Nebulized Heparin in Burn Patients with Inhalation Trauma—Safety and Feasibility


 ,
,
Abstract
:1. Introduction
2. Materials and Methods
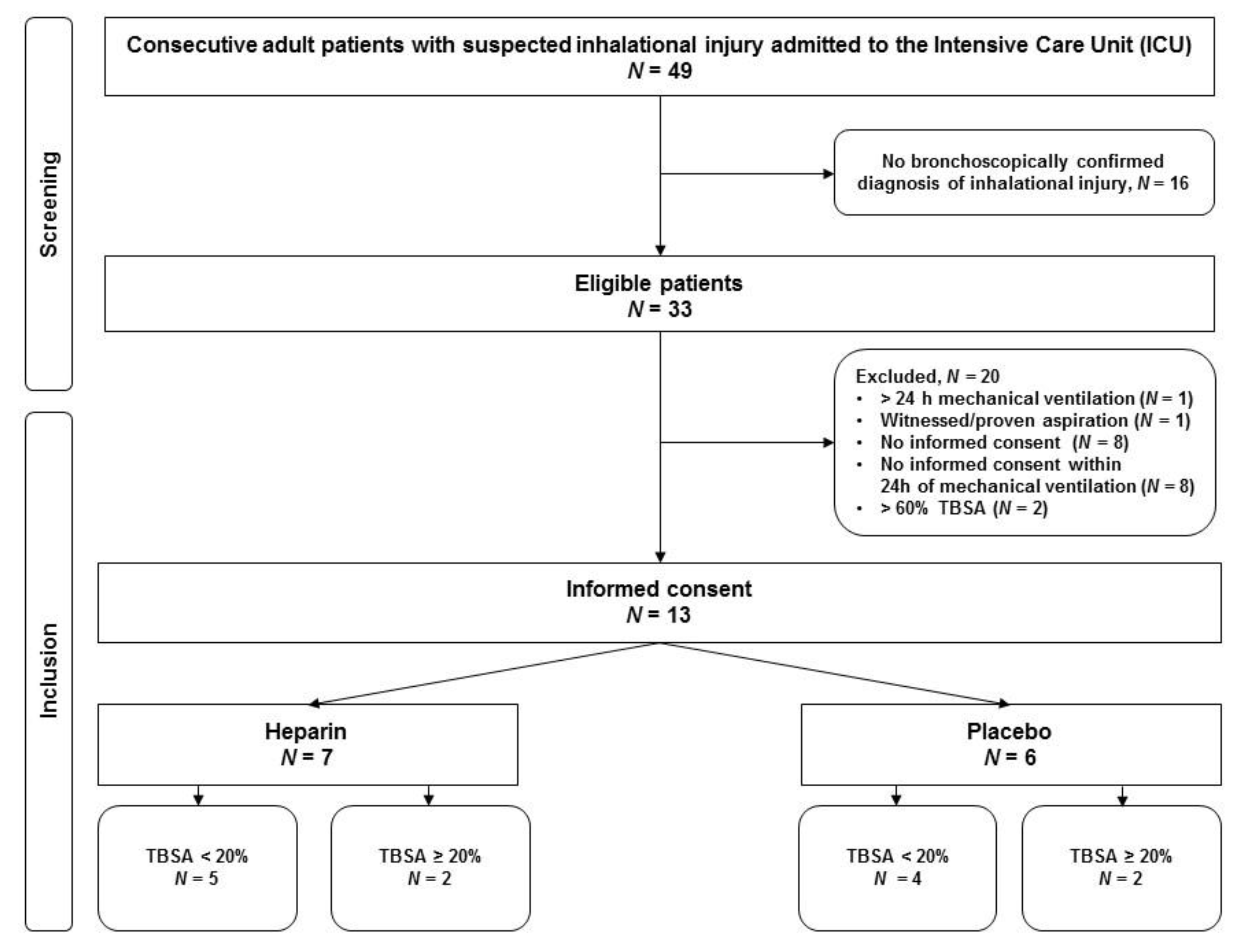
2.1. Patients
2.2. Study Medication and Procedures
2.3. Outcomes
2.4. Data Collection
2.5. Sample Size Calculation
2.6. Statistical Analysis
3. Results
3.1. Safety
3.2. Study-Related Serious Adverse Events
3.3. Other Serious Adverse Events Not Related to the Study
3.4. Feasibility
4. Discussion
5. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- Hollingsed, T.C.; Saffle, J.; Barton, R.G.; Craft, W.B.; Morris, S.E. Etiology and consequences of respiratory failure in thermally injured patients. Am. J. Surg. 1993, 166, 592–596. [Google Scholar] [CrossRef]
- Latenser, B.A.; Miller, S.F.; Bessey, P.Q.; Browning, S.M.; Caruso, D.M.; Gomez, M.; Jeng, J.C.; Krichbaum, J.A.; Lentz, C.W.; Saffle, J.R.; et al. National Burn Repository 2006: A ten-year review. J. Burn. Care Res. 2007, 28, 635–658. [Google Scholar] [CrossRef] [PubMed]
- Rehberg, S.; Maybauer, M.O.; Enkhbaatar, P.; Maybauer, D.M.; Yamamoto, Y.; Traber, D.L. Pathophysiology, management and treatment of smoke inhalation injury. Expert Rev. Respir. Med. 2009, 3, 283–297. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Holt, J.; Saffle, J.R.; Morris, S.E.; Cochran, A. Use of Inhaled Heparin/N-acetylcystine in Inhalation Injury: Does it help? J. Burn. Care Res. 2008, 29, 192–195. [Google Scholar] [CrossRef] [PubMed]
- Miller, A.C.; Elamin, E.M.; Suffredini, A.F. Inhaled anticoagulation regimens for the treatment of smoke inhalation-associated acute lung injury: A systematic review. Crit. Care Med. 2014, 42, 413–419. [Google Scholar] [CrossRef] [Green Version]
- Murakami, K.; Traber, D.L. Pathophysiological basis of smoke inhalation injury. News Physiol. Sci. Int. J. Physiol. Prod. Jt. Int. Union Physiol. Sci. Am. Physiol. Soc. 2003, 18, 125–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Glas, G.J.; Neto, A.S.; Horn, J.; Cochran, A.; Dixon, B.; Elamin, E.M.; Faraklas, I.; Dissanaike, S.; Miller, A.C.; Schultz, M.J. Nebulized heparin for patients under mechanical ventilation: An individual patient data meta-analysis. Ann. Intensiv. Care 2016, 6, 33. [Google Scholar] [CrossRef] [Green Version]
- Glas, G.J.; Müller, J.; Binnekade, J.M.; Cleffken, B.I.; Colpaert, K.; Dixon, B.; Juffermans, N.P.; Knape, P.; Levi, M.; Loef, B.G.; et al. HEPBURN-investigating the efficacy and safety of nebulized heparin versus placebo in burn patients with inhalation trauma: Study protocol for a multi-center randomized controlled trial. Trials 2014, 15, 91. [Google Scholar] [CrossRef] [Green Version]
- Albright, J.M.; Davis, C.S.; Bird, M.D.; Ramirez, L.; Kim, H.; Burnham, E.L.; Gamelli, R.L.; Kovacs, E.J. The acute pulmonary inflammatory response to the graded severity of smoke inhalation injury*. Crit. Care Med. 2012, 40, 1113–1121. [Google Scholar] [CrossRef] [Green Version]
- Dixon, B.; Schultz, M.J.; Smith, R.; Roberts, K.M.; Santamaria, J.D.; Campbell, D.J. Nebulized heparin is associated with fewer days of mechanical ventilation in critically ill patients: A randomized controlled trial. Crit. Care 2010, 14, R180. [Google Scholar] [CrossRef] [Green Version]
- Lu, Q.; Yang, J.; Liu, Z.; Gutiérrez, C.; Aymard, G.; Rouby, J.J. Nebulized Ceftazidime and Amikacin in Ventilator-associated Pneumonia Caused by Pseudomonas aeruginosa. Am. J. Respir. Crit. Care Med. 2011, 184, 106–115. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tonnelier, A.; Lellouche, F.; Bouchard, P.A.; L’Her, E.; Hodgson, C.L.; Fan, E. Impact of Humidification and Nebulization During Expiratory Limb Protection: An Experimental Bench Study. Respir. Care 2012, 58, 1315–1322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ari, A. Aerosol Therapy in Pulmonary Critical Care. Respir. Care 2015, 60, 858–879. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kallet, R.H. Adjunct therapies during mechanical ventilation: Airway clearance techniques, therapeutic aerosols, and gases. Respir. Care 2013, 58, 1053–1073. [Google Scholar] [CrossRef] [Green Version]
- Quon, B.S.; Goss, C.H.; Ramsey, B.W. Inhaled antibiotics for lower airway infections. Ann. Am. Thorac. Soc. 2014, 11, 425–434. [Google Scholar] [CrossRef]
- Elsharnouby, N.M.; Eid, H.; Elezz, N.F.A.; Aboelatta, Y.A. Heparin/N-acetylcysteine: An adjuvant in the management of burn inhalation injury. J. Crit. Care 2014, 29, 182.e1–182.e4. [Google Scholar] [CrossRef]
- Miller, A.C.; Rivero, A.; Ziad, S.; Smith, D.J.; Elamin, E.M. Influence of Nebulized Unfractionated Heparin and N-Acetylcysteine in Acute Lung Injury After Smoke Inhalation Injury. J. Burn. Care Res. 2009, 30, 249–256. [Google Scholar] [CrossRef]
- Yip, L.Y.; Lim, Y.F.; Chan, H.N. Safety and potential anticoagulant effects of nebulised heparin in burns patients with inhalational injury at Singapore General Hospital Burns Centre. Burn. J. Int. Soc. Burn. Inj. 2011, 37, 1154–1160. [Google Scholar] [CrossRef]
- Kashefi, N.; Dissanaike, S. Does a nebulized heparin/N-acetylcysteine protocol improve clinical outcomes in adult patients with inhalation injury? J. Burn. Care Res. 2013, 1, S82. [Google Scholar]
- McIntire, A.M.; Harris, S.A.; Whitten, J.A.; Fritschle-Hilliard, A.C.; Foster, D.R.; Sood, R.; Walroth, T.A. Outcomes Following the Use of Nebulized Heparin for Inhalation Injury (HIHI Study). J. Burn. Care Res. 2017, 38, 45–52. [Google Scholar] [CrossRef]
- McGinn, K.A.; Weigartz, K.; Lintner, A.; Scalese, M.J.; Kahn, S.A. Nebulized Heparin with N-Acetylcysteine and Albuterol Reduces Duration of Mechanical Ventilation in Patients with Inhalation Injury. J. Pharm. Pract. 2017, 32, 163–166. [Google Scholar] [CrossRef] [PubMed]
- Lundy, J.; Chung, K.K.; Pamplin, J.C.; Ainsworth, C.R.; Jeng, J.C.; Friedman, B.C. Update on Severe Burn Management for the Intensivist. J. Intensiv. Care Med. 2016, 31, 499–510. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Heparin N = 7 | Placebo N = 6 | p | |
|---|---|---|---|
| Age | 67 (59–81) | 51 (40–61) | 0.08 |
| Gender, male | 4 | 4 | 0.73 |
| TBSA % | 12 (1–23) | 3 (1–44) | 0.88 |
| ABSI | 7 (6–9) | 6 (5–10) | 1.0 |
| Inhalation injury score | 0.62 | ||
| Clinical a | 4 (2–4) | 3 (3–5) | |
| Bronchoscopic b | 1 (1–2) | 1 (1–3) | 0.83 |
| SAPS II | 51 (37–65) | 56 (42–72) | 0.83 |
| LIS c on ICU admission day | 1.5 (1–2.3) | 1.5 (1–1.8) | 0.84 |
| APTT on ICU admission day | 34 (27–43) | 31 (27–38) | 0.51 |
| Ventilator-free days and alive at day 28 | 16 (4–24) | 20 (7–24) | 0.62 |
| ICU-free days and alive at day 90 | 71 (0–75) | 49 (3–82) | 0.73 |
| ARDS, N | - | 1 | - |
| Pneumonia, N | 2 | 1 | - |
| Burn wound infection, N | - | 1 | - |
| Heparin N = 7 | Placebo N = 6 | |
|---|---|---|
| Patients with withheld dosages, N | 3 | 2 |
| Number of scheduled/withhold dosages (% withheld) | 427/129 (30) | 299/45 (15) |
| Reasons for temporary withholding of scheduled dosages, number of dosages (% of scheduled dosages) | ||
| prolonged APTT (> 150 s) | 10 (2) | 0 |
| physicians request: | ||
| blood stained sputum or BAL | 36 (8) | 29 (10) |
| increased bleeding risk 1 | 72 (17) | 0 |
| logistical reasons | 4 (1) | 0 |
| surgical procedure | 3 (1) | 10 (3) |
| reason not specified (protocol violation) | 4 (1) | 6 (2) |
| Number of stopped nebulizations 2 | 70 | 0 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Glas, G.J.; Horn, J.; Binnekade, J.M.; Hollmann, M.W.; Muller, J.; Cleffken, B.; Colpaert, K.; Dixon, B.; Juffermans, N.P.; Knape, P.; et al. Nebulized Heparin in Burn Patients with Inhalation Trauma—Safety and Feasibility. J. Clin. Med. 2020, 9, 894. https://doi.org/10.3390/jcm9040894
Glas GJ, Horn J, Binnekade JM, Hollmann MW, Muller J, Cleffken B, Colpaert K, Dixon B, Juffermans NP, Knape P, et al. Nebulized Heparin in Burn Patients with Inhalation Trauma—Safety and Feasibility. Journal of Clinical Medicine. 2020; 9(4):894. https://doi.org/10.3390/jcm9040894
Chicago/Turabian StyleGlas, Gerie J., Janneke Horn, Jan M. Binnekade, Markus W. Hollmann, Jan Muller, Berry Cleffken, Kirsten Colpaert, Barry Dixon, Nicole P. Juffermans, Paul Knape, and et al. 2020. "Nebulized Heparin in Burn Patients with Inhalation Trauma—Safety and Feasibility" Journal of Clinical Medicine 9, no. 4: 894. https://doi.org/10.3390/jcm9040894