Presence of Cutaneous Complement Deposition Distinguishes between Immunological and Histological Features of Bullous Pemphigoid—Insights from a Retrospective Cohort Study

Abstract
:1. Introduction
2. Methods
2.1. Study Population and Definition of Patients
2.2. Definition of Covariates
2.3. Statistical Analysis
3. Results
3.1. Demographic Characteristics of the Study Population
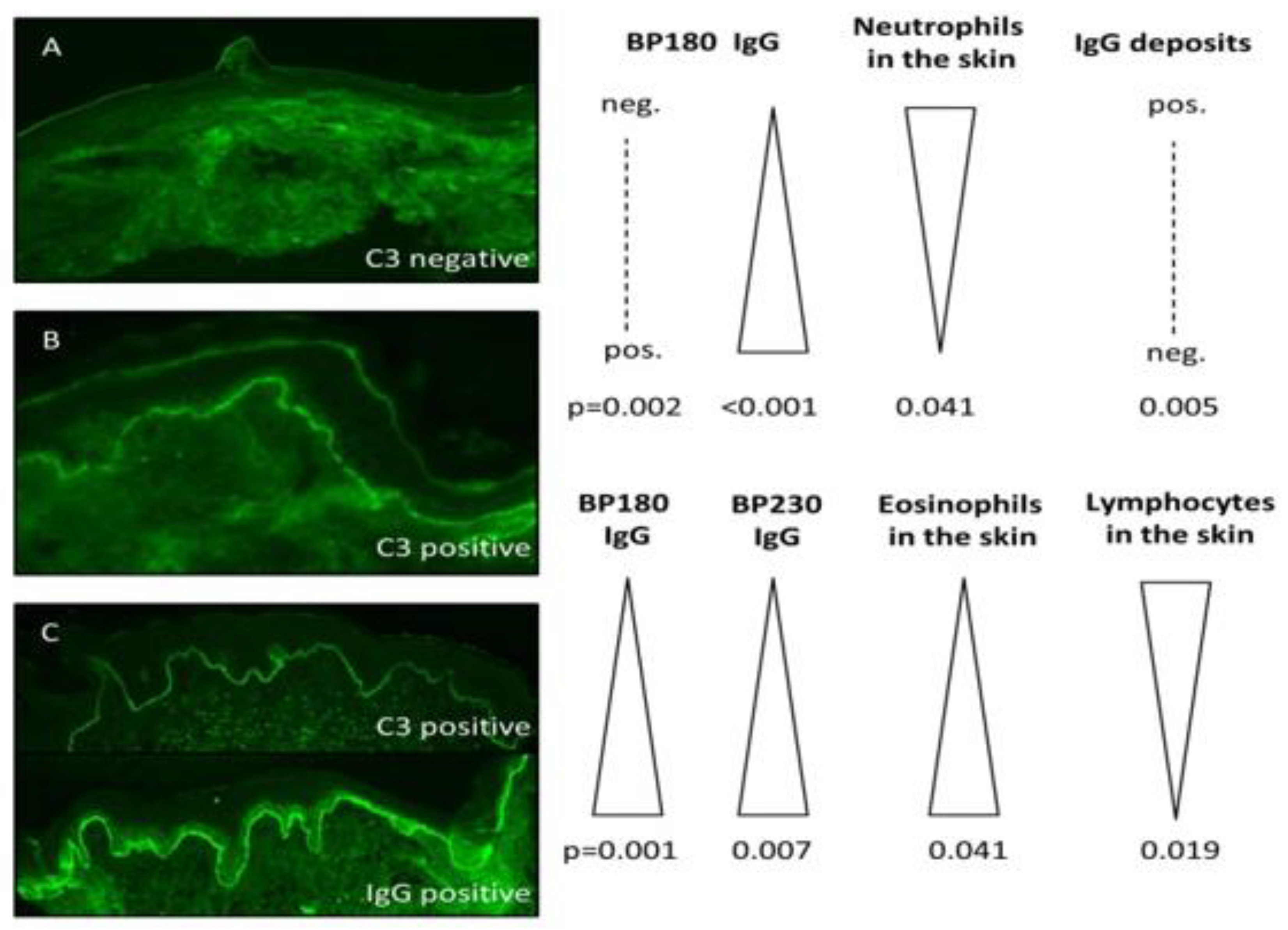
3.2. The Main Results of Direct Immunofluorescence Analysis
3.3. Features of Patients with C3 Deposition
3.4. Factors Associated with C3 Deposition
3.5. Features of Patients with Isolated C3 Deposition
4. Discussion
4.1. The Role of Complement in the Pathogenesis of BP
4.2. Interpretation of the Main Study Findings
4.3. Strengths and Limitations
Supplementary Materials
Author Contributions
Funding
Conflicts of Interest
References
- Schmidt, E.; Zillikens, D. Pemphigoid diseases. Lancet 2013, 381, 320–332. [Google Scholar] [CrossRef]
- Amber, K.T.; Murrell, D.F.; Schmidt, E.; Joly, P.; Borradori, L. Autoimmune Subepidermal Bullous Diseases of the Skin and Mucosae: Clinical Features, Diagnosis, and Management. Clin. Rev. Allergy Immunol. 2018, 54, 26–51. [Google Scholar] [CrossRef]
- Kridin, K.; Ahn, C.; Huang, W.C.; Ansari, A.; Sami, N. Treatment Update of Autoimmune Blistering Diseases. Dermatol. Clin. 2019, 37, 215–228. [Google Scholar] [CrossRef]
- Kridin, K.; Kowalski, E.H.; Kneiber, D.; Laufer-Britva, R.; Amber, K.T. From bench to bedside: Evolving therapeutic targets in autoimmune blistering disease. J. Eur. Acad. Dermatol. Venereol. 2019, jdv.15816. [Google Scholar] [CrossRef]
- Kridin, K.; Bergman, R. Mortality in Patients with Bullous Pemphigoid: A Retrospective Cohort Study, Systematic Review and Meta-analysis. Acta Derm. Venereol. 2018. [Google Scholar] [CrossRef] [Green Version]
- Van Beek, N.; Zillikens, D.; Schmidt, E. Diagnosis of autoimmune bullous diseases. J. Dtsch. Dermatol. Ges. 2018, 16, 1077–1091. [Google Scholar] [CrossRef] [Green Version]
- Edwards, G.; Diercks, G.F.H.; Seelen, M.A.J.; Horvath, B.; Van Doorn, M.B.A.; Damman, J. Complement activation in autoimmune bullous dermatoses: A comprehensive review. Front. Immunol. 2019, 10, 1477. [Google Scholar] [CrossRef] [Green Version]
- Liu, Z.; Giudice, G.J.; Swartz, S.J.; Fairley, J.A.; Till, G.O.; Troy, J.L.; Diaz, L.A. The role of complement in experimental bullous pemphigoid. J. Clin. Investig. 1995, 95, 1539–1544. [Google Scholar] [CrossRef] [Green Version]
- Heimbach, L.; Li, Z.; Berkowitz, P.; Zhao, M.; Li, N.; Rubenstein, D.S.; Diaz, L.A.; Liu, Z. The C5a receptor on mast cells is critical for the autoimmune skin-blistering disease bullous pemphigoid. J. Biol. Chem. 2011, 286, 15003–15009. [Google Scholar] [CrossRef] [Green Version]
- Nelson, K.C.; Zhao, M.; Schroeder, P.R.; Li, N.; Wetsel, R.A.; Diaz, L.A.; Liu, Z. Role of different pathways of the complement cascade in experimental bullous pemphigoid. J. Clin. Investig. 2006, 116, 2892–2900. [Google Scholar] [CrossRef]
- Natsuga, K.; Nishie, W.; Shinkuma, S.; Ujiie, H.; Nishimura, M.; Sawamura, D.; Shimizu, H. Antibodies to Pathogenic Epitopes on Type XVII Collagen Cause Skin Fragility in a Complement-Dependent and-Independent Manner. J. Immunol. 2012, 188, 5792–5799. [Google Scholar] [CrossRef] [Green Version]
- Ujiie, H.; Sasaoka, T.; Izumi, K.; Nishie, W.; Shinkuma, S.; Natsuga, K.; Nakamura, H.; Shibaki, A.; Shimizu, H. Bullous Pemphigoid Autoantibodies Directly Induce Blister Formation without Complement Activation. J. Immunol. 2014, 193, 4415–4428. [Google Scholar] [CrossRef] [Green Version]
- Iwata, H.; Kamio, N.; Aoyama, Y.; Yamamoto, Y.; Hirako, Y.; Owaribe, K.; Kitajima, Y. IgG from patients with bullous pemphigoid depletes cultured keratinocytes of the 180-kDa bullous pemphigoid antigen (type XVII collagen) and weakens cell attachment. J. Investig. Derm. 2009, 129, 919–926. [Google Scholar] [CrossRef] [Green Version]
- Hiroyasu, S.; Ozawa, T.; Kobayashi, H.; Ishii, M.; Aoyama, Y.; Kitajima, Y.; Hashimoto, T.; Jones, J.C.R.; Tsuruta, D. Bullous pemphigoid IgG induces BP180 internalization via a macropinocytic pathway. Am. J. Pathol. 2013, 182, 828–840. [Google Scholar] [CrossRef] [Green Version]
- Karsten, C.M.; Beckmann, T.; Holtsche, M.M.; Tillmann, J.; Tofern, S.; Schulze, F.S.; Heppe, E.N.; Ludwig, R.J.; Zillikens, D.; König, I.R.; et al. Tissue destruction in bullous pemphigoid can be complement independent and may be mitigated by C5aR2. Front. Immunol. 2018, 9, 488. [Google Scholar] [CrossRef]
- Chiorean, R.M.; Baican, A.; Mustafa, M.B.; Lischka, A.; Leucuta, D.C.; Feldrihan, V.; Hertl, M.; Sitaru, C. Complement-activating capacity of autoantibodies correlates with disease activity in bullous pemphigoid patients. Front. Immunol. 2018, 9, 2687. [Google Scholar] [CrossRef]
- Romeijn, T.R.; Jonkman, M.F.; Knoppers, C.; Pas, H.H.; Diercks, G.F.H. Complement in bullous pemphigoid: Results from a large observational study. Br. J. Dermatol. 2017, 176, 517–519. [Google Scholar] [CrossRef]
- Witte, M.; Zillikens, D.; Schmidt, E. Diagnosis of autoimmune blistering diseases. Front. Med. 2018, 5, 296. [Google Scholar] [CrossRef]
- Schmidt, E.; Sticherling, M.; Sárdy, M.; Goebeler, M.; Hertl, M.; Hofmann, S.C.; Hunzelmann, N.; Kern, J.S.; Kramer, H. S2k guidelines for the treatment of pemphigus vulgaris/foliaceus and bullous pemphigoid: 2019 update. J. Dtsch Derm. Ges 2020, 18, 516–526. [Google Scholar] [CrossRef]
- Murrell, D.F.; Daniel, B.S.; Joly, P.; Borradori, L.; Amagai, M.; Hashimoto, T.; Caux, F.; Marinovic, B.; Sinha, A.A.; Hertl, M.; et al. Definitions and outcome measures for bullous pemphigoid: Recommendations by an international panel of experts. J. Am. Acad. Derm. 2012, 66, 479–485. [Google Scholar] [CrossRef] [Green Version]
- Kridin, K. Peripheral eosinophilia in bullous pemphigoid: Prevalence and influence on the clinical manifestation. Br. J. Derm. 2018, 179, 1141–1147. [Google Scholar] [CrossRef]
- Nishie, W.; Sawamura, D.; Goto, M.; Ito, K.; Shibaki, A.; McMillan, J.R.; Sakai, K.; Nakamura, H.; Olasz, E.; Yancey, K.B.; et al. Humanization of autoantigen. Nat. Med. 2007, 13, 378–383. [Google Scholar] [CrossRef]
- Liu, Z.; Sui, W.; Zhao, M.; Li, Z.; Li, N.; Thresher, R.; Giudice, G.J.; Fairley, J.A.; Sitaru, C.; Zillikens, D.; et al. Subepidermal blistering induced by human autoantibodies to BP180 requires innate immune players in a humanized bullous pemphigoid mouse model. J. Autoimmun. 2008, 31, 331–338. [Google Scholar] [CrossRef] [Green Version]
- Li, Q.; Ujiie, H.; Shibaki, A.; Wang, G.; Moriuchi, R.; Qiao, H.; Morioka, H.; Shinkuma, S.; Natsuga, K.; Long, H.A.; et al. Human IgG1 Monoclonal Antibody against Human Collagen 17 Noncollagenous 16A Domain Induces Blisters via Complement Activation in Experimental Bullous Pemphigoid Model. J. Immunol. 2010, 185, 7746–7755. [Google Scholar] [CrossRef] [Green Version]
- Sitaru, C.; Mihai, S.; Otto, C.; Chiriac, M.T.; Hausser, I.; Dotterweich, B.; Saito, H.; Rose, C.; Ishiko, A.; Zillikens, D. Induction of dermal-epidermal separation in mice by passive transfer of antibodies specific to type VII collagen. J. Clin. Investig. 2005, 115, 870–878. [Google Scholar] [CrossRef] [Green Version]
- Karsten, C.M.; Pandey, M.K.; Figge, J.; Kilchenstein, R.; Taylor, P.R.; Rosas, M.; McDonald, J.U.; Orr, S.J.; Berger, M.; Petzold, D.; et al. Anti-inflammatory activity of IgG1 mediated by Fc galactosylation and association of FcγRIIB and dectin-1. Nat. Med. 2012, 18, 1401–1406. [Google Scholar] [CrossRef]
- Kasprick, A.; Holtsche, M.M.; Rose, E.L.; Hussain, S.; Schmidt, E.; Petersen, F.; Panicker, S.; Ludwig, R.J. The Anti-C1s Antibody TNT003 Prevents Complement Activation in the Skin Induced by Bullous Pemphigoid Autoantibodies. J. Investig. Derm. 2018, 138, 458. [Google Scholar] [CrossRef] [Green Version]
- Freire, P.C.; Muñoz, C.H.; Derhaschnig, U.; Schoergenhofer, C.; Firbas, C.; Parry, G.C.; Panicker, S.; Gilbert, J.C.; Stingl, G.; Jilma, B.; et al. Specific Inhibition of the Classical Complement Pathway Prevents C3 Deposition along the Dermal-Epidermal Junction in Bullous Pemphigoid. J. Investig. Derm. 2019, 139, 2417–2424. [Google Scholar] [CrossRef]
- Sezin, T.; Murthy, S.; Attah, C.; Seutter, M.; Holtsche, M.M.; Hammers, C.M.; Schmidt, E.; Meshrkey, F.; Mousavi, S.; Zillikens, D.; et al. Dual inhibition of complement factor 5 and leukotriene B4 synergistically suppresses murine pemphigoid disease. JCI Insight 2019, 4. [Google Scholar] [CrossRef]
- Verschoor, A.; Brockman, M.A.; Knipe, D.M.; Carroll, M.C. Cutting Edge: Myeloid Complement C3 Enhances the Humoral Response To Peripheral Viral Infection. J. Immunol. 2001, 167, 2446–2451. [Google Scholar] [CrossRef]
- Yalcindag, A.; He, R.; Laouini, D.; Alenius, H.; Carroll, M.; Oettgen, H.C.; Geha, R.S. The complement component C3 plays a critical role in both T H1 and T H2 responses to antigen. J. Allergy Clin. Immunol. 2006, 117, 1455–1461. [Google Scholar] [CrossRef] [PubMed]
- Dainichi, T.; Nishie, W.; Yamagami, Y.; Sonobe, H.; Ujiie, H.; Kaku, Y.; Kabashima, K. Bullous pemphigoid suggestive of complement-independent blister formation with anti-BP180 IgG4 autoantibodies. Br. J. Dermatol. 2016, 175, 187–190. [Google Scholar] [CrossRef] [PubMed]
- Sitaru, C.; Mihai, S.; Zillikens, D. The relevance of the IgG subclass of autoantibodies for blister induction in autoimmune bullous skin diseases. Arch. Dermatol. Res. 2007, 299, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shiraishi, S.; Iio, T.; Shirakata, Y.; Sayama, K.; Nishimukai, H.; Miki, Y. Bullous pemphigoid in a patient with a C4 deficiency. Br. J. Derm. 1991, 124, 296–298. [Google Scholar] [CrossRef]
- Tsuji-Abe, Y.; Akiyama, M.; Yamanaka, Y.; Kikuchi, T.; Sato-Matsumura, K.C.; Shimizu, H. Correlation of clinical severity and ELISA indices for the NC16A domain of BP180 measured using BP180 ELISA kit in bullous pemphigoid. J. Derm. Sci. 2005, 37, 145–149. [Google Scholar] [CrossRef]
- Daneshpazhooh, M.; Ghiasi, M.; Lajevardi, V.; Nasiri, N.; Balighi, K.; Teimourpour, A.; Khosravi, H.; Saeidi, V.; Mahmoudi, H.; Chams-Davatchi, C. BPDAI and ABSIS correlate with serum anti-BP180 NC16A IgG but not with anti-BP230 IgG in patients with bullous pemphigoid. Arch. Derm. Res. 2018, 310, 255–259. [Google Scholar] [CrossRef]
- Schmidt, E.; Obe, K.; Bröcker, E.B.; Zillikens, D. Serum levels of autoantibodies to BP180 correlate with disease activity in patients with bullous pemphigoid. Arch. Derm. 2000, 136, 174–178. [Google Scholar] [CrossRef] [Green Version]
- Van Beek, N.; Lüttmann, N.; Huebner, F.; Recke, A.; Karl, I.; Schulze, F.S.; Zillikens, D.; Schmidt, E. Correlation of serum levels of ige autoantibodies against BP180 with bullous pemphigoid disease activity. JAMA Dermatol. 2017, 153, 30–38. [Google Scholar] [CrossRef]
- Lin, L.; Betsuyaku, T.; Heimbach, L.; Li, N.; Rubenstein, D.; Shapiro, S.D.; An, L.; Giudice, G.J.; Diaz, L.A.; Senior, R.M.; et al. Neutrophil elastase cleaves the murine hemidesmosomal protein BP180/type XVII collagen and generates degradation products that modulate experimental bullous pemphigoid. Matrix Biol. 2012, 31, 38–44. [Google Scholar] [CrossRef] [Green Version]
- Schmidt, E.; Reimer, S.; Kruse, N.; Jainta, S.; Bröcker, E.B.; Marinkovich, M.P.; Giudice, G.J.; Zillikens, D. Autoantibodies to BP180 associated with bullous pemphigoid release interleukin-6 and interleukin-8 from cultured human keratinocytes. J. Investig. Derm. 2000, 115, 842–848. [Google Scholar] [CrossRef] [Green Version]
- Schulze, F.S.; Beckmann, T.; Nimmerjahn, F.; Ishiko, A.; Collin, M.; Köhl, J.; Goletz, S.; Zillikens, D.; Ludwig, R.; Schmidt, E. Fcγ receptors III and IV mediate tissue destruction in a novel adult mouse model of bullous pemphigoid. Am. J. Pathol. 2014, 184, 2185–2196. [Google Scholar] [CrossRef] [PubMed]
- Luo, Y.; Tan, G.; Yu, M.; Li, K.; Liu, Y.; Guo, Q.; Zeng, F.; Wang, L. Correlation of Cutaneous Immunoreactants in Lesional Skin with the Serological Disorders and Disease Activity of Systemic Lupus Erythematosus. PLoS ONE 2013, 8, e70983. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| BP with C3 Deposition (n = 196) | BP without C3 Deposition (n = 37) | p Value | |
|---|---|---|---|
| Age at diagnosis; years | |||
| Mean (SD) | 79.1 (10.1) | 80.0 (7.7) | 0.613 |
| Median (range) | 80.6 (49.6–98.2) | 80.7 (64.4–96.6) | |
| Sex, n (%) | |||
| Male | 85 (43.4%) | 16 (43.2%) | 0.989 |
| Female | 111 (56.6%) | 21 (56.8%) | |
| Distribution of bullous lesions; n (%) | |||
| Head and neck | 54 (27.6%) | 9 (24.3%) | 0.685 |
| Trunk | 146 (74.5%) | 28 (75.7%) | 0.879 |
| Limbs | 161 (82.1%) | 35 (94.6%) | 0.057 |
| Hands/feet | 83 (42.3%) | 12 (32.4%) | 0.260 |
| Mucous membranes | 25 (12.8%) | 1 (2.7%) | 0.075 |
| DPP4i-associated BP, n (%) | 17 (8.7%) | 4 (10.8%) | 0.677 |
| Mean BPDAI severity score (SD) a | |||
| Erosion/blister cutaneous activity | 22.2 (16.0) | 18.4 (10.5) | 0.341 |
| Urticaria/Erythema activity | 12.4 (15.3) | 15.5 (17.2) | 0.492 |
| Pruritus score | 18.5 (9.3) | 21.8 (8.1) | 0.152 |
| Damage score | 2.3 (3.4) | 1.7 (2.2) | 0.352 |
| BP with C3 Deposition (n = 196) | BP without C3 Deposition (n = 37) | p Value | |
|---|---|---|---|
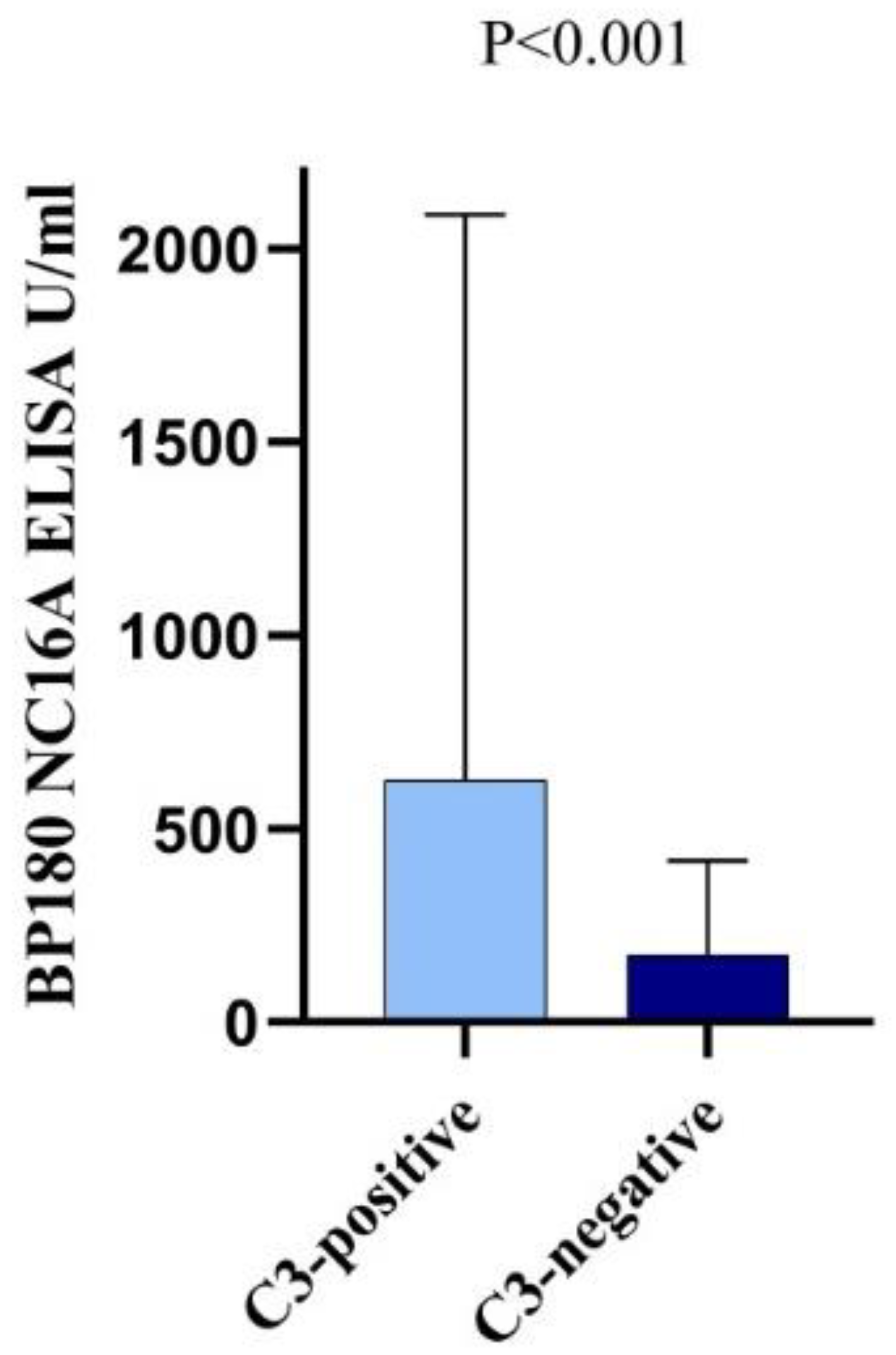
| BP180 NC16A ELISA a | |||
| Seropositivity, n (%) | 164 (86.3%) | 24 (64.9%) | 0.002 |
| ELISA value, mean (SD); U/mL | 645.2 (1418.5) | 172.5 (243.9) | <0.001 |
| BP230 ELISA b | |||
| Seropositivity, n (%) | 25 (48.1%) | 7 (43.8%) | 0.762 |
| ELISA value, mean (SD); U/mL | 79.7 (160.5) | 181.8 (483.1) | 0.418 |
| Indirect immunofluorescence seropositivity, n (%) | |||
| Salt split human skin c | 180 (93.8%) | 34 (91.9%) | 0.676 |
| Monkey esophagus d | 148 (78.3%) | 30 (81.1%) | 0.706 |
| Linear deposits of immunoreactants by direct immunofluorescence, n (%) | |||
| IgG | 152 (77.6%) | 36 (97.3%) | 0.005 |
| IgA | 18 (9.2%) | 5 (13.5%) | 0.418 |
| IgM | 6 (3.1%) | 1 (2.7%) | 0.907 |
| Two immunoreactant deposition | 134 (68.4%) | 5 (13.5%) | <0.001 |
| Three immunoreactant deposition | 21 (10.7%) | 0 (0.0%) | 0.037 |
| Histological findings, n (%) | |||
| Cell-rich infiltrate e | 59 (80.8%) | 8 (66.7%) | 0.266 |
| Dominance of eosinophils f | 89 (80.2%) | 12 (66.7%) | 0.197 |
| Dominance of neutrophils f | 6 (5.4%) | 1 (5.6%) | 0.979 |
| Dominance of lymphocytes f | 16 (14.4%) | 5 (27.8%) | 0.154 |
| Presence of eosinophils g | 122 (93.1%) | 19 (90.5%) | 0.663 |
| Presence of neutrophils g | 39 (29.8%) | 11 (52.4%) | 0.041 |
| Presence of lymphocytes g | 84 (64.1%) | 18 (85.7%) | 0.051 |
| Eosinophil count, mean (SD); cells/µL h | 1295.0 (1072.9) | 1026.3 (749.8) | 0.909 |
| C-reactive protein, mean (SD); mg/L i | 29.2 (26.7) | 32.2 (38.4) | 0.736 |
| Univariate OR | 95% Confidence Interval | p Value | Multivariate OR | 95% Confidence Interval | p Value | |
|---|---|---|---|---|---|---|
| Age at diagnosis ≥80.6 years | 0.95 | 0.47–1.91 | 0.880 | |||
| Male sex | 1.01 | 0.50–2.04 | 0.989 | |||
| Head and neck involvement | 1.18 | 0.52–2.67 | 0.685 | |||
| Trunk involvement | 0.94 | 0.42–2.12 | 0.685 | |||
| Limbs involvement | 0.26 | 0.06–1.14 | 0.057 | 0.87 | 0.17–4.52 | 0.873 |
| Hand and feet involvement | 1.53 | 0.73–3.22 | 0.260 | |||
| Mucosal involvement | 5.26 | 0.69–40.11 | 0.075 | 2.26 | 0.27–19.3 | 0.455 |
| BP180 NC16A ELISA seropositivity | 3.42 | 1.55–7.54 | 0.002 | 4.25 | 1.38–13.05 | 0.012 |
| BP230 ELISA seropositivity | 1.19 | 0.39–3.68 | 0.762 | |||
| Positive indirect immunofluorescence | ||||||
| Salt-split human skin | 1.32 | 0.36–4.94 | 0.676 | |||
| Monkey esophagus | 0.84 | 0.35–2.06 | 0.706 | |||
| Linear deposits of immunoreactants in direct immunofluorescence | ||||||
| IgG | 0.10 | 0.01–0.72 | 0.005 | 0.20 | 0.02–1.84 | 0.156 |
| IgA | 0.65 | 0.22–1.87 | 0.418 | |||
| IgM | 1.14 | 0.13–9.73 | 0.907 | |||
| Histology | ||||||
| Cell-rich infiltrate | 2.11 | 0.55–8.00 | 0.266 | |||
| Presence of eosinophils | 1.43 | 0.29–7.11 | 0.663 | |||
| Presence of neutrophils | 0.39 | 0.15–0.98 | 0.041 | 0.33 | 0.12–0.91 | 0.033 |
| Presence of lymphocytes | 0.30 | 0.08–1.06 | 0.051 | 0.32 | 0.08–1.23 | 0.098 |
| Peripheral eosinophilia | 0.69 | 0.14–3.29 | 0.641 |
| BP with Isolated C3 Deposition (n = 41) | BP with C3 Alongside Other Immunoreactants Deposition (n = 155) | p Value | |
|---|---|---|---|
| Age at diagnosis; years | |||
| Mean (SD) | 78.0 (11.6) | 79.4 (9.7) | 0.437 |
| Sex, n (%) | |||
| Male | 16 (39.0%) | 69 (44.5%) | 0.528 |
| Female | 25 (61.0%) | 86 (55.5%) | |
| DPP4i-associated BP, n (%) | 3 (7.3%) | 14 (9.0%) | 0.677 |
| Mean BPDAI severity score (SD) a | |||
| Erosion/blister cutaneous activity | 17.7 (16.0) | 18.4 (10.5) | 0.173 |
| Urticaria/Erythema activity | 12.4 (14.9) | 23.2 (16.1) | 0.185 |
| Pruritus score | 16.3 (9.8) | 19.1 (9.2) | 0.255 |
| Damage score | 2.5 (3.5) | 2.3 (3.4) | 0.860 |
| BP180 NC16A ELISA b | |||
| Seropositivity, n (%) | 30 (78.9%) | 134 (88.2%) | 0.140 |
| ELISA value, mean (SD); U/mL | 273.6 (388.3) | 738.1 (1561.5) | 0.001 |
| BP230 ELISA c | |||
| Seropositivity, n (%) | 3 (30.0%) | 22 (52.4%) | 0.203 |
| ELISA value, mean (SD); U/mL | 16.7 (20.0) | 94.7 (175.4) | 0.007 |
| Indirect immunofluorescence seropositivity, n (%) | |||
| Salt split human skin d | 34 (85.0%) | 146 (96.1%) | 0.010 |
| Monkey esophagus e | 28 (70.0%) | 120 (80.5%) | 0.151 |
| Histological findings in lesional skin specimens, n (%) | |||
| Cell-rich infiltrate f | 7 (87.5%) | 52 (80.0%) | 0.611 |
| Dominance of eosinophils g | 12 (63.2%) | 77 (83.7%) | 0.041 |
| Dominance of neutrophils g | 1 (5.3%) | 5 (5.4%) | 0.976 |
| Dominance of lymphocytes g | 6 (31.6%) | 10 (10.9%) | 0.019 |
| Presence of eosinophils h | 19 (90.5%) | 103 (93.6%) | 0.600 |
| Presence of neutrophils h | 6 (28.6%) | 33 (30.0%) | 0.896 |
| Presence of lymphocytes h | 14 (66.7%) | 70 (63.6%) | 0.791 |
| Eosinophil count, mean (SD); cells/µL i | 1038.9 (886.6) | 1386.1 (1122.9) | 0.150 |
| C-reactive protein, mean (SD); mg/L j | 27.2 (26.5) | 29.7 (26.9) | 0.753 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2020 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ständer, S.; Holtsche, M.M.; Schmidt, E.; Hammers, C.M.; Zillikens, D.; Ludwig, R.J.; Kridin, K. Presence of Cutaneous Complement Deposition Distinguishes between Immunological and Histological Features of Bullous Pemphigoid—Insights from a Retrospective Cohort Study. J. Clin. Med. 2020, 9, 3928. https://doi.org/10.3390/jcm9123928
Ständer S, Holtsche MM, Schmidt E, Hammers CM, Zillikens D, Ludwig RJ, Kridin K. Presence of Cutaneous Complement Deposition Distinguishes between Immunological and Histological Features of Bullous Pemphigoid—Insights from a Retrospective Cohort Study. Journal of Clinical Medicine. 2020; 9(12):3928. https://doi.org/10.3390/jcm9123928
Chicago/Turabian StyleStänder, Sascha, Maike M. Holtsche, Enno Schmidt, Christoph M. Hammers, Detlef Zillikens, Ralf J. Ludwig, and Khalaf Kridin. 2020. "Presence of Cutaneous Complement Deposition Distinguishes between Immunological and Histological Features of Bullous Pemphigoid—Insights from a Retrospective Cohort Study" Journal of Clinical Medicine 9, no. 12: 3928. https://doi.org/10.3390/jcm9123928