Longitudinal Relationships between Asthma-Specific Quality of Life and Asthma Control in Children; The Influence of Chronic Rhinitis

 , ,
, ,
Abstract
:1. Introduction
- 1)
- between asthma control and asthma-specific QoL;
- 2)
- between clinical characteristics (e.g., the presence of chronic rhinitis, daily dosage of inhaled corticosteroids, lung function impairment, use of rescue medication, FeNO, and the occurrence of asthma exacerbations) and asthma-specific QoL.
2. Methods
2.1. Study Design and Patients
2.2. Study Parameters
2.3. Questionnaires on Asthma Control, Asthma-Specific QoL, and the International Study of Asthma and Allergies in Childhood (ISAAC)
2.4. FeNO
2.5. Dynamic Spirometry and Reversibility
2.6. Bronchial Hyperresponsiveness
2.7. Atopy
2.8. Medication Titration
2.9. Definition of Exacerbation
2.10. ISAAC Questionnaire and Chronic Rhinitis
2.11. Exposure to Second-Hand Smoke
2.12. Data Collection
2.13. Data Analysis
3. Results
3.1. Patient Characteristics
3.2. Influence of Chronic Rhinitis on QoL at Baseline
3.3. Course and Variability of Asthma-Specific QoL during the Study
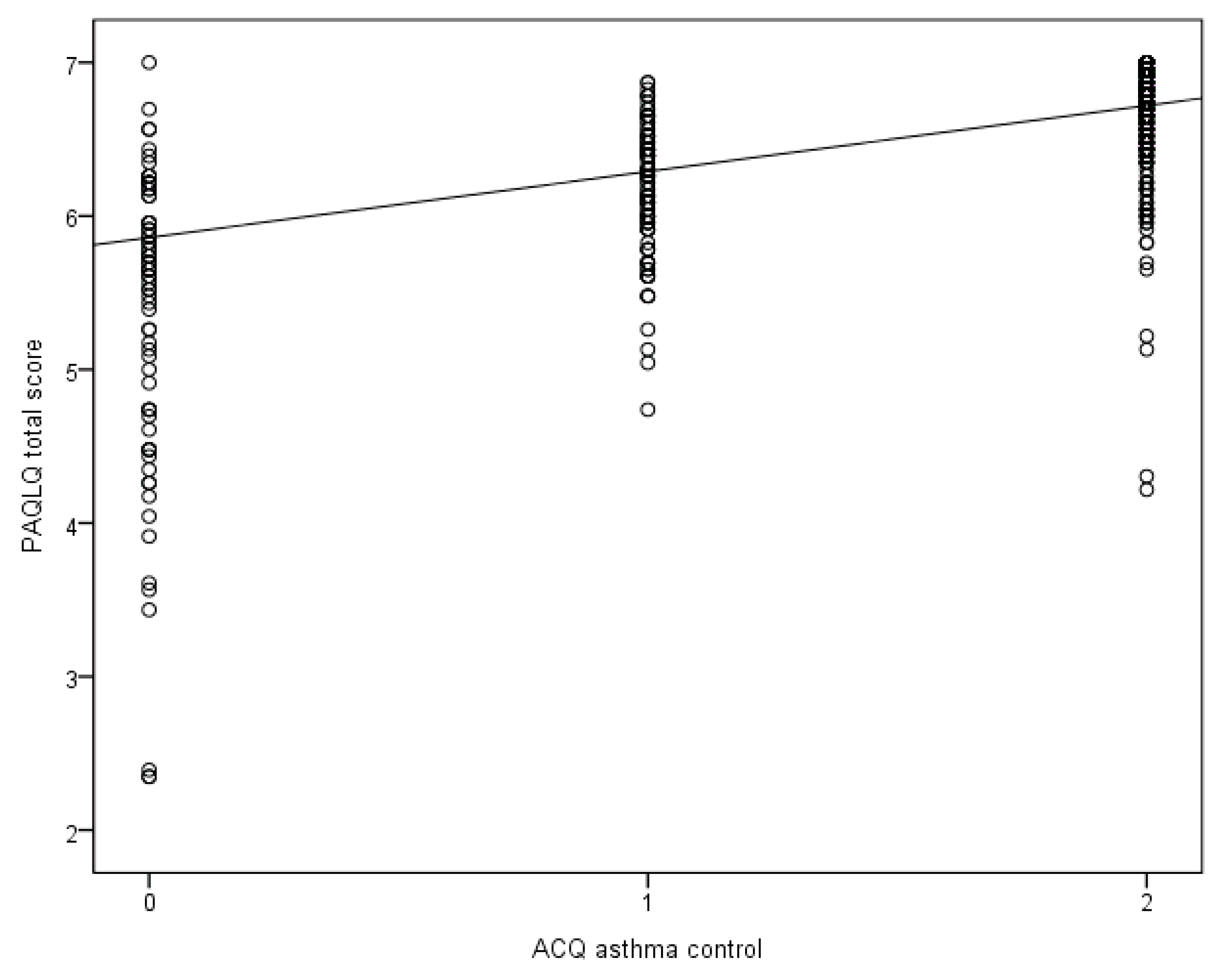
3.4. Association between Asthma Control and PAQLQ Scores during a One Year Follow-up
3.5. Factors Independently Related to PAQLQ Scores during One Year Follow-up
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Dean, B.B.; Calimlim, B.C.; Sacco, P.; Aguilar, D.; Maykut, R.; Tinkelman, D. Uncontrolled asthma: Assessing quality of life and productivity of children and their caregivers using a cross-sectional Internet-based survey. Health Qual. Life Outcomes 2010, 8, 96. [Google Scholar] [CrossRef] [Green Version]
- Wildhaber, J.; Carroll, W.D.; Brand, P.L. Global impact of asthma on children and adolescents’ daily lives: The room to breathe survey. Pediatric Pulmonol. 2012, 47, 346–357. [Google Scholar] [CrossRef] [PubMed]
- Global Strategy for Asthma Management and Prevention. Global Initiative for Asthma (GINA). 2019. Available online: https://ginasthma.org/gina-reports/ (accessed on 12 August 2019).
- National Heart Lung and Blood Instutute NAEaPP. Expert Panel Report 3: Guidelines for the Diagnosis and Management of Asthma-Summary Report 2007. J. Allergy Clin. Immunol. 2007, 120, S94. [Google Scholar] [CrossRef]
- Van de Griendt, J. Astma bij Kinderen; Herziene Richtlijnen van de Sectie Kinderlongziekten van de NVK Asthma in Children; The Paediatric Department of the Dutch Paediatric Society: Amsterdam, The Netherlands, 2013. [Google Scholar]
- Burkhart, P.V.; Svavarsdottir, E.K.; Rayens, M.K.; Oakley, M.G.; Orlygsdottir, B. Adolescents with asthma: Predictors of quality of life. J. Adv. Nurs. 2009, 65, 860–866. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, P.K.; Kenzik, K.M.; Thompson, L.A.; DeWalt, D.A.; Revicki, D.A.; Shenkman, E.A.; Huang, I.C. Exploring factors influencing asthma control and asthma-specific health-related quality of life among children. Respir. Res. 2013, 14, 26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juniper, E.F.; Guyatt, G.H.; Feeny, D.H.; Ferrie, P.J.; Griffith, L.E.; Townsend, M. Measuring quality of life in children with asthma. Qual. Life Res. 1996, 5, 35–46. [Google Scholar] [CrossRef]
- Juniper, E.F.; Wisniewski, M.E.; Cox, F.M.; Emmett, A.H.; Nielsen, K.E.; O’byrne, P.M. Relationship between quality of life and clinical status in asthma: A factor analysis. Eur. Respir. J. 2004, 23, 287–291. [Google Scholar] [CrossRef] [Green Version]
- Okelo, S.O.; Wu, A.W.; Krishnan, J.A.; Rand, C.S.; Skinner, E.A.; Diette, G.B. Emotional quality-of-life and outcomes in adolescents with asthma. J. Pediatric 2004, 145, 523–529. [Google Scholar] [CrossRef]
- Raat, H.; Bueving, H.J.; de Jongste, J.C.; Grol, M.H.; Juniper, E.F.; Van Der Wouden, J.C. Responsiveness, longitudinal- and cross-sectional construct validity of the Pediatric Asthma Quality of Life Questionnaire (PAQLQ) in Dutch children with asthma. Qual. Life Res. 2005, 14, 265–272. [Google Scholar] [CrossRef]
- Schmier, J.K.; Manjunath, R.; Halpern, M.T.; Jones, M.L.; Thompson, K.; Diette, G.B. The impact of inadequately controlled asthma in urban children on quality of life and productivity. Ann. Allergy Asthma Immunol. 2007, 98, 245–251. [Google Scholar] [CrossRef]
- Annett, R.D.; Bender, B.G.; Skipper, B.; Allen, C. Predicting moderate improvement and decline in pediatric asthma quality of life over 24 months. Qual. Life Res. 2010, 19, 1517–1527. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Van Vliet, D.; Alonso, A.; Rijkers, G.; Heynens, J.; Rosias, P.; Muris, J.; Jobsis, Q.; Dompeling, E. Prediction of asthma exacerbations in children by innovative exhaled inflammatory markers: Results of a longitudinal study. PLoS ONE 2015, 10, e0119434. [Google Scholar] [CrossRef] [PubMed]
- Dales, R.E.; Spitzer, W.O.; Tousignant, P.; Schechter, M.; Suissa, S. Clinical interpretation of airway response to a bronchodilator. Epidemiologic considerations. Am. Rev. Respir. Dis. 1988, 138, 317–320. [Google Scholar] [CrossRef] [PubMed]
- Juniper, E.F.; Gruffydd-Jones, K.; Ward, S.; Svensson, K. Asthma Control Questionnaire in children: Validation, measurement properties, interpretation. Eur. Respir. J. 2010, 36, 1410–1416. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Juniper, E.F.; O’Byrne, P.M.; Guyatt, G.H.; Ferrie, P.J.; King, D.R. Development and validation of a questionnaire to measure asthma control. Eur. Respir. J. 1999, 14, 902–907. [Google Scholar] [CrossRef]
- Juniper, E.F.; Svensson, K.; Mork, A.C.; Stahl, E. Modification of the asthma quality of life questionnaire (standardised) for patients 12 years and older. Health Qual. Life Outcomes 2005, 3, 58. [Google Scholar] [CrossRef] [Green Version]
- American Thoracic, S.; European Respiratory, S. ATS/ERS recommendations for standardized procedures for the online and offline measurement of exhaled lower respiratory nitric oxide and nasal nitric oxide, 2005. Am. J. Respir. Crit. Care Med. 2005, 171, 912–930. [Google Scholar]
- Miller, M.R.; Hankinson, J.; Brusasco, V.; Burgos, F.; Casaburi, R.; Coates, A.; Crapo, R.; Enright, P.v.d.; Van der Grinten, C.P.M.; Gustafsson, P.; et al. Standardisation of spirometry. Eur. Respir. J. 2005, 26, 319–338. [Google Scholar] [CrossRef] [Green Version]
- Sterk, P.J.; Fabbri, L.M.; Quanjer, P.H.; Cockcroft, D.W.; O’Byrne, P.M.; Anderson, S.D.; Juniper, E.F.; Malo, J.L. Airway responsiveness. Standardized challenge testing with pharmacological, physical and sensitizing stimuli in adults. Report Working Party Standardization of Lung Function Tests, European Community for Steel and Coal. Official Statement of the European Respiratory Society. Eur. Respir. J. Suppl. 1993, 16, 53–83. [Google Scholar]
- Reddel, H.K.; Taylor, D.R.; Bateman, E.D.; Boulet, L.-P.; Boushey, Н.A.; Busse, W.W.; Casale, T.B.; Chanez, P.; Enright, P.L.; Gibson, P.G.; et al. Exacerbations. An official American Thoracic Society/European Respiratory Society statement: Asthma control and exacerbations: Standardizing endpoints for clinical asthma trials and clinical practice. Am. J. Respir. Crit. Care Med. 2009, 180, 59–99. [Google Scholar] [CrossRef] [Green Version]
- Asher, M.I.; Keil, U.; Anderson, H.R.; Beasley, R.; Crane, J.; Martinez, F.; Mitchell, E.A.; Pearce, N.; Sibbald, B.; Stewart, A.W.; et al. International Study of Asthma and Allergies in Childhood (ISAAC): Rationale and methods. Eur. Respir. J. 1995, 8, 483–491. [Google Scholar] [CrossRef]
- Fitzmaurice, G.M.L.N.; Ware, J.H. Applied longitudinal analysis; John Wiley & Sons, Inc.: Hoboken, NJ, USA, 2004. [Google Scholar]
- Carranza Rosenzweig, J.R.; Edwards, L.; Lincourt, W.; Dorinsky, P.; ZuWallack, R.L. The relationship between health-related quality of life, lung function and daily symptoms in patients with persistent asthma. Respir. Med. 2004, 98, 1157–1165. [Google Scholar] [CrossRef] [Green Version]
- De Jongste, J.C.; Carraro, S.; Hop, W.C.; Baraldi, E.; CHARISM Study Group. Daily telemonitoring of exhaled nitric oxide and symptoms in the treatment of childhood asthma. Am. J. Respir. Crit. Care Med. 2009, 179, 93–97. [Google Scholar] [CrossRef]
- Luskin, A.T.; Chipps, B.E.; Rasouliyan, L.; Miller, D.P.; Haselkorn, T.; Dorenbaum, A. Impact of asthma exacerbations and asthma triggers on asthma-related quality of life in patients with severe or difficult-to-treat asthma. J. Allergy Clin. Immunol. Pract. 2014, 2, 544–552.e2. [Google Scholar] [CrossRef]
- Petsios, K.T.; Priftis, K.N.; Hatziagorou, E.; Tsanakas, J.N.; Antonogeorgos, G.; Matziou, V.N. Determinants of quality of life in children with asthma. Pediatric Pulmonol. 2013, 48, 1171–1180. [Google Scholar] [CrossRef]
- Mancuso, C.A.; Peterson, M.G. Different methods to assess quality of life from multiple follow-ups in a longitudinal asthma study. J. Clin. Epidemiol. 2004, 57, 45–54. [Google Scholar] [CrossRef]
- Annett, R.D.; Bender, B.G.; DuHamel, T.R.; Lapidus, J. Factors influencing parent reports on quality of life for children with asthma. J. Asthma 2003, 40, 577–587. [Google Scholar] [CrossRef]
- Eiser, C.; Morse, R. Can parents rate their child’s health-related quality of life? Results of a systematic review. Qual. Life Res. 2001, 10, 347–357. [Google Scholar] [CrossRef]
- Montalbano, L.; Cilluffo, G.; Gentile, M.; Ferrante, G.; Malizia, V.; Cibella, F.; Viegi, G.; Passalacqua, G.; La Grutta, S. Development of a nomogram to estimate the quality of life in asthmatic children using the Childhood Asthma Control Test. Pediatric Allergy Immunol. 2016, 27, 514–520. [Google Scholar] [CrossRef]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Step up |
| Uncontrolled asthma in 1 visit, or |
| partly controlled asthma during 2 consecutive visits. |
| No change in treatment |
| One visit with controlled asthma, or |
| one visit with partly controlled asthma. |
| Step down |
| Two consecutive visits with controlled asthma. |
| Parameter | Value |
|---|---|
| Mean age [range], in years | 10 [6–17] |
| Sex male/female, n | 50/46 |
| ACQ score, median [IQR] | 0.6 [0.3–1] |
| PAQLQ total score, median [IQR] | 6.4 [5.9–6.7] |
| Symptoms domain, median [IQR] | 6.4 [5.5–6.7] |
| Activity limitations domain, median [IQR] | 6.2 [5.3–6.6] |
| Emotional functioning domain, median [IQR] | 6.9 [6.5–7.0] |
| FeNO, ppb: median [IQR] | 12.5 [8.0–31.0] |
| FEV1 % predicted, mean ± SD | 96.8 ± 14.2 |
| Reversibility, increase in FEV1 % predicted: mean ± SD | 6.6 ± 8.5 |
| ICS dose of inhaled fluticasone or equivalent, mean ± SD * | 269 ± 175 |
| PC20, mg/mL: median [IQR] † | 1.2 [0.3–2.9] |
| Atopic, n % ‡ | 76 |
| Chronic rhinitis, % | 70 |
| Wheezing episodes past year, % | 58 |
| Parental smoking, % | 26 |
| Exposure to second-hand smoke, % | 8 |
| PAQLQ total score | PAQLQ symptoms domain | PAQLQ activity limitations domain | |||||||
|---|---|---|---|---|---|---|---|---|---|
| β | CI | Pvalue | β | CI | Pvalue | β | CI | Pvalue | |
| ACQ asthma level of control* | 0.43 | 0.37, 0.50 | <0.01 | 0.63 | 0.54, 0.71 | <0.01 | 0.60 | 0.50, 0.69 | <0.01 |
| Fluticasone daily dosage or equivalent per 100 µg † | −0.04 | −0.07, −0.008 | 0.01 | −0.06 | −0.10, −0.02 | <0.01 | −0.04 | −0.08, −0.0004 | 0.05 |
| Season‡ | ‡ | ‡ | 0.01 | 0.01 | - | - | - | ||
| Sex§ | - | - | - | - | - | - | −0.19 | −0.36, −0.02 | 0.03 |
| PAQLQ total score | PAQLQ symptoms domain | PAQLQ activity limitations domain | |||||||
|---|---|---|---|---|---|---|---|---|---|
| β | CI | Pvalue | β | CI | Pvalue | β | CI | Pvalue | |
| GINA asthma level of control* | 0.38 | 0.30, 0.46 | <0.01 | 0.57 | 0.47, 0.66 | <0.01 | 0.56 | 0.44, 0.67 | <0.01 |
| Wheezing episodes preceding year no/yes† | −0.29 | −0.10, −0.49 | <0.01 | −0.42 | −0.16, −0.69 | <0.01 | −0.36 | −0.05, −0.66 | 0.02 |
| Age in years‡ | - | - | - | −0.04 | −0.08, <0.01 | 0.03 | −0.05 | −0.1, −0.01 | 0.02 |
| Exacerbation in previous 2 months no/yes§ | - | - | - | −0.19 | −0.35, −0.02 | 0.03 | - | - | - |
| PAQLQ total score | PAQLQ symptoms domain | PAQLQ activity limitations domain | |||||||
|---|---|---|---|---|---|---|---|---|---|
| β | CI | Pvalue | β | CI | Pvalue | β | CI | Pvalue | |
| FEV1 per 10% predicted value * | 0.05 | 0.01, 0.08 | <0.01 | 0.08 | 0.03, 0.12 | <0.01 | 0.06 | 0.00, 0.11 | 0.04 |
| β2-agonist use † | −0.25 | −0.32, −0.18 | <0.01 | −0.40 | −0.49, −0.31 | <0.01 | −0.39 | −0.49, 0.28 | <0.01 |
| Exacerbation previous 2 months no/yes ‡ | −0.18 | −0.30, −0.07 | <0.01 | −0.36 | −0.51, −0.20 | <0.01 | - | - | - |
| Wheezing episodes preceding year no/yes § | −0.23 | −0.06, −0.41 | 0.01 | −0.30 | −0.06, −0.54 | 0.02 | −0.27 | −0.01, −0.53 | 0.04 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
van Vliet, D.; Essers, B.A.; Winkens, B.; Heynens, J.W.; Muris, J.W.; Jöbsis, Q.; Dompeling, E. Longitudinal Relationships between Asthma-Specific Quality of Life and Asthma Control in Children; The Influence of Chronic Rhinitis. J. Clin. Med. 2020, 9, 555. https://doi.org/10.3390/jcm9020555
van Vliet D, Essers BA, Winkens B, Heynens JW, Muris JW, Jöbsis Q, Dompeling E. Longitudinal Relationships between Asthma-Specific Quality of Life and Asthma Control in Children; The Influence of Chronic Rhinitis. Journal of Clinical Medicine. 2020; 9(2):555. https://doi.org/10.3390/jcm9020555
Chicago/Turabian Stylevan Vliet, Dillys, Brigitte A. Essers, Bjorn Winkens, Jan W. Heynens, Jean W. Muris, Quirijn Jöbsis, and Edward Dompeling. 2020. "Longitudinal Relationships between Asthma-Specific Quality of Life and Asthma Control in Children; The Influence of Chronic Rhinitis" Journal of Clinical Medicine 9, no. 2: 555. https://doi.org/10.3390/jcm9020555