Twelve Weeks of Strengthening Exercise for Patients with Rheumatoid Arthritis: A Prospective Intervention Study

 , , and
, , and
Abstract
:1. Introduction
2. Material and Methods
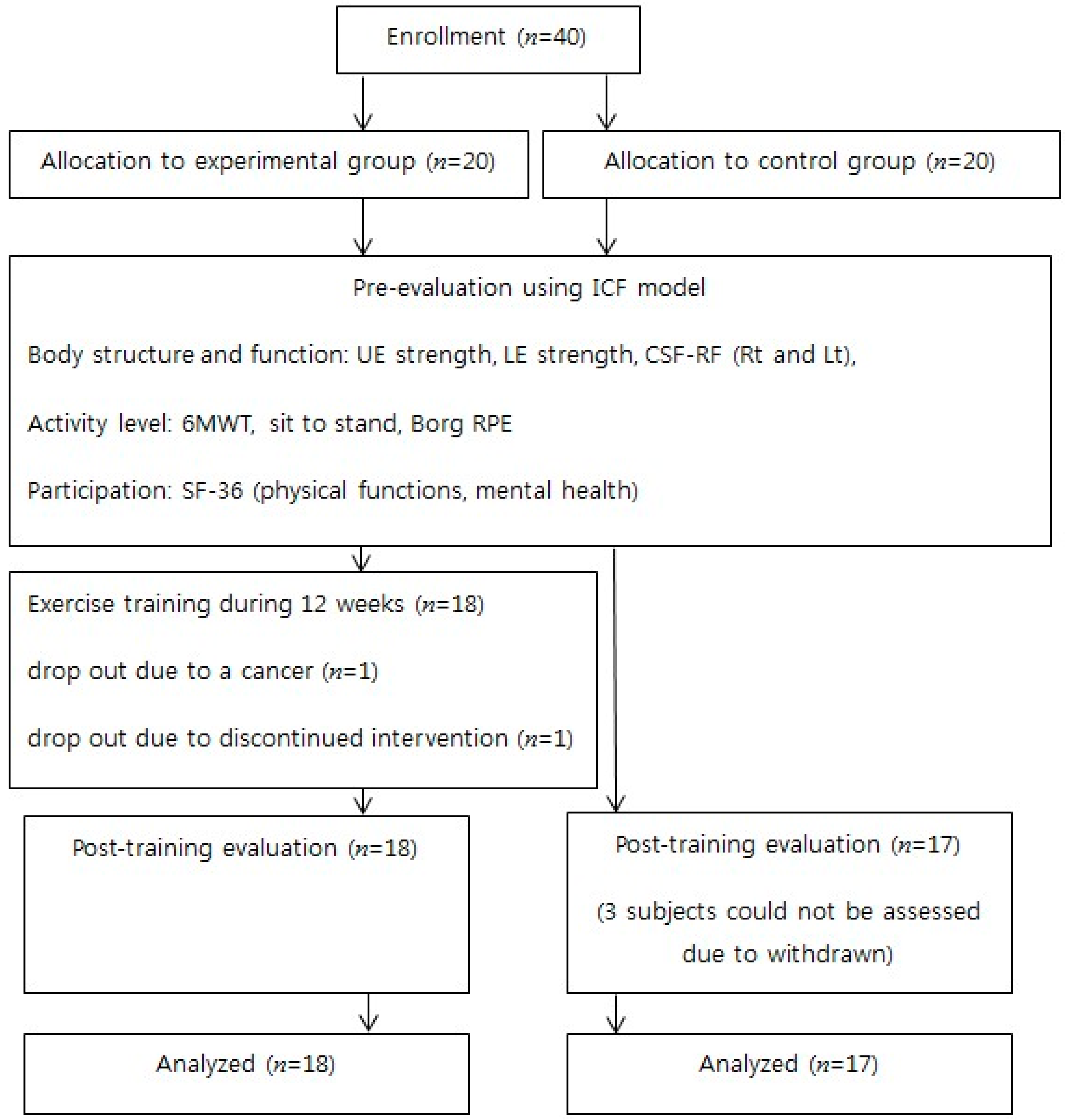
2.1. Participants
2.2. Exercise Program
2.3. Assessments
2.3.1. Body Structure and Function
2.3.2. Activity
2.3.3. Social Participation and Quality of Life
2.4. Statistical Analyses
3. Results
3.1. Baseline Characteristics and Clinical Data
3.2. Post-Training Change
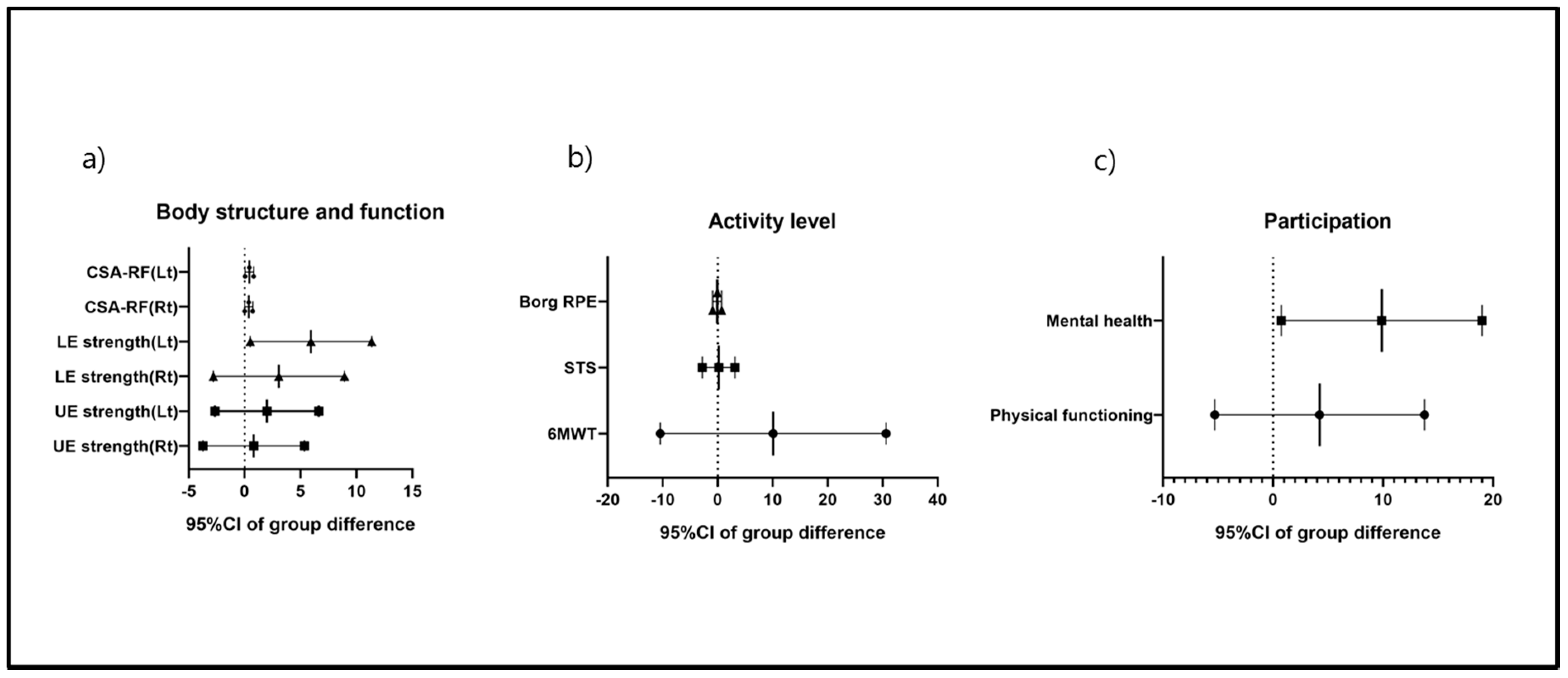
3.2.1. Body Structure and Function
3.2.2. Activity Levels
3.2.3. Participation
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
Abbreviations
| RA | Rheumatoid arthritis |
| CSA-RF | The cross-sectional area of the rectus femoris |
| 6MWT | 6 min walk test |
| SF-36 | 36-Item Short Form Health Survey |
References
- Metsios, G.S.; Stavropoulos-Kalinoglou, A.; Kitas, G.D. The role of exercise in the management of rheumatoid arthritis. Expert Rev. Clin. Immunol. 2015, 11, 1121–1130. [Google Scholar] [CrossRef] [PubMed]
- Stavropoulos-Kalinoglou, A.; Metsios, G.S.; van Zanten, J.J.V.; Nightingale, P.; Kitas, G.D.; Koutedakis, Y. Individualised aerobic and resistance exercise training improves cardiorespiratory fitness and reduces cardiovascular risk in patients with rheumatoid arthritis. Ann. Rheum. Dis. 2013, 72, 1819–1825. [Google Scholar] [CrossRef] [PubMed]
- Williams, M.A.; Williamson, E.M.; Heine, P.J.; Nichols, V.; Glover, M.J.; Dritsaki, M.; Adams, J.; Dosanjh, S.; Underwood, M.; Rahman, A.; et al. Strengthening And stretching for Rheumatoid Arthritis of the Hand (SARAH). A randomised controlled trial and economic evaluation. Health Technol. Assess. 2015, 19, 1–222. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Jong, Z.; Munneke, M.; Zwinderman, A.H.; Kroon, H.M.; Jansen, A.; Ronday, K.H.; van Schaardenburg, D.; Dijkmans, B.A.; Van den Ende, C.H.; Breedveld, F.C.; et al. Is a long-term high-intensity exercise program effective and safe in patients with rheumatoid arthritis? Results of a randomized controlled trial. Arthritis Rheum. 2003, 48, 2415–2424. [Google Scholar] [CrossRef] [Green Version]
- Hurkmans, E.J.; van den Berg, M.H.; Ronday, K.H.; Peeters, A.J.; le Cessie, S.; Vlieland, T.P. Maintenance of physical activity after Internet-based physical activity interventions in patients with rheumatoid arthritis. Rheumatology 2010, 49, 167–172. [Google Scholar] [CrossRef] [Green Version]
- van den Berg, M.H.; Ronday, H.K.; Peeters, A.J.; le Cessie, S.; van der Giesen, F.J.; Breedveld, F.C.; Vliet Vlieland, T.P. Using internet technology to deliver a home-based physical activity intervention for patients with rheumatoid arthritis: A randomized controlled trial. Arthritis Rheum. 2006, 55, 935–945. [Google Scholar] [CrossRef]
- Verhoeven, F.; Tordi, N.; Prati, C.; Demougeot, C.; Mougin, F.; Wendling, D. Physical activity in patients with rheumatoid arthritis. Jt. Bone Spine 2016, 83, 265–270. [Google Scholar] [CrossRef]
- van Gestel, A.M.; Haagsma, C.J.; van Riel, P.L. Validation of rheumatoid arthritis improvement criteria that include simplified joint counts. Arthritis Rheum. 1998, 41, 1845–1850. [Google Scholar] [CrossRef]
- Nelson, M.E.; Rejeski, W.J.; Blair, S.N.; Duncan, P.W.; Judge, J.O.; King, A.C.; Macera, C.A.; Castaneda-Sceppa, C. Physical activity and public health in older adults: Recommendation from the American College of Sports Medicine and the American Heart Association. Med. Sci. Sports Exerc. 2007, 39, 1435–1445. [Google Scholar] [CrossRef] [Green Version]
- Page, P.; Ellenbecker, T.S. Strength Band Training; Human Kinetics: Champaign, IL, USA, 2011. [Google Scholar]
- Andrews, A.W.; Thomas, M.W.; Bohannon, R.W. Normative values for isometric muscle force measurements obtained with hand-held dynamometers. Phys. Ther. 1996, 76, 248–259. [Google Scholar] [CrossRef] [Green Version]
- Hammond, K.; Mampilly, J.; Laghi, F.A.; Goyal, A.; Collins, E.G.; McBurney, C.; Jubran, A.; Tobin, M.J. Validity and reliability of rectus femoris ultrasound measurements: Comparison of curved-array and linear-array transducers. J. Rehabil. Res. Dev. 2014, 51, 1155–1164. [Google Scholar] [CrossRef] [PubMed]
- Vlietstra, L.; Stebbings, S.; Meredith-Jones, K.; Abbott, J.H.; Treharne, G.J.; Waters, D.L. Sarcopenia in osteoarthritis and rheumatoid arthritis: The association with self-reported fatigue, physical function and obesity. PLoS ONE 2019, 14, e0217462. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, K.B.; Lim, S.H.; Ko, E.H.; Kim, Y.S.; Lee, K.S.; Hwang, B.Y. Factors related to community ambulation in patients with chronic stroke. Top. Stroke Rehabil. 2015, 22, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Morishita, S.; Tsubaki, A.; Nakamura, M.; Nashimoto, S.; Fu, J.B.; Onishi, H. Rating of perceived exertion on resistance training in elderly subjects. Expert Rev. Cardiovasc. Ther. 2019, 17, 135–142. [Google Scholar] [CrossRef]
- Koh, S.B.; Chang, S.J.; Kang, M.G.; Cha, B.S.; Park, J.K. Reliability and Validity on Measurement Instrument for Health Status Assessment in Occupational Workers. Korean J. Prev. Med. 1997, 30, 251–266. [Google Scholar]
- Ware, J.E.; Snow, K.K.; Kosinski, M.; Gandek, B.; Institute NEMCHH. SF-36 Health Survey: Manual and Interpretation Guide; The Health Institute, New England Medical Center: Boston, MA, USA, 1993. [Google Scholar]
- Ware, J.E., Jr.; Sherbourne, C.D. The MOS 36-item short-form health survey (SF-36). I. Conceptual framework and item selection. Med. Care 1992, 30, 473–483. [Google Scholar] [CrossRef]
- Pereira Nunes Pinto, A.C.; Natour, J.; de Moura Castro, C.H.; Eloi, M.; Lombardi Junior, I. Acute effect of a resistance exercise session on markers of cartilage breakdown and inflammation in women with rheumatoid arthritis. Int. J. Rheum. Dis. 2017, 20, 1704–1713. [Google Scholar] [CrossRef]
- Hurkmans, E.; van der Giesen, F.J.; Vliet Vlieland, T.P.; Schoones, J.; Van den Ende, E.C. Dynamic exercise programs (aerobic capacity and/or muscle strength training) in patients with rheumatoid arthritis. Cochrane Database Syst. Rev. 2009, CD006853. [Google Scholar] [CrossRef]
- Kofotolis, N.; Kellis, E.; Vlachopoulos, S.P.; Gouitas, I.; Theodorakis, Y. Effects of Pilates and trunk strengthening exercises on health-related quality of life in women with chronic low back pain. J. Back Musculoskelet. Rehabil. 2016, 29, 649–659. [Google Scholar] [CrossRef]
- Kumar, T.; Kumar, S.; Nezamuddin, M.; Sharma, V.P. Efficacy of core muscle strengthening exercise in chronic low back pain patients. J. Back Musculoskelet. Rehabil. 2015, 28, 699–707. [Google Scholar] [CrossRef]
- Iversen, M.D.; Brandenstein, J.S. Do dynamic strengthening and aerobic capacity exercises reduce pain and improve functional outcomes and strength in people with established rheumatoid arthritis? Phys. Ther. 2012, 92, 1251–1257. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, T.; Pope, J. Cervical spine involvement in rheumatoid arthritis over time: Results from a meta-analysis. Arthritis Res. Ther. 2015, 17, 148. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baek, I.W.; Joo, Y.B.; Park, K.S.; Kim, K.J. Risk factors for cervical spine instability in patients with rheumatoid arthritis. Clin. Rheumatol. 2020. [Google Scholar] [CrossRef] [PubMed]
- Hakkinen, A.; Makinen, H.; Ylinen, J.; Hannonen, P.; Sokka, T.; Neva, M.; Kautiainen, H.; Kauppi, M. Stability of the upper neck during isometric neck exercises in rheumatoid arthritis patients with atlantoaxial disorders. Scand. J. Rheumatol. 2008, 37, 343–347. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| Warm-Up Stretch Exercises | Shoulder and deltoid stretches | Duration and intensity |
| Biceps and wrist flexor stretches | 2 repeats, 15 min | |
| Quadriceps stretch | ||
| Hamstring and low back stretches | ||
| Groin stretch | ||
| Calf stretch | ||
| Upper back stretch | ||
| Neck flexor stretch | ||
| Neck rotator stretch | ||
| Resistive Band Exercises | Resistance band squats | 15 repeats, 3 sets, 45 min; |
| Resistance band bent-over rowing | rest of 2 min between exercises | |
| Standing alternate chest presses | ||
| Diagonal woodchops | ||
| Triceps extension with resistance band | ||
| Resistance band lunges | ||
| Lateral rowing with resistance band | ||
| Biceps curls with resistance band |
| Outcomes | EG (n = 18) Mean (SD)/Median (IQR) | CG (n = 17) Mean (SD)/Median (IQR) | p-Value |
|---|---|---|---|
| Height (cm) | 158.3 (4.7) | 0.853 | |
| 158.1 (4.7) | 158.4 (4.8) | ||
| Age (years) | 50.4 (7.9) | 0.015 * | |
| 53.6 (5.2) | 47.1 (9.0) | ||
| Weight (kg) | 59.8 (9.3) | 0.898 | |
| 60 (9.2) | 59.59 (9.7) | ||
| BMI (kg/m2) | 24.0 (3.6) | 0.879 | |
| 24.1 (3.8) | 23.9 (3.6) | ||
| Disease duration (years) | 5.6 (7.0) | 0.987 | |
| 5.3 (6.9) | 6.0 (7.3) | ||
| Body function and structure | |||
| UE strength (Rt) | 43.4 (12.4) | 51.0 (8.6) | 0.046 * |
| UE strength (Lt) | 44.4 (8.9) | 47.2 (8.9) | −0.366 |
| LE strength (Rt) | 55.1 (7.2) | 54.4 (6.5) | 0.768 |
| LE strength (Lt) | 54.3 (6.4) | 53.0 (5.6) | 0.508 |
| CSA-RF (Rt) | 1.0 (0.3) | 1.4 (0.8) | 0.043 * |
| CSA-RF (Lt) | 0.9 (0.2) | 1.4 (0.8) | 0.025 * |
| Activity level | |||
| 6MWT | 508.6 (48.5) | 494.7 (49.9) | 0.407 |
| STS | 15.5 (14.8:19.3) | 15.0 (14.0:18.0) | 0.499 |
| Borg | 2.0 (1.8:3.0) | 2.0 (1.5:3.0) | 0.884 |
| Participation | |||
| Physical function | 71.4 (12.5) | 72.7 (17.0) | 0.803 |
| Mental health | 53.9 (9.8) | 58.6 (6.8) | 0.111 |
| Outcomes | EG (n = 18) Mean Change (95%CI) | CG (n = 17) Mean Change (95%CI) | Group Difference Mean Change (95%CI) | p-Value |
|---|---|---|---|---|
| Body function and structure | ||||
| UE strength (Rt) | 1.2 (−1.8:4.0) | 0.3 (−2.7:3.3) | 0.8 (−3.7:5.3) | 0.716 |
| UE strength (Lt) | 2.4 (−0.6:5.4) | 0.4 (−2.7:3.5) | 2.0 (−2.7:6.6) | 0.389 |
| LE strength (Rt) | 6.0 (2.3:9.8) † | 3.0 (−0.9:6.8) | 3.1 (−2.8:8.9) | 0.295 |
| LE strength (Lt) | 6.6 (3.1:10.1) † | 0.7 (−2.9:4.3) | 5.9 (0.5:11.4) | 0.033 * |
| CSA-RF(Rt) | 0.4 (0.2:0.6) † | 0.03 (−0.2:0.3) | 0.4 (0.01:0.7) | 0.044 * |
| CSA-RF(Lt) | 0.6 (0.4:0.9) † | 0.2 (−0.1:0.4) | 0.4 (0.04:0.8) | 0.033 * |
| Activity level | ||||
| 6MWT | 30.3 (17.2:43.4) † | 20.2 (6.7:33.8) † | 10.1 (−10.4:30.6) | 0.323 |
| Sit-to-stand | 3.5 (1.6:5.4) † | 3.3 (1.3:5.3) † | 0.2 (−2.8:3.2) | 0.903 |
| Borg scale | −0.2 (−0.7:0.4) | −0.1 (−0.6:0.5) | −0.1 (−0.9:0.7) | 0.809 |
| Participation | ||||
| Physical function | 10.1 (4.0:16.2) † | 5.8 (−0.5:12.1) | 4.2 (−5.3:13.8) | 0.371 |
| Mental health | 10.9 (5.1:16.8) † | 1.0 (−5.0:7.1) | 9.9 (0.8:19.0) | 0.035 * |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sul, B.; Lee, K.B.; Joo, Y.B.; Hong, B.Y.; Kim, J.-S.; Kim, K.-J.; Park, K.-S.; Park, Y.-J.; Lim, S.H. Twelve Weeks of Strengthening Exercise for Patients with Rheumatoid Arthritis: A Prospective Intervention Study. J. Clin. Med. 2020, 9, 2792. https://doi.org/10.3390/jcm9092792
Sul B, Lee KB, Joo YB, Hong BY, Kim J-S, Kim K-J, Park K-S, Park Y-J, Lim SH. Twelve Weeks of Strengthening Exercise for Patients with Rheumatoid Arthritis: A Prospective Intervention Study. Journal of Clinical Medicine. 2020; 9(9):2792. https://doi.org/10.3390/jcm9092792
Chicago/Turabian StyleSul, Bomi, Kyoung Bo Lee, Young Bin Joo, Bo Young Hong, Joon-Sung Kim, Ki-Jo Kim, Kyung-Su Park, Yune-Jung Park, and Seong Hoon Lim. 2020. "Twelve Weeks of Strengthening Exercise for Patients with Rheumatoid Arthritis: A Prospective Intervention Study" Journal of Clinical Medicine 9, no. 9: 2792. https://doi.org/10.3390/jcm9092792