Altered GH-IGF-1 Axis in Severe Obese Subjects is Reversed after Bariatric Surgery-Induced Weight Loss and Related with Low-Grade Chronic Inflammation

 ,
,  , and
, and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Patients and Controls
2.2. Parameters Analyzed
2.3. Analytical Procedures
2.4. Calculations
2.5. Statistical Analysis
3. Results
3.1. Characteristics of the Obese Patients and the Control Group
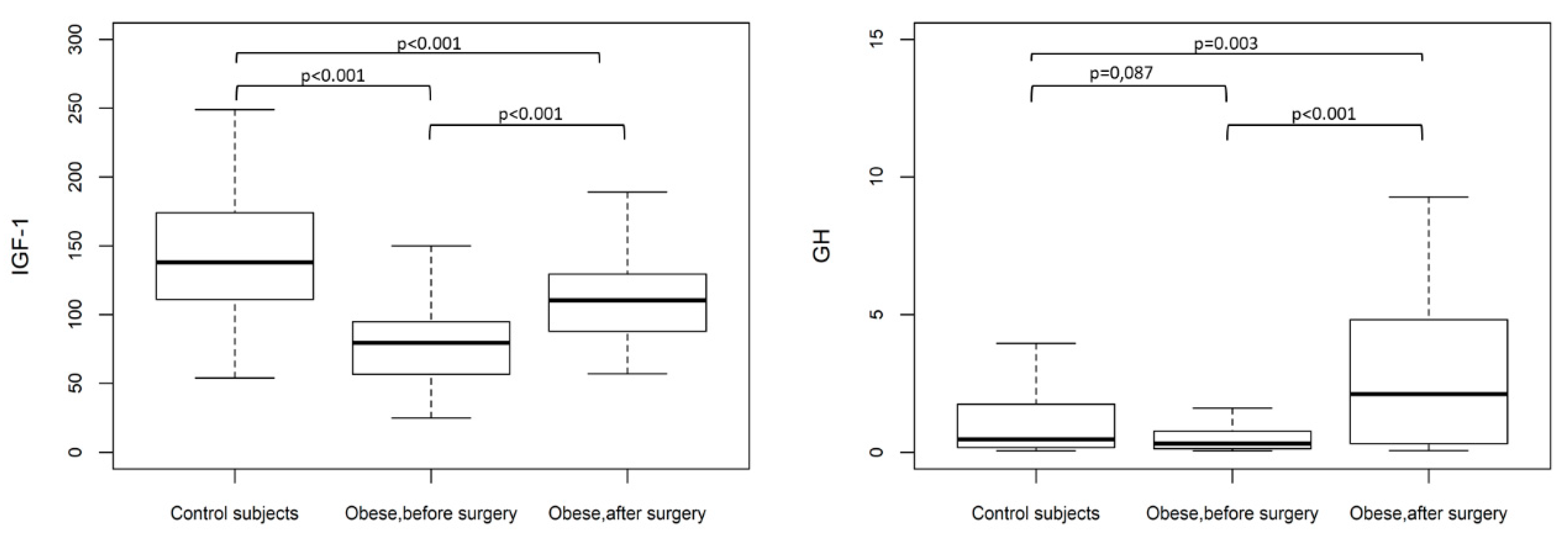
3.2. Fasting Serum Levels
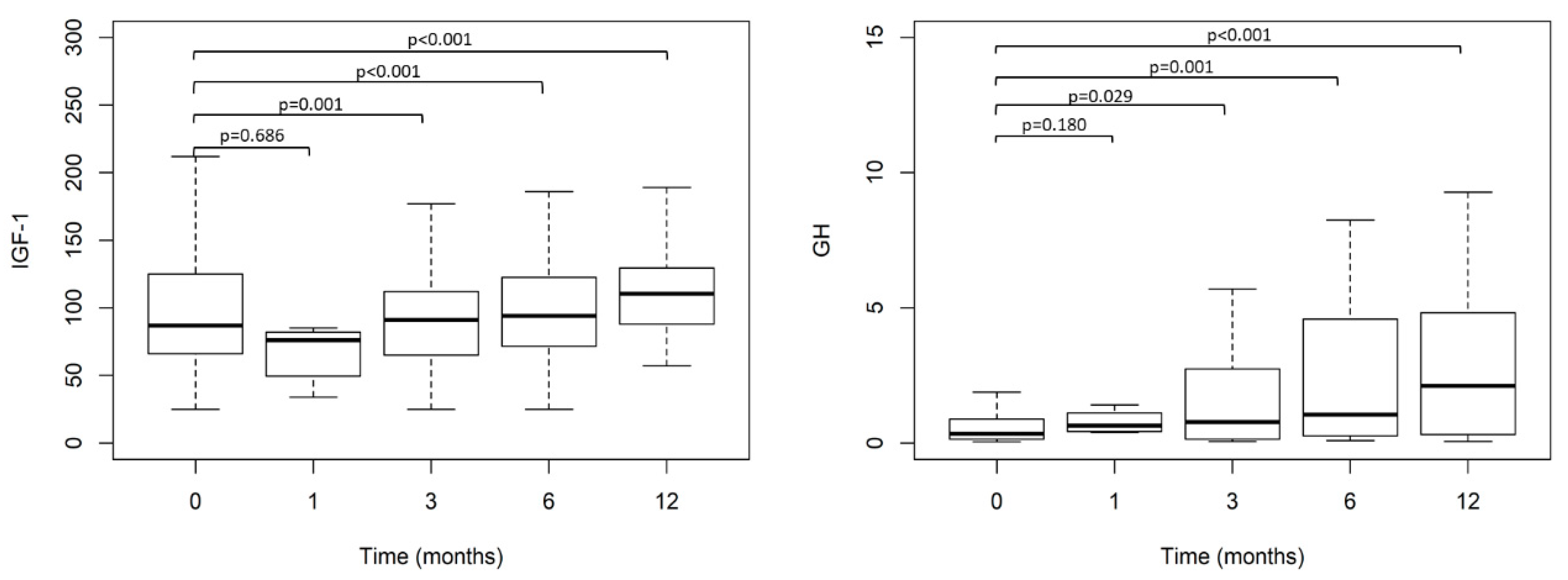
3.3. Time Course of the Clinical and Analytical Parameters
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Afshin, A. Health Effects of Overweight and Obesity in 195 Countries over 25 Years. N. Engl. J. Med. 2017, 377, 13–27. [Google Scholar] [CrossRef]
- Gutiérrez-Fisac, J.L.; Guallar-Castillón, P.; León-Muñoz, L.M.; Graciani, A.; Banegas, J.R.; Rodríguez-Artalejo, F. Prevalence of general and abdominal obesity in the adult population of Spain, 2008–2010: The ENRICA study. Obes. Rev. 2011, 13, 388–392. [Google Scholar] [CrossRef] [PubMed]
- Ward, Z.J.; Bleich, S.N.; Cradock, A.L.; Barrett, J.L.; Giles, C.M.; Flax, C.; Long, M.W.; Gortmaker, S.L. Projected U.S. State-Level Prevalence of Adult Obesity and Severe Obesity. N. Engl. J. Med. 2019, 381, 2440–2450. [Google Scholar] [CrossRef] [PubMed]
- Magkos, F.; Fraterrigo, G.; Yoshino, J.; Luecking, C.; Kirbach, K.; Kelly, S.C.; Fuentes, L.D.L.; He, S.; Okunade, A.L.; Patterson, B.W.; et al. Effects of Moderate and Subsequent Progressive Weight Loss on Metabolic Function and Adipose Tissue Biology in Humans with Obesity. Cell Metab. 2016, 23, 591–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Varela-Rodríguez, B.M.; Juiz-Valiña, P.; Varela, L.; Outeiriño-Blanco, E.; Bravo, S.B.; García-Brao, M.J.; Mena, E.; Noguera, J.F.; Valero-Gasalla, J.; Cordido, F.; et al. Beneficial Effects of Bariatric Surgery-Induced by Weight Loss on the Proteome of Abdominal Subcutaneous Adipose Tissue. J. Clin. Med. 2020, 9, 213. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Reges, O.; Greenland, P.; Dicker, D.; Leibowitz, M.; Hoshen, M.B.; Gofer, I.; Rasmussen-Torvik, L.J.; Balicer, R.D. Association of Bariatric Surgery Using Laparoscopic Banding, Roux-en-Y Gastric Bypass, or Laparoscopic Sleeve Gastrectomy vs Usual Care Obesity Management with All-Cause Mortality. JAMA 2018, 319, 279–290. [Google Scholar] [CrossRef] [Green Version]
- Juiz-Valiña, P.; Outeiriño-Blanco, E.; Pértega, S.; Varela-Rodríguez, B.M.; García-Brao, M.J.; Mena, E.; Pena-Bello, L.; Cordido, M.; Sangiao-Alvarellos, S.; Cordido, F. Effect of Weight Loss after Bariatric Surgery on Thyroid-Stimulating Hormone Levels in Euthyroid Patients with Morbid Obesity. Nutrients 2019, 11, 1121. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juiz-Valiña, P.; Cordido, M.; Outeiriño-Blanco, E.; Pértega, S.; Varela-Rodríguez, B.M.; García-Brao, M.J.; Mena, E.; Pena-Bello, L.; Sangiao-Alvarellos, S.; Cordido, F.; et al. Central Resistance to Thyroid Hormones in Morbidly Obese Subjects Is Reversed after Bariatric Surgery-Induced Weight Loss. J. Clin. Med. 2020, 9, 359. [Google Scholar] [CrossRef] [Green Version]
- Pena-Bello, L.; Seoane-Pillado, T.; Sangiao-Alvarellos, S.; Outeiriño-Blanco, E.; Varela-Rodríguez, B.M.; Juiz-Valiña, P.; Cordido, F.; Cordido, F. Oral glucose-stimulated growth hormone (GH) test in adult GH deficiency patients and controls: Potential utility of a novel test. Eur. J. Intern. Med. 2017, 44, 55–61. [Google Scholar] [CrossRef]
- Pena-Bello, L.; Pértega-Díaz, S.; Outeiriño-Blanco, E.; Garcia-Buela, J.; Tovar, S.; Sangiao-Alvarellos, S.; Diéguez, C.; Cordido, F. Effect of Oral Glucose Administration on Rebound Growth Hormone Release in Normal and Obese Women: The Role of Adiposity, Insulin Sensitivity and Ghrelin. PLoS ONE 2015, 10, e0121087. [Google Scholar] [CrossRef]
- Álvarez-Castro, P.; Sangiao-Alvarellos, S.; Brandón-Sandá, I.; Cordido, F. Función endocrina en la obesidad. Endocrinología Y Nutrición 2011, 58, 422–432. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rasmussen, M.H.; Hvidberg, A.; Hilsted, J.; Juul, A.; Main, K.M.; Gotfredsen, A.; E Skakkebaek, N.; E Skakkebae, N. Massive weight loss restores 24-hour growth hormone release profiles and serum insulin-like growth factor-I levels in obese subjects. J. Clin. Endocrinol. Metab. 1995, 80, 1407–1415. [Google Scholar] [CrossRef] [PubMed]
- Cordido, F.; Penalva, A.; Dieguez, C.; Casanueva, F.F. Massive growth hormone (GH) discharge in obese subjects after the combined administration of GH-releasing hormone and GHRP-6: Evidence for a marked somatotroph secretory capability in obesity. J. Clin. Endocrinol. Metab. 1993, 76, 819–823. [Google Scholar] [PubMed]
- Yu, A.P.; Ugwu, F.N.; Tam, B.T.; Lee, P.H.; Ma, V.; Pang, S.; Chow, A.S.; Cheng, K.K.; Lai, C.W.; Wong, C.S.; et al. Obestatin and growth hormone reveal the interaction of central obesity and other cardiometabolic risk factors of metabolic syndrome. Sci. Rep. 2020, 10, 1–10. [Google Scholar] [CrossRef]
- Cordido, F.; Casanueva, F.F.; Vidal, J.I.; Diéguez, C. Study of Insulin-Like Growth Factor I in Human Obesity. Horm. Res. 1991, 36, 187–191. [Google Scholar] [CrossRef]
- Aleidi, S.M.; Shayeb, E.; Bzour, J.; Abu-Rish, E.Y.; Hudaib, M.; Al Alawi, S.; Bustanji, Y. Serum level of insulin-like growth factor-I in type 2 diabetic patients: Impact of obesity. Horm. Mol. Biol. Clin. Investig. 2019, 39. [Google Scholar] [CrossRef]
- Frystyk, J.; Brick, D.J.; Gerweck, A.V.; Utz, A.L.; Miller, K.K. Bioactive insulin-like growth factor-I in obesity. J. Clin. Endocrinol. Metab. 2009, 94, 3093–3097. [Google Scholar] [CrossRef] [Green Version]
- Utz, A.L.; Yamamoto, A.; Sluss, P.; Breu, J.; Miller, K.K. Androgens may mediate a relative preservation of IGF-I levels in overweight and obese women despite reduced growth hormone secretion. J. Clin. Endocrinol. Metab. 2008, 93, 4033–4040. [Google Scholar] [CrossRef] [Green Version]
- Engstrom, B.E.; Burman, P.; Holdstock, C.; Ohrvall, M.; Sundbom, M.; Karlsson, F.A. Effects of gastric bypass on the GH/IGF-I axis in severe obesity—And a comparison with GH deficiency. Eur. J. Endocrinol. 2006, 154, 53–59. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Barrea, L.; Laudisio, D.; Di Somma, C.; Pugliese, G.; Salzano, C.; Colao, A.; Savastano, S. Somatotropic Axis and Obesity: Is There Any Role for the Mediterranean Diet? Nutrients 2019, 11, 2228. [Google Scholar] [CrossRef] [Green Version]
- L’Allemand, D.; Schmidt, S.; Rousson, V.; Brabant, G.; Gasser, T.; Grüters-Kieslich, A. Associations between body mass, leptin, IGF-I and circulating adrenal androgens in children with obesity and premature adrenarche. Eur. J. Endocrinol. 2002, 146, 537–543. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Frystyk, J.; Vestbo, E.; Skjærbaek, C.; Mogensen, C.; Ørskov, H. Free insulin-like growth factors in human obesity. Metabolism 1995, 44, 37–44. [Google Scholar] [CrossRef]
- Ricco, R.C.; Ricco, R.G.; Queluz, M.C.; De Paula, M.T.S.; Atique, P.V.; Custódio, R.J.; Filho, H.T.; Liberatori, R.D.R.; Martinelli, C.E. IGF-1R mRNA expression is increased in obese children. Growth Horm. IGF Res. 2018, 39, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Stanley, T.L.; Feldpausch, M.N.; Murphy, C.A.; Grinspoon, S.K.; Makimura, H. Discordance of IGF-1 and GH stimulation testing for altered GH secretion in obesity. Growth Horm. IGF Res. 2014, 24, 10–15. [Google Scholar] [CrossRef] [Green Version]
- Vottero, A.; Guzzetti, C.; Loche, S. New Aspects of the Physiology of the GH-IGF-1 Axis. Endocr. Dev. 2013, 24, 96–105. [Google Scholar] [CrossRef]
- Haywood, N.J.; Slater, T.A.; Matthews, C.J.; Wheatcroft, S.B. The insulin like growth factor and binding protein family: Novel therapeutic targets in obesity & diabetes. Mol. Metab. 2018, 19, 86–96. [Google Scholar] [CrossRef]
- Schneider, H.J.; Saller, B.; Klotsche, J.; Erwa, W.; Wittchen, H.-U.; März, W.; Stalla, G.K. Opposite associations of age-dependent insulin-like growth factor-I standard deviation scores with nutritional state in normal weight and obese subjects. Eur. J. Endocrinol. 2006, 154, 699–706. [Google Scholar] [CrossRef] [Green Version]
- Schneider, H.J.; Klotsche, J.; Saller, B.; Böhler, S.; Sievers, C.; Pittrow, D.; Ruf, G.; März, W.; Erwa, W.; Zeiher, A.M.; et al. Associations of age-dependent IGF-I SDS with cardiovascular diseases and risk conditions: Cross-sectional study in 6773 primary care patients. Eur. J. Endocrinol. 2008, 158, 153–161. [Google Scholar] [CrossRef]
- De Marinis, L.; Bianchi, A.; Mancini, A.; Gentilella, R.; Perrelli, M.; Giampietro, A.; Porcelli, T.; Tilaro, L.; Fusco, A.; Valle, D.; et al. Growth Hormone Secretion and Leptin in Morbid Obesity before and after Biliopancreatic Diversion: Relationships with Insulin and Body Composition. J. Clin. Endocrinol. Metab. 2004, 89, 174–180. [Google Scholar] [CrossRef] [Green Version]
- Beeken, R.J.; Croker, H.; Heinrich, M.; Obichere, A.; Finer, N.; Murphy, N.; Goldin, R.; Guppy, N.J.; Wilson, R.; Fisher, A.; et al. The Impact of Diet-Induced Weight Loss on Biomarkers for Colorectal Cancer: An Exploratory Study (INTERCEPT). Obesity 2017, 25, S95–S101. [Google Scholar] [CrossRef] [Green Version]
- Bakdash, J.Z.; Marusich, L.R. Repeated Measures Correlation. Front. Psychol. 2017, 8, 456. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Luque, R.M.; Gahete, M.D.; Valentine, R.J.; Kineman, R.D. Examination of the direct effects of metabolic factors on somatotrope function in a non-human primate model, Papio anubis. J. Mol. Endocrinol. 2006, 37, 25–38. [Google Scholar] [CrossRef] [PubMed]
- Lanzi, R.; Manzoni, M.F.; Andreotti, A.C.; Malighetti, M.E.; Bianchi, E.; Sereni, L.P.; Caumo, A.; Luzi, L.; Pontiroli, A.E. Evidence for an inhibitory effect of physiological levels of insulin on the growth hormone (GH) response to GH-releasing hormone in healthy subjects. J. Clin. Endocrinol. Metab. 1997, 82, 2239–2243. [Google Scholar] [CrossRef] [PubMed]
- Clasey, J.L.; Weltman, A.; Patrie, J.; Weltman, J.Y.; Pezzoli, S.; Bouchard, C.; Thorner, M.O.; Hartman, M.L. Abdominal visceral fat and fasting insulin are important predictors of 24-hour GH release independent of age, gender, and other physiological factors. J. Clin. Endocrinol. Metab. 2001, 86, 3845–3852. [Google Scholar] [CrossRef]
- Cornford, A.S.; Barkan, A.L.; Horowitz, J.F. Rapid suppression of growth hormone concentration by overeating: Potential mediation by hyperinsulinemia. J. Clin. Endocrinol. Metab. 2011, 96, 824–830. [Google Scholar] [CrossRef] [Green Version]
- Garin, M.C.; Burns, C.M.; Kaul, S.; Cappola, A.R. Clinical review: The human experience with ghrelin administration. J. Clin. Endocrinol. Metab. 2013, 98, 1826–1837. [Google Scholar] [CrossRef] [Green Version]
- Nass, R.; Farhy, L.S.; Liu, J.; Prudom, C.E.; Johnson, M.L.; Veldhuis, P.; Pezzoli, S.S.; Oliveri, M.C.; Gaylinn, B.; Geysen, H.M.; et al. Evidence for acyl-ghrelin modulation of growth hormone release in the fed state. J. Clin. Endocrinol. Metab. 2008, 93, 1988–1994. [Google Scholar] [CrossRef] [Green Version]
- Karra, E.; Batterham, R.L. The role of gut hormones in the regulation of body weight and energy homeostasis. Mol. Cell. Endocrinol. 2010, 316, 120–128. [Google Scholar] [CrossRef]
- Maccario, M.; Tassone, F.; Gianotti, L.; Lanfranco, F.; Grottoli, S.; Arvat, E.; Muller, E.E.; Ghigo, E. Effects of recombinant human insulin-like growth factor I administration on the growth hormone (gh) response to GH-releasing hormone in obesity. J. Clin. Endocrinol. Metab. 2001, 86, 167–171. [Google Scholar]
- Cirillo, F.; Lazzeroni, P.; Sartori, C.; Street, M.E. Inflammatory Diseases and Growth: Effects on the GH–IGF Axis and on Growth Plate. Int. J. Mol. Sci. 2017, 18, 1878. [Google Scholar] [CrossRef] [Green Version]
- Kojta, I.; Chacińska, M.; Błachnio-Zabielska, A.U. Obesity, Bioactive Lipids, and Adipose Tissue Inflammation in Insulin Resistance. Nutrients 2020, 12, 1305. [Google Scholar] [CrossRef] [PubMed]
- Fornari, R.; Marocco, C.; Francomano, D.; Fittipaldi, S.; Lubrano, C.; Bimonte, V.M.; Donini, L.M.; Nicolai, E.; Aversa, A.; Lenzi, A.; et al. Insulin growth factor-1 correlates with higher bone mineral density and lower inflammation status in obese adult subjects. Eat. Weight Disord. Stud. Anorex. Bulim. Obes. 2017, 23, 375–381. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Sun, H.; Ma, B.; Gao, J.; Yin, J.; Qu, S. Insulin-Like Growth Factor 1 Related to Chronic Low-Grade Inflammation in Patients with Obesity and Early Change of its Levels After Laparoscopic Sleeve Gastrectomy. Obes. Surg. 2020, 30, 3326–3332. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Arnao, J.; Miell, J.P.; Ross, R.J. Influence of thyroid hormones on the GH-IGF-I axis. Trends Endocrinol. Metab. 1993, 4, 169–173. [Google Scholar] [CrossRef]
- Yamauchi, I.; Sakane, Y.; Yamashita, T.; Hirota, K.; Ueda, Y.; Kanai, Y.; Yamashita, Y.; Kondo, E.; Fujii, T.; Taura, D.; et al. Effects of growth hormone on thyroid function are mediated by type 2 iodothyronine deiodinase in humans. Endocrine 2018, 59, 353–363. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fleseriu, M.; Hashim, I.A.; Karavitaki, N.; Melmed, S.; Murad, M.H.; Salvatori, R.; Samuels, M.H. Hormonal Replacement in Hypopituitarism in Adults: An Endocrine Society Clinical Practice Guideline. J. Clin. Endocrinol. Metab. 2016, 101, 3888–3921. [Google Scholar] [CrossRef] [PubMed]
- Porretti, S.; Giavoli, C.; Ronchi, C.; Lombardi, G.; Zaccaria, M.; Valle, D.; Arosio, M.; Beck-Peccoz, P. Recombinant Human GH Replacement Therapy and Thyroid Function in a Large Group of Adult GH-Deficient Patients: When Doesl-T4Therapy Become Mandatory? J. Clin. Endocrinol. Metab. 2002, 87, 2042–2045. [Google Scholar] [CrossRef]
- Van Der Spoel, E.; Roelfsema, F.; Akintola, A.A.; Jansen, S.W.; Slagboom, P.E.; Westendorp, R.G.J.; Blauw, G.J.; Pijl, H.; Van Heemst, D. Interrelationships Between Pituitary Hormones as Assessed From 24-hour Serum Concentrations in Healthy Older Subjects. J. Clin. Endocrinol. Metab. 2019, 105, 105. [Google Scholar] [CrossRef]
- Kopchick, J.J.; Berryman, D.E.; Puri, V.; Lee, K.Y.; Jorgensen, J.O.L. The effects of growth hormone on adipose tissue: Old observations, new mechanisms. Nat. Rev. Endocrinol. 2019, 16, 135–146. [Google Scholar] [CrossRef]
- Høyer, K.L.; Høgild, M.L.; List, E.O.; Lee, K.Y.; Kissinger, E.; Sharma, R.; Magnusson, N.E.; Puri, V.; Kopchick, J.J.; Jørgensen, J.O.L.; et al. The acute effects of growth hormone in adipose tissue is associated with suppression of antilipolytic signals. Physiol. Rep. 2020, 8, e14373. [Google Scholar] [CrossRef]
- Berryman, D.E.; Glad, C.A.; O List, E.; Johannsson, G. The GH/IGF-1 axis in obesity: Pathophysiology and therapeutic considerations. Nat. Rev. Endocrinol. 2013, 9, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Bredella, M.A.; Gerweck, A.V.; Lin, E.; Landa, M.G.; Torriani, M.; Schoenfeld, D.A.; Hemphill, L.C.; Miller, K.K. Effects of GH on Body Composition and Cardiovascular Risk Markers in Young Men with Abdominal Obesity. J. Clin. Endocrinol. Metab. 2013, 98, 3864–3872. [Google Scholar] [CrossRef] [PubMed]
- Bredella, M.A.; Karastergiou, K.; Bos, S.A.; Gerweck, A.V.; Torriani, M.; Fried, S.K.; Miller, K.K. GH administration decreases subcutaneous abdominal adipocyte size in men with abdominal obesity. Growth Horm. IGF Res. 2017, 35, 17–20. [Google Scholar] [CrossRef] [PubMed]
- Høgild, M.L.; Bak, A.M.; Pedersen, S.B.; Rungby, J.; Frystyk, J.; Møller, N.; Jessen, N.; Jørgensen, J.O.L. Growth hormone signaling and action in obese versus lean human subjects. Am. J. Physiol. Endocrinol. Metab. 2019, 316, E333–E344. [Google Scholar] [CrossRef]
- Glad, C.A.; Svensson, P.-A.; Nystrom, F.H.; Jacobson, P.; Carlsson, L.M.S.; Johannsson, G.; Andersson-Assarsson, J.C. Expression of GHR and Downstream Signaling Genes in Human Adipose Tissue—Relation to Obesity and Weight Change. J. Clin. Endocrinol. Metab. 2018, 104, 1459–1470. [Google Scholar] [CrossRef]
- Carlzon, D.; Svensson, J.; Petzold, M.; Karlsson, M.; Ljunggren, Ö.; Tivesten, Å.; Mellström, D.; Ohlsson, C. Both Low and High Serum IGF-1 Levels Associate with Increased Risk of Cardiovascular Events in Elderly Men. J. Clin. Endocrinol. Metab. 2014, 99, E2308–E2316. [Google Scholar] [CrossRef] [Green Version]
- Burgers, A.M.G.; Biermasz, N.R.; Schoones, J.W.; Pereira, A.M.; Renehan, A.; Zwahlen, M.; Egger, M.; Dekkers, O.M. Meta-Analysis and Dose-Response Metaregression: Circulating Insulin-Like Growth Factor I (IGF-I) and Mortality. J. Clin. Endocrinol. Metab. 2011, 96, 2912–2920. [Google Scholar] [CrossRef]
- Ricotti, R.; Solito, A.; Zani, E.M.; Caputo, M.; Genoni, G.; Barone-Adesi, F.; Mancioppi, V.; Agosti, E.; Aimaretti, G.; Bellone, S.; et al. The relationship between cortisol and IGF-I influences metabolic alteration in pediatric overweight and obesity. Eur. J. Endocrinol. 2020, 182, 255–264. [Google Scholar] [CrossRef]
- Cordido, F.; Garcia-Buela, J.; Sangiao-Alvarellos, S.; Martínez, T.; Vidal, O. The Decreased Growth Hormone Response to Growth Hormone Releasing Hormone in Obesity Is Associated to Cardiometabolic Risk Factors. Mediat. Inflamm. 2010, 2010, 1–8. [Google Scholar] [CrossRef] [Green Version]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Control Subjects | Obese Subjects | p | |
|---|---|---|---|
| Median (IR) | Median (IR) | ||
| Age (years) | 42.0 (37.3; 53.0) | 45.2 (39.1; 50.8) | 0.794 |
| Sex (n, %) | 0.143 | ||
| Female | 73.2% | 83.6% | |
| Male | 26.8% | 16.4% | |
| BMI (kg/m2) | 23.2 (21.1; 24.1) | 47.8 (43.8; 53.0) | <0.001 |
| Body fat (%) | 27.6 (20.5; 30.4) | 51.1 (48.0; 54.2) | <0.001 |
| Type of surgery (%) | --- | ||
| Roux-en-Y gastric bypass | 50.9% | ||
| Sleeve gastrectomy | 49.1% |
| Control Subjects | Obese Subjects | p | |
|---|---|---|---|
| Median (IR) | Median (IR) | ||
| IGF-1 (µg/L) | 138.0 (111; 174) | 79.5 (56.6; 95.0) | <0.001 |
| GH (µg/L) | 0.5 (0.2; 1.7) | 0.3 (0.1; 0.8) | 0.087 |
| TSH (µU/mL) | 1.9 (1.3; 2.5) | 2.8 (1.5; 4.9) | 0.002 |
| Free T4 (ng/dL) | 1.2 (1.1; 1.2) | 1.4 (1.3; 1.7) | <0.001 |
| Fasting Glucose (mg/dL) | 89.0 (84.0; 95.0) | 96.0 (81.5; 115.5) | 0.030 |
| Fasting Insulin (µIU/mL) | 3.5 (2.9; 6,2) | 6.0 (2.8; 9.6) | 0.009 |
| HOMA-IR | 0.8 (0.6; 1.5) | 1.4 (0.6; 2.7) | 0.004 |
| Obese Patients Before Surgery | Obese Patients Twelve Months after Surgery | Change | p | |
|---|---|---|---|---|
| Median (IR) | Median (IR) | Median (IR) | ||
| IGF-1 (µg/L) | 79.5 (56.6; 95.0) | 110.5 (88.0; 129.5) | −30.5 (−52.0; −11.0) | <0.001 |
| GH (µg/L) | 0.3 (0.1; 0.8) | 2.1 (0.3; 4.8) | −2.0 (−3.6; −0.1) | <0.001 |
| Weight (kg) | 123.1 (105.4; 146.0) | 83.5 (69.5; 98.0) | 43.1 (36.7; 55.3) | <0.001 |
| BMI (kg/m2) | 47.8 (43.8; 53.0) | 30.4 (26.9; 35.6) | 16.5 (13.8; 19.5) | <0.001 |
| Body fat (%) | 51.1 (48.0; 54.2) | 33.0 (25.7; 40.8) | 16.7 (11.2; 20.3) | <0.001 |
| TSH (µU/mL) | 2.8 (1.5; 4.9) | 2.3 (1.4; 3.2) | 0.7 (−0.4; 2.5) | 0.001 |
| Free T4 (ng/dL) | 1.4 (1.3; 1.7) | 1.1 (1.0; 1.2) | 0.3 (0.2; 0.6) | <0.001 |
| Fasting Glucose (mg/dL) | 96.0 (81.5; 115.5) | 84.0 (77.0; 90.0) | 12.0 (−2.0; 26.5) | <0.001 |
| Fasting Insulin (µIU/mL) | 6.0 (2.8; 9.6) | 5.4 (2.9; 8.5) | 0.3 (−1.8; 3.4) | 0.256 |
| HOMA-IR | 1.4 (0.6; 2.7) | 1.1 (0.6; 2.0) | 0.3 (−0.4; 1.0) | 0.037 |
| C-Peptide (ng/mL) | 2.1 (1.4; 3.2) | 1.8 (1.4; 2.3) | 0.1 (−0.6; 1.0) | 0.194 |
| C-Reactive Protein (mg/dL) | 0.7 (0.4; 1.2) | 0.1 (0.02; 0.3) | 0.5 (0.1; 0.8) | <0.001 |
| IGF-1 | GH | |||||
|---|---|---|---|---|---|---|
| B | SE | p | B | SE | p | |
| Intercept | 113.25 | 18.67 | <0.001 | 2.06 | 1.06 | 0.052 |
| Linear time (months after surgery) | 1.91 | 0.43 | <0.001 | 0.21 | 0.04 | <0.001 |
| Basal BMI (kg/m2) | −0.58 | 0.33 | 0.083 | −0.01 | 0.02 | 0.679 |
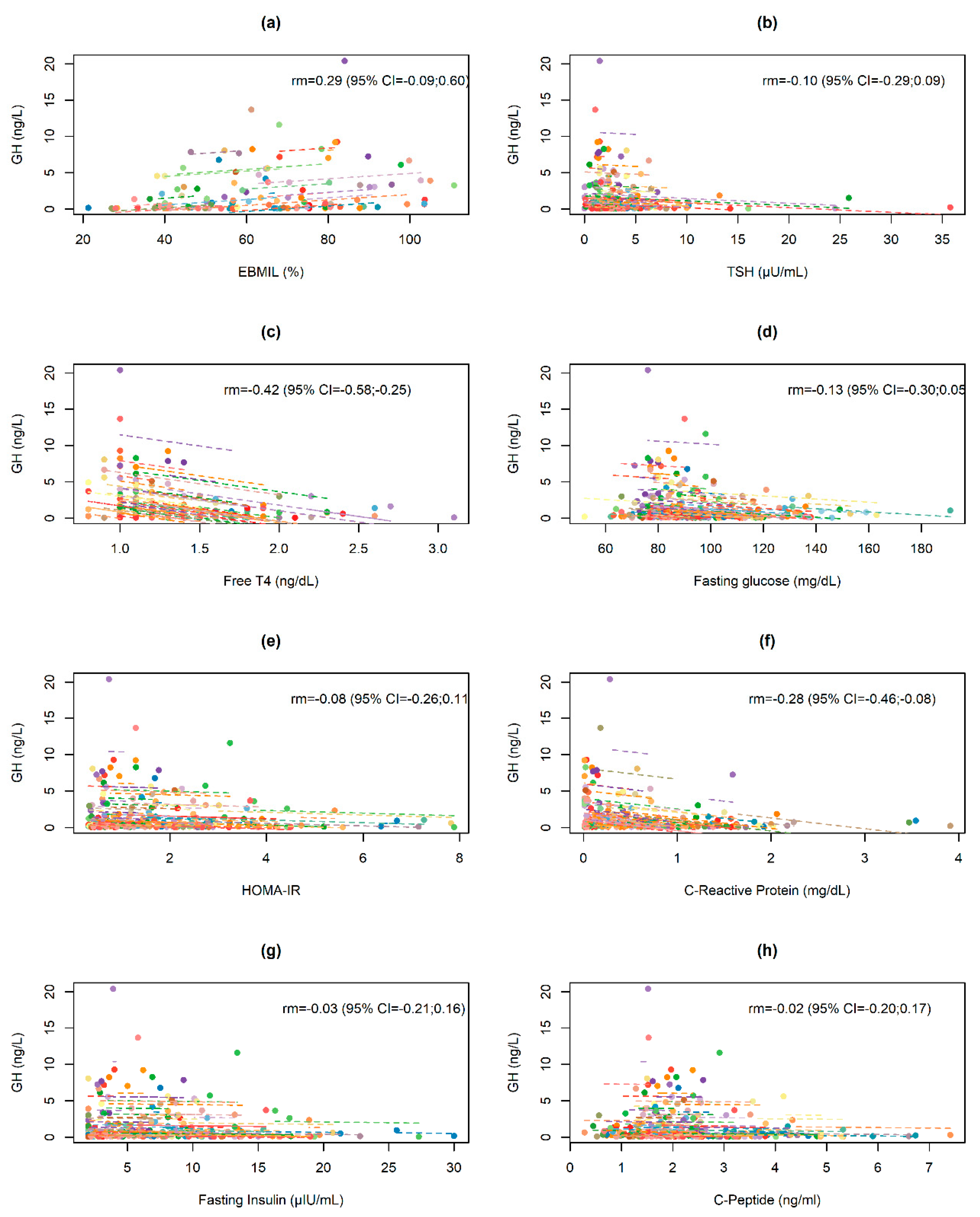
| Free T4 (ng/dL) | 3.15 | 5.34 | 0.555 | −0.62 | 0.31 | 0.045 |
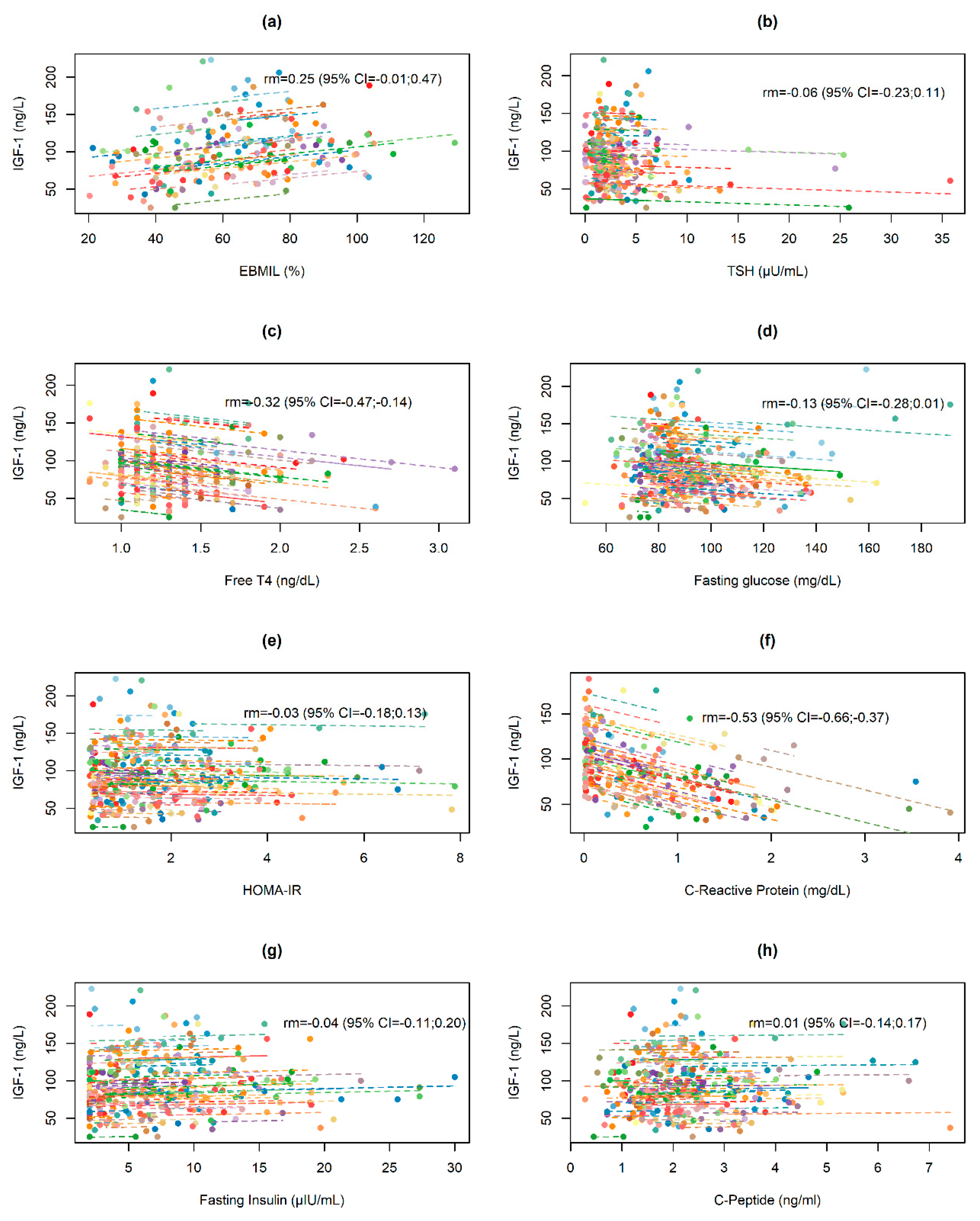
| C-Reactive Protein (mg/dL) | −12.29 | 3.23 | <0.001 | 0.01 | 0.20 | 0.997 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Juiz-Valiña, P.; Pena-Bello, L.; Cordido, M.; Outeiriño-Blanco, E.; Pértega, S.; Varela-Rodriguez, B.; Garcia-Brao, M.J.; Mena, E.; Sangiao-Alvarellos, S.; Cordido, F. Altered GH-IGF-1 Axis in Severe Obese Subjects is Reversed after Bariatric Surgery-Induced Weight Loss and Related with Low-Grade Chronic Inflammation. J. Clin. Med. 2020, 9, 2614. https://doi.org/10.3390/jcm9082614
Juiz-Valiña P, Pena-Bello L, Cordido M, Outeiriño-Blanco E, Pértega S, Varela-Rodriguez B, Garcia-Brao MJ, Mena E, Sangiao-Alvarellos S, Cordido F. Altered GH-IGF-1 Axis in Severe Obese Subjects is Reversed after Bariatric Surgery-Induced Weight Loss and Related with Low-Grade Chronic Inflammation. Journal of Clinical Medicine. 2020; 9(8):2614. https://doi.org/10.3390/jcm9082614
Chicago/Turabian StyleJuiz-Valiña, Paula, Lara Pena-Bello, Maria Cordido, Elena Outeiriño-Blanco, Sonia Pértega, Barbara Varela-Rodriguez, Maria Jesus Garcia-Brao, Enrique Mena, Susana Sangiao-Alvarellos, and Fernando Cordido. 2020. "Altered GH-IGF-1 Axis in Severe Obese Subjects is Reversed after Bariatric Surgery-Induced Weight Loss and Related with Low-Grade Chronic Inflammation" Journal of Clinical Medicine 9, no. 8: 2614. https://doi.org/10.3390/jcm9082614