Impact of Having a Planned Additional Operation at Time of Liver Transplant on Graft and Patient Outcomes


Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients
2.2. Clinical Data
2.3. Outcomes
2.4. Statistical Analysis
3. Results
3.1. Patient Characteristics
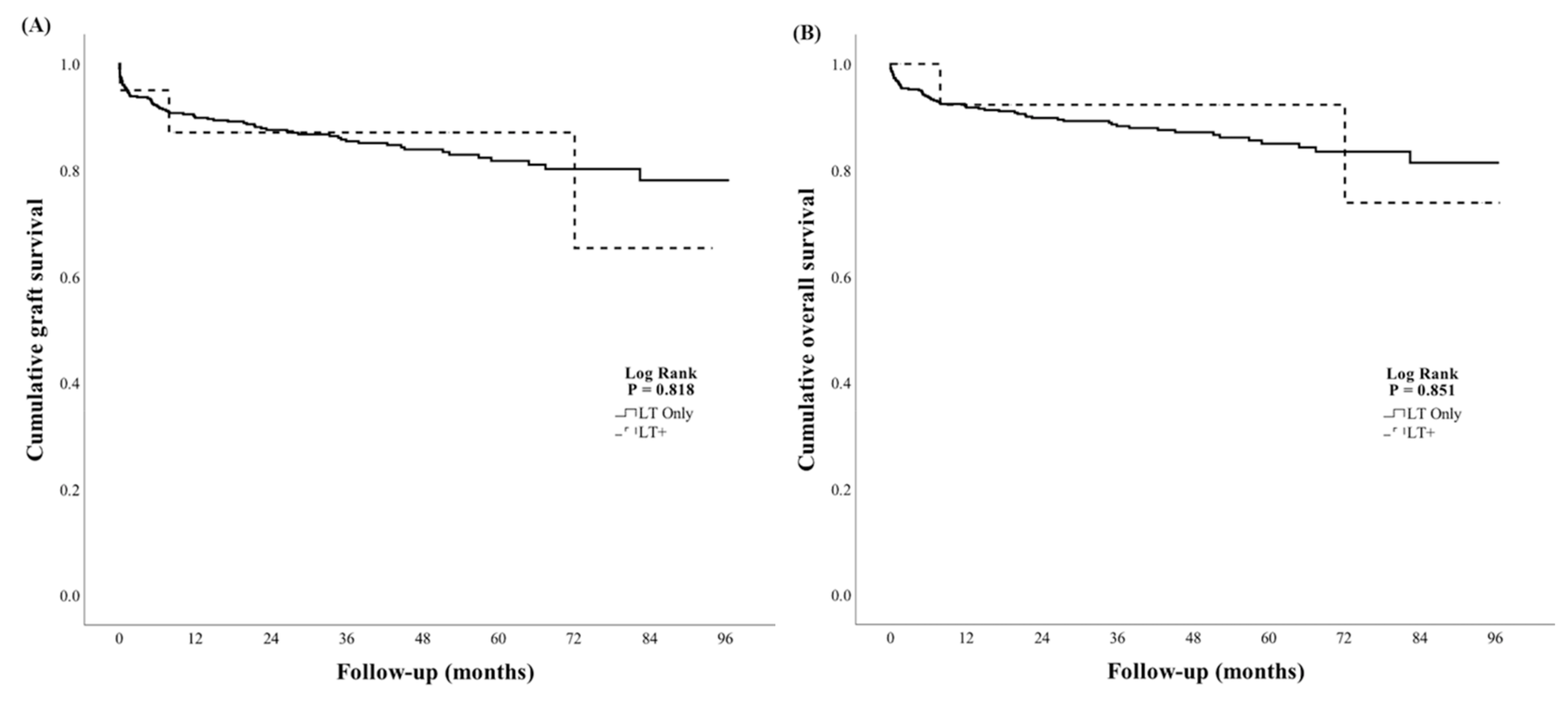
3.2. Liver Graft and Patient Survival Outcomes
3.3. Operative Outcomes
3.4. Hospital Lengths of Stay and Readmissions
4. Discussion
Author Contributions
Funding
Conflicts of Interest
References
- ANZLTR. Australia New Zealand Liver Transplant Registry Report 2017; ANZLTR: Brisbane, Australia, 2017. [Google Scholar]
- Gerken, G.; Paul, A. Challenges in Liver Transplantation. Visc. Med. 2016, 32, 232–233. [Google Scholar] [CrossRef] [Green Version]
- Song, A.T.W.; Avelino-Silva, V.I.; Pecora, R.A.A.; Pugliese, V.; D’Albuquerque, L.A.C.; Abdala, E. Liver transplantation: Fifty years of experience. World J. Gastroenterol. 2014, 20, 5363–5374. [Google Scholar] [CrossRef] [PubMed]
- Paolo, F.; Barbieri, S.; Galligioni, H.; Michieletto, E.; Carollo, C.; Ori, C. Intensive care management of liver transplanted patients. World J. Hepatol. 2011, 3, 61–71. [Google Scholar]
- Aduen, J.F.; Sujay, B.; Dickson, R.C.; Heckman, M.G.; Hewitt, W.R.; Stapelfeldt, W.H.; Steers, J.L.; Harnois, D.M.; Kramer, D.J. Outcomes After Liver Transplant in Patients Aged 70 Years or Older Compared With Those Younger Than 60 Years. Mayo Clin. Proc. 2009, 84, 973–978. [Google Scholar] [CrossRef]
- Haugen, C.E.; Holscher, C.M.; Garonzik-Wang, J.; Pozo, M.; Warsame, F.; McAdams-DeMarco, M.; Segev, D.L. National Trends in Liver Transplantation in Older Adults. J. Am. Geriatr. Soc. 2018, 66, 2321–2326. [Google Scholar] [CrossRef] [Green Version]
- Collins, B.H.; Pirsch, J.D.; Becker, Y.; Hanaway, M.J.; Van Der Werf, W.J.; D’alessandro, A.M.; Knechtle, S.J.; Odorico, J.S.; Leverson, G.; Musat, A.; et al. Long-term results of liver transplantation in patients 60 years of age and older12. Transplantation 2000, 70, 780–783. [Google Scholar] [CrossRef]
- Reverter, E.; Cirera, I.; Albillos, A.; Debernardi-Venon, W.; Abraldes, J.G.; Llop, E.; Flores, A.; Martínez-Palli, G.; Blasi, A.; Martínez, J.; et al. The prognostic role of hepatic venous pressure gradient in cirrhotic patients undergoing elective extrahepatic surgery. J. Hepatol. 2019, 71, 942–950. [Google Scholar] [CrossRef]
- Del Olmo, J.A.; Flor-Lorente, B.; Flor-Civera, B.; Rodriguez, F.; Serra, M.A.; Escudero, A.; Lledó, S.; Rodrigo, J.M. Risk Factors for Nonhepatic Surgery in Patients with Cirrhosis. World J. Surg. 2003, 27, 647–652. [Google Scholar] [CrossRef]
- Friedman, L.S. Surgery in the Patient with Liver Disease. Trans. Am. Clin. Clim. Assoc. 2010, 121, 192–205. [Google Scholar] [CrossRef]
- Hackl, C.; Schlitt, H.J.; Renner, P.; Lang, S.A. Liver surgery in cirrhosis and portal hypertension. World J. Gastroenterol. 2016, 22, 2725–2735. [Google Scholar] [CrossRef]
- Nesher, E.; Mor, E.; Shlomai, A.; Naftaly-Cohen, M.; Yemini, R.; Yussim, A.; Brown, M.; Keidar, A. Simultaneous Liver Transplantation and Sleeve Gastrectomy: Prohibitive Combination or a Necessity? Obes. Surg. 2017, 27, 1387–1390. [Google Scholar] [CrossRef] [PubMed]
- Ayloo, S.; Armstrong, J.; Hurton, S.; Molinari, M. Obesity and liver transplantation. World J. Transplant. 2015, 5, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Yoshizumi, T.; Taketomi, A.; Soejima, Y.; Ikegami, T.; Uchiyama, H.; Kayashima, H.; Harada, N.; Yamashita, Y.-I.; Kawanaka, H.; Nishizak, T.; et al. The beneficial role of simultaneous splenectomy in living donor liver transplantation in patients with small-for-size graft. Transpl. Int. 2008, 21, 833–842. [Google Scholar] [CrossRef] [PubMed]
- Neumann, U.P.; Langrehr, J.M.; Kaisers, U.; Lang, M.; Schmitz, V.; Neuhaus, P. Simultaneous splenectomy increases risk for opportunistic pneumonia in patients after live transplantation. Transpl. Int. 2002, 15, 226–232. [Google Scholar] [CrossRef] [PubMed]
- Lima, B.; Nowicki, E.R.; Miller, C.M.; Hashimoto, K.; Smedira, N.G.; Gonzalez-Stawinski, G.V. Outcomes of Simultaneous Liver Transplantation and Elective Cardiac Surgical Procedures. Ann. Thorac. Surg. 2011, 92, 1580–1584. [Google Scholar] [CrossRef] [PubMed]
- Raichlin, E.; Daly, R.C.; Rosen, C.B.; McGregor, C.G.; Charlton, M.R.; Frantz, R.P.; Clavell, A.L.; Rodeheffer, R.J.; Pereira, N.L.; Kremers, W.K.; et al. Combined Heart and Liver Transplantation: A Single-Center Experience. Transplantation 2009, 88, 219–225. [Google Scholar] [CrossRef]
- Kishi, Y.; Sugawara, Y.; Akamatsu, N.; Kaneko, J.; Tamura, S.; Kokudo, N.; Makuuchi, M. Splenectomy and preemptive interferon therapy for hepatitis C patients after living-donor liver transplantation. Clin. Transplant. 2005, 19, 769–772. [Google Scholar] [CrossRef]
- Dhupar, R.; De Vera, M.E.; Marsh, J.W.; Fontes, P.A.; Steel, J.L.; Zeh, H.J.; Gamblin, T.C. Simultaneous pancreatectomy and liver transplantation: A single-institution experience. HPB 2009, 11, 242–246. [Google Scholar] [CrossRef] [Green Version]
- Feng, S.; Goodrich, N.; Bragg-Gresham, J.; Dykstra, D.; Punch, J.; Debroy, M.; Greenstein, S.; Merion, R. Characteristics Associated with Liver Graft Failure: The Concept of a Donor Risk Index. Arab. Archaeol. Epigr. 2006, 6, 783–790. [Google Scholar] [CrossRef] [Green Version]
- Wiesner, R.H.; Edwards, E.; Freeman, R.; Harper, A.; Kim, R.; Kamath, P.; Kremers, W.; Lake, J.; Howard, T.; Merion, R.M.; et al. Model for end-stage liver disease (MELD) and allocation of donor livers. Gastroenterol. 2003, 124, 91–96. [Google Scholar] [CrossRef] [Green Version]
- Olthoff, K.; Kulik, L.; Samstein, B.; Kaminski, M.; Abecassis, M.; Emond, J.; Shaked, A.; Christie, J.D. Validation of a current definition of early allograft dysfunction in liver transplant recipients and analysis of risk factors. Liver Transplant. 2010, 16, 943–949. [Google Scholar] [CrossRef] [PubMed]
- Mehta, R.L.; Kellum, J.A.; Shah, S.V.; Molitoris, B.A.; Ronco, C.; Warnock, D.G.; Levin, A. Acute Kidney Injury Network: Report of an initiative to improve outcomes in acute kidney injury. Crit. Care 2007, 11, R31. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Troisi, R.; Hesse, U.J.; Decruyenaere, J.; Morelli, M.C.; Palazzo, U.; Pattyn, P.; Colardyn, F.; Maene, L.; De Hemptinne, B. Functional, life-threatening disorders and splenectomy following liver transplantation. Clin. Transplant. 1999, 13, 380–388. [Google Scholar] [CrossRef] [PubMed]
- Chu, H.-C.; Hsieh, C.-B.; Hsu, K.-F.; Fan, H.-L.; Hsieh, T.-Y.; Chen, T.-W. Simultaneous splenectomy during liver transplantation augments anti-viral therapy in patients infected with hepatitis C virus. Am. J. Surg. 2015, 209, 180–186. [Google Scholar] [CrossRef]
- Heimbach, J.K.; Watt, K.D.S.; Poterucha, J.J.; Ziller, N.F.; Cecco, S.D.; Charlton, M.R.; Hay, J.E.; Wiesner, R.H.; Sanchez, W.; Rosen, C.B.; et al. Combined Liver Transplantation and Gastric Sleeve Resection for Patients With Medically Complicated Obesity and End-Stage Liver Disease. Arab. Archaeol. Epigr. 2012, 13, 363–368. [Google Scholar] [CrossRef]
- Zamora-Valdes, D.; Watt, K.D.; Kellogg, T.A.; Poterucha, J.J.; Di Cecco, S.R.; Francisco-Ziller, N.M.; Taner, T.; Rosen, C.B.; Heimbach, J.K. Long-term outcomes of patients undergoing simultaneous liver transplantation and sleeve gastrectomy. Hepatol. 2018, 68, 485–495. [Google Scholar] [CrossRef] [Green Version]
- Kelly, M.E.; Spolverato, G.; Le, G.; Mavros, M.; Doyle, F.; Pawlik, T.; Winter, D. Synchronous colorectal liver metastasis: A network meta-analysis review comparing classical, combined, and liver-first surgical strategies. J. Surg. Oncol. 2014, 111, 341–351. [Google Scholar] [CrossRef]
- Joshi, D.; Bjarnason, I.; Belgaumkar, A.; O’Grady, J.; Suddle, A.; Heneghan, M.A.; Aluvihare, V.; Rela, M.; Heaton, N.; Agarwal, K. The impact of inflammatory bowel disease post-liver transplantation for primary sclerosing cholangitis. Liver Int. 2011, 33, 53–61. [Google Scholar] [CrossRef]
- Liu, K.; Strasser, S.I.; Koorey, D.J.; Leong, R.W.; Solomon, M.; McCaughan, G.W. Interactions between primary sclerosing cholangitis and inflammatory bowel disease: Implications in the adult liver transplant setting. Expert Rev. Gastroenterol. Hepatol. 2017, 11, 949–960. [Google Scholar] [CrossRef]


{kind=link}
| LT Only n = 527 | LT+ n = 20 | p | |
|---|---|---|---|
| Number of transplants per year group (%) | 0.062 | ||
| 2011–2013 | 139 (96) | 6 (4) | |
| 2014–2016 | 209 (99) | 3 (1) | |
| 2017–2019 | 179 (94) | 11 (6) | |
| Male (%) | 375 (71) | 16 (75) | 0.390 |
| Median age (IQR) | 54 (47–59) | 46 (38–60) | 0.131 |
| Primary indication for LT (%) | 0.601 | ||
| HCC | 142 (27) | 5 (25) | 0.847 |
| HCV | 102 (19) | 4 (20) | 0.943 |
| Alcoholic liver disease | 71 (13) | 5 (25) | 0.143 |
| NAFLD | 40 (8) | 2 (10) | 0.691 |
| ALF | 3 (1) | 0 (0) | 0.739 |
| Others | 169 (32) | 4 (20) | 0.255 |
| Re-transplant patient (%) | 27 (5) | 2 (10) | 0.339 |
| Inpatient at time of transplant offer (%) | 184 (35) | 6 (30) | 0.650 |
| Median pre-transplant MELD score (IQR) | 19 (14–25) | 13(10–25) | 0.141 |
| DCD donor (%) | 39 (7) | 1 (5) | 0.686 |
| DRI (%) | 1.6 (1.4–1.9) | 1.5 (1.4–1.7) | 0.192 |
| Split graft (%) | 63 (12) | 3 (15) | 0.681 |
| Additional Operation | n = 20 (%) | Timing in Relation to Implantation of the Donor Liver | Surgical Team |
|---|---|---|---|
| Abdominal operation | 17 (85) | ||
| Gastrointestinal | |||
| Total colectomy for Crohn’s colitis | 2 (10) | After | Transplant |
| Hemicolectomy for villous adenoma with dysplasia | 2 (10) | After | Colorectal |
| Sleeve gastrectomy for obesity | 2 (10) | After | Transplant |
| Small bowel resection of jejunal stromal tumor | 1 (5) | After | Transplant |
| Subtotal colectomy and ileostomy for colonic adenomas # | 1 (5) | After | Colorectal |
| Resection of ampullary hamartoma | 1 (5) | Before | Transplant |
| Ileocolic resection and formation of stoma for Crohn’s stricture of terminal ileum | 1 (5) | After | Transplant |
| Splenic * | |||
| Splenectomy for splenic artery aneurysm at hilum | 2 (10) | 1 Before, 1 After | Transplant |
| Splenic artery aneurysm ligation/excision | 2 (10) | Before | Transplant |
| Splenectomy for prevention of antibody mediated rejection in a re-transplanted patient | 1 (5) | Before | Transplant |
| Other | |||
| Whipple procedure for hilar cholangiocarcinoma | 1 (5) | After | Transplant |
| Partial nephrectomy for renal cell carcinoma | 1 (5) | Before | Urology |
| Cardiac operation | 3 (15) | ||
| Cardiac valve replacement for severe tricuspid regurgitation | 1 (5) | Before | Cardiothoracic |
| Cardiac valve replacement for severe aortic regurgitation | 1 (5) | Before | Cardiothoracic |
| Coronary artery bypass graft and atrial septal defect closure | 1 (5) | Before | Cardiothoracic |
| LT Only | LT+ | p | |
|---|---|---|---|
| EAD * (%) | 129 (25) | 3 (15) | 0.325 |
| AKIN 1 at 24 h (%) | 122 (23) | 6 (30) | 0.487 |
| AKIN 2 at 24 h (%) | 77 (15) | 2 (10) | 0.557 |
| AKIN 3 at 24 h (%) | 38 (7) | 1 (5) | 0.700 |
| AKI any at 24 h (%) | 237 (45) | 9 (45) | 0.984 |
| AKIN 1 at 48 h (%) | 105 (20) | 3 (15) | 0.572 |
| AKIN 2 at 48 h (%) | 91 (18) | 5 (25) | 0.389 |
| AKIN 3 at 48 h (%) | 65 (13) | 2 (10) | 0.739 |
| AKI any at 48 h (%) | 262 (50) | 10 (50) | 0.980 |
| LT Only | LT+ | p | |
|---|---|---|---|
| Total operative time in minutes (IQR) | 355 (289–425) | 451 (410–518) | 0.002 |
| Estimated blood loss in mL (IQR) | 3678 (2000–6183) | 4300 (2000–9000) | 0.625 |
| Units of blood products transfused intraoperatively (IQR) | |||
| PRBC | 4 (1–8) | 5 (0–12) | 0.748 |
| FFP | 6 (2–10) | 4 (2–13) | 0.691 |
| Platelets | 1 (0–2) | 0 (0–2) | 0.416 |
| Cryoprecipitate units | 8 (0–15) | 8 (0–10) | 0.532 |
| Cellsaver (mL) | 633 (220–1290) | 821 (230–1544) | 0.756 |
| Unplanned return to theater (%) | 109 (21) | 5 (25) | 0.644 |
| Hospital stay post-transplant (IQR) | 18 (13–27) | 18 (14–29) | 0.904 |
| Total ICU days (IQR) | 6 (4–10) | 6 (5–10) | 0.919 |
| Number of ICU stays (IQR) | 1 (1–1) | 1 (1–1) | 0.657 |
| Readmission in 30 days (%) | 151 (30) | 9 (45) | 0.154 |
| Readmission in 90 days (%) | 227 (46) | 13 (65) | 0.091 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Salimi, S.; Pandya, K.; Sastry, V.; West, C.; Virtue, S.; Wells, M.; Crawford, M.; Pulitano, C.; McCaughan, G.W.; Majumdar, A.; et al. Impact of Having a Planned Additional Operation at Time of Liver Transplant on Graft and Patient Outcomes. J. Clin. Med. 2020, 9, 608. https://doi.org/10.3390/jcm9020608
Salimi S, Pandya K, Sastry V, West C, Virtue S, Wells M, Crawford M, Pulitano C, McCaughan GW, Majumdar A, et al. Impact of Having a Planned Additional Operation at Time of Liver Transplant on Graft and Patient Outcomes. Journal of Clinical Medicine. 2020; 9(2):608. https://doi.org/10.3390/jcm9020608
Chicago/Turabian StyleSalimi, Shirin, Keval Pandya, Vinay Sastry, Claire West, Susan Virtue, Mark Wells, Michael Crawford, Carlo Pulitano, Geoffrey W. McCaughan, Avik Majumdar, and et al. 2020. "Impact of Having a Planned Additional Operation at Time of Liver Transplant on Graft and Patient Outcomes" Journal of Clinical Medicine 9, no. 2: 608. https://doi.org/10.3390/jcm9020608