Sarcoscore: A Novel Approach for Assessing Sarcopenia and Functional Disability in Older Adults

 , ,
, ,
Abstract
:1. Introduction
2. Methods
2.1. Study Design
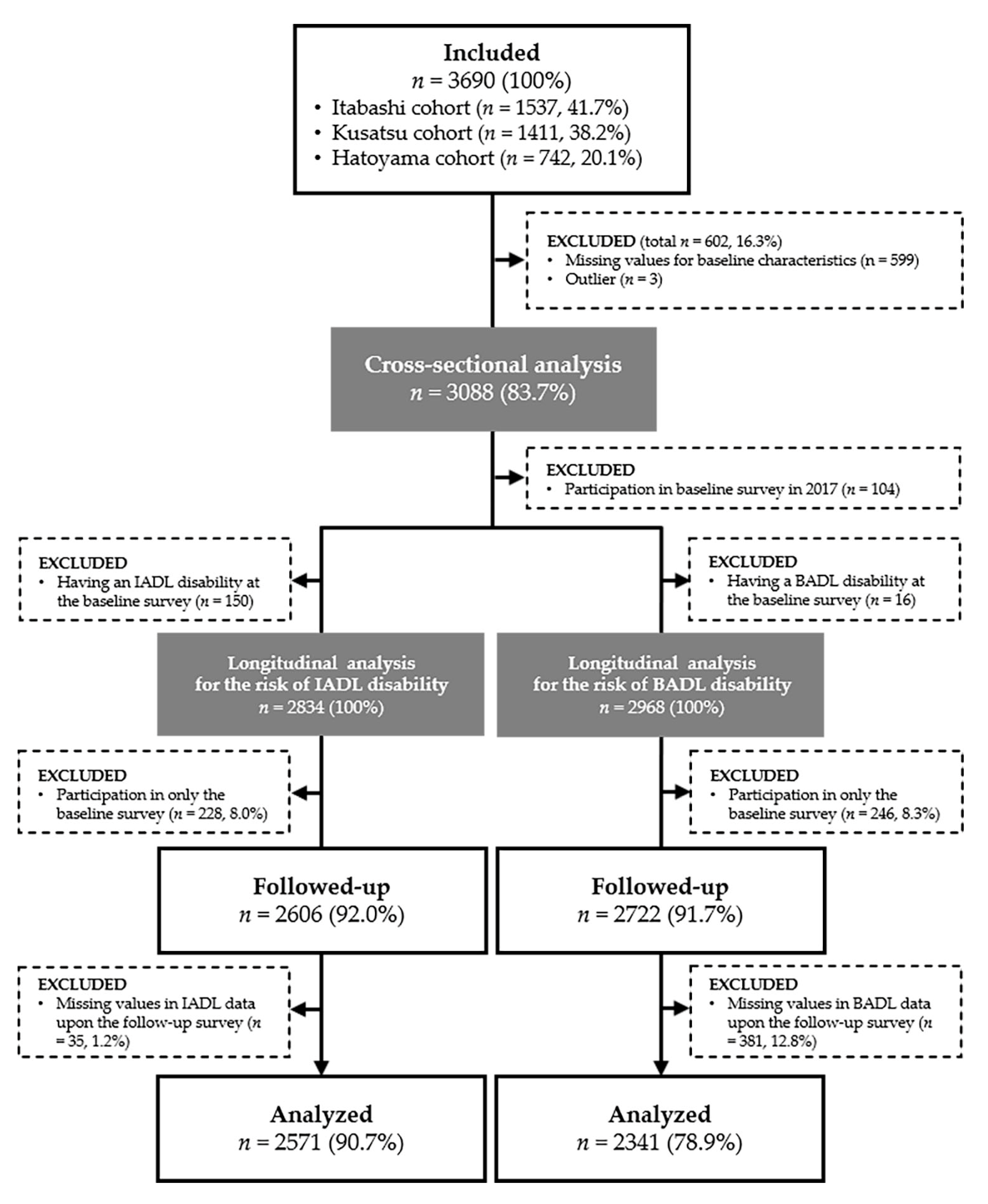
2.2. Setting and Participants
2.2.1. Itabashi Cohort Study
2.2.2. Kusatsu Longitudinal Study
2.2.3. Hatoyama Cohort Study
2.3. Measurements
2.3.1. Sarcoscore
2.3.2. Walking Speed (WS)
2.3.3. Handgrip Strength (HGS)
2.3.4. Skeletal Muscle Index (SMI)
2.4. Primary Outcome Measures
2.5. Other Covariates
2.6. Statistical Analysis
3. Results
3.1. Development of Sarcoscore by using Principal Component Analysis
3.2. Cut-off Values of Sarcoscore for Discriminating Sarcopenia Diagnosed by AWGS Criteria
3.3. Sarcoscore and Baseline Characteristics
3.4. Sarcoscore and the Risk of Functional Disabilities
4. Discussion
5. Conclusions
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bauer, J.; Morley, J.E.; Schols, A.M.; Ferrucci, L.; Cruz-Jentoft, A.J.; Dent, E.; Baracos, V.E.; Crawford, J.A.; Doehner, W.; Heymsfield, S.B.; et al. Sarcopenia: A Time for Action. An SCWD Position Paper. J. Cachex Sarcopenia Muscle 2019, 10, 956–961. [Google Scholar] [CrossRef] [PubMed]
- Landi, F.; Liperoti, R.; Russo, A.; Giovannini, S.; Tosato, M.; Capoluongo, E.D.; Bernabei, R.; Onder, G. Sarcopenia as a risk factor for falls in elderly individuals: Results from the ilSIRENTE study. Clin. Nutr. 2012, 31, 652–658. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Huang, P.; Dou, Q.; Wang, C.; Zhang, W.; Yang, Y.; Wang, J.; Xie, X.; Zhou, J.; Zeng, Y. Falls among older adults with sarcopenia dwelling in nursing home or community: A meta-analysis. Clin. Nutr. 2020, 39, 33–39. [Google Scholar] [CrossRef] [Green Version]
- Hirani, V.; Blyth, F.; Naganathan, V.; Le Couteur, D.; Seibel, M.; Waite, L.M.; Handelsman, D.; Cumming, R. Sarcopenia Is Associated with Incident Disability, Institutionalization, and Mortality in Community-Dwelling Older Men: The Concord Health and Ageing in Men Project. J. Am. Med. Dir. Assoc. 2015, 16, 607–613. [Google Scholar] [CrossRef]
- Bianchi, L.; Ferrucci, L.; Cherubini, A.; Maggio, M.; Bandinelli, S.; Savino, E.; Brombo, G.; Zuliani, G.; Guralnik, J.M.; Landi, F.; et al. The Predictive Value of the EWGSOP Definition of Sarcopenia: Results from the InCHIANTI Study. J. Gerontol. Ser. A: Boil. Sci. Med. Sci. 2015, 71, 259–264. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Rolland, Y.; Van Kan, G.A.; Bandinelli, S.; Vellas, B.; Ferrucci, L.; Kritchevsky, S. Sarcopenia-related parameters and incident disability in older persons: Results from the “invecchiare in Chianti” study. J. Gerontol. Ser. A: Boil. Sci. Med. Sci. 2014, 70, 457–463. [Google Scholar] [CrossRef] [Green Version]
- Zhang, X.; Zhang, W.; Wang, C.; Tao, W.; Dou, Q.; Yang, Y. Sarcopenia as a predictor of hospitalization among older people: A systematic review and meta-analysis. BMC Geriatr. 2018, 18, 188. [Google Scholar] [CrossRef]
- Liu, P.; Hao, Q.; Hai, S.; Wang, H.; Cao, L.; Dong, B. Sarcopenia as a predictor of all-cause mortality among community-dwelling older people: A systematic review and meta-analysis. Maturitas 2017, 103, 16–22. [Google Scholar] [CrossRef]
- Baumgartner, R.N.; Koehler, K.M.; Gallagher, D.; Romero, L.; Heymsfield, S.; Ross, R.R.; Garry, P.J.; Lindeman, R.D. Epidemiology of sarcopenia among the elderly in New Mexico. Am. J. Epidemiol. 1998, 147, 755–763. [Google Scholar] [CrossRef]
- Schaap, L.; Koster, A.; Visser, M. Adiposity, Muscle Mass, and Muscle Strength in Relation to Functional Decline in Older Persons. Epidemiol. Rev. 2012, 35, 51–65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Schaap, L.; Van Schoor, N.M.; Lips, P.; Visser, M. Associations of Sarcopenia Definitions, and Their Components, With the Incidence of Recurrent Falling and Fractures: The Longitudinal Aging Study Amsterdam. J. Gerontol. Ser. A: Boil. Sci. Med. Sci. 2017, 73, 1199–1204. [Google Scholar] [CrossRef] [PubMed]
- Cooper, R.; Kuh, D.; Hardy, R. Mortality Review Group Objectively measured physical capability levels and mortality: Systematic review and meta-analysis. BMJ 2010, 341, c4467. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Guralnik, J.; Simonsick, E.M.; Ferrucci, L.; Glynn, R.J.; Berkman, L.F.; Blazer, D.G.; Scherr, P.A.; Wallace, R.B. A Short Physical Performance Battery Assessing Lower Extremity Function: Association with Self-Reported Disability and Prediction of Mortality and Nursing Home Admission. J. Gerontol. 1994, 49, M85–M94. [Google Scholar] [CrossRef] [PubMed]
- Molfino, A.; Anker, S.; Argiles, J.; Aversa, Z.; Bauer, J.; Biolo, G.; Boirie, Y.; Bosaeus, I.; Cederholm, T.; Costelli, P.; et al. Consensus definition of sarcopenia, cachexia and pre-cachexia: Joint document elaborated by Special Interest Groups (SIG) “cachexia-anorexia in chronic wasting diseases” and “nutrition in geriatrics”. Clin. Nutr. 2010, 29, 154–159. [Google Scholar]
- Fielding, R.A.; Vellas, B.; Evans, W.J.; Bhasin, S.; Morley, J.E.; Newman, A.B.; Van Kan, G.A.; Andrieu, S.; Bauer, J.; Breuillé, D.; et al. Sarcopenia: An Undiagnosed Condition in Older Adults. Current Consensus Definition: Prevalence, Etiology, and Consequences. International Working Group on Sarcopenia. J. Am. Med. Dir. Assoc. 2011, 12, 249–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Morley, J.E.; Abbatecola, A.M.; Argiles, J.M.; Baracos, V.; Bauer, J.; Bhasin, S.; Cederholm, T.; Coats, A.J.; Cummings, S.R.; Evans, W.J.; et al. Sarcopenia with limited mobility: An international consensus. J. Am. Med. Dir. Assoc. 2011, 12, 40–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Studenski, S.; Peters, K.W.; Alley, D.E.; Cawthon, P.M.; McLean, R.R.; Harris, T.B.; Ferrucci, L.; Guralnik, J.M.; Fragala, M.S.; Kenny, A.M.; et al. The FNIH sarcopenia project: Rationale, study description, conference recommendations, and final estimates. J. Gerontol. Ser. A: Boil. Sci. Med. Sci. 2014, 69, 547–558. [Google Scholar] [CrossRef]
- Chen, L.-K.; Liu, L.-K.; Woo, J.; Assantachai, P.; Auyeung, T.-W.; Bahyah, K.S.; Chou, M.-Y.; Chen, L.-Y.; Hsu, P.-S.; Krairit, O.; et al. Sarcopenia in Asia: Consensus Report of the Asian Working Group for Sarcopenia. J. Am. Med. Dir. Assoc. 2014, 15, 95–101. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Baeyens, J.P.; Bauer, J.M.; Boirie, Y.; Cederholm, T.; Landi, F.; Martin, F.C.; Michel, J.-P.; Rolland, Y.; Schneider, S.M.; et al. Sarcopenia: European consensus on definition and diagnosis: Report of the European Working Group on Sarcopenia in Older People. Age Ageing 2010, 39, 412–423. [Google Scholar] [CrossRef] [Green Version]
- Woo, J.; Leung, J.; Morley, J. Defining Sarcopenia in Terms of Incident Adverse Outcomes. J. Am. Med. Dir. Assoc. 2015, 16, 247–252. [Google Scholar] [CrossRef] [PubMed]
- Fujiwara, Y.; Suzuki, H.; Kawai, H.; Hirano, H.; Yoshida, H.; Kojima, M.; Ihara, K.; Obuchi, S. Physical and Sociopsychological Characteristics of Older Community Residents with Mild Cognitive Impairment as Assessed by the Japanese Version of the Montreal Cognitive Assessment. J. Geriatr. Psychiatry Neurol. 2013, 26, 209–220. [Google Scholar] [CrossRef] [PubMed]
- Kera, T.; Kawai, H.; Hirano, H.; Kojima, M.; Watanabe, Y.; Fujiwara, Y.; Ihara, K.; Obuchi, S. Comparison of body composition and physical and cognitive function between older Japanese adults with no diabetes, prediabetes and diabetes: A cross-sectional study in community-dwelling Japanese older people. Geriatr. Gerontol. Int. 2018, 18, 1031–1037. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, Y.; Yoshida, H.; Fujiwara, Y.; Motohashi, Y.; Shinkai, S. A Prospective Study of Gait Performance and Subsequent Cognitive Decline in a General Population of Older Japanese. J. Gerontol. Ser. A: Boil. Sci. Med. Sci. 2012, 67, 796–803. [Google Scholar] [CrossRef] [Green Version]
- Murayama, H.; Nishi, M.; Shimizu, Y.; Kim, M.-J.; Yoshida, H.; Amano, H.; Fujiwara, Y.; Shinkai, S. The Hatoyama Cohort Study: Design and Profile of Participants at Baseline. J. Epidemiol. 2012, 22, 551–558. [Google Scholar] [CrossRef] [Green Version]
- Shinkai, S.; Watanabe, S.; Kumagai, S.; Fujiwara, Y.; Amano, H.; Yoshida, H.; Ishizaki, T.; Yukawa, H.; Suzuki, T.; Shibata, H. Walking speed as a good predictor for the onset of functional dependence in a Japanese rural community population. Age Ageing 2000, 29, 441–446. [Google Scholar] [CrossRef] [Green Version]
- Peters, D.M.; Fritz, S.L.; Krotish, D.E. Assessing the Reliability and Validity of a Shorter Walk Test Compared with the 10-Meter Walk Test for Measurements of Gait Speed in Healthy, Older Adults. J. Geriatr. Phys. Ther. 2013, 36, 24–30. [Google Scholar] [CrossRef]
- Mathiowetz, V.; Weber, K.; Volland, G.; Kashman, N. Reliability and validity of grip and pinch strength evaluations. J. Hand Surg. 1984, 9, 222–226. [Google Scholar] [CrossRef]
- Wang, C.-Y.; Chen, L.-Y. Grip Strength in Older Adults: Test-Retest Reliability and Cutoff for Subjective Weakness of Using the Hands in Heavy Tasks. Arch. Phys. Med. Rehabil. 2010, 91, 1747–1751. [Google Scholar] [CrossRef]
- Kim, M.; Shinkai, S.; Murayama, H.; Mori, S. Comparison of segmental multifrequency bioelectrical impedance analysis with dual-energy X-ray absorptiometry for the assessment of body composition in a community-dwelling older population. Geriatr. Gerontol. Int. 2014, 15, 1013–1022. [Google Scholar] [CrossRef]
- Janssen, I.; Baumgartner, R.N.; Ross, R.; Rosenberg, I.H.; Roubenoff, R. Skeletal muscle cutpoints associated with elevated physical disability risk in older men and women. Am. J. Epidemiol. 2004, 159, 413–421. [Google Scholar] [CrossRef] [PubMed]
- Lawton, M.P.; Brody, E.M. Assessment of Older People: Self-Maintaining and Instrumental Activities of Daily Living. Gerontology 1969, 9, 179–186. [Google Scholar] [CrossRef] [Green Version]
- Katz, S.; Ford, A.B.; Jackson, B.A.; Jaffe, M.W.; Moskowitz, R.W. Studies of Illness in the Aged. JAMA 1963, 185, 914. [Google Scholar] [CrossRef] [PubMed]
- Koyano, W.; Shibata, H.; Nakazato, K.; Haga, H.; Suyama, Y. Measurement of competence: Reliability and validity of the TMIG Index of Competence. Arch. Gerontol. Geriatr. 1991, 13, 103–116. [Google Scholar] [CrossRef]
- Ishizaki, T.; Watanabe, S.; Suzuki, T.; Shibata, H.; Haga, H. Predictors for functional decline among nondisabled older Japanese living in a community during a 3-year follow-up. J. Am. Geriatr. Soc. 2000, 48, 1424–1429. [Google Scholar] [CrossRef]
- Fujiwara, Y.; Yoshida, H.; Amano, H.; Fukaya, T.; Liang, J.; Uchida, H.; Shinkai, S. Predictors of Improvement or Decline in Instrumental Activities of Daily Living among Community-Dwelling Older Japanese. Gerontology 2008, 54, 373–380. [Google Scholar] [CrossRef]
- Suzuki, T.; Yoshida, H.; Kim, H.; Yukawa, H.; Sugiura, M.; Furuna, T.; Nishizawa, S.; Kumagai, S.; Shinkai, S.; Ishizaki, T.; et al. Walking speed as a good predictor for maintenance of I-ADL among the rural community elderly in Japan: A 5-year follow-up study from TMIG-LISA. Geriatr. Gerontol. Int. 2003, 3, S6–S14. [Google Scholar] [CrossRef]
- Boyle, P.A.; Buchman, A.S.; Wilson, R.S.; Bienias, J.L.; Bennett, D.A. Physical Activity Is Associated with Incident Disability in Community-Based Older Persons. J. Am. Geriatr. Soc. 2007, 55, 195–201. [Google Scholar] [CrossRef]
- Shinkai, S.; Amano, H.; Watanabe, S.; Kumagai, S.; Fujiwara, Y.; Yoshida, Y.; Ishizaki, T.; Suzuki, T.; Shibata, H. Predictors for the onset of functional decline among initially non-disabled older people living in a community during a 6-year follow-up. Geriatr. Gerontol. Int. 2003, 3, S31–S39. [Google Scholar] [CrossRef]
- Tsoi, K.K.; Chan, J.Y.C.; Hirai, H.W.; Wong, S.Y.-S.; Kwok, T.C.Y. Cognitive Tests to Detect Dementia. JAMA Intern. Med. 2015, 175, 1450. [Google Scholar] [CrossRef] [Green Version]
- Cesari, M.; Pahor, M.; Lauretani, F.; Zamboni, V.; Bandinelli, S.; Bernabei, R.; Guralnik, J.M.; Ferrucci, L. Skeletal Muscle and Mortality Results from the InCHIANTI Study. J. Gerontol. Ser. A: Boil. Sci. Med. Sci. 2009, 64, 377–384. [Google Scholar] [CrossRef] [PubMed]
- McLean, R.R.; Shardell, M.D.; Alley, D.E.; Cawthon, P.M.; Fragala, M.S.; Harris, T.B.; Kenny, A.M.; Peters, K.W.; Ferrucci, L.; Guralnik, J.M.; et al. Criteria for clinically relevant weakness and low lean mass and their longitudinal association with incident mobility impairment and mortality: The foundation for the National Institutes of Health (FNIH) sarcopenia project. J. Gerontol. Ser. A: Boil. Sci. Med. Sci. 2014, 69, 576–583. [Google Scholar] [CrossRef] [PubMed]
- Granic, A.; Davies, K.; Martin-Ruiz, C.; Jagger, C.; Kirkwood, T.B.L.; Von Zglinicki, T.; Sayer, A.A. Grip strength and inflammatory biomarker profiles in very old adults. Age Ageing 2017, 46, 976–982. [Google Scholar] [CrossRef] [Green Version]
- Verghese, J.; Holtzer, R.; Oh-Park, M.; Derby, C.A.; Lipton, R.B.; Wang, C. Inflammatory Markers and Gait Speed Decline in Older Adults. Journals Gerontol. Ser. A: Boil. Sci. Med. Sci. 2011, 66, 1083–1089. [Google Scholar] [CrossRef] [PubMed]
- Schaap, L.; Pluijm, S.M.; Deeg, R.J.; Visser, M. Inflammatory Markers and Loss of Muscle Mass (Sarcopenia) and Strength. Am. J. Med. 2006, 119, 526.e9–526.e17. [Google Scholar] [CrossRef] [PubMed]
- Stenholm, S.; Maggio, M.; Lauretani, F.; Bandinelli, S.; Ceda, G.; Di Iorio, A.; Giallauria, F.; Guralnik, J.M.; Ferrucci, L. Anabolic and Catabolic Biomarkers as Predictors of Muscle Strength Decline: The InCHIANTI Study. Rejuvenation Res. 2010, 13, 3–11. [Google Scholar] [CrossRef]
- Meng, Y.; Wu, H.; Yang, Y.; Du, H.; Xia, Y.; Guo, X.; Liu, X.; Li, C.; Niu, K. Relationship of anabolic and catabolic biomarkers with muscle strength and physical performance in older adults: A population-based cross-sectional study. BMC Musculoskelet. Disord. 2015, 16, 202. [Google Scholar] [CrossRef] [Green Version]
- Calvani, R.; Marini, F.; Cesari, M.; Tosato, M.; Anker, S.D.; Von Haehling, S.; Miller, R.R.; Bernabei, R.; Landi, F.; Marzetti, E.; et al. Biomarkers for physical frailty and sarcopenia: State of the science and future developments. J. Cachex-Sarcopenia Muscle 2015, 6, 278–286. [Google Scholar] [CrossRef]
- Phillips, A.; Strobl, R.; Vogt, S.; Ladwig, K.-H.; Thorand, B.; Grill, E. Sarcopenia is associated with disability status—Results from the KORA-Age study. Osteoporos. Int. 2017, 28, 2069–2079. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| All | Tercile of the Sarcoscore | ||||
|---|---|---|---|---|---|
| Low | Middle | High | p for Trend | ||
| n = 3088 | n = 1030 | n = 1028 | n = 1030 | ||
| Age, years | 71.4 (5.8) | 74.6 (6.2) | 70.9 (5.2) | 68.6 (4.1) | <0.001 |
| Sex, women | 1665 (53.9) | 548 (53.2) | 570 (55.4) | 547 (53.1) | 0.965 |
| Height, cm | 156.6 (8.8) | 153.5 (8.7) | 156.7 (8.2) | 159.7 (8.4) | <0.001 |
| Weight, kg | 56.8 (10.6) | 52.0 (9.2) | 56.4 (9.3) | 62.1 (10.6) | <0.001 |
| Body mass index, kg/cm2 | 23.1 (3.2) | 22.0 (3.0) | 22.9 (2.8) | 24.3 (3.4) | <0.001 |
| Education, <9 years | 193 (6.3) | 136 (13.2) | 36 (3.5) | 21 (2.0) | <0.001 |
| Hospitalization, yes | 269 (8.7) | 127 (12.3) | 71 (6.9) | 71 (6.9) | <0.001 |
| Medical history | |||||
| Stroke, yes | 187 (6.1) | 80 (7.8) | 62 (6.0) | 45 (4.4) | 0.001 |
| Heart disease, yes | 441 (14.3) | 169 (16.4) | 152 (14.8) | 120 (11.7) | 0.002 |
| Hypertension, yes | 1316 (42.6) | 469 (45.5) | 417 (40.6) | 430 (41.7) | 0.082 |
| Hyperlipidemia, yes | 965 (31.3) | 320 (31.1) | 325 (31.6) | 320 (31.1) | >0.990 |
| Diabetes, yes | 393 (12.7) | 155 (15.0) | 134 (13.0) | 104 (10.1) | 0.001 |
| COPD, yes | 94 (3.0) | 37 (3.6) | 30 (2.9) | 27 (2.6) | 0.201 |
| MMSE, point | 28.1 (2.2) | 27.5 (2.7) | 28.3 (2.1) | 28.6 (1.6) | <0.001 |
| Cognitive impairment, yes | 120 (3.9) | 77 (7.5) | 30 (2.9) | 13 (1.3) | 0.001 |
| IADL disability, yes | 152 (4.9) | 99 (9.6) | 37 (3.6) | 16 (1.6) | <0.001 |
| BADL disability, yes | 18 (1.5) | 15 (1.5) | 3 (0.3) | 0 (0.0) | <0.001 |
| Sarcoscore, point | 50.0 (10.0) | 39.1 (6.3) | 50.4 (2.3) | 60.6 (5.0) | <0.001 |
| Walking speed, m/sec | 1.34 (0.20) | 1.18 (0.23) | 1.36 (0.19) | 1.50 (0.21) | <0.001 |
| Handgrip strength, kg | 27.2 (8.8) | 21.8 (7.1) | 27.1 (7.3) | 32.6 (8.5) | <0.001 |
| Skeletal muscle index, kg/m2 | 6.56 (1.03) | 6.03 (0.90) | 6.53 (0.89) | 7.12 (0.99) | <0.001 |
| Events/All | Crude Model | Adjusted Model a | |||
|---|---|---|---|---|---|
| HR (95% CI) | p | HR (95% CI) | p | ||
| IADL Disability | |||||
| AWGS criteria | |||||
| Non-sarcopenia | 219/2326 | Reference | Reference | ||
| Sarcopenia | 59/245 | 2.73 (2.05–3.64) | <0.001 | 1.79 (1.32–2.43) | <0.001 |
| Sarcoscore criteria b | |||||
| High sarcoscore, >38.27 | 205/2326 | Reference | Reference | ||
| Low sarcoscore, ≤38.27 | 73/245 | 4.06 (3.11–5.31) | <0.001 | 2.19 (1.64–2.93) | <0.001 |
| Sarcoscore, for +1 point | 278/2571 | 0.93 (0.92–0.94) | <0.001 | 0.96 (0.94–0.97) | <0.001 |
| BADL Disability | |||||
| AWGS criteria | |||||
| Non-sarcopenia | 58/2109 | Reference | Reference | ||
| Sarcopenia | 30/232 | 5.43 (3.49–8.45) | <0.001 | 3.22 (1.97–5.27) | <0.001 |
| Sarcoscore criteria b | |||||
| High sarcoscore, >38.00 | 53/2109 | Reference | Reference | ||
| Low sarcoscore, ≤38.00 | 35/232 | 7.95 (5.18–12.19) | <0.001 | 4.28 (2.63–6.96) | <0.001 |
| Sarcoscore, for +1 point | 88/2341 | 0.90 (0.88–0.91) | <0.001 | 0.92 (0.90–0.94) | <0.001 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Osuka, Y.; Kim, H.; Kawai, H.; Taniguchi, Y.; Yokoyama, Y.; Seino, S.; Obuchi, S.; Kitamura, A.; Shinkai, S. Sarcoscore: A Novel Approach for Assessing Sarcopenia and Functional Disability in Older Adults. J. Clin. Med. 2020, 9, 692. https://doi.org/10.3390/jcm9030692
Osuka Y, Kim H, Kawai H, Taniguchi Y, Yokoyama Y, Seino S, Obuchi S, Kitamura A, Shinkai S. Sarcoscore: A Novel Approach for Assessing Sarcopenia and Functional Disability in Older Adults. Journal of Clinical Medicine. 2020; 9(3):692. https://doi.org/10.3390/jcm9030692
Chicago/Turabian StyleOsuka, Yosuke, Hunkyung Kim, Hisashi Kawai, Yu Taniguchi, Yuri Yokoyama, Satoshi Seino, Shuichi Obuchi, Akihiko Kitamura, and Shoji Shinkai. 2020. "Sarcoscore: A Novel Approach for Assessing Sarcopenia and Functional Disability in Older Adults" Journal of Clinical Medicine 9, no. 3: 692. https://doi.org/10.3390/jcm9030692