Liver Transplant Patients with High Preoperative Serum Bilirubin Levels Are at Increased Risk of Postoperative Delirium: A Retrospective Study

 , ,
, ,
Abstract
:1. Introduction
2. Experimental Section
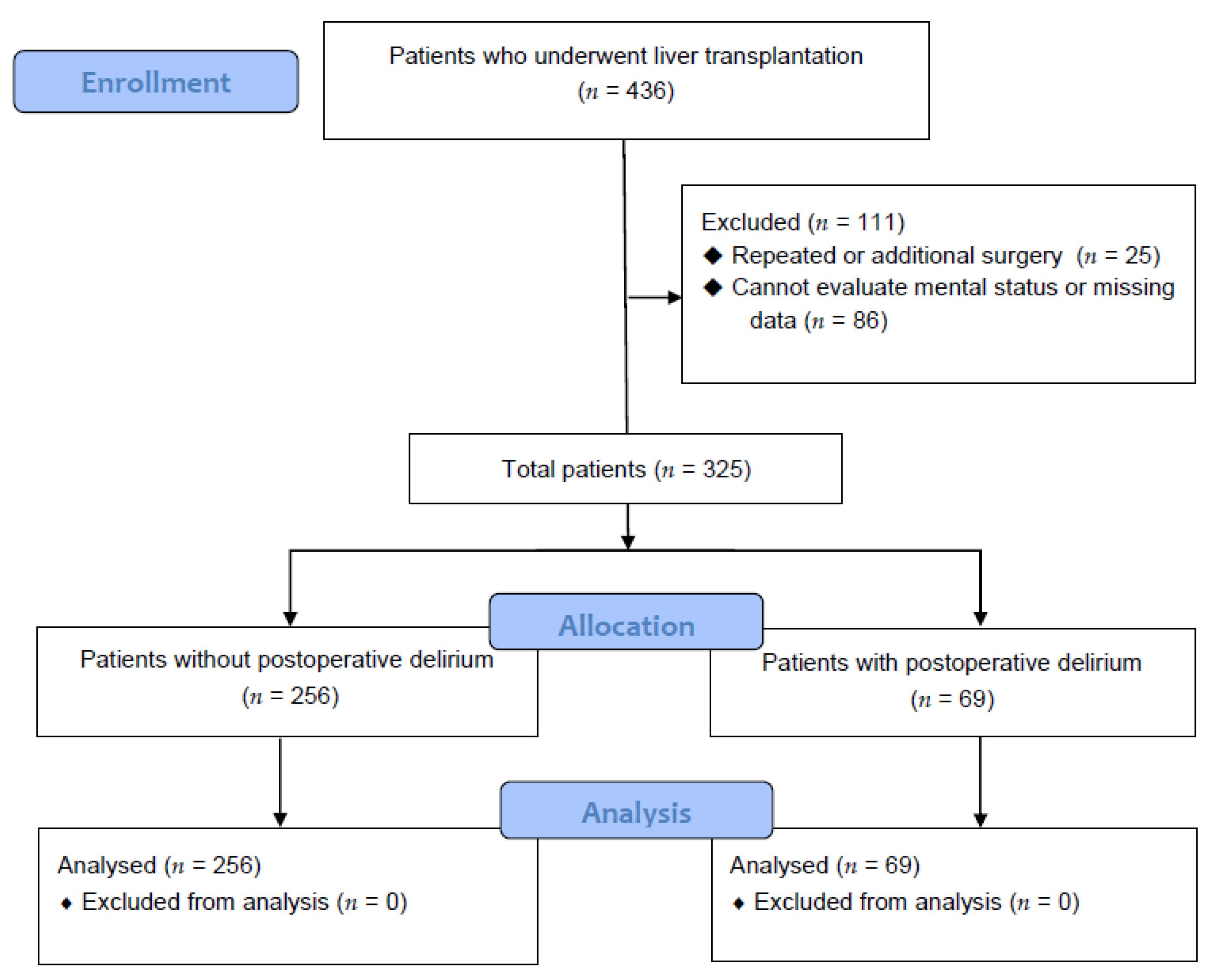
2.1. Patient Population
2.2. Data Collection
2.3. Definition of Delirium
2.4. Intraoperative Protocol
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Lewis, M.B.; Howdle, P.D. Neurologic complications of liver transplantation in adults. Neurology 2003, 61, 1174–1178. [Google Scholar] [CrossRef] [PubMed]
- Vizzini, G.; Asaro, M.; Miraglia, R.; Gruttadauria, S.; Fili, D.; D’Antoni, A.; Petridis, I.; Marrone, G.; Pagano, D.; Gridelli, B. Changing picture of central nervous system complications in liver transplant recipients. Liver Transpl. 2011, 17, 1279–1285. [Google Scholar] [CrossRef] [PubMed]
- Pinero, F.; Cheang, Y.; Mendizabal, M.; Cagliani, J.; Gonzalez Campana, A.; Pages, J.; Colaci, C.; Barreiro, M.; Alonso, C.; Malla, I.; et al. Incidence, risk factors, and outcomes related with neurological events after liver transplantation in adult and pediatric recipients. Pediatr. Transplant. 2018, 22, e13159. [Google Scholar] [CrossRef] [PubMed]
- Amodio, P. Hepatic encephalopathy: Diagnosis and management. Liver Int. 2018, 38, 966–975. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rompianesi, G.; Montalti, R.; Cautero, N.; De Ruvo, N.; Stafford, A.; Bronzoni, C.; Ballarin, R.; De Pietri, L.; Di Benedetto, F.; Gerunda, G.E. Neurological complications after liver transplantation as a consequence of immunosuppression: Univariate and multivariate analysis of risk factors. Transpl. Int. 2015, 28, 864–869. [Google Scholar] [CrossRef] [PubMed]
- Balderramo, D.; Prieto, J.; Cardenas, A.; Navasa, M. Hepatic encephalopathy and post-transplant hyponatremia predict early calcineurin inhibitor-induced neurotoxicity after liver transplantation. Transpl. Int. 2011, 24, 812–819. [Google Scholar] [CrossRef]
- Chiu, N.M.; Chen, C.L.; Cheng, A.T. Psychiatric consultation for post-liver-transplantation patients. Psychiatry Clin. Neurosci. 2009, 63, 471–477. [Google Scholar] [CrossRef]
- Lescot, T.; Karvellas, C.J.; Chaudhury, P.; Tchervenkov, J.; Paraskevas, S.; Barkun, J.; Metrakos, P.; Goldberg, P.; Magder, S. Postoperative delirium in the intensive care unit predicts worse outcomes in liver transplant recipients. Can. J. Gastroenterol. 2013, 27, 207–212. [Google Scholar] [CrossRef]
- Lee, H.; Oh, S.Y.; Yu, J.H.; Kim, J.; Yoon, S.; Ryu, H.G. Risk Factors of Postoperative Delirium in the Intensive Care Unit After Liver Transplantation. World J. Surg. 2018, 42, 2992–2999. [Google Scholar] [CrossRef]
- Mancuso, C. Bilirubin and brain: A pharmacological approach. Neuropharmacology 2017, 118, 113–123. [Google Scholar] [CrossRef]
- Dennery, P.A.; Seidman, D.S.; Stevenson, D.K. Neonatal hyperbilirubinemia. N. Engl. J. Med. 2001, 344, 581–590. [Google Scholar] [CrossRef] [PubMed]
- Yang, S.; Gu, C.; Mandeville, E.T.; Dong, Y.; Esposito, E.; Zhang, Y.; Yang, G.; Shen, Y.; Fu, X.; Lo, E.H.; et al. Anesthesia and Surgery Impair Blood-Brain Barrier and Cognitive Function in Mice. Front. Immunol. 2017, 8, 902. [Google Scholar] [CrossRef] [PubMed]
- Belcher, J.M.; Garcia-Tsao, G.; Sanyal, A.J.; Bhogal, H.; Lim, J.K.; Ansari, N.; Coca, S.G.; Parikh, C.R. Association of AKI with mortality and complications in hospitalized patients with cirrhosis. Hepatology 2013, 57, 753–762. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yoon, J.S.; Kim, Y.R.; Choi, J.W.; Ko, J.S.; Gwak, M.S.; Kim, G.S. Risk factors of postoperative delirium following liver transplantation. Korean J. Anesthesiol. 2009, 57, 584–589. [Google Scholar] [CrossRef] [PubMed]
- Pandharipande, P.P.; Girard, T.D.; Jackson, J.C.; Morandi, A.; Thompson, J.L.; Pun, B.T.; Brummel, N.E.; Hughes, C.G.; Vasilevskis, E.E.; Shintani, A.K.; et al. Long-term cognitive impairment after critical illness. N. Eng. J. Med. 2013, 369, 1306–1316. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Jackson, J.C.; Ely, E.W. Cognitive impairment after critical illness: Etiologies, risk factors, and future directions. Semin. Respir. Critic. Care Med. 2013, 34, 216–222. [Google Scholar] [CrossRef]
- Wiesner, R.; Edwards, E.; Freeman, R.; Harper, A.; Kim, R.; Kamath, P.; Kremers, W.; Lake, J.; Howard, T.; Merion, R.M.; et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterology 2003, 124, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Watchko, J.F.; Tiribelli, C. Bilirubin-induced neurologic damage—Mechanisms and management approaches. N. Engl. J. Med. 2013, 369, 2021–2030. [Google Scholar] [CrossRef]
- Hanko, E.; Tommarello, S.; Watchko, J.F.; Hansen, T.W. Administration of drugs known to inhibit P-glycoprotein increases brain bilirubin and alters the regional distribution of bilirubin in rat brain. Pediatr. Res. 2003, 54, 441–445. [Google Scholar] [CrossRef] [Green Version]
- Ghersi-Egea, J.F.; Gazzin, S.; Strazielle, N. Blood-brain interfaces and bilirubin-induced neurological diseases. Curr. Pharm. Des. 2009, 15, 2893–2907. [Google Scholar] [CrossRef]
- Boettger, S.; Nunez, D.G.; Meyer, R.; Richter, A.; Fernandez, S.F.; Rudiger, A.; Schubert, M.; Jenewein, J. Delirium in the intensive care setting: A reevaluation of the validity of the CAM-ICU and ICDSC versus the DSM-IV-TR in determining a diagnosis of delirium as part of the daily clinical routine. Palliat. Support. Care 2017, 15, 675–683. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Control Group (n = 256) | Delirium Group (n = 69) | p Value | |
|---|---|---|---|
| Age (years) | 53.20 ± 8.20 | 54.12 ± 7.65 | 0.404 |
| Sex (F/M) | 187 (73.05)/69 (26.95) | 48 (69.57)/21 (30.43) | 0.566 |
| Body mass index (kg/m2) | 22.47 ± 3.14 | 20.93 ± 3.43 | 0.001 * |
| Cause of LT | <0.0001 * | ||
| Alcoholic cirrhosis | 56 (21.88) | 35 (50.73) | |
| HBV and HCV | 168 (65.63) | 24 (34.78) | |
| NBNC LC | 10 (3.91) | 5 (7.25) | |
| Toxic hepatitis | 16 (6.25) | 3 (4.35) | |
| Primary biliary cirrhosis | 6 (2.34) | 2 (2.90) | |
| MELD score | 18.35 ± 11.50 | 28.32 ± 11.71 | <0.0001 * |
| Hypertension | 51 (19.92) | 12 (17.39) | 0.637 |
| Diabetes mellitus | 70 (27.34) | 14 (20.29) | 0.235 |
| Ischemic heart disease | 2 (0.78) | 3 (4.35) | 0.066 |
| Congestive heart failure | 1 (0.39) | 1 (1.45) | 0.380 |
| Cerebrovascular accidents | 0 (0.00) | 2 (2.90) | 0.045 * |
| Cardiac arrhythmia | 6 (2.34) | 3 (4.35) | 0.407 |
| With diuretics | 47 (18.36) | 24 (34.78) | 0.003 * |
| With insulin | 11 (4.30) | 8 (11.59) | 0.038 * |
| With psychiatric medication | 10 (3.91) | 10 (14.49) | 0.003 * |
| Sleep disorder | 22 (8.59) | 16 (23.19) | 0.001 * |
| Previous delirium | 8 (3.13) | 7 (10.14) | 0.022 * |
| Physical activity(self/assistance) | 219 (85.55)/37 (14.45) | 51 (73.91)/18 (26.09) | 0.022 * |
| Control Group (n = 256) | Delirium Group (n = 69) | p Value | |
|---|---|---|---|
| Hemoglobin (g/dL) | 10.98 ± 2.30 | 9.62 ± 1.95 | <0.0001 * |
| Platelet (×103/mL) | 68.50 (46.00, 101.25) | 52.00 (37.00, 79.00) | 0.017 * |
| Creatinine (mg/dL) | 0.79 (0.65, 0.99) | 1.14 (0.72, 1.92) | <0.0001 * |
| AST (unit/L) | 47.00 (34.00, 75.25) | 63.00 (40.00, 117.00) | 0.001 * |
| ALT (unit/L) | 31.00 (20.00, 49.00) | 34.00 (21.00, 52.00) | 0.446 |
| Protein (g/dL) | 6.04 ± 0.85 | 5.69 ± 0.96 | 0.003 * |
| Albumin (g/dL) | 3.16 ± 0.57 | 3.11 ± 0.57 | 0.527 |
| Bilirubin (mg/dL) | 2.40 (1.30, 12.62) | 16.60 (3.90, 29.00) | <0.0001 * |
| ≤3.5 mg/dL | 156 (60.94) | 15 (21.74) | <0.0001 * |
| >3.5 mg/dL | 100 (39.06) | 54 (78.26) | |
| PT (INR) | 1.48 (1.22, 2.12) | 1.98 (1.65, 2.80) | <0.0001 * |
| Use insulin during operation (unit) | 5.00 (0.00, 10.00) | 5.00 (0.00, 10.00) | 0.851 |
| Sodium (mEq/L) | 136.66 ± 5.32 | 134.58 ± 5.66 | 0.005 * |
| Potassium (mEq/L) | 3.97 ± 0.51 | 4.03 ± 0.74 | 0.537 |
| Control Group (n = 256) | Delirium Group (n = 69) | p Value | |
|---|---|---|---|
| Anesthetic duration (h) | 10.88 ± 2.30 | 10.65 ± 3.21 | 0.506 |
| Estimated blood loss (L) | 2.50 (1.50, 4.55) | 4.0 (2.50, 6.00) | <0.0001 * |
| Total fluid intake (L) | 7.04 (5.39, 9.60) | 9.22 (7.33, 12.55) | <0.0001 * |
| pRBC (unit) | 5.15 ± 5.43 | 9.30 ± 6.13 | <0.0001 * |
| Fresh frozen plasma (unit) | 5.08 ± 5.62 | 8.88 ± 6.02 | <0.0001 * |
| Cryoprecipitate (unit) | 0.00 (0.00, 0.00) | 0.00 (0.00, 0.00) | 0.525 |
| Platelet (unit) | 0.00 (0.00, 0.00) | 0.00 (0.00, 2.00) | 0.008 * |
| Control Group (n = 256) | Delirium Group (n = 69) | p Value | |
|---|---|---|---|
| Hemoglobin (g/dL) | 9.04 ± 1.48 | 9.08 ± 1.55 | 0.837 |
| Platelet (×103/mL) | 52.50 (39.00, 76.25) | 48.00 (36.00, 67.00) | 0.232 |
| PT (INR) | 1.75 (1.52, 1.98) | 1.78 (1.55, 2.04) | 0.293 |
| Bilirubin (mg/dL) | 4.10 (2.10, 7.03) | 6.40 (4.00, 10.50) | <0.0001 * |
| Protein (g/dL) | 5.29 ± 0.67 | 5.01 ± 0.69 | 0.002 * |
| Albumin (g/dL) | 3.66 ± 0.47 | 3.51 ± 0.52 | 0.019 * |
| Creatinine (mg/dL) | 1.05 ± 0.49 | 1.30 ± 0.54 | <0.0001 * |
| Sodium (mEq/L) | 139.54 ± 3.72 | 138.68 ± 3.85 | 0.093 |
| Potassium (mEq/L) | 4.00 ± 0.40 | 4.07 ± 0.45 | 0.206 |
| Stay in intensive care unit (days) | 7.00 (5.00, 11.00) | 12.00 (7.00, 18.00) | <0.0001 * |
| Infection | 11 (4.30) | 7 (10.14) | 0.074 |
| Time from surgery to discharge (days) | 27.00 (22.00, 38.00) | 40.00 (28.00, 54.00) | <0.0001 * |
| Predictors | OR | 95% CI | p Value * | OR | 95% CI | p Value † | ||
|---|---|---|---|---|---|---|---|---|
| Lower | Upper | Lower | Upper | |||||
| Bilirubin (3.5<) | 5.616 | 3.007 | 10.489 | <0.0001 * | 2.864 | 1.381 | 5.941 | 0.005 † |
| Age | 1.015 | 0.981 | 1.050 | 0.403 | ||||
| Sex | 0.843 | 0.471 | 1.510 | 0.567 | ||||
| Body mass index | 0.847 | 0.770 | 0.932 | 0.001 * | 0.853 | 0.770 | 0.944 | 0.005 † |
| Alcoholic liver disease | 3.676 | 2.106 | 6.419 | <0.0001 * | 1.630 | 0.850 | 3.127 | 0.141 |
| with Diuretics | 2.372 | 1.318 | 4.269 | 0.004 * | 2.181 | 1.105 | 4.303 | 0.025 † |
| with Insulin | 2.921 | 1.126 | 7.575 | 0.028 * | ||||
| Psychiatric medication | 4.169 | 1.659 | 10.477 | 0.002 * | 2.813 | 0.942 | 8.400 | 0.064 |
| Previous delirium | 2.089 | 1.101 | 3.963 | 0.024 * | ||||
| Hb before surgery | 0.736 | 0.639 | 0.849 | <0.0001 * | ||||
| Albumin before surgery | 0.859 | 0.538 | 1.373 | 0.526 | ||||
| Na before surgery | 0.932 | 0.887 | 0.979 | 0.005 * | ||||
| Cr before surgery | 1.903 | 1.427 | 2.538 | 0.0001 * | 1.504 | 1.097 | 2.063 | 0.011 † |
| Anesthetic duration | 0.963 | 0.863 | 1.076 | 0.505 | ||||
| Intraoperative EBL (L) | 1.165 | 1.050 | 1.292 | 0.004 * | ||||
| Total_fluid (L) | 1.089 | 1.033 | 1.148 | 0.002 * | ||||
| pRBC (pint) | 1.123 | 1.071 | 1.177 | <0.0001 * | 1.043 | 0.985 | 1.104 | 0.146 |
| Hb after surgery | 1.019 | 0.853 | 1.217 | 0.836 | ||||
| Albumin after surgery | 0.523 | 0.303 | 0.905 | 0.021 * | ||||
| Na after surgery | 0.941 | 0.876 | 1.010 | 0.094 | ||||
| K after surgery | 1.512 | 0.796 | 2.873 | 0.207 | ||||
| Infection | 2.515 | 0.936 | 6.752 | 0.067 | ||||
| Odds Ratio | 95% Confidence Interval | p Value | |||
|---|---|---|---|---|---|
| Lower | Upper | ||||
| Univariate | Bilirubin (3.5<) | 5.616 | 3.007 | 10.489 | <0.0001 * |
| Multivariable analysis | |||||
| Model 1 | Bilirubin (3.5<) | 2.864 | 1.381 | 5.941 | 0.005 † |
| Model 2 | Bilirubin (3.5<) | 2.794 | 1.340 | 5.828 | 0.006 † |
| Model 3 | Bilirubin (3.5<) | 3.266 | 1.617 | 6.597 | 0.001 † |
| Model 4 | Bilirubin (3.5<) | 3.195 | 1.574 | 6.484 | 0.001 † |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Park, K.H.; Son, H.J.; Choi, Y.J.; Park, G.H.; Lee, Y.S.; Park, J.Y.; Ri, H.-S.; Shim, J.R. Liver Transplant Patients with High Preoperative Serum Bilirubin Levels Are at Increased Risk of Postoperative Delirium: A Retrospective Study. J. Clin. Med. 2020, 9, 1591. https://doi.org/10.3390/jcm9051591
Park KH, Son HJ, Choi YJ, Park GH, Lee YS, Park JY, Ri H-S, Shim JR. Liver Transplant Patients with High Preoperative Serum Bilirubin Levels Are at Increased Risk of Postoperative Delirium: A Retrospective Study. Journal of Clinical Medicine. 2020; 9(5):1591. https://doi.org/10.3390/jcm9051591
Chicago/Turabian StylePark, Kyu Hee, Hyo Jung Son, Yoon Ji Choi, Gene Hyun Park, Yoon Sook Lee, Ju Yeon Park, Hyun-Su Ri, and Jae Ryong Shim. 2020. "Liver Transplant Patients with High Preoperative Serum Bilirubin Levels Are at Increased Risk of Postoperative Delirium: A Retrospective Study" Journal of Clinical Medicine 9, no. 5: 1591. https://doi.org/10.3390/jcm9051591