the spiritual dimension).
Levin wrote (
Levin 2017) that there is no need to recreate the wheel; that is, we need to know what research is already there, and to read and critically examine already published research, enabling the building of new informed knowledge. In general terms, Levin asserted that reputable medical journals had published research in this field dating back to the 19th century. In his review, Levin suggested three types of reactions are prominent in this field of study, now, and over the past three and a half decades: the first type he called reactive (defensive apologetics); the second he called quixotic (ideologic crusade); and the third he called dispassionate (deep description) and commitment to unpacking the lived experiences of those experiencing the phenomena. According to Levin, it is this third type that ought to form the model from which research can fruitfully develop. Levin was writing from a North American perspective, which views this area more particularly through the lens of religion than it does through the spiritual dimension. A question that might be asked by the different disciplines of research and practice is: Of what value is a qualitative study of religion? It seems to me that this view of religion could be well suited to learning about the lived experiences of people of faith; however, at the same time, it may not provide the kinds of answers that medical practitioners have traditionally used to reveal new knowledge.
3.1. Seeing People as Whole Human Beings
I want to continue the narrative with a broad picture of what it means to be a human being. To understand what it means to be human, we need to see the whole person, to take in a picture of body, mind, and spirit. We are not simply biological beings; we can only be understood completely, if at all, by taking into account the human body, mind, and spirit (
Frankl 1984). Humans are complex beings, and we have many features in common; yet, each of us is a wonderfully created and unique person, held in community with others.
Soon after the dawn of the twenty-first century,
Sulmasy (
2002), a medical doctor, philosopher, and bioethicist, wrote a key article emphasizing the necessity of considering the whole person in need of care, adding the often-forgotten dimension of the spiritual to the already clearly accepted biopsychosocial paradigm. At that time, Sulmasy challenged those in healthcare to rethink their view of the person in need of care. Sulmasy proposed “that human persons are intrinsically spiritual” (
Sulmasy 2002, p. 25). At the same time, it is important to consider that both the body and the spirit are needed, which is consistent with the Pauline writings from the New Testament (“do you not know that your body is a temple of the Holy Spirit?” (1 Corinth. 6:19 NRSV)), which emphasise that, in Christian understanding, the human body is essential for this indwelling of God’s Spirit. This gives the body an important place in God’s plan, and it emphasises the holistic nature of the human being. This view of the human person denies a dualistic perception of the person; the person is of one entity, and not a separate body and soul, or spirit. Sulmasy’s article was a timely move towards thinking and acting wholistically in the provision of healthcare. In this article, more than twenty years later, we can legitimately argue for the centrality of the spiritual dimension of being human within whole-person care. It is from this basis that we now briefly consider human religious and spiritual needs in multicultural and multifaith societies.
Human religious needs are, for the most part, worked out through the major world faiths: Judaism, Christianity, Islam, Buddhism, and Hinduism, as well as other religions. Complexity of the practices of the major faiths is further played out through cultural influences in different countries; we see that there are Eastern perceptions and Western perceptions in terms of what the same religious faith may look like and be experienced, even within the one religious faith of Christianity. When you add to this the fact that, in the twenty-first century, many populations of Western countries live in multicultural and multifaith communities, it is evident that a multiplicity of variations in the practices of religious faith may be present in any given Western society. Some of these variations may arise from the growing lack of confidence of people in the established church institutions, while part of it may be due to the nuances in cultures and influences of social media in twenty-first-century Western societies.
Geertz (
1968) illustrated this phenomenon in his study of the Muslim religion in different cultures through periods of history in Morocco and Indonesia. He wrote that, while the faith remained the same, the way that the faith was practised changed over time within the particular culture.
3.2. Cohort Differences in Ageing
Another factor that creates differences in the health and well-being of people within society is the cohort into which one is born. Each cohort has different social, educational, and health opportunities and challenges as its members come to maturity and live out their lives. These opportunities and challenges are seen in numbers of social indictors and attitudes towards life in each cohort. In recent studies of the now ageing baby boomer cohort, it has become clear that its members are similar to those of the cohorts that have gone before them; however, they also differ in a number of important ways. Some of the differences are related to retirement timing, patterns of housing, and gender changes in work in patterns among ageing baby boomers (
Byles et al. 2013). Baby boomers are making different choices about the way that they want to live in retirement, with not so many wanting to live with family in later life, while friends were becoming more central in their lives. It is likely that a higher proportion of ageing baby boomers will not wish to move to residential care unless there is no other alternative (
Dychtwald 2015;
Quine and Carter 2006). Most research on ageing and retirement has focused on the physical and social aspects of ageing, while little attention has been paid to religious and spiritual ageing among baby boomers. For example, a study of ageing baby boomers in Australia (
MacKinlay and Burns 2017) found that higher proportions of this cohort saw spirituality as important, but they had lower levels of religious affiliation than was the case for the builder cohort before them. The builder cohort had higher levels of religious affiliation, while spirituality was not as well understood by them. Cohort differences in religious and spiritual needs warrant attention from elder care, pastoral care, and healthcare providers. These differences not only relate to the way religion is practised by different cohorts, but also have implications for the design of purpose-built elder care facilities in relation to lifestyle choices, quiet spaces, and environmentally friendly places. These cohort differences may lead to re-thinking religious and spiritual needs of the large upcoming ageing cohort of baby boomers, who are rapidly overtaking the previous cohort in their numbers, with differing needs in their later years.
4. The Relationship between Religion and Spirituality
I am not going to specifically define spirituality or religion, as this has been addressed in numerous articles and books over the past couple of decades (
Koenig et al. 2001;
Koenig 2015;
Harrington 2016;
MacKinlay 2017;
Peteet et al. 2019;
de Brito Sena et al. 2021). A common criticism of spirituality is that it is hard to define. A question: Is it spirituality that is hard to define, or do at least some of the problems of spirituality lie in the eyes of the beholders; that is, in all of us who have an interest in the domain of the spiritual? We each see, from our own enculturated position, our own health and ageing perspective, our own age cohort, and our own religious or secular viewpoint, and then, we only see what we expect to see, and we may therefore risk being disappointed.
In the past, we have often used the terms “religion”, “religiosity”, and “spirituality” indiscriminately. Indeed, the common expression heard within the community over the last several decades is: “I’m spiritual, but not religious” (
MacKinlay 2017).
Sheldrake (
2016) pointed to the need to consider the context of the spiritual, the importance of culture, issues regarding political aspects of spirituality, and that spirituality may express the values and commitments of the group.
With the diversity in the numbers of disciplines that are now taking an interest in matters of the spiritual, Sheldrake asserted that theology must take notice of the varied disciplines, methodologies, and domains of practice (
Sheldrake 2016, p. 19), and engage in the dialogue. Sheldrake’s view of the spiritual is more inclusive than those of some others (for instance, the very individualistic perspectives found in the data from the studies of
Bellah et al. (
1985), citing one instance of a nurse who had her very own religion, which she named for herself: “Sheilarism”, unique and one of a kind).
Broadly, when differentiating between religion and spirituality, we could say that religious faiths tend to bring people together in community, with shared religious practices and beliefs, while spirituality often takes a modern Western view of the autonomous human being, complete and individual within themselves. From my personal perspective, based on my faith world view and influenced by research findings, my own and others’, over a number of decades, I would like to share how I see spirituality at this point in my life, as an octogenarian. I see spirituality as an essential component of being—it is what brings meaning into my life, it lies at the very core of my being, and is the source of my inner strength. Spirituality, for me, is closely associated with deep relationship—connectedness and intimacy—which is to be known as I am known (
Carroll and Dyckman 1986, p. 123). I cannot separate my spirituality from my religious practices; these are my responses to my faith. For me, my spirit connects with God’s Spirit, and it concerns the journey of the transformation of myself over time. I now turn to consider concepts and understandings of religion and spirituality, as relevant to this article.
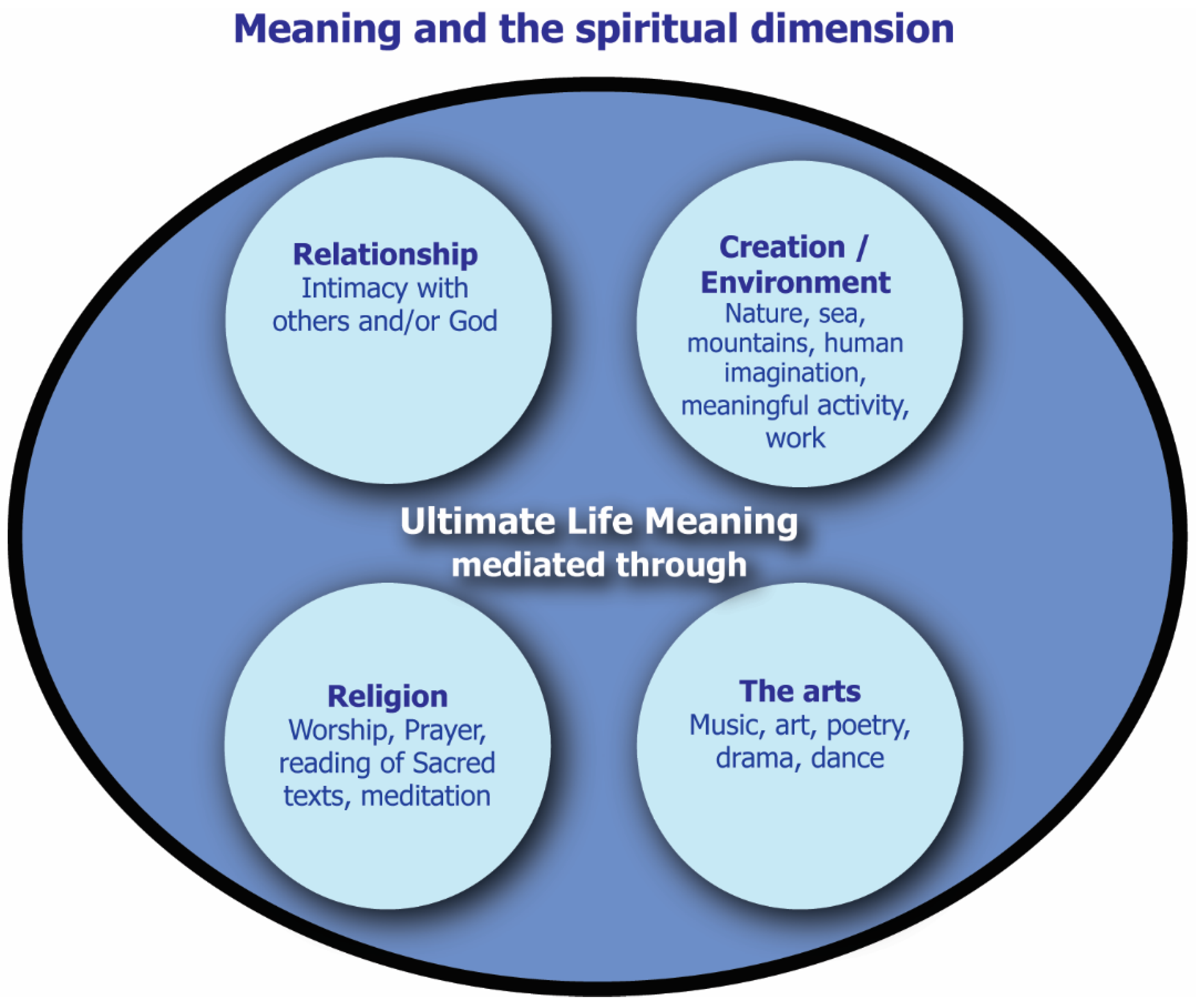
4.1. How Is Spirituality Mediated by Human Beings?
Debate continues about what spirituality is and is not, and its relation to religion. I see this as an important question which has engaged many authors in this field. I like to illustrate the relationship between religion and spirituality (illustrated in
Figure 1) on earlier research (
MacKinlay 1998,
2006,
2021;
MacKinlay and Trevitt 2012): First, I see the spiritual as essentially, reflecting all that brings meaning into the life of a person, both within themselves and in their responses to others and to the world. This sense of meaning is evolving through the lifespan unless it is blocked for some reason. I see four main ways in which the spiritual dimension (meaning) is mediated: through relationship (human and/or divine); through creativity/creation/the natural environment; through the arts; and through religion. I explain each of these briefly.
4.2. Relationship and Spirituality
Of course, relationship is well recognised in the field of psychology. However, I contend that there is a spiritual dimension to relationship too. This spiritual perspective of relationship is perhaps best expressed as connectedness, and it is the greatest depth to which relationship can be expressed and experienced. At the very depth, it is Love. It is possible to connect effectively with others when the person feels comfortable within themselves. This notion of the spiritual dimension of relatedness can be both with others and/or with the divine, however, it is understood and expressed by the person. This depth of meaning through relationship can be experienced, at times, even in a deep pastoral conversation, one-on-one, where suddenly one knows that they are on sacred ground. At such times, words may not be necessary. The conversation has moved and at that moment, nothing is more important than this present sense of being and the interaction between the two people. The conversation holds the story that is being shared, even in the silences. The narrative is revealing identity, at the depths of being, shared between storyteller and story listener. The deep sharing of one’s story is a means of entry into deeper relationship, and is a spiritual experience to be treasured.
4.3. Creativity/Creation/Natural Environment
Have you ever been overwhelmed at the sight of a glorious sunrise or sunset? By the wonderful vista of a shining sea? As humans, we are sometimes “struck” by the experience of the “numinous” (
Otto 1952), by something that takes us out of the everyday mundane experience of life, or by something that may be remembered for a long time to come. Likewise, those who work in research, or who write, may suddenly be drawn into a sense of wonder at a new discovery, or into the experience of having written or read something of immense significance to them. Human imagination lies at the heart of all creativity and invention. There is a spark that brings inspiration and wonder.
4.4. The Arts
It is hard to separate the arts from creativity and, in fact, they are closely linked. Both creativity/creation and the arts are the products of human imagination. In the natural environment, which I see as connected to creation and to creativity, it is often the person who responds in wonder; however, the person may also become a co-creator through activities such as gardening. In the arts, it is the person, or a group of people, that actively engages with imagination, creativity, and physical being in bringing art, dance, music, drama, and poetry into existence. The arts, then, become a source of joy for others as well, and the arts can express both the heights and depths of human emotion. It is significant that people who have dementia, and even advanced dementia, can often still actively participate in art forms. At these times, one may be privileged to see the joy of connecting on the faces of those with dementia.
4.5. Religion
Religion is a way of bringing all of the components of the ways in which humans express the spiritual dimension together, and this is expressed in community through formal worship, prayer, meditation, and other forms of religious practice. Religion may be played out in the major religious faiths of the world, or religious behaviours may be played out in very secular ways. A well-functioning religious faith will include each of the other three aspects of mediating spirituality: relationship, creativity/creation, and the arts. The human need to find meaning may be met through the expressions of meaning carried by symbols and rituals. This occurs in situations of the felt need for expressions of national celebration, grief, or tragedy. People who have no religious affiliations still engage in spirituality through relationship, through creativity/environment, and through the arts, and they also engage in various aspects of ritual and symbol.
5. What, Then, Do We Know about Spirituality?
There is little dispute, at this point in history, that the spiritual dimension is deeply connected with finding meaning, and that the search for meaning is often engaged in story work and narrative (
MacKinlay 2017,
2019;
Gibson 2019). Story, itself, becomes the vehicle for the transmission of the individual narrative, and for the affirmation of that narrative by others. Meaning is a crucial factor in human well-being. This has been clearly recognised by numbers of researchers now. Relationship is another important component of the spiritual, and especially in terms of connecting deeply with other human beings and, for those with religious affiliation, relationship with the God of their understanding. Self-transcendence or transformation is associated with the spiritual dimension; but, it is also associated with religious faith, most scholars include all these aspects in their definitions of spirituality. As well, mystery continues to exist about some deep aspects of life, which
Otto (
1952) defined as the numinous or the sacred, which may also be felt and understood as an expression of the spiritual. Feelings of the sacred may strike people unexpectedly, whether they are religious or not (
Otto 1952).
6. Spirituality—A General or Developmental Perspective in the Context of Ageing?
There are different views as to whether religion and spirituality change through the lifespan. Implications of accepting an unchanging spirituality over the lifespan may lead to an easier acceptance of a general framework for whole-person care, such as recommended by
Puchalski et al. (
2014). However, even if this was so, recognition of heightening of spiritual needs, at various times, may make the general framework unpractical (for instance, in palliative care, ageing, and mental health, to provide just three examples). It is also important to consider that the spiritual dimension is not only about spiritual needs, but also a dimension with potential for continued spiritual growth and development, and for transformation or self-transcendence across the life-long journey.
The view of the potential for continuing spiritual change through life challenges the general framework that fails to see spirituality in developmental mode. The possibility of spiritual growth (and spiritual distress) may occur throughout life. This developmental mode is highlighted in
Erikson et al.’s (
1986) stages of psychosocial development, which is widely acknowledged as a life-long process.
Erikson et al. (
1986) and J.
Erikson (
1997), both acknowledged that, in the ninth and final life stage of psychosocial development, struggle becomes a factor, and the dystonic may create increasing challenges for octogenarians and nonagenarians. The Eriksons also acknowledged this final life stage as a spiritual stage, where the dynamic stages of psychosocial development could be reversed to bring the negative to the fore. Thus, the stage of integrity versus despair becomes despair versus integrity, with despair becoming the dominant position. Yet, this final and more precarious stage, they said, may become a time of spiritual growth (
Erikson 1997).
Other important scholars who have written specifically on ageing were Robert
Butler (
[1963] 1968), well known for his early work on reminiscence in the 1960s, who was closely followed by Peter
Coleman (
1994). These ground-breaking researchers in psychiatry and psychology changed a generation’s thinking on gerontology from the 1960s onward. Mel
Kimble (
1990), with his leadership in scholarship (
Kimble et al. 1995;
Kimble and McFadden 2003) in pastoral theology, offered a vision for ageing and the spiritual dimension that reached beyond the biomedical paradigm. Following these developments in scholarship, a new focus of study was seen with the work of
Goldsmith (
1996) on specialist ageing and pastoral studies in dementia and dementia care, while
Kitwood (
1997) pioneered the critical breakthrough of knowledge that began with the notion that, in dementia, the person comes first. Swinton’s work, and especially his book
Dementia: Living in the memories of God (
Swinton 2012), written from a practical theological perspective on disability and dementia, brought yet another important direction to the scholarship. Gradually, voices from theology have been heard within the multiplicity of voices of elder care and health professionals.
6.1. The Challenges of Studying Religion and the Spiritual Dimension
Definitions of spirituality continue to be published within current healthcare research, and a systematic review of the research on defining spirituality in healthcare was conducted by
de Brito Sena et al. (
2021). Searches were conducted through PubMed from a total of 493 articles, 166 were included in the final analysis. Their review found 24 “spirituality dimensions” (
de Brito Sena et al. 2021 pp. 3, 8). Most of these are related to connectedness and meaning of life. On closer inspection of the 24 ”spirituality dimensions”, it becomes clear that the numbers of these can be realistically grouped as the major themes and related subthemes of spirituality, and, indeed, as the authors claim, most of them fit into connectedness and meaning. I note that some may not really be spiritual at all; for example, “human aspect”, “dynamic process”, “values”, and “practices/behaviours”. I suggest that these terms would need to be set within a context that identified them as spiritual, and that they could not be designated as “spiritual” without further information. Of course, it is important to move beyond definitions, at some point, to examine the implications of the research findings and to translate knowledge into practice.
There are a number of challenges to be aware of in study of this field. Appropriate research methods are important; however, so is who and what we study. If our interest is in older adults, then we should choose to study or search out research reports of older adults in the field of our interest. None of us have the gift of unlimited time to cover the whole field, and so, in gerontology, we will necessarily confine ourselves to issues of later life, and to mostly cross-sectional studies. However, longitudinal studies are also valuable to consider (even though they are often too expensive to conduct over long periods of time, and it is impractical to follow the same cohort of people over many years). There are numbers of national longitudinal metadata studies that are available these days that follow the same participants in study waves across many years that provide rich data, and especially in health and social research; these can be used for comparison against the findings of smaller cross-sectional studies.
de Brito Sena et al.’s (
2021) recent systematic review drew on the work of
Koenig (
2008) and
la Cour and Götke (
2012) to describe spirituality as “a broad and complex concept which varies its understanding according to different cultural, religious and academic backgrounds” (p. 1). If we consider religion or spirituality in terms of our own disciplines of practice and study, we will tend to apply our specific knowledge and ways of thinking to the study of religion and spirituality. For instance, if we look at religion through the lenses of science, we will tend to see religion framed in scientific terms. The same may be said of the way that we look at the spiritual dimension, or spirituality. An important question becomes: Are we using the best means of studying the phenomenon of interest?
We need to be cognisant of culture as well, and of the ways in which religion and spirituality are played out in various cultures (
Geertz 1968). We would also be wise to ask what perspectives of religion or the spiritual do we wish to know about, and, indeed, why we are interested. Our choices of research methods are also important, and different disciplines of practice tend to favour particular methods of study. For example, there are implications for the outcomes of research based on the choice of research methodology we adopt. We could seek to follow, as passive observers, the outward evidence of the religious faiths of others, or their spiritual behaviours, and base our findings on observations or on surveys. Or we could take a different approach, which is to place the consumers of health, ageing, and spirituality at the centre of the research process in the study of their lived experiences. However, in whatever way we choose to study, we, too, must admit that we are engaged in this dialogue and discovery; we bring all that we are and know to engage with the phenomenon under study. But even as we study, we too are at risk of being changed by what we see, and we perhaps will learn new ways of being. Furthermore, as we engage in the study, we too may influence the very phenomenon that we study. Perhaps this influence will be by way of the questions that we ask and, importantly, the questions we do not ask. Research, of course, is not an end in itself, but a means of learning new information that may lead to better health and to better life experiences. To be of real value, the outcomes must be translatable to practice.
6.2. Translating Spirituality Research into Elder Care
A recent article by
Peteet et al. (
2019) on integrating spirituality into care of older adults concentrated on integrating religious/spiritual (R/S) involvement into healthcare, particularly from the medical and psychiatric perspective. The article addressed the perceived consideration that many older adults want spiritual care to be offered in relation to their healthcare. The authors offered spiritual history as an important component of care.
Puchalski et al. (
2014) considered questions of setting national and international consensuses for whole-person care integrating spirituality, where they argued for agreed standards for spiritual care set within whole-person care. A salutary recommended standard of spiritual care from the
Puchalski et al. (
2014) report is presented in the list in Appendix 3. In the
Recommended Standards for Spiritual Care (Top 12), Statement Number 5 of 12 is “Spirituality in health care is developed in partnership with faith traditions and belief groups” (
Puchalski et al. 2014, p. 656). Over recent decades, there has been a tendency to isolate spirituality from faith traditions and belief groups; this may damage the whole effort to provide the best spiritual care. It is of importance to note that in the
de Brito Sena et al. (
2021) systematic review and conceptual framework of spirituality in healthcare, their results recognised “that spirituality and religiosity are related and overlapping, varying according to the cultural context and to the dynamic quality of the spirituality itself” (
de Brito Sena et al. 2021, p. 4). This recognition is vital to the development of the way forward in the practice of spiritual care in healthcare.
7. Research Methods for Spirituality and Ageing: Fit for Purpose?
How might we learn more about the spiritual dimension? We need an openness to explore ways of finding new knowledge. Collaboration with researchers from different disciplines, and thinking outside the square, are going to be important in growing knowledge in this field. The separate and combined narratives of researchers and practitioners from different disciplines will form rich and rewarding ways of seeing the whole picture, as in a tapestry, where those working together each provide enriching components to the whole. Combination of narratives will assist in the active translation of research into practice, and remains an essential factor in the way forward; we need fresh lenses for seeing the questions that arise among those with whom we work and live. The establishment of long-term relationships between those who provide spiritual care and those who research are vital; often, the best research questions come from those closest to older people: the clients and the residents. This is why we must continue to listen to the lived experiences of older people, those with dementia, those who are frail, as well as those who are engaged in ageing well.
Human imagination sparks questions that are important to what it means to be human, about our spirituality, and how we and our stories are both personal and communal. The stories are, in essence, the carriers of meaning, which are being revised at the personal and communal levels over time. Study of stories and how they reveal the spiritual is challenging, as accepted scientific modes of investigation do not easily fit the questions of spirituality. The fit would be easier if we were only looking at designing activities to keep older people entertained; however, that would be to demean the spiritual, as well as older people. Each generation needs to ask and examine afresh these deep human questions. In our day, this may be in terms of what we do not know so well about the spiritual dimension. We may continue to ask questions about the intersections between the social and the spiritual. For instance, if relationship is fundamentally important to our deepest connections with others—how is it important? How does relationship differ in the social and spiritual dimensions? In the study of effects of religious practices, how do factors of religion and social contact interact? What might it be about worship that may make a difference to health and well-being?
Recent studies are more likely to control for variables such as social factors and spiritual measures, as well as meaning and psychometric measures. However, we may need to accept that the depth of spirituality is, at least to some extent, resistant to quantitative measurement. By applying psychometric testing, we are more likely to obtain answers applicable to psychological and social questions than to spiritual questions. I suspect that we are beginning to realise that, although there seem to be close relationships between the psychological and spiritual, the spiritual domain does not lend itself well to scientific testing. On the other hand, the study of the human lived experience seems to provide rich data on the spiritual, as separate from the psychosocial. It is to these qualitative methods that we must turn, as
Levin (
2017) has suggested, to find new and valid knowledge of the spiritual. Not all knowledge is scientific knowledge.
Research Challenges for the Future
More recent research on spirituality tends to use qualitative studies (for example, phenomenological, ethnographic, grounded theories) or mixed methods, with a focus on the lived experiences of older people that can provide rich data of the participants’ views of their daily lives and experiences.
We are now more likely to listen to the voices of those who live the experience of the phenomenon that we are interested in, which was the case in a recent study on frailty (
MacKinlay 2021). In that study, using a phenomenological approach, we conducted individual in-depth interviews with frail older people in residential care, to learn of their lived experiences of finding meaning in the face of frailty. One of the notable insights from the data was the importance to participants of finding inner strength within their vulnerabilities.
We need a larger picture of life for older people, and this picture must engage and respect the experiences of older people. Stereotypes of ageing are so powerful that they may shape the attitudes and beliefs of what is possible in the experience of life for older people. In turn, these stereotypes also influence people in the wider community and those who work in elder care; the narratives of ageing are indeed powerful. The picture of possibilities for ageing must include the voices of family caregivers, professionals, and volunteers. But, too often, it is the voices of the receivers of care that are neglected. We must aim to work in collaboration with older people and with those who provide care for older people, and address the real questions of spirituality in the process of ageing and care.
We need quality research that will develop new knowledge, and that new knowledge must be translated and must inform practice in a timely manner. Appropriate education and accreditation of the practitioners of spiritual care must be highlighted across disciplines.
Questions for each discipline might include what a general framework would look like if adapted to the special needs of the particular discipline. In ageing, this framework will have several foci, it will develop strategies for spiritual growth and development for ageing well, and it will inform the development of inner strength. Another focus in ageing work will be on the final life career; that is, the journey towards dying and death. One further important factor is education on the spiritual dimension for older people, and not only for health and care providers. Not all older people are aware of the opportunities that exist for ageing well, as this has not been a part of the narrative that they have known. Finding meaning in life makes a crucial difference to the well-being of older people (
Frankl 1984;
Kimble 1990;
Koenig et al. 2001;
MacKinlay 2017). We increasingly talk of health literacy, and this conversation would benefit from the inclusion of spiritual literacy within the wider community, as well as in elder care.
8. Conclusions
The narrative of spirituality and ageing continues, and is shaped by many factors, which include the people of a society, education, social influences, health systems, religions, and research. To take just one aspect of this as we move forward, I believe that there are benefits to be gained by the cross-disciplinary work in spirituality and ageing, and that, for this, we need a willingness to communicate across the gaps, and to learn to see through the eyes of others as well as our own, whatever our discipline of practice. Demarcations between disciplines of care and scholarship can block new ventures and fertile avenues of inquiry. Listening to each other and visioning together is vital. It is also vitally important to include the people whose lives we care for—the clients and patients—in our conversations.
Spirituality in ageing is not simply about care for the weak and vulnerable, although this is something important that we often concentrate our energies on. The spiritual dimension in later life is also about the older person maximising their spiritual well-being and finding meaning in their existence. It is in this vein that the notion of spiritual tasks and process of ageing (
MacKinlay 2017), and the continuing development of spiritual growth in the final life career, necessitate special knowledge and skills of practitioners to engage effectively with these older people. The kinds of losses of relationships in later life are profound, and different in nature to losses in earlier life, even though earlier experiences of loss may nurture and prepare people for the larger losses at this late-life time. Moreover, added issues may be experienced including frailty, dementia, and the final life career that encompasses the process of dying at the end of a very long life. However, on the other side of the ledger are the bonuses of living life to the full, despite the losses and disabilities; of finding meaning; of realising what the whole of one’s life has been about; and of deepening relationships, in special instances.
The spiritual journey is about connecting with our individual and community narratives, and it is about finding meaning at the end of our lives, and about knowing that our lives were lived well and that they have meaning. Knowledge of spirituality and its place in our lives is gaining more attention, generally; however, there are also crucial points of heightened importance in the journey of ageing and spirituality. Two of these crucial points are the onset of frailty and dementia, and their trajectories invite dialogue around end-of-life matters, when spiritual needs are more likely to be raised. It is in these circumstances that the search for personal life meaning is more likely to be raised, as well as questions such as “why am I here?” and “what has been the purpose of my life?” I am thankful for having the privilege to be on this journey with other older people and those with whom I work. We have yet more to learn about later life, and the lived experience of those who journey.



{kind=link}
