Relationship between HIF-1 and Circadian Clock Proteins in Obstructive Sleep Apnea Patients—Preliminary Study


Abstract
:1. Introduction
2. Materials and Methods
2.1. Sample
2.2. Material Collection and Protein Level Assessment
2.3. Statistical Analysis
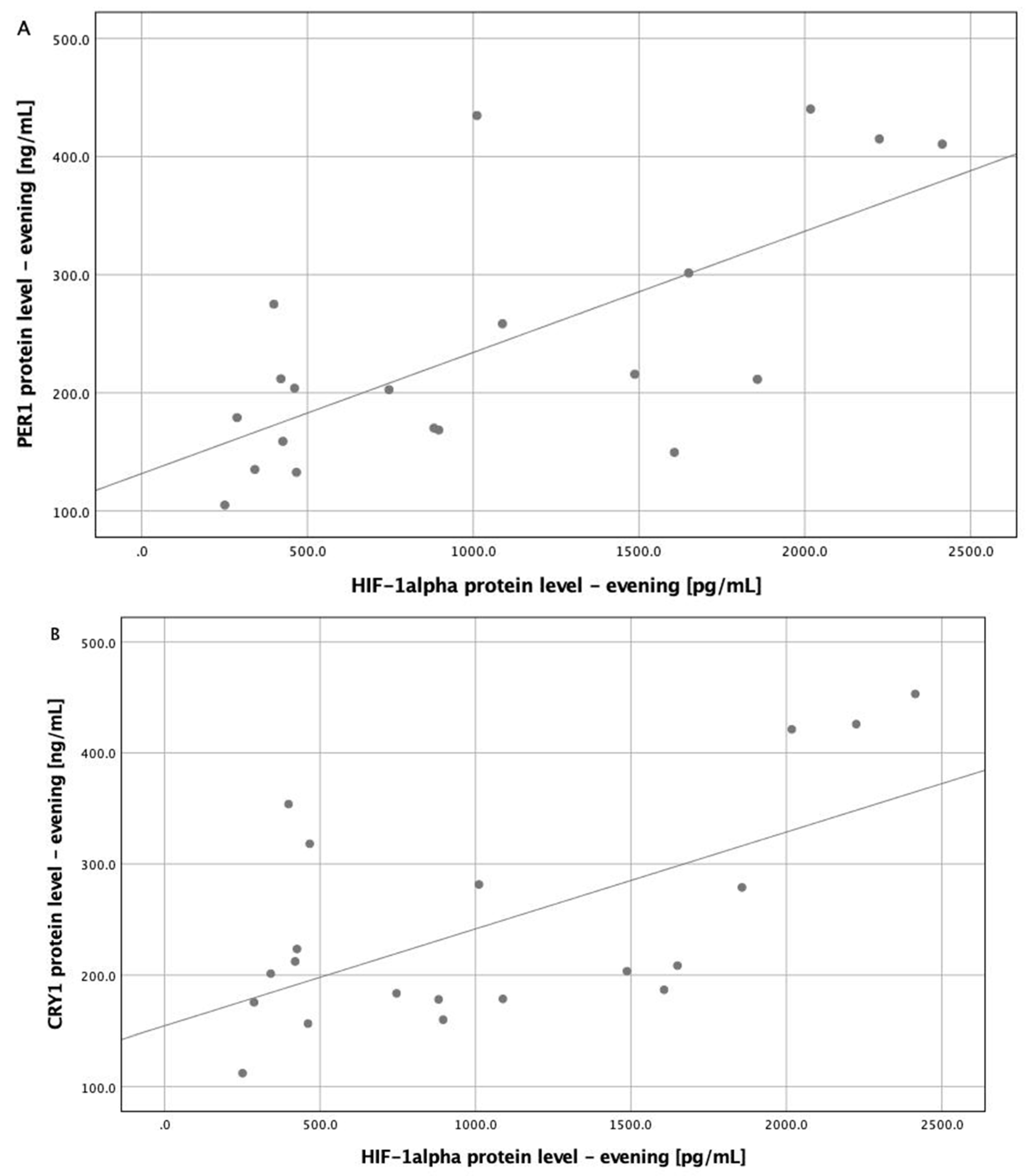
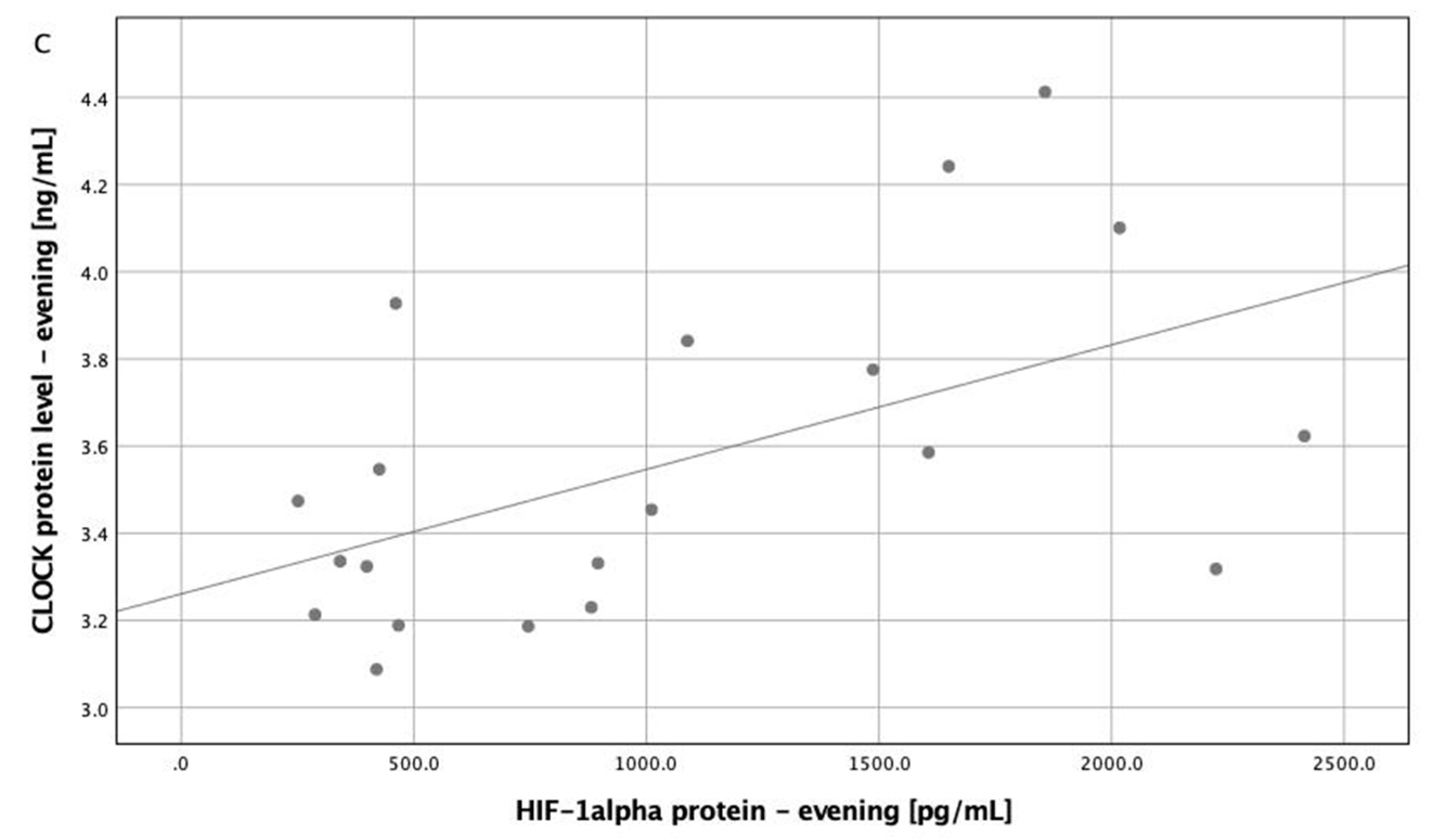
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Heinzer, R.; Vat, S.; Marques-Vidal, P.; Marti-Soler, H.; Andries, D.; Tobback, N.; Mooser, V.; Preisig, M.; Malhotra, A.; Waeber, G.; et al. Prevalence of sleep-disordered breathing in the general population: The HypnoLaus study. Lancet Respir. Med. 2015, 3, 310–318. [Google Scholar] [CrossRef] [Green Version]
- Semenza, G.L. Hypoxia-inducible factors in physiology and medicine. Cell 2012, 148, 399–408. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabryelska, A.; Szmyd, B.; Panek, M.; Szemraj, J.; Kuna, P.; Białasiewicz, P. Serum hypoxia-inducible factor-1α protein level as a diagnostic marker of obstructive sleep apnea. Pol. Arch. Intern. Med. 2020, 130, 158–160. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gabryelska, A.; Stawski, R.; Sochal, M.; Szmyd, B.; Białasiewicz, P. Influence of one-night CPAP therapy on the changes of HIF-1α protein in OSA patients—A pilot study. J. Sleep Res. 2020. [Google Scholar] [CrossRef] [PubMed]
- Takahashi, J.S. Transcriptional architecture of the mammalian circadian clock. Nat. Rev. Genet. 2017, 18, 164–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Burioka, N.; Koyanagi, S.; Endo, M.; Takata, M.; Fukuoka, Y.; Miyata, M.; Takeda, K.; Chikumi, H.; Ohdo, S.; Shimizu, E. Clock gene dysfunction in patients with obstructive sleep apnoea syndrome. Eur. Respir. J. 2008, 32, 105–112. [Google Scholar] [CrossRef] [PubMed]
- Moreira, S.; Rodrigues, R.; Barros, A.B.; Pejanovic, N.; Neves-Costa, A.; Pedroso, D.; Pereira, C.; Fernandes, D.; Rodrigues, J.V.; Barbara, C.; et al. Changes in Expression of the CLOCK Gene in Obstructive Sleep Apnea Syndrome Patients Are Not Reverted by Continuous Positive Airway Pressure Treatment. Front. Med. (Lausanne) 2017, 4, 187. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kapur, V.K.; Auckley, D.H.; Chowdhuri, S.; Kuhlmann, D.C.; Mehra, R.; Ramar, K.; Harrod, C.G. Clinical Practice Guideline for Diagnostic Testing for Adult Obstructive Sleep Apnea: An American Academy of Sleep Medicine Clinical Practice Guideline. JCSM 2017, 13, 479–504. [Google Scholar] [CrossRef] [PubMed]
- Gabryelska, A.; Łukasik, Z.M.; Makowska, J.S.; Białasiewicz, P. Obstructive Sleep Apnea: From Intermittent Hypoxia to Cardiovascular Complications via Blood Platelets. Front. Neurol. 2018, 9, 635. [Google Scholar] [CrossRef] [PubMed]
- Yang, M.-Y.; Lin, P.-W.; Lin, H.-C.; Lin, P.-M.; Chen, I.-Y.; Friedman, M.; Hung, C.-F.; Salapatas, A.M.; Lin, M.-C.; Lin, S.-F. Alternations of Circadian Clock Genes Expression and Oscillation in Obstructive Sleep Apnea. J. Clin. Med. 2019, 8, 1634. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Canales, M.T.; Holzworth, M.; Bozorgmehri, S.; Ishani, A.; Weiner, I.D.; Berry, R.B.; Beyth, R.J.; Gumz, M. Clock gene expression is altered in veterans with sleep apnea. Physiol. Genom. 2019, 51, 77–82. [Google Scholar] [CrossRef] [PubMed]
- Firsov, D.; Bonny, O. Circadian rhythms and the kidney. Nat. Rev. Nephrol. 2018, 14, 626–635. [Google Scholar] [CrossRef] [PubMed]
- Adamovich, Y.; Ladeuix, B.; Golik, M.; Koeners, M.P.; Asher, G. Rhythmic Oxygen Levels Reset Circadian Clocks through HIF1α. Cell Metab. 2017, 25, 93–101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Manella, G.; Aviram, R.; Bolshette, N.; Muvkadi, S.; Golik, M.; Smith, D.F.; Asher, G. Hypoxia induces a time- and tissue-specific response that elicits intertissue circadian clock misalignment. Proc. Natl. Acad. Sci. USA 2020, 117, 779–786. [Google Scholar] [CrossRef] [PubMed]
- Chilov, D.; Hofer, T.; Bauer, C.; Wenger, R.H.; Gassmann, M. Hypoxia affects expression of circadian genes PER1 and CLOCK in mouse brain. FASEB J. 2001, 15, 2613–2622. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| OSA Group (n = 10) | Control Group (n = 10) | p Value | |
|---|---|---|---|
| Age (years) | 50.30 ± 9.75 | 49.00 ± 10.19 | 0.774 |
| BMI (kg/m2) | 34.48 ± 2.95 | 28.1 ± 4.1 | 0.001 |
| Sex | 90%M | 70%M | 0.264 |
| HIF-1α evening (pg/mL) | 1287.64 (452.31–2069.13) | 606.45 (327.97–1073.51) | 0.020 |
| HIF-1α morning (pg/mL) | 1236.97 ± 871.44 | 742.06 ± 450.65 | 0.043 |
| HIF-1β evening (ng/mL) | 72.59 ± 0.94 | 71.50 ± 1.32 | 0.047 |
| HIF-1β morning (ng/mL) | 72.38 ± 1.08 | 71.26 ± 1.65 | 0.091 |
| CLOCK evening (ng/mL) | 3.73 ± 0.35 | 3.38 ± 0.33 | 0.037 |
| CLOCK morning (ng/mL) | 3.52 ± 0.15 | 3.31 ± 0.20 | 0.019 |
| BMAL1 evening (ng/mL) | 9.32 ± 0.51 | 9.00 ± 0.40 | 0.132 |
| BMAL1 morning (ng/mL) | 9.52 ± 0.47 | 8.87 ± 0.61 | 0.016 |
| PER1 evening (ng/mL) | 266.75 (209.54–419.87) | 169.32 (134.50–204.97) | 0.004 |
| PER1 morning (ng/mL) | 38.01 (30.05–68.96) | 23.84 (18.22–38.39) | 0.029 |
| CRY1 evening (ng/mL) | 280.26 (197.31–422.36) | 185.21 (171.59–209.50) | 0.035 |
| CRY1 morning (ng/mL) | 39.38 (30.55–43.43) | 27.95 (15.97–40.84) | 0.105 |
| TST (h) | 6.43 ± 0.83 | 6.08 ± 0.68 | 0.321 |
| Percentage of time of TST spent in REM stage (%) | 19.03 ± 7.01 | 20.85 ± 8.09 | 0.597 |
| Arousal Index | 24.80 (20.15–34.18) | 15.20 (6.73–19.75) | 0.005 |
| AHI | 56.40 (44.98–65.33) | 1.30 (0.38–3.00) | <0.001 |
| AHI REM | 29.81 (17.11–56.67) | 0.00 (0.00–4.88) | <0.001 |
| AHI nREM | 46.99 (33.54–64.91) | 1.07 (0.20–1.42) | <0.001 |
| ODI | 57.85 (45.00–84.83) | 2.00 (0.98–3.00) | <0.001 |
| Awake SpO2 | 89.85 (83.65–93.60) | 93.85 (92.45–94.85) | 0.005 |
| Mean SpO2 of desaturation | 84.60 (74.50–89.73) | 91.75 (90.35–92.90) | <0.001 |
| Minimal SpO2 | 63.45 (40.85–75.18) | 88.90 (84.73–91.90) | <0.001 |
| Time spent with SpO2 below 90% (min) | 107.95 (73.05–278.58) | 0.55 (0.00–5.50) | <0.001 |
| Percentage of time with SpO2 90% (%) | 27.96 (20.44–64.69) | 0.15 (0.00–1.48) | <0.001 |
| Corrected Model | HIF-1α Protein Level-Evening | AHI | ODI | BMI | |||
|---|---|---|---|---|---|---|---|
| p Value | R Squared | p Value | |||||
| Protein Level | Multivariate General Linear Model | - | 0.025 | 0.123 | 0.131 | 1.505 | |
| CLOCK evening | 0.046 | 0.455 | 0.056 | 0.064 | 0.074 | 0.699 | |
| CLOCK morning | 0.059 | 0.435 | 0.654 | 0.086 | 0.356 | 0.115 | |
| BMAL1 evening | 0.707 | 0.126 | 0.687 | 0.387 | 0.596 | 0.415 | |
| BMAL1 morning | 0.057 | 0.438 | 0.143 | 0.795 | 0.674 | 0.321 | |
| PER1 evening | 0.008 | 0.583 | 0.020 | 0.379 | 0.627 | 0.784 | |
| PER1 morning | 0.006 | 0.593 | 0.972 | 0.012 | 0.003 | 0.662 | |
| CRY1 evening | 0.043 | 0.461 | 0.052 | 0.903 | 0.706 | 0.707 | |
| CRY1 morning | 0.487 | 0.194 | 0.629 | 0.604 | 0.746 | 0.400 | |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Gabryelska, A.; Sochal, M.; Turkiewicz, S.; Białasiewicz, P. Relationship between HIF-1 and Circadian Clock Proteins in Obstructive Sleep Apnea Patients—Preliminary Study. J. Clin. Med. 2020, 9, 1599. https://doi.org/10.3390/jcm9051599
Gabryelska A, Sochal M, Turkiewicz S, Białasiewicz P. Relationship between HIF-1 and Circadian Clock Proteins in Obstructive Sleep Apnea Patients—Preliminary Study. Journal of Clinical Medicine. 2020; 9(5):1599. https://doi.org/10.3390/jcm9051599
Chicago/Turabian StyleGabryelska, Agata, Marcin Sochal, Szymon Turkiewicz, and Piotr Białasiewicz. 2020. "Relationship between HIF-1 and Circadian Clock Proteins in Obstructive Sleep Apnea Patients—Preliminary Study" Journal of Clinical Medicine 9, no. 5: 1599. https://doi.org/10.3390/jcm9051599