High Intensity Training to Treat Chronic Nonspecific Low Back Pain: Effectiveness of Various Exercise Modes

 , , ,
, , ,
Abstract
:1. Introduction
2. Materials and methods
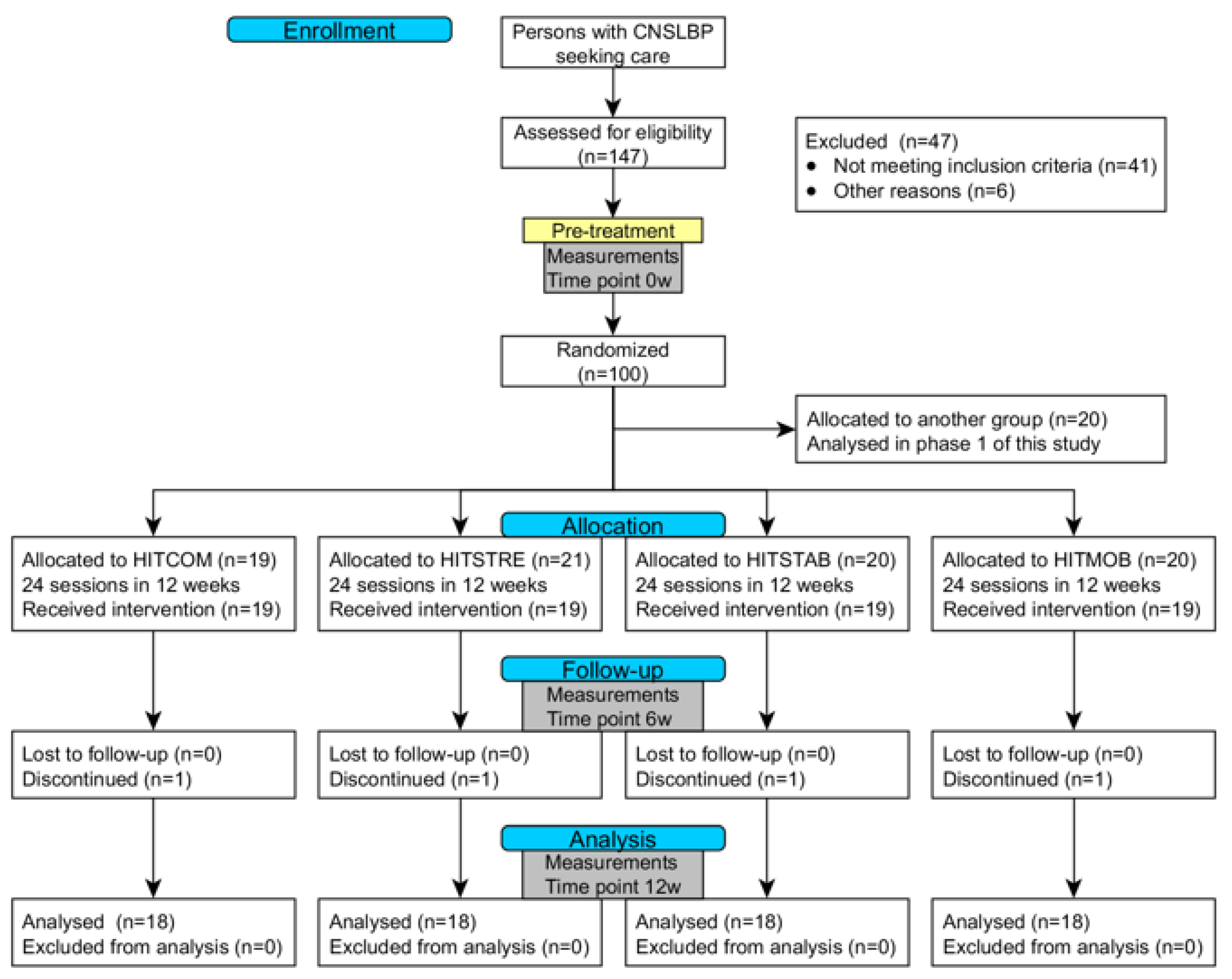
2.1. Trial Design
2.2. Participants and Recruitment
2.3. Randomization and Blinding
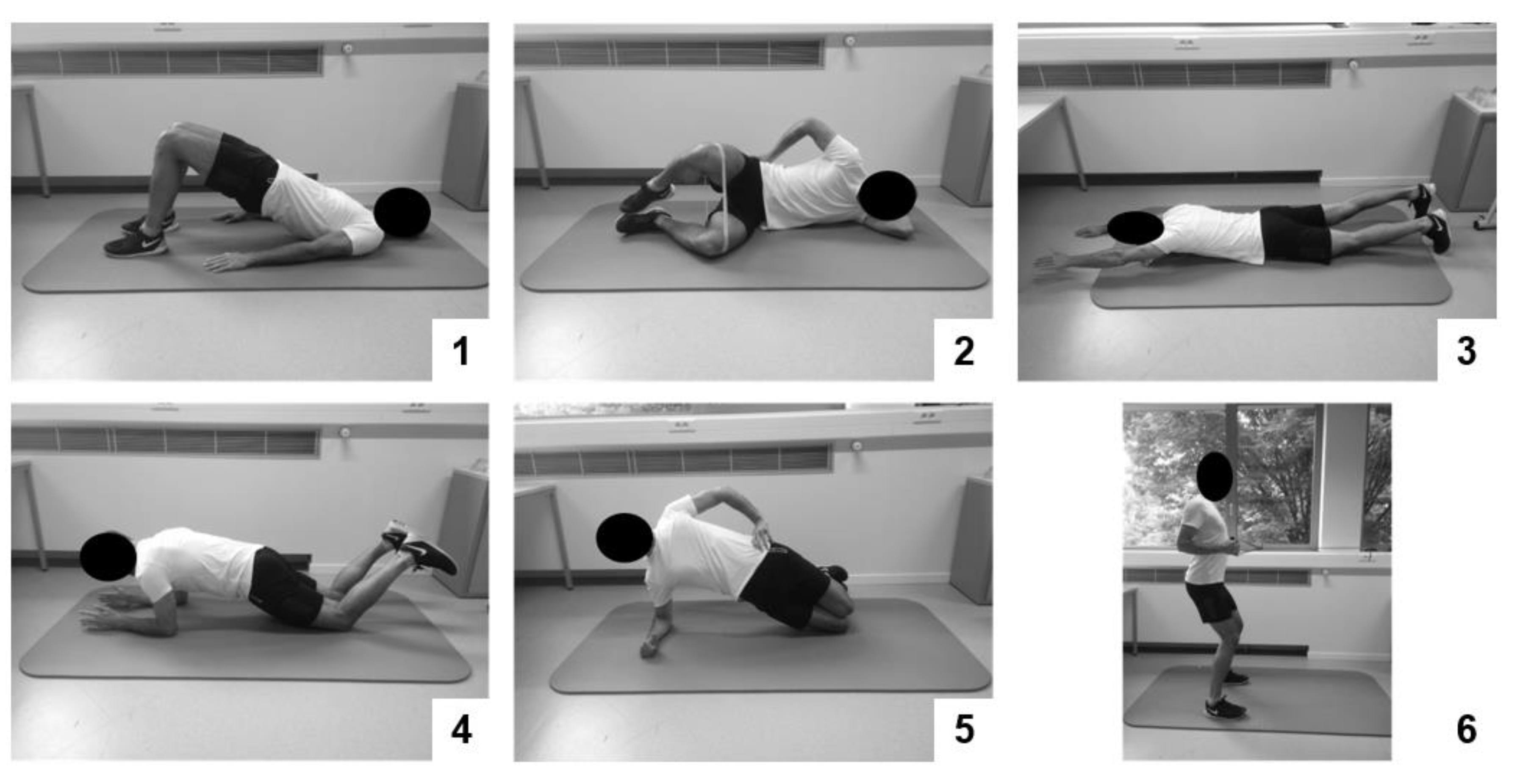
2.4. Interventions
2.5. Testing Procedure and Outcomes
2.6. Data Analysis
3. Results
3.1. Recruitment and Baseline Data
3.2. Treatment Adherence, Dropouts, and Adverse Events
3.3. Outcomes after the Training Program
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Hoy, D.; March, L.; Brooks, P.; Blyth, F.; Woolf, A.; Bain, C.; Williams, G.; Smith, E.; Vos, T.; Barendregt, J.; et al. The global burden of low back pain: Estimates from the Global Burden of Disease 2010 study. Ann. Rheum. Dis. 2014, 73, 968–974. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Palazzo, C.; Ravaud, J.; Papelard, A.; Ravaud, P.; Poiraudeau, S. The burden of musculoskeletal conditions. PLoS ONE 2014, 9, e90633. [Google Scholar] [CrossRef]
- Airaksinen, O.; Brox, J.I.; Cedraschi, C.; Hildebrandt, J.; Klaber-Moffett, J.; Kovacs, F.; Mannion, A.F.; Reis, S.; Staal, J.B.; Ursin, H. Chapter 4. European guidelines for the management of chronic nonspecific low back pain. Eur. Spine J. 2006, 15, S192–S300. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holtermann, A.; Clausen, T.; Jorgensen, M.B.; Mork, P.J.; Andersen, L.L. Should physical activity recommendation depend on state of low back pain? Eur. J. Pain 2014, 18, 575–581. [Google Scholar] [CrossRef]
- Meucci, R.D.; Fassa, A.G.; Faria, N.M.X. Prevalence of chronic low back pain: Systematic review. Revista Saude Publica 2015, 49, 73. [Google Scholar] [CrossRef] [PubMed]
- Vos, T.; Flaxman, A.D.; Naghavi, M.; Lozano, R.; Michaud, C.; Ezzati, M.; Shibuya, K.; Salomon, J.A.; Abdalla, S.; Aboyans, V.; et al. Years lived with disability (YLDs) for 1160 sequelae of 289 diseases and injuries 1990–2010: A systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012, 380, 2163–2196. [Google Scholar] [CrossRef]
- Dagenais, S.; Caro, J.; Haldeman, S. A systematic review of low back pain cost of illness studies in the United States and internationally. Spine J. 2008, 8, 8–20. [Google Scholar] [CrossRef]
- Gore, M.; Sadosky, A.; Stacey, B.R.; Tai, K.; Leslie, D. The burden of chronic low back pain: Clinical comorbidities, treatment patterns, and health care costs in usual care settings. Spine 2012, 37, E668–E677. [Google Scholar] [CrossRef] [Green Version]
- Rossignol, M.; Poitras, S.; Dionne, C.; Tousignant, M.; Truchon, M.; Arsenault, B.; Allard, P.; Coté, M.; Neveu, A. An interdisciplinary guideline development process: The Clinic on Low-back pain in Interdisciplinary Practice (CLIP) low-back pain guidelines. Implement. Sci. 2007, 2, 36. [Google Scholar] [CrossRef] [Green Version]
- Koes, B.W.; van Tulder, M.; Lin, C.-C.; Macedo, L.G.; McAuley, J.; Maher, C. An updated overview of clinical guidelines for the management of non-specific low back pain in primary care. Eur. Spine J. 2010, 19, 2075–2094. [Google Scholar] [CrossRef] [Green Version]
- Oliveira, C.B.; Maher, C.G.; Pinto, R.Z.; Traeger, A.C.; Lin, C.-C.; Chenot, J.; van Tulder, M.; Koes, B.W. Clinical practice guidelines for the management of non-specific low back pain in primary care: An updated overview. Eur. Spine J. 2018, 27, 2791–2803. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hayden, J.A.; van Tulder, M.W.; Tomlinson, G. Systematic review: Strategies for using exercise therapy to improve outcomes in chronic low back pain. Ann. Intern. Med. 2005, 142, 776–785. [Google Scholar] [CrossRef] [PubMed]
- Owen, P.J.; Miller, C.T.; Mundell, N.L.; Verswijveren, S.J.; Tagliaferri, S.D.; Brisby, H.; Bowe, S.J.; Belavy, D.L. Which specific modes of exercise training are most effective for treating low back pain? Network meta-analysis. Br. J. Sports Med. 2019. Epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Wewege, M.A.; Booth, J.; Parmenter, B.J. Aerobic vs. resistance exercise for chronic non-specific low back pain: A systematic review and meta-analysis. J. Back Musculoskelet. Rehabil. 2018, 31, 889–899. [Google Scholar] [CrossRef]
- Searle, A.; Spink, M.; Ho, A.; Chuter, V. Exercise interventions for the treatment of chronic low back pain: A systematic review and meta-analysis of randomised controlled trials. Clin. Rehabil. 2015, 29, 1155–1167. [Google Scholar] [CrossRef]
- Van Middelkoop, M.; Rubinstein, S.M.; Verhagen, A.P.; Ostelo, R.W.; Koes, B.W.; van Tulder, M.W.W. Exercise therapy for chronic nonspecific low-back pain. Best. Pract. Res. Clin. Rheumatol. 2010, 24, 193–204. [CrossRef]
- Coury, H.J.; Moreira, R.F.; Dias, N.B. Evaluation of the effectiveness of workplace exercise in controlling neck, shoulder and low back pain: A systematic review. Braz. J. Phys. Ther. 2009, 13, 461–479. [Google Scholar] [CrossRef] [Green Version]
- Sveaas, S.H.; Bilberg, A.; Berg, I.J.; Provan, S.A.; Rollefstad, S.; Semb, A.G.; Hagen, K.B.; Johansen, M.W.; Pedersen, E.; Dagfinrud, H. High intensity exercise for 3 months reduces disease activity in axial spondyloarthritis (axSpA): A multicentre randomised trial of 100 patients. Brit. J. Sports Med. 2019, 54, 292–297. [Google Scholar] [CrossRef]
- Farup, J.; Dalgas, U.; Keytsman, C.; Eijnde, B.O.; Wens, I. High Intensity Training May Reverse the Fiber Type Specific Decline in Myogenic Stem Cells in Multiple Sclerosis Patients. Front. Physiol. 2016, 7, 193. [Google Scholar] [CrossRef] [Green Version]
- Guiraud, T.; Nigam, A.; Gremeaux, V.; Meyer, P.; Juneau, M.; Bosquet, L. High-intensity interval training in cardiac rehabilitation. Sports Med. 2012, 42, 587–605. [Google Scholar] [CrossRef]
- Gloeckl, R.; Marinov, B.; Pitta, F. Practical recommendations for exercise training in patients with COPD. Eur. Respir. Rev. 2013, 22, 178–186. [Google Scholar] [CrossRef] [PubMed]
- Weston, K.S.; Wisløff, U.; Coombes, J.S. High-intensity interval training in patients with lifestyle-induced cardiometabolic disease: A systematic review and meta-analysis. Brit. J. Sports Med. 2014, 48, 1227–1234. [Google Scholar] [CrossRef] [PubMed]
- Gibala, M.J.; Little, J.P.; MacDonald, M.J.; Hawley, J.A. Physiological adaptations to low-volume, high-intensity interval training in health and disease. J. Physiol. 2012, 590, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Verbunt, J.A.; Smeets, R.J.; Wittink, H.M. Cause or effect? Deconditioning and chronic low back pain. Pain 2010, 149, 428–430. [Google Scholar] [CrossRef] [PubMed]
- Kankaanpää, M.; Taimela, S.; Laaksonen, D.; Hänninen, O.; Airaksinen, O. Back and hip extensor fatigability in chronic low back pain patients and controls. Arch. Phys. Med. Rehabil. 1998, 79, 412–417. [Google Scholar] [CrossRef]
- Steele, J.; Bruce-Low, S.; Smith, D. A reappraisal of the deconditioning hypothesis in low back pain: Review of evidence from a triumvirate of research methods on specific lumbar extensor deconditioning. Curr. Med Res. Opin. 2014, 30, 865–911. [Google Scholar] [CrossRef]
- Kraemer, W.J.; Patton, J.F.; Gordon, S.E.; Harman, E.A.; Deschenes, M.R.; Reynolds, K.; Newton, R.U.; Triplett, N.T.; Dziados, J.E. Compatibility of high-intensity strength and endurance training on hormonal and skeletal muscle adaptations. J. Appl. Physiol. 1995, 78, 976–989. [Google Scholar] [CrossRef]
- Verbrugghe, J.; Agten, A.; Stevens, S.; Hansen, D.; Demoulin, C.; Eijnde, B.O.; Vandenabeele, F.; Timmermans, A. Exercise Intensity Matters in Chronic Nonspecific Low Back Pain Rehabilitation. MSSE 2019, 51, 2434–2442. [Google Scholar] [CrossRef]
- Balagué, F.; Mannion, A.F.; Pellisé, F.; Cedraschi, C. Non-specific low back pain. Lancet 2012, 379, 482–491. [Google Scholar] [CrossRef] [Green Version]
- Digiovine, N.M.; Jobe, F.W.; Pink, M.; Perry, J. An electromyographic analysis of the upper extremity in pitching. J. Shoulder Elb. Surg. 1992, 1, 15–25. [Google Scholar] [CrossRef]
- Swinkels-Meewisse, E.; Swinkels, R.; Verbeek, A.; Vlaeyen, J.; Oostendorp, R. Psychometric properties of the Tampa Scale for kinesiophobia and the fear-avoidance beliefs questionnaire in acute low back pain. Man. Ther. 2003, 8, 29–36. [Google Scholar] [CrossRef] [PubMed]
- Washburn, R.A.; Zhu, W.; McAuley, E.; Frogley, M.; Figoni, S.F. The physical activity scale for individuals with physical disabilities: Development and evaluation. Arch. Phys. Med. Rehab. 2002, 83, 193–200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fairbank, J.C.; Pynsent, P.B. The Oswestry disability index. Spine 2000, 25, 2940–2953. [Google Scholar] [CrossRef] [PubMed]
- Horn, K.K.; Jennings, S.; Richardson, G.; van Vliet, D.; Hefford, C.; Abbott, J.H. The patient-specific functional scale: Psychometrics, clinimetrics, and application as a clinical outcome measure. JOSPT 2012, 42, 30-D17. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual analog scale for pain (vas pain), numeric rating scale for pain (nrs pain), mcgill pain questionnaire (mpq), short-form mcgill pain questionnaire (sf-mpq), chronic pain grade scale (cpgs), short form-36 bodily pain scale (sf-36 bps), and measure of intermittent and constant osteoarthritis pain (icoap). Arthrit. Care Res. 2011, 63, S240–S252. [Google Scholar]
- Biodex Medical Systems Inc. Dual Position Back Ex/Flex Attachment Operation Manual; Shirley: New York, NY, USA, 2020. [Google Scholar]
- Verbrugghe, J.; Agten, A.; Eijnde, B.O.; Vandenabeele, F.; de Baets, L.; Huybrechts, X.; Timmermans, A. Reliability and Agreement of Isometric Functional Trunk and Isolated Lumbar Strength Assessment In Healthy Persons And Persons With Chronic Nonspecific Low Back Pain. Phys. Ther. Sports 2019, 38, 1–7. [Google Scholar] [CrossRef]
- Verbrugghe, J.; Agten, A.; Oe, B.; Olivieri, E.; Huybrechts, X.; Seelen, H.; Vandenabeele, F.; Timmermans, A. Feasibility of high intensity training in nonspecific chronic low back pain: A clinical trial. J. Back Musculoskelet 2018, 31, 657–666. [Google Scholar] [CrossRef] [Green Version]
- Portney, L.G.; Watkins, M.P. Foundations of Clinical Research: Applications to Practice; Pearson/Prentice Hall: Upper Saddle River, NJ, USA, 2009. [Google Scholar]
- Ostelo, R.W.; Deyo, R.A.; Stratford, P.; Waddell, G.; Croft, P.; von Korff, M.; Bouter, L.M.; de Vet, H.C. Interpreting change scores for pain and functional status in low back pain: Towards international consensus regarding minimal important change. Spine 2008, 33, 90–94. [Google Scholar] [CrossRef] [Green Version]
- Stratford, P.; Gill, C.; Westaway, M.; Binkley, J. Assessing disability and change on individual patients: A report of a patient specific measure. Physiother. Can. 1995, 47, 258–263. [Google Scholar] [CrossRef]
- Myers, J.; Prakash, M.; Froelicher, V.; Do, D.; Partington, S.; Atwood, J.E. Exercise capacity and mortality among men referred for exercise testing. N. Engl. J. Med. 2002, 346, 793–801. [Google Scholar] [CrossRef]
- Smith, B.E.; Littlewood, C.; May, S. An update of stabilisation exercises for low back pain: A systematic review with meta-analysis. BMC Musculoskel Disord 2014, 15, 416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Meng, X.-G.; Yue, S.-W. Efficacy of aerobic exercise for treatment of chronic Low back pain: A meta-analysis. Am. J. Phys. Med. Rehab. 2015, 94, 358–365. [Google Scholar] [CrossRef] [PubMed]
- Steiger, F.; Wirth, B.; de Bruin, E.D.; Mannion, A.F. Is a positive clinical outcome after exercise therapy for chronic non-specific low back pain contingent upon a corresponding improvement in the targeted aspect(s) of performance? A systematic review. Eur. Spine J. 2012, 21, 575–598. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Roussel, N.A.; Nijs, J.; Meeus, M.; Mylius, V.; Fayt, C.; Oostendorp, R. Central sensitization and altered central pain processing in chronic low back pain: Fact or myth? Clin. J. Pain. 2013, 29, 625–638. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Booth, J.; Moseley, G.L.; Schiltenwolf, M.; Cashin, A.; Davies, M.; Hübscher, M. Exercise for chronic musculoskeletal pain: A biopsychosocial approach. Musculoskelet. Care 2017, 15, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Hartvigsen, J.; Hancock, M.J.; Kongsted, A.; Louw, Q.; Ferreira, M.L.; Genevay, S.; Hoy, D.; Karppinen, J.; Pransky, G.; Sieper, J.; et al. What low back pain is and why we need to pay attention. Lancet 2018, 391, 2356–2367. [Google Scholar] [CrossRef] [Green Version]




{kind=link}
{kind=link}
{kind=link}
| Variables | HITCOM (n = 19) | HITSTRE (n = 21) | HITSTAB (n = 20) | HITMOB (n = 20) | p-Value |
|---|---|---|---|---|---|
| Gender (m/f) | 6/13 | 8/13 | 8/12 | 12/8 | |
| Age (years) | 44.9 (8.6) | 46.4 (9.5) | 42.0 (10.9) | 42.7 (9.3) | 0.162 |
| Symptom duration (years) | 14.3 (8.3) | 15.0 (8.8) | 8.8 (6.0) | 15.8 (11.1) | 0.001 |
| BMI (kg/m2) | 25.4 (4.0) | 25.4 (4.1) | 23.7 (3.4) | 25.1 (2.3) | 0.232 |
| Physical activity (PASIPD) | 15.7 (10.4) | 14.2 (10.9) | 16.5 (12.7) | 17.8 (12.2) | 0.891 |
| Kinesiophobia (TSK) | 32.0 (6.0) | 34.3 (5.4) | 33.1 (5.4) | 36.6 (6.4) | 0.131 |
| HITCOM (n = 18) | HITSTRE (n = 19) | HITSTAB (n = 20) | HITMOB (n = 17) | Interaction | ||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Variables | PRE | POST | Δ | PRE | POST | Δ | PRE | POST | Δ | PRE | POST | Δ | p-Value | CI |
| Pain intensity | 5.7 | 2.5 | −3.2 * | 5.1 | 3.1 | −2.0 * | 5.9 | 2.8 | −3.2 * | 6.0 | 2.5 | −3.4 * | 0.176 | (3.9;4.5) |
| NPRS, 0–10 | (1.3) | (1.2) | (1.5) | (1.9) | (1.8) | (1.9) | (1.3) | (2.1) | (2.3) | (1.4) | (1.5) | (2.0) | ||
| Disability | 22.8 | 7.8 | −14.6 * | 20.0 | 14.6 | −5.4 * | 22.0 | 12.4 | −9.6 * | 21.6 | 12.2 | −9.6 * | 0.107 | (7.4;9.1) |
| MODI, % | (9.4) | (5.6) | (8.0) | (10.2) | (10.0) | (10.6) | (11.2) | (4.8) | (12.2) | (9.4) | (8.0) | (7.4) | ||
| Functioning | 44 | 70 | 26 * | 42 | 64 | 21 * | 48 | 64 | 18 * | 36 | 66 | 32 * | 0.334 | (51;58) |
| PSFS, % | (17) | (15) | (20) | (17) | (18) | (18) | (18) | (14) | (19) | (16) | (21) | (25) | ||
| Exercise capacity | 31.2 | 36.1 | 4.4 * | 33.1 | 36.3 | 3.2 * | 34.9 | 37.3 | 2.4 * | 33.3 | 36.4 | 3.0 * | 0.191 | (33.0;36.9) |
| VO2max, mL/kg/min | (9.3) | (8.0) | (3.5) | (10.6) | (11.1) | (4.2) | (4.7) | (4.5) | (3.4) | (8.4) | (9.4) | (3.6) | ||
| Exercise capacity | 14.3 | 17.0 | 2.5 * | 14.6 | 16.1 | 1.6 * | 14.6 | 16.8 | 2.2 * | 14.1 | 16.2 | 2.2 * | 0.193 | (14.8;16.2) |
| Cycling time, min | (3.8) | (3.5) | (1.0) | (3.8) | (3.1) | (1.6) | (2.5) | (2.2) | (1.1) | (2.8) | (3.0) | (1.0) | ||
| Muscle strength | 1.40 | 1.45 | 0.04 | 1.33 | 1.28 | −0.05 | 1.49 | 1.59 | 0.09 | 1.42 | 1.58 | 0.17 * | 0.218 | (1.38;1.52) |
| Abdominal, Nm/kg | (0.29) | (0.28) | (0.18) | (0.36) | (0.44) | (0.53) | (0.27) | (0.25) | (0.19) | (0.43) | (0.43) | (0.12) | ||
| Muscle strength | 3.10 (0.84) | 3.49 | 0.31 * | 3.06 | 3.16 | 0.11 | 3.36 | 3.44 | 0.08 | 3.02 | 3.06 | 0.04 | 0.527 | (3.03;3.42) |
| Back, Nm/kg | (0.73) | (0.45) | (1.10) | (0.91) | (0.59) | (0.70) | (0.70) | (0.47) | (1.14) | (0.92) | (0.45) | |||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Verbrugghe, J.; Agten, A.; Stevens, S.; Hansen, D.; Demoulin, C.; Eijnde, B.O.; Vandenabeele, F.; Timmermans, A. High Intensity Training to Treat Chronic Nonspecific Low Back Pain: Effectiveness of Various Exercise Modes. J. Clin. Med. 2020, 9, 2401. https://doi.org/10.3390/jcm9082401
Verbrugghe J, Agten A, Stevens S, Hansen D, Demoulin C, Eijnde BO, Vandenabeele F, Timmermans A. High Intensity Training to Treat Chronic Nonspecific Low Back Pain: Effectiveness of Various Exercise Modes. Journal of Clinical Medicine. 2020; 9(8):2401. https://doi.org/10.3390/jcm9082401
Chicago/Turabian StyleVerbrugghe, Jonas, Anouk Agten, Sjoerd Stevens, Dominique Hansen, Christophe Demoulin, Bert O. Eijnde, Frank Vandenabeele, and Annick Timmermans. 2020. "High Intensity Training to Treat Chronic Nonspecific Low Back Pain: Effectiveness of Various Exercise Modes" Journal of Clinical Medicine 9, no. 8: 2401. https://doi.org/10.3390/jcm9082401