Profile of Patients with Novel Coronavirus Disease 2019 (COVID-19) in Osaka Prefecture, Japan: A Population-Based Descriptive Study

 , ,
, ,  , and
, and
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Settings
2.2. Official Data Collection of COVID-19 Cases in Osaka Prefecture
2.3. Statistical Analyses
3. Results
3.1. The Description of Features
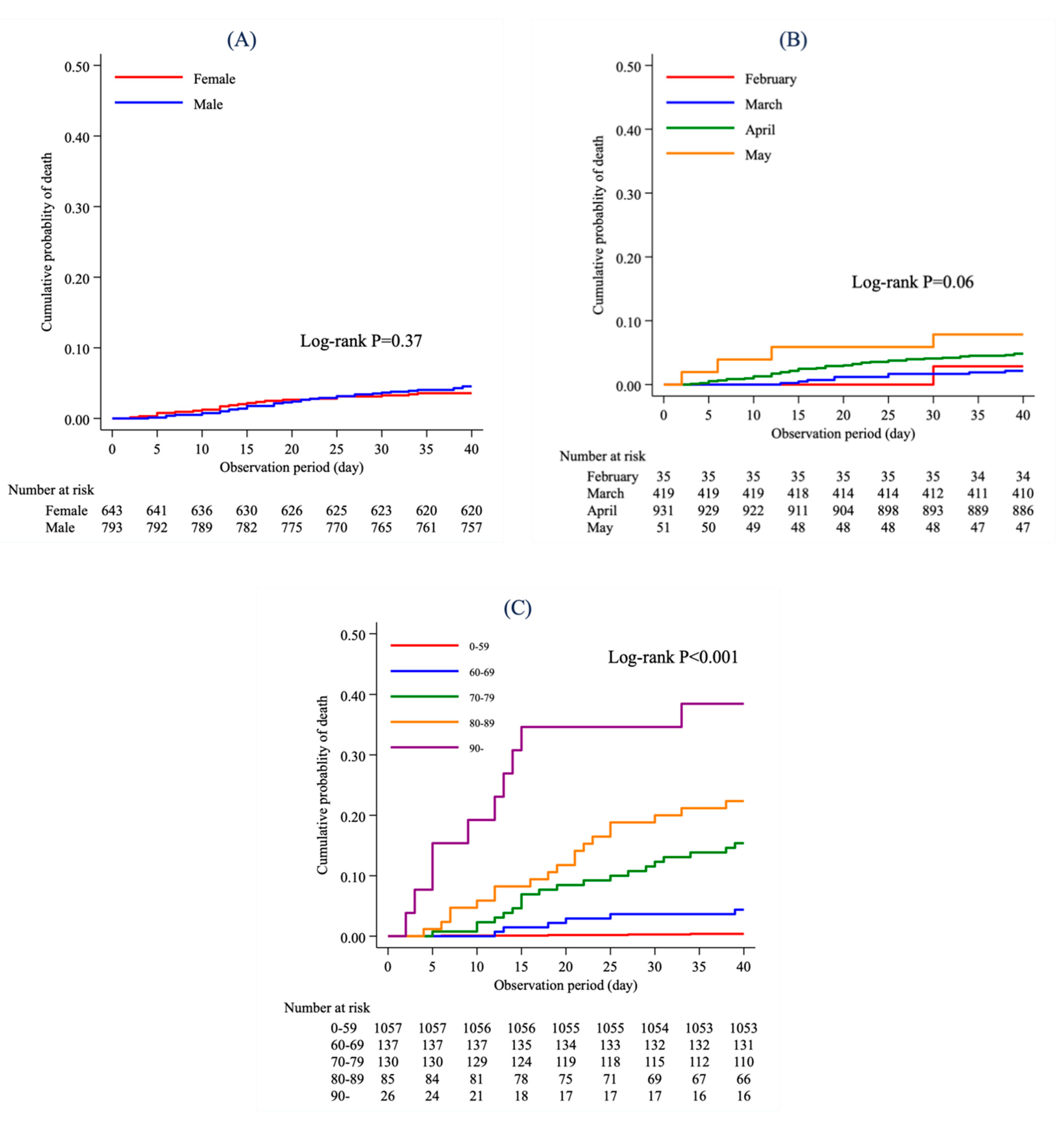
3.2. Mortality Analyses
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lai, C.; Wang, C.; Wang, Y.; Hsueh, S.; Ko, W.; Hsueh, P. Global Epidemiology of Coronavirus Disease 2019 (COVID-19): Disease Incidence, Daily Cumulative Index, Mortality, and Their Association with Country Healthcare Resources And Economic Status. Int. J. Antimicrob. Agents 2020, 55, 105946. [Google Scholar] [CrossRef] [PubMed]
- The Statistics of Patients with COVID-19. Available online: https://www.mhlw.go.jp/stf/seisakunitsuite/bunya/0000121431_00086.html (accessed on 16 July 2020).
- Huang, C.; Wang, Y.; Li, X.; Ren, L.; Zhao, J.; Hu, Y.; Zhang, L.; Fan, G.; Xu, J.; Gu, X.; et al. Clinical Features of Patients Infected with 2019 Novel Coronavirus in Wuhan, China. Lancet 2020, 395, 497–506. [Google Scholar] [CrossRef] [Green Version]
- Rodriguez-Morales, A.; Cardona-Ospina, J.; Gutiérrez-Ocampo, E.; Villamizar-Peña, R.; Holguin-Rivera, Y.; Escalera-Antezana, J.; Alvarado-Arnez, L.; Bonilla-Aldana, D.; Franco-Paredes, C.; Henao-Martinez, A.; et al. Clinical, Laboratory and Imaging Features of COVID-19: A Systematic Review and Meta-Analysis. Travel Med. Infect. Dis. 2020, 34, 101623. [Google Scholar] [CrossRef] [PubMed]
- The Press Releases and Documents about COVID-19 Patients. Available online: http://www.pref.osaka.lg.jp/iryo/osakakansensho/hodo.html (accessed on 2 July 2020).
- The Treatment Guidelines about COVID-19. Available online: https://www.mhlw.go.jp/content/000631552.pdf (accessed on 2 July 2020).
- The Countermeasures for COVID-19 Pandemic. Available online: http://www.pref.osaka.lg.jp/iryo/osakakansensho/corona.html (accessed on 2 July 2020).
- Gebhard, C.; Regitz-Zagrosek, V.; Neuhauser, H.; Morgan, R.; Klein, S. Impact of Sex and Gender on COVID-19 Outcomes in Europe. Biol. Sex Differ. 2020, 11, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Wang, M.; Zhang, J.; Ye, D.; Wang, Z.; Liu, J.; He, H.; Shen, B.; Luo, Z.; Ye, J.; Xu, Y.; et al. Time-Dependent Changes in the Clinical Characteristics and Prognosis of Hospitalized COVID-19 Patients in Wuhan, China: A Retrospective Study. Clin. Chim. Acta 2020, 510, 220–227. [Google Scholar] [CrossRef] [PubMed]
- Liang, W.; Liang, H.; Ou, L.; Chen, B.; Chen, A.; Li, C.; Li, Y.; Guan, W.; Sang, L.; Lu, J.; et al. Development and Validation of a Clinical Risk Score to Predict the Occurrence of Critical Illness in Hospitalized Patients with COVID-19. JAMA Intern. Med. 2020, 180, 1081–1089. [Google Scholar] [CrossRef] [PubMed]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical Course and Risk Factors for Mortality of Adult Inpatients with COVID-19 in Wuhan, China: A Retrospective Cohort Study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Cummings, M.; Baldwin, M.; Abrams, D.; Jacobson, S.; Meyer, B.; Balough, E.; Aaron, J.; Claassen, J.; Rabbani, L.; Hastie, J.; et al. Epidemiology, Clinical Course, and Outcomes of Critically Ill Adults with COVID-19 in New York City: A Prospective Cohort Study. Lancet 2020, 395, 1763–1770. [Google Scholar] [CrossRef]
- Imam, Z.; Odish, F.; Gill, I.; O’Connor, D.; Armstrong, J.; Vanood, A.; Ibironke, O.; Hanna, A.; Ranski, A.; Halalau, A. Older Age and Comorbidity Are Independent Mortality Predictors in a Large Cohort of 1305 COVID-19 Patients in Michigan, United States. J. Intern. Med. 2020. [Google Scholar] [CrossRef] [PubMed]
- Baqui, P.; Bica, I.; Marra, V.; Ercole, A.; van der Schaar, M. Ethnic and Regional Variations in Hospital Mortality from COVID-19 in Brazil: A Cross-Sectional Observational Study. Lancet Glob. Health 2020, 8, e1018–e1026. [Google Scholar] [CrossRef]
- Li, L.; Huang, T.; Wang, Y.; Wang, Z.; Liang, Y.; Huang, T.; Zhang, H.; Sun, W.; Wang, Y. COVID-19 Patients’ Clinical Characteristics, Discharge Rate, and Fatality Rate of Meta-Analysis. J. Med. Virol. 2020, 92, 577–583. [Google Scholar] [CrossRef] [PubMed]
- Suleyman, G.; Fadel, R.; Malette, K.; Hammond, C.; Abdulla, H.; Entz, A.; Demertzis, Z.; Hanna, Z.; Failla, A.; Dagher, C.; et al. Clinical Characteristics and Morbidity Associated with Coronavirus Disease 2019 in a Series of Patients in Metropolitan Detroit. JAMA Netw. Open 2020, 3, e2012270. [Google Scholar] [CrossRef] [PubMed]
- Götzinger, F.; Santiago-García, B.; Noguera-Julián, A.; Lanaspa, M.; Lancella, L.; Calò Carducci, F.; Gabrovska, N.; Velizarova, S.; Prunk, P.; Osterman, V.; et al. COVID-19 in Children and Adolescents in Europe: A Multinational, Multicentre Cohort Study. Lancet Child. Adolesc. Health 2020, 4, 653–661. [Google Scholar] [CrossRef]
- Wang, L.; He, W.; Yu, X.; Hu, D.; Bao, M.; Liu, H.; Zhou, J.; Jiang, H. Coronavirus Disease 2019 in Elderly Patients: Characteristics and Prognostic Factors Based on 4-Week Follow-Up. J. Infect. 2020, 80, 639–645. [Google Scholar] [CrossRef] [PubMed]
- To, K.; Tsang, O.; Leung, W.; Tam, A.; Wu, T.; Lung, D.; Yip, C.; Cai, J.; Chan, J.; Chik, T.; et al. Temporal Profiles of Viral Load in Posterior Oropharyngeal Saliva Samples and Serum Antibody Responses during Infection by SARS-Cov-2: An Observational Cohort Study. Lancet Infect. Dis. 2020, 20, 565–574. [Google Scholar] [CrossRef] [Green Version]
- Opal, S.; Girard, T.; Ely, E. The Immunopathogenesis of Sepsis in Elderly Patients. Clin. Infect. Dis. 2005, 41 (Suppl. 7), S504–S512. [Google Scholar] [CrossRef] [Green Version]


{kind=link}
| Total | Features | ||||||||||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Fever | Cough | Headache | Sore Throat | General Malaise | Mucus/ Nasal obstruction/ Sneeze | Low Back Pain | Arthralgia | Diarrhea | Shortness of Breath | Pneumonia | |||||||||||||
| Total, n (%) | 244 | 187 | (76.6) | 108 | (44.3) | 6 | (2.5) | 29 | (11.9) | 65 | (26.6) | 32 | (13.1) | 1 | (0.4) | 1 | (0.4) | 2 | (0.8) | 19 | (7.8) | 87 | (35.7) |
| Age group, n (%) | |||||||||||||||||||||||
| 0–9 | 4 | 1 | (25.0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 2 | (50.0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) |
| 10–19 | 3 | 1 | (33.3) | 1 | (33.3) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) |
| 20–29 | 47 | 35 | (74.5) | 24 | (51.1) | 1 | (2.1) | 8 | (17.0) | 14 | (29.8) | 11 | (23.4) | 0 | (0) | 0 | (0) | 0 | (0) | 3 | (6.4) | 13 | (27.7) |
| 30–39 | 38 | 22 | (57.9) | 13 | (34.2) | 1 | (2.6) | 2 | (5.3) | 7 | (18.4) | 6 | (15.8) | 0 | (0) | 0 | (0) | 0 | (0) | 2 | (5.3) | 11 | (29.0) |
| 40–49 | 63 | 52 | (82.5) | 34 | (54.0) | 2 | (3.2) | 10 | (15.9) | 13 | (20.6) | 6 | (9.5) | 1 | (1.6) | 0 | (0) | 0 | (0) | 4 | (6.4) | 24 | (38.1) |
| 50–59 | 39 | 30 | (76.9) | 18 | (46.2) | 1 | (2.6) | 6 | (15.4) | 15 | (38.5) | 4 | (10.3) | 0 | (0) | 1 | (2.6) | 1 | (2.6) | 4 | (10.3) | 14 | (35.9) |
| 60–69 | 26 | 23 | (88.5) | 10 | (38.5) | 1 | (3.9) | 2 | (7.7) | 9 | (34.6) | 1 | (3.9) | 0 | (0) | 0 | (0) | 0 | (0) | 2 | (7.7) | 12 | (46.2) |
| 70–79 | 18 | 17 | (94.4) | 4 | (22.2) | 0 | (0) | 1 | (5.6) | 5 | (27.8) | 2 | (11.1) | 0 | (0) | 0 | (0) | 1 | (5.6) | 1 | (5.6) | 7 | (38.9) |
| ≥80 | 6 | 6 | (100.0) | 4 | (66.7) | 0 | (0) | 0 | (0) | 2 | (33.3) | 0 | (0) | 0 | (0) | 0 | (0) | 0 | (0) | 3 | (50.0) | 6 | (100.0) |
| Gender, n (%) | |||||||||||||||||||||||
| Male | 125 | 102 | (81.6) | 60 | (48.0) | 4 | (3.2) | 10 | (8.0) | 33 | (26.4) | 10 | (8.0) | 0 | (0) | 1 | (0.8) | 2 | (1.6) | 10 | (8.0) | 55 | (44.0) |
| Female | 119 | 85 | (71.4) | 48 | (40.3) | 2 | (1.7) | 19 | (16.0) | 32 | (26.9) | 22 | (18.5) | 1 | (0.8) | 0 | (0) | 0 | (0) | 9 | (7.6) | 32 | (26.9) |
| Onset Month | ||||||
|---|---|---|---|---|---|---|
| February | March | April | May | Unknown | ||
| Age at Onset | 0–59 | 27 (77.1) | 345 (82.3) | 655 (70.4) | 30 (57.7) | 236 (68.4) |
| 60–69 | 6 (17.1) | 28 (6.7) | 97 (10.4) | 6 (11.5) | 24 (7.0) | |
| 70–79 | 2 (5.7) | 29 (6.9) | 94 (10.1) | 5 (9.6) | 46 (13.3) | |
| 80–89 | 0 (0.0) | 17 (4.1) | 60 (6.4) | 8 (15.4) | 33 (9.6) | |
| ≥90 | 0 (0.0) | 0 (0.0) | 24 (2.6) | 3 (5.8) | 6 (1.7) | |
| Unknown | 0 (0.0) | 0 (0.0) | 1 (0.1) | 0 (0.0) | 0 (0.0) | |
| Total | 35 | 419 | 931 | 52 | 345 | |
| Male (N = 977) | Female (N = 805) | |||||
|---|---|---|---|---|---|---|
| Number of Patients | Number of Deaths | Percentage of Death | Number of Patients | Number of Deaths | Percentage of Death | |
| Age at onset | ||||||
| 0–59 | 701 | 5 | 0.7 | 592 | 0 | 0.0 |
| 60–69 | 90 | 8 | 8.9 | 71 | 1 | 1.4 |
| 70–79 | 108 | 21 | 19.4 | 68 | 9 | 13.2 |
| 80–89 | 71 | 19 | 26.8 | 47 | 12 | 25.5 |
| ≥90 | 7 | 0 | 0.0 | 26 | 11 | 42.3 |
| Unknown | 0 | 0 | 1 | 0 | 0.0 | |
| Onset month | ||||||
| February | 14 | 1 | 7.1 | 21 | 0 | 0.0 |
| March | 256 | 7 | 2.7 | 163 | 4 | 2.5 |
| April | 502 | 31 | 6.2 | 429 | 19 | 4.4 |
| May | 21 | 2 | 9.5 | 31 | 3 | 9.7 |
| Unknown | 184 | 12 | 6.5 | 161 | 7 | 4.3 |
| Number of Patients | Number of Deaths | HR (95% CI) | |
|---|---|---|---|
| Sex | |||
| Female | 643 | 23 | Ref |
| Male | 793 | 36 | 1.69 (0.95–3.02) |
| Onset month | |||
| February | 35 | 1 | 2.06 (0.21–20.00) |
| March | 419 | 9 | 1.03 (0.29–3.59) |
| April | 931 | 45 | 1.15 (0.39–3.39) |
| May | 51 | 4 | Ref |
| Age group at onset | |||
| 0–59 | 1057 | 4 | Ref |
| 60–69 | 137 | 6 | 12.02 (3.37–42.93) |
| 70–79 | 130 | 20 | 44.62 (15.16–131.30) |
| 80–89 | 85 | 19 | 68.38 (22.93–203.89) |
| ≥90 | 26 | 10 | 144.71 (42.55–492.15) |
| Unknown | 1 | 0 | Unconverged |
| Residence | |||
| Other cities | 793 | 26 | Ref |
| Osaka City | 604 | 27 | 1.76 (1.02–3.04) |
| Unknown | 39 | 6 | 3.73 (1.33–10.45) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takeuchi, T.; Imanaka, T.; Katayama, Y.; Kitamura, T.; Sobue, T.; Shimazu, T. Profile of Patients with Novel Coronavirus Disease 2019 (COVID-19) in Osaka Prefecture, Japan: A Population-Based Descriptive Study. J. Clin. Med. 2020, 9, 2925. https://doi.org/10.3390/jcm9092925
Takeuchi T, Imanaka T, Katayama Y, Kitamura T, Sobue T, Shimazu T. Profile of Patients with Novel Coronavirus Disease 2019 (COVID-19) in Osaka Prefecture, Japan: A Population-Based Descriptive Study. Journal of Clinical Medicine. 2020; 9(9):2925. https://doi.org/10.3390/jcm9092925
Chicago/Turabian StyleTakeuchi, Taro, Tomoka Imanaka, Yusuke Katayama, Tetsuhisa Kitamura, Tomotaka Sobue, and Takeshi Shimazu. 2020. "Profile of Patients with Novel Coronavirus Disease 2019 (COVID-19) in Osaka Prefecture, Japan: A Population-Based Descriptive Study" Journal of Clinical Medicine 9, no. 9: 2925. https://doi.org/10.3390/jcm9092925