Optimal Antithrombotic Treatment of Patients with Atrial Fibrillation Early after an Acute Coronary Syndrome—Triple Therapy, Dual Antithrombotic Therapy with an Anticoagulant… Or, Rather, Temporary Dual Antiplatelet Therapy?



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
:1. Introduction
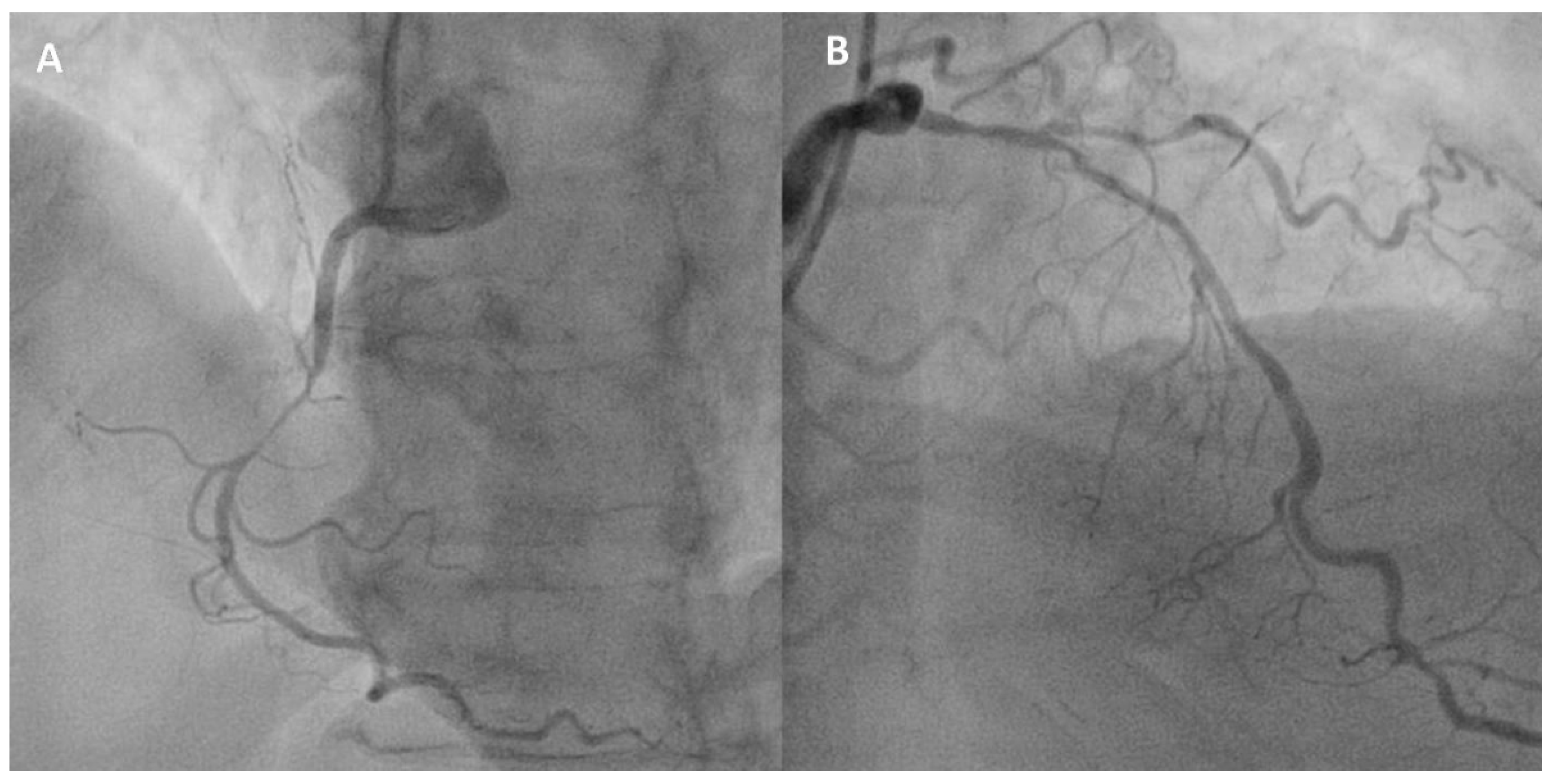
2. Case Vignette
3. Case Discussion
- Do we really know the tradeoff (benefit vs. risk) in such patients for a strategy based on early OAC initiation or continuation soon after revascularization in AF–ACS patients, especially with a low CHA2DS2VASc score and a high coronary risk, compared with a DAPT-only strategy?
- Should we then apply the same “in-or-out” thresholds for an obligatory anticoagulant prescription derived from non-ACS populations to such a specific clinical setting, even in the early phases after a coronary stenting?
- Should it not be reasonable to withhold OAC for some time, e.g., for the first month after revascularization in such AF–ACS patients, especially now that prasugrel and ticagrelor are widely available and known to be superior to clopidogrel in preventing atherothrombotic events and stent thrombosis [8,9]?
4. Prevention of Cardioembolic Stroke and Systemic Embolic Events
5. Prevention of Coronary Ischemic Events
6. Bleeding Risk with Differing Antithrombotic Strategies
7. Other Supporting Clues for an Early DAPT Strategy from ENTRUST-AF PCI
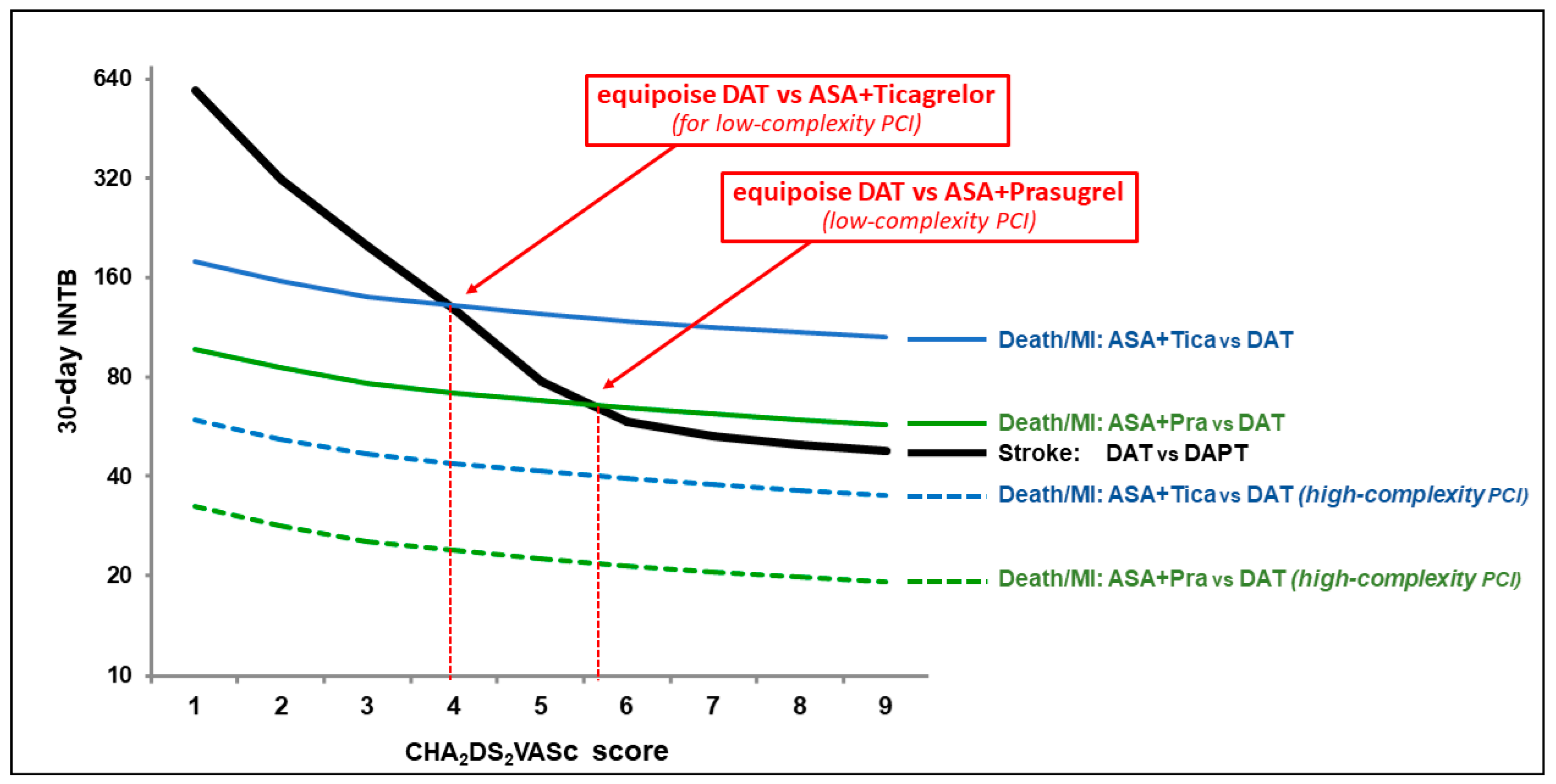
8. What to Do Then When a High Coronary Risk Occurs with a Low Cardioembolic Risk? A Role for Modern DAPT First, and DAT Later?
9. Limitations
10. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Dewilde, W.; Oirbans, T.; Verheugt, F.W.; Kelder, J.C.; De Smet, B.J.; Herrman, J.-P.; Adriaenssens, T.; Vrolix, M.; Heestermans, A.A.; Vis, M.M.; et al. Use of clopidogrel with or without aspirin in patients taking oral anticoagulant therapy and undergoing percutaneous coronary intervention: An open-label, randomised, controlled trial. Lancet 2013, 381, 1107–1115. [Google Scholar] [CrossRef]
- Cannon, C.P.; Bhatt, D.L.; Oldgren, J.; Lip, G.Y.; Ellis, S.G.; Kimura, T.; Maeng, M.; Merkely, B.; Zeymer, U.; Gropper, S.; et al. Dual Antithrombotic Therapy with Dabigatran after PCI in Atrial Fibrillation. N. Engl. J. Med. 2017, 377, 1513–1524. [Google Scholar] [CrossRef] [PubMed]
- Gibson, C.M.; Mehran, R.; Bode, C.; Halperin, J.; Verheugt, F.W.; Wildgoose, P.; Birmingham, M.; Ianus, J.; Burton, P.; Van Eickels, M.; et al. Prevention of Bleeding in Patients with Atrial Fibrillation Undergoing PCI. N. Engl. J. Med. 2016, 375, 2423–2434. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lopes, R.D.; Heizer, G.; Aronson, R.; Vora, A.N.; Massaro, T.; Mehran, R.; Goodman, S.G.; Windecker, S.; Darius, H.; Li, J.; et al. Antithrombotic Therapy after Acute Coronary Syndrome or PCI in Atrial Fibrillation. N. Engl. J. Med. 2019, 380, 1509–1524. [Google Scholar] [CrossRef] [Green Version]
- Vranckx, P.; Valgimigli, M.; Eckardt, L.; Tijssen, J.; Lewalter, T.; Gargiulo, G.; Batushkin, V.; Campo, G.; Lysak, Z.; Vakaliuk, I.; et al. Edoxaban-based versus vitamin K antagonist-based antithrombotic regimen after successful coronary stenting in patients with atrial fibrillation (ENTRUST-AF PCI): A randomised, open-label, phase 3b trial. Lancet 2019, 394, 1335–1343. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Collet, J.-P.; Haude, M.; Byrne, R.; Chung, E.H.; Fauchier, L.; Halvorsen, S.; Lau, D.H.; Lopez-Cabanillas, N.; Lettino, M.; et al. 2018 Joint European consensus document on the management of antithrombotic therapy in atrial fibrillation patients presenting with acute coronary syndrome and/or undergoing percutaneous cardiovascular interventions. Europace 2019, 21, 192–193. [Google Scholar] [CrossRef]
- Raval, A.N.; Cigarroa, J.E.; Chung, M.K.; Diaz-Sandoval, L.J.; Diercks, D.; Piccini, J.P.; Jung, H.S.; Washam, J.B.; Welch, B.G.; Zazulia, A.R.; et al. Management of Patients on Non-Vitamin K Antagonist Oral Anticoagulants in the Acute Care and Periprocedural Setting: A Scientific Statement From the American Heart Association. Circulation 2017, 135, e604–e633. [Google Scholar] [CrossRef]
- Wallentin, L.; Becker, R.C.; Budaj, A.; Cannon, C.P.; Emanuelsson, H.; Held, C.; Horrow, J.; Husted, S.; James, S.; Katus, H.; et al. Ticagrelor versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2009, 361, 1045–1057. [Google Scholar] [CrossRef]
- Wiviott, S.D.; Braunwald, E.; McCabe, C.H.; Montalescot, G.; Ruzyllo, W.; Gottlieb, S.; Neumann, F.-J.; Ardissino, D.; De Servi, S.; Murphy, S.A.; et al. Prasugrel versus Clopidogrel in Patients with Acute Coronary Syndromes. N. Engl. J. Med. 2007, 357, 2001–2015. [Google Scholar] [CrossRef] [Green Version]
- Hart, R.G.; Pearce, L.A.; Aguilar, M.I. Meta-analysis: Antithrombotic Therapy to Prevent Stroke in Patients Who Have Nonvalvular Atrial Fibrillation. Ann. Intern. Med. 2007, 146, 857. [Google Scholar] [CrossRef]
- Connolly, S.; Pogue, J.; Hart, R.; Chrolavicius, S.; Pfeffer, M.; Hohnloser, S.; Yusuf, S. Clopidogrel plus aspirin versus oral anticoagulation for atrial fibrillation in the Atrial fibrillation Clopidogrel Trial with Irbesartan for prevention of Vascular Events (ACTIVE W): A randomised controlled trial. Lancet 2006, 367, 1903–1912. [Google Scholar] [CrossRef] [PubMed]
- Camm, A.J.; Lip, G.Y.; De Caterina, R.; Savelieva, I.; Atar, D.; Hohnloser, S.H.; Kirchhof, P.; ESC Committee for Practice Guidelines (CPG). 2012 focused update of the ESC Guidelines for the management of atrial fibrillation: An update of the 2010 ESC Guidelines for the management of atrial fibrillation--developed with the special contribution of the European Heart Rhythm Association. Eur. Heart J. 2012, 33, 2719–2747. [Google Scholar] [PubMed] [Green Version]
- Olesen, J.B.; Lip, G.Y.H.; Hansen, M.L.; Hansen, T.; Tolstrup, J.S.; Lindhardsen, J.; Selmer, C.; Ahlehoff, O.; Olsen, A.-M.S.; Gislason, G.; et al. Validation of risk stratification schemes for predicting stroke and thromboembolism in patients with atrial fibrillation: Nationwide cohort study. BMJ 2011, 342, 124. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fox, K.A.; Frederick, F.A.A., Jr.; Goodman, S.G.; Steg, P.G.; Pieper, K.; Quill, A.; Gore, J.M. Time course of events in acute coronary syndromes: Implications for clinical practice from the GRACE registry. Nat. Clin. Pract. Neurol. 2008, 5, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Limbruno, U.; Goette, A.; De Caterina, R. Commentary: Temporarily omitting oral anticoagulants early after stenting for acute coronary syndromes patients with atrial fibrillation. Int. J. Cardiol. 2020. [Google Scholar] [CrossRef]
- Stone, G.W.; Généreux, P.; Harrington, R.A.; White, H.D.; Gibson, C.M.; Steg, P.G.; Hamm, C.W.; Mahaffey, K.W.; Price, M.J.; Prats, J.; et al. Impact of lesion complexity on peri-procedural adverse events and the benefit of potent intravenous platelet adenosine diphosphate receptor inhibition after percutaneous coronary intervention: Core laboratory analysis from 10 854 patients from the CHAMPION PHOENIX trial. Eur. Heart J. 2018, 39, 4112–4121. [Google Scholar] [CrossRef] [Green Version]
- Choi, H.-I.; Ahn, J.-M.; Kang, S.H.; Lee, P.H.; Kang, S.-J.; Lee, S.-W.; Kim, Y.-H.; Lee, C.W.; Park, S.-W.; Park, D.-W.; et al. Prevalence, Management, and Long-Term (6-Year) Outcomes of Atrial Fibrillation Among Patients Receiving Drug-Eluting Coronary Stents. JACC: Cardiovasc. Interv. 2017, 10, 1075–1085. [Google Scholar] [CrossRef]
- Hess, C.N.; Peterson, E.D.; Peng, S.A.; De Lemos, J.A.; Fosbøl, E.L.; Thomas, L.; Bhatt, D.L.; Saucedo, J.F.; Wang, T.Y. Use and Outcomes of Triple Therapy Among Older Patients With Acute Myocardial Infarction and Atrial Fibrillation. J. Am. Coll. Cardiol. 2015, 66, 616–627. [Google Scholar] [CrossRef] [Green Version]
- Gray, M.P.; Saba, S.; Zhang, Y.; Hernandez, I. Outcomes of Patients With Atrial Fibrillation Newly Recommended for Oral Anticoagulation Under the 2014 American Heart Association/American College of Cardiology/Heart Rhythm Society Guideline. J. Am. Heart Assoc. 2018, 7, e007881. [Google Scholar] [CrossRef] [Green Version]
- Douketis, J.D.; Spyropoulos, A.C.; Kaatz, S.; Becker, R.C.; Caprini, J.A.; Dunn, A.S.; Garcia, D.A.; Jacobson, A.; Jaffer, A.K.; Kong, D.F.; et al. Perioperative Bridging Anticoagulation in Patients with Atrial Fibrillation. N. Engl. J. Med. 2015, 373, 823–833. [Google Scholar] [CrossRef] [Green Version]
- Ulvenstam, A.; Henriksson, R.; Söderström, L.; Mooe, T. Ischemic stroke rates decrease with increased ticagrelor use after acute myocardial infarction in patients treated with percutaneous coronary intervention. Eur. J. Prev. Cardiol. 2018, 25, 1219–1230. [Google Scholar] [CrossRef] [PubMed]
- Henriksson, R.; Ulvenstam, A.; Söderström, L.; Mooe, T. Increase in ticagrelor use over time is associated with lower rates of ischemic stroke following myocardial infarction. BMC Cardiovasc. Disord. 2019, 19, 51. [Google Scholar] [CrossRef] [PubMed]
- Rozenbaum, Z.; Elis, A.; Shuvy, M.; Vorobeichik, D.; Shlomo, N.; Shlezinger, M.; Goldenberg, I.; Kimhi, O.; Pereg, D. CHA2DS2-VASc score and clinical outcomes of patients with acute coronary syndrome. Eur. J. Intern. Med. 2016, 36, 57–61. [Google Scholar] [CrossRef] [PubMed]
- Renda, G.; Ricci, F.; Patti, G.; Aung, N.; Petersen, S.E.; Gallina, S.; Hamrefors, V.; Melander, O.; Sutton, R.; Engstrom, G.; et al. CHA2DS2VASc score and adverse outcomes in middle-aged individuals without atrial fibrillation. Eur. J. Prev. Cardiol. 2019, 26, 1987–1997. [Google Scholar] [CrossRef]
- D’Ascenzo, F.; Bollati, M.; Clementi, F.; Castagno, D.; Lagerqvist, B.; Hernández, J.M.D.L.T.; Berg, J.M.T.; Brodie, B.R.; Urban, P.; Jensen, L.O.; et al. Incidence and predictors of coronary stent thrombosis: Evidence from an international collaborative meta-analysis including 30 studies, 221,066 patients, and 4276 thromboses. Int. J. Cardiol. 2013, 167, 575–584. [Google Scholar] [CrossRef] [Green Version]
- Brodie, B.; Pokharel, Y.; Garg, A.; Kissling, G.; Hansen, C.; Milks, S.; Cooper, M.; McAlhany, C.; Stuckey, T. Predictors of Early, Late, and Very Late Stent Thrombosis After Primary Percutaneous Coronary Intervention With Bare-Metal and Drug-Eluting Stents for ST-Segment Elevation Myocardial Infarction. JACC Cardiovasc. Interv. 2012, 5, 1043–1051. [Google Scholar] [CrossRef] [Green Version]
- Gargiulo, G.; Goette, A.; Tijssen, J.; Eckardt, L.; Lewalter, T.; Vranckx, P.; Valgimigli, M. Safety and efficacy outcomes of double vs. triple antithrombotic therapy in patients with atrial fibrillation following percutaneous coronary intervention: A systematic review and meta-analysis of non-vitamin K antagonist oral anticoagulant-based randomized clinical trials. Eur. Heart J. 2019, 40, 3757–3767. [Google Scholar] [CrossRef] [Green Version]
- Guedeney, P.; Mesnier, J.; Sorrentino, S.; Abcha, F.; Zeitouni, M.; Lattuca, B.; Silvain, J.; De Rosa, S.; Indolfi, C.; Collet, J.-P.; et al. Early Aspirin Discontinuation Following Acute Coronary Syndrome or Percutaneous Coronary Intervention: A Systematic Review and Meta-Analysis of Randomized Controlled Trials. J. Clin. Med. 2020, 9, 680. [Google Scholar] [CrossRef] [Green Version]
- Alexander, J.H.; Wojdyla, D.; Vora, A.N.; Thomas, L.; Granger, C.B.; Goodman, S.G.; Aronson, R.; Windecker, S.; Mehran, R.; Lopes, R.D. Risk/Benefit Tradeoff of Antithrombotic Therapy in Patients With Atrial Fibrillation Early and Late After an Acute Coronary Syndrome or Percutaneous Coronary Intervention. Circulation 2020, 141, 1618–1627. [Google Scholar] [CrossRef] [Green Version]
- Lamberts, M.; Olesen, J.B.; Ruwald, M.H.; Hansen, C.M.; Karasoy, D.; Kristensen, S.L.; Køber, L.; Torp-Pedersen, C.M.; Gislason, G.H.; Hansen, M.L. Bleeding After Initiation of Multiple Antithrombotic Drugs, Including Triple Therapy, in Atrial Fibrillation Patients Following Myocardial Infarction and Coronary Intervention: A Nationwide Cohort Study. Circulation 2012, 126, 1185–1193. [Google Scholar] [CrossRef] [Green Version]
- Rossini, R.; Capodanno, D.; Lettieri, C.; Tarantini, G.; Nijaradze, T.; Romano, M.; Lortkipanidze, N.; Cicorella, N.; Biondi-Zoccai, G.; Sirbu, V.; et al. Prevalence, Predictors, and Long-Term Prognosis of Premature Discontinuation of Oral Antiplatelet Therapy After Drug Eluting Stent Implantation. Am. J. Cardiol. 2011, 107, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Pilgrim, T.; Kalesan, B.; Zanchin, T.; Pulver, C.; Jung, S.; Mattle, H.; Carrel, T.; Moschovitis, A.; Stortecky, S.; Wenaweser, P.; et al. Impact of atrial fibrillation on clinical outcomes among patients with coronary artery disease undergoing revascularisation with drug-eluting stents. EuroIntervention 2013, 8, 1061–1071. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- De Caterina, R.; Limbruno, U. Antithrombotic treatment strategies after PCI. Lancet 2020, 395, 865. [Google Scholar] [CrossRef]





© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Limbruno, U.; De Sensi, F.; Cresti, A.; Picchi, A.; Lena, F.; De Caterina, R. Optimal Antithrombotic Treatment of Patients with Atrial Fibrillation Early after an Acute Coronary Syndrome—Triple Therapy, Dual Antithrombotic Therapy with an Anticoagulant… Or, Rather, Temporary Dual Antiplatelet Therapy? J. Clin. Med. 2020, 9, 2673. https://doi.org/10.3390/jcm9082673
Limbruno U, De Sensi F, Cresti A, Picchi A, Lena F, De Caterina R. Optimal Antithrombotic Treatment of Patients with Atrial Fibrillation Early after an Acute Coronary Syndrome—Triple Therapy, Dual Antithrombotic Therapy with an Anticoagulant… Or, Rather, Temporary Dual Antiplatelet Therapy? Journal of Clinical Medicine. 2020; 9(8):2673. https://doi.org/10.3390/jcm9082673
Chicago/Turabian StyleLimbruno, Ugo, Francesco De Sensi, Alberto Cresti, Andrea Picchi, Fabio Lena, and Raffaele De Caterina. 2020. "Optimal Antithrombotic Treatment of Patients with Atrial Fibrillation Early after an Acute Coronary Syndrome—Triple Therapy, Dual Antithrombotic Therapy with an Anticoagulant… Or, Rather, Temporary Dual Antiplatelet Therapy?" Journal of Clinical Medicine 9, no. 8: 2673. https://doi.org/10.3390/jcm9082673