A New Site Preparation Protocol That Supports Bone Quality Evaluation and Provides Predictable Implant Insertion Torque


Abstract
:1. Introduction
2. Materials and Methods
2.1. In Vitro Bone Surrogate
2.2. In Vitro Bovine Trabecular Bone
2.3. In Vivo Yucatan Minipig
2.4. In Vivo Clinical Handling Surveys
2.5. Statistical Evaluation
3. Results
3.1. Correlation of OS1 Torque and Bone Density
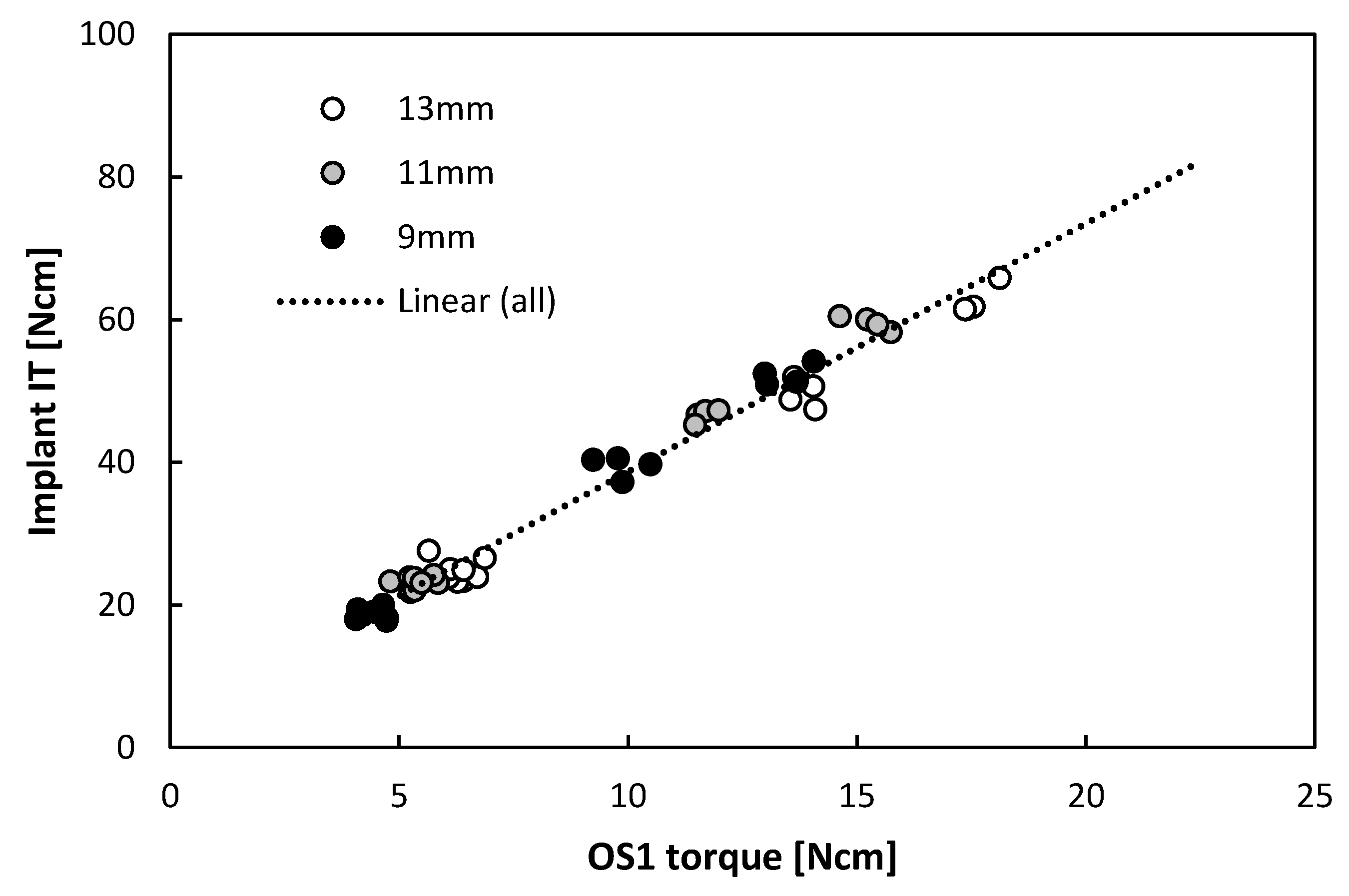
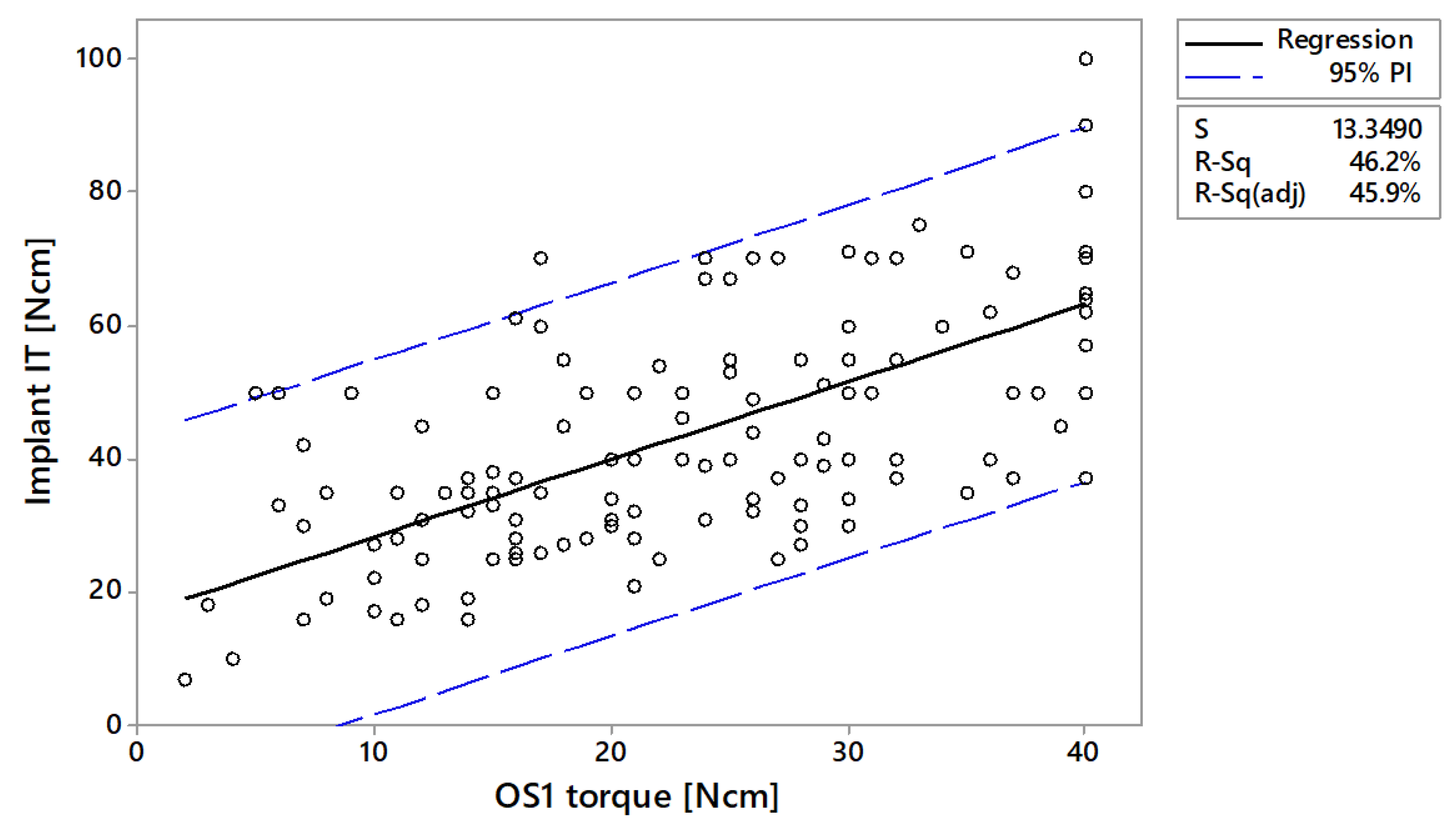
3.2. Correlation of OS1 Torque and Implant Insertion Torque
3.3. Clinicians’ Estimation of Bone Quality In Vivo
3.4. Implant Insertion Torques In Vivo
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Floyd, P.; Palmer, P.; Palmer, R. Radiographic technique. Br. Dent. J. 1999, 187, 359–365. [Google Scholar] [CrossRef] [PubMed]
- Chan, H.L.; Misch, K.; Wang, H.L. Dental imaging in implant treatment planning. Implant Dent. 2010, 19, 288–298. [Google Scholar] [CrossRef] [PubMed]
- Kim, I.H.; Singer, S.R.; Mupparapu, M. Review of cone beam computed tomography guidelines in North America. Quintessence Int. 2019, 50, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Carter, D.R.; Hayes, W.C. Bone compressive strength: The influence of density and strain rate. Science 1976, 194, 1174–1176. [Google Scholar] [CrossRef]
- Leichter, I.; Margulies, J.Y.; Weinreb, A.; Mizrahi, J.; Robin, G.C.; Conforty, B.; Makin, M.; Bloch, B. The relationship between bone density, mineral content, and mechanical strength in the femoral neck. Clin. Orthop. Relat. Res. 1982, 163, 272–281. [Google Scholar] [CrossRef]
- Lughmani, W.A.; Farukh, F.; Bouazza-Marouf, K.; Ali, H. Drilling resistance: A method to investigate bone quality. Acta Bioeng. Biomech. 2017, 19, 55–62. [Google Scholar] [PubMed]
- Voumard, B.; Maquer, G.; Heuberger, P.; Zysset, P.K.; Wolfram, U. Peroperative estimation of bone quality and primary dental implant stability. J. Mech. Behav. Biomed. Mater. 2019, 92, 24–32. [Google Scholar] [CrossRef]
- Lindh, C.; Oliveira, G.H.C.; Leles, C.R.; do Carmo Matias Freire, M.; Ribeiro-Rotta, R.F. Bone quality assessment in routine dental implant treatment among Brazilian and Swedish specialists. Clin. Oral Implant. Res. 2014, 25, 1004–1009. [Google Scholar] [CrossRef]
- Linck, G.K.; Ferreira, G.M.; De Oliveira, R.C.; Lindh, C.; Leles, C.R.; Ribeiro-Rotta, R.F. The Influence of Tactile Perception on Classification of Bone Tissue at Dental Implant Insertion. Clin. Implant Dent. Relat. Res. 2016, 18, 601–608. [Google Scholar] [CrossRef]
- Alghamdi, H.S. Methods to Improve Osseointegration of Dental Implants in Low Quality (Type-IV) Bone: An Overview. J. Funct. Biomater. 2018, 9, 7. [Google Scholar] [CrossRef] [Green Version]
- Stavropoulos, A.; Cochran, D.; Obrecht, M.; Pippenger, B.E.; Dard, M. Effect of Osteotomy Preparation on Osseointegration of Immediately Loaded, Tapered Dental Implants. Adv. Dent. Res. 2016, 28, 34–41. [Google Scholar] [CrossRef] [PubMed]
- Gilmer, B.B.; Lang, S.D. Dual Motor Drill Continuously Measures Drilling Energy to Calculate Bone Density and Screw Pull-out Force in Real Time. J. Am. Acad. Orthop. Surg. Glob. Res. Rev. 2018, 2, e053. [Google Scholar] [CrossRef] [PubMed]
- Karl, M.; Buder, T.; Krafft, T.; Grobecker-Karl, T. Reliability of clinical techniques for evaluating alveolar bone quality and primary implant stability. Quintessence Int. 2019, 50, 388–393. [Google Scholar] [CrossRef] [PubMed]
- Krafft, T.; Winter, W.; Wichmann, M.; Karl, M. In vitro validation of a novel diagnostic device for intraoperative determination of alveolar bone quality. Int. J. Oral Maxillofac. Implant. 2012, 27, 318–328. [Google Scholar]
- Susin, C.; Finger Stadler, A.; Musskopf, M.L.; de Sousa Rabelo, M.; Ramos, U.D.; Fiorini, T. Safety and efficacy of a novel, gradually anodized dental implant surface: A study in Yucatan mini pigs. Clin. Implant Dent. Relat. Res. 2019, 21, 44–54. [Google Scholar] [CrossRef] [Green Version]
- Lekholm, U.; Zarb, G.A. Patient Selection and Preparation. In Tissue-Integrated Prosthesis. Osseointegration in Clinical Dentistry; Branemark, P.I., Zarb, G.A., Albrektsson, T., Eds.; Quintessence Publishing Co., Inc.: Chicago, IL, USA, 1985; Volume 1, pp. 199–208. [Google Scholar]
- Coelho, P.G.; Jimbo, R. Osseointegration of metallic devices: Current trends based on implant hardware design. Arch. Biochem. Biophys. 2014, 561, 99–108. [Google Scholar] [CrossRef]
- Sakka, S.; Baroudi, K.; Nassani, M.Z. Factors associated with early and late failure of dental implants. J. Investig. Clin. Dent. 2012, 3, 258–261. [Google Scholar] [CrossRef]
- Tretto, P.H.W.; Fabris, V.; Cericato, G.O.; Sarkis-Onofre, R.; Bacchi, A. Does the instrument used for the implant site preparation influence the bone-implant interface? A systematic review of clinical and animal studies. Int. J. Oral Maxillofac. Surg. 2019, 48, 97–107. [Google Scholar] [CrossRef] [Green Version]
- Chen, C.H.; Coyac, B.R.; Arioka, M.; Leahy, B.; Tulu, U.S.; Aghvami, M.; Holst, S.; Hoffmann, W.; Quarry, A.; Bahat, O.; et al. A Novel Osteotomy Preparation Technique to Preserve Implant Site Viability and Enhance Osteogenesis. J. Clin. Med. 2019, 8, 170. [Google Scholar] [CrossRef] [Green Version]
- Lee, J.; Chavez, C.L.; Park, J. Parameters affecting mechanical and thermal responses in bone drilling: A review. J. Biomech. 2018, 71, 4–21. [Google Scholar] [CrossRef]
- Di Stefano, D.A.; Arosio, P.; Gastaldi, G.; Gherlone, E. The insertion torque-depth curve integral as a measure of implant primary stability: An in vitro study on polyurethane foam blocks. J. Prosthet. Dent. 2018, 120, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Wang, T.M.; Lee, M.S.; Wang, J.S.; Lin, L.D. The effect of implant design and bone quality on insertion torque, resonance frequency analysis, and insertion energy during implant placement in low or low- to medium-density bone. Int. J. Prosthodont. 2015, 28, 40–47. [Google Scholar] [CrossRef] [PubMed]
- Gehrke, S.A.; Guirado, J.L.C.; Bettach, R.; Fabbro, M.D.; Martinez, C.P.; Shibli, J.A. Evaluation of the insertion torque, implant stability quotient and drilled hole quality for different drill design: An in vitro Investigation. Clin. Oral Implant. Res. 2018, 29, 656–662. [Google Scholar] [CrossRef] [PubMed]
- MatWeb. Sawbones Solid Rigid Polyurethane Foam 20 pcf Density. Available online: http://www.matweb.com/search/datasheettext.aspx?matguid=d7487588e1504732abe583d6d9252bfa (accessed on 5 November 2019).
- Lee, J.H.; Kim, H.J.; Yun, J.H. Three-dimensional microstructure of human alveolar trabecular bone: A micro-computed tomography study. J. Periodontal Implant Sci. 2017, 47, 20–29. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Gredes, T.; Kubasiewicz-Ross, P.; Gedrange, T.; Dominiak, M.; Kunert-Keil, C. Comparison of surface modified zirconia implants with commercially available zirconium and titanium implants: A histological study in pigs. Implant Dent. 2014, 23, 502–507. [Google Scholar] [CrossRef]
- Linares, A.; Domken, O.; Dard, M.; Blanco, J. Peri-implant soft tissues around implants with a modified neck surface. Part 1. Clinical and histometric outcomes: A pilot study in minipigs. J. Clin. Periodontol. 2013, 40, 412–420. [Google Scholar] [CrossRef]








{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study Category | Evaluated Parameter | Inclusion | Exclusion |
|---|---|---|---|
| In vitro |
| All | None |
| Implants placed immediately after OS1 | None | |
| In vivo |
| All | Data incomplete |
| Implants placed immediately after OS1 | Data incomplete |
| Estimated Bone Quality [16] | Minipig | Human |
|---|---|---|
| n = 29 | n = 191 | |
| Type I | n = 0 (0%) | n = 12 (6%) |
| Type II | n = 10 (35%) | n = 36 (19%) |
| Type III | n = 14 (48%) | n = 95 (50%) |
| Type IV | n = 5 (17%) | n = 48 (25%) |
| OS1 Torque Range [Ncm] | Minipig | Human | ||
|---|---|---|---|---|
| Implant IT Mean ± SD 1 [Ncm] | Implant IT 95% PI 2 [Ncm] | Implant IT Mean ± SD 1 [Ncm] | Implant IT 95% PI 2 [Ncm] | |
| 0–10 | N/A (n = 1) | 0–29 | 27.8 ± 13.5 (n = 17) | 0–54 |
| 10–20 | N/A (n = 0) | 0–41 | 34.2 ± 11.5 (n = 44) | 2–67 |
| 20–30 | 28.3 ± 5.8 (n = 3) | 9–55 | 45.2 ± 13.7 (n = 46) | 13–78 |
| 30–40 | 48.8 ± 7.7 (n = 25) | 25–69 | 62.1 ± 14.9 (n = 39) | 25–90 |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Velikov, S.; Susin, C.; Heuberger, P.; Irastorza-Landa, A. A New Site Preparation Protocol That Supports Bone Quality Evaluation and Provides Predictable Implant Insertion Torque. J. Clin. Med. 2020, 9, 494. https://doi.org/10.3390/jcm9020494
Velikov S, Susin C, Heuberger P, Irastorza-Landa A. A New Site Preparation Protocol That Supports Bone Quality Evaluation and Provides Predictable Implant Insertion Torque. Journal of Clinical Medicine. 2020; 9(2):494. https://doi.org/10.3390/jcm9020494
Chicago/Turabian StyleVelikov, Stefan, Cristiano Susin, Peter Heuberger, and Ainara Irastorza-Landa. 2020. "A New Site Preparation Protocol That Supports Bone Quality Evaluation and Provides Predictable Implant Insertion Torque" Journal of Clinical Medicine 9, no. 2: 494. https://doi.org/10.3390/jcm9020494