Does ADHD Symptomatology Influence Treatment Outcome and Dropout Risk in Eating Disorders? A longitudinal Study

 ,
,  , and
, and 
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Assessment
2.3. Treatment
2.4. Follow-Up
2.5. Ethics
2.6. Statistical Analyses
3. Results
3.1. Characteristics of the Sample
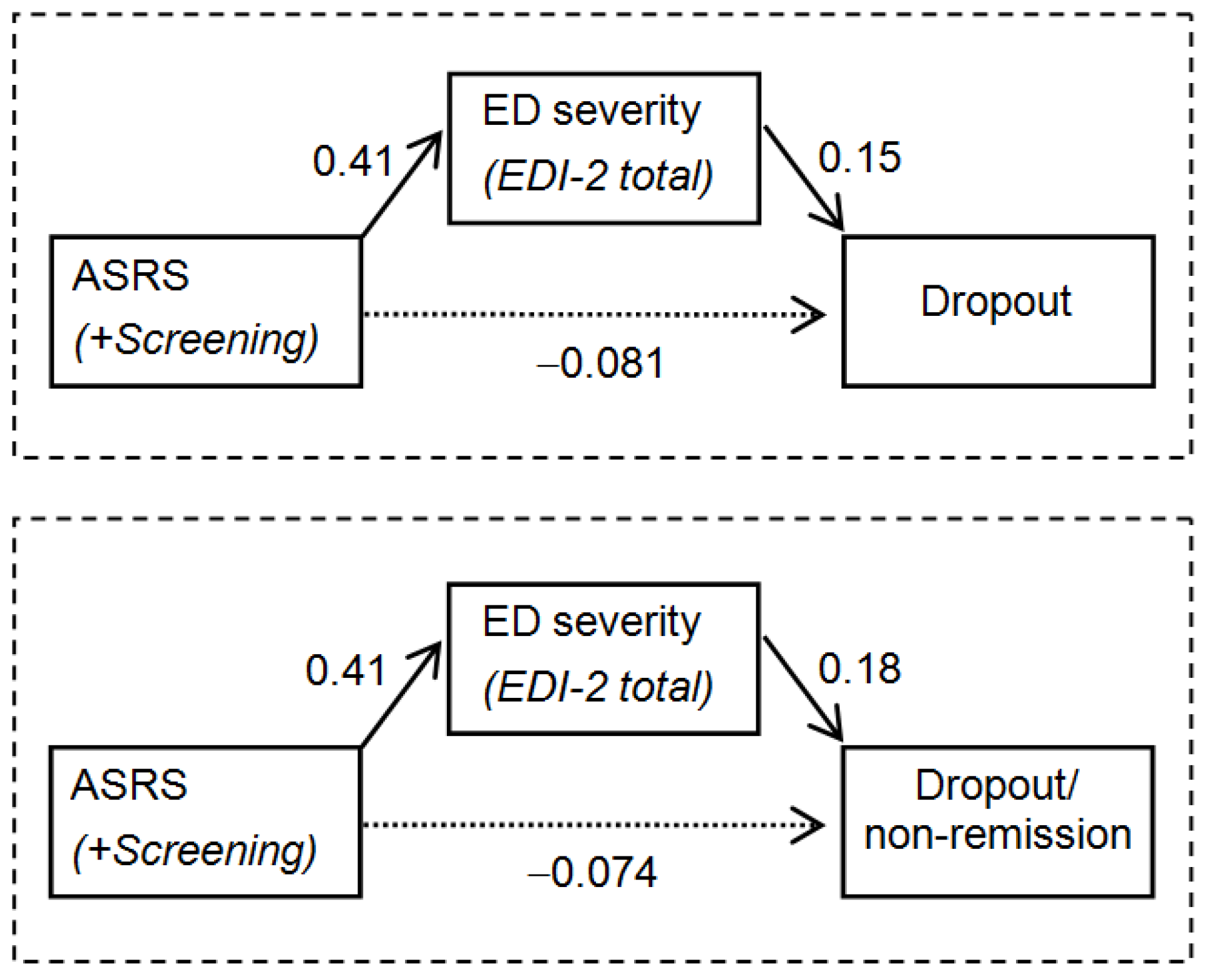
3.2. Path Analysis
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Bleck, J.; DeBate, R.D. Exploring the co-morbidity of attention-deficit/hyperactivity disorder with eating disorders and disordered eating behaviors in a nationally representative community-based sample. Eat. Behav. 2013, 14, 390–393. [Google Scholar] [CrossRef] [PubMed]
- Mikami, A.Y.; Hinshaw, S.P.; Patterson, K.A.; Lee, J.C. Eating Pathology Among Adolescent Girls With Attention-Deficit/Hyperactivity Disorder. J. Abnorm. Psychol. 2008, 117, 225–235. [Google Scholar] [CrossRef] [Green Version]
- Mikami, A.Y.; Hinshaw, S.P.; Arnold, L.E.; Hoza, B.; Hechtman, L.; Newcorn, J.H.; Abikoff, H.B. Bulimia nervosa symptoms in the multimodal treatment study of children with ADHD. Int. J. Eat. Disord. 2010, 43, 248–259. [Google Scholar] [CrossRef]
- Nazar, B.P.; Pinna, C.M.D.S.; Coutinho, G.; Segenreich, D.; Duchesne, M.; Appolinario, J.C.; Mattos, P. Review of literature of attention-deficit/hyperactivity disorder with comorbid eating disorders. Rev. Bras. Psiquiatr. 2008, 30, 384–389. [Google Scholar] [CrossRef] [Green Version]
- Blinder, B.J.; Cumella, E.J.; Sanathara, V.A. Psychiatric comorbidities of female inpatients with eating disorders. Psychosom. Med. 2006, 68, 454–462. [Google Scholar] [CrossRef]
- Farber, S.K. The Comorbidity of Eating Disorders and Attention-Deficit Hyperactivity Disorder. Eat. Disord. 2009, 18, 81–89. [Google Scholar] [CrossRef] [PubMed]
- Stulz, N.; Hepp, U.; Gächter, C.; Martin-Soelch, C.; Spindler, A.; Milos, G. The severity of ADHD and eating disorder symptoms: A correlational study. BMC Psychiatry 2013, 13, 44. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Svedlund, N.E.; Norring, C.; Ginsberg, Y.; von Hausswolff-Juhlin, Y. Symptoms of Attention Deficit Hyperactivity Disorder (ADHD) among adult eating disorder patients. BMC Psychiatry 2017, 17, 19. [Google Scholar] [CrossRef] [Green Version]
- Wentz, E.; Lacey, J.H.; Waller, G.; Råstam, M.; Turk, J.; Gillberg, C. Childhood onset neuropsychiatric disorders in adult eating disorder patients. Eur. Child. Adolesc. Psychiatry 2005, 14, 431–437. [Google Scholar] [CrossRef] [Green Version]
- Yates, W.R.; Lund, B.C.; Johnson, C.; Mitchell, J.; McKee, P. Attention-deficit hyperactivity symptoms and disorder in eating disorder inpatients. Int. J. Eat. Disord. 2009, 42, 375–378. [Google Scholar] [CrossRef]
- Reinblatt, S.P.; Leoutsakos, J.-M.S.; Mahone, E.M.; Forrester, S.; Wilcox, H.C.; Riddle, M.A. Association between binge eating and attention-deficit/hyperactivity disorder in two pediatric community mental health clinics. Int. J. Eat. Disord. 2015, 48, 505–511. [Google Scholar] [CrossRef] [PubMed]
- Levin, R.L.; Rawana, J.S. Attention-deficit/hyperactivity disorder and eating disorders across the lifespan: A systematic review of the literature. Clin. Psychol. Rev. 2016, 50, 22–36. [Google Scholar] [CrossRef] [PubMed]
- Sonneville, K.R.; Calzo, J.P.; Horton, N.J.; Field, A.E.; Crosby, R.D.; Solmi, F.; Micali, N. Childhood hyperactivity/inattention and eating disturbances predict binge eating in adolescence. Psychol. Med. 2015, 45, 2511–2520. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nazar, B.P.; de Sousa Pinna, C.M.; Suwwan, R.; Duchesne, M.; Freitas, S.R.; Sergeant, J.; Mattos, P. ADHD Rate in Obese Women With Binge Eating and Bulimic Behaviors From a Weight-Loss Clinic. J. Atten. Disord. 2016, 20, 610–616. [Google Scholar] [CrossRef]
- Sepúlveda, A.R.; Solano, S.; Blanco, M.; Lacruz, T.; Veiga, O. Feasibility, acceptability, and effectiveness of a multidisciplinary intervention in childhood obesity from primary care: Nutrition, physical activity, emotional regulation, and family. Eur. Eat. Disord. Rev. 2020, 28, 184–198. [Google Scholar] [CrossRef]
- Mestre-Bach, G.; Steward, T.; Potenza, M.N.; Granero, R.; Fernández-Aranda, F.; Mena-Moreno, T.; Magaña, P.; Vintró-Alcaraz, C.; del Pino-Gutiérrez, A.; Menchón, J.M.; et al. The Role of ADHD Symptomatology and Emotion Dysregulation in Gambling Disorder. J. Atten. Disord. 2019, 108705471989437. [Google Scholar] [CrossRef]
- Aymamí, N.; Jiménez-Murcia, S.; Granero, R.; Ramos-Quiroga, J.A.; Fernández-Aranda, F.; Claes, L.; Sauvaget, A.; Grall-Bronnec, M.; Gómez-Peña, M.; Savvidou, L.G.; et al. Clinical, Psychopathological, and Personality Characteristics Associated with ADHD among Individuals Seeking Treatment for Gambling Disorder. Res. Artic. Clin. 2015. [Google Scholar] [CrossRef]
- Yao, S.; Kuja-Halkola, R.; Martin, J.; Lu, Y.; Lichtenstein, P.; Hübel, C.; Almqvist, C.; Magnusson, P.K.; Bulik, C.M.; Larsson, H.; et al. Associations Between Attention-Deficit/Hyperactivity Disorder and Various Eating Disorders: A Swedish Nationwide Population Study Using Multiple Genetically Informative Approaches. Biol. Psychiatry 2019, 86, 577–586. [Google Scholar] [CrossRef] [Green Version]
- Fernández-Aranda, F.; Agüera, Z.; Castro, R.; Jiménez-Murcia, S.; Ramos-Quiroga, J.A.; Bosch, R.; Fagundo, A.B.; Granero, R.; Penelo, E.; Claes, L.; et al. ADHD symptomatology in eating disorders: A secondary psychopathological measure of severity? BMC Psychiatry 2013, 13, 166. [Google Scholar] [CrossRef] [Green Version]
- Barkley, R.A.; Murphy, K.; Kwasnik, D. Psychological adjustment and adaptive impairments in young adults with ADHD. J. Atten. Disord. 1996, 1, 41–54. [Google Scholar] [CrossRef]
- Schredl, M.; Alm, B.; Sobanski, E. Sleep quality in adult patients with attention deficit hyperactivity disorder (ADHD). Eur. Arch. Psychiatry Clin. Neurosci. 2007, 257, 164–168. [Google Scholar] [CrossRef]
- Malloy-Diniz, L.; Fuentes, D.; Leite, W.B.; Correa, H.; Bechara, A. Impulsive behavior in adults with attention deficit/hyperactivity disorder: Characterization of attentional, motor and cognitive impulsiveness. J. Int. Neuropsychol. Soc. JINS 2007. [Google Scholar] [CrossRef]
- Scheres, A.; Lee, A.; Sumiya, M. Temporal reward discounting and ADHD: Task and symptom specific effects. J. Neural. Transm. 2008, 115, 221–226. [Google Scholar] [CrossRef] [PubMed]
- Donfrancesco, R.; Di Trani, M.; Porfirio, M.C.; Giana, G.; Miano, S.; Andriola, E. Might the temperament be a bias in clinical study on attention-deficit hyperactivity disorder (ADHD)?: Novelty Seeking dimension as a core feature of ADHD. Psychiatry Res. 2015, 227, 333–338. [Google Scholar] [CrossRef] [PubMed]
- Valko, L.; Doehnert, M.; Müller, U.C.; Schneider, G.; Albrecht, B.; Drechsler, R.; Maechler, M.; Steinhausen, H.C.; Brandeis, D. Differences in neurophysiological markers of inhibitory and temporal processing deficits in children and adults with ADHD. J. Psychophysiol. 2009, 23, 235–246. [Google Scholar] [CrossRef]
- Svedlund, N.E.; Norring, C.; Ginsberg, Y.; von Hausswolff-Juhlin, Y. Are treatment results for eating disorders affected by ADHD symptoms? A one-year follow-up of adult females. Eur. Eat. Disord. Rev. 2018, 26, 337–345. [Google Scholar] [CrossRef]
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 4th ed.; American Psychiatric Association: Washington, DC, USA, 2000. [Google Scholar]
- APA American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, 5th ed.; American Psychiatric Association: Washington, DC, USA, 2013. [Google Scholar]
- Kessler, R.C.; Adler, L.; Ames, M.; Demler, O.; Faraone, S.; Hiripi, E.; Howes, M.J.; Jin, R.; Secnik, K.; Spencer, T.; et al. The World Health Organization adult ADHD self-report scale (ASRS): A short screening scale for use in the general population. Psychol. Med. 2005, 35, 245–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ramos-Quiroga, J.A.; Daigre, C.; Valero, S.; Bosch, R.; Gómez-Barros, N.; Nogueira, M.; Palomar, G.; Roncero, C.; Casas, M. Validation of the Spanish version of the attention deficit hyperactivity disorder adult screening scale (ASRS v. 1.1): A novel scoring strategy. Rev. Neurol. 2009, 48, 449–452. [Google Scholar] [CrossRef] [PubMed]
- Garner, D.M. Inventario de Trastornos de la Conducta Alimentaria (EDI-2)-Manual; TEA: Madrid, Spain, 1998. [Google Scholar]
- Corral, S.; González, M.; Pereña, J.; Seisdedos, N. Adaptación española del Inventario de trastornos de la conducta alimentaria, Inventario de Trastornos de la Conducta Alimentaria; TEA: Madrid, Spain, 1998. [Google Scholar]
- Agüera, Z.; Sánchez, I.; Granero, R.; Riesco, N.; Steward, T.; Martín-Romera, V.; Jiménez-Murcia, S.; Romero, X.; Caroleo, M.; Segura-García, C.; et al. Short-Term Treatment Outcomes and Dropout Risk in Men and Women with Eating Disorders. Eur. Eat. Disord. Rev. 2017, 25, 293–301. [Google Scholar] [CrossRef] [PubMed]
- Riesco, N.; Agüera, Z.; Granero, R.; Jiménez-Murcia, S.; Menchón, J.M.; Fernández-Aranda, F. Other Specified Feeding or Eating Disorders (OSFED): Clinical heterogeneity and cognitive-behavioral therapy outcome. Eur. Psychiatry 2018, 54, 109–116. [Google Scholar] [CrossRef] [Green Version]
- StataCorp Stata Statistical Software, Release 16; StataCorp LLC: College Station, TX, USA, 2019.
- Singer, J.D.; Willett, J.B.; Willett, J.B. Applied Longitudinal Data Analysis: Modeling Change and Event Occurrence; Oxford University Press: New York, NY, USA, 2003. [Google Scholar]
- Barrett, P. Structural equation modelling: Adjudging model fit. Pers. Individ. Dif. 2007, 42, 815–824. [Google Scholar] [CrossRef]
- Bidwell, L.C.; Karoly, H.C.; Hutchison, K.E.; Bryan, A.D. ADHD symptoms impact smoking outcomes and withdrawal in response to Varenicline treatment for smoking cessation. Drug Alcohol Depend. 2017, 179, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Carroll, K.M.; Rounsaville, B.J. History and significance of childhood attention deficit disorder in treatment-seeking cocaine abusers. Compr. Psychiatry 1993, 34, 75–82. [Google Scholar] [CrossRef]
- Sullivan, M.A.; Rudnik-Levin, F. Attention Deficit/Hyperactivity Disorder and Substance Abuse. Ann. N. Y. Acad. Sci. 2006, 931, 251–270. [Google Scholar] [CrossRef]
- Van Emmerik-van Oortmerssen, K.; Blankers, M.; Vedel, E.; Kramer, F.; Goudriaan, A.E.; van den Brink, W.; Schoevers, R.A. Prediction of drop-out and outcome in integrated cognitive behavioral therapy for ADHD and SUD: Results from a randomized clinical trial. Addict. Behav. 2020, 103, 106228. [Google Scholar] [CrossRef] [PubMed]
- Faraone, S.V.; Biederman, J. What is the prevalence of adult ADHD? Results of a population screen of 966 adults. J. Atten. Disord. 2005, 9, 384–391. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Sociodemographic | n | % | Therapy Outcomes | n | % | |
|---|---|---|---|---|---|---|
| Marital | Single | 91 | 66.9% | Total sample (n = 136) | ||
| Married/Partner | 34 | 25.0% | Dropout | 64 | 47.0% | |
| Divorced/Separated | 11 | 8.1% | Non-remission | 16 | 11.8% | |
| Education | Primary | 32 | 23.5% | Partial remission | 25 | 18.4% |
| Secondary | 83 | 61.0% | Full remission | 31 | 22.8% | |
| University | 21 | 15.5% | Completers subsample (n = 72) | |||
| Age and ED severity level | Mean | SD | Non-remission | 16 | 22.2% | |
| Chronological age (years) | 28.74 | 9.59 | Partial remission | 25 | 34.7% | |
| EDI-2 total score | 97.91 | 44.52 | Full remission | 31 | 43.1% | |
| ADHD (ASRS screening) | n | % | ||||
| Positive screening | 46 | 33.8% | ||||
| Negative screening | 90 | 66.2% | ||||
| 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | 12 | 13 | 14 | 15 | ||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| 1. | ASRS: inattention | 0.166 | 0.882 † | 0.252 † | 0.356 † | 0.384 † | 0.287 † | 0.287 † | 0.425 † | 0.183 | 0.033 | 0.220 | 0.312 † | 0.419 † | 0.420 † |
| 2. | ASRS: hyperactive | --- | 0.609 † | 0.372 † | 0.282 † | 0.341 † | 0.226 | 0.086 | 0.207 | 0.214 | 0.116 | 0.336 † | 0.210 | 0.149 | 0.342 † |
| 3. | ASRS: total | --- | 0.379 † | 0.419 † | 0.474 † | 0.337 † | 0.267 | 0.438 † | 0.246 † | 0.078 | 0.337 † | 0.346 † | 0.402 † | 0.497 † | |
| 4. | EDI-2: Drive.thinness | --- | 0.622 † | 0.582 † | 0.367 † | 0.341 | 0.483 † | 0.297 † | 0.339 † | 0.364 † | 0.628 † | 0.440 † | 0.720 † | ||
| 5. | EDI-2: Body.dissatisf. | --- | 0.503 † | 0.483 † | 0.383 | 0.596 † | 0.283 † | 0.211 | 0.429 † | 0.506 † | 0.457 † | 0.751 † | |||
| 6. | EDI-2: Interoc.awar. | --- | 0.508 † | 0.500 | 0.700 † | 0.371 † | 0.305 † | 0.604 † | 0.666 † | 0.637 † | 0.838 † | ||||
| 7. | EDI-2: Bulimia | --- | 0.238 | 0.430 † | 0.032 | 0.056 | 0.385 † | 0.486 † | 0.262 † | 0.562 † | |||||
| 8. | EDI-2: Interp.distrust | --- | 0.561 † | 0.306 † | 0.168 | 0.347 † | 0.385 † | 0.697 † | 0.626 † | ||||||
| 9. | EDI-2: Ineffectiveness | --- | 0.503 † | 0.296 † | 0.568 † | 0.650 † | 0.749 † | 0.865 † | |||||||
| 10. | EDI-2: Maturity fears | --- | 0.277 † | 0.366 † | 0.279 † | 0.496 † | 0.549 † | ||||||||
| 11. | EDI-2: Perfectionism | --- | 0.331 † | 0.314 † | 0.299 † | 0.438 † | |||||||||
| 12. | EDI-2: Impulse.regul. | --- | 0.541 † | 0.576 † | 0.717 † | ||||||||||
| 13. | EDI-2: Ascetic | --- | 0.503 † | 0.768 † | |||||||||||
| 14. | EDI-2: Social.insec. | --- | 0.790 † | ||||||||||||
| 15. | EDI-2: Total score | --- |
| Treatment Outcome | Completers (n = 72) | Dropout (n = 64) | p | ||
|---|---|---|---|---|---|
| ADHD screening (+); n-% | 25 | 34.7% | 21 | 32.8% | 0.814 |
| Short-term therapy outcome | Full/partial remission (n = 56) | Dropout/non-remission (n = 80) | p | ||
| ADHD screening (+); n-% | 21 | 37.5% | 25 | 31.3% | 0.448 |
| Outcome at follow-up | Remission (n = 87) | Non-remission (n = 36) | p | ||
| ADHD screening (+); n-% | 29 | 33.3% | 12 | 33.3% | 1.00 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Testa, G.; Baenas, I.; Vintró-Alcaraz, C.; Granero, R.; Agüera, Z.; Sánchez, I.; Riesco, N.; Jiménez-Murcia, S.; Fernández-Aranda, F. Does ADHD Symptomatology Influence Treatment Outcome and Dropout Risk in Eating Disorders? A longitudinal Study. J. Clin. Med. 2020, 9, 2305. https://doi.org/10.3390/jcm9072305
Testa G, Baenas I, Vintró-Alcaraz C, Granero R, Agüera Z, Sánchez I, Riesco N, Jiménez-Murcia S, Fernández-Aranda F. Does ADHD Symptomatology Influence Treatment Outcome and Dropout Risk in Eating Disorders? A longitudinal Study. Journal of Clinical Medicine. 2020; 9(7):2305. https://doi.org/10.3390/jcm9072305
Chicago/Turabian StyleTesta, Giulia, Isabel Baenas, Cristina Vintró-Alcaraz, Roser Granero, Zaida Agüera, Isabel Sánchez, Nadine Riesco, Susana Jiménez-Murcia, and Fernando Fernández-Aranda. 2020. "Does ADHD Symptomatology Influence Treatment Outcome and Dropout Risk in Eating Disorders? A longitudinal Study" Journal of Clinical Medicine 9, no. 7: 2305. https://doi.org/10.3390/jcm9072305