1. Introduction
Religion and spirituality (R/S) have shown to be a protective factor in (mental) health (
Koenig 2015). In line with this, patients suffering from mental illness can experience a comforting, positive side of R/S. At the same time, for many psychiatric patients, their R/S also can have a distressing, negative side (
Pargament and Exline 2020). These two aspects have been referred to as the ‘double-edged sword’ of R/S (
Pargament and Lomax 2013).
The distressing side of religion has been described and studied in various ways.
Pargament et al. (
1998) have described negative religious coping styles, including spiritual discontent, punishing God reappraisals, interpersonal religious discontent, demonic reappraisal and reappraisal of God’s powers. In a later study, they distinguished the following three main types of ‘spiritual struggle’: intrapersonal, divine, and interpersonal (
Pargament et al. 2005). Intrapersonal struggle may consist of feelings of guilt or doubt. Divine struggles can include anger or anxiety towards God. Interpersonal struggles can be conflicts and tensions with families, friends or congregations.
Exline et al. (
2000) developed the so-called ‘
religious comfort and strain scale’, describing thirteen possible items of religious strain, clustered in the following three subscales: alienation (abandonment, experiencing God to be far away), fear and guilt, and religious rifts (conflicts with religious others). In a later study, Exline distinguished the following six subcategories of religious and spiritual struggles: divine, demonic, interpersonal, moral, doubt and ultimate meaning (
Exline et al. 2014). In addition, other researchers have focused on ‘
God representations’ (
Schaap-Jonker et al. 2008), next to positive perceptions, distinguishing several negative representations as feelings of anxiety or anger towards God and viewing God’s actions as ruling/punishing or passive. These various themes touch on each other, and have in common that they describe negative experiences with respect to R/S. Recently,
Pargament and Exline (
2021) combined their knowledge concerning the three groups of R/S struggles and the six types of R/S struggles. For the current study, the term ‘religious/spiritual struggle’ is used, in line with
Pargament and Exline (
2020) defining this as tensions, strains and conflicts in relation to what people hold sacred.
R/S struggles are not reserved for psychiatric patients and are regularly studied in large-scale community surveys. However, clear associations with mental health have been demonstrated. R/S struggles can have a negative impact on mental health and hinder treatment and recovery processes (
Koenig 2009). They have been associated with higher depression and suicidality (
Exline et al. 2000;
Pargament et al. 2011). In addition, researchers showed associations with anxiety, paranoid ideation, obsessive-compulsiveness and somatization (
McConnell et al. 2006). Longitudinal studies show that R/S struggles significantly predict an increase in depression (
Braam and Koenig 2019) and negative psychological adjustment (
Bockrath et al. 2021) and that psychological distress also leads to R/S struggles (
Cowden et al. 2022). This emphasizes the importance of attending to R/S struggles in clinical practice. Prevalence of religious struggle in mental health care is considerable, ranging from 40% among Muslims with depression (
Abu-Raiya et al. 2015) to 50% among a population of mainly Christian patients with depression (
Murphy et al. 2016). Numbers may be highly related to the type of population, as well as to the method of defining R/S struggles. In the Netherlands, as a relatively secularized country,
Van Uden et al. (
2014, p. 29) have studied the area of negative religious coping in the context of mental health care. They concluded that among 16–36% of their study population, which consisted of mental health patients, religion has a predominantly negative role.
Although the theme has been mapped and described diversely, there remains several gaps in our knowledge. Many cross-sectional studies describe clinical associations with, for example, negative religious coping (
Braam et al. 2010) or negative God representations (
Schaap-Jonker et al. 2013). Several longitudinal studies have focused on associations between R/S struggles and other indexes of emotional and psychological well-being (
Exline 2013, p. 464;
Braam and Koenig 2019;
Bockrath et al. 2021;
Cowden et al. 2022;
Haverkamp et al. 2020) over time. However, studies that investigate the presence of R/S struggles most frequently are quantitative in nature, and often performed in population-based samples (and not specifically among psychiatric patients). Furthermore, R/S struggles have been studied predominantly in Christian and some Muslim populations, e.g., in Christian patients with depression (
Murphy et al. 2016) or Muslim dialysis patients (
Haverkamp et al. 2020). Religious affiliation indeed is a significant predictor of the presence of R/S struggles, but spirituality without affiliation can also be predictive (
Vittengl 2018).
Exline et al. (
2000) reported that people without religious affiliation had more rifts and alienation compared with others. In addition, theists and atheists are shown to have equal scores on a scale for spiritual crises (
Piedmont et al. 2020). It might be relevant to study the area of R/S struggles both in religious and less religious groups.
To our knowledge, qualitative research concerning R/S struggles in a population of psychiatric inpatients is scarce and such an approach may offer detailed and nuanced insights into the lived experiences and needs of patients suffering from R/S struggles. In this way, mental health professionals will have better awareness of how R/S struggles influence the life of their patients. This is more important because for patients, it is often hard for them to address difficult themes with regard to R/S themselves and frequently, fear and shame play a role (
Exline and Grubbs 2011;
van Nieuw Amerongen-Meeuse et al. 2019). One may question the specific relevance of R/S themes above psychosocial or biological factors. It is, therefore, important for mental health care professionals to realize that R/S struggles can not only function as symptoms of illness, but also as driving factors, inducing emotional distress, separate from personality characteristics (
Fox and Piedmont 2020). Religious impairment seems to be able to provoke psychological dysfunction (
Piedmont et al. 2007). Since the presence of R/S struggles and psychological distress can lead to a downward spiral (
Cowden et al. 2022), more insight into how to address the difficult themes concerning R/S may be beneficial for treatment success. The following research question is addressed: how do religious struggles play a role in psychiatric inpatients with various diagnoses in a secular and a Christian mental health care institution and what approaches do they experience to be helpful?
2. Method
The current qualitative study was performed in cooperation between the University of Humanistic Studies (Utrecht, the Netherlands), the Center for Research and Innovation in Christian Mental Health Care (KICG), Amersfoort, and the Faculty of Religion and Theology of the Vrije Universiteit Amsterdam, the Netherlands. The mental health clinics involved in the study were Eleos mental health care in Bosch en Duin, and Altrecht mental health care, Utrecht, the Netherlands. The study was approved by the scientific boards of the KICG and Altrecht mental health care (CWO No. 1525). The cooperating research team consisted of a clinical psychiatrist/professor (ABr), a psychologist/theologian/professor (HSJ), a psychologist (GW) and a medical doctor/post doc researcher (JvNA).
2.1. Sample and Participants
The research sample consisted of patients receiving inpatient care (77%) or day care patients (23%) in the following two mental health care institutions: Eleos, Christian mental health care (CC, N = 15), and Altrecht, mental health care (SC, N = 20). In this way, both a more heterogeneous Christian population, as well as a more varied population concerning outlook on life were included in the study. Eleos mental health care provides regular care by Christian health care professionals, and both in conversations and the therapy program, there is room to integrate R/S into care. Altrecht mental health care is a regular, secular institution, offering, at most once a week, sessions of meaning making and individual conversations with a spiritual counselor, but not including any specific R/S program.
Patients were in the age of 18–65 years and the mean age of the patients was 45.3 years (SD 12.6). The psychiatric diagnoses showed considerable variation and many patients had more than one diagnostic classification. The most common diagnoses were as follows: depression (51%), anxiety disorders (46%), personality disorders (46%), psychotic disorders (23%) and autism spectrum disorders (11%). Religious affiliation of participants differed between the two clinics; the CC represented pietistic reformed (N = 5), orthodox reformed (N = 5) and evangelical (N = 5) patients and the SC represented orthodox reformed (N = 3), evangelical (N = 3), ecumenical (N = 2), roman catholic (N = 3), Christian without denomination (N = 4) and non-affiliated (N = 7) patients.
2.2. Data Collection
Data collection was part of a larger study (
van Nieuw Amerongen-Meeuse et al. 2018,
2019,
2020). Patients had been recruited by their clinician, by a nurse or by the first author, who visited the wards and also interviewed the participants. They were asked to participate in a face-to-face semi-structured interview, concerning the role of religion and spirituality in mental health care. From the patients invited to participate, about 70% agreed to do so. The main reason not to participate was a lack of energy due to illness and treatment. Patients received detailed information about the study and gave written consent to assure anonymity would be provided, termination of the interviews was allowed at any time and the interview would not influence treatment. The participants agreed that the researcher took notice of their DSM-5 diagnoses for the analysis. The interviews lasted 30–60 min, no other persons were present during the interviews and no repeat interviews were conducted. The questions most relevant for the current study are presented in
Table 1. For a more extended description of the sample and data collection, one can refer to the work of van Nieuw Amerongen-Meeuse et al. 2019).
2.3. Data Analysis
The interviews were audiotaped and transcribed verbatim. Data were analyzed using a narrative approach. An important assumption within narrative analysis is that storytelling serves the purpose of creating meaning from one’s lived experiences (
Riessman 2008). The interviews contained a significant amount of information concerning patients’ R/S, its function during their illness and experienced R/S troubles, as well as R/S support. To gain insight into the function of R/S struggles, the relations between R/S support and R/S struggles and the (un)helpful approaches patients experienced, an inductive narrative analysis seemed appropriate. A narrative analysis offers insight into how patients experience the totality of these matters, and how they construct their story of R/S struggles in the context of their illness. In addition to the narrative approach, a deductive thematic analysis was applied, in order to examine to what extent the theory on R/S struggles, following the work of
Pargament and Exline (
2021), could be recognized in the current population. Based on the narratives, a final conceptual model was created as a result of different preliminary models trying to capture the main codes and their interrelations, as perceived by the researchers.
For the narrative analysis, the model fitting to relatively homogeneous empirical material, as described by
Blom and Nygren (
2010), was followed. First, the interviews were naively read and memoranda from these readings resulted in a primary understanding of the material as a whole. Second, two researchers (the first author and a student research assistant) cut four transcripts into narrative blocks and compared and contrasted them to develop inductive narrative core codes. After this, the first author performed a structural analysis and coding of all transcripts, resulting in a primary totality of codes. At this point, the code table was discussed and reorganized with one of the co-authors (GW), on the basis of double-coding of four interviews. All interviews were then partially recoded for a second time by the first author, using the adapted code table, resulting in a secondary totality of codes. This functioned as a basis for the results section.
For the deductive thematic content analysis, the six categories of R/S struggles, as described in the introduction (
Exline et al. 2014), were analyzed regarding their presence and function in the interviews. These were as follows: divine struggles, demonic struggles, interpersonal struggles, moral struggles, questions of doubt and questions of ultimate meaning. Two of the authors independently determined the presence of the types of struggles per interview and discussed their findings until they reached consensus.
3. Results
3.1. Illustrative Cases
Klaas (36) has suffered from schizophrenia, the paranoid type, since he was a young adolescent. During acute psychoses, fear for the devil plays a main role, which is accompanied by fear for nonreligious mental health professionals. He does not trust them. He describes his experiences as ‘the hell on earth’. A friend, who is a pastoral counselor, explained to him that God may use nonreligious people, and that helped him to gain trust. Apart from moments of crises, he sometimes feels God to be far away. He has the following question: why am I alone for such a long time? At the same time, he believes that God is full of understanding and will guide him out of these troubles. He once experienced answer to his prayer by the arrival of a friend, solving his loneliness for the moment and he sometimes feels God’s presence by enjoying nature (CC3, man (36), orthodox reformed, schizophrenia).
Irmgard (46) suffers from depression. She is also diagnosed with a dependent personality disorder. Her R/S background is liberal Christian, and coming from abroad, she has troubles finding a denomination that fits her. She thinks people in the Netherlands are at a distance, ‘it is every man for himself’. She doubts God’s existence and does not feel at home in churches that are too strict and that do not allow doubts. In the past, she also had experiences of being heard by God, but during her depression, these experiences have all gone. She admitted that her husband is considering a divorce and she feels very lonely. She enjoyed exploring the matters of meaning in life issues during her stay in the mental health clinic, but does not know whether there are spiritual counselors. Group sessions with attention to meaning in life are disappointing to her because the professional mentions ‘a job’ as meaningful and all other depressed patients have troubles in defining meaning in life. When another patient encouraged and embraced her, they received a reprimand, but she very much longs for connectedness and love (SC11, woman (46), not affiliated, dependent personality disorder).
3.2. Experience, Awareness and the Meaning of R/S Struggles
The narratives of the respondents show that their R/S struggle was first experienced in terms of negative feelings or a lack of positive feelings. Patients experienced anxiety, insecurity, loneliness, disappointment, meaninglessness, mistrust, sadness, despair, guilt, shame, anger, misunderstanding others or feeling misunderstood themselves. Feelings, on the one hand, were present towards others, including God, the devil or other persons. On the other hand, feelings also could be present towards themselves. A complicating factor for some was an experienced taboo on doubt or anger towards God. Regularly, a lack of positive feelings (such as peace, connectedness, joy and hope) was also a considerable part of the struggle. The previously mentioned female patient stated the following: “When you are depressed, the principle of hope possibly does not work”. Some patients mentioned a lack of support because they considered their faith not strong enough.
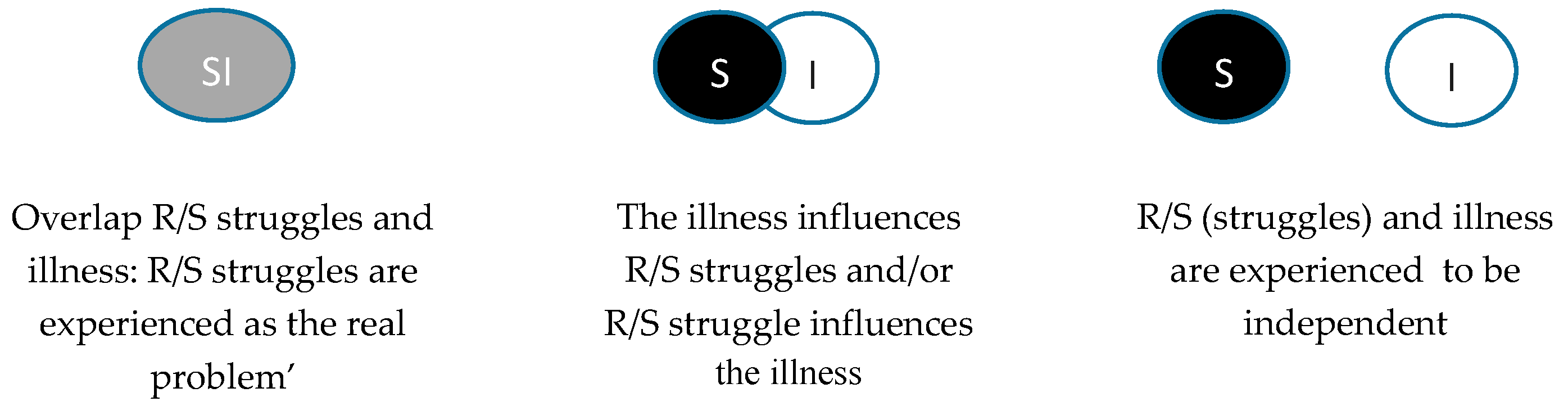
Patients’ views of the function of the R/S struggles differed, as shown in
Figure 1. Some patients had the opinion that R/S was their real problem. These patients experienced a complete overlap between illness and R/S, and some reported, either in the past or currently, that they do not consider themselves as ill. One patient reported the following: “You can try to separate things, but in my opinion […] faith is my problem” (CC1, woman orthodox reformed, 37, anxiety, psychotic and personality disorder, possibly autism). Others reported that their R/S was damaged or attacked by the illness, as shown by the following example: “When things would be going well I am faithful and give thanks. Now it is not going well, I really question where God is” (SC8, man, 40, orthodox reformed, dependent personality disorder, OCD, possibly autism) and “My dips make me leave my faith, I guess” (CC3, man (36), orthodox reformed, schizophrenia). A third category stated that R/S in their experience was separated from their illness. Some of these patients stated that R/S only supported them, shown by the following statement: “Precisely, when it is going so bad, then you attach the more to it [faith, JvNA]” (CC2, woman, 55, depression bipolar II disorder). Nevertheless, some of these patients still reported R/S struggles, for example with others.
Patients interpreted the situation in different ways. They experienced the illness as God punishing them, as special spiritual experiences, or most often as a type of suffering that belongs to human life. For many patients, both R/S support and R/S struggles were present, but those who experienced R/S struggles and hardly experienced any R/S support reported the most feelings of despair.
3.3. R/S Struggles Are Tightly Related to Someone’s R/S Background and Beliefs or Doubts
For all patients, their R/S struggles were related to their R/S background, R/S beliefs (and common functioning of faith) and possible R/S transformations in the past. The intensity in which patients suffered from R/S struggles varied and was often dependent on how important R/S was to them; the more importance, the more chance of struggles. Sometimes, these aspects clearly influenced their R/S struggles. Some participants were not educated with any kind of religion, but a few of them reported various spiritual beliefs and some became Christian. The majority of the interviewed patients (N = 26) had a more or less intense religious upbringing, varying from nominal Roman Catholicism or liberal Protestantism to Strict Calvinism. When faith was a holdfast for patients, they suffered more from losing their grip, as shown by the following statement: “Faith is the most important thing to me, and that is precisely the problem. So therefore I am so much off balance” (CC1, woman orthodox reformed, 37, anxiety, psychotic and personality disorder, possibly autism). When the experience of God’s presence, for example, was important to patients, during their depression, they suffered more from feelings of abandonment and loneliness with regard to their commonly experienced relation with God. Non-religious participants sometimes reported doubt, questions of meaning or interpersonal struggles, but the experienced intensity was different from that of religious participants.
Especially in the case of strict religious education, patients sometimes experienced troubles by what they described as a more ‘easy faith’. For example, one of the patients stated the following: “I have the feeling to be attacked by that” (CC9, woman 27, pietistic reformed, depression and borderline personality disorder). Some patients reported firm positive beliefs. Others switched between predominantly positive or negative beliefs, corresponding with their mood. The same woman quoted above said the following: “The one day I read the Bible it is just curses that reach me, and the other day it is comfort. When it is comforting it helps me a lot that day, but when I am feeling somewhat depressed I read the curses and that makes things even more heavy.” Some patients reported mainly doubts, which were far more problematic to one person than to the other. A part of the patients also mentioned troubles or disagreement with certain beliefs. Beliefs and doubts also regularly revealed a relation with the type of illness.
3.4. The Burden of Illness and Other Events Can Play a Main Role in Types and Levels of R/S Struggle
The illness itself was a ‘major’ event that often influenced the patient’s R/S and many of them reported R/S struggles as a result of their illness. The illness and its causes, for example, often led to questions (most often, ‘Why me?’ and ‘Where is/was God?’) or influenced their mood. Furthermore, it caused difficulties, for example in maintaining R/S rituals, keeping R/S commandments or trusting (non)religious people. One patient stated the following: “On the one hand, my vulnerable child so to say … I long very hard to belong to God. And on the other hand very much that punishing … questions about, struggles about for example honor your father and your mother, and you know I do not hate anyone, even not now, but to love your enemies … And you should do well and love one another, but I feel falling short … Because I cannot say I love my parents, I do care for them but I cannot say I love them, and that is something God demands” (CC7, woman (35), orthodox reformed, PTSD and dependent personality disorder). The timing of the trajectory and the prognosis also played a role in the presence of R/S struggles. During acute stages of disease, R/S struggles could be strongly experienced by the patients, but sometimes also resolved by, for example, medical treatment. Despair was more often present in cases of long-lasting problems with less hope of recovery. In addition, a difference appeared between the tendency of patients to experience R/S struggles more inside themselves (such as shame or guilt) or more towards God and others (such as anger or anxiety).
3.5. Model
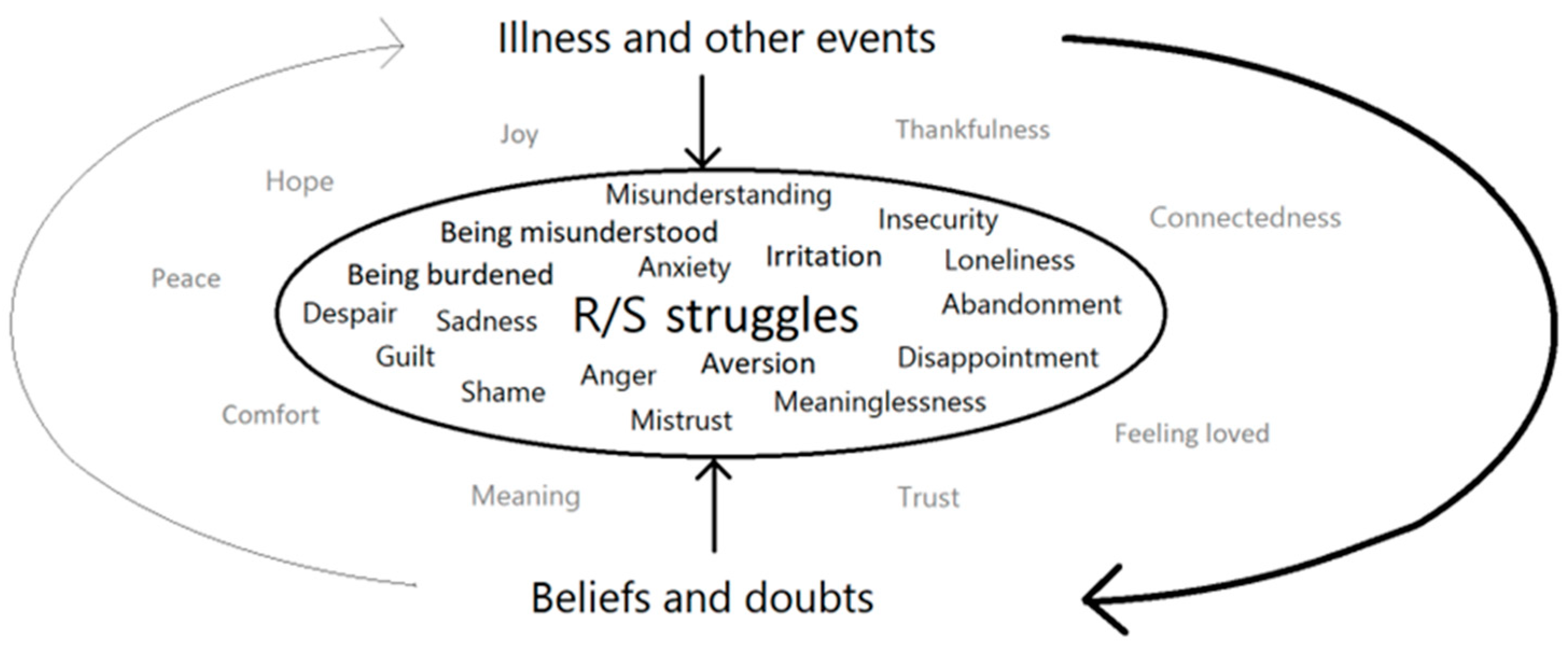
Based on the narratives, a model is proposed, as shown in
Figure 2. The inner circle illustrates that R/S struggles, at their core, are experienced by the presence of feelings such as abandonment, disappointment or anxiety and/or the absence of feelings such as thankfulness, joy and hope. The presence of ‘negative’ feelings and lack of ‘positive’ feelings is influenced by the illness and other events, either supporting or distressing, as well as by someone’s beliefs and doubts. The model illustrates that the illness could easily influence someone’s mood, and longer lasting complex problems with low treatment response and significant consequences could lead to despair. In addition, positive events could function as sources of support. Furthermore, specific beliefs (e.g., God is holy) or doubt (e.g., I do not know whether God exists) are not necessarily R/S struggles, but can easily lead to struggles, or affect the content of struggles, such as feelings of guilt or uncertainty, especially during hard times. In addition, the illness and other events influenced patients’ beliefs and doubts directly (thick arrow); the arrival of a friend, for example, could give someone the belief that God heard his/her prayer, whereas a lack of recovery could lead another patient to believe that God abandoned him/her. Finally, some patients also reported that beliefs and doubts influenced their illness (thin arrow); doubt about God’s existence, for instance, could enhance existential anxiety.
3.6. The Six Categories of Theory
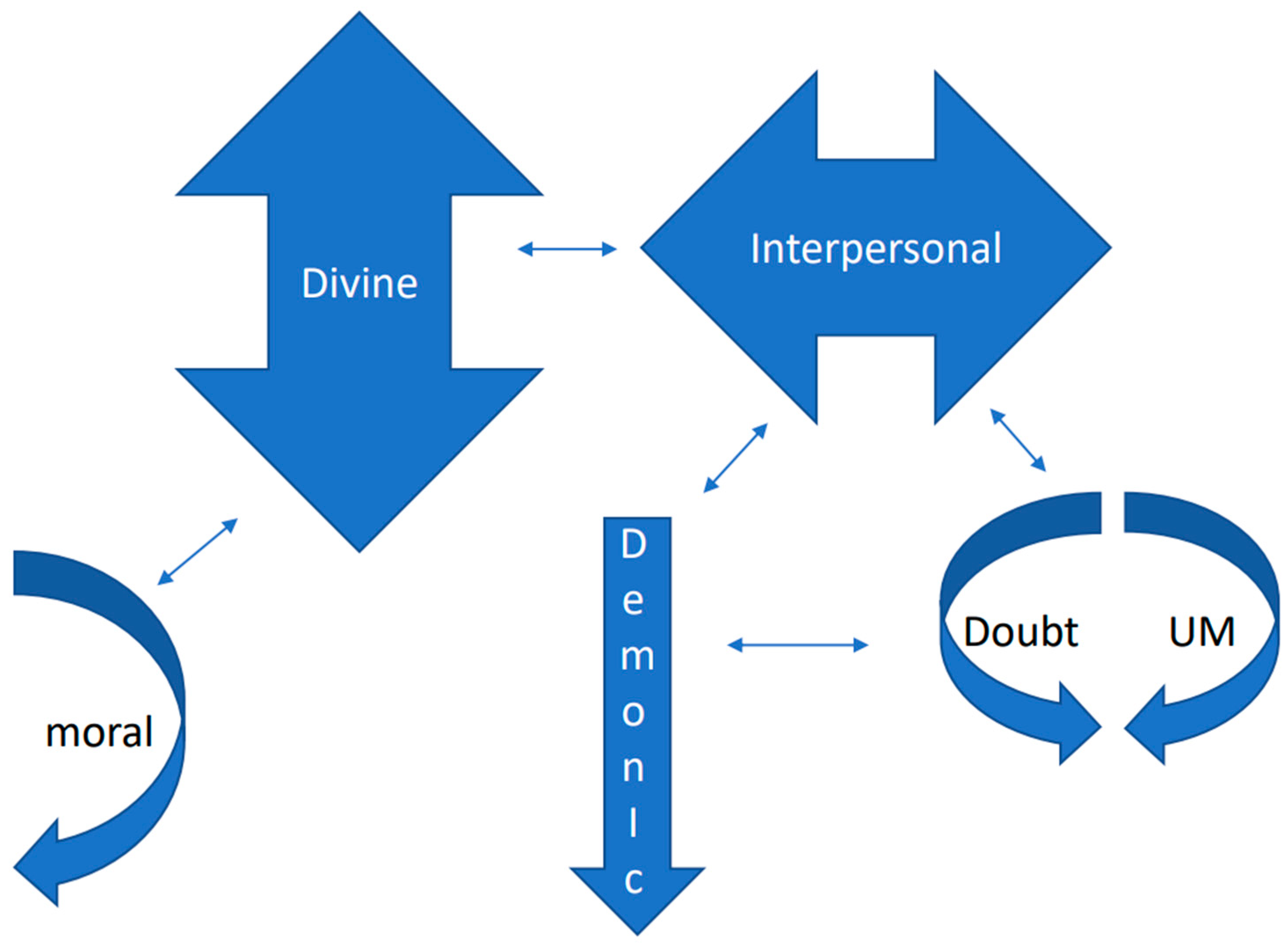
All types of R/S struggles as described in the theory were present in the interviews and many were interrelated, as shown in
Figure 3. Divine struggles were by far the most present and were always experienced as a real struggle, including a lack of understanding, anger, anxiety and fear, abandonment and mistrust. Regularly, the emphasis was not that God had left the patients, but that they had lost God. In addition, patients reported anguish for the future by feeling lost. The other five categories significantly varied in the intensity in which patients experienced them to be problematic. Interpersonal struggles were the second most present type of struggle, consisting of feelings of misunderstanding, shame, anger, disappointment, mistrust and insecurity. Moral struggles were present as the third most prevalent category, but they were often related to the divine; patients felt guilty about God, and sometimes also about interpersonal struggles (see quote CC7, woman (35) above). Demonic struggles were sometimes present. These struggles could either be interpreted as hallucinatory (in the past) or as a fight between good and bad, truth and falsehood. Finally, questions of doubt and ultimate meaning were present among a minority of the patients and, not frequently but sometimes, these were tormenting and led to feelings of despair.
3.7. R/S Struggles Can Be Approached in Three Ways
First, most of the patients that reported R/S struggles mentioned that they appreciate space to share their struggles, as a receptive approach of mental health professionals (1). To them, it was very helpful when a health professional was present and listened to their struggles without judging them. Sometimes, their struggles diminished to some extent. Furthermore, empathetic presence itself without sharing R/S struggles was experienced as helpful. In addition, patients felt relief when they could share negative emotions and heard from the mental health professionals that feelings of anger, for example (towards God or others), were not necessarily wrong. Patients did not need to share their struggles with many others, but sharing this information with a few health professionals that they trusted was important to many of them.
Second, many patients appreciated an active approach of mental health professionals (2). They appreciated mental health professionals asking further questions about their R/S struggles and deepening the conversation, providing some explanation or a little encouragement. Patients appreciated assistance in rituals by mental health professionals, especially when they were not able to fulfill them themselves, which regularly gave them feelings of guilt. In addition, they valued the stimulus to express their R/S struggles, or R/S support, for example in creative therapy, as demonstrated by the following statement: “The creative therapist initiated this. I said that it was an issue for me (R/S, JvNA) and he suggested to express this (…). That helped me to regain these feelings, the comfort of it” (SC11, woman (46), not affiliated, dependent personality disorder). The active approach was often valued because of the reticence of patients to share their struggles. Whether or not it helped was not certain beforehand. Encouraging patients too actively, for example, could have negative consequences, but it could also be appreciated. Generally, patients did not expect interventions such as answers or special advice.
Third, several respondents also mentioned the benefits of the more directive approach of mental health professionals towards R/S struggles (3). The benefits mentioned were as follows: R/S advice, with the professionals offering a different perspective and sometimes providing one’s own view on the situation. However, again, not all approaches were considered helpful. Sharing one’s own view sometimes was experienced negatively, especially when fighting with the patient’s beliefs, as demonstrated by the following statement: “I said something about faith and the nurse enhanced my feelings of guilt […]. I told that I felt guilty and that I should have made other choices […]. And he made all kind of remarks, yes if you had done this it would have been going differently, and God, well yes it is in the Bible like this and in the Bible like that and it is in the Bible like this … It all were separate verses because of which my feelings of guilt increased you know …” (CC 7, woman (35), orthodox reformed, PTSD and dependent personality disorder). The same patient, however, also shared their positive experiences from contact with her EMDR therapist, shown by the following statement: “In some way he fulfills a parental role […]. The way he reacts, and just how he explains that God didn’t want it this way and that God also judges what my brother did, and that it all should not have happened, that it is not my fault … [crying].” The quotes show that the act of mental health professionals sharing their own view can be very helpful for patients or even make the situation worse. Carefully offering an alternative perspective in an open way most of the time was received very well by patients. Giving advice in specific circumstances was sometimes experienced as helpful, but when provided without being asked or when it conflicted with the advice of others or with one’s own R/S, it was not perceived as helpful. Generally, patients appreciated an individual R/S sensitive approach and rejected a general approach or easy answers.
4. Discussion
Religious and spiritual (R/S) struggle narratives in a population of psychiatric inpatients are unique to the individual. The new insights of the current study do not so much extend the types and subtypes of R/S struggles as described by others (
Elliot and Reuter 2021;
Tabik et al. 2020;
Wilt et al. 2020;
Pargament and Exline 2021), but confirm them. However, our findings offer nuances and more detailed insight into how R/S struggles may develop and function in patients with mental illness. Additionally, the results argue that a three-step model might be helpful when addressing R/S struggles in mental health care.
Central to our findings is the proposed model, illustrating how R/S struggles are constructed by means of individual beliefs and (the related interpretation of) a variety of past and current events, such as the illness and its causes. Present or absent feelings have a central space in the model, and could be viewed as the core experience of R/S struggles, although R/S struggles should not be reduced to simply bad feelings. Speaking about ‘positive’ or ‘negative’ feelings, beliefs or experiences also should not be taken lightly. The patients themselves were relieved to hear that anger should not always be a ‘bad emotion’, and also anger towards others can be a sign of connectedness (
Karreman and Bekker 2012). In comparison with the results of a qualitative study by
Elliot and Reuter (
2021), both the ‘risky refuge’ and ‘abuse in religious settings’ categories should be gathered under ‘events’ that are likely to result in R/S struggles.
The model shows some comparisons with the ABC theory of Albert
Ellis (
1991). He states that external events influence someone’s beliefs and that beliefs influence someone’s emotions. One of the differences with our model is that in our model, specific events, such as the illness, could either directly or indirectly, via someone’s beliefs, influence R/S feelings. In addition, in our model, there is a suggestion that R/S beliefs can also influence illness (=event). The experiences of the patients in our results are in line with research that shows that R/S struggles can both precede or follow psychological problems (
Cowden et al. 2022;
Fox and Piedmont 2020), whereby in cases of R/S struggle, preceding illness patients often experienced total overlap. Overlap was present more often; R/S struggle and support often were simultaneously present, which is important to note when taking note of study results that describe positive religious and negative religious coping (
Phillips and Stein 2007;
Winter et al. 2009). Furthermore, various types of struggles could be experienced at the same time. A major activating event in our study for many patients might have been the illness, or its cause(s). Questions such as ‘why me?’ and ‘where is God?’ were often prevalent.
R/S struggle experiences were influenced by R/S beliefs. Although all people can experience various types of R/S struggles, patients to whom religion and spirituality are important are more likely to suffer from R/S, particularly in the context of mental health care. The religious background of people and the beliefs that are communicated within their community influence their God representations (
Schaap-Jonker et al. 2013). In the current study population, the R/S background of patients mattered with regard to their tendency either to feel, on the one hand, that they had acted in a wrong or unforgivable manner or, on the other hand, angry with God. In some strict churches, anger towards God is likely to be more taboo than in less strict denominations. The same strict churches have a higher emphasis on human guilt, which was visible in the interviews and has been described before (
Künkler et al. 2020). In turn, doubts were more present among patients with low R/S involvement, but mostly, this was not very problematic in these cases. Doubts among highly religious patients, however, were experienced as a type of torment, and are known to have a highly negative impact on mental health (
Galek et al. 2007).
Broadly speaking, the intensity of the R/S struggles was in line with the level of importance of R/S to patients, although this was not necessarily related to whether or not the patients were affiliated with religion. Some participants had specific R/S beliefs about the illness and its causes. Sometimes, patients viewed the illness, for example, as punishment or as a special spiritual experience. In other cases, they believed the illness to be a common form of suffering. They had different interpretations of the situation. The patients with ‘overlap’ experienced their illness itself as an R/S struggle (and sometimes, this was not experienced as a struggle but as an R/S experience). This is, for example, conceivable in cases of psychosis or mania (
Ouwehand et al. 2014). Others thought their R/S was being attacked by their illness. A third group experienced R/S and illness as unrelated. In their R/S beliefs, character and personality also seemed to matter (which is illustrated in the paragraph below).
The six categories of R/S struggles described by
Pargament and Exline (
2021) were recognized in the current study. Many individual differences, however, existed in the intensity and meaning of these different types of R/S struggles, as experienced by different patients. Generally, divine struggles seemed to be experienced most frequently and most intensely. Some nuances with respect to this category could also be distinguished. The ‘divine struggles measure’, as formulated by Exline and colleagues (2014), consists of five questions, regarding feelings that God had let someone down, angriness, abandonment, punishment and questioning God’s love. In the current study, some patients indeed reported feelings of abandonment or being punished, e.g., during depression. However, other patients with the same diagnosis had the idea that they themselves had lost God, and they themselves had abandoned God, leading to feelings of guilt. Therefore, the experience of divine struggles, including the language used, as well as the emphasis on feelings, differed between individuals. The same event (depression) can be accompanied by various interpretations/beliefs and lead to different feelings of R/S struggle. In the example above, it is likely that someone’s character, as well as R/S background and beliefs, influence the tendency either to externalize (God has abandoned me) or internalize (I have abandoned God). As shown, the experience of ‘guilt’ is very tightly related to divine struggles in the current population. Next to the six categories mentioned, our respondents also reported struggles with some teachings of religion (
Tabik et al. 2020), which could be understood as interpersonal R/S struggles. In addition, struggles with commitment/time were present (
Wilt et al. 2020), sometimes leading to feelings of guilt, being viewed as intrapersonal moral struggles. These findings illustrate the interrelations between the six different categories.
R/S struggles can be approached in three ways. The own perception of patients with respect to illness and R/S struggles matters in this regard. However, in all cases, patients benefit by having space to share or not to share their feelings, and not being judged.
Pargament and Exline (
2022, p. 155), in their book ‘Working with spiritual struggles’, recommend people to ‘Be present to spiritual struggles’, which is confirmed by the research participants in the current study. Normalizing and acceptance (or recognition) are valued, especially when shame and taboos play a role. This is in line with the theory of presence (
Baart 2001), stating that an essential part of care is to be near others, a fact that caregivers can sensibly fine-tune to the one who seeks help. Unconditional acceptance is one of the factors in establishing treatment alliance (
Rogers 1957).
In some cases, especially when R/S struggles are experienced as struggles, an active approach may be an incentive, for example, to rediscover R/S resources of support. One may question may be to what extent is it the task of mental health professionals in clinical care to actively address R/S struggles. It is, therefore, important to realize that sometimes, patients are more open to mental health professionals in comparison with spiritual caregivers, supposing that they will understand their problems better, or because shame does play a lesser role in that context. Patients’ relation to the sacred is one of the aspects of their life and ‘existential recovery’ is part of the total process of recovery. Referral to spiritual caregivers regularly could be appropriate, since they are educated for this purpose and can offer specialized care in the field of R/S. However, in many cases, other mental health care professionals might be the first professional to attempt to deal with a patient’s R/S struggles, and patients indicate that they prefer interaction with them about these matters, especially in clinical settings in which nurses are 24/7 available (
van Nieuw Amerongen-Meeuse et al. 2019). To take the third step and be directive may be a point of discussion. Mental health professionals are supposed not to proselytize (
Moreira-Almeida et al. 2016). At the same time, patients may prefer reciprocal contact and they appreciate self-disclosure in some cases. Stating that the values of the caregiver have no influence is not realistic (
Richards and Bergin 2005). Furthermore, several patients in our study mentioned examples in which a directive approach, without being too intrusive or imperative, helped them. Alternative perspectives may help people, in the same way that ‘rethinking’ can help. Possibly, this could help patients to (re)invent R/S as a source of support and experience the (past) R/S struggles as ways of personal growth.
4.1. Strengths and Limitations
The narrative analysis offers advantages, but also has its limitations. The interviews used were undertaken for the purpose of a study on R/S care needs, which might be considered both as a strength and limitation at the same time. The strength is that the interviewer will not have been direct concerning R/S struggles. A limitation is that the current subject was not explored in more depth. The patients that participated in the current study may not fully reflect the population, since patients who attach more importance to R/S may be more likely to participate in research such as this. Furthermore, many Christians participated in the current study and the number of unaffiliated patients was relatively low. Therefore, little can be said about the generalizability of our findings. In addition, the background of the researchers will always have an influence, was although we tried to minimize this by having a varied team of researchers. A limitation is that diagnosis seemed to also partly relate to the types of R/S struggles that were present, but it was not possible to work that out for the current study. Some diagnostic groups (e.g., bipolar I) were missing and overlap in classifications was highly present.
4.2. Implications and Recommendations
The current study offers some important findings for future research. It is worthwhile studying the course of R/S struggles over time. Additionally, it would be interesting and relevant to find out the best ways to approach different types of R/S struggles. Possibly, certain specific interventions, used as tools in clinical practice, can be developed and tested regarding their effect on reducing R/S struggles and enhancing positive R/S coping (
Hefti 2011;
Rosmarin et al. 2021). It is important to realize that in the current study, the perspective of patients at one moment in time was studied. Mental illness, recovery and the role of R/S are processes and the different methods of R/S coping can influence the patient’s level of R/S struggles, as well as the chance of treatment success (
Phillips and Stein 2007). Furthermore, the presence of various types of struggles and suitable approaches per diagnostic group could be worked out, and in addition, it could be worthwhile studying R/S struggles in physical illnesses.
Some implications for clinical practice are suggested. Mental health professionals are recommended to be aware of the fact that R/S struggles, for many patients, do not only the presence of ‘negative’, but also the absence of the ‘positive’, feelings and experiences. It is important to realize that R/S background and common functions of R/S highly matter to patients, but that the illness also has its specific influences. Not every R/S struggle is experienced as a struggle to a patient, possibly in line with the level of patients’ insight of their illness. Mental health professionals may realize that some types of R/S struggles may depend more on the type of illness than others. Some struggles diminish along with recovery, but others may remain for a long time. Generally, attention to R/S struggles by mental health professionals is desirable, not only because these struggles frequently appear alongside the illness, but also because disruptions in one’s sense of ultimate existential existence creates its own, unique source of emotional distress that is both profound and extensive, distorting patients’ sense of identity (
Fox and Piedmont 2020). R/S struggles, therefore, may not always diminish in line with recovery, and might benefit from specific attention, which could help in the prevention of mental illness.
In addition to enhanced awareness, it is recommended that mental health professionals are always receptive towards R/S struggles, frequently active and sometimes directive. They are recommended to examine whether R/S is important to patients and in what way patients (have) experience(d) R/S support. Especially in cases of long-lasting problems, patients may need R/S help, either from mental health professionals or spiritual caregivers. Attention to enhancing R/S support may be effective, but it is also important to pay attention to present R/S struggles. Some patients may need a listening ear, others benefit from a different perspective and others find it beneficial to search together to find the best help for their R/S struggles.
Generally, our results sustain the idea that mental health professionals are sufficiently aware of the substantial presence of individual R/S struggles among mental health care patients and commit themselves to the best approach. Training concerning how to pay attention to R/S care needs can be appropriate, as suggested by others (
Hefti 2011). Promoting people’s general sense of meaning in life, in which R/S for many plays a role, seems to have the potential to buffer the negative sequelae of R/S struggles (
Appel et al. 2020).

 ,
, 



{kind=link}
{kind=link}
{kind=link}