Clinical Characteristics and Outcome of Patients with Infective Endocarditis Diagnosed in a Department of Internal Medicine

 , ,
, ,
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Site
2.2. Inclusion and Exclusion Criteria
2.3. Data Collection and Definitions
2.4. Data Analysis
2.5. Ethics
3. Results
3.1. Study Population
3.2. Clinical, Biological and Imaging Characteristics at IE Diagnosis
3.3. Microbiology
3.4. Echocardiography
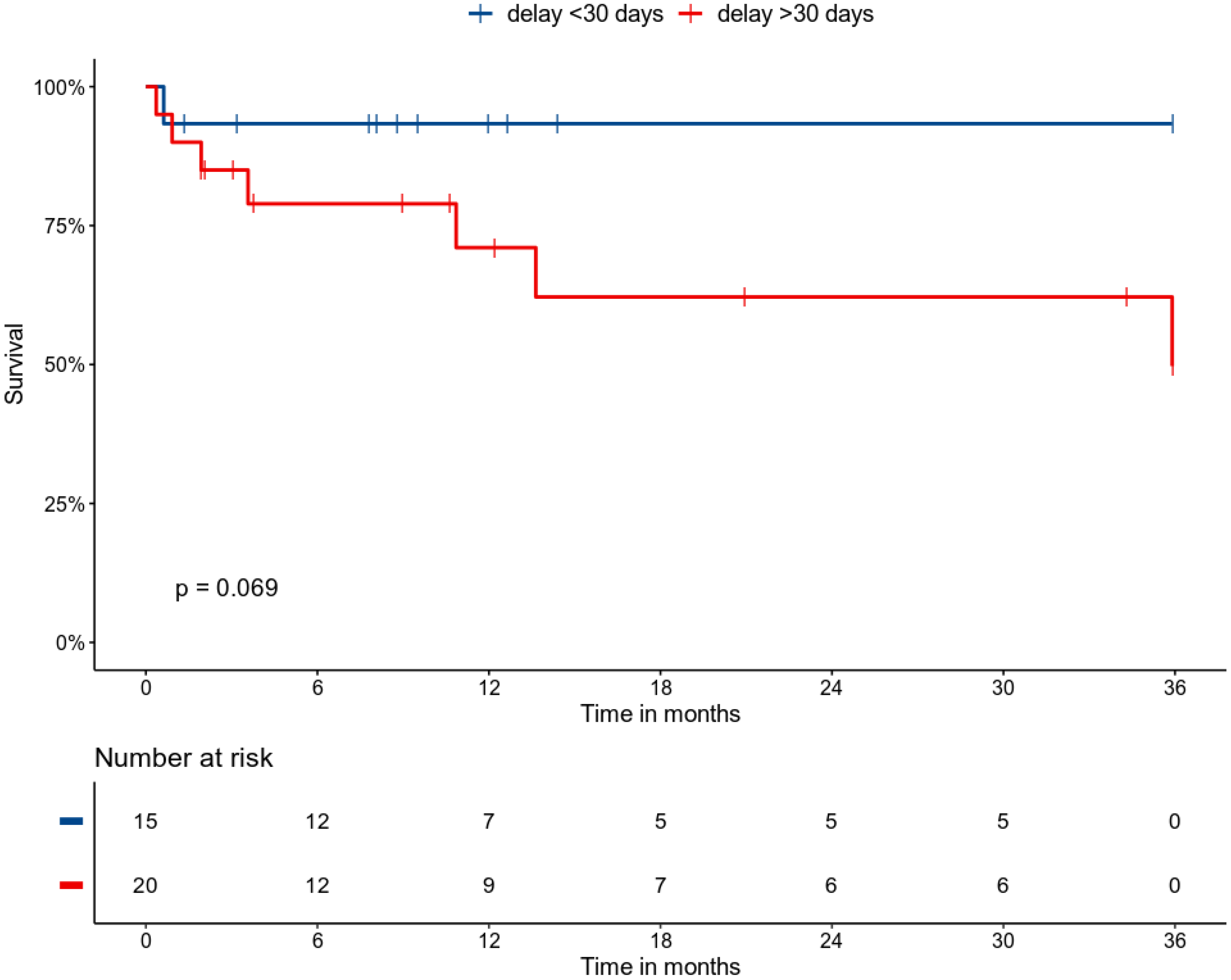
3.5. Treatment, Follow-Up, and Survival
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Cahill, T.J.; Prendergast, B.D. Infective endocarditis. Lancet 2016, 387, 882–893. [Google Scholar] [CrossRef] [Green Version]
- Hoen, B.; Duval, X. Clinical practice. Infective endocarditis. N. Engl. J. Med. 2013, 368, 1425–1433. [Google Scholar] [CrossRef] [PubMed]
- Pant, S.; Patel, N.J.; Deshmukh, A.; Golwala, H.; Patel, N.; Badheka, A.; Hirsch, G.A.; Mehta, J.L. Trends in infective endocarditis incidence, microbiology, and valve replacement in the United States from 2000 to 2011. J. Am. Coll. Cardiol. 2015, 65, 2070–2076. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ambrosioni, J.; Hernandez-Meneses, M.; Téllez, A.; Pericàs, J.; Falces, C.; Tolosana, J.M.; Vidal, B.; Almela, M.; Quintana, E.; Llopis, J.; et al. The changing epidemiology of infective endocarditis in the twenty-first century. Curr. Infect. Dis. Rep. 2017, 19, 21. [Google Scholar] [CrossRef] [PubMed]
- Hoen, B.; Alla, F.; Selton-Suty, C.; Béguinot, I.; Bouvet, A.; Briançon, S.; Casalta, J.-P.; Danchin, N.; Delahaye, F.; Etienne, J.; et al. Changing profile of infective endocarditis: Results of a 1-year survey in France. JAMA 2002, 288, 75–81. [Google Scholar] [CrossRef]
- Cabell, C.H.; Jollis, J.G.; Peterson, G.E.; Corey, G.R.; Anderson, D.J.; Sexton, D.J.; Woods, C.W.; Reller, L.B.; Ryan, T.; Fowler, V.G. Changing patient characteristics and the effect on mortality in endocarditis. Arch. Intern. Med. 2002, 162, 90–94. [Google Scholar] [CrossRef] [Green Version]
- Murdoch, D.R.; Corey, G.R.; Hoen, B.; Miró, J.M.; Fowler, V.G.; Bayer, A.S.; Karchmer, A.W.; Olaison, L.; Pappas, P.A.; Moreillon, P.; et al. Clinical presentation, etiology, and outcome of infective endocarditis in the 21st century: The International Collaboration on Endocarditis-Prospective Cohort Study. Arch. Intern. Med. 2009, 169, 463–473. [Google Scholar] [CrossRef] [Green Version]
- Silverman, M.E.; Upshaw, C.B. Extracardiac manifestations of infective endocarditis and their historical descriptions. Am. J. Cardiol. 2007, 100, 1802–1807. [Google Scholar] [CrossRef]
- Osler, W. The Gulstonian lectures, on malignant endocarditis. Br. Med. J. 1885, 1, 467–470. [Google Scholar] [CrossRef] [Green Version]
- Cantier, M.; Mazighi, M.; Klein, I.; Desilles, J.P.; Wolff, M.; Timsit, J.F.; Sonneville, R. Neurologic complications of infective endocarditis: Recent findings. Curr. Infect. Dis. Rep. 2017, 19, 41. [Google Scholar] [CrossRef]
- Heiro, M.; Nikoskelainen, J.; Engblom, E.; Kotilainen, E.; Marttila, R.; Kotilainen, P. Neurologic manifestations of infective endocarditis: A 17-year experience in a teaching hospital in Finland. Arch. Intern. Med. 2000, 160, 2781–2787. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Servy, A.; Valeyrie-Allanore, L.; Alla, F.; Lechiche, C.; Nazeyrollas, P.; Chidiac, C.; Hoen, B.; Chosidow, O.; Duval, X.; Association Pour l’Etude et la Prévention de l’Endocardite Infectieuse Study Group. Prognostic value of skin manifestations of infective endocarditis. JAMA Dermatol. 2014, 150, 494–500. [Google Scholar] [CrossRef] [PubMed]
- Alpert, J.S. Osler’s nodes and Janeway lesions are not the result of small-vessel vasculitis. Am. J. Med. 2013, 126, 843–844. [Google Scholar] [CrossRef] [PubMed]
- Loricera, J.; Blanco, R.; Hernández, J.L.; Calvo-Río, V.; Ortiz-Sanjuán, F.; Mata, C.; Rueda-Gotor, J.; Álvarez, L.; González-Vela, M.C.; González-López, M.A.; et al. Cutaneous vasculitis associated with severe bacterial infections. A study of 27 patients from a series of 766 cutaneous vasculitis. Clin. Exp. Rheumatol. 2015, 33, 36–43. [Google Scholar]
- González-Juanatey, C.; González-Gay, M.A.; Llorca, J.; Crespo, F.; García-Porrúa, C.; Corredoira, J.; Vidán, J.; González-Juanatey, J.R. Rheumatic manifestations of infective endocarditis in non-addicts. A 12-year study. Medicine 2001, 80, 9–19. [Google Scholar]
- Casey, J.D.; Vaidya, A.; Solomon, D.H.; Gaziano, T.A. Interactive medical case: A patient with migrating polyarthralgias. N. Engl. J. Med. 2013, 368, e33. [Google Scholar] [CrossRef]
- Boils, C.L.; Nasr, S.H.; Walker, P.D.; Couser, W.G.; Larsen, C.P. Update on endocarditis-associated glomerulonephritis. Kidney Int. 2015, 87, 1241–1249. [Google Scholar] [CrossRef] [Green Version]
- Subra, J.F.; Michelet, C.; Laporte, J.; Carrere, F.; Reboul, P.; Cartier, F.; Saint-André, J.P.; Chevailler, A. The presence of cytoplasmic antineutrophil cytoplasmic antibodies (C-ANCA) in the course of subacute bacterial endocarditis with glomerular involvement, coincidence or association? Clin. Nephrol. 1998, 49, 15–18. [Google Scholar]
- Kang, D.-H.; Kim, Y.-J.; Kim, S.-H.; Sun, B.J.; Kim, D.-H.; Yun, S.-C.; Song, J.-M.; Choo, S.J.; Chung, C.-H.; Song, J.-K.; et al. Early surgery versus conventional treatment for infective endocarditis. N. Engl. J. Med. 2012, 366, 2466–2473. [Google Scholar] [CrossRef] [Green Version]
- Holland, T.L.; Baddour, L.M.; Bayer, A.S.; Hoen, B.; Miro, J.M.; Fowler, V.G. Infective endocarditis. Nat. Rev. Dis. Primers 2016, 2, 16059. [Google Scholar] [CrossRef]
- Habib, G.; Lancellotti, P.; Antunes, M.J.; Bongiorni, M.G.; Casalta, J.-P.; Del Zotti, F.; Dulgheru, R.; El Khoury, G.; Erba, P.A.; Iung, B.; et al. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur. Heart J. 2015, 36, 3075–3128. [Google Scholar] [PubMed]
- Osler, W. Chronic infectious endocarditis. QJM 1909, os2, 219–230. [Google Scholar]
- Habib, G.; Badano, L.; Tribouilloy, C.; Vilacosta, I.; Zamorano, J.L.; Galderisi, M.; Voigt, J.-U.; Sicari, R.; Cosyns, B.; Fox, K.; et al. Recommendations for the practice of echocardiography in infective endocarditis. Eur. J. Echocardiogr. 2010, 11, 202–219. [Google Scholar] [CrossRef] [PubMed] [Green Version]


{kind=link}
| Characteristics | Number of Patients (%) |
|---|---|
| Gender (male), n (%) | 23 (65.7%) |
| Age at diagnosis, median (IQR) | 59 (51–71) |
| Diagnostic delay *, median (IQR) | 41 (19–153) |
| Predisposing cardiac condition, n (%) | 16 (45.7%) |
| Aortic valve disorder, n (%) | 9 (25.7%) |
| Bicuspid aortic valve, n (%) | 4 (11.4%) |
| Degenerative aortic stenosis, n (%) | 3 (8.6%) |
| Aortic biologic prothesis, n (%) | 1 (2.9%) |
| Mitral valve disorder, n (%) | 5 (14.3%) |
| Acute rheumatic fever, n (%) | 2 (5.7%) |
| Cardiac pace-maker, n (%) | 1 (2.9%) |
| Comorbid conditions | |
| Cancer or hematological malignancy, n (%) | 6 (17.1%) |
| Atrial fibrillation, n (%) | 6 (17.1%) |
| Hypertension, n (%) | 5 (14.3%) |
| Diabetes mellitus, n (%) | 5 (14.3%) |
| Dyslipidemia, n (%) | 7 (20.0%) |
| Current tobacco smoking, n (%) | 9 (25.7%) |
| Current alcohol drinking, n (%) | 8 (22.9%) |
| Intravenous drug user, n (%) | 0 (0%) |
| Drug-induced immunosuppression, n (%) | 5 (14.3%) |
| Recent dental care, n (%) | 4 (11.4%) |
| Recent antibiotic use, n (%) | 19 (54.3%) |
| Characteristics | Number of Patients (%) ¤ |
|---|---|
| General manifestations | |
| Fever >38 °C, n (%) | 20 (57.1%) |
| Constitutional symptoms, n (%) | 19 (54.3%) |
| Neurological and ophthalmic manifestations | |
| Clinical manifestations, n (%) | 11 (31.4%) |
| Imaging abnormalities, n (%) # | 8 (26.7%) |
| Focal ischemic lesions, n (%) | 4 (13.3%) |
| Multiple ischemic lesions, n (%) | 2 (6.7%) |
| Subarachnoid hemorrhage, n (%) | 2 (6.7%) |
| Intraparenchymal hemorrhage, n (%) | 2 (6.7%) |
| Cerebral vasculitis, n (%) | 1 (3.3%) |
| Optic fundus abnormalities, n (%) $ | 2 (16.6%) |
| Cardiac manifestations | |
| Heart failure, n (%) | 7 (20.0%) |
| Murmur, n (%) | 22 (62.9%) |
| New-onset murmur, n (%) | 4 (11.4%) |
| New-onset EKG abnormalities, n (%) | 8 (22.9%) |
| Embolic manifestations | |
| Any embolic manifestation, n (%) | 19 (54.3%) |
| Digital emboli, n (%) | 7 (20.0%) |
| Lower limb emboli, n (%) | 4 (11.4%) |
| Cerebral emboli, n (%) | 5 (14.3%) |
| Renal emboli, n (%) | 3 (8.6%) |
| Splenic emboli, n (%) | 2 (5.7%) |
| Bone emboli, n (%) | 2 (5.7%) |
| Rheumatic manifestations | |
| Myalgia, n (%) | 7 (20.0%) |
| Arthralgia, n (%) | 10 (28.6%) |
| Rachialgia, n (%) | 12 (34.3%) |
| Peripheral arthritis, n (%) | 5 (14.3%) |
| Skin manifestations | |
| All manifestations, n (%) | 19 (54.3%) |
| Purpura, n (%) | 8 (22.9%) |
| Janeway palmo-plantar lesions, n (%) | 3 (8.6%) |
| Skin biopsy showing vasculitis, n (%) * | 7 (87.5%) |
| Hematological abnormalities | |
| Polyadenopathy, n (%) | 5 (14.3%) |
| Splenomegaly, n (%) | 1 (2.9%) |
| Anemia, n (%) | 27 (77.1%) |
| Leukocytosis, n (%) | 11 (31.4%) |
| Thrombopenia, n (%) | 4 (11.4%) |
| Renal manifestations | |
| Acute kidney injury, n (%) | 7 (20.0%) |
| Proteinuria, n (%) | 7 (20.0%) |
| Leukocyturia/hematuria, n (%) | 5 (14.3%) |
| Characteristics | Number of Patients (%) |
|---|---|
| IE with positive blood cultures, n (%) | 23 (65.7%) |
| IE with negative blood cultures, n (%) | 12 (34.3%) |
| IE with negative microbiology, n (%) | 8 (22.9%) |
| Identified bacteria | |
| Streptococcus sp., n (%) | 12 (34.3%) |
| Streptococcus pyogenes, n (%) | 1 (2.9%) |
| Streptococcus agalactiae, n (%) | 1 (2.9%) |
| Non-haemolytic streptococci, n (%) | 10 (28.6%) |
| Staphylococcus sp., n (%) | 9 (25.7%) |
| Staphylococcus aureus, n (%) | 2 (5.9%) |
| Negative coagulase staphylococci, n (%) | 7 (20.0%) |
| Enterococcus sp., n (%) | 5 (14.3%) |
| Enterococcus faecalis, n (%) | 3 (8.6%) |
| Enterococcus faecium, n (%) | 1 (2.9%) |
| Characteristics | Number of Patients (%) |
|---|---|
| Valves involved | |
| Aortic valve, n (%) | 19 (57.6%) |
| Mitral valve, n (%) | 14 (42.4%) |
| Tricuspid valve, n (%) | 2 (6.1%) |
| Mono-valvular involvement, n (%) | 28 (84.8%) |
| Bi-valvular involvement, n (%) | 4 (12.1%) |
| Pacemaker, n (%) | 1 (3.0%) |
| Nature of lesions | |
| 1 vegetation, n (%) | 18 (54.5%) |
| ≥2 vegetations, n (%) | 14 (42.4%) |
| Valvular destruction, n (%) | 7 (21.2%) |
| Abscess, n (%) | 2 (6.1%) |
| Number of TTE examination before definite diagnosis | |
| 1 TTE, n (%) | 19 (57.6%) |
| 2 TTE, n (%) | 8 (24.2%) |
| 3 TTE, n (%) | 6 (18.2%) |
| Number of TOE examination before definite diagnosis | |
| 1 TOE, n (%) | 25 (75.8%) |
| 2 TOE, n (%) | 6 (18.2%) |
| 3 TOE, n (%) | 2 (6.1%) |
| Variables | HR | CI95% | p-Value |
|---|---|---|---|
| Gender (male) | 0.53 | 0.13–2.18 | 0.38 |
| Age (per year) | 1.07 | 1.01–1.14 | 0.03 |
| Current smoking | 1.34 | 0.33–5.44 | 0.69 |
| Current alcohol drinking | 0.55 | 0.11–2.61 | 0.46 |
| Immunosuppression | 4.1 | 1.32–12.72 | 0.02 |
| Duration of symptoms > 30 days | 5.6 | 0.66–47.11 | 0.11 |
| Predisposing condition | 1.87 | 0.47–7.46 | 0.37 |
| Fever | 0.71 | 0.18–2.73 | 0.61 |
| Constitutional symptoms | 1.59 | 0.42–6.02 | 0.5 |
| Neurological symptoms | 3.49 | 0.79–15.48 | 0.1 |
| Acute kidney injury | 4.5 | 1.13–17.88 | 0.03 |
| Embolic manifestations | 1.11 | 0.24–3.34 | 0.88 |
| Heart failure | 2.67 | 0.68–10.54 | 0.16 |
| Skin manifestations | 0.8 | 0.22–2.92 | 0.73 |
| C-reactive protein (mg/L) | 1 | 0.995–1.005 | 0.87 |
| Immunological manifestations | 1.5 | 0.39–5.86 | 0.56 |
| Transfer to ICU | 3.38 | 0.85–13.55 | 0.09 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kreitmann, L.; Montaigne, D.; Launay, D.; Morell-Dubois, S.; Maillard, H.; Lambert, M.; Hachulla, E.; Sobanski, V. Clinical Characteristics and Outcome of Patients with Infective Endocarditis Diagnosed in a Department of Internal Medicine. J. Clin. Med. 2020, 9, 864. https://doi.org/10.3390/jcm9030864
Kreitmann L, Montaigne D, Launay D, Morell-Dubois S, Maillard H, Lambert M, Hachulla E, Sobanski V. Clinical Characteristics and Outcome of Patients with Infective Endocarditis Diagnosed in a Department of Internal Medicine. Journal of Clinical Medicine. 2020; 9(3):864. https://doi.org/10.3390/jcm9030864
Chicago/Turabian StyleKreitmann, Louis, David Montaigne, David Launay, Sandrine Morell-Dubois, Hélène Maillard, Marc Lambert, Eric Hachulla, and Vincent Sobanski. 2020. "Clinical Characteristics and Outcome of Patients with Infective Endocarditis Diagnosed in a Department of Internal Medicine" Journal of Clinical Medicine 9, no. 3: 864. https://doi.org/10.3390/jcm9030864