Knowledge, Attitudes, Practices, and Burden During the COVID-19 Pandemic in People with Parkinson’s Disease in Germany

 , and
, and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants and Assessments
2.2. Statistical Analysis
3. Results
3.1. Description of the Cohort
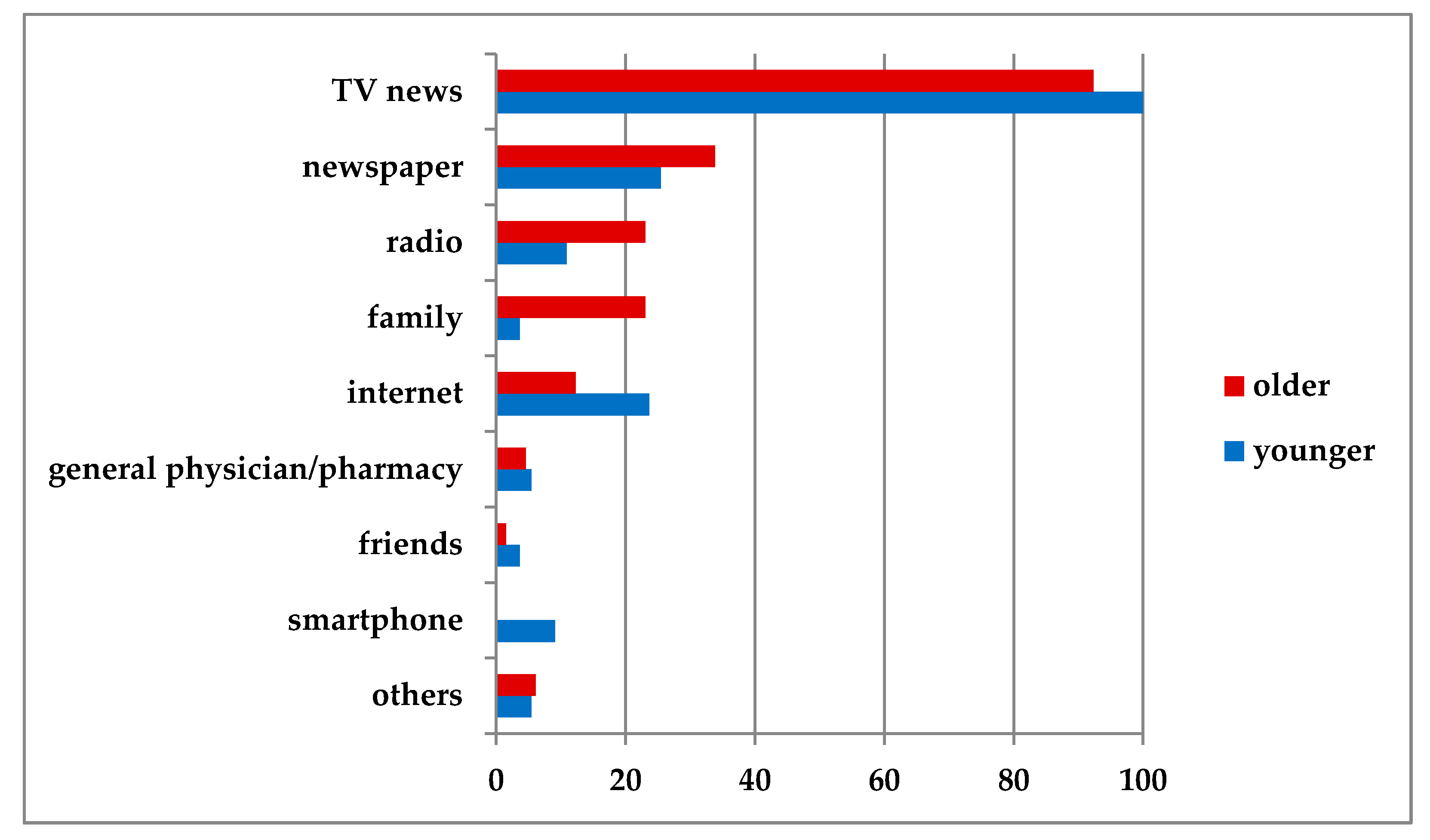
3.2. Knowledge
3.3. Attitudes
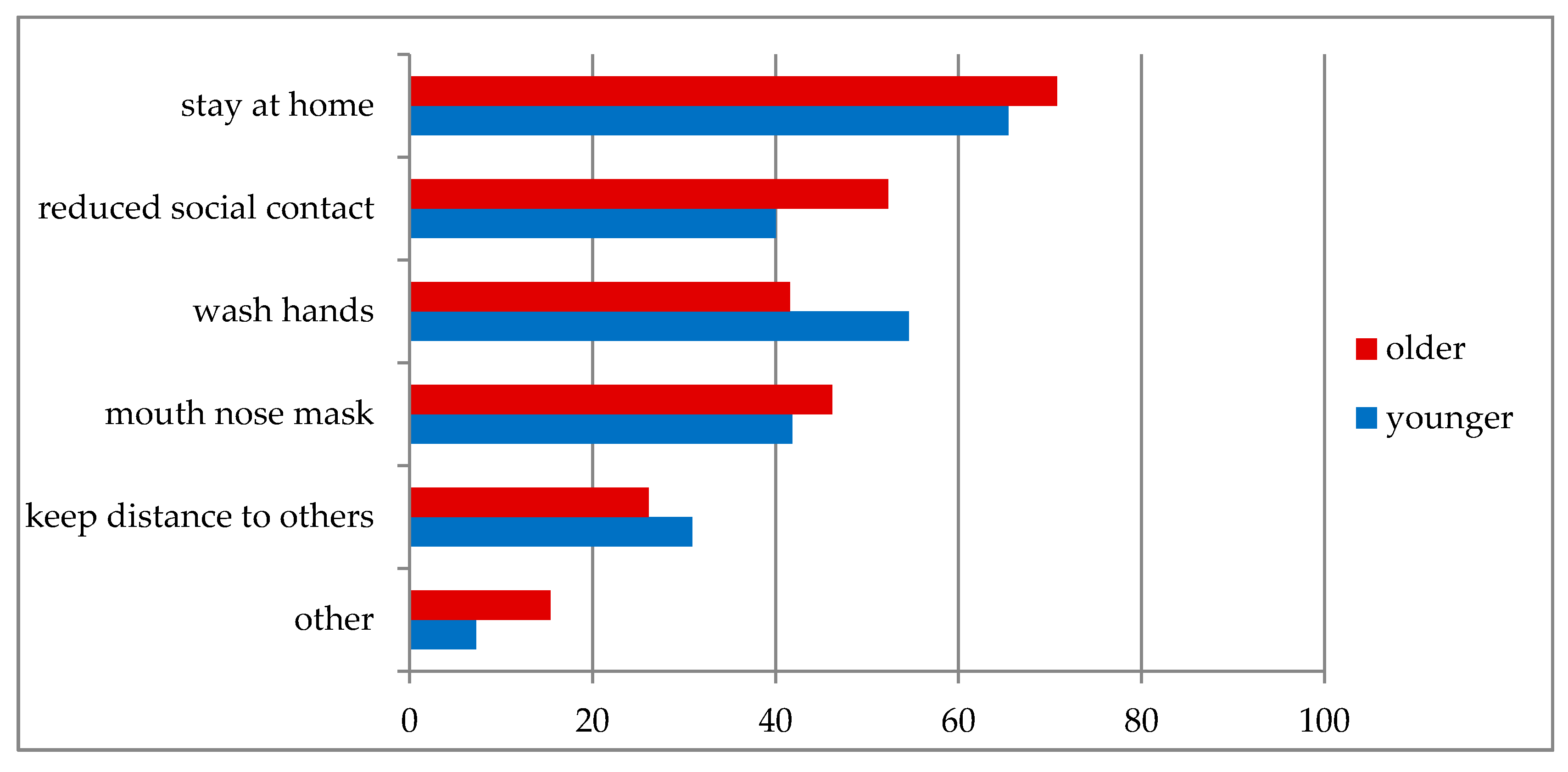
3.4. Practices
3.5. Burdens and Restrictions
3.6. Association between KAP and Clinical Parameters
3.7. Adherence to Preventive Measures
4. Discussion
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shahid, Z.; Bs, R.K.; Bs, B.M.; Kepko, D.; Bs, D.R.; Patel, R.; Mbbs, C.S.A.; Vunnam, R.R.; Sahu, N.; Bhatt, D.; et al. COVID-19 and Older Adults: What We Know. J. Am. Geriatr. Soc. 2020, 68, 926–929. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nascimento, I.J.B.D.; Cacic, N.; Abdulazeem, H.M.; von Groote, T.; Jayarajah, U.; Weerasekara, I.; Esfahani, M.A.; Civile, V.T.; Marušić, A.; Jeroncic, A.; et al. Novel Coronavirus Infection (COVID-19) in Humans: A Scoping Review and Meta-Analysis. J. Clin. Med. 2020, 9, 941. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Helmich, R.C.; Bloem, B.R. The Impact of the COVID-19 Pandemic on Parkinson’s Disease: Hidden Sorrows and Emerging Opportunities. J. Park. Dis. 2020, 10, 351–354. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Koo, J.R.; Cook, A.R.; Park, M.; Sun, Y.; Sun, H.; Lim, J.T.; Tam, C.; Dickens, B.L. Interventions to mitigate early spread of SARS-CoV-2 in Singapore: A modelling study. Lancet Infect. Dis. 2020. [Google Scholar] [CrossRef] [Green Version]
- Prem, K.; Liu, Y.; Russell, T.W.; Kucharski, A.J.; Eggo, R.M.; Davies, N.; Jit, M.; Klepac, P.; Flasche, S.; Clifford, S.; et al. The effect of control strategies to reduce social mixing on outcomes of the COVID-19 epidemic in Wuhan, China: A modelling study. Lancet Public Health 2020, 5, 261–270. [Google Scholar] [CrossRef] [Green Version]
- Tachfouti, N.; Slama, K.; Berraho, M.; Nejjari, C. The impact of knowledge and attitudes on adherence to tuberculosis treatment: A case-control study in a Moroccan region. Pan Afr. Med. J. 2012, 12, 52. [Google Scholar] [PubMed]
- Person, B.; Sy, F.; Holton, K.; Govert, B.; Liang, A.; Garza, B.; Gould, D.; Hickson, M.; McDonald, M.; Meijer, C.; et al. Fear and Stigma: The Epidemic within the SARS Outbreak. Emerg. Infect. Dis. 2004, 10, 358–363. [Google Scholar] [CrossRef]
- Zhong, B.-L.; Luo, W.; Li, H.-M.; Zhang, Q.-Q.; Liu, X.-G.; Li, W.-T.; Li, Y. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: A quick online cross-sectional survey. Int. J. Boil. Sci. 2020, 16, 1745–1752. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S. Parkinson’s disease and COVID-19: Perceptions and implications in patients and caregivers. Mov. Disord. 2020. [Google Scholar] [CrossRef] [PubMed]
- Nasreddine, Z.S.; Phillips, N.A.; Badirian, V.; Charbonneau, S.; Whitehead, V.; Collin, I.; Cummings, J.L.; Chertkow, H.; Bédirian, V. The Montreal Cognitive Assessment, MoCA: A Brief Screening Tool for Mild Cognitive Impairment. J. Am. Geriatr. Soc. 2005, 53, 695–699. [Google Scholar] [CrossRef] [PubMed]
- Goetz, C.G. Movement Disorder Society-sponsored revision of the Unified Parkinson’s Disease Rating Scale (MDS-UPDRS): Process, format, and clinimetric testing plan. Mov. Disord. 2007, 22, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Chaudhuri, K.R. International multicenter pilot study of the first comprehensive self-completed nonmotor symptoms questionnaire for Parkinson’s disease: The NMSQuest study. Mov. Disord. 2006, 21, 916–923. [Google Scholar] [CrossRef] [PubMed]
- Romenets, S.R.; Wolfson, C.; Galatas, C.; Pelletier, A.; Altman, R.; Wadup, L.; Postuma, R.B. Validation of the non-motor symptoms questionnaire (NMS-Quest). Park. Relat. Disord. 2012, 18, 54–58. [Google Scholar] [CrossRef] [PubMed]
- Prell, T.; Schaller, D.; Perner, C.; Franke, G.H.; Witte, O.W.; Kunze, A.; Grosskreutz, J. Comparison of anonymous versus nonanonymous responses to a medication adherence questionnaire in patients with Parkinson’s disease. Patient Prefer. Adher. 2019, 13, 151–155. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Prell, T.; Grosskreutz, J.; Mendorf, S.; Franke, G.H.; Witte, O.W.; Kunze, A. Clusters of non-adherences to medication in neurological patients. Res. Soc. Adm. Pharm. 2019, 15, 1419–1424. [Google Scholar] [CrossRef] [PubMed]
- Prell, T.; Grosskreutz, J.; Mendorf, S.; Witte, O.W.; Kunze, A. Data on adherence to medication in neurological patients using the German Stendal Adherence to Medication Score (SAMS). Data Brief 2019, 23, 103855. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Control | PD Older | PD Younger | ||||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | p | ||
| Gender | female | 6 | 28.6 | 22 | 38.6 | 13 | 31.0 | 0.612 |
| male | 15 | 71.4 | 35 | 61.4 | 29 | 69.0 | ||
| Marital state | married | 15 | 71.4 | 47 | 83.9 | 33 | 80.5 | 0.077 |
| divorced/widowed | 2 | 9.5 | 7 | 12. | 7 | 17.1 | ||
| single | 4 | 19.0 | 2 | 3.6 | 1 | 2.4 | ||
| Living situation | with others/relatives | 15 | 71.4 | 48 | 84.2 | 37 | 88.1 | 0.239 |
| alone | 6 | 28.6 | 9 | 15.8 | 5 | 11.9 | ||
| Education level | low | 8 a | 38.1 | 13 a | 22.8 | 6 a | 14.3 | 0.011 |
| middle | 6 a,b | 28.6 | 13 a | 22.8 | 22 b | 52.4 | ||
| high | 7 a | 33.3 | 31 a | 54.4 | 14 a | 33.3 | ||
| Occupation | pensioned | 13 a | 61.9 | 57 | 100.0 | 38 b | 90.5 | <0.001 |
| employed | 7 a | 33.3 | 0 | 0.0 | 2 b | 4.8 | ||
| unemployed | 1 a | 4.8 | 0 | 0.0 | 2 a | 4.8 | ||
| M | 95%CI | M | 95%CI | M | 95%CI | |||
| Age (years) + | 68.0 | 64.0, 78.0 | 78.0 | 77.0, 79.0 | 65.5 | 63.0, 68.0 | <0.001 | |
| BDI + | 7.0 | 3.0, 9.0 | 9.0 | 8.0, 13.0 | 11.0 | 10.0, 14.0 | 0.001 | |
| MoCa + | 24.0 | 23.0, 26.0 | 22.0 | 22.0, 23.0 | 25.0 | 25.0, 27.0 | <0.001 | |
| MDS-UPDRS III + | 30.0 | 30.0, 38.0 | 22.0 | 21.0, 33.0 | 0.06 | |||
| NMSQ * | 10.4 | 9.0, 11.7 | 10.5 | 9.2, 11.9 | 0.87 | |||
| SAMS + | 5.0 | 5.0, 8.0 | 6.0 | 4.0, 9.0 | 5.0 | 4.0, 9.0 | 0.69 | |
| Control | PD Older | PD Younger | ||||||
|---|---|---|---|---|---|---|---|---|
| n | % | n | % | n | % | p | ||
| Knowledge | ||||||||
| Information | Very well-informed | 10 a | 47.6 | 19 a | 35.2 | 13 a | 31.0 | 0.022 |
| Well-informed | 5 a | 23.8 | 21 a | 38.9 | 17 a | 40.5 | ||
| Sufficiently informed | 0 | 0.0 | 11 a | 20.4 | 5 a | 11.9 | ||
| Poorly informed | 1 a | 4.8 | 3 a | 5.6 | 2 a | 4.8 | ||
| Excessively informed | 5 a | 23.8 | 0 b | 0.0 | 5 a | 11.9 | ||
| Active search for additional information | Yes | 6 a | 28.6 | 22 a,b | 39.3 | 25 b | 61.0 | 0.027 |
| No | 15 a | 71.4 | 34 a,b | 60.9 | 16 b | 39.0 | ||
| Advice from family to remain at home | Yes | 14 | 77.8 | 37 | 67.3 | 24 | 57.1 | 0.427 |
| No | 4 | 22.2 | 17 | 30.9 | 18 | 42.9 | ||
| No Family | 0 | 0.0 | 1 | 1.8 | 0 | 0.0 | ||
| Familiar with RKI | Yes | 15 a,b | 71.4 | 33 a | 57.9 | 34 b | 81.0 | 0.048 |
| No | 6 a,b | 28.6 | 24 a | 42.1 | 8 b | 19.0 | ||
| Can correctly describe aims of measures | Yes | 10 | 47.6 | 39 | 68.4 | 30 | 71.4 | 0.146 |
| No | 11 | 52.4 | 18 | 31.6 | 12 | 28.6 | ||
| Attitude | ||||||||
| Virus perceived as dangerous | Yes | 14 a | 66.7 | 55 b | 96.5 | 39 b | 97.5 | 0.000 |
| No | 7 a | 33.3 | 2 b | 3.5 | 1 b | 2.5 | ||
| Current restrictions perceived as | Necessary | 16 | 76.2 | 47 | 85.5 | 34 | 81.0 | 0.670 |
| Sufficient | 4 | 19.0 | 7 | 12.7 | 5 | 11.9 | ||
| Excessive | 1 | 4.8 | 1 | 1.8 | 3 | 7.1 | ||
| Situation perceived as threatening | Yes | 12 | 57.1 | 37 | 67.3 | 26 | 65.0 | 0.710 |
| No | 9 | 42.9 | 18 | 32.7 | 14 | 35.0 | ||
| Reporting of fears/worries | Yes | 12 | 57.1 | 32 | 56.1 | 26 | 61.9 | 0.656 |
| No | 9 | 42.9 | 23 | 40.4 | 16 | 38.1 | ||
| Practices | ||||||||
| Change in behaviour | Yes | 18 | 85.7 | 38 | 67.9 | 34 | 81.0 | 0.162 |
| No | 3 | 14.3 | 18 | 32.1 | 8 | 19.0 | ||
| Reduction of social contacts/remaining at home | Yes | 21 | 100.0 | 48 | 87.3 | 38 | 90.5 | 0.233 |
| No | 0 | 0.0 | 7 | 12.7 | 4 | 9.5 | ||
| Grandchildren | Yes | 14 | 66.7 | 44 | 80.0 | 29 | 70.7 | 0.396 |
| No | 7 | 33.3 | 11 | 20.0 | 12 | 29.3 | ||
| Personal contact with Grandchildren | Yes | 1 | 7.7 | 6 a | 13.6 | 6 | 20.7 | 0.390 |
| No | 11 | 84.6 | 31 | 70.5 | 22 | 75.9 | ||
| No regardless of corona virus | 1 | 7.7 | 7 | 15.9 | 1 | 3.4 | ||
| Burden | ||||||||
| Affliction because of discontinued contact | Yes | 9 | 64.3 | 22 | 50.0 | 17 | 58.6 | 0.807 |
| No | 3 | 21.4 | 9 | 20.5 | 5 | 17.2 | ||
| Daily life restricted | Yes | 14 | 66.7 | 27 | 49.1 | 27 | 64.3 | 0.212 |
| No | 7 | 33.3 | 28 | 50.9 | 15 | 35.7 | ||
| Mobility deteriorated | Yes | 3 | 14.3 | 15 | 27.3 | 16 | 38.1 | 0.136 |
| No | 18 | 85.7 | 40 | 72.7 | 26 | 61.9 | ||
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zipprich, H.M.; Teschner, U.; Witte, O.W.; Schönenberg, A.; Prell, T. Knowledge, Attitudes, Practices, and Burden During the COVID-19 Pandemic in People with Parkinson’s Disease in Germany. J. Clin. Med. 2020, 9, 1643. https://doi.org/10.3390/jcm9061643
Zipprich HM, Teschner U, Witte OW, Schönenberg A, Prell T. Knowledge, Attitudes, Practices, and Burden During the COVID-19 Pandemic in People with Parkinson’s Disease in Germany. Journal of Clinical Medicine. 2020; 9(6):1643. https://doi.org/10.3390/jcm9061643
Chicago/Turabian StyleZipprich, Hannah M., Ulrike Teschner, Otto W. Witte, Aline Schönenberg, and Tino Prell. 2020. "Knowledge, Attitudes, Practices, and Burden During the COVID-19 Pandemic in People with Parkinson’s Disease in Germany" Journal of Clinical Medicine 9, no. 6: 1643. https://doi.org/10.3390/jcm9061643