The Reality of Patient-Reported Outcomes of Health-Related Quality of Life in an Italian Cohort of Patients with Inflammatory Bowel Disease: Results from a Cross-Sectional Study


 ,
,  ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Interventions
2.3. Questionnaire
2.4. Ethical Considerations
2.5. Statistical Analysis
3. Results
3.1. Demographic and Clinical Characteristics of Study Population
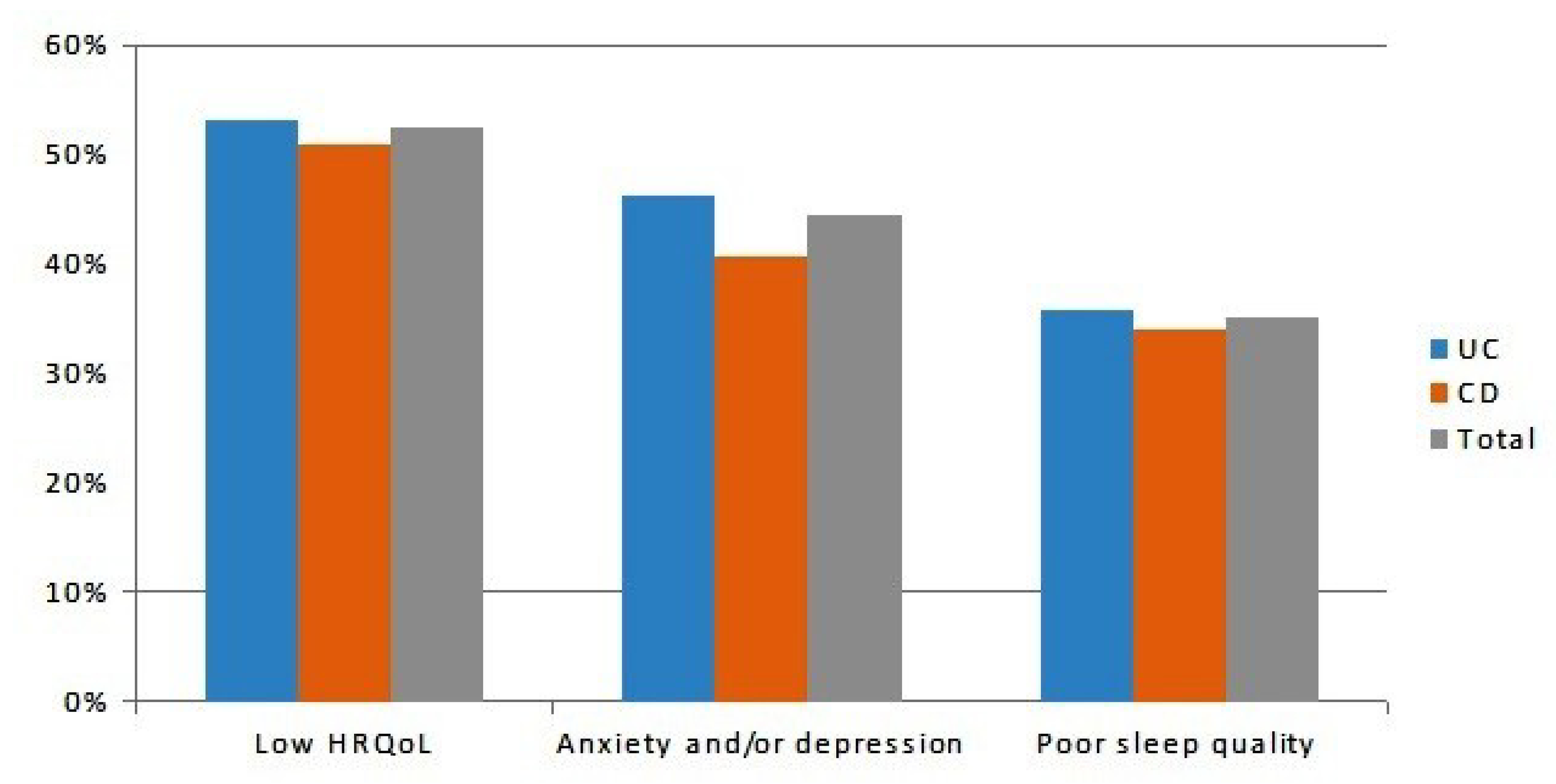
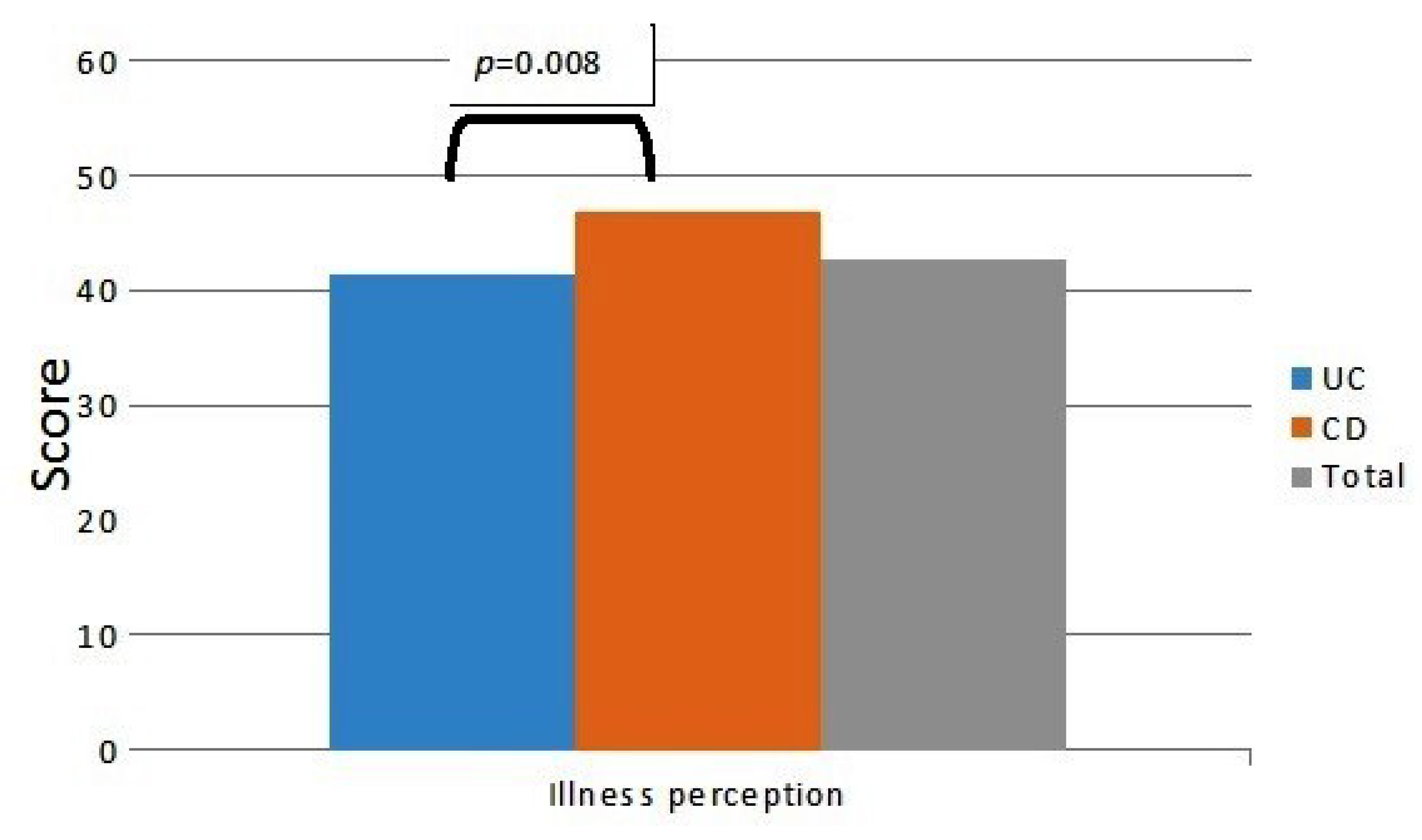
3.2. Factors Associated with Low Quality of Life
3.3. Impact on Working and Social Activities
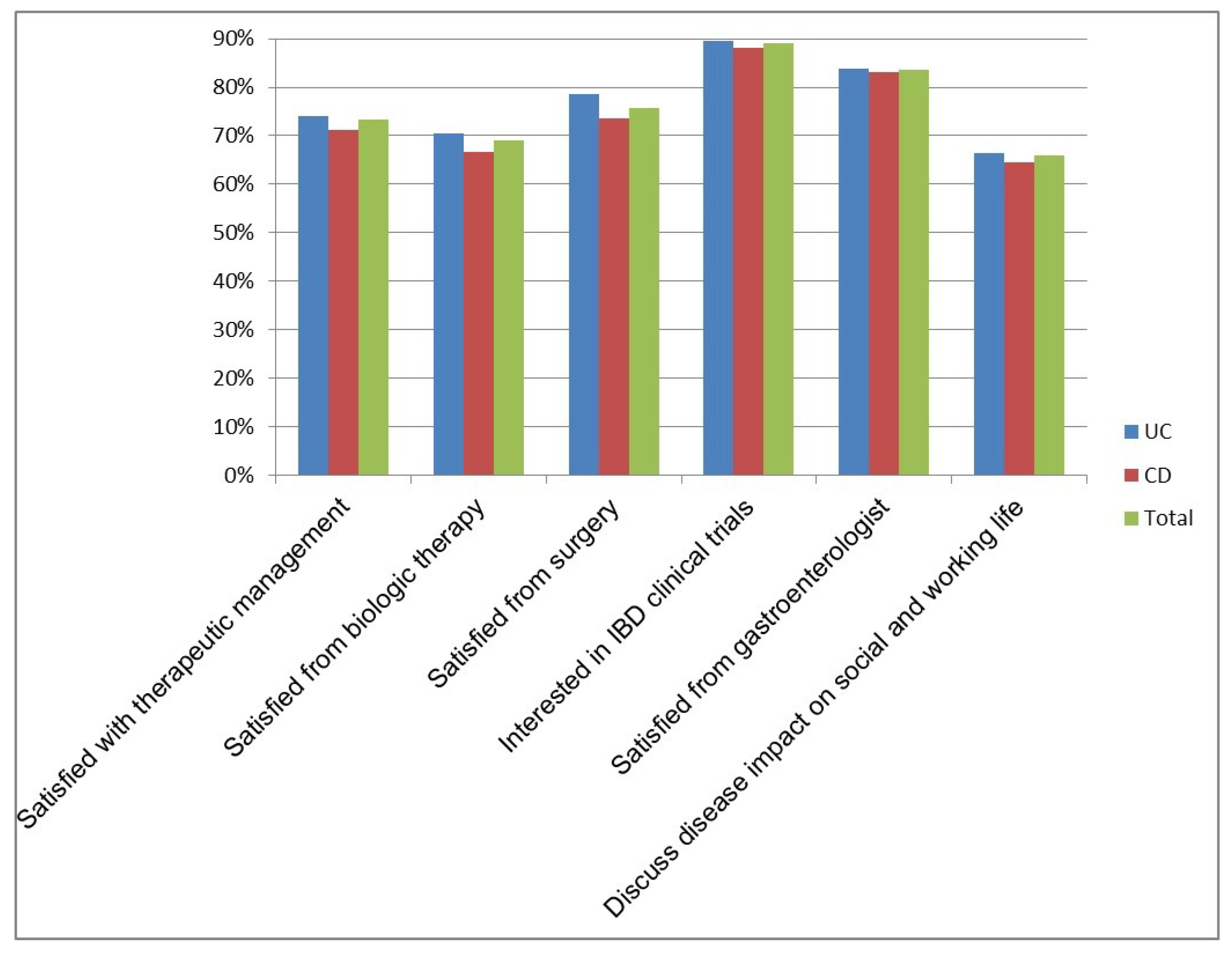
3.4. Reality of Health-Related Quality of Life and Perceived Unmet Needs
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Ng, S.C.; Shi, H.Y.; Hamidi, N.; Underwood, F.E.; Tang, W.; Benchimol, E.I.; Panaccione, R.; Ghosh, S.; Wu, J.C.Y.; Chan, F.K.L.; et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: A systematic review of population-based studies. Lancet 2017, 390, 2769–2778. [Google Scholar] [CrossRef]
- Lamb, C.A.; Kennedy, N.A.; Raine, T.; Hendy, P.A.; Smith, P.J.; Limdi, J.K.; Hayee, B.; Lomer, M.; Parkes, G.C.; Selinger, C.P.; et al. British Society of Gastroenterology consensus guidelines on the management of inflammatory bowel disease in adults. Gut 2019, 68, s1–s106. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tursi, A.; Mocci, G.; Faggiani, R.; Allegretta, L.; Della Valle, N.; Forti, G.; Franceschi, M.; Ferronato, A.; Gallina, S.; LaRussa, T.; et al. Infliximab biosimilar CT-P13 is effective and safe in treating inflammatory bowel diseases: A real-life multicenter, observational study in Italian primary inflammatory bowel disease centers. Ann. Gastroenterol. 2019, 32, 392–399. [Google Scholar] [CrossRef]
- Ishak, W.W.; Pan, D.; Steiner, A.; Feldman, E.; Danovitch, I.; Melmed, G.Y.; Mann, A.; Mirocha, J. Patient-Reported Outcomes of Quality of Life, Functioning, and GI/Psychiatric Symptom Severity in Patients with Inflammatory Bowel Disease (IBD). Inflamm. Bowel Dis. 2017, 23, 798–803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daperno, M.; Armuzzi, A.; Danese, S.; Fries, W.; Liguori, G.; Orlando, A.; Papi, C.; Principi, M.; Rizzello, F.; Viscido, A.; et al. Unmet Medical Needs in the Management of Ulcerative Colitis: Results of an Italian Delphi Consensus. Gastroenterol. Res. Pr. 2019, 2019, 3108025–3108029. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Karimi, M.; Brazier, J. Health, Health-Related Quality of Life, and Quality of Life: What is the Difference? PharmacoEconomics 2016, 34, 645–649. [Google Scholar] [CrossRef]
- Vegni, E.; Gilardi, D.; Bonovas, S.; Corrò, B.E.; Menichetti, J.; Leone, D.; Mariangela, A.; Furfaro, F.; Danese, S.; Fiorino, G. Illness Perception in Inflammatory Bowel Disease Patients is Different Between Patients With Active Disease or in Remission: A Prospective Cohort Study. J. Crohn’s Coliti 2018, 13, 417–423. [Google Scholar] [CrossRef]
- Knowles, S.R.; Keefer, L.; Wilding, H.; Hewitt, C.; Graff, L.A.; Mikocka-Walus, A. Quality of Life in Inflammatory Bowel Disease: A Systematic Review and Meta-analyses-Part II. Inflamm. Bowel Dis. 2018, 24, 966–976. [Google Scholar] [CrossRef]
- Leone, D.; Gilardi, D.; Corrò, B.E.; Menichetti, J.; Vegni, E.; Correale, C.; Mariangela, A.; Furfaro, F.; Bonovas, S.; Peyrin-Biroulet, L.; et al. Psychological Characteristics of Inflammatory Bowel Disease Patients: A Comparison Between Active and Nonactive Patients. Inflamm. Bowel Dis. 2019, 25, 1399–1407. [Google Scholar] [CrossRef]
- Fu, H.; Kaminga, A.C.; Peng, Y.; Feng, T.; Wang, T.; Wu, X.; Yang, T. Associations between disease activity, social support and health-related quality of life in patients with inflammatory bowel diseases: The mediating role of psychological symptoms. BMC Gastroenterol. 2020, 20, 1–8. [Google Scholar] [CrossRef]
- Choi, K.; Chun, J.; Han, K.; Park, S.; Soh, H.; Kim, J.; Lee, J.; Lee, H.J.; Im, J.P.; Kim, J.S. Risk of Anxiety and Depression in Patients with Inflammatory Bowel Disease: A Nationwide, Population-Based Study. J. Clin. Med. 2019, 8, 654. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Targownik, L.E.; Sexton, K.A.; Bernstein, M.T.; Beatie, B.; Sargent, M.; Walker, J.R.; Graff, L. The Relationship Among Perceived Stress, Symptoms, and Inflammation in Persons with Inflammatory Bowel Disease. Am. J. Gastroenterol. 2015, 110, 1001–1012. [Google Scholar] [CrossRef] [PubMed]
- Brooks, A.J.; Norman, P.; Peach, E.J.; Ryder, A.; Scott, A.J.; Narula, P.; Corfe, B.M.; Lobo, A.J.; Rowse, G. Prospective Study of Psychological Morbidity and Illness Perceptions in Young People with Inflammatory Bowel Disease. J. Crohns Colitis 2019, 13, 1003–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bortoli, A.; Daperno, M.; Kohn, A.; Politi, P.; Marconi, S.; Monterubbianesi, R.; Castiglione, F.; Corbellini, A.; Merli, M.; Casella, G.; et al. Patient and physician views on the quality of care in inflammatory bowel disease: Results from SOLUTION-1, a prospective IG-IBD study. J. Crohns Colitis 2014, 8, 1642–1652. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Harvey, R.; Bradshaw, J. A simple index of Crohn’s-disease activity. Lancet 1980, 315, 514. [Google Scholar] [CrossRef]
- Tursi, A.; Brandimarte, G.; Papa, A.; Giglio, A.; Elisei, W.; Giorgetti, G.M.; Forti, G.; Morini, S.; Hassan, C.; Pistoia, M.A.; et al. Treatment of Relapsing Mild-to-Moderate Ulcerative Colitis with the Probiotic VSL#3 as Adjunctive to a Standard Pharmaceutical Treatment: A Double-Blind, Randomized, Placebo-Controlled Study. Am. J. Gastroenterol. 2010, 105, 2218–2227. [Google Scholar] [CrossRef] [Green Version]
- Jowett, S.; Seal, C.; Barton, R.; Welfare, M. The Short Inflammatory Bowel Disease Questionnaire Is Reliable and Responsive To Clinically Important Change in Ulcerative Colitis. Am. J. Gastroenterol. 2001, 96, 2921–2928. [Google Scholar] [CrossRef]
- Djukanovic, I.; Carlsson, J.; Årestedt, K. Is the Hospital Anxiety and Depression Scale (HADS) a valid measure in a general population 65–80 years old? A psychometric evaluation study. Health Qual. Life Outcomes 2017, 5, 193. [Google Scholar] [CrossRef] [Green Version]
- Broadbent, E.; Petrie, K.J.; Main, J.; Weinman, J. The Brief Illness Perception Questionnaire (BIPQ). J. Psychosom. Res. 2006, 60, 631–637. [Google Scholar] [CrossRef]
- Lönnfors, S.; Vermeire, S.; Greco, M.; Hommes, D.; Bell, C.; Avedano, L. IBD and health-related quality of life — Discovering the true impact. J. Crohns Colitis 2014, 8, 1281–1286. [Google Scholar] [CrossRef] [Green Version]
- Mancina, R.M.; Pagnotta, R.; Pagliuso, C.; Albi, V.; Bruno, D.; Garieri, P.; Doldo, P.; Spagnuolo, R. Gastrointestinal Symptoms of and Psychosocial Changes in Inflammatory Bowel Disease: A Nursing-Led Cross-Sectional Study of Patients in Clinical Remission. Medicina 2020, 56, 45. [Google Scholar] [CrossRef] [Green Version]
- Jäghult, S.; Saboonchi, F.; Johansson, U.-B.; Wredling, R.; Kapraali, M. Identifying predictors of low health-related quality of life among patients with inflammatory bowel disease: Comparison between Crohn’s disease and ulcerative colitis with disease duration. J. Clin. Nurs. 2011, 20, 1578–1587. [Google Scholar] [CrossRef] [PubMed]
- Kalafateli, M.; Triantos, C.; Theocharis, G.; Giannakopoulou, D.; Koutroumpakis, E.; Chronis, A.; Sapountzis, A.; Margaritis, V.; Thomopoulos, K.; Nikolopoulou, V. Health-related quality of life in patients with inflammatory bowel disease: A single-center experience. Ann. Gastroenterol. 2013, 26, 243–248. [Google Scholar]
- Simrén, M.; Axelsson, J.; Gillberg, R.; Abrahamsson, H.; Svedlund, J.; Bjornsson, E.S. Quality of life in inflammatory bowel disease in remission: The impact of IBS-like symptoms and associated psychological factors. Am. J. Gastroenterol. 2002, 97, 389–396. [Google Scholar] [CrossRef]
- Knowles, S.R.; Graff, L.; Wilding, H.E.; Hewitt, C.; Keefer, L.; Mikocka-Walus, A. Quality of Life in Inflammatory Bowel Disease: A Systematic Review and Meta-analyses—Part I. Inflamm. Bowel Dis. 2018, 24, 742–751. [Google Scholar] [CrossRef] [PubMed]
- Burisch, J.; Weimers, P.; Pedersen, N.; Cukovic-Cavka, S.; Vucelić, B.; Kaimakliotis, I.; Duricova, D.; Bortlik, M.; Shonova, O.; Vind, I.; et al. Health-related quality of life improves during one year of medical and surgical treatment in a European population-based inception cohort of patients with Inflammatory Bowel Disease—An ECCO-EpiCom study. J. Crohn’s Colitis 2014, 8, 1030–1042. [Google Scholar] [CrossRef] [Green Version]
- Keller, R.; Mazurak, N.; Fantasia, L.; Fusco, S.; Malek, N.P.; Wehkamp, J.; Enck, P.; Klag, T. Quality of life in inflammatory bowel diseases: It is not all about the bowel. Intest. Res. 2020. [Google Scholar] [CrossRef] [Green Version]
- Williet, N.; Sarter, H.; Gower-Rousseau, C.; Adrianjafy, C.; Olympie, A.; Buisson, A.; Beaugerie, L.; Peyrin-Biroulet, L. Patient reported-outcomes in a French nationwide survey of inflammatory bowel disease patients. J. Crohns Colitis 2016, 11, 165–174. [Google Scholar] [CrossRef] [Green Version]
- Neuendorf, R.; Harding, A.; Stello, N.; Hanes, D.; Wahbeh, H. Depression and anxiety in patients with Inflammatory Bowel Disease: A systematic review. J. Psychosom. Res. 2016, 87, 70–80. [Google Scholar] [CrossRef]
- Marafini, I.; Longo, L.; Lavasani, D.M.; Rossi, A.; Salvatori, S.; Pianigiani, F.; Calabrese, E.; Siracusano, A.; Di Lorenzo, G.; Monteleone, G. High Frequency of Undiagnosed Psychiatric Disorders in Inflammatory Bowel Diseases. J. Clin. Med. 2020, 9, 1387. [Google Scholar] [CrossRef]
- Kubesch, A.; Boulahrout, P.; Filmann, N.; Blumenstein, I.; Hausmann, J. Real-world data about emotional stress, disability and need for social care in a German IBD patient cohort. PLoS ONE 2020, 15, e0227309. [Google Scholar] [CrossRef] [PubMed]
- Zhang, C.K.; Hewett, J.; Hemming, J.; Grant, T.; Zhao, H.; Abraham, C.; Oikonomou, I.; Kanakia, M.; Cho, J.H.; Proctor, D.D.; et al. The influence of depression on quality of life in patients with inflammatory bowel disease. Inflamm. Bowel Dis. 2013, 19, 1732–1739. [Google Scholar] [CrossRef] [Green Version]
- Ananthakrishnan, A.N.; Long, M.D.; Martin, C.F.; Sandler, R.S.; Kappelman, M.D. Sleep Disturbance and Risk of Active Disease in Patients With Crohn’s Disease and Ulcerative Colitis. Clin. Gastroenterol. Hepatol. 2013, 11, 965–971. [Google Scholar] [CrossRef] [Green Version]
- Mahdavi, S.B.; Habibi, F.; Habibi, M.E.; Gharavinia, A.; Akbarpour, M.J.; Baghaei, A.; Emami, M.H. Quality of life in inflammatory bowel disease patients: A cross-sectional study. J. Res. Med. Sci. 2017, 22, 104. [Google Scholar] [CrossRef] [PubMed]
- Graff, L.; Vincent, N.; Walker, J.R.; Clara, I.; Carr, R.; Ediger, J.; Miller, N.; Rogala, L.; Rawsthorne, P.; Lix, L.; et al. A population-based study of fatigue and sleep difficulties in inflammatory bowel disease. Inflamm. Bowel Dis. 2011, 17, 1882–1889. [Google Scholar] [CrossRef] [PubMed]
- McCombie, A.; Gearry, R.B.; Mulder, R.T. Coping Strategies and Psychological Outcomes of Patients with Inflammatory Bowel Disease in the First 6 Months After Diagnosis. Inflamm. Bowel Dis. 2015, 21, 1. [Google Scholar] [CrossRef]
- Stapersma, L.; Brink, G.V.D.; Van Der Ende, J.; Bodelier, A.G.; Van Wering, H.M.; Hurkmans, P.C.W.M.; Mearin, M.L.; Jong, A.E.V.D.M.; Escher, J.C.; Utens, E. Illness Perceptions and Depression Are Associated with Health-Related Quality of Life in Youth with Inflammatory Bowel Disease. Int. J. Behav. Med. 2019, 26, 415–426. [Google Scholar] [CrossRef] [Green Version]
- Bulut, E.A.; Yuzbasioglu, S. The influence of disease type and activity to sexual life and health quality in inflammatory bowel disease. Turk. J. Gastroenterol. 2018, 30, 33–39. [Google Scholar] [CrossRef]
- LaRussa, T.; Suraci, E.; Marasco, R.; Imeneo, M.; Dumitrascu, D.L.; Abenavoli, L.; Luzza, F. Barriers and Facilitators In Conducting Clinical Trials In Inflammatory Bowel Disease: A Monocentric Italian Survey. Rev. Recent Clin. Trials 2020, 15, 1. [Google Scholar] [CrossRef]
- Cioffi, I.; Imperatore, N.; Di Vincenzo, O.; Santarpia, L.; Rispo, A.; Marra, M.; Testa, A.; Contaldo, F.; Castiglione, F.; Pasanisi, F. Association between Health-Related Quality of Life and Nutritional Status in Adult Patients with Crohn’s Disease. Nutrition 2020, 12, 746. [Google Scholar] [CrossRef] [Green Version]
- Ponsioen, C.Y.; De Groof, E.J.; Eshuis, E.J.; Gardenbroek, T.J.; Bossuyt, P.M.M.; Hart, A.; Warusavitarne, J.; Buskens, C.; Van Bodegraven, A.A.; Brink, M.A.; et al. Laparoscopic ileocaecal resection versus infliximab for terminal ileitis in Crohn’s disease: A randomised controlled, open-label, multicentre trial. Lancet Gastroenterol. Hepatol. 2017, 2, 785–792. [Google Scholar] [CrossRef]
- Calvert, M.; Blazeby, J.; Altman, D.G.; Revicki, D.A.; Moher, D.; Brundage, M.D.; CONSORT PRO Group. Reporting of Patient-Reported Outcomes in Randomized Trials. JAMA 2013, 309, 814–822. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Daperno, M.; Bortoli, A.; Kohn, A.; Politi, P.; Marconi, S.; Ardizzone, S.; Cortelezzi, C.C.; Grasso, G.; Ferraris, L.; Milla, M.; et al. Patient and physician views on the quality of care for inflammatory bowel disease after one-year follow-up: Results from SOLUTION-2, a prospective IG-IBD study. Dig. Liver Dis. 2017, 49, 997–1002. [Google Scholar] [CrossRef] [PubMed]
- Danese, S.; Allez, M.; Van Bodegraven, A.A.; Dotan, I.; Gisbert, J.P.; Hart, A.; Lakatos, P.L.; Magro, F.; Peyrin-Biroulet, L.; Schreiber, S.; et al. Unmet Medical Needs in Ulcerative Colitis: An Expert Group Consensus. Dig. Dis. 2019, 37, 266–283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Calixto, R.P.; Flores, C.; Francesconi, C.F. Inflammatory bowel disease: Impact on scores of quality of life, depression and anxiety in patients attending a tertiary care center in Brazil. Arq. Gastroenterol. 2018, 55, 202–207. [Google Scholar] [CrossRef] [PubMed]
- Jordan, C.D.; Ohlsen, R.; Hayee, B.; Chalder, T. A qualitative study exploring the experience of people with IBD and elevated symptoms of anxiety and low mood and the type of psychological help they would like. Psychol. Health 2017, 33, 634–651. [Google Scholar] [CrossRef]
- Ghosh, S.; Mitchell, R. Impact of inflammatory bowel disease on quality of life: Results of the European Federation of Crohn’s and Ulcerative Colitis Associations (EFCCA) patient survey. J. Crohns Colitis 2007, 1, 10–20. [Google Scholar] [CrossRef] [Green Version]
- Parra, R.S.; Chebli, J.M.F.; Amarante, H.M.B.S.; Flores, C.; Parente, J.M.L.; Ramos, O.; Fernandes, M.; Rocha, J.J.R.; Feitosa, M.R.; Feres, O.; et al. Quality of life, work productivity impairment and healthcare resources in inflammatory bowel diseases in Brazil. World J. Gastroenterol. 2019, 25, 5862–5882. [Google Scholar] [CrossRef]
- Aniwan, S.; Bruining, D.H.; Park, S.H.; Al-Bawardy, B.; Kane, S.V.; Prabhu, N.C.; Kisiel, J.B.; Raffals, L.E.; Papadakis, K.A.; Pardi, D.S.; et al. The Combination of Patient-Reported Clinical Symptoms and an Endoscopic Score Correlates Well with Health-Related Quality of Life in Patients with Ulcerative Colitis. J. Clin. Med. 2019, 8, 1171. [Google Scholar] [CrossRef] [Green Version]
- Allegretti, J.R.; Cole, E.B.; Korzenik, J.R. Barriers to enrollment in inflammatory bowel disease randomized controlled trials: An investigation of patient perspectives. Inflamm. Bowel Dis. 2012, 18, 2092–2098. [Google Scholar] [CrossRef]
- Coenen, S.; Haeck, M.; Ferrante, M.; Noman, M.; Van Assche, G.; Vermeire, S. Quality of care in an inflammatory bowel disease clinical trial center: A prospective study evaluating patients’ satisfaction. Acta Gastroenterol. Belg. 2020, 83, 25–31. [Google Scholar] [PubMed]
- Elkjaer, M.; Moser, G.; Reinisch, W.; Durovicova, D.; Lukáš, M.; Vucelic, B.; Wewer, V.; Colombel, J.F.; Shuhaibar, M.; O’Morain, C.; et al. IBD patients need in health quality of care ECCO consensus. J. Crohns Colitis 2008, 2, 181–188. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Der Eijk, I.; Vlachonikolis, I.G.; Munkholm, P.; Nijman, J.; Bernklev, T.; Politi, P.L.; Odes, S.; Tsianos, E.V.; Stockbrügger, R.W.; Russel, M.G. The Role of Quality of Care in Health-related Quality of Life in Patients with IBD. Inflamm. Bowel Dis. 2004, 10, 392–398. [Google Scholar] [CrossRef] [PubMed]
- Matthiasson, S.E.; Panes, J.; Louis, E.; Holley, D.; Buch, M.; Paridaens, K. National differences in ulcerative colitis experience and management among patients from five European countries and Canada: An online survey. J. Crohns Colitis 2013, 7. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variable | CD n = 59 | UC n = 143 | Overall n = 202 |
|---|---|---|---|
| Gender, n (%) | |||
| Female | 25 (42) | 67 (47) | 92 (46) |
| Male | 34 (58) | 76 (53) | 110 (54) |
| Age, median (range), years | 47 (19–80) | 50 (17–82) | 48 (17–82) |
| Pediatric onset, n (%) * | 10 (23) | 15 (14) | 25 (17) |
| BMI, mean ± SD, kg/m2 | 23 ± 2 | 24 ± 3 | 24 ± 3 |
| BMI > 24.9, n (%) | 12 (28) | 42 (39) | 54 (36) |
| Smoking, n (%) | 13 (26) | 38 (25) | 51 (25) |
| Marriage/cohabiting, n (%) | 25 (50) | 77 (51) | 102 (51) |
| High education, n (%) | 36 (83) | 80 (75) | 116 (77) |
| IBD surgery, n (%) ** | 19 (38) | 17 (11) | 36 (18) |
| Disease duration, mean ± SD, years | 13 ± 11 | 15 ± 10 | 14 ± 11 |
| Steroid-dependance, n (%) | 21 (42) | 54 (35) | 75 (37) |
| Biologic experienced, n (%) *** | 25 (50) | 45 (30) | 70 (35) |
| Variable | Low HRQoL n = 106 | Normal HRQoL n = 96 | p-Value | OR (95% CI) Adjusted a | p-Value (MVA) |
|---|---|---|---|---|---|
| Gender, n (%) Female Male | 51 (48.1) 55 (51.9) | 41 (42.7) 55 (57.3) | 0.441 | 0.641(0.319–1.286) | 0.210 |
| Age, median (range), years | 47 (17–82) | 43 (17–74) | 0.299 | 0.977 (0.947–1.007) | 0.128 |
| Type of disease, n (%) UC CD | 76 (53.2) 30 (50.8) | 67 (46.8) 29 (49.2) | 0.566 | 2.449 (1.057–5.675) | 0.037 |
| Pediatric onset, n (%) | 18 (17) | 7 (7.3) | 0.038 | 0.380 (0.115–1.251) | 0.111 |
| Family history of IBD, n (%) | 18 (20.5) | 13 (18.1) | 0.702 | 1.314 (0.734–3.103) | 0.672 |
| Overweight, n (%) | 41 (38.7) | 39 (40.6) | 0.778 | 1.169 (0.568–2.407) | 0.818 |
| Smoking, n (%) | 26 (24.5) | 25 (26) | 0.805 | 1.269 (0.560–2.875) | 0.568 |
| High education, n (%) | 59 (55.7) | 59 (61.5) | 0.404 | 1.114 (0.527–2.356) | 0.777 |
| Marriage/cohabiting, n (%) | 59 (55.7) | 43 (44.8) | 0.123 | 0.701 (0.309–1.593) | 0.397 |
| IBD surgery, n (%) | 25 (23.6) | 12 (12.5) | 0.042 | 3.533 (1.218–10.204) | 0.021 |
| Disease duration, mean ± SD, years | 15.42 ± 11.3 | 13.23 ± 8.4 | 0.142 | 2.974 (1.304–6.781) | 0.010 |
| Steroid-dependence, n (%) | 44 (41.5) | 31 (32.3) | 0.176 | 0.932 (0.443–1.960) | 0.852 |
| Biologic experienced, n (%) | 43 (40.6) | 27 (28.1) | 0.064 | 0.658 (0.292–1.482) | 0.312 |
| Poor sleep quality, n (%) | 52 (49.1) | 19 (19.9) | 0.001 | 2.609 (1.211–0.618) | 0.014 |
| Illness perception score, mean ± SD | 48.08 ± 11.5 | 37.13 ± 15 | 0.001 | 1.039 (1.011–1.067) | 0.006 |
| Anxiety/depression status, n (%) | 65 (61.3) | 27 (28.1) | 0.001 | 2.145 (1.028–4.464) | 0.042 |
| Variable | Impact on Work n = 126 | No Impact on Work n = 76 | p-Value |
|---|---|---|---|
| Gender, n (%) Female Male | 66 (52) 60 (48) | 26 (34) 50 (66) | 0.012 |
| Age, median (range), years | 45 (17–82) | 45 (17–80) | 0.649 |
| Type of disease, n (%) UC CD | 92 (73) 34 (27) | 51 (67) 25 (33) | 0.371 |
| Variable | Impact on Social Activities n = 149 | No Impact on Social Activities n = 53 | p-Value |
|---|---|---|---|
| Gender, n (%) Female Male | 71 (48) 78 (52) | 21 (40) 32 (60) | 0.313 |
| Age, median (range), years | 43 (17–82) | 52 (26–81) | 0.07 |
| Type of disease, n (%) UC CD | 104 (70) 45 (30) | 39 (74) 14 (26) | 0.603 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Larussa, T.; Flauti, D.; Abenavoli, L.; Boccuto, L.; Suraci, E.; Marasco, R.; Imeneo, M.; Luzza, F. The Reality of Patient-Reported Outcomes of Health-Related Quality of Life in an Italian Cohort of Patients with Inflammatory Bowel Disease: Results from a Cross-Sectional Study. J. Clin. Med. 2020, 9, 2416. https://doi.org/10.3390/jcm9082416
Larussa T, Flauti D, Abenavoli L, Boccuto L, Suraci E, Marasco R, Imeneo M, Luzza F. The Reality of Patient-Reported Outcomes of Health-Related Quality of Life in an Italian Cohort of Patients with Inflammatory Bowel Disease: Results from a Cross-Sectional Study. Journal of Clinical Medicine. 2020; 9(8):2416. https://doi.org/10.3390/jcm9082416
Chicago/Turabian StyleLarussa, Tiziana, Danilo Flauti, Ludovico Abenavoli, Luigi Boccuto, Evelina Suraci, Raffaella Marasco, Maria Imeneo, and Francesco Luzza. 2020. "The Reality of Patient-Reported Outcomes of Health-Related Quality of Life in an Italian Cohort of Patients with Inflammatory Bowel Disease: Results from a Cross-Sectional Study" Journal of Clinical Medicine 9, no. 8: 2416. https://doi.org/10.3390/jcm9082416