The Effect of Integrated Care Management on Dementia in Atrial Fibrillation

 , , ,
, , ,  and
and
Abstract
:1. Introduction
2. Experimental Section
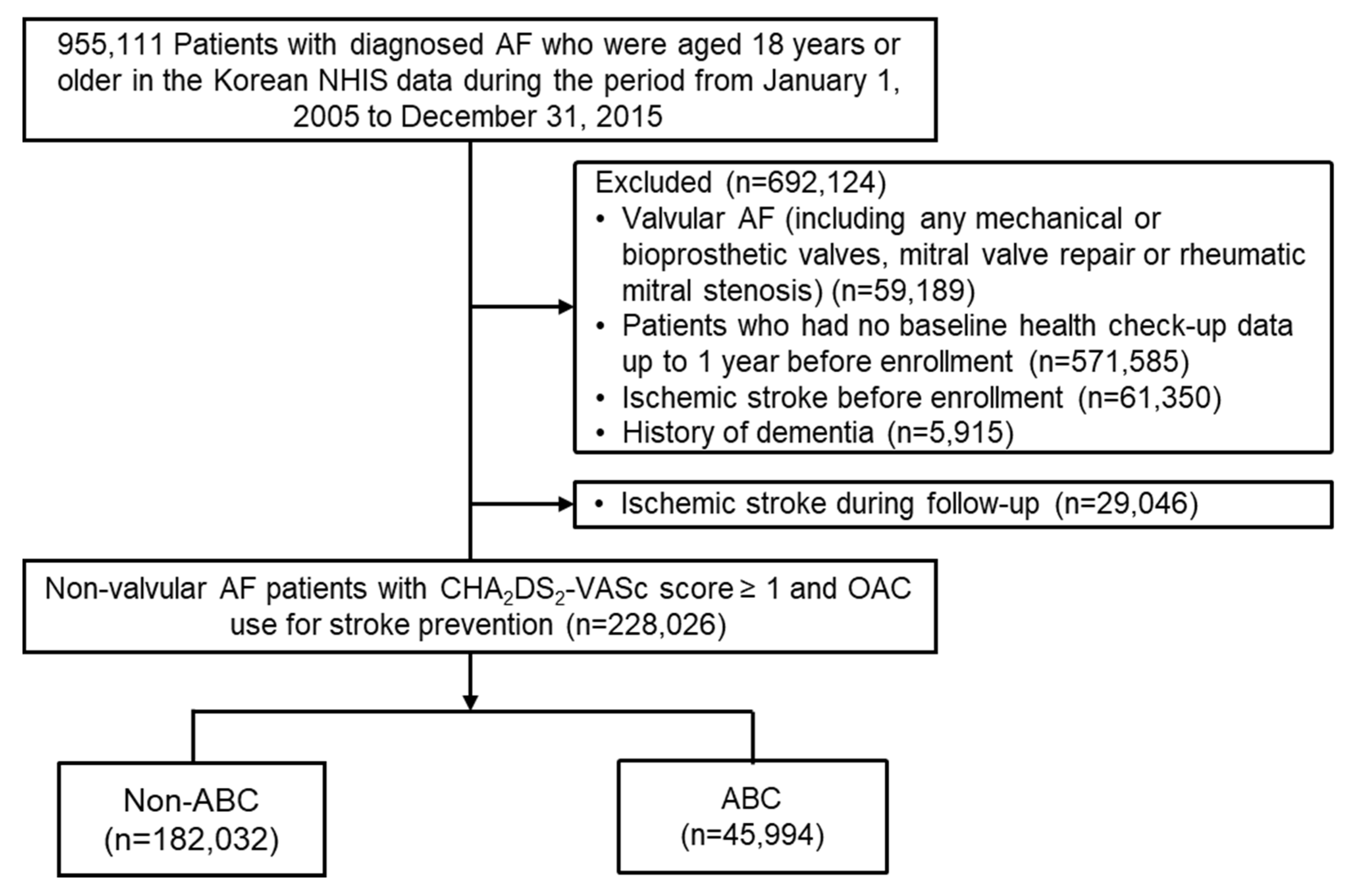
2.1. Study Cohort
2.2. Definition of the ABC Pathway-Compliant Group
2.3. Covariates, Primary and Secondary Outcome
2.4. Statistical Analysis
3. Results
3.1. Baseline Characteristics
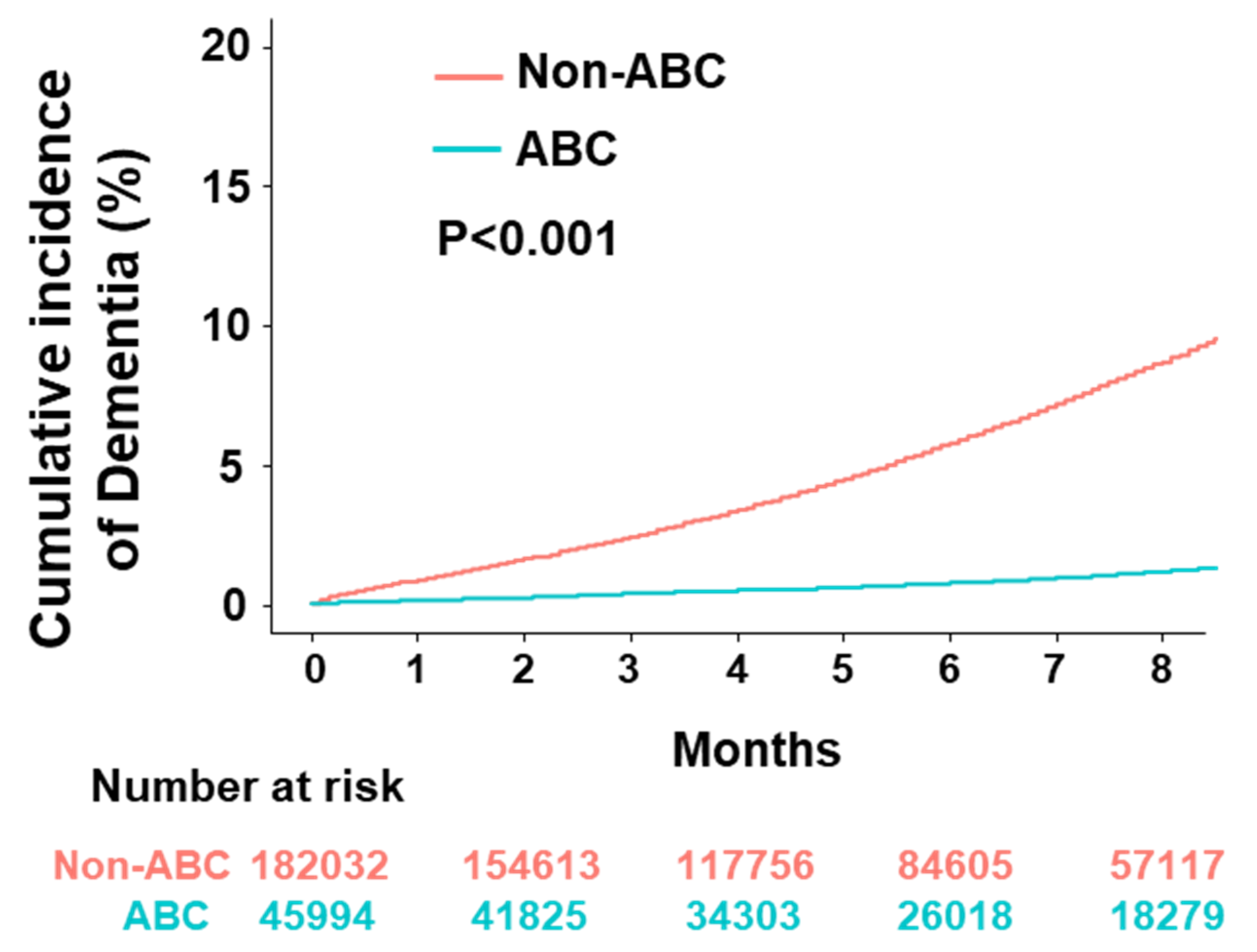
3.2. Dementia
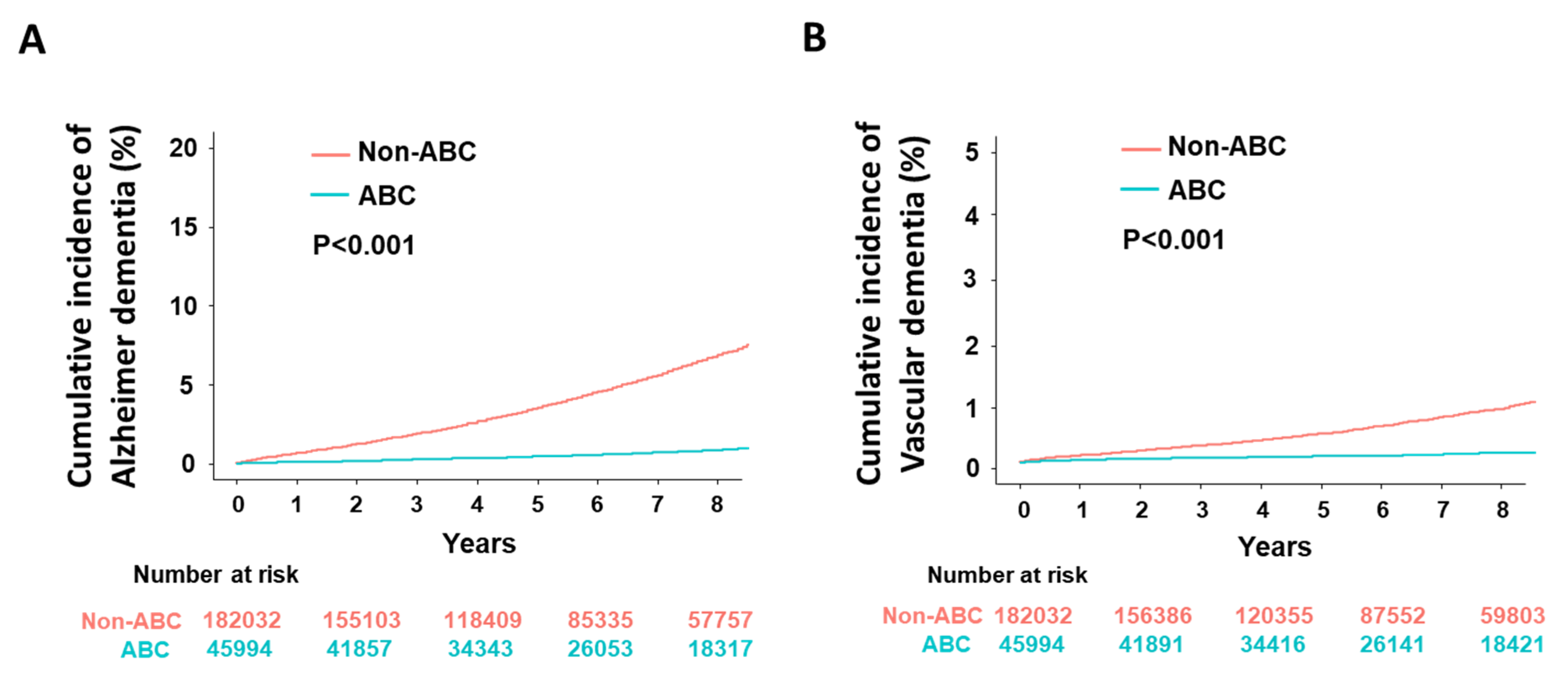
3.3. Alzheimer’s and Vascular Dementia
3.4. Subgroup Analysis
4. Discussion
4.1. AF and Dementia
4.2. Dementia and Integrated AF Management
4.3. Study Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lee, H.; Kim, T.-H.; Baek, Y.-S.; Uhm, J.-S.; Pak, H.-N.; Lee, M.-H.; Joung, B. The trends of atrial fibrillation-related hospital visit and cost, treatment pattern and mortality in korea: 10-year nationwide sample cohort data. Korean Circ. J. 2017, 47, 56–64. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Yang, P.-S.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Pak, H.-N.; Lee, M.-H.; Joung, B.; et al. 10-year nationwide trends of the incidence, prevalence, and adverse outcomes of non-valvular atrial fibrillation nationwide health insurance data covering the entire Korean population. Am. Heart J. 2018, 202, 20–26. [Google Scholar] [CrossRef] [Green Version]
- Stewart, S.; Hart, C.; Hole, D.J.; McMurray, J.J. A population-based study of the long-term risks associated with atrial fibrillation: 20-year follow-up of the Renfrew/Paisley study. Am. J. Med. 2002, 113, 359–364. [Google Scholar] [CrossRef]
- Ott, A.; Breteler, M.; De Bruyne, M.C.; Van Harskamp, F.; Grobbee, D.E.; Hofman, A. Atrial fibrillation and dementia in a population-based study. The Rotterdam study. Stroke 1997, 28, 316–321. [Google Scholar] [CrossRef]
- Bunch, T.J.; Weiss, J.P.; Crandall, B.G.; May, H.; Bair, T.L.; Osborn, J.S.; Anderson, J.L.; Muhlestein, J.B.; Horne, B.D.; Lappé, N.L.; et al. Atrial fibrillation is independently associated with senile, vascular, and Alzheimer’s dementia. Heart Rhythm. 2010, 7, 433–437. [Google Scholar] [CrossRef]
- Dublin, S.; Anderson, M.L.; Haneuse, S.J.; Heckbert, S.R.; Crane, P.; Breitner, J.C.S.; McCormick, W.; Bowen, J.D.; Teri, L.; McCurry, S.M.; et al. Atrial fibrillation and risk of dementia: A prospective cohort study. J. Am. Geriatr. Soc. 2011, 59, 1369–1375. [Google Scholar] [CrossRef] [Green Version]
- Kim, D.; Yang, P.-S.; Yu, H.T.; Kim, T.-H.; Jang, E.; Sung, J.-H.; Pak, H.-N.; Lee, M.Y.; Lee, M.-H.; Lip, G.Y.H.; et al. Risk of dementia in stroke-free patients diagnosed with atrial fibrillation: Data from a population-based cohort. Eur. Heart J. 2019, 40, 2313–2323. [Google Scholar] [CrossRef] [Green Version]
- Gomez-Outes, A.; Lagunar-Ruíz, J.; Terleira-Fernández, A.-I.; Rojas, G.C.; Suárez-Gea, M.L.; Vargas-Castrillón, E. Causes of death in anticoagulated patients with atrial fibrillation. J. Am. Coll. Cardiol. 2016, 68, 2508–2521. [Google Scholar] [CrossRef]
- Fauchier, L.; Villejoubert, O.; Clementy, N.; Bernard, A.; Pierre, B.; Angoulvant, D.; Ivanes, F.; Babuty, D.; Lip, G.Y. Causes of death and influencing factors in patients with atrial fibrillation. Am. J. Med. 2016, 129, 1278–1287. [Google Scholar] [CrossRef]
- Kotecha, D.; Breithardt, G.; Camm, A.J.; Lip, G.Y.H.; Schotten, U.; Ahlsson, A.; Arnar, D.; Atar, D.; Auricchio, A.; Bax, J.; et al. Integrating new approaches to atrial fibrillation management: The 6th AFNET/EHRA Consensus Conference. Europace 2018, 20, 395–407. [Google Scholar] [CrossRef]
- Kirchhof, P.; Benussi, S.; Kotecha, D.; Ahlsson, A.; Atar, D.; Casadei, B.; Castellà, M.; Diener, H.-C.; Heidbuchel, H.; Hendriks, J.; et al. 2016 ESC guidelines for the management of atrial fibrillation developed in collaboration with EACTS. Eur. Heart J. 2016, 37, 2893–2962. [Google Scholar] [CrossRef] [Green Version]
- Joung, B.; Lee, J.M.; Lee, K.H.; Kim, T.-H.; Choi, E.-K.; Lim, W.-H.; Kang, K.-W.; Shim, J.; Lim, H.E.; Park, J.; et al. 2018 Korean guideline of atrial fibrillation management. Korean Circ. J. 2018, 48, 1033–1080. [Google Scholar] [CrossRef] [Green Version]
- Lip, G.Y.H. The ABC pathway: An integrated approach to improve AF management. Nat. Rev. Cardiol. 2017, 14, 627–628. [Google Scholar] [CrossRef]
- Proietti, M.; Romiti, G.F.; Olshansky, B.; Lane, D.A.; Lip, G.Y. Improved outcomes by integrated care of anticoagulated patients with atrial fibrillation using the simple ABC (Atrial Fibrillation Better Care) pathway. Am. J. Med. 2018, 131, 1359–1366.e6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pastori, D.; Pignatelli, P.; Menichelli, D.; Violi, F.; Lip, G.Y. Integrated care management of patients with atrial fibrillation and risk of cardiovascular events: The ABC (Atrial fibrillation Better Care) pathway in the ATHERO-AF study cohort. Mayo Clin. Proc. 2019, 94, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Yoon, M.; Yang, P.-S.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Sung, J.-H.; Pak, H.-N.; Lee, M.-H.; et al. Improved population-based clinical outcomes of patients with atrial fibrillation by compliance with the Simple ABC (Atrial Fibrillation Better Care) pathway for integrated care management: A nationwide cohort study. Thromb. Haemost. 2019, 119, 1695–1703. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Yang, P.-S.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Pak, H.-N.; Lee, M.-H.; Joung, B.; et al. Increasing trends in hospital care burden of atrial fibrillation in Korea, 2006 through 2015. Heart 2018, 104, 2010–2017. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.; Yang, P.-S.; Kim, T.-H.; Jang, E.; Shin, H.; Kim, H.Y.; Yu, H.T.; Uhm, J.-S.; Kim, J.-Y.; Pak, H.-N.; et al. Ideal blood pressure in patients with atrial fibrillation. J. Am. Coll. Cardiol. 2018, 72, 1233–1245. [Google Scholar] [CrossRef]
- Kim, T.H.; Yang, P.S.; Kim, D.; Yu, H.T.; Uhm, J.S.; Kim, J.Y.; Pak, H.N.; Lee, M.H.; Joung, B.; Lip, G.Y.H.; et al. CHA2DS2-VASc score for identifying truly low-risk atrial fibrillation for stroke: A Korean nationwide cohort study. Stroke 2017, 48, 2984–2990. [Google Scholar] [CrossRef]
- Kim, T.-H.; Yang, P.-S.; Uhm, J.-S.; Kim, J.-Y.; Pak, H.-N.; Lee, M.-H.; Joung, B.; Lip, G.Y. CHA 2 DS 2-VASc score (congestive heart failure, hypertension, age ≥75 [doubled], diabetes mellitus, prior stroke or transient ischemic attack [doubled], vascular disease, age 65–74, female) for stroke in Asian patients with atrial fibrillation: A Korean nationwide sample cohort study. Stroke 2017, 48, 1524–1530. [Google Scholar] [CrossRef]
- Kim, T.-H.; Yang, P.-S.; Yu, H.T.; Jang, E.; Shin, H.; Kim, H.Y.; Uhm, J.-S.; Kim, J.-Y.; Sung, J.-H.; Pak, H.-N.; et al. Effect of hypertension duration and blood pressure level on ischaemic stroke risk in atrial fibrillation: Nationwide data covering the entire Korean population. Eur. Heart J. 2019, 40, 809–819. [Google Scholar] [CrossRef] [Green Version]
- Wortmann, M. Dementia: A global health priority-highlights from an ADI and World Health Organization report. Alzheimer’s Res. Ther. 2012, 4, 40. [Google Scholar] [CrossRef] [Green Version]
- Gallagher, C.; Elliott, A.D.; Wong, C.X.; Rangnekar, G.; E Middeldorp, M.; Mahajan, R.; Lau, D.H.; Sanders, P.; Hendriks, J.M. Integrated care in atrial fibrillation: A systematic review and meta-analysis. Heart 2017, 103, 1947–1953. [Google Scholar] [CrossRef]
- Lip, G.Y.H.; Banerjee, A.; Boriani, G.; Chiang, C.E.; Fargo, R.; Freedman, B.; Lane, D.A.; Ruff, C.T.; Turakhia, M.; Werring, D.; et al. Antithrombotic therapy for atrial fibrillation: Chest guideline and expert panel report. Chest 2018, 154, 1121–1201. [Google Scholar] [CrossRef] [Green Version]
- Friberg, L.; Andersson, T.; Rosenqvist, M. Less dementia and stroke in low-risk patients with atrial fibrillation taking oral anticoagulation. Eur. Heart J. 2019, 40, 2327–2335. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kim, D.; Yang, P.-S.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Sung, J.-H.; Pak, H.-N.; Lee, M.-H.; et al. The optimal drug adherence to maximize the efficacy and safety of non-vitamin K antagonist oral anticoagulant in real-world atrial fibrillation patients. Europace 2019, 22, 547–557. [Google Scholar] [CrossRef]
- Lee, S.S.; Kong, K.A.; Kim, D.; Lim, Y.-M.; Yang, P.-S.; Yi, J.-E.; Kim, M.; Kwon, K.; Pyun, W.B.; Joung, B.; et al. Clinical implication of an impaired fasting glucose and prehypertension related to new onset atrial fibrillation in a healthy Asian population without underlying disease: A nationwide cohort study in Korea. Eur. Heart J. 2017, 38, 2599–2607. [Google Scholar] [CrossRef] [PubMed]
- Kim, D.; Yang, P.-S.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Sung, J.-H.; Pak, H.-N.; Lee, M.-H.; et al. Blood pressure control and dementia risk in midlife patients with atrial fibrillation. Hypertension 2020, 75, 1296–1304. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Non-ABC (n = 182,032) | ABC (n = 45,994) | p-Value | |
|---|---|---|---|
| Age, years | 64 (55–71) | 49 (41–57) | <0.001 |
| Female | 70,218 (38.6) | 18,016 (39.2) | 0.019 |
| Economic status | 12 (5,17) | 13 (6,17) | <0.001 |
| CHA2DS2-VASc score | 2 (1, 3) | 0 (0, 1) | <0.001 |
| mHAS-BLED score * | 2 (1, 3) | 0 (0, 1) | <0.001 |
| Charlson comorbidity index | 3 (1, 4) | 1 (0, 2) | <0.001 |
| Heart failure | 41,557 (22.8) | 627 (1.4) | <0.001 |
| Hypertension | 117,688 (64.7) | 2425 (5.3) | <0.001 |
| Diabetes | 35,819 (19.7) | 807 (1.8) | <0.001 |
| Myocardial infarction | 12,838 (7.1) | 157 (0.3) | <0.001 |
| Vascular disease | 27,489 (15.1) | 383 (0.8) | <0.001 |
| Chronic kidney disease | 6089 (3.3) | 358 (0.8) | <0.001 |
| Liver disease | 70,974 (39.0) | 13,365 (29.1) | <0.001 |
| Malignancy | 36,768 (20.2) | 6876 (14.9) | <0.001 |
| Hyperthyroidism | 16,121 (8.9) | 3498 (7.6) | <0.001 |
| Hypothyroidism | 13,870 (7.6) | 2629 (5.7) | <0.001 |
| COPD | 23,033 (12.7) | 1735 (3.8) | <0.001 |
| History of bleeding | 12,525 (6.9) | 1667 (3.6) | <0.001 |
| Medication | |||
| Oral anticoagulants (Baseline) | 5822 (3.2) | 1166 (2.5) | <0.001 |
| Oral anticoagulants (Follow-up) | 46,569 (25.6) | 7705 (16.8) | <0.001 |
| Antiplatelet agents | 68,141 (37.4) | 2339 (5.1) | <0.001 |
| Beta blocker | 59,148 (32.5) | 2794 (6.1) | <0.001 |
| Statin | 44,226 (24.3) | 2791 (6.1) | <0.001 |
| Calcium channel blocker | 69,697 (38.3) | 1664 (3.6) | <0.001 |
| ACE-inhibitor/ARB | 66,533 (36.6) | 1605 (3.5) | <0.001 |
| Antiarrhythmic drugs † | 7087 (3.9) | 544 (1.2) | <0.001 |
| Multivariable Adjustment | ||
|---|---|---|
| OR (95% CI) | p-Value | |
| Age (per 10-year increase) | 0.91 (0.90–0.91) | <0.001 |
| Female | 1.05 (1.05–1.05) | <0.001 |
| High economic status | 1.02 (1.01–1.02) | <0.001 |
| Heart failure | 0.97 (0.96–0.97) | <0.001 |
| Hypertension | 0.76 (0.76–0.76) | <0.001 |
| Diabetes | 0.93 (0.92–0.93) | <0.001 |
| Myocardial infarction | 0.96 (0.95–0.96) | <0.001 |
| Peripheral arterial disease | 0.97 (0.96–0.97) | <0.001 |
| Chronic kidney disease | 1.02 (1.01–1.03) | <0.001 |
| COPD | 1.02 (1.01–1.02) | <0.001 |
| Liver disease | 0.98 (0.98–0.98) | <0.001 |
| Malignancy | 1.02 (1.01–1.02) | <0.001 |
| Hyperthyroidism | 0.98 (0.98–0.99) | <0.001 |
| Hypothyroidism | 0.99 (0.99–1.00) | 0.011 |
| Intracranial hemorrhage | 0.97 (0.95–0.98) | <0.001 |
| Cases, n (%) | Event Rate (/100 Person-Years) | Age & Sex Adjusted HR (95% CI) | Adjusted HR (95% CI) * | |
|---|---|---|---|---|
| Dementia | ||||
| Non-ABC | 12,165 | 1.11 (1.09–1.13) | 1 (Reference) | 1 (Reference) |
| ABC | 538 | 0.17 (0.16–0.19) | 0.74 (0.68–0.81) | 0.80 (0.73–0.87) |
| Alzheimer’s dementia | ||||
| Non-ABC | 9731 | 0.88 (0.86–0.90) | 1 (Reference) | 1 (Reference) |
| ABC | 410 | 0.13 (0.12–0.14) | 0.74 (0.67–0.82) | 0.79 (0.71–0.88) |
| Vascular dementia | ||||
| Non-ABC | 1274 | 0.11 (0.11–0.12) | 1 (Reference) | 1 (Reference) |
| ABC | 72 | 0.02 (0.18–0.29) | 0.68 (0.53–0.88) | 0.76 (0.59–0.98) |
| Cases, n (%) | Event Rate (/100 Person-Years) | Age & Sex Adjusted HR (95% CI) | Adjusted HR (95% CI) * | |
|---|---|---|---|---|
| ≥70 years (n = 57,480) | ||||
| Non-ABC | 8186 | 3.05 (2.98–3.11) | 1 (Reference) | 1 (Reference) |
| ABC | 129 | 2.22 (1.86–2.64) | 0.83 (0.70–0.99) | 0.82 (0.69–0.98) |
| ≥60 and <70 years (n = 67,073) | ||||
| Non-ABC | 3415 | 0.89 (0.86–0.92) | 1 (Reference) | 1 (Reference) |
| ABC | 221 | 0.52 (0.45–0.59) | 0.86 (0.75–0.99) | 0.93 (0.81–1.08) |
| ≥50 and <60 years (n = 56,161) | ||||
| Non-ABC | 503 | 0.18 (0.17–0.20) | 1 (Reference) | 1 (Reference) |
| ABC | 147 | 0.15 (0.13–0.18) | 0.92 (0.77–1.11) | 1.05 (0.84–1.30) |
| <50 years (n = 47,312) | ||||
| Non-ABC | 61 | 0.03 (0.03–0.04) | 1 (Reference) | 1 (Reference) |
| ABC | 41 | 0.02 (0.02–0.03) | 0.86 (0.58–1.30) | 0.94 (0.58–1.54) |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Yang, P.-S.; Sung, J.-H.; Jang, E.; Yu, H.T.; Kim, T.-H.; Uhm, J.-S.; Kim, J.-Y.; Pak, H.-N.; Lee, M.-H.; Lip, G.Y.H.; et al. The Effect of Integrated Care Management on Dementia in Atrial Fibrillation. J. Clin. Med. 2020, 9, 1696. https://doi.org/10.3390/jcm9061696
Yang P-S, Sung J-H, Jang E, Yu HT, Kim T-H, Uhm J-S, Kim J-Y, Pak H-N, Lee M-H, Lip GYH, et al. The Effect of Integrated Care Management on Dementia in Atrial Fibrillation. Journal of Clinical Medicine. 2020; 9(6):1696. https://doi.org/10.3390/jcm9061696
Chicago/Turabian StyleYang, Pil-Sung, Jung-Hoon Sung, Eunsun Jang, Hee Tae Yu, Tae-Hoon Kim, Jae-Sun Uhm, Jong-Youn Kim, Hui-Nam Pak, Moon-Hyoung Lee, Gregory Y. H. Lip, and et al. 2020. "The Effect of Integrated Care Management on Dementia in Atrial Fibrillation" Journal of Clinical Medicine 9, no. 6: 1696. https://doi.org/10.3390/jcm9061696