Left Ventricular Geometry and Replacement Fibrosis Detected by cMRI Are Associated with Major Adverse Cardiovascular Events in Nonischemic Dilated Cardiomyopathy

 ,
,
Abstract
:1. Introduction
2. Methods
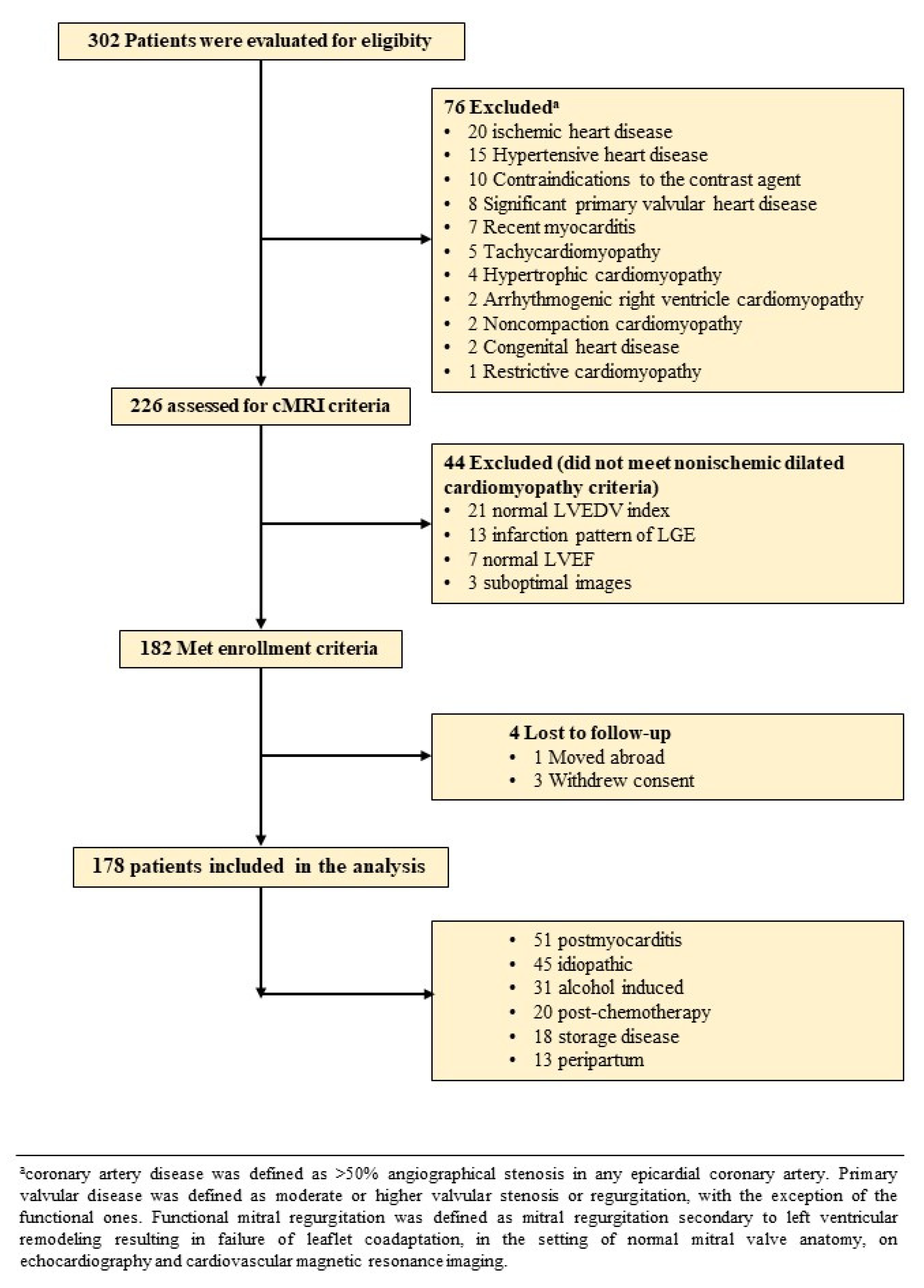
2.1. Study Population
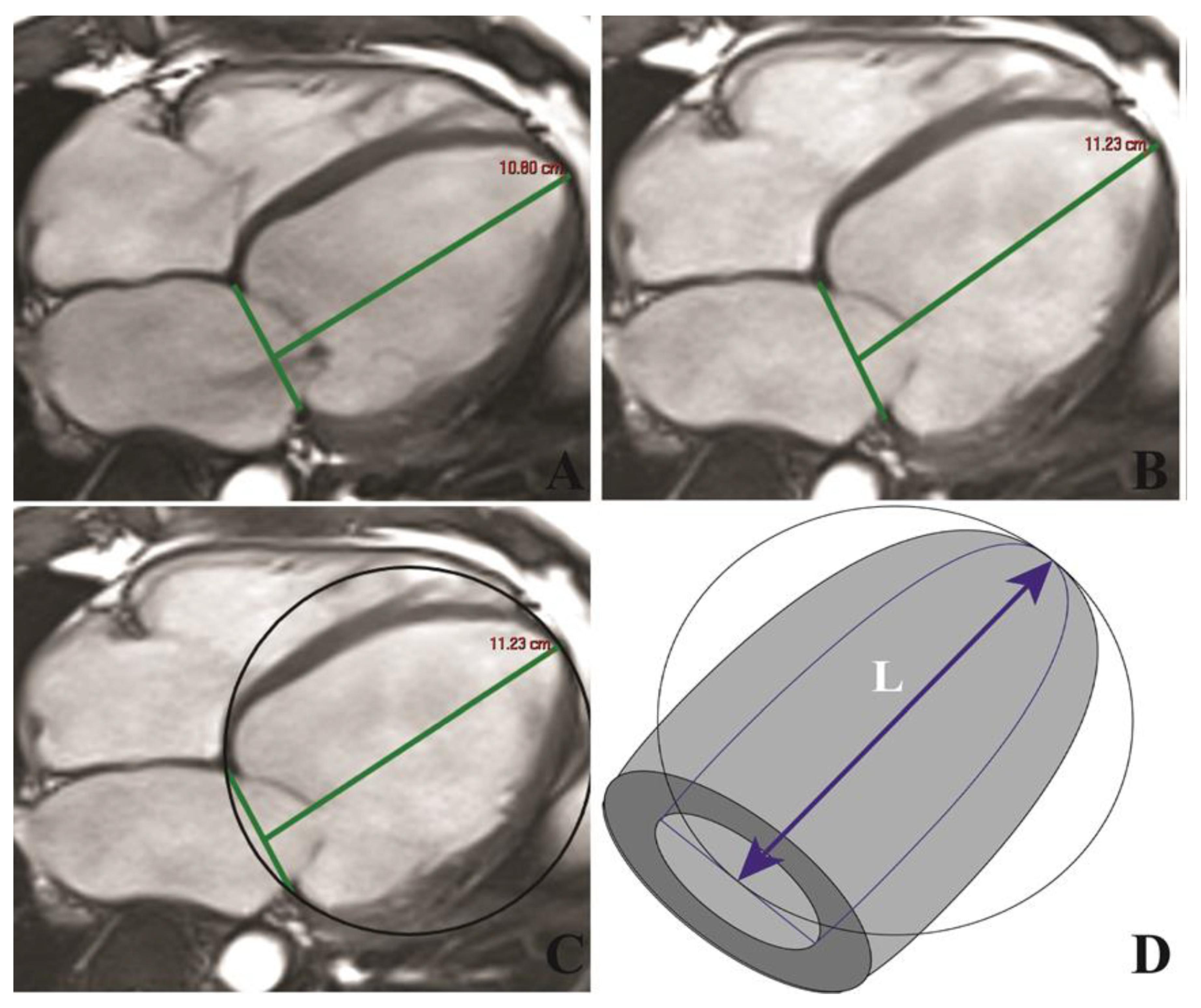
2.2. cMRI
2.3. Follow-Up of Clinical Outcomes
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Reproducibility of cMRI Measurements
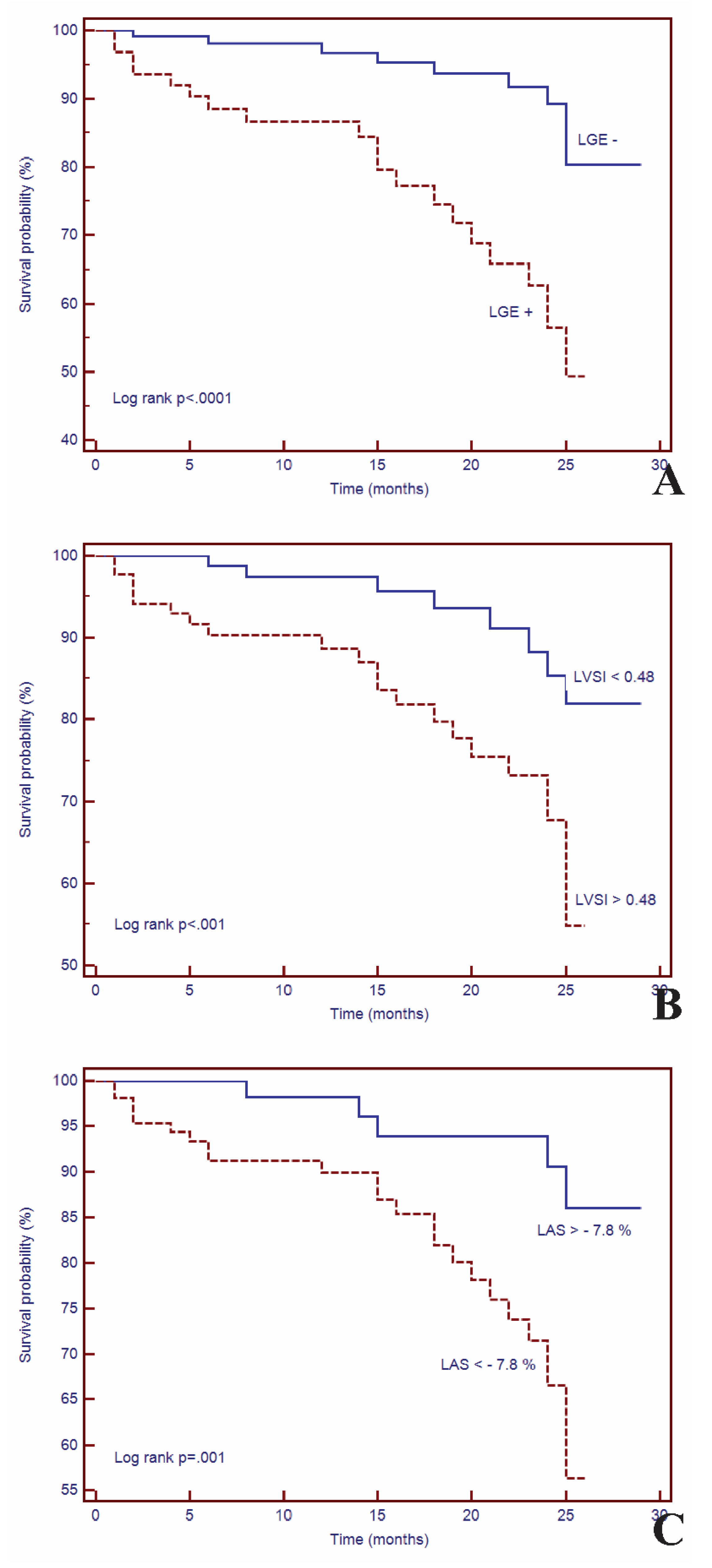
3.3. Survival Analysis
3.4. Univariate and Multivariate Cox Analysis
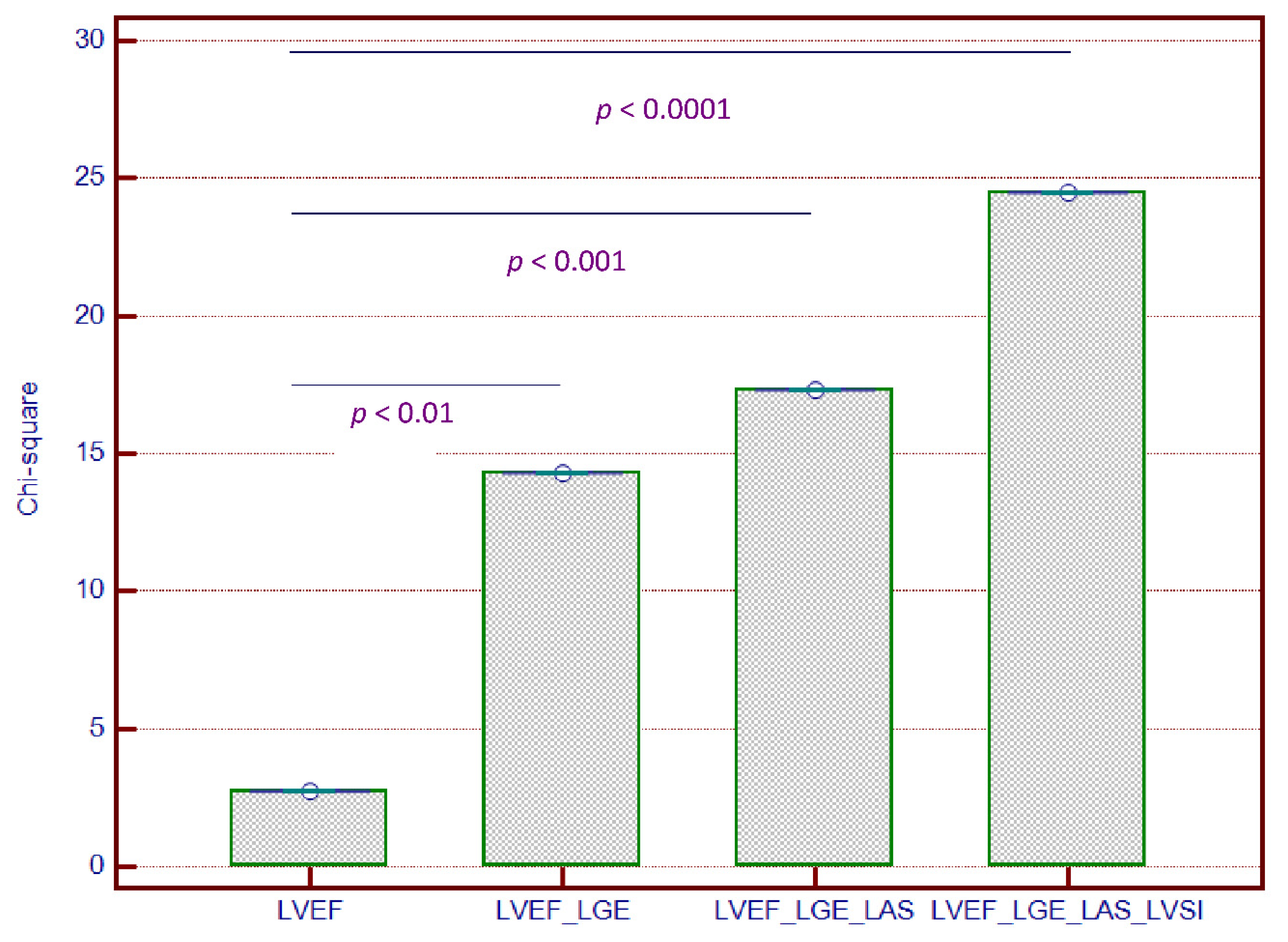
3.5. Incremental Predictive Value of cMRI-Based LV Geometry and Strain for Outcomes
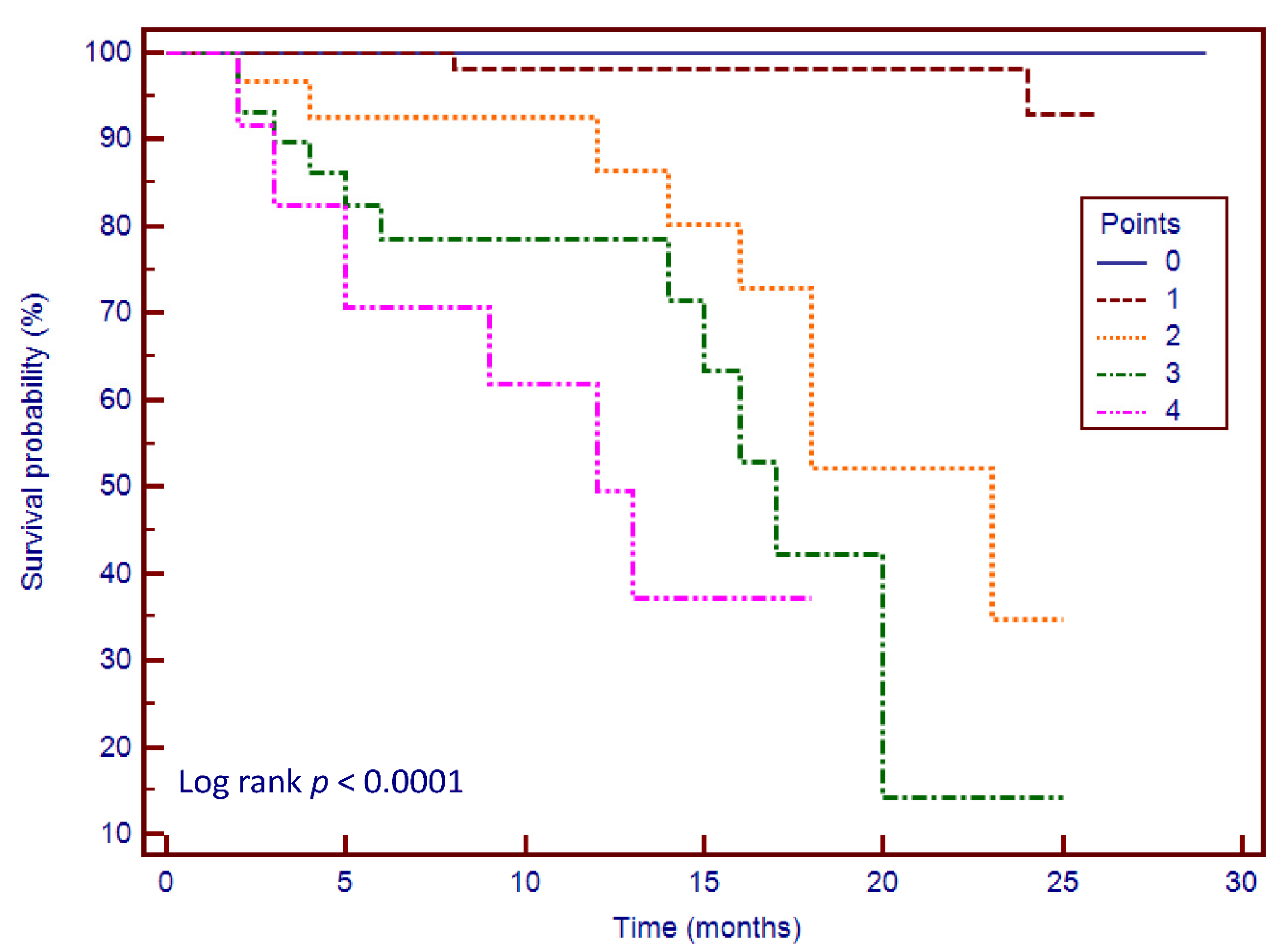
3.6. Risk Stratification Scoring System
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Pinto, Y.M.; Elliott, P.M.; Arbustini, E.; Adler, Y.; Anastasakis, A.; Böhm, M.; Duboc, D.; Gimeno, J.; de Groote, P.; Imazio, M.; et al. Proposal for a Revised Definition of Dilated Cardiomyopathy, Hypokinetic Non-Dilated Cardiomyopathy, and Its Implications for Clinical Practice: A Position Statement of the ESC Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2016, 37, 1850–1858. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Felker, G.M.; Thompson, R.E.; Hare, J.M.; Hruban, R.H.; Clemetson, D.E.; Howard, D.L.; Baughman, K.L.; Kasper, E.K. Underlying Causes and Long-Term Survival in Patients with Initially Unexplained Cardiomyopathy. N. Engl. J. Med. 2000, 342, 1077–1084. [Google Scholar] [CrossRef] [PubMed]
- Kadish, A.; Dyer, A.; Daubert, J.P.; Quigg, R.; Estes, N.A.M.; Anderson, K.P.; Calkins, H.; Hoch, D.; Goldberger, J.; Shalaby, A.; et al. Prophylactic Defibrillator Implantation in Patients with Nonischemic Dilated Cardiomyopathy. N. Engl. J. Med. 2004, 350, 2151–2158. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.F.; Coats, A.J.S.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the Diagnosis and Treatment of Acute and Chronic Heart Failure. Eur. Heart J. 2016, 37, 2129–2200. [Google Scholar] [CrossRef]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS Guideline for Management of Patients With Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death. J. Am. Coll. Cardiol. 2018, 72, e91–e220. [Google Scholar] [CrossRef]
- Buxton, A.E.; Ellison, K.E.; Lorvidhaya, P.; Ziv, O. Left Ventricular Ejection Fraction for Sudden Death Risk Stratification and Guiding Implantable Cardioverter-Defibrillators Implantation. J. Cardiovasc. Pharmacol. 2010, 55, 450–455. [Google Scholar]
- Iles, L.M.; Ellims, A.H.; Llewellyn, H.; Hare, J.L.; Kaye, D.M.; McLean, C.A.; Taylor, A.J. Histological Validation of Cardiac Magnetic Resonance Analysis of Regional and Diffuse Interstitial Myocardial Fibrosis. Eur. Heart J.Cardiovasc. Imaging 2015, 16, 14–22. [Google Scholar] [CrossRef]
- Halliday, B.P.; Gulati, A.; Ali, A.; Guha, K.; Newsome, S.; Arzanauskaite, M.; Vassiliou, V.S.; Lota, A.; Izgi, C.; Tayal, U.; et al. Association Between Midwall Late Gadolinium Enhancement and Sudden Cardiac Death in Patients With Dilated Cardiomyopathy and Mild and Moderate Left Ventricular Systolic Dysfunction. Circulation 2017, 135, 2106–2115. [Google Scholar] [CrossRef] [Green Version]
- Gulati, A.; Jabbour, A.; Ismail, T.F.; Guha, K.; Khwaja, J.; Raza, S.; Morarji, K.; Brown, T.D.H.; Ismail, N.A.; Dweck, M.R.; et al. Association of Fibrosis With Mortality and Sudden Cardiac Death in Patients with Nonischemic Dilated Cardiomyopathy. JAMA 2013, 309, 896. [Google Scholar] [CrossRef] [Green Version]
- Di Marco, A.; Anguera, I.; Schmitt, M.; Klem, I.; Neilan, T.G.; White, J.A.; Sramko, M.; Masci, P.G.; Barison, A.; Mckenna, P.; et al. Late Gadolinium Enhancement and the Risk for Ventricular Arrhythmias or Sudden Death in Dilated Cardiomyopathy. JACC Heart Fail. 2017, 5, 28–38. [Google Scholar] [CrossRef]
- Yancy, C.W.; Jessup, M.; Bozkurt, B.; Butler, J.; Casey, D.E.; Drazner, M.H.; Fonarow, G.C.; Geraci, S.A.; Horwich, T.; Januzzi, J.L.; et al. 2013 ACCF/AHA Guideline for the Management of Heart Failure. J. Am. Coll. Cardiol. 2013, 62, e147–e239. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Coelho-Filho, O.R.; Mongeon, F.-P.; Mitchell, R.; Moreno, H.; Nadruz, W.; Kwong, R.; Jerosch-Herold, M. Role of Transcytolemmal Water-Exchange in Magnetic Resonance Measurements of Diffuse Myocardial Fibrosis in Hypertensive Heart Disease. Circ. Cardiovasc. Imaging 2013, 6, 134–141. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Arenja, N.; Andre, F.; Riffel, J.H.; aus dem Siepen, F.; Hegenbart, U.; Schönland, S.; Kristen, A.V.; Katus, H.A.; Buss, S.J. Prognostic Value of Novel Imaging Parameters Derived from Standard Cardiovascular Magnetic Resonance in High Risk Patients with Systemic Light Chain Amyloidosis. J. Cardiovasc. Magn. Reson. 2019, 21, 53. [Google Scholar] [CrossRef] [Green Version]
- Tsadok, Y.; Friedman, Z.; Haluska, B.A.; Hoffmann, R.; Adam, D. Myocardial Strain Assessment by Cine Cardiac Magnetic Resonance Imaging Using Non-Rigid Registration. Magn. Reson. Imaging 2016, 34, 381–390. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Liang, Y.; Li, W.; Zeng, R.; Sun, J.; Wan, K.; Xu, Y.; Cao, Y.; Zhang, Q.; Han, Y.; Chen, Y. Left Ventricular Spherical Index Is an Independent Predictor for Clinical Outcomes in Patients With Nonischemic Dilated Cardiomyopathy. JACC Cardiovasc. Imaging 2019, 12, 1578–1580. [Google Scholar] [CrossRef]
- Muthalaly, R.G.; Kwong, R.Y.; John, R.M.; van der Geest, R.J.; Tao, Q.; Schaeffer, B.; Tanigawa, S.; Nakamura, T.; Kaneko, K.; Tedrow, U.B.; et al. Left Ventricular Entropy Is a Novel Predictor of Arrhythmic Events in Patients With Dilated Cardiomyopathy Receiving Defibrillators for Primary Prevention. JACC Cardiovasc. Imaging 2019, 12, 1177–1184. [Google Scholar] [CrossRef]
- Kramer, C.M.; Barkhausen, J.; Flamm, S.D.; Kim, R.J.; Nagel, E. Standardized Cardiovascular Magnetic Resonance (CMR) Protocols 2013 Update. J. Cardiovasc. Magn. Reson. 2013, 15, 91. [Google Scholar] [CrossRef] [Green Version]
- Cerqueira, M.D.; Weissman, N.J.; Dilsizian, V.; Jacobs, A.K.; Kaul, S.; Laskey, W.K.; Pennell, D.J.; Rumberger, J.A.; Ryan, T.; Verani, M.S. Standardized Myocardial Segmentation and Nomenclature for Tomographic Imaging of the Heart. Circulation 2002, 105, 539–542. [Google Scholar] [CrossRef]
- Bondarenko, O.; Beek, A.; Hofman, M.; Kühl, H.; Twisk, J.; van Dockum, W.; Visser, C.; van Rossum, A. Standardizing the Definition of Hyperenhancement in the Quantitative Assessment of Infarct Size and Myocardial Viability Using Delayed Contrast-Enhanced CMR. J. Cardiovasc. Magn. Reson. 2005, 7, 481–485. [Google Scholar] [CrossRef]
- Gao, P.; Yee, R.; Gula, L.; Krahn, A.D.; Skanes, A.; Leong-Sit, P.; Klein, G.J.; Stirrat, J.; Fine, N.; Pallaveshi, L.; et al. Prediction of Arrhythmic Events in Ischemic and Dilated Cardiomyopathy Patients Referred for Implantable Cardiac Defibrillator. Circ. Cardiovasc. Imaging 2012, 5, 448–456. [Google Scholar] [CrossRef] [Green Version]
- Piek, A.; de Boer, R.A.; Silljé, H.H.W. The Fibrosis-Cell Death Axis in Heart Failure. Heart Fail. Rev. 2016, 21, 199–211. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doltra, A.; Amundsen, B.; Gebker, R.; Fleck, E.; Kelle, S. Emerging Concepts for Myocardial Late Gadolinium Enhancement MRI. Curr. Cardiol. Rev. 2013, 9, 185–190. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lehrke, S.; Lossnitzer, D.; Schob, M.; Steen, H.; Merten, C.; Kemmling, H.; Pribe, R.; Ehlermann, P.; Zugck, C.; Korosoglou, G.; et al. Use of Cardiovascular Magnetic Resonance for Risk Stratification in Chronic Heart Failure: Prognostic Value of Late Gadolinium Enhancement in Patients with Non-Ischaemic Dilated Cardiomyopathy. Heart 2011, 97, 727–732. [Google Scholar] [CrossRef]
- Sree Raman, K.; Nucifora, G.; Leong, D.P.; Marx, C.; Shah, R.; Woodman, R.J.; Molaee, P.; Shirazi, M.G.; McGavigan, A.D.; De Pasquale, C.G.; et al. Long Term Prognostic Importance of Late Gadolinium Enhancement in First-Presentation Non-Ischaemic Dilated Cardiomyopathy. Int. J. Cardiol. 2019, 280, 124–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Halliday, B.P.; Baksi, A.J.; Gulati, A.; Ali, A.; Newsome, S.; Izgi, C.; Arzanauskaite, M.; Lota, A.; Tayal, U.; Vassiliou, V.S.; et al. Outcome in Dilated Cardiomyopathy Related to the Extent, Location, and Pattern of Late Gadolinium Enhancement. JACC Cardiovasc. Imaging 2019, 12, 1645–1655. [Google Scholar] [CrossRef] [PubMed]
- Becker, M.A.J.; Cornel, J.H.; van de Ven, P.M.; van Rossum, A.C.; Allaart, C.P.; Germans, T. The Prognostic Value of Late Gadolinium-Enhanced Cardiac Magnetic Resonance Imaging in Nonischemic Dilated Cardiomyopathy. JACC Cardiovasc. Imaging 2018, 11, 1274–1284. [Google Scholar] [CrossRef] [PubMed]
- Stolfo, D.; Merlo, M.; Pinamonti, B.; Barbati, G.; Di Lenarda, A.; Sinagra, G. Evolution of Left Ventricular Sphericity Index in Idiopathic Dilated Cardiomyopathy: Clinical and Prognostic Implications. Eur. Heart J. 2013, 34 (Suppl. 1), P1196. [Google Scholar] [CrossRef] [Green Version]
- Marchal, P.; Lairez, O.; Cognet, T.; Chabbert, V.; Barrier, P.; Berry, M.; Mejean, S.; Roncalli, J.; Rousseau, H.; Carrie, D.; et al. Relationship between Left Ventricular Sphericity and Trabeculation Indexes in Patients with Dilated Cardiomyopathy: A Cardiac Magnetic Resonance Study. Eur. Heart J.Cardiovasc. Imaging 2013, 14, 914–920. [Google Scholar] [CrossRef] [Green Version]
- Ben Halima, A.; Zidi, A. The Cardiac Magnetic Resonance Sphericity Index in the Dilated Cardiomyopathy: New Diagnostic and Prognostic Marker. Arch. Cardiovasc. Dis. Suppl. 2018, 10, 42. [Google Scholar] [CrossRef]
- Ambale-Venkatesh, B.; Yoneyama, K.; Sharma, R.K.; Ohyama, Y.; Wu, C.O.; Burke, G.L.; Shea, S.; Gomes, A.S.; Young, A.A.; Bluemke, D.A.; et al. Left Ventricular Shape Predicts Different Types of Cardiovascular Events in the General Population. Heart 2017, 103, 499–507. [Google Scholar] [CrossRef]
- Nakamori, S.; Ismail, H.; Ngo, L.H.; Manning, W.J.; Nezafat, R. Left Ventricular Geometry Predicts Ventricular Tachyarrhythmia in Patients with Left Ventricular Systolic Dysfunction: A Comprehensive Cardiovascular Magnetic Resonance Study. J. Cardiovasc. Magn. Reson. 2017, 19, 79. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gjesdal, O.; Almeida, A.L.C.; Hopp, E.; Beitnes, J.O.; Lunde, K.; Smith, H.-J.; Lima, J.A.C.; Edvardsen, T. Long Axis Strain by MRI and Echocardiography in a Postmyocardial Infarct Population. J. Magn. Reson. Imaging 2014, 40, 1247–1251. [Google Scholar] [CrossRef] [PubMed]
- Schuster, A.; Backhaus, S.J.; Stiermaier, T.; Kowallick, J.T.; Stulle, A.; Koschalka, A.; Lotz, J.; Kutty, S.; Bigalke, B.; Gutberlet, M.; et al. Fast Manual Long-Axis Strain Assessment Provides Optimized Cardiovascular Event Prediction Following Myocardial Infarction. Eur. Heart J.Cardiovasc. Imaging 2019, 20, 1262–1270. [Google Scholar] [CrossRef] [PubMed]
- Gjesdal, O.; Yoneyama, K.; Mewton, N.; Wu, C.; Gomes, A.S.; Hundley, G.; Prince, M.; Shea, S.; Liu, K.; Bluemke, D.A.; et al. Reduced Long Axis Strain Is Associated with Heart Failure and Cardiovascular Events in the Multi-Ethnic Study of Atherosclerosis. J. Magn. Reson. Imaging 2016, 44, 178–185. [Google Scholar] [CrossRef]
- Agoston-Coldea, L.; Bheecarry, K.; Cionca, C.; Petra, C.; Strimbu, L.; Ober, C.; Lupu, S.; Fodor, D.; Mocan, T. Incremental Predictive Value of Longitudinal Axis Strain and Late Gadolinium Enhancement Using Standard CMR Imaging in Patients with Aortic Stenosis. J. Clin. Med. 2019, 8, 165. [Google Scholar] [CrossRef] [Green Version]
- Riffel, J.H.; Keller, M.G.P.; Rost, F.; Arenja, N.; Andre, F.; aus dem Siepen, F.; Fritz, T.; Ehlermann, P.; Taeger, T.; Frankenstein, L.; et al. Left Ventricular Long Axis Strain: A New Prognosticator in Non-Ischemic Dilated Cardiomyopathy? J. Cardiovasc. Magn. Reson. 2016, 18, 36. [Google Scholar] [CrossRef] [Green Version]
- Kano, N.; Okumura, T.; Hiraiwa, H.; Watanabe, N.; Kondo, T.; Fukaya, K.; Sawamura, A.; Morimoto, R.; Bando, Y.; Murohara, T. Prognostic Impact of Combination of Sphericity Index and Late Gadolinium Enhancement on Cardiac Magnetic Resonance in Patients with Dilated Cardiomyopathy. J. Card. Fail. 2016, 22, S177. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All Patients n = 178 | LGE− n = 114 | LGE+ n = 64 | p-Value | |
|---|---|---|---|---|
| Clinical characteristics | ||||
| - Age, mean (SD), years | 48 (14.4) | 47 (15.0) | 45 (13.4) | NS |
| - Male gender, n (%) | 133 (74.7) | 83 (72.8) | 50 (78.1) | NS |
| - Body-mass index, kg/m2 | 27.4 (4.8) | 27.3 (4.4) | 27.5 (5.7) | NS |
| - Heart rate, mean (SD), bpm | 73 (16.0) | 71 (14.3) | 76 (18.3) | <0.05 |
| - Systolic blood pressure, mean (SD), mmHg | 133 (18.9) | 134 (18.4) | 130 (19.5) | NS |
| - Hypertension, n (%) | 98 (55.1) | 69 (60.5) | 29 (45.5) | <0.05 |
| - Diabetes mellitus, n (%) | 58 (32.5) | 41 (35.9) | 17 (26.5) | NS |
| - Dyslipidemia, n (%) | 104 (58.4) | 67 (58.8) | 37 (57.8) | NS |
| - Smoking, n (%) | 58 (32.5) | 39 (34.2) | 19 (29.6) | NS |
| - NYHA functional class I/II/III, n | 29/59/27 | 19/39/19 | 10/20/8 | <0.05 |
| Electrocardiogram | ||||
| - Atrial fibrillation, n (%) | 26 (14.6) | 18 (15.7) | 8 (12.5) | NS |
| - Left bundle branch block, n (%) | 15 (8.4) | 10 (8.7) | 5 (7.8) | NS |
| - Right bundle branch block, n (%) | 17 (9.5) | 12 (10.5) | 5 (7.8) | NS |
| - Significant Q waves, n (%) | 21 (11.8) | 14 (12.3) | 7 (10.9) | NS |
| Medications | ||||
| - Beta-blockers, n (%) | 142 (79.7) | 91 (79.8) | 51 (79.6) | NS |
| - ACEIs or ARBs, n (%) | 130 (73.0) | 84 (73.6) | 46 (71.8) | NS |
| - Calcium channel blockers, n (%) | 28 (15.7) | 18 (15.7) | 10 (15.6) | NS |
| - Statins, n (%) | 105 (58.9) | 67 (58.7) | 38 (59.3) | NS |
| - Antiplatelet therapy, n (%) | 68 (38.2) | 44 (38.5) | 25 (37.5) | NS |
| - Diuretics, n (%) | 111 (62.3) | 70 (61.4) | 41 (64.0) | NS |
| - Digitalis, n (%) | 13 (7.3) | 8 (7.0) | 5 (7.8) | NS |
| Biomarker levels | ||||
| - NT-proBNP, median (IQR), pg/mL | 2639.5 (378–11,960) | 2600 (378–9893) | 2679 (570–11,960) | NS |
| - eGFR, mean (SD), ml/min/1.73 m2 | 87.1 (21.2) | 87.7 (20.4) | 86.1 (22.6) | NS |
| Echocardiography | ||||
| - E/E’ ratio, mean (SD) | 9.27 (2.5) | 8.2 (2.4) | 12.3 (2.6) | <0.001 |
| - DT, mean (SD), ms | 217 (56.7) | 215 (53.4) | 221 (63.1) | NS |
| - sPAP, mean (SD), mmHg | 30.8 (12.0) | 30.1 (12.5) | 32.2 (11.0) | NS |
| Cardiovascular magnetic resonance | ||||
| - LVEDV index, mean (SD), mL/m2 | 132.3 (34.5) | 124.8 (30.2) | 145.5 (37.8) | <0.001 |
| - LVESV index, mean (SD), mL/m2 | 87.5 (34.4) | 78.6 (29.6) | 103.5 (36.8) | <0.001 |
| - LVM index, mean (SD), g/m2 | 86.7 (20.6) | 83.7 (19.6) | 92.0 (21.6) | <0.01 |
| - LVEF, mean (SD), % | 35.0 (9.3) | 37.8 (7.7) | 29.9 (9.7) | <0.001 |
| - LAV index, mean (SD), mL/m2 | 55.8 (21.3) | 53.1 (20.4) | 60.6 (22.2) | <0.05 |
| - LAS, mean (SD), % | −9.6 (5.3) | −10.7 (5.4) | −7.8 (4.6) | <0.001 |
| - LVSI, mean (SD) | 0.40 (0.12) | 0.38 (0.11) | 0.43 (0.13) | <0.001 |
| - TAPSE, mean (SD), mm | 18.6 (5.2) | 19.5 (5.3) | 16.9 (4.7) | 0.001 |
| - RVEDV index, mean (SD), mL/m2 | 53.4 (21.2) | 52.7 (19.2) | 54.7 (24.4) | NS |
| - RVESV index, mean (SD), mL/m2 | 29.0 (15.5) | 27.2 (11.9) | 32.2 (20.0) | <0.01 |
| - RVEF, mean (SD), % | 46.8 (9.55) | 49.0 (8.7) | 42.8 (9.7) | <0.01 |
| - LV-LGE mass median (IQR), g | 30.5 (1–88) | |||
| - LV-LGE mass/LVM, median (IQR), % | 17.2 (0.6–54) |
| Parameters | Coefficient Kappa | 95% Confidence Interval | Standard Error |
|---|---|---|---|
| Inter-observer | |||
| LVEF | 0.91 | 0.872 to 0.941 | 0.026 |
| LAS | 0.97 | 0.909 to 0.989 | 0.012 |
| LGE | 0.88 | 0.771 to 0.939 | 0.066 |
| LVSI | 0.93 | 0.856 to 0.952 | 0.029 |
| Intra-observer | |||
| LVEF | 0.98 | 0.977 to 0.992 | 0.009 |
| LAS | 0.98 | 0.967 to 0.991 | 0.004 |
| LGE | 0.90 | 0.835 to 0.948 | 0.023 |
| LVSI | 0.92 | 0.871 to 0.928 | 0.032 |
| No Events n = 147 | Events n = 31 | Univariable Analysis | Multivariable Analysis | |||
|---|---|---|---|---|---|---|
| Unadjusted HR (95% CI) | p Value | Adjusted HR (95% CI) | p Value | |||
| Age, years | 48 (13.8) | 48 (17.5) | 1.00 (0.98–1.03) | NS | ||
| Male gender, n, % | 111 (75.5) | 22 (37.9) | 1.14 (0.53–2.48) | NS | ||
| Body-mass index, kg/m2 | 27.7 (4.8) | 25.8 (4.5) | 0.94 (0.87–1.01) | NS | ||
| Systolic blood pressure | 134 (19.2) | 130 (17.4) | 0.99 (0.97–1.01) | NS | ||
| NT-proBNP, pg/mL | 2564 (378–11960) | 2834 (834–9892) | 1.00 (0.99–1.01) | NS | ||
| eGFR, ml/min/1.73 m2 | 86.3 (20.1) | 91.0 (25.9) | 1.01 (0.97–1.03) | NS | ||
| LVEDV index, mL/m2 | 131.4 (35.6) | 136.6 (32.7) | 1.01 (0.99–1.01) | NS | ||
| LVESV index, mL/m2 | 86.4 (34.5) | 93.1 (33.8) | 1.05 (0.98–1.07) | NS | ||
| LVM index, g/m2 | 87.0 (20.7) | 85.2 (20.8) | 0.99 (0.97–1.01) | NS | ||
| LVEF, % | 35.5 (9.2) | 32.4 (9.4) | 0.97 (0.93–1.01) | NS | ||
| LAV index, mL/m2 | 54.7 (21.7) | 61.3 (18.6) | 1.01 (1.00–1.03) | NS | ||
| LGE+ | 43 (29.2) | 21 (67.7) | 4.03 (1.90–8.52) | <0.0001 | 1.77 (2.79–12.51) | <0.0001 |
| LGE mass, g | 11.3 (10.6) | 28.8 (19.3) | 1.23 (1.90–4.52) | <0.0001 | 1.43 (1.01–6.12) | <0.001 |
| LAS, % | −10.0 (5.6) | −7.8 (3.6) | 1.19 (1.01–2.18) | <0.001 | 1.32 (1.54–9.14) | 0.001 |
| LVSI, % | 0.38 (0.11) | 0.48 (0.13) | 2.13 (1.05–8.11) | <0.001 | 1.17 (1.14–7.19) | <0.01 |
| E/E’ ratio | 9.1 (2.3) | 15.7 (4.8) | 1.08 (0.95–1.22) | <0.05 | 1.02 (0.92–1.01) | NS |
| TAPSE, mm | 18.8 (5.2) | 17.4 (5.4) | 0.77 (0.70–0.84) | NS | ||
| RVEDV index, mL/m2 | 53.3 (19.7) | 53.8 (27.6) | 1.00 (0.98–1.02) | NS | ||
| RVESV index, mL/m2 | 28.2 (13.5) | 32.4 (13.9) | 1.02 (1.00–1.04) | NS | ||
| RVEF, % | 47.5 (9.3) | 43.4 (10.2) | 0.84 (0.79–0.88) | NS | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cojan-Minzat, B.O.; Zlibut, A.; Muresan, I.D.; Cionca, C.; Horvat, D.; Kiss, E.; Revnic, R.; Florea, M.; Ciortea, R.; Agoston-Coldea, L. Left Ventricular Geometry and Replacement Fibrosis Detected by cMRI Are Associated with Major Adverse Cardiovascular Events in Nonischemic Dilated Cardiomyopathy. J. Clin. Med. 2020, 9, 1997. https://doi.org/10.3390/jcm9061997
Cojan-Minzat BO, Zlibut A, Muresan ID, Cionca C, Horvat D, Kiss E, Revnic R, Florea M, Ciortea R, Agoston-Coldea L. Left Ventricular Geometry and Replacement Fibrosis Detected by cMRI Are Associated with Major Adverse Cardiovascular Events in Nonischemic Dilated Cardiomyopathy. Journal of Clinical Medicine. 2020; 9(6):1997. https://doi.org/10.3390/jcm9061997
Chicago/Turabian StyleCojan-Minzat, Bianca Olivia, Alexandru Zlibut, Ioana Danuta Muresan, Carmen Cionca, Dalma Horvat, Eva Kiss, Radu Revnic, Mira Florea, Razvan Ciortea, and Lucia Agoston-Coldea. 2020. "Left Ventricular Geometry and Replacement Fibrosis Detected by cMRI Are Associated with Major Adverse Cardiovascular Events in Nonischemic Dilated Cardiomyopathy" Journal of Clinical Medicine 9, no. 6: 1997. https://doi.org/10.3390/jcm9061997